Impact of Psychotherapy on Psychosocial Functioning in Borderline Personality Disorder Patients

Abstract
:1. Introduction
2. Methods
2.1. Identification and Selection of Studies
2.2. Risk of Bias and Data Extraction
2.3. Meta-Analysis
3. Results
3.1. Selection and Inclusion
3.2. Characteristics of Included Studies
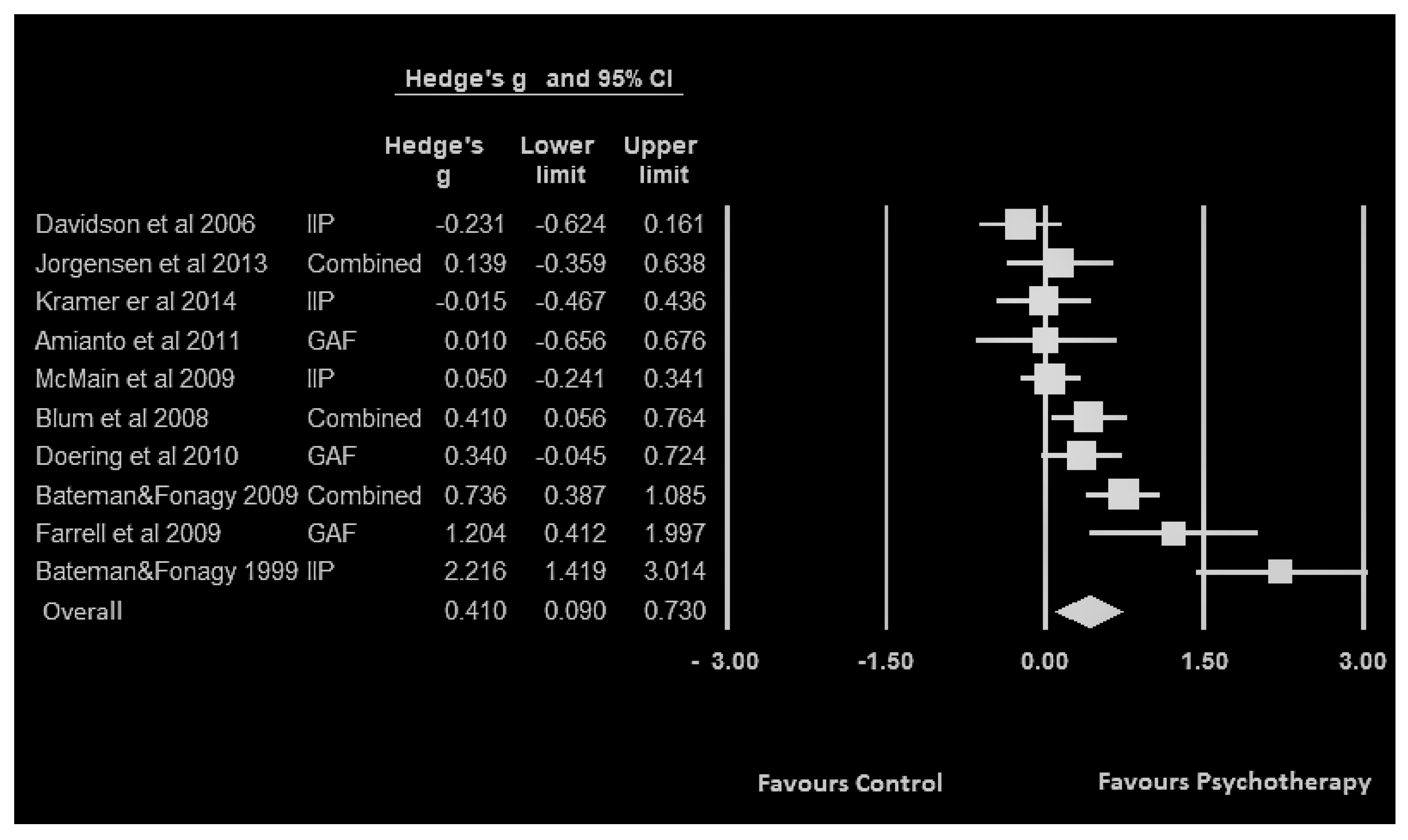
3.3. Findings
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
Abbreviations
| BPD | Borderline Personality Disorder |
| GAF | Global Assessment of Functioning |
| SAS-SR | Social Adjustment Scale–Self-Report |
| IIP | Inventory of Interpersonal Problems |
| SB-APP | Sequential Brief Adlerian Psychodynamic Psychotherapy |
| MBT | Mentalization-based treatment |
| PH | Partial Hospitalization |
| STEPPS | Systems Training for Emotional Predictability and Problem Solving |
| CBT | Cognitive Behavior Therapy |
| TFP | Transference Focused Psychotherapy |
| MBT | Mentalization-based treatment |
| MOTR | Motive-oriented therapeutic relationship |
| DBT | Dialectical Behaviour Therapy |
| STM | Supervised Team Management |
| SPT | Standard Psychiatric Care |
| SCM | Structured Clinical Management |
| TAU | Treatment As Usual |
| ECP | Experienced Community Psychotherapists |
| ST | Supportive Therapy |
| GPM | General Psychiatric Management |
References
- Johnson, D.M.; Shea, M.; Yen, S.; Battle, C.L.; Zlotnick, C.; Sanislow, C.A.; Grilo, C.M.; Skodol, A.E.; Bender, D.S.; Mcglashan, T.H.; et al. Gender differences in borderline personality disorder: Findings from the collaborative longitudinal personality disorders study. Compr. Psychiatry 2003, 44, 284–292. [Google Scholar] [CrossRef] [Green Version]
- Skodol, A.E. Impact of personality pathology on psychosocial functioning. Curr. Opin. Psychol. 2018, 21, 33–38. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Arlington, VA, USA, 2017. [Google Scholar]
- Skodol, A.E.; Gunderson, J.G.; McGlashan, T.H.; Dyck, I.R.; Stout, R.L.; Bender, D.S.; Grilo, C.M.; Shea, M.T.; Zanarini, M.C.; Morey, L.C.; et al. Functional impairment in patients with schizotypal, borderline, avoidant, or or obsessive-compulsive personality disorder. Am. J. Psychiatry 2002, 2, 276–283. [Google Scholar] [CrossRef]
- Gunderson, J.G.; Stout, R.L.; McGlashan, T.H.; Shea, M.T.; Morey, L.C.; Grilo, C.M.; Zanarini, M.C.; Yen, S.; Markowitz, J.C.; Sanislow, C.; et al. Ten-Year Course of Borderline Personality Disorder: Psychopathology and Function From the Collaborative Longitudinal Personality Disorders Study. Arch. Gen. Psychiatry 2011, 8, 827–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, B.F.; Chou, S.P.; Goldstein, R.B.; Huang, B.; Stinson, F.S.; Saha, T.D.; Smith, S.M.; Dawson, D.A.; Pulay, A.J.; Pickering, R.P.; et al. Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: Results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions. J. Clin. Psychiatry 2008, 69, 533–545. [Google Scholar] [CrossRef]
- Ellison, W.D.; Rosenstein, L.K.; Morgan, T.A.; Zimmerman, M. Community and Clinical Epidemiology of Borderline Personality Disorder. Psychiatr. Clin. N. Am. 2018, 41, 561–573. [Google Scholar] [CrossRef] [Green Version]
