Epidemiological Characteristics and Spatiotemporal Trend Analysis of Human Brucellosis in China, 1950–2018


Abstract
:1. Introduction
2. Method
2.1. Data Source
2.2. Ethical Considerations
2.3. Statistical Analysis
3. Results
3.1. Demographic Features
3.2. Geographic Distribution
3.3. Brucellosis and GDP per Capita
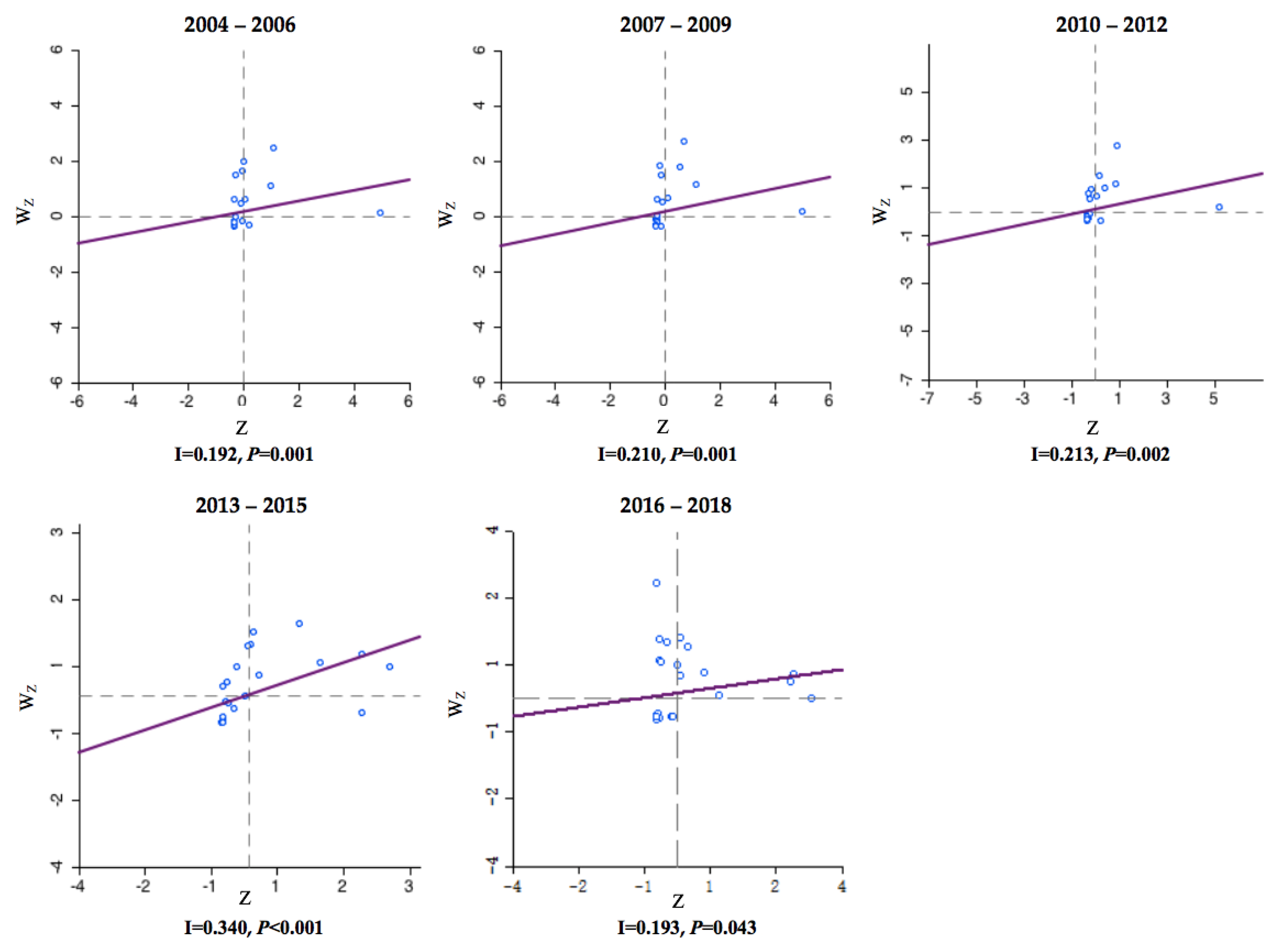
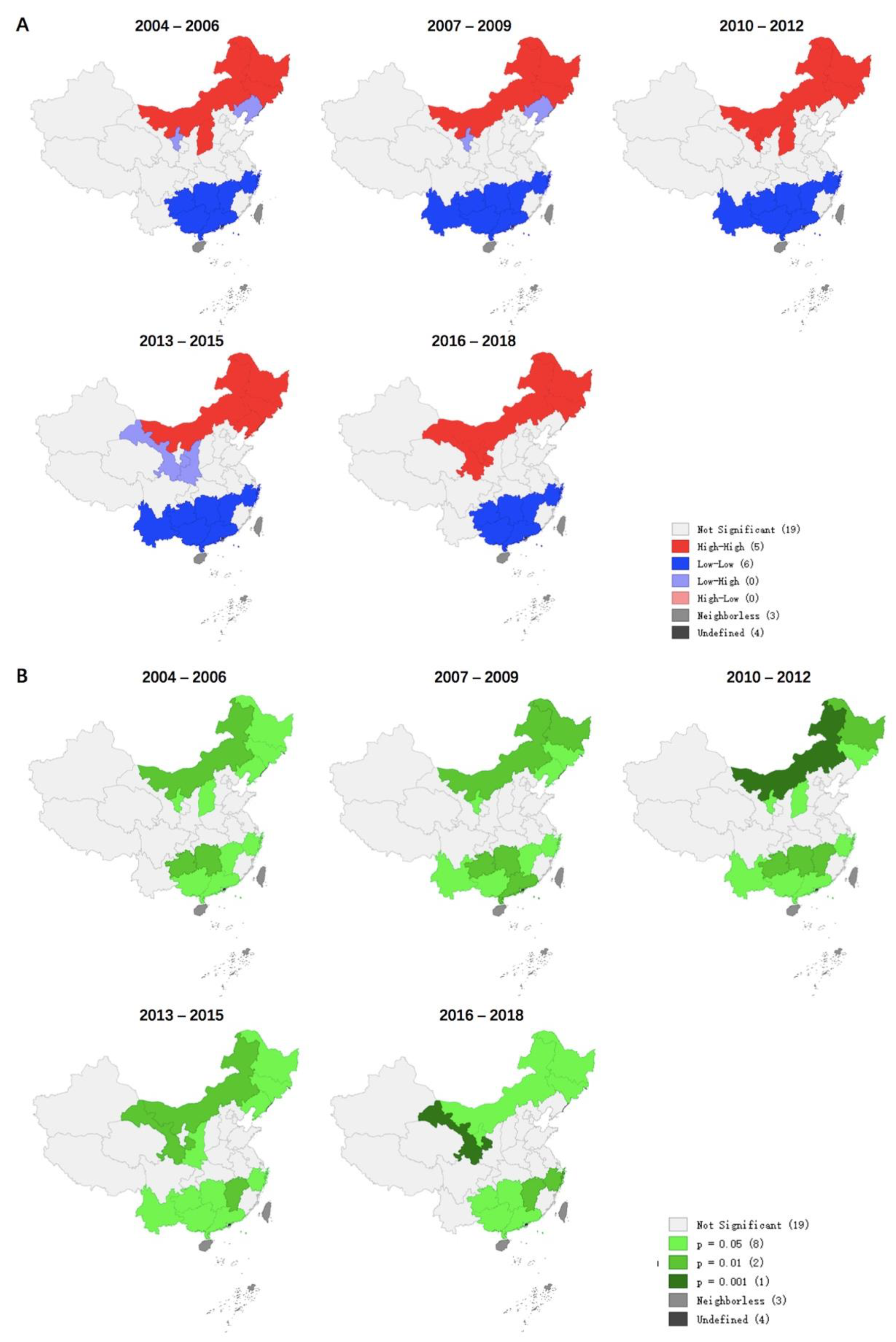
3.4. Distribution of Four Different Clusters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Pappas, G.; Papadimitriou, P.; Akritidis, N.; Christou, L.; Tsianos, E.V. The new global map of human brucellosis. Lancet Infect. Dis. 2006, 6, 91–99. [Google Scholar] [CrossRef]
- Mohamed, N.S.; Stephen, M.B.; Nammalwar, S. Brucellosis: A re-emerging zoonosis. Vet. Microbiol. 2010, 140, 392–398. [Google Scholar]
- Mingtao, L.; Guiquan, S.; Wenyi, Z.; Jin, Z. Model-Based Evaluation of Strategies to Control Brucellosis in China. Int. J. Environ. Res. Public Health 2017, 14, 3. [Google Scholar]
- Overview of National Infectious Diseases in 2018. Available online: http://www.nhc.gov.cn/jkj/s3578/201904/050427ff32704a5db64f4ae1f6d57c6c.shtml (accessed on 24 April 2019).
