3. Literature Review
The links between the quality of the environment and the population health, the incidence of illnesses and deaths and their burden on public health expenditure are scientifically and practically proven facts. Researchers and policymakers, however, need to understand the reasons behind the occurrence of these situations and what actions are to be taken in healthcare and health related spending. Thus, by carefully calibrating these measures, policymakers can either resize these expenditures or maximize the effect of the funds available for health-care, and subsequently, for the environmental protection.
According to The European Health Report 2012, the social and environmental determinants of healthcare comprise a full set of social and physical conditions in which people live and work, including socioeconomic (i.e., income level and security, employment, gender and years of education), demographic, environmental and cultural factors, together with the healthcare system [
20]. Alongside income (or GDP/capita), which is considered the most important factor explaining differences across countries regarding the level and growth of total healthcare expenditures [
23,
24,
25,
26,
27], scholars and practitioners include population age structure and epidemiological needs [
28,
29], technological progress and variation in medical practice [
30] and health system characteristics, through service provision [
31], financing structure [
26] and external funds (especially in developing countries) [
29,
32,
33,
34]. Income (at national and individual level) is, however, not the only factor associated with health-care spending, and data show notable differences regarding health-care spending between countries with similar income levels. Moreover, Hansen and King [
35] considered that income levels could not be sufficient enough to assess health-care expenditure, and Blomqvist and Carter [
36] demonstrated that health expenditure could increase faster than economic growth rates.
In different words, the socio-economic viewpoint is far from being complete, and many researchers consider that, in the last century, socio-economic determinants had excessively shaped the philosophy and actions undertaken in the field of public health; meanwhile, the environment and natural systems have been considered as implicit support and a (practically inexhaustible) resource for human development [
2], and “somehow, modern public health had almost forgotten the primacy of the human environmental interface, despite this being a component part of the original sanitarian vision” [
37]. Therefore, many researchers and international decision-making organizations consider that environmental determinants should be included in the public health equation.
Despite a plethora of literature concerning the relationship between health expenditure and economic growth (estimated by GDP/capita), there are relatively few studies addressing the influence of multiple determinants (such as economic growth, renewable energy consumption and the environmental protection expenses) on health expenditure. Thus, in the following paragraphs, we will firstly review the studies addressing the impact of environmental pollution (air, in particular, as well as water and soil), and afterwards, those related to the issue of renewable energy.
3.1. Health Expenditure, Economic Growth and Air Pollution
Jerrett et al. [
38] explored the relationship between health care expenditures and environmental factors in Canada, and found that both the total toxic pollutant emissions and per capita environmental expenditures are in a significant relationship with health expenditure. They argue that higher pollution regions/countries report higher per capita health expenditure, while environmental investments and responsible environmental behavior lead to lower healthcare spending. In the case of developed economies (i.e., Australia, by analyzing the relationship environmental quality, or degradation, and health expenditure) over the 1995–2017 time period, Moosa [
39] arrived at a rather unusual (counter-intuitive) conclusion: when a country is on a downward Environmental Kuznets Curve (EKC), healthcare expenditure is negatively related to environmental degradation. Apergis et al. [
40] found a positive impact of CO
2 emissions on health-care spending in 50 U.S. states and this effect is stronger for those states which allocate higher funds for health-care expenditure. Blázquez-Fernández et al. [
41] analyzed the impact of per capita income and environmental air quality variables on health expenditure determinants in 29 OECD countries, during the 1995–2014 time period. Their results show that per capita income has a positive effect on health expenditure, but this relationship is not as statistically significant as expected when lag-time is incorporated [
41] (p. 389). The authors try to answer the question regarding how air pollution could affect health care expenditure by including in the relationship between health expenditures and income (per capita) several other air-pollutants, such as nitrogen oxides, sulfur oxide and carbon monoxide emissions. Their conclusions show clear health related benefits, and implicitly, savings on health care expenditure, when decision-makers support and promote growth based on cleaner fuels and pay more attention to the quality of the environment. However, different levels of economic development, budgetary restrictions and constraints, various fiscal policy frameworks, or health policies result in different outcomes and results in each country.