- Cristea, I.A.; Gentili, C.; Cotet, C.D.; Palomba, D.; Barbui, C.; Cuijpers, P. Efficacy of Psychotherapies for Borderline Personality Disorder: A Systematic Review and Meta-analysis. JAMA Psychiatry 2017, 74, 319. [Google Scholar] [CrossRef]
- Sinnaeve, R.; Van Den Bosch, L.M.C.; Van Steenbergen-Weijenburg, K.M. Change in interpersonal functioning during psychological interventions for borderline personality disorder—A systematic review of measures and efficacy. Personal. Ment. Health 2015, 9, 173–194. [Google Scholar] [CrossRef]
- Zanarini, M.C.; Frankenburg, F.R.; Reich, D.B.; Fitzmaurice, G. The 10-year course of psychosocial functioning among patients with borderline personality disorder and axis II comparison subjects. Acta Psychiatr. Scand. 2010, 122, 103–109. [Google Scholar] [CrossRef]
- Bateman, A.; Fonagy, P. Effectiveness of Partial Hospitalization in the Treatment of Borderline Personality Disorder: A Randomized Controlled Trial. Am. J. Psychiatry 1999, 10, 1563–1569. [Google Scholar] [CrossRef]
- Bateman, A.; Fonagy, P. Randomized Controlled Trial of Outpatient Mentalization-Based Treatment Versus Structured Clinical Management for Borderline Personality Disorder. Am. J. Psychiatry 2009, 166, 1355–1364. [Google Scholar] [CrossRef] [PubMed]
- McMain, S.F.; Links, P.S.; Gnam, W.H.; Guimond, T.; Cardish, R.J.; Korman, L.; Streiner, D.L. A Randomized Trial of Dialectical Behavior Therapy Versus General Psychiatric Management for Borderline Personality Disorder. Am. J. Psychiatry 2008, 166, 1365–1374. [Google Scholar] [CrossRef] [Green Version]
- Farrell, J.M.; Shaw, I.A.; Webber, M.A. A schema-focused approach to group psychotherapy for outpatients with borderline personality disorder: A randomized controlled trial. J. Behav. Ther. Exp. Psychiatry 2009, 40, 317–328. [Google Scholar] [CrossRef]
- Jørgensen, C.R.; Freund, C.; Bøye, R.; Jordet, H.; Andersen, D.; Kjølbye, M. Outcome of mentalization-based and supportive psychotherapy in patients with borderline personality disorder: A randomized trial. Acta Psychiatr. Scand. 2012, 127, 305–317. [Google Scholar] [CrossRef] [PubMed]
- Amianto, F.; Ferrero, A.; Pierò, A.; Cairo, E.; Rocca, G.; Simonelli, B.; Fassina, S.; Abbate-Daga, G.; Fassino, S. Supervised team management, with or without structured psychotherapy, in heavy users of a mental health service with borderline personality disorder: A two-year follow-up preliminary randomized study. BMC Psychiatry 2011, 11, 181. [Google Scholar] [CrossRef] [Green Version]
- Blum, N.; John, D.S.; Pfohl, B.; Stuart, S.; Mccormick, B.; Allen, J.; Arndt, S.; Black, D.W. Systems Training for Emotional Predictability and Problem Solving (STEPPS) for Outpatients With Borderline Personality Disorder: A Randomized Controlled Trial and 1-Year Follow-Up. Am. J. Psychiatry 2008, 165, 468–478. [Google Scholar] [CrossRef]
