Effects of Mind–Body Interventions Involving Meditative Movements on Quality of Life, Depressive Symptoms, Fear of Falling and Sleep Quality in Older Adults: A Systematic Review with Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
- Full-text articles published in English in a peer-reviewed journal;
- Participants were older adults aged 59 years or above and the mean age of study samples was ≥65 years (P);
- Mind–body interventions involving meditative movements as a generic term for interventions at low to moderate intensity uniting a meditative state of mind, conscious breath and movement such as Tai Chi or Yoga (I);
- Control groups that did not follow physical exercise intervention like aerobic exercise, strength exercise, any mind–body intervention, stretching, or relaxation exercise (CON) as comparators (e.g., wait-list control group, inactive control group, health education or usual care) (C);
- Parameters related to quality of life, depressive symptoms, fear of falling and sleep quality served as outcome measures (O);
- (Cluster) randomized controlled intervention studies with pre- and post-testing (S);
- A PEDro (Physiotherapy Evidence Database) score of at least five to achieve high methodological quality.
- Older adults with mental disorders such as mild cognitive impairment (MCI), dementia or depression;
- No adequate control condition or control group;
- No regular supervised intervention during the study period;
- Intervention not delivered in group format;
- Intervention without movement (e.g., guided imagery);
- Outcome not assignable to target outcomes (see inclusion criteria).
2.3. Assessment of Methodological Study Quality
2.4. Data Extraction and Interventions
2.5. Statistical Analysis
3. Results
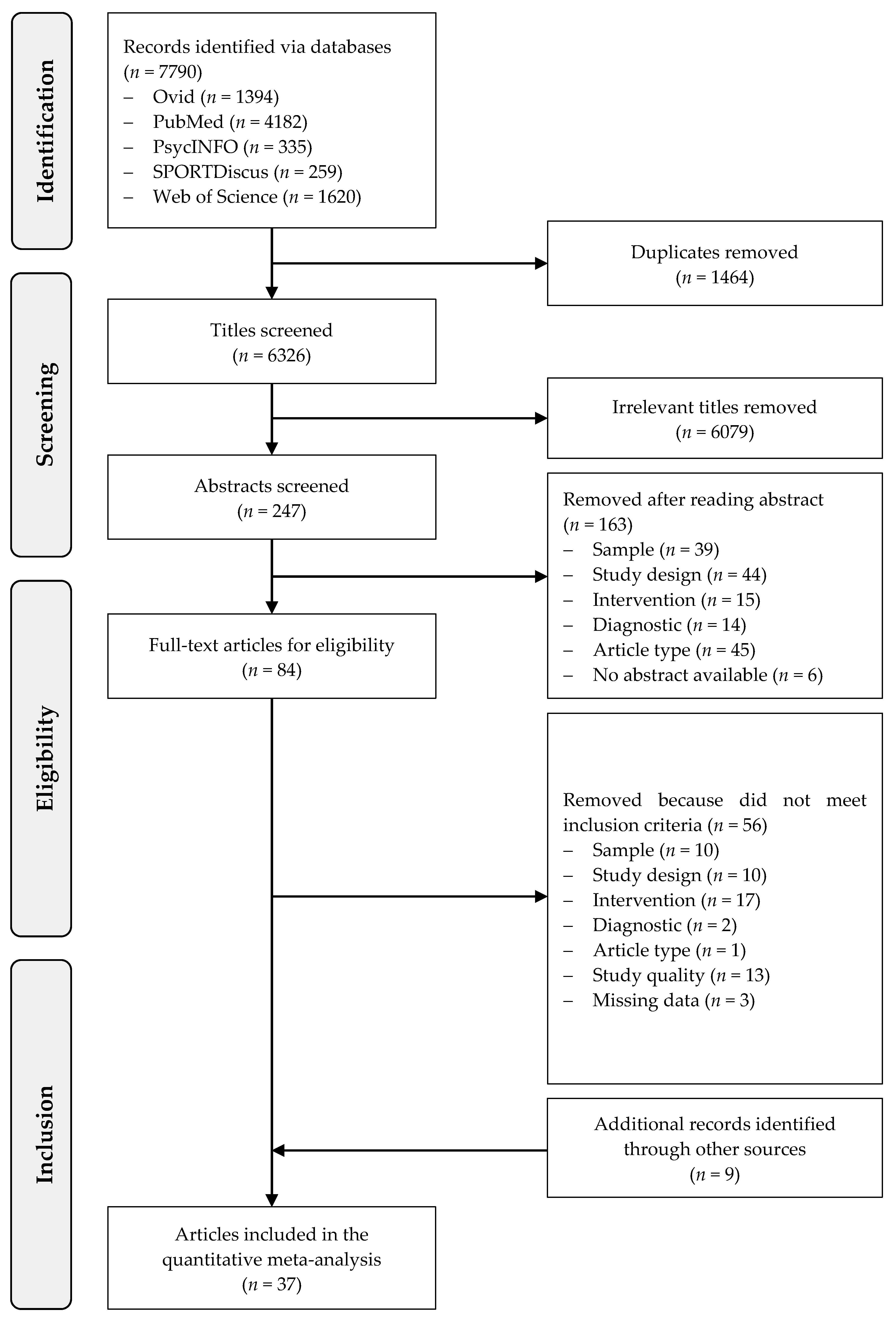
3.1. Trial Flow
3.2. Study Characteristics
3.2.1. Participants
3.2.2. Interventions
3.2.3. Outcomes and Instruments
3.3. Risk of Bias Assessment
3.4. Effects on Quality of Life
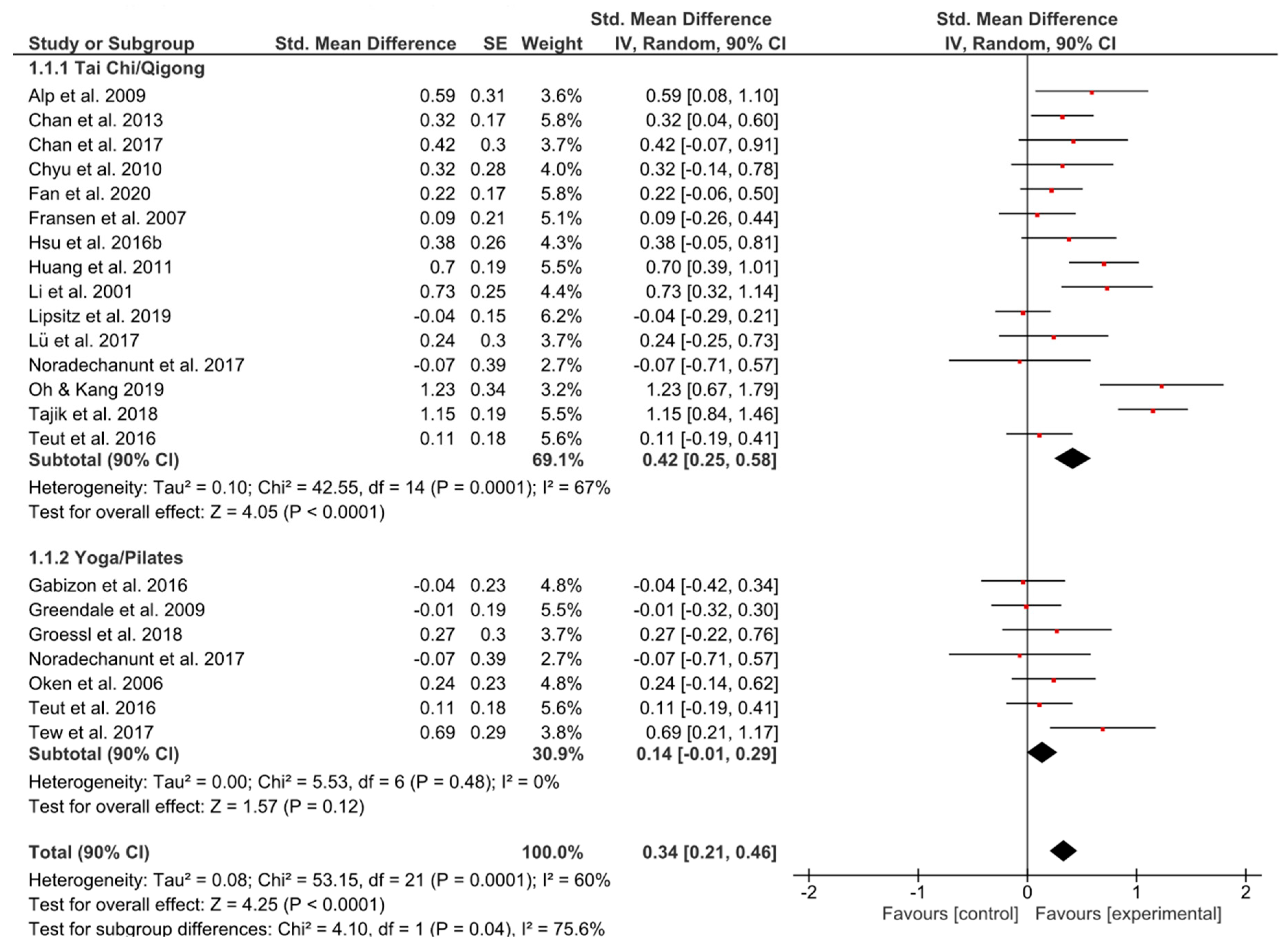
3.4.1. Overall
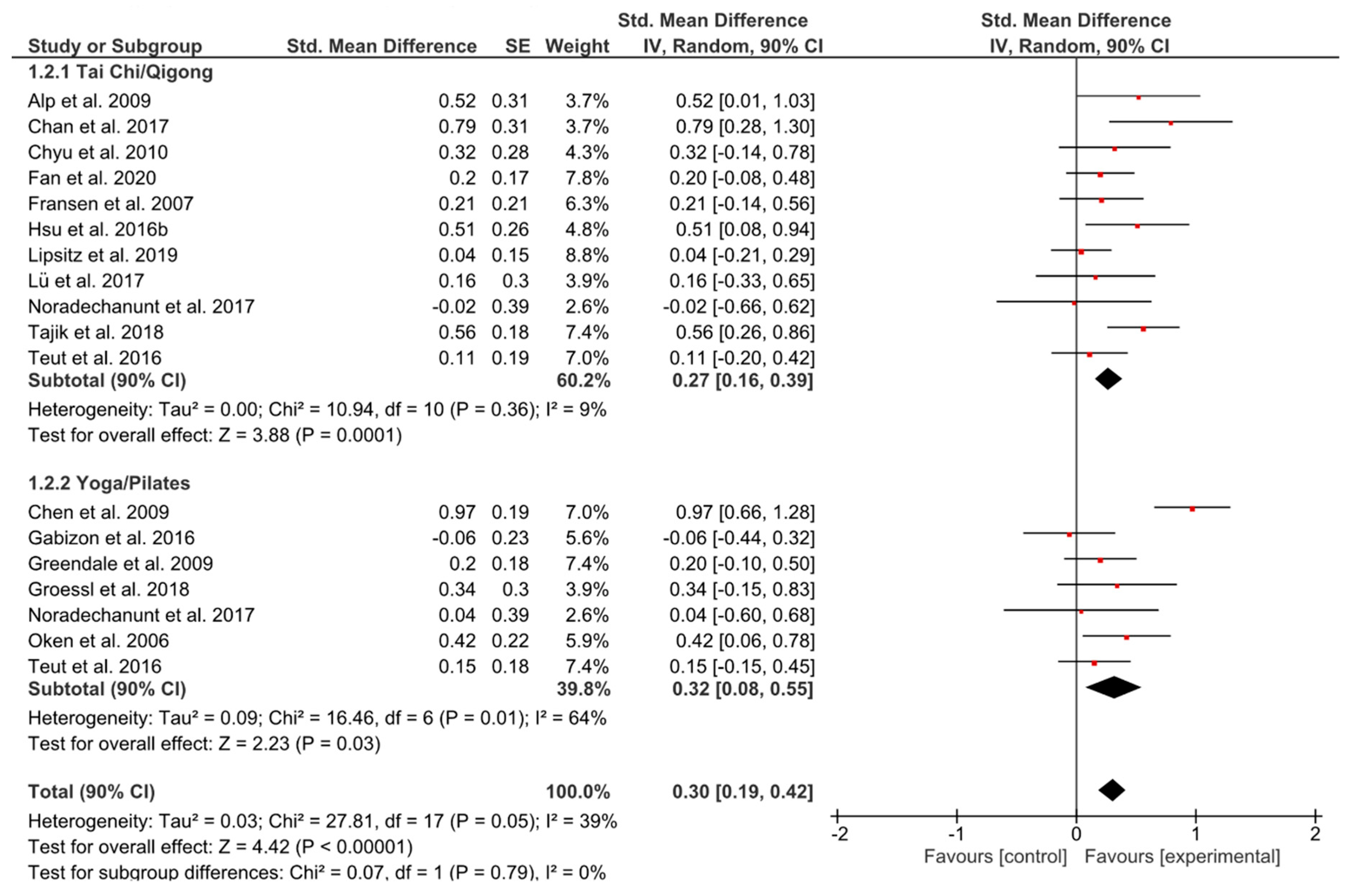
3.4.2. Physical Functioning