Other researches show that the effects of environmental degradation and, implicitly, air pollution are more severe in developing countries [
42], making it more complicated to counter the negative effects and improve healthcare. Preker et al. [
43] estimated the total tangible healthcare expenditure attributable to human pollution affecting air, soil and water. The conclusions, although somewhat expected, are alarming in terms of the negative impact of pollution, especially for fragile healthcare systems in poor countries. Thus, for 2013, the authors found that healthcare expenditure attributable to man-made pollution accounts between 3% and 9% of global spending on health care. Although the expenditure levels of developing countries hold a share of below 15% of this total, “the relative share of spending for pollution related illness is substantial, especially in very low-income countries. Cancer, chronic respiratory and cardio/cerebrovascular illnesses account for the largest health care spending items linked to pollution even in lower- and middle-income countries” [
43] (p. 711). The authors pointed out that when adding to the expenditure list the intangible losses and the opportunity costs generated by lower labor productivity due to polluted environment, the financial impact of pollution on health becomes quite substantial, both at individual (or household) level and national level, and especially among the poorly developed countries [
44].
By analyzing Sub-Saharan African Countries, Zaman et al. [
45] found out that although increasing consumption of fossil fuel energy is associated with GDP growth, and implicitly the possibility of additional health allocations and increased life expectancy, it is also associated with carbon dioxide emissions, which increase spending on health per capita. On one hand, increases in life expectancy significantly decrease the health care provisions of per capita health levels; on the other hand, life expectancy is negatively affected by poor sanitation and low environmental protection spending levels, which also adds to the budgets dedicated to healthcare expenditures.
The case of China, from this point of view at least, is paradigmatic. Thus, many researchers have noted that China’s rapid economic growth has been accompanied by a considerable increase in pollution, which has caused extensive damage to the health of its inhabitants, and has implicitly altered public health spending; in the same time, it has also increased inequalities. Hence, Yang and Liu [
46] have shown that the deterioration of health caused by pollution further increases the inequality of access to healthcare services, affects the level of disposable income and its share budgeted for healthcare. The research findings highlight that the negative effects are particularly acute for people with low incomes coming from poor rural areas, thus validating, to some extent at least, the concept of an “environment-health-poverty trap”. Lu et al. [
47], by investigating 30 Chinese provinces between 2002–2014, or Hao et al. [
48], by using panel data on Chinese provinces for 1998–2015 time period, proved the negative effect of environmental pollution on public health, increased medical expenses of Chinese residents, but also that public services and education can contribute to the decrease of the individual burden of medical expenses.
Using a model examining the relationship between health expenditure, income, CO
2 emissions and PM
10 (particulate matter) emissions, for a panel of MENA (Middle East and North Africa) countries during 1995–2014, Khoshnevis Yazdi and Khanalizadeh [
49] found an “overwhelming evidence between health expenditures and its determinants” [
49] (p. 1189). Thus, economic growth in these countries will increase the consumption of fossil fuels, environmental degradation, and will lead to higher risk of pollution-induced health diseases and mortality. They will lead to an increase in healthcare expenditures as share of the GDP, but in the context of significant budget constraints, this means diminishing funds allocated towards other sectors (such as education or environmental protection). However, without adequate education and with poor environmental protection, the negative health effects will worsen and the vicious circle will continue. Even so, the authors state that the only solution is to raise real GDP in MENA countries, in order to create resources available for investments in key sectors (including the health sector).
Ghorashi and Alavi Rad [
50] examined the causal relationship between CO
2 emissions, health expenditures and economic growth, by using dynamic simultaneous equation models for Iran over the 1972–2012 time period. Their results confirm previous studies [
51,
52,
53] regarding the bidirectional causality relationship between CO
2 emissions and economic growth, and, respectively, the unidirectional causality relationship between health expenditures and economic growth. The authors show that without an active environmental protection policy and an increase of technological transfer pace, the environmental damage can severely affect both the health levels of the population, but it can also compromise economic development. A similar solution, of “controlling pollution, particularly CO
2 emissions and health expenditures without compromising economic growth” has been proposed also for the case of Pakistan by Wang et al. [
54], who found a bidirectional relationship between health expenditures and CO
2 emissions, and between health expenditure and economic growth in the long run, as well as a unidirectional causality from carbon emissions to health-related expenditures in the short-run.
