The Matthew Effect in Recovery from Smartphone Addiction in a 6-Month Longitudinal Study of Children and Adolescents †

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Procedure and Participants
2.2. Measures
2.2.1. Smartphone Addiction Scale-Short Version (SAS-SV)
2.2.2. Internet Addiction Test (IAT)
2.2.3. Survey on the Pattern of Digital-Media Use
2.2.4. Dry Eye Symptoms (DES) Checklist
2.2.5. Junior Temperament Character Inventory (JTCI)
2.2.6. Depression Assessment
2.2.7. Anxiety Assessment
2.2.8. Barratt Impulsiveness Scale-11 (BIS-11)
2.2.9. Conners-Wells’ Adolescent Self-Report Scale-Short Form (CASS-S)
2.2.10. Goal Instability
2.2.11. Adolescents Happiness Index (AHI)
2.2.12. Rosenberg Self-Esteem Scale (RSES)
2.2.13. Pediatric Quality of Life (pedsQL)
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guazzini, A.; Duradoni, M.; Capelli, A.; Meringolo, P. An Explorative Model to Assess Individuals’ Phubbing Risk. Future Internet 2019, 11, 21. [Google Scholar] [CrossRef] [Green Version]
- O’Dea, S. Smartphone Penetration Rate by Country 2018. Available online: https://www.statista.com/statistics/539395/smartphone-penetration-worldwide-by-country/ (accessed on 4 April 2020).
- Ministry of Science and ICT; National Information Society Agency. 2019 The Survey on Smartphone Overdependence. 2020. Available online: https://www.nia.or.kr/site/nia_kor/ex/bbs/View.do?cbIdx=65914&bcIdx=21939&parentSeq=21939 (accessed on 1 May 2020).
- Sohn, S.; Rees, P.; Wildridge, B.; Kalk, N.J.; Carter, B. Prevalence of problematic smartphone usage and associated mental health outcomes amongst children and young people: A systematic review, meta-analysis and GRADE of the evidence. BMC Psychiatry 2019, 19, 356. [Google Scholar] [CrossRef] [Green Version]
- Panova, T.; Carbonell, X. Is smartphone addiction really an addiction? J. Behav. Addict. 2018, 7, 252–259. [Google Scholar] [CrossRef]
- Yu, S.; Sussman, S. Does Smartphone Addiction Fall on a Continuum of Addictive Behaviors? Int. J. Environ. Res. Public Health 2020, 17, 422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elhai, J.D.; Levine, J.C.; Hall, B.J. The relationship between anxiety symptom severity and problematic smartphone use: A review of the literature and conceptual frameworks. J. Anxiety Disord. 2019, 62, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Quarter of Children Under Six Have A Smartphone, Study Finds. Agency reporter, 8 April 2018.
- Beyens, I.; Nathanson, A.I. Electronic Media Use and Sleep Among Preschoolers: Evidence for Time-Shifted and Less Consolidated Sleep. Health Commun. 2019, 34, 537–544. [Google Scholar] [CrossRef] [Green Version]
- Grant, J.E.; Lust, K.; Chamberlain, S.R. Problematic smartphone use associated with greater alcohol consumption, mental health issues, poorer academic performance, and impulsivity. J. Behav. Addict. 2019, 8, 335–342. [Google Scholar] [CrossRef]
- Kim, Y.J.; Jang, H.M.; Lee, Y.; Lee, D.; Kim, D.J. Effects of Internet and Smartphone Addictions on Depression and Anxiety Based on Propensity Score Matching Analysis. Int. J. Environ. Res. Public Health 2018, 15, 859. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.Y.; Lee, D.; Nam, C.R.; Kim, D.Y.; Park, S.; Kwon, J.G.; Kweon, Y.S.; Lee, Y.; Kim, D.J.; Choi, J.S. Distinct patterns of Internet and smartphone-related problems among adolescents by gender: Latent class analysis. J. Behav. Addict. 2018, 7, 454–465. [Google Scholar] [CrossRef]
- Yang, J.; Fu, X.; Liao, X.; Li, Y. Association of problematic smartphone use with poor sleep quality, depression, and anxiety: A systematic review and meta-analysis. Psychiatry Res. 2020, 284, 112686. [Google Scholar] [CrossRef]
- Vahedi, Z.; Saiphoo, A. The association between smartphone use, stress, and anxiety: A meta-analytic review. Stress Health J. Int. Soc. Investig. Stress 2018, 34, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.H.; Kim, K.W.; Moon, N.J. Smartphone use is a risk factor for pediatric dry eye disease according to region and age: A case control study. Bmc Ophthalmol. 2016, 16, 188. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Choi, Y.H.; Kim, J. Effects of the cervical flexion angle during smartphone use on muscle fatigue and pain in the cervical erector spinae and upper trapezius in normal adults in their 20s. J. Phys. Ther. Sci. 2017, 29, 921–923. [Google Scholar] [CrossRef] [Green Version]