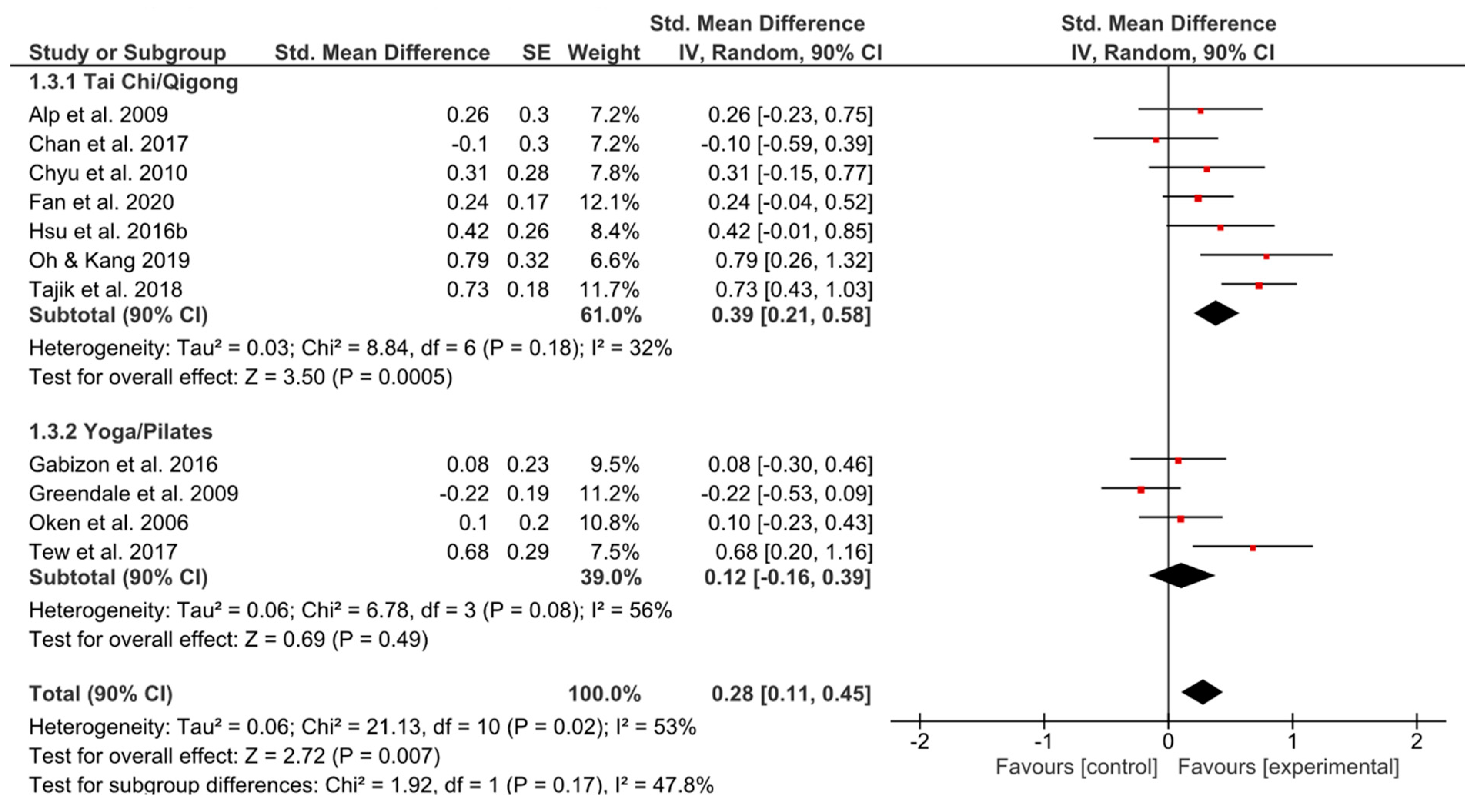
3.4.3. Psychological Functioning
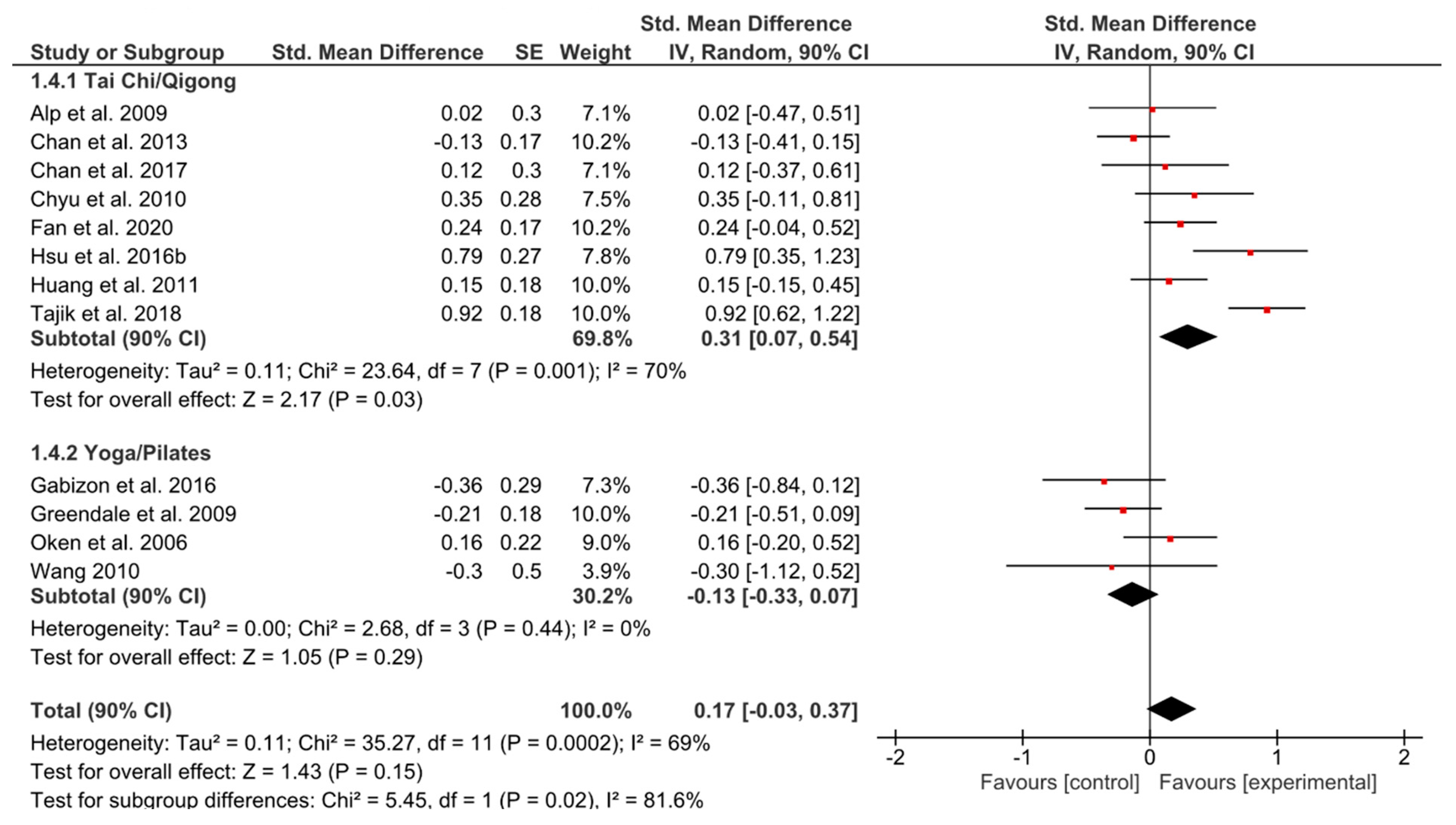
3.4.4. Social Functioning
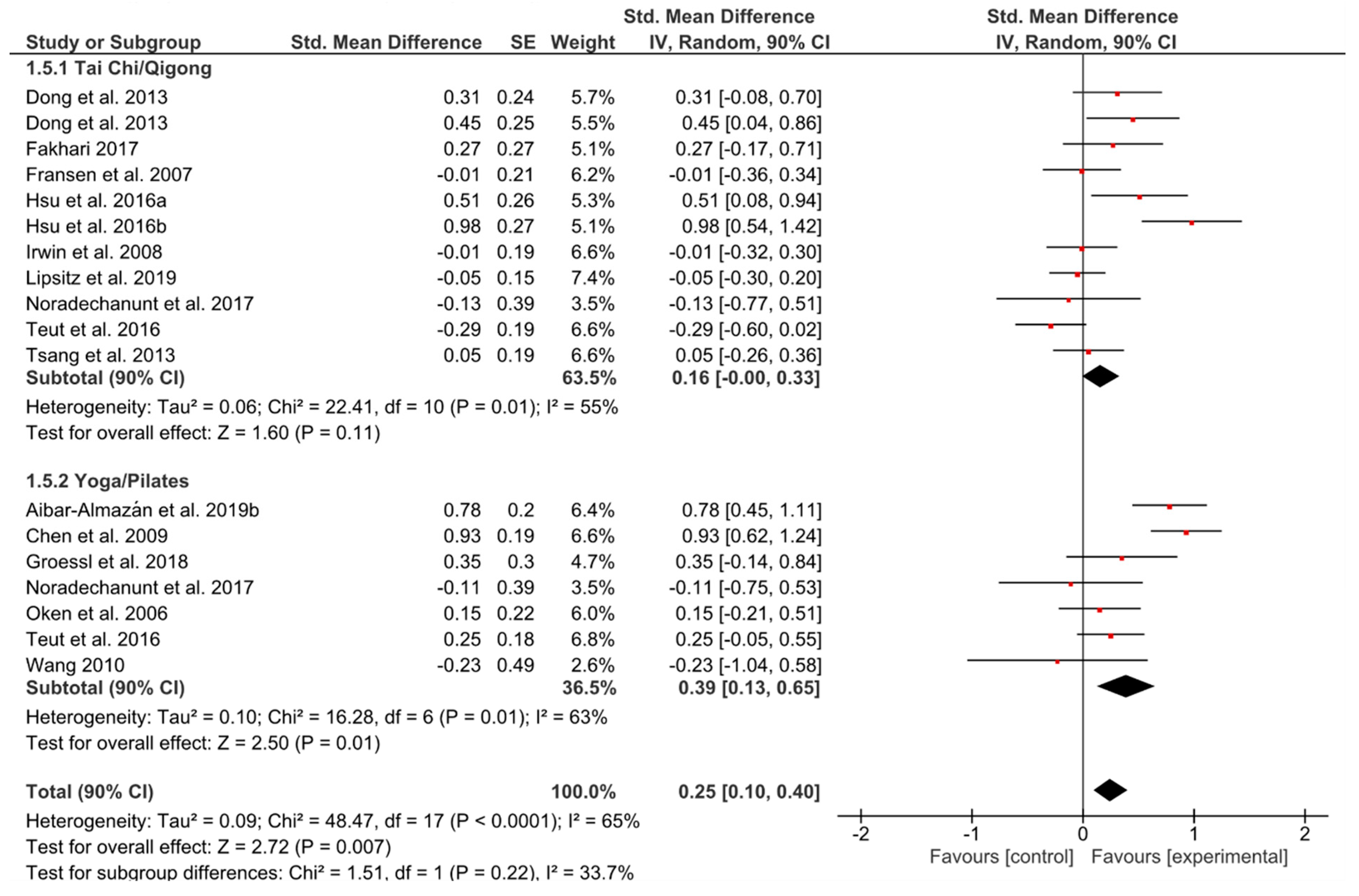
3.5. Effects on Depressive Symptoms, Fear of Falling and Sleep Quality
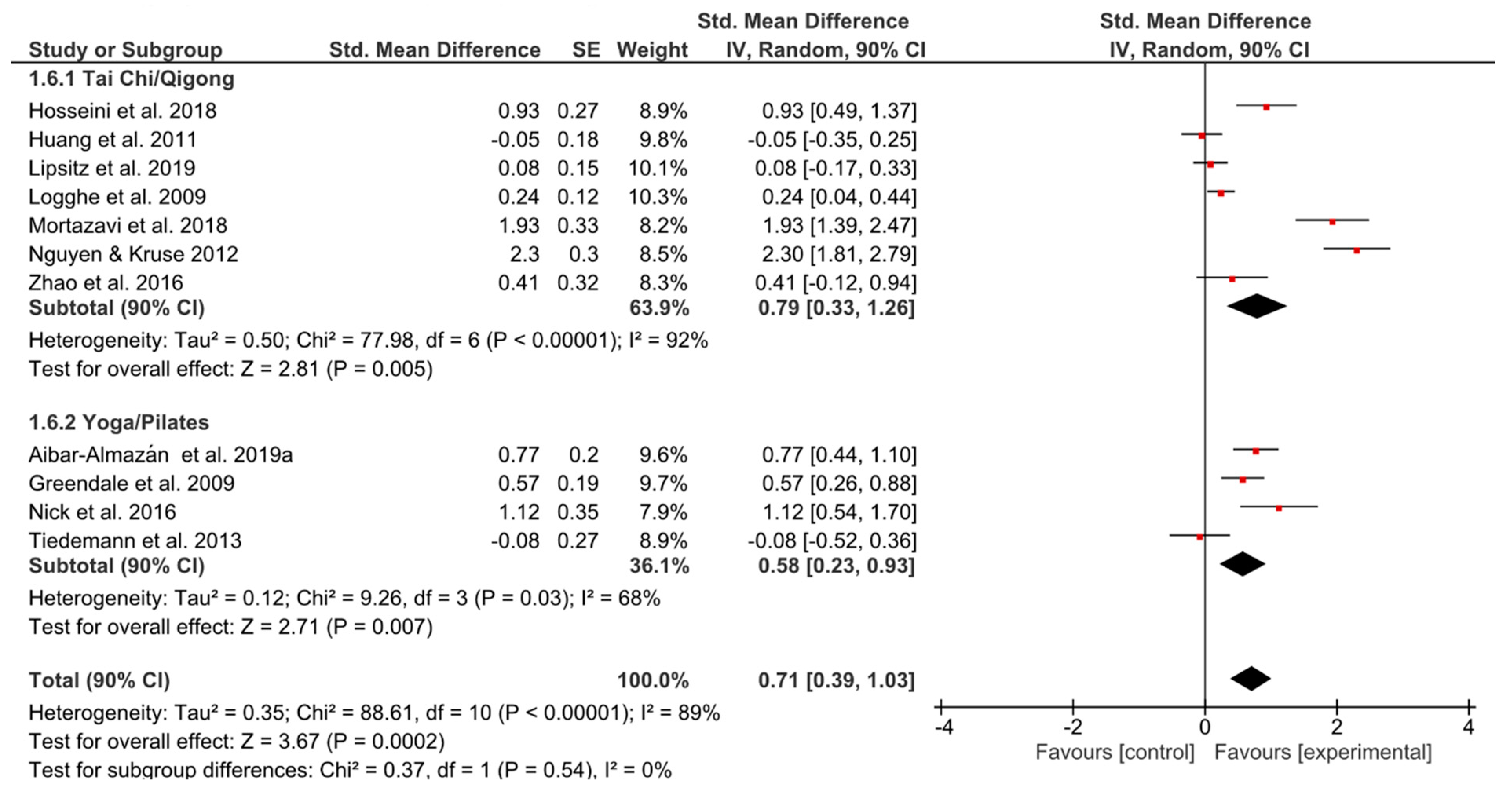
3.5.1. Depressive Symptoms
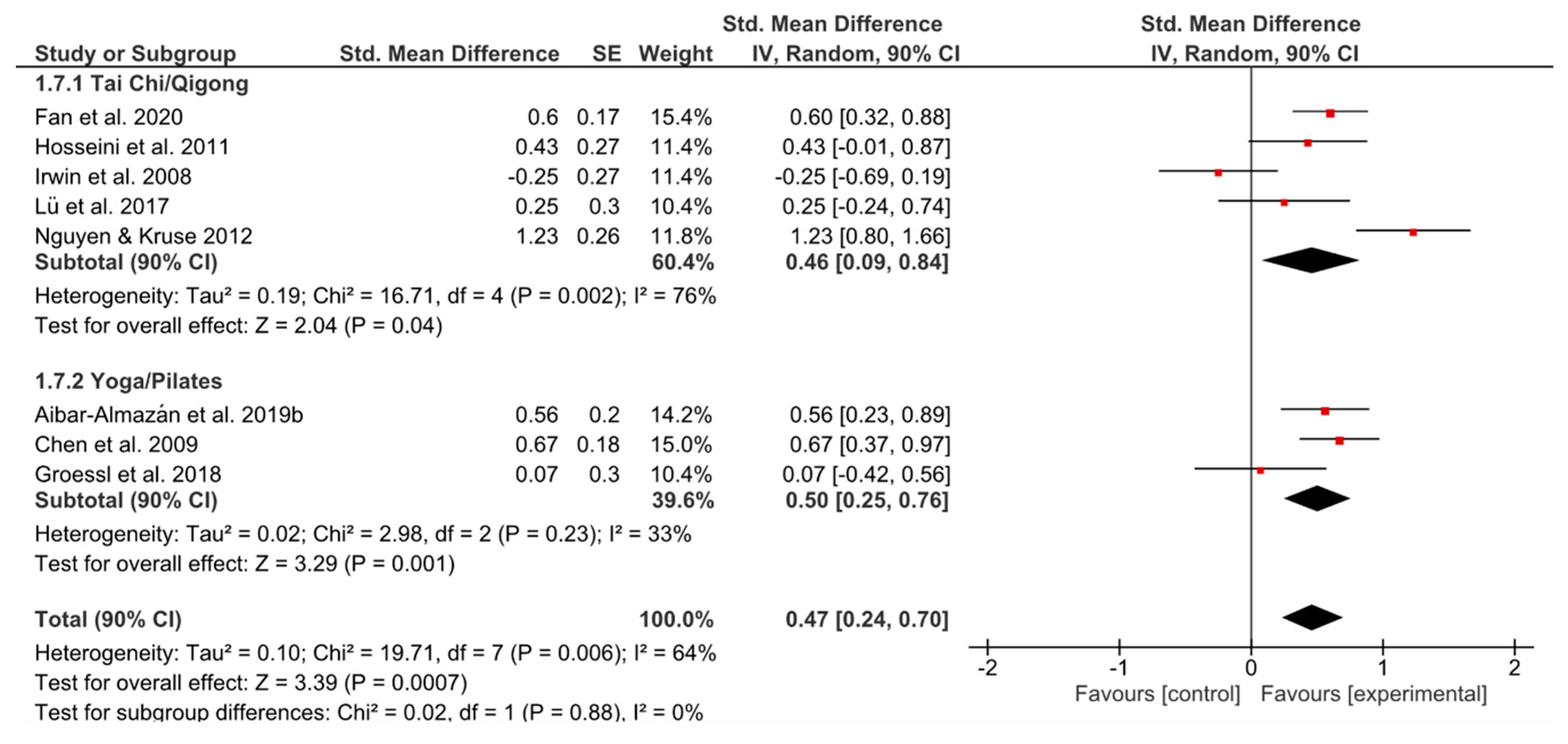
3.5.2. Fear of Falling
3.5.3. Sleep Quality
3.6. Effects of Training Frequency
4. Discussion
4.1. Strengths and Limitations
4.2. Implications and Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- McCombe, G.; Fogarty, F.; Swan, D.; Hannigan, A.; Fealy, G.M.; Kyne, L.; Meagher, D.; Cullen, W. Identified mental disorders in older adults in primary care: A cross-sectional database study. Eur. J. Gen. Pract. 