3.2. Health Expenditure, Economic Growth and Renewable Energy
Although relatively newly addressed, the relationship between renewable energy and health expenditure can provide valuable insights for better understand the nexus health expenditure—GDP environment. Romm and Ervin [
55] considered that “the vast majority of air pollution is energy related”; as the world’s states develop, they require increased amounts of energy, which is typically produced from traditional resources and by using pollution-intensive methods. Thus, we note that “environmental problems at an urban, regional, and global levels will be seriously aggravated, at a terrible cost to human health and quality of life” [
55] (p. 398). For these authors, the key of sustainable development is through pollution prevention and resource-efficient technologies, in order to improve the environment, while at the same time lowering the energy bills of consumers and businesses. Without adhering to a certain type of economic intervention, they admit that this option requires large levels of public (and private) investments, enforcement measures and sanctions; however, the alternatives are simple: we either have a “sustainable, profitable, and environmentally sound” development, or a “on short term, costly, and potentially devastating from an environmental and human health perspective” [
55] (p. 398) type of development. Higher costs related to the implementation and support of renewable energy can be recovered, however, from the health-related savings associated with the effects of pollution. In different words, investments in sustainable development are “the nexus of energy, transportation, air quality, climate change and health” [
56] (p. 48); these investment will lead to a reduction in carbon emissions, which will significantly improve the health problems associated with climate change and air pollution, and said investments will implicitly reduce the burden of health costs associated to the quality of the environment. In fact, the environmental risk factors identified as responsible for the majority of disease burdens and for the excessive overloading of health-care spending can largely be avoided by implementing effective and sustainable policy interventions: improving air quality, access to safe drinking and sewage, sanitation and clean energy sources and by significantly contributing “to the achievement of the Millennium Development Goals of environmental sustainability, health and development” [
57] (p. 2182).
Ben Jebli [
58] investigated the relationship between health, real GDP, combustible renewables and waste consumption, rail transportation and carbon dioxide (CO
2) emissions for the case of Tunisia for the 1990–2011 period. He found that, in the short-run, there is a unidirectional causality ranging from real GDP to health, from health-care to combustible renewables and waste consumption and from all variables to CO
2 emissions. In the long run, combustible renewables and waste consumption have a positive and statistically significant impact on health levels, while CO
2 emissions and rail transportation both contribute to the decrease of the health indicator. Similar to Romm and Ervin [
55] or Erickson and Jennings [
56], Ben Jebli [
58] proposes to decision-makers to exploit waste and renewable fuels, to use renewable energy for national rail transportation, to invest in renewable energy projects in order to eliminate pollution caused by emissions, thus ensuring the economy’s growth and to reduce energy dependence, and subsequently, to improve health quality.
In a study aimed at investigating the long run relationship between health expenditure, real income, CO
2 emissions and renewable energy consumption (all per capita) for BRICS-T countries (Brazil, Russia, India, China, South Africa, Turkey) during 2000–2015, Çetin [
59] confirmed that when “CO
2 emissions per capita increases, health expenditure per capita will also increase due to the worsened health status caused by the pollution effect” [
59] (p. 365). Moreover, he showed that “renewable energy sources not only support sustainable development but they also mitigate health costs and increase the savings levels even the impact of CO
2 emissions on health expenditure is still stronger than the remedial impact of renewable energy sources” [
59] (pp. 365–366), i.e., the renewable energy sources could temper health expenses for environmental attributable diseases, but not decisively. In a study conducted on a panel of ASEAN (Association of South East Asian Nations) member states, Khan [
60] confirmed that polluting industrial activities and CO
2 emissions “have both a significant and negative effect on human health and environmental sustainability and increase the public health expenditure” [
60]; meanwhile, the use of renewable energy will assist in the increase of economic performance and implicitly, aid in the efforts to increase environmental protection.