- Eitivipart, A.C.; Viriyarojanakul, S.; Redhead, L. Musculoskeletal disorder and pain associated with smartphone use: A systematic review of biomechanical evidence. Hong Kong Physiother. J. Off. Publ. Hong Kong Physiother. Assoc. Ltd. Wu Li Chih Liao 2018, 38, 77–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.H.; Li, Y.; Kim, S.H.; Jin, R.; Kim, Y.H.; Choi, W.; You, I.C.; Yoon, K.C. The influences of smartphone use on the status of the tear film and ocular surface. PLoS ONE 2018, 13, e0206541. [Google Scholar] [CrossRef] [PubMed]
- Alsalameh, A.M.; Harisi, M.J.; Alduayji, M.A.; Almutham, A.A.; Mahmood, F.M. Evaluating the relationship between smartphone addiction/overuse and musculoskeletal pain among medical students at Qassim University. J. Fam. Med. Prim. Care 2019, 8, 2953–2959. [Google Scholar] [CrossRef]
- Kim, H.J.; Min, J.Y.; Kim, H.J.; Min, K.B. Accident risk associated with smartphone addiction: A study on university students in Korea. J. Behav. Addict. 2017, 6, 699–707. [Google Scholar] [CrossRef]
- Guo, N.; Luk, T.T.; Ho, S.Y.; Lee, J.J.; Shen, C.; Oliffe, J.; Chan, S.S.; Lam, T.H.; Wang, M.P. Problematic Smartphone Use and Mental Health in Chinese Adults: A Population-Based Study. Int. J. Environ. Res. Public Health 2020, 17, 844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, Q.; Sun, R.; Fu, E.; Jia, G.; Xiang, Y. Parent-child relationship and smartphone use disorder among Chinese adolescents: The mediating role of quality of life and the moderating role of educational level. Addict. Behav. 2020, 101, 106065. [Google Scholar] [CrossRef] [PubMed]
- Karsay, K.; Schmuck, D.; Matthes, J.; Stevic, A. Longitudinal Effects of Excessive Smartphone Use on Stress and Loneliness: The Moderating Role of Self-Disclosure. Cyberpsychology Behav. Soc. Netw. 2019, 22, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Lapierre, M.A.; Zhao, P.; Custer, B.E. Short-Term Longitudinal Relationships Between Smartphone Use/Dependency and Psychological Well-Being Among Late Adolescents. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2019, 65, 607–612. [Google Scholar] [CrossRef]
- Lee, J.E.; Jang, S.-I.; Ju, Y.J.; Kim, W.; Lee, H.J.; Park, E.-C. Relationship between Mobile Phone Addiction and the Incidence of Poor and Short Sleep among Korean Adolescents: A Longitudinal Study of the Korean Children & Youth Panel Survey. J. Korean Med. Sci. 2017, 32, 1166–1172. [Google Scholar]
- Tossell, C.; Kortum, P.; Shepard, C.; Rahmati, A.; Zhong, L. Exploring Smartphone Addiction: Insights from Long-Term Telemetric Behavioral Measures. Int. J. Interact. Mob. Technol. 2015, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Feliciano, L.; Yochim, B.; Steers, M.E.; Jay, A.A.; Segal, D.L. Understanding Research in Clinical and Counseling Psychology, 2nd ed.; Jay, C., Hersen, T.M., Eds.; Routledge Taylor & Francis: New York, NY, USA, 2011. [Google Scholar]
- Lee, B.H.; Lee, H.K. Longitudinal study shows that addictive Internet use during adolescence was associated with heavy drinking and smoking cigarettes in early adulthood. Acta Paediatrica (Oslo Norway 1992) 2017, 106, 497–502. [Google Scholar] [CrossRef]
- Duradoni, M.; Innocenti, F.; Guazzini, A. Well-Being and Social Media: A Systematic Review of Bergen Addiction Scales. Future Internet 2020, 12, 24. [Google Scholar] [CrossRef] [Green Version]
- Vadlin, S.; Aslund, C.; Nilsson, K.W. A longitudinal study of the individual—And group-level problematic gaming and associations with problem gambling among Swedish adolescents. Brain Behav. 2018, 8, e00949. [Google Scholar] [CrossRef]
- Latulippe, K.; Hamel, C.; Giroux, D. Social Health Inequalities and eHealth: A Literature Review with Qualitative Synthesis of Theoretical and Empirical Studies. J. Med. Internet Res. 2017, 19, e136. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Xing, W. Exploring the Influence of Parental Involvement and Socioeconomic Status on Teen Digital Citizenship: A Path Modeling Approach. J. Educ. Technol. Soc. 2018, 21, 186–199. [Google Scholar]
- Lee, H.; Kim, J.W.; Choi, T.Y. Risk Factors for Smartphone Addiction in Korean Adolescents: Smartphone Use Patterns. J. Korean Med. Sci. 2017, 32, 1674–1679. [Google Scholar] [CrossRef]
- Muñoz-Miralles, R.; Ortega-González, R.; López-Morón, M.R.; Batalla-Martínez, C.; Manresa, J.M.; Montellà-Jordana, N.; Chamarro, A.; Carbonell, X.; Torán-Monserrat, P. The problematic use of Information and Communication Technologies (ICT) in adolescents by the cross sectional JOITIC study. BMC Pediatr. 2016, 16, 140. [Google Scholar] [CrossRef]
- United States Conference of Catholic Bishops Matthew 25:29. Available online: http://www.usccb.org/bible/mt/25:29 (accessed on 5 May 2020).