- Ministry of Health of the People’s Republic of China. Measures for the management of infectious diseases. Jiang Xi Zhong Yi Yao 1955, 8, 4–7. [Google Scholar]
- Shengjie, L.; Hang, Z.; Weiyi, X.; Gilbert, M.; Zhuojie, H.; Jianxing, Y.; Wenwu, Y.; Liping, W.; Qiulan, C.; Yu, L.; et al. Changing Epidemiology of Human Brucellosis, China, 1955–2014. Emerg. Infect. Dis. 2017, 23, 184–194. [Google Scholar]
- Deqiu, S.; Xiaodong, L.; Jiming, Y. Epidemiology and control of brucellosis in China. Vet. Microbiol. 2002, 90, 165–182. [Google Scholar] [CrossRef]
- Xuhua, R.; Xiaohong, C.; Miaomiao, W.; Jiajia, C.; Hongbo, N. Brucellosis seroprevalence in ovine and caprine flocks in China during 2000–2018: A systematic review and meta-analysis. BMC Vet. Res. 2018, 14, 393. [Google Scholar]
- Rongjiong, Z.; Songsong, X.; Xiaobo, L.; Lihua, S.; Yan, Z.; Yuexin, Z.; Wang, K. A Systematic Review and Meta-Analysis of Epidemiology and Clinical Manifestations of Human Brucellosis in China. Biomed. Res. Int. 2018, 2018, 5712920. [Google Scholar]
- Shang, D. Progress in the study of prevention and control of Brucellosis in China in last 50 years. Zhonghua Liu Xing Bing Xue Za Zhi 2000, 21, 55–57. [Google Scholar]
- Linhua, Z.; Fan, M.; Qiang, H.; Zhen, J.; Xiangdong, S. Transmission dynamics and optimal control of brucellosis in Inner Mongolia of China. Math. Biosci. Eng. 2018, 15, 543–567. [Google Scholar]
- Yinjun, L.; Xinlou, L.; Liang, S.; Liqun, F.; Wuchun, C. Epidemiological features and risk factors associated with the spatial and temporal distribution of human brucellosis in China. BMC Infect. Dis. 2013, 13, 547. [Google Scholar]
- Zhijun, Z.; Shuang, Y.; Xichun, W.; Shicun, D.; Jie, X.; Yufei, W.; Zeliang, C.; Zhihua, R.; Guangneng, P. Human brucellosis in the People’s Republic of China during 2005–2010. Int. J. Infect. Dis. 2013, 17, e289–e292. [Google Scholar]
- Weili, K. Brucellosis infection increasing in Southern China. Eur. J. Intern. Med. 2018, 51, e16–e18. [Google Scholar]
- Cárdenas, L.; Awada, L.; Tizzani, P.; Cáceres, P.; Casal, J. Characterization and evolution of countries affected by bovine brucellosis (1996–2014). Transbound. Emerg. Dis. 2019, 66, 1280–1290. [Google Scholar] [CrossRef]
- Yuan, Z.; Jin, Q. Differential responses of infectious diseases to economic growth in China. Int. J. Infect. Dis. 2011, 15, e578–e579. [Google Scholar]
- Ting, W.; Xiang, W.; Ping, T.; Yongfei, B.; Yuhua, Z.; Changfu, Y.; Zhikai, C.; Jing, C.; Huaxiang, R.; Lingjia, Z.; et al. Spatio-temporal cluster and distribution of human brucellosis in Shanxi Province of China between 2011 and 2016. Sci. Rep. 2018, 8, 16977. [Google Scholar]
- Hansong, Z.; Linglan, W.; Daihua, L.; Rongtao, H.; Jianming, O.; Wu, C.; Boping, W.; Wenlong, H.; Zhonghang, X.; Guangmin, C.; et al. Analysis on epidemiology and spatial-temporal clustering of human brucellosis in Fujian province, 2011–2016. Zhonghua Liu Xing Bing Xue Za Zhi 2017, 38, 1212–1217. [Google Scholar]
- Kongfu, W.; Hong, Z.; Jian, H.; Deshan, Y.; Xiaoting, Y.; Zhongyi, J.; Faxiang, G.; Yao, C.; Haixia, L.; Yunhe, Z.; et al. Epidemiological and spatial-temporal distribution of several natural focus diseases in Gansu province, 2014–2018. Zhonghua Liu Xing Bing Xue Za Zhi 2019, 40, 947–952. [Google Scholar]
- Jia, P.; Joyner, A. Human brucellosis occurrences in inner mongolia, China: A spatio-temporal distribution and ecological niche modeling approach. BMC Infect. Dis. 2015, 15, 36. [Google Scholar] [CrossRef] [Green Version]
- Peng, C.; Li, Y.J.; Huang, D.S.; Guan, P. Spatial-temporal distribution of human brucellosis in mainland China from 2004 to 2017 and an analysis of social and environmental factors. Environ. Health Prev. Med. 2020, 25, 1. [Google Scholar] [CrossRef] [Green Version]
- National Bureau of Statistics of China. Gross Domestic Product(GDP). Available online: http://data.stats.gov.cn/easyquery.htm?cn=C01 (accessed on 19 January 2020).