- Davidson, K.; Norrie, J.; Tyrer, P.; Gumley, A.; Tata, P.; Murray, H.; Palmer, S. The Effectiveness of Cognitive Behavior Therapy for Borderline Personality Disorder: Results from the Borderline Personality Disorder Study of Cognitive Therapy (BOSCOT) Trial. J. Personal. Disord. 2006, 20, 450–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doering, S.; Hörz, S.; Rentrop, M.; Fischer-Kern, M.; Schuster, P.; Benecke, C.; Buchheim, A.; Martius, P.; Buchheim, P. Transference-focused psychotherapy v. treatment by community psychotherapists for borderline personality disorder: Randomised controlled trial. Br. J. Psychiatry 2010, 196, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Kramer, U.; Kolly, S.; Berthoud, L.; Keller, S.; Preisig, M.; Caspar, F.; Berger, T.; Roten, Y.D.; Marquet, P.; Despland, J.-N. Effects of Motive-Oriented Therapeutic Relationship in a Ten-Session General Psychiatric Treatment of Borderline Personality Disorder: A Randomized Controlled Trial. Psychother. Psychosom. 2014, 83, 176–186. [Google Scholar] [CrossRef]
- Borenstein, M.; Higgins, J.P.T.; Hedges, L.V.; Rothstein, H.R. Basics of meta-analysis:I2is not an absolute measure of heterogeneity. Res. Synth. Methods 2017, 8, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley-Blackwell: Chichester, UK, 2019; p. 408. [Google Scholar]
- Aas, I.H. Global Assessment of Functioning (GAF): Properties and frontier of current knowledge. Ann. Gen. Psychiatry 2010, 9, 20:1–20:11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waugh, M.H.; Mcclain, C.M.; Mariotti, E.C.; Mulay, A.L.; Devore, E.N.; Lenger, K.A.; Russell, A.N.; Florimbio, A.R.; Lewis, K.C.; Ridenour, J.M.; et al. Comparative Content Analysis of Self-Report Scales for Level of Personality Functioning. J. Personal. Assess. 2020, 102, 1–13. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Included Studies | Tools * | Trt in Intervention Grp+ | Trt in Ctrl Grp++ |
|---|---|---|---|
| Amianto et al. 2011 [16] | GAF | SB-APP + STM | STM |
| Bateman and Fonagy 1999 [11] | IIP | MBT-PH | SPT |
| Bateman and Fonagy 2009 [12] | GAF, IIP, SAS-SR | MBT | SCM |
| Blum et al. 2008 [17] | GAF, SAS-SR | STEPPS + TAU | TAU |
| Davidson et al. 2006 [18] | IIP | CBT + TAU | TAU |
| Doering et al. 2010 [19] | GAF | TFP | ECP |
| Farrell et al. 2009 [14] | GAF | SFT + TAU | TAU |
| Jorgensen et al. 2013 [15] | GAF, SAS-SR, IIP | MBT | ST |
| Kramer et al. 2014 [20] | IIP | MOTR + GPM | GPM |
| McMain et al. 2009 [13] | IIP | DBT | GPM |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zahediabghari, S.; Boursiquot, P.; Links, P. Impact of Psychotherapy on Psychosocial Functioning in Borderline Personality Disorder Patients. Int. J. Environ. Res. Public Health 2020, 17, 4610. https://doi.org/10.3390/ijerph17124610
Zahediabghari S, Boursiquot P, Links P. Impact of Psychotherapy on Psychosocial Functioning in Borderline Personality Disorder Patients. International Journal of Environmental Research and Public Health. 2020; 17(12):4610. https://doi.org/10.3390/ijerph17124610
Chicago/Turabian StyleZahediabghari, Soheil, Philippe Boursiquot, and Paul Links. 2020. "Impact of Psychotherapy on Psychosocial Functioning in Borderline Personality Disorder Patients" International Journal of Environmental Research and Public Health 17, no. 12: 4610. https://doi.org/10.3390/ijerph17124610