- Merton, R.K. The Matthew effect in science: The reward and communication systems of science are considered. Science 1968, 159, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.; Lee, J.-Y.; Won, W.-Y.; Park, J.-W.; Min, J.-A.; Hahn, C.; Gu, X.; Choi, J.-H.; Kim, D.-J. Development and Validation of a Smartphone Addiction Scale (SAS). PLoS ONE 2013, 8, e56936. [Google Scholar] [CrossRef] [PubMed]
- Kwon, M.; Kim, D.J.; Cho, H.; Yang, S. The smartphone addiction scale: Development and validation of a short version for adolescents. PLoS ONE 2013, 8, e83558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health & Welfare; Korean Academy of Medical Science; Korean Ophthalmological Society. The Symptoms and Complications of Dry Eye Syndrome. Available online: http://health.cdc.go.kr/health/mobileweb/content/group_view.jsp?CID=F98951A125 (accessed on 1 March 2020).
- Cloninger, C.R.; Svrakic, D.M.; Przybeck, T.R. A psychobiological model of temperament and character. Arch. Gen. Psychiatry 1993, 50, 975–990. [Google Scholar] [CrossRef]
- Lyoo, I.K.; Han, C.H.; Lee, S.J.; Yune, S.K.; Ha, J.H.; Chung, S.J.; Choi, H.; Seo, C.S.; Hong, K.E. The reliability and validity of the junior temperament and character inventory. Compr. Psychiatry 2004, 45, 121–128. [Google Scholar] [CrossRef]
- Jeong, H.; Lee, H.K.; Kwon, Y.-S.; Yim, H.W.; Lee, S.-Y. Gaming disorder and bidirectional relationships with aggression and impulsivity. Curr. Opin. Behav. Sci. 2020, 31, 69–75. [Google Scholar] [CrossRef]
- Cho, S.C.; Lee, Y.S. Development of the Korean form of the Kovacs’ Childeren’s Depression Inventory. J. Korean Neuropsychiatr. Assoc. 1990, 29, 943–956. [Google Scholar]
- Beck, A.; Steer, R.; Brown, G. Manual for the Beck depression inventory-II (BDI-II). Behav. Res. Ther. 1996, 37, 183–190. [Google Scholar]
- Cho, S.C.; Choi, C.J. Development of the Korean form of the State-Trait anxiety Inventory for Children. Seoul J. Psychiatry 1989, 14, 150–157. [Google Scholar]
- Kim, J.T. Relationship between State-Train Anxiety and Socializing; Korea University: Seoul, Korea, 1978. [Google Scholar]
- Patton, J.H.; Stanford, M.S.; Barratt, E.S. Factor structure of the Barratt impulsiveness scale. J. Clin. Psychol. 1995, 51, 768–774. [Google Scholar] [CrossRef]
- HS, L. Manual for Impulsivity Test; Guidance Korea: Seong Nam, Korea, 1992. [Google Scholar]
- Bahn, G.H.; Shin, M.S.; Cho, S.C.; Hong, K.E. A Preliminary Study For The Development Of The Assessment Scale For Adhd In Adolescents:Reliability And Validity For Cass(S). J. Korean Acad. Child Adolesc. Psychiatry 2001, 12, 218–224. [Google Scholar]
- Robbins, S.B.; Payne, E.C.; Chartrand, J.M. Goal instability and later life adjustment. Psychol. Aging 1990, 5, 447–450. [Google Scholar] [CrossRef]
- Lee, E.H. The role of goal instability and resolving style of problems between nurses’ job stressors and emotional exhaustion. Korean J. Woman Psychol. 2008, 13, 397–413. [Google Scholar] [CrossRef]
- Kim, B.H.; Bang, S.Y.; Lee, H.K.; Cho, S.S.; Choi, S.; Ryu, C.S. Developing and Study of happiness index of Korean Adolescents; Happy Home Foundation: Seoul, Korea, 2007. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Choi, E.S. Psychometric test of the PedsQLTM 4.0 Generic Core Scale in Korean adolescents. 2004. Available online: http://dcollection.yonsei.ac.kr/public_resource/pdf/000000125930_20200701160223.pdf (accessed on 3 May 2020).