- Chatfield, C.; Mohammad, Y. Holt-Winters Forecasting: Some Practical Issues. J. R. Stat. Soc. 1988, 37, 129–140. [Google Scholar] [CrossRef]
- Raghava, M.V.; Prabhakaran, V.; Jayaraman, T.; Muliyil, J.; Oommen, A.; Dorny, P.; Vercruysse, J.; Rajshekhar, V. Detecting hot spots using cluster analysis and GIS. Trans. R. Soc. Trop. Med. Hyg. 2010, 104, 602–612. [Google Scholar]
- Ahmadi, A.K.; Zahrani, A.A. Spatial Autocorrelation of Cancer Incidence in Saudi Arabia. Int. J. Environ. Res. Public Health 2013, 10, 7207–7228. [Google Scholar] [CrossRef] [PubMed]
- Luc, A. Local Indicators of Spatial Association—LISA. Geogr. Anal. 2010, 27, 93–115. [Google Scholar]
- Anselin, L.; Rey, S. Properties of Tests for Spatial Dependence in Linear-Regression Models. Geogr. Anal. 1991, 23, 112–131. [Google Scholar] [CrossRef]
- Proceedings of Expert Seminar on Animal Brucellosis Diagnosis and Control Strategy in Asia; FAO/Ministry of Agriculture of the People’s Republic of China: Beijing, China, 1992; Volume 1–3, pp. 29–32.
- Shiyi, Z.; Linlin, J.; Zhiwen, N.; Tiefeng, L.; Xingfei, Z. Implementation and evaluation of main technical measures for the prevention and treatment of brucellosis at home and abroad. China J. Endem. Dis. Control. 2000, 1, 30. [Google Scholar]
- Standards and Regulations for the Prevention and Control of Endemic Diseases; General Office of the CPC Central Committee: Beijing, China, 1983; pp. 35–39.
- Hui, W. Analysis of the development prospects of pasteurized milk in China. In Proceedings of the Second China Dairy Conference 2011, Wuhan, China, 17–18 June 2011; Volume 2, pp. 50–52. [Google Scholar]
- Buyu, J.; Jiang, H. Surveillance data of brucellosis in China, 2005–2016. Dis. Surveill. 2018, 3, 188–192. [Google Scholar]
- Senlin, J.; Yongli, Z.; Shiyi, Z. Analysis of 1990 to 2001 surveillance effect of national major surveillance place for brucellosis. Chin. J. Control. Endem. Dis. 2002, 17, 185–188. [Google Scholar]
- National Beef and Mutton Production Development Plan (2013–2020); National Development and Reform Commission of China: Beijing, China, 2013.