2018, 24, 84–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations (UN), Department of Economic and Social Affairs, Population Division. World Population Prospects 2019: Highlights. 2019. Available online: https://population.un.org/wpp/Publications/Files/WPP2019_Highlights.pdf (accessed on 9 March 2020).
- Chou, C.-H.; Hwang, C.-L.; Wu, Y.-T. Effect of Exercise on physical function, daily living activities, and quality of life in the frail older adults: A meta-analysis. Arch. Phys. Med. Rehabil. 2012, 93, 237–244. [Google Scholar] [CrossRef]
- Chang, P.-S.; Knobf, T.; Oh, B.; Funk, M. Physical and psychological health outcomes of Qigong exercise in older adults: A systematic review and meta-analysis. Am. J. Chin. Med. 2019, 47, 301–322. [Google Scholar] [CrossRef] [PubMed]
- Rogers, C.E.; Larkey, L.K.; Keller, C. A review of clinical trials of Tai Chi and Qigong in older adults. West. J. Nurs. Res. 2009, 31, 245–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payne, P.; Crane-Godreau, M.A. Meditative movement for depression and anxiety. Front. Psychiatry 2013, 4, 71. [Google Scholar] [CrossRef] [Green Version]
- Morone, N.E.; Greco, C.M. Mind-body interventions for chronic pain in older adults: A structured review. Pain Med. 2007, 8, 359–375. [Google Scholar] [CrossRef]