- Nakhoul, L.; Obeid, S.; Sacre, H.; Haddad, C.; Soufia, M.; Hallit, R.; Akel, M.; Salameh, P.; Hallit, S. Attachment style and addictions (alcohol, cigarette, waterpipe and internet) among Lebanese adolescents: A national study. BMC Psychol. 2020, 8, 33. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Shen, L.X.; Yan, C.H.; Hu, H.; Yang, F.; Wang, L.; Kotha, S.R.; Ouyang, F.; Zhang, L.N.; Liao, X.P.; et al. Parent-adolescent interaction and risk of adolescent internet addiction: A population-based study in Shanghai. BMC Psychiatry 2014, 14, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanafi, E.; Siste, K.; Wiguna, T.; Kusumadewi, I.; Nasrun, M.W. Temperament profile and its association with the vulnerability to smartphone addiction of medical students in Indonesia. PLoS ONE 2019, 14, e0212244. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, A.; Avila, J.J.; Palao, D.J.; Montejo, A.L. Influence of Personality Traits on the Severity of Alcohol Use Disorders. J. Clin. Med. 2018, 7, 127. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.; Namkoong, K.; Lee, J.; Lee, B.O.; Jung, Y.C. Lateral orbitofrontal gray matter abnormalities in subjects with problematic smartphone use. J. Behav. Addict. 2019, 8, 404–411. [Google Scholar] [CrossRef]
- Schweizer, A.; Berchtold, A.; Barrense-Dias, Y.; Akre, C.; Suris, J.C. Adolescents with a smartphone sleep less than their peers. Eur. J. Pediatr. 2017, 176, 131–136. [Google Scholar] [CrossRef]