4. Data and Methodology
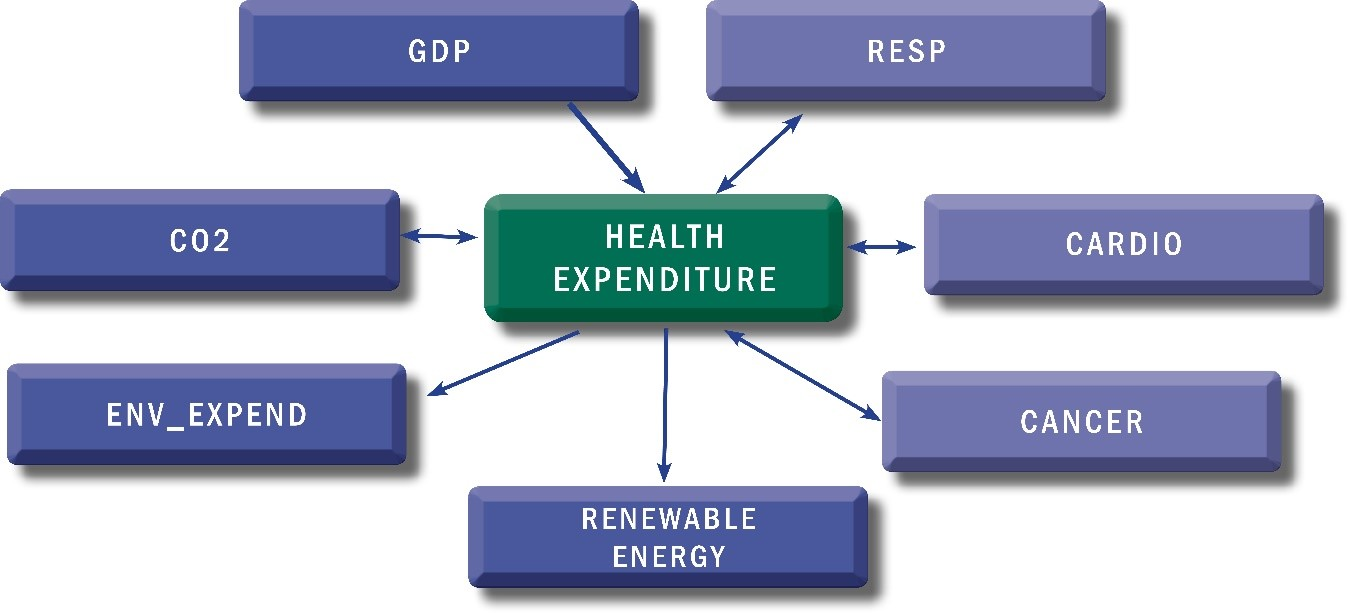
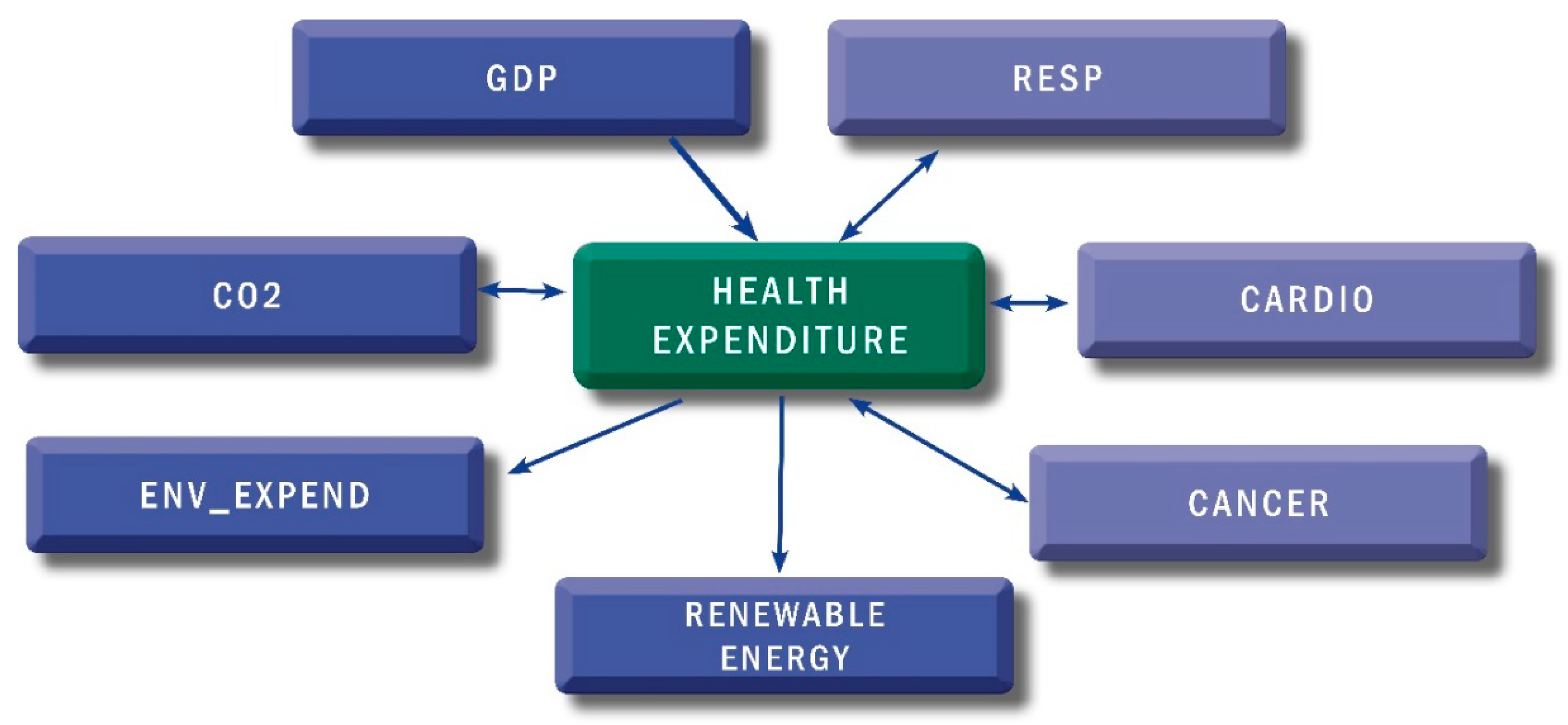
In this article, we aim at examining the long-term relationship between health expenditure (HE) and other determinants, such as: Gross Domestic Product per capita (GDP), emissions of carbon dioxide (CO
2), environmental expenditure (ENV), renewable energy consumption (RENEW) and deaths caused by non-communicable diseases (NCDs) in the 28 European Union countries. For the purpose of this study we consider the following series as proxies of non-communicable diseases: (1) the diseases of the respiratory system (RESP), (2) the diseases of the circulatory system (CARDIO) and (3) the malignant neoplasms (CANCER), which are considered (alongside diabetes) as major NCDs in the EU [
21]. Regarding the selection of variables, some considerations are necessary: we have selected all deaths caused by NCDs, i.e., RESP, CARDIO and CANCER, although some cardiac diseases and many respiratory diseases are sustained through infectious (aggravated or not by the presence of the environmental risk factors or changes in climate [
7] and [
61]), given that the main database we used does not discriminate more in-depth [
62]. Moreover, risks factors for non-communicable diseases also come from other areas, but are related to the environment, i.e., overweight, low physical activity and unintentional and intentional injuries [
7]. For example, at a global level, environmental factors accounted for 19% of the injuries from interpersonal violence [
7]. However, given the above-mentioned statistical reasons, the deaths due to unintentional injuries (i.e., road traffic accidents, unintentional poisonings, falls, fires, drownings) or intentional injuries (i.e., self-harm or interpersonal violence), although related to environmental risk factors or country income level, have not been considered for the purposes of the present analysis.
In order to evaluate the relationship between these variables, we have used a panel data analysis. The panel data were retrieved from the earliest possible year, namely the year 2000, and continued until the last available year, namely 2014, and a balanced panel of these countries was constructed.