- Bricker, B.J.; Halling, M.S. Differentiation of Brucella abortus bv. 1, 2, and 4, Brucella melitensis, Brucella ovis, and Brucella suis bv. 1 by PCR. J. Clin. Microbiol. 1994, 32, 2660–2666. [Google Scholar] [CrossRef] [Green Version]
- Fekete, A.; Bantle, J.A.; Halling, M.S.; Sanborn, R.M. Preliminary development of a diagnostic test for Brucella using polymerase chain reaction. J. Appl. Bacteriol. 1990, 69, 216–227. [Google Scholar] [CrossRef]
- Redkar, R.; Rose, S.; Bricker, B.; DelVecchio, V. Real-time detection of Brucella abortus, Brucella melitensis and Brucella suis. Mol. Cell. Probes 2001, 15, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Dal, T.; Kara, S.S.; Cikman, A.; Balkan, C.E.; Acikgoz, Z.C.; Zeybek, H.; Uslu, H.; Durmaz, R. Comparison of multiplex real-time polymerase chain reaction with serological tests and culture for diagnosing human brucellosis. J. Infect. Public Health 2019, 12, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Jiqiu, W.; Xiaochen, Z.; Ying, X.; Ying, W.; Tiefeng, L.; Dali, W. Epidemiological characteristics and influence factors of human brucellosis in Jilin Province in 2011–2017. Chin. J. Endem. 2019, 5, 390–394. [Google Scholar]
- Changqing, L.; Chao, T.; Dongni, C.; Wenzeng, Z.; Yuxin, M.; Yan, W.; Shixun, S.; Jixin, S.; Songjian, Z. Epidemiological characteristics of brucellosis in Shunyi District, Beijing, 2010–2014. Chin. J. Vector Biol. Control 2016, 27, 381–382. [Google Scholar]
- Yingmei, Z.; Gang, S.; Junfeng, Z.; Jun, Z. Experience and exploration of comprehensive prevention and control of animal brucellosis in Heilongjiang Province. In Proceedings of the 3rd National Zoonotic Symposium, Lyon, France, 12–15 June 2011. [Google Scholar]
- Li, K.; Zhang, L.; Shahzad, M.; Mehmood, K.; Li, J. Increasing incidence and changing epidemiology of brucellosis in China (2004–2016). Travel Med. Infect. Dis. 2019, 2019, 101464. [Google Scholar] [CrossRef] [PubMed]
- Yujing, S.; Shengjie, L.; Qiulan, C.; Di, M.; Yu, L.; Xinxu, L.; Wenwu, Y.; Hongjie, Y. Epidemic characteristics of brucellosis in humans from 2015 to 2016 in North and South China. Zhonghua Liu Xing Bing Xue Za Zhi 2017, 38, 435–440. [Google Scholar]
- Zhiru, A.; Hanwu, Z.; Deming, X.; Xingxian, L. Brucellosis epidemic in Guangdong. South China Prev. Med. 1984, 3, 111–119. [Google Scholar]
- Yunlong, B.; Lintian, B.; Jinfeng, H. Investigation Report of Brucellosis in Yunnan Livestock. Yunnan Anim. Husb. Vet. Med. 1989, 1, 6–7. [Google Scholar]