- Heo, J.Y.; Kim, K.; Fava, M.; Mischoulon, D.; Papakostas, G.I.; Kim, M.J.; Kim, D.J.; Chang, K.J.; Oh, Y.; Yu, B.H.; et al. Effects of smartphone use with and without blue light at night in healthy adults: A randomized, double-blind, cross-over, placebo-controlled comparison. J. Psychiatr. Res. 2017, 87, 61–70. [Google Scholar] [CrossRef]
- Jeong, H.; Yim, H.W.; Lee, S.Y.; Lee, H.K.; Potenza, M.N.; Kwon, J.H.; Koo, H.J.; Kweon, Y.S.; Bhang, S.Y.; Choi, J.S. Discordance between self-report and clinical diagnosis of Internet gaming disorder in adolescents. Sci. Rep. 2018, 8, 10084. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.; Fendrich, M. Modeling sources of self-report bias in a survey of drug use epidemiology. Ann. Epidemiol. 2005, 15, 381–389. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Recovered Group (n = 21) | Persistent Group (n = 35) | p | |
|---|---|---|---|
| Age (years) | 12.2 ± 3.0 | 13.7 ± 2.5 | 0.083 |
| Sex | 0.822 | ||
| Male | 15 (71.4%) | 24 (68.6%) | |
| Female | 6 (28.6%) | 11 (31.4%) | |
| Education status of mother | 0.288 | ||
| High school or lower | 13 (61.9%) | 22 (75.9%) | |
| College or higher | 8 (38.1%) | 7 (24.0%) | |
| Subjective economic status † | 0.537 | ||
| Low | 7 (36.8%) | 11 (35.5%) | |
| Middle | 6 (31.6%) | 6 (19.4%) | |
| Upper-middle or above | 6 (31.6%) | 14 (45.2%) | |
| Living without father | 7 (33.3%) | 12 (35.3%) | 0.882 |
| Living without mother | 0 (0%) | 5 (14.7%) | 0.065 |
| Conversation time with mother (min) | |||