Table 3 provides information about variables and the sources of data. Since all variables are expressed in different units of measurement (i.e., current prices, current international
$, metric tons, terajoule), before analyzing any aggregation, the data needed to be transformed into a normal form. Thus, we converted the variables into their natural logarithmic forms, as the natural logarithms of all variables smooth out the entire data used for analysis. Additionally, if the coefficients are estimated by variables that have been transformed into their natural logarithmic forms, the results can be interpreted in terms of elasticity.
Time series variables have different properties, such as those related to stationarity. The testing of stationarity can be performed by unit root tests, which can be determined on the basis of a presumption of cross section independence. For panel data, the variables of the analyzed countries are correlated with each other due to regional interconnections between these countries. Thus, in order to test for cross section dependence, we used the Lagrange multiplier (LM) test of Breusch and Pagan [
65], and the cross-sectional dependence (CD) test suggested by Pesaran [
66]. The equation of the LM test according to Breusch and Pagan is:
These tests have as null hypotheses the cross-sectional independence and the alternative hypotheses is cross-sectional dependence. Given the shortcomings of the Breusch and Pagan LM test when N is high, Pesaran [
66] proposed an alternative based on pairwise correlation coefficients rather than their squares used in the LM test. Thus, the equation of the CD test is:
where N denotes the sample size, T denotes the time period of the study and
denotes the correlations’ coefficients of the residuals of different cross-sections of country i and j.
In
Table A1, we present the results of cross-sectional dependence by using the LM test suggested by Breusch and Pagan [
65] and CD test suggested by Pesaran [
66]. The results demonstrate that the null hypotheses regarding the cross-sectional independence is rejected and the alternative hypotheses regarding cross-sectional dependence is accepted at the significant level of 1%.