- Xuhua, R.; Jiajia, C.; Miaomiao, W.; Xiaohong, C.; Haoxian, W.; Yu, G.; Hongbo, N.; Xiaoxuan, Z.; Xiaobo, W. Brucellosis seroprevalence in dairy cattle in China during 2008–2018: A systematic review and meta-analysis. Acta Trop. 2019, 189, 117–123. [Google Scholar]
- Sujuan, Z.; Weimin, X.; Xingyi, J.; Heng, W.; Yang, Y.; Tang, Y.; Jia, W. Retrospective analysis of epidemiological characteristics of brucellosis in Zhejiang Province. Zhonghua Di Fang Bing Xue Za Zhi 2014, 33, 425–428. [Google Scholar]
- Weizhong, Z.; Liangliang, C.; Wenwen, T.; Jihong, H.; Zhongming, T.; Jiangang, Z.; Jianfang, X.; Chunjun, B. Investigation on the awareness of brucellosis in some occupational populations in Jiangsu Province. Zhonghua Di Fang Bing Xue Za Zhi 2013, 32, 508–511. [Google Scholar]
- Peiyan, L.; Zhengran, L.; Jinxin, H.; Haitao, B.; Guomin, T.; Xinhui, W.; Yuting, Z.; Sitian, W. A Cross-Sectional Study of Cognition and Behavior of Mongolian Residents in Pastoral Area of Tongliao City on the Risk of Brucellosis. Xian Dai Yu Fang Yi Xue 2019, 46, 4162–4165. [Google Scholar]
- Yanwei, B.; Siyuan, Z.; Rile, G. Analysis on the prevention and control of human brucellosis in Xilin Gol League of Inner Mongolia Autonomous Region from 2010 to 2018. Dis. Surveill. 2019, 34, 1064–1067. [Google Scholar]
- Ying, L.; Wengang, L.; Jianwen, L.; Xiusheng, W.; Ruifeng, Z.; Tao, S.; Yushuang, S.; Zheng, L.; Yiman, D.; Zhixuan, L. Survey of “knowledge, trust and action” among high-risk groups in areas with high incidence of brucellosis in Tianjin. Zhong Guo Dong Wu Jian Yi 2019, 36, 22–28. [Google Scholar]
- Aworh, M.K.; Okolocha, E.; Kwaga, J.; Fasina, F.; Lazarus, D.; Suleman, I.; Poggensee, G.; Nguku, P.; Peter, N. Human brucellosis: Seroprevalence and associated exposure factors among abattoir workers in Abuja, Nigeria—2011. Pan Afr. Med. J. 2013, 17, 103. [Google Scholar] [CrossRef]
- Kansiime, C.; Mugisha, A.; Makumbi, F.; Mugisha, S.; Rwego, I.B.; Sempa, J.; Kiwanuka, S.N.; Asiimwe, B.B.; Rutebemberwa, E. Knowledge and perceptions of brucellosis in the pastoral communities adjacent to Lake Mburo National Park, Uganda. BMC Public Health 2014, 14, 242. [Google Scholar] [CrossRef] [Green Version]
- Neiderud, C.J. How urbanization affects the epidemiology of emerging infectious diseases. Infect. Ecol. Epidemiol. 2015, 5, 27060. [Google Scholar] [CrossRef]
- National Bureau of Statistics of China. China Statistical Yearbook; National Bureau of Statistics of China: Beijing, China, 2018.