| Weekday (average) | 150.7 ± 166.6 | 71.7 ± 92.7 | 0.002 ** |
| Weekend (average) | 215.5 ± 327.1 | 142.8 ± 264.0 | 0.092 |
| Smartphone use start (age) | 8.5 ± 1.5 | 9.2 ± 2.3 | 0.369 |
| Ownership of smartphone (+) † | 20 (95.2%) | 34 (97.1%) | >0.999 |
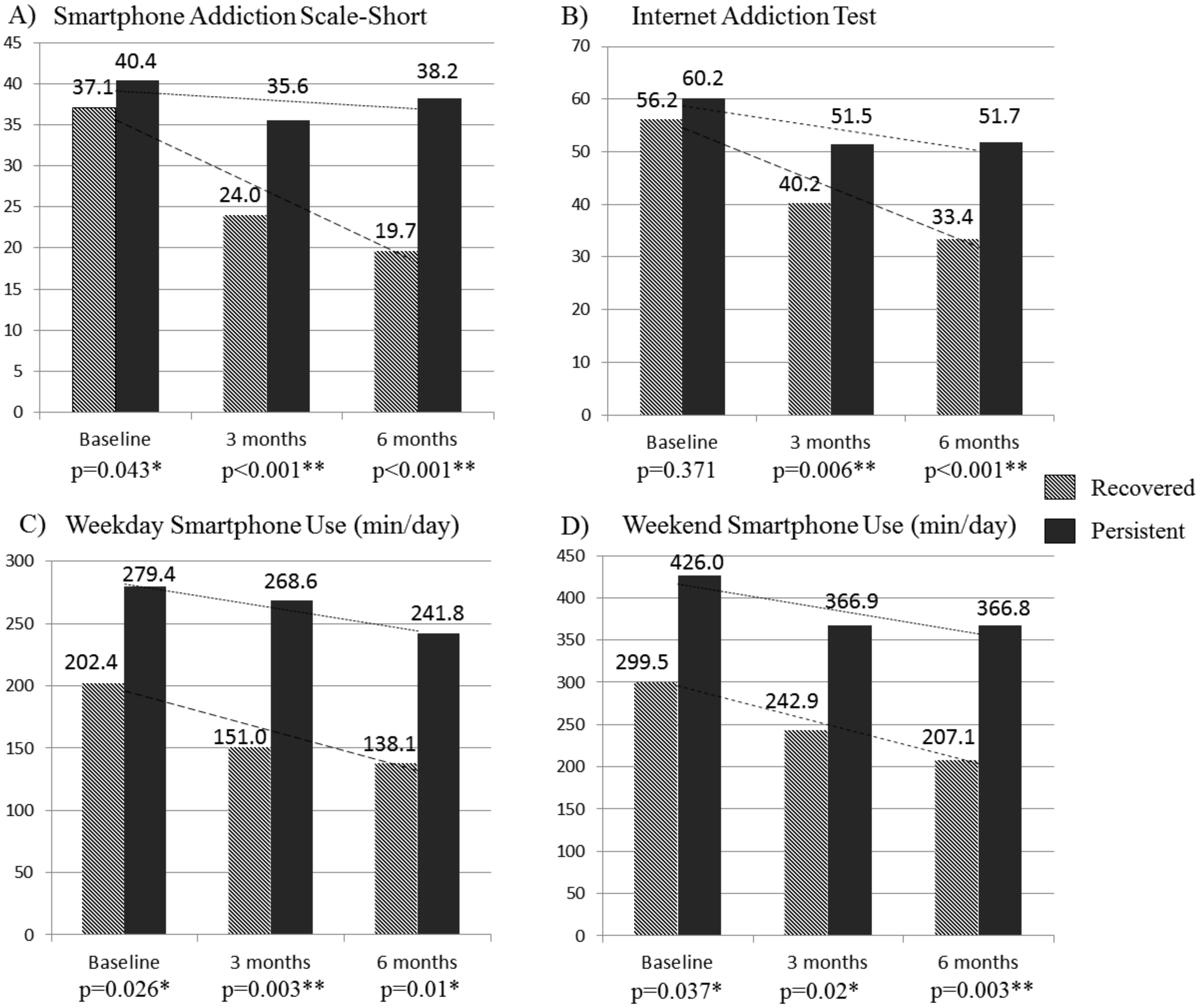
| Smartphone Addiction Scale-Short | 37.1 ± 5.6 | 40.4 ± 6.0 | 0.043 * |
| Internet Addiction Test score | 56.2 ± 14.9 | 60.22 ± 14.7 | 0.371 |
| Mobile/smartphone use time (min) | |||
| Weekday (average) | 202.4 ± 111.8 | 279.43 ± 146.9 | 0.026 * |
| Weekend (average) | 299.5 ± 137.5 | 426.00 ± 226.2 | 0.037 * |
| Internet use time (min) | |||
| Weekday (average) | 211.4 ± 84.0 | 282.9 ± 132.2 | 0.044 * |
| Weekend (average) | 352.9 ± 158.7 | 444.0 ± 200.2 | 0.108 |
| Internet content use | |||
| News | 9 (42.9%) | 11 (31.4%) | 0.388 |
| Adult material | 3 (14.3%) | 12 (34.3%) | 0.102 |
| Online game | 13 (61.9%) | 26 (74.3%) | 0.329 |
| Blog | 9 (42.9%) | 6 (17.1%) | 0.035 |
| Social networking service | 14 (66.7%) | 20 (57.1%) | 0.480 |
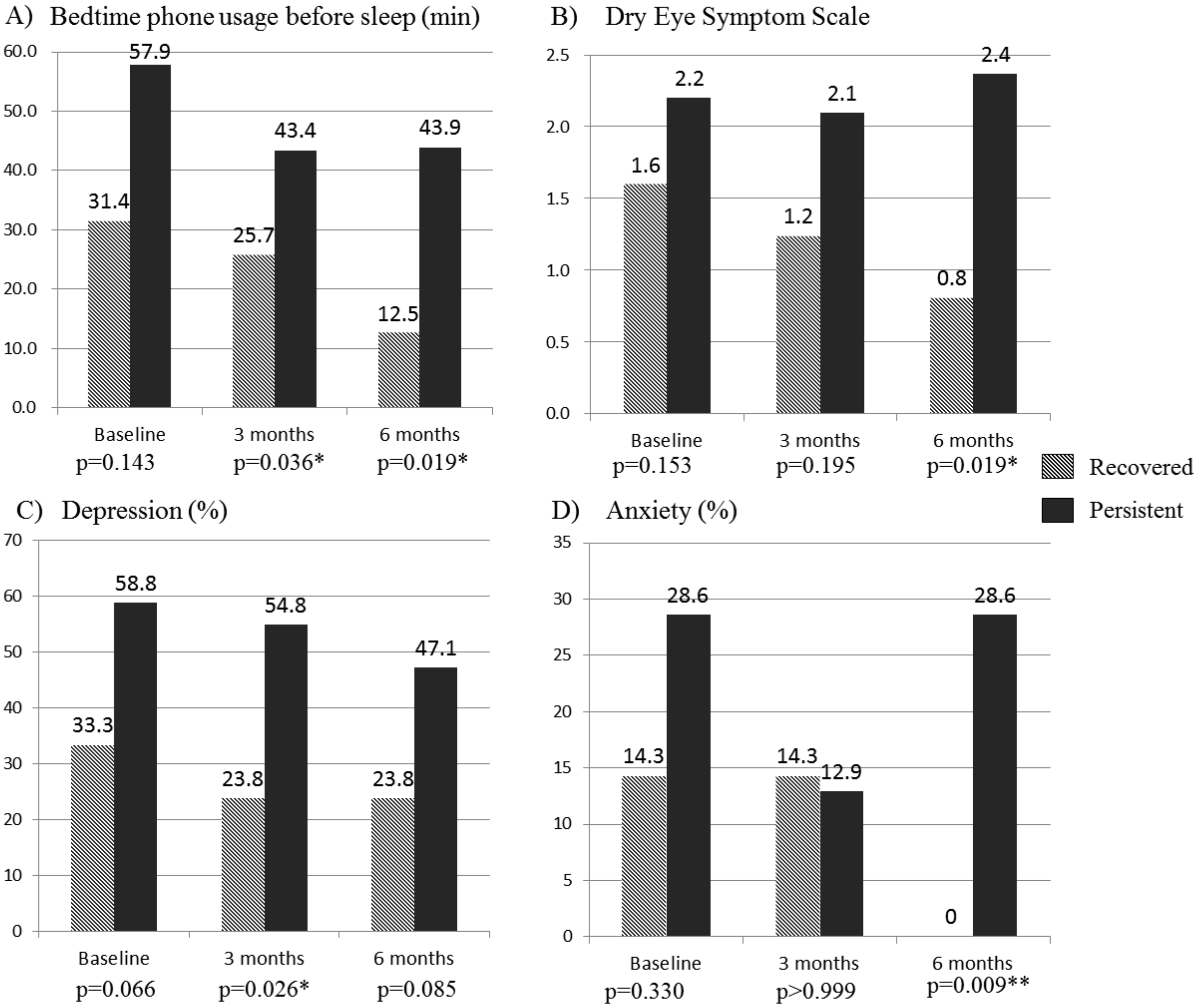
| Bedtime phone use before sleep (min) | 31.4 ± 38.2 | 57.86 ± 61.1 | 0.143 |
| Recovered Group (n = 21) | Persistent Group (n = 35) | p | |
|---|---|---|---|
| Psychological Assessment | |||
| Novelty seeking (T-score) | 52.1 ± 8.3 | 52.0 ± 10.3 | 0.658 |
| Harm avoidance (T-score) | 46.8 ± 12.0 | 55.8 ± 10.2 | 0.014 * |
| History of Psychiatric diagnosis † | |||
| Depression (+) | 2 (9.5%) | 8 (22.9%) | 0.290 |