After the confirmation of the cross-sectional dependence, the next step of the empirical analysis is to determine whether the series are stationary. In this regard, we employed three different types of panel unit root tests: Im, Pesaran and Shin W-stat [
67], ADF—Fisher Chi-square [
68] and PP—Fisher Chi-square [
69]. It is important to note that all the series have the same order of integration. Thus, if the series are not stationary at the same level, cointegration analysis cannot be used. In this regard, if some series are stationary at level and others are stationary on first difference level, the ARDL (Autoregressive Distributed Lag) Bounds test will be used. It allows the use of data with different levels of stationarity, but limited at level I (0) and I (1) or a mixture of both and it can also estimate the cointegration equation with a very small number of sample cases (see Pesaran and Smith [
70], Pesaran et al. [
71,
72]).
Table A2 shows the results of unit root tests, indicating that all variables are stationary (at a significance level of 5%) at first difference with intercept, except the variable Diseases of the respiratory system (RESP), which is stationary at its level, at a significance level of 5%. Therefore, we can state that our data suffers from either I (0) or I (1), and in addition, these estimations give us the possibility of estimating the short and long-run relationships along with the error correction coefficient. Moreover, as variables are static at level or on their first differences levels, applying cointegration analysis on the variables is possible.
In order to study the cointegration, the Pedroni Johansen cointegration and the Fisher test were performed. The results are presented in
Table A3. We estimated the Pedroni [
73] heterogenous panel cointegration test and used the panel fixed effect estimators [
74]. The panel tests proposed by Pedroni [
73] are based on the within-dimension approach, while the group tests are based on the between-dimension approach. The first includes four statistics: panel v-Statistic, panel rho-Statistic, panel PP-Statistic and panel ADF-statistics, while the group tests include three statistics: group rho-Statistic, group PP-Statistic and group ADF-statistics. All seven statistics are based on an average of the individual autoregressive coefficient related to the residual unit root tests of each country belonging to the panel data set. Considering the first panel cointegration tests, for two out of four Pedroni tests (i.e., panel PP-statistic and panel ADF-statistic), the null hypothesis suggests that there is a cointegration between the variables. Thus, we can state that there is a long-run relationship between health expenditure, GDP, CO
2 emissions, renewable energy and non-communicable diseases. Similarly, for the group test based on between dimensions, the null hypothesis suggests that the variables are cointegrated for two out of three tests (i.e., group PP-Statistic and group ADF-statistics). According to previous literature, the results of the PP group statistics, which are both heterogeneous and non-parametric, are considered as having the highest power in the Pedroni test. In our case, the statistics of this group PP reject the null hypothesis due to a lack of cointegration at a certain level of significance, and in conclusion, the variables are cointegrated.
To estimate the long- and short-term relationship between studied variables, and also in order to investigate the possible heterogeneous dynamic problem in different countries, the most appropriate method that can be used for the analysis of dynamic panels is the ARDL (p, q) model in the error correction form. The model estimation will be based on the Pooled mean group (PMG) developed by Pesaran et al. [
71]. The general ARDL specification is formulated as follows:
where i represents the number of cross sections (i = 1, 2, …, N), t represents the time (t = 1, 2, …, T),
is a vector of K × 1 explanatory variables for group i and
represents the fixed effect.
A specific feature of co-integrated variables is their response to any deviation from long-term equilibrium. This feature is based on the error correction dynamics of the variables in the system that are affected by the deviation from equilibrium. Thus, this equation can be re-parametrized [
75] into the error correction (ECM) equation:
where y is the natural logarithm of health expenditure per capita, X is a set of independent variables including the natural logarithm of GDP, CO
2, renewable energy, environmental expenditure and non-communicable diseases and
and
represent the short-run coefficients of exogenous and endogenous variables respectively.
is the error correction parameters that measure the speed of adjustment and
is the long-run parameters that captures the long run equilibrium relationship between y and X, with short run effects measured by
, which represent the parameters associated with the
variables.