- Tong, W.; Perring, C.; Kinzig, A.; James, P.C.; Ben, A.M.; Peter, D. Economic growth, urbanization, globalization, and the risks of emerging infectious diseases in China: A review. Ambio 2017, 46, 18–29. [Google Scholar]
- Wei, K.F.; Zhang, H.; He, J.; Gou, F.X.; Cheng, Y.; Liu, X.F. Spatial distribution of Brucellosis in Gansu province, 2013–2018. Zhonghua Liu Xing Bing Xue Za Zhi 2019, 40, 1099–1105. [Google Scholar]
- Fosgate, G.T.; Carpenter, T.E.; Chomel, B.B.; Case, J.T.; Reilly, K.F. Time-Space Clustering of Human Brucellosis, California, 1973–1992. Emerg. Infect. Dis. 2002, 8, 672–678. [Google Scholar] [CrossRef]
- Abdullayev, R.; Kracalik, I.; Ismayilova, R.; Ustun, N.; Talibzade, A.; Blackburn, J.K. Analyzing the spatial and temporal distribution of human brucellosis in Azerbaijan (1995–2009) using spatial and spatio-temporal statistics. BMC Infect. Dis. 2012, 12, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corbel, J.M. Brucellosis in Humans and Animals; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Fanyu, L.; Ping, W.; Di, W.; Zhichen, Y.; Yan, L.; Chaoling, G.; Ruize, W.; Qing, Z.; Yan, Y. Investigation on the status of brucellosis infection in sheep farmers in western pastoral area of Jilin Province. J. Jilin Univ. 2015, 41, 175–180. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
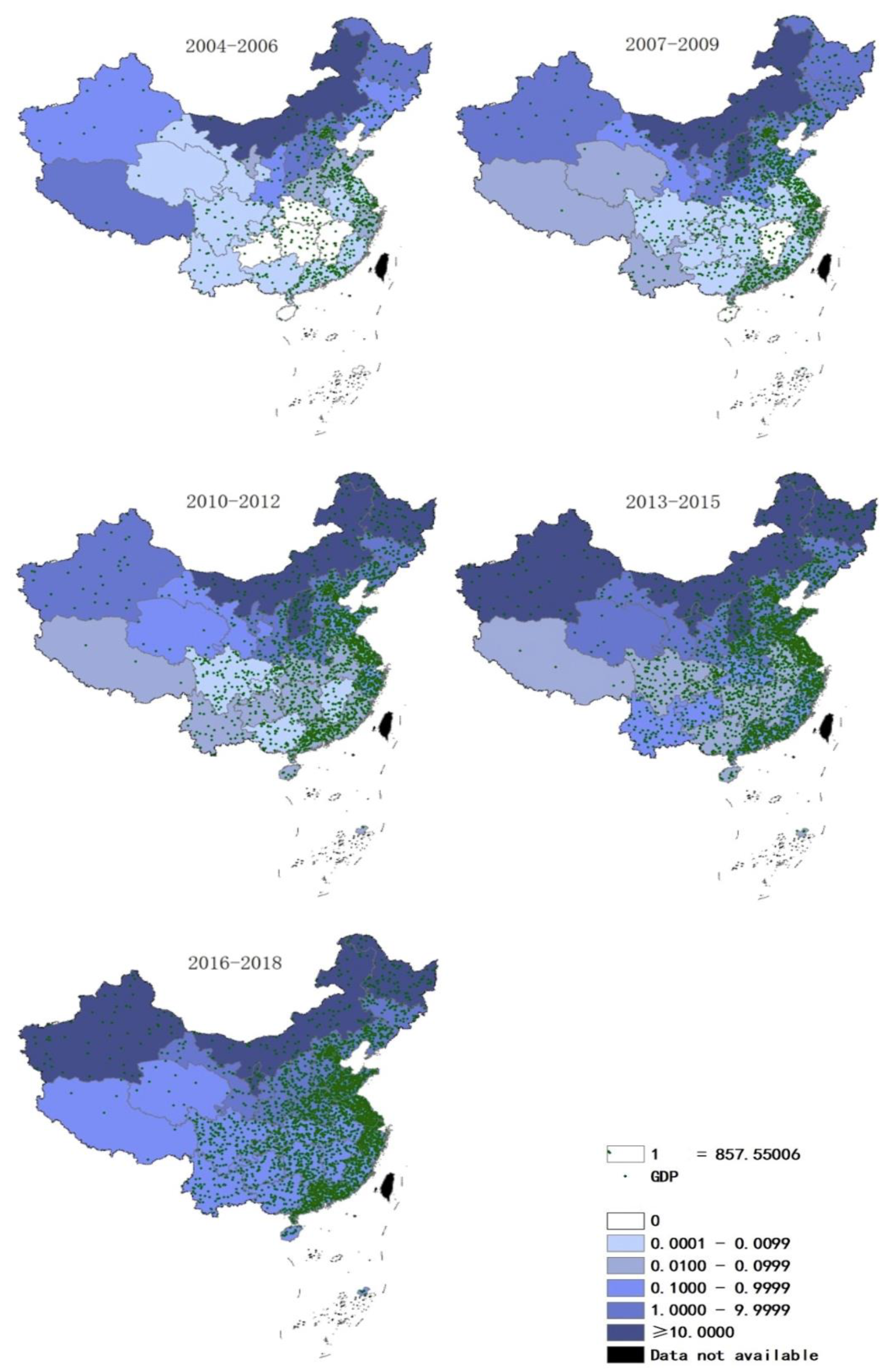
| Time Period | r | p |
|---|---|---|
| 2004–2006 | −0.336 | 0.312 |
| 2007–2009 | −0.274 | 0.272 |
| 2010–2012 | −0.286 | 0.148 |
| 2013–2015 | −0.224 | 0.233 |
| 2016–2018 | −0.360 | 0.047 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, H.; Zhang, S.; Wang, T.; Zhao, C.; Zhang, X.; Hu, J.; Han, C.; Hu, F.; Luo, J.; Li, B.; et al. Epidemiological Characteristics and Spatiotemporal Trend Analysis of Human Brucellosis in China, 1950–2018. Int. J. Environ. Res. Public Health 2020, 17, 2382. https://doi.org/10.3390/ijerph17072382
Yang H, Zhang S, Wang T, Zhao C, Zhang X, Hu J, Han C, Hu F, Luo J, Li B, et al. Epidemiological Characteristics and Spatiotemporal Trend Analysis of Human Brucellosis in China, 1950–2018. International Journal of Environmental Research and Public Health. 2020; 17(7):2382. https://doi.org/10.3390/ijerph17072382
Chicago/Turabian StyleYang, Huixin, Siwen Zhang, Taijun Wang, Chenhao Zhao, Xiangyi Zhang, Jing Hu, Chenyu Han, Fangfang Hu, Jingjing Luo, Biao Li, and et al. 2020. "Epidemiological Characteristics and Spatiotemporal Trend Analysis of Human Brucellosis in China, 1950–2018" International Journal of Environmental Research and Public Health 17, no. 7: 2382. https://doi.org/10.3390/ijerph17072382