| Attention deficit hyperactivity disorder (+) | 4 (19.0%) | 7 (20.0%) | >0.999 |
| Depression (+) status | 7 (33.3%) | 20 (58.8%) | 0.066 |
| CDI (n = 14) ∮ | 10.6 ± 4.8 | 18.0 ± 6.9 | 0.060 |
| BDI (n = 41) ∮ | 17.3 ± 17.9 | 18.7 ± 12.8 | 0.306 |
| Anxiety (+) status † | 3 (14.3%) | 10 (28.6%) | 0.330 |
| SAIC (n = 14) ∮ | 27.0 ± 3.5 | 35.2 ± 2.9 | 0.002 ** |
| STAI-X (n = 42) ∮ | 43.2 ± 14.9 | 47.4 ± 13.4 | 0.355 |
| Barratt Impulsiveness Scale-II | 56.1 ± 9.1 | 61.0 ± 6.9 | 0.036 * |
| Goal instability | 29.9 ± 13.0 | 38.9 ± 10.8 | 0.008 ** |
| CASS-Short form | 25.9 ± 9.8 | 28.8 ± 10.6 | 0.436 |
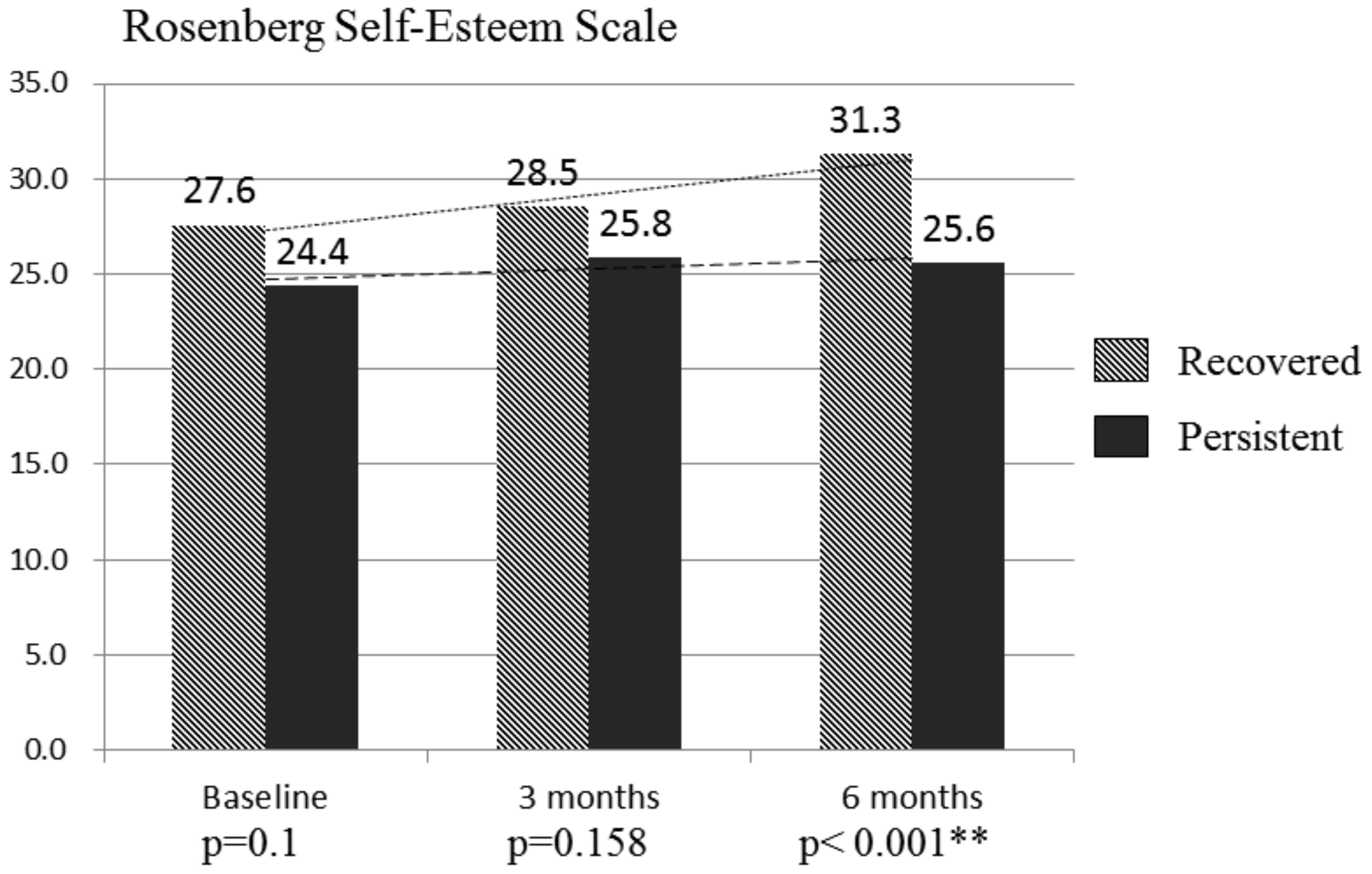
| Rosenberg Self-Esteem Scale | 27.6 ± 6.4 | 24.4 ± 5.4 | 0.100 |
| Quality of life | 1911.9 ± 350.3 | 1472.1 ± 420.4 | <0.001 ** |
| Happiness scale | 60.1 ± 16.1 | 49.1 ± 12.9 | 0.006 ** |
| Physical Assessment | |||
| Body mass index | 22.6 ± 5.0 | 21.9 ± 5.9 | 0.264 |
| Dry Eye Scale | 1.6 ± 2.2 | 2.2 ± 2.1 | 0.153 |
| Musculoskeletal pain (+) | |||
| Neck | 2 (9.5%) | 15 (42.9%) | 0.009 ** |
| Shoulder † | 1 (4.8%) | 9 (25.7%) | 0.072 |
| Hand/Wrist/Finger † | 2 (9.5%) | 7 (20.0%) | 0.459 |
| Recovered Group (n = 21) | Persistent Group (n = 35) | p | Cohens’ d | ||
|---|---|---|---|---|---|
| Barratt Impulsiveness Scale-II | 3 months | 54.3 ± 11.1 | 57.0 ± 9.3 | 0.373 | 0.26 |
| 6 months | 53.0 ± 10.1 | 57.0 ± 8.5 | 0.1 | 0.43 | |
| Goal instability | 3 months | 28.2 ± 10.6 | 33.9 ± 11.5 | 0.073 | 0.52 |
| 6 months | 25.5 ± 12.1 | 34.7 ± 13.0 | 0.011 * | 0.73 | |