Therefore, the Pooled mean group allows the determination of the short-run and long-run coefficients, the intercepts and the speed of adjustment to the long run equilibrium relationship. The main requirements for the consistency of this technique reside, firstly, in the existence of a long-run relationship between the variables analyzed, and as this happens, the error correction parameter has to be negative and statistically significant. Moreover, the residual of the error correction model must be independent and the exogenous variables can be treated as independent. For these conditions, we include the lags of the ARDL (p, q) model for the endogenous variable (p) and exogenous variable (q) in the error-correction form. This estimator is useful especially when there are reasons to expect long-run equilibrium relationships between variables to be similar across the European Union countries, because they might have similar levels of economic growth, similar levels of health expenditure and similar degrees of pollution.
In terms of a short-run relationship and the slope coefficients between individual countries, they are allowed to be country-specific, due to the very comprehensive impact of external shocks and stabilization policies.
5. Results
The long-term elasticities are estimated by ARDL panel method for all the three models. All models presented in
Table A4 take the same form as Equation (2), augmented to include each individual non-communicable disease: the malignant neoplasms (CANCER), the diseases of the circulatory system (CARDIO) and the diseases of the respiratory system (RESP). In order to detect how variation in environmental expenditure produces changes in NCD’s effect on health expenditure and how variation in NCDs produces changes in environmental expenditure’s effect on health, we have included a product-variable in each model, LnENV x lnNCDs.
Table A4 shows both long-run and short-run estimation results. With regards to the long-run relationship, the error correction term (ECT) involves a possible long-run relationship between the variables in all three models, because ECT is statistically significant at 1% level and is negative. In line with other studies [
41,
48,
49,
76,
77,
78,
79,
80], the GDP per capita results show a significant and positive long-run effect on health expenditure per capita in 28 EU countries in all three models. Thus, the 1% increase in GDP per capita could lead to an increase of 2.39%, 1.08% and 1.14%, respectively, of health expenditure in the long run. The high values of the coefficients have shown that, as expected, GDP is an important factor in EU countries in terms of the levels and increases of health expenditures in the long-run.
Regarding the effect of CO2 emissions per capita on health expenditure, the long-run estimations revealed that emissions cause an increase in health expenditure in all 28 EU countries, and in all three models. The CO2 emissions coefficient is statistically significant at the 1% level. In the selected sample, the CO2 emissions could lead to an increase of 0.7%, 0.6% and 1%, respectively, of health expenditure in the long-run. The implication is that air pollution generates increases in health expenditure, but at lower levels compared to the GDP. Therefore, if emerging economies would accept the price of worsening the environment by deploying an ample economic development, these economies should also accept to cover higher health expenditure due to the negative effects of air pollution.
When analyzing the impact of renewable energy on health expenditure, there is a 1% increase in renewable energy consumption per capita, which could lead to a decrease of 0.26%–0.30% of health expenditure per capita in the long-run. These results are consistent with the findings of Çetin [
59] and Khan [
60], and show that the use of renewable energy could reduce the possible effects of pollution on health. However, the long-run coefficients in the sample show that the increasing impact of CO
2 emissions on health expenditure is higher than the low impact of renewable energies.
The coefficients of the product term in our equations do not have a simple causal interpretation, as they describe how the causal effect of an explanatory variable on the dependent variable is affected by the variation of the other variable [
81]. Thus, in the interaction of non-communicable diseases and environmental expenditure on health-care, the product term’s coefficient seems to describe both how variation in environmental expenditure produces changes in NCD’s effect on health expenditure, and how variation in NCDs produces changes in environmental expenditure’s effect on health. Thus, in the first model that includes the diseases of the respiratory system (RESP), the product term coefficient is negative, while the coefficients of the variable ENV and RESP are positive. Consequently, a 1% increase in the diseases of the respiratory system (RESP) could lead to an increase of 2.13% of health expenditure when no environmental expenditure exists. However, variation in environmental expenditure produces changes in the diseases of the respiratory system (RESP) with an effect on health expenditure; thus, a 1% increase in the environmental expenditure leads to a decrease of 0.14% of changes in the diseases of the respiratory system (RESP) and their effect on health expenditure (from 2.13% to 1.99%). In the second model, which includes the diseases of the circulatory system (CARDIO), the results are similar: a 1% increase in the diseases of the circulatory system (CARDIO) could lead to an increase of 2.14% in regards to health expenditure when no environmental expenditure exists. However, when investigating how the variation in environmental expenditure produces changes in the effects of diseases of the circulatory system (CARDIO) on health expenditure, the results are as follows: a 1% increase in the environmental expenditure leads to a decrease of 0.18% in changes of the diseases effect on health expenditure (i.e., from 2.14% to 1.96%). The long-run coefficient of the malignant neoplasms (CANCER) is statistically significant at 5% level and this non-communicable disease could lead to an increase of 0.92% of health expenditure in the long-run. Resuming, when the quality of the environment decreases, there is a negative impact on human health, which will lead to a health deterioration, by spending more in order to better take care of one’s health.