| Quality of life | 3 months | 1994.1 ± 246.7 | 1591.7 ± 405.9 | <0.001 ** | 1.2 |
| 6 months | 2078.6 ± 271.7 | 1612.1 ± 451.7 | <0.001 ** | 1.25 | |
| Happiness scale | 3 months | 60.9 ± 16.8 | 52.0 ± 16.1 | 0.077 | 0.54 |
| 6 months | 60.7 ± 11.1 | 50.0 ± 14.2 | 0.003 ** | 0.84 | |
| Cramer’s V | |||||
| Neck pain | 3 months | 3 (14.3%) | 8 (24.2%) | 0.691 † | 0.17 (p = 0.46) |
| 6 months | 2 (10.0%) | 10 (35.7%) | 0.043 * | 0.29 (p = 0.04) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-Y.; Lee, H.K.; Choi, J.-S.; Bang, S.-y.; Park, M.-H.; Jung, K.-I.; Kweon, Y.-S. The Matthew Effect in Recovery from Smartphone Addiction in a 6-Month Longitudinal Study of Children and Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 4751. https://doi.org/10.3390/ijerph17134751
Lee S-Y, Lee HK, Choi J-S, Bang S-y, Park M-H, Jung K-I, Kweon Y-S. The Matthew Effect in Recovery from Smartphone Addiction in a 6-Month Longitudinal Study of Children and Adolescents. International Journal of Environmental Research and Public Health. 2020; 17(13):4751. https://doi.org/10.3390/ijerph17134751
Chicago/Turabian StyleLee, Seung-Yup, Hae Kook Lee, Jung-Seok Choi, Soo-young Bang, Min-Hyeon Park, Kyu-In Jung, and Yong-Sil Kweon. 2020. "The Matthew Effect in Recovery from Smartphone Addiction in a 6-Month Longitudinal Study of Children and Adolescents" International Journal of Environmental Research and Public Health 17, no. 13: 4751. https://doi.org/10.3390/ijerph17134751