7. Conclusions
During the last few decades, we have witnessed a sustained endorsement of the primacy of socio-economic factors (i.e., economic power, distribution of knowledge and opportunities, education) in order to safeguard a proper human existence. Gradually, however, an increasingly rich scientific literature, accompanied by serious signals from international and non-governmental organizations, has highlighted the vital role of a functioning natural environment in sustaining human dignity, well-being and health [
83].
In this article, we have analyzed both the long-run and the short-run relationship between economic growth, environmental pollution and NCDs on health expenditure in the 28 EU countries over the 2000–2014 time period, employing the Panel Autoregressive Distributed Lag (ARDL) method. Using the Pedroni Johansen cointegration, we have found that the variables are cointegrated. Our results show that the GDP has the greatest impact on health expenditure. Therefore, a 1% increase in GDP per capita could lead to an average increase of 2% of health expenditure in the long run, i.e., countries with higher GDP per capita have a greater potential for health expenditure growth. Regarding CO2 emissions, we found that they determine a decrease of health expenditure in the short-run and a growth in the long-run, i.e., a 1% increase in CO2 emissions per capita could lead to an increase between 0.6% and 1% of health expenditure in the long run (depending on which of the three deployed models is chosen). We can argue that the impact of CO2 emissions on health expenditure is dependent on economic growth, and this in turn would lead to higher health spending. Ideally, this growth should occur on the basis of clean, renewable energies (i.e., the mediating role of renewable energy), and the effects of this growth should generate increases of health expenditure. However, this may not apply for all countries, some EU member states included. Renewable energies influence the level of health expenditure in all EU countries, but to a lower degree than CO2 emissions. The long-run coefficients of our sample show that the increasing impact of CO2 emissions on health expenditure is higher than the (low) impact of renewable energies. Therefore, we consider that EU countries should carefully follow a development agenda of renewable energy sources, not simply as a means to protect the environment, but also to lower the costs of diseases attributable to environmental risk factors or the environmental protection expenditures. As expected, environmental expenditure also has a significant and positive impact on health expenditure. Moreover, the variation in environmental expenditure produces changes in NCD’s effect on health expenditure, i.e., a 1% increase in the environmental expenditure leads to a decrease in the NCDs effect on health expenditure. Therefore, when no environmental expenditure exists, a 1% increase in the diseases of the respiratory system (RESP) could lead to an increase of 2.13% of health expenditure. In case of the circulatory system (CARDIO) and malignant neoplasms (CANCER), in the long-term, a 1% increase of them could lead to an increase of 2.14% 0.92%, respectively of health expenditure when no environmental expenditure exists.
We have found that the relationship between the environment and health goes beyond the effects of economic development, pollution and NCDs, which nonetheless remain important aspects of public health. The results of our research can provide substantial arguments for political decisions in order to maximize the efficiency of healthcare spending concurrent with a better environmental protection, thus, enabling the increase of GDP both in the medium- and long-run, based on technological developments aiming at improving the quality of life, rather than targeting economic growth at all costs. Major political decisions which have consequences for society and negatively affect people’s health must not ignore the health-environment nexus. Health and environmental policies must be planned out for the medium and long-term, being effective and with positive consequences on human health, in order “to recognize and respond to the centrality of the environment for health” [
2] (p. 106). By reinterpreting the essential consequences of the natural environment on human health, the environment should be recognized as a crucial element, of equal importance as socio-economic factors, on national and global policies for public health and for environmental protection.
In this study, we have faced some limitations, mainly related to the difficulty of obtaining a comprehensive dataset for a long period of time and a significant number of different variables. Thus, the time period taken into account was reduced to 15 years. Moreover, for some key variables, such as those related to non-communicable diseases morbidity, and which could have been included as explanatory variables in the estimated models, insufficient data were available for the entire analyzed period. These limitations, although they do not discredit the results of this analysis, should be addressed in subsequent studies. Furthermore, further research aiming at investigating all EU countries could include more variables related to environmental quality, variables related to different types of health expenditure and variables revealing the economic differences between developed and developing countries.







{kind=link}
{kind=link}