- Zou, L.; Sasaki, J.E.; Zeng, N.; Wang, C.; Sun, L. A systematic review with meta-analysis of mindful exercises on rehabilitative outcomes among poststroke patients. Arch. Phys. Med. Rehabil. 2018, 99, 2355–2364. [Google Scholar] [CrossRef]
- Larkey, L.; Jahnke, R.; Etnier, J.; Gonzalez, J. Meditative movement as a category of exercise: Implications for research. J. Phys. Act. Heal. 2009, 6, 230–238. [Google Scholar] [CrossRef] [Green Version]
- Wahbeh, H.; Elsas, S.-M.; Oken, B.S. Mind-body interventions—Applications in neurology. Neurology 2008, 70, 2321–2328. [Google Scholar] [CrossRef] [Green Version]
- Zou, L.; Sasaki, J.E.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M. A Systematic review and meta-analysis of Baduanjin Qigong for health benefits: Randomized controlled trials. Evidence-based Complement. Altern. Med. 2017. [Google Scholar] [CrossRef]
- Eyre, H.A.; Acevedo, B.; Yang, H.; Siddarth, P.; Van Dyk, K.; Ercoli, L.; Leaver, A.M.; Cyr, N.S.; Narr, K.; Baune, B.T.; et al. Changes in neural connectivity and memory following a Yoga intervention for older adults: A pilot study. J. Alzheimer’s Dis. 2016, 52, 673–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, J.S.Y.; Deng, K.; Wu, J.; Yan, J.H.; Heyn, P.C. Effects of meditation and mind-body exercises on older adults’ cognitive performance: A meta-analysis. Gerontologist 2019, 59, e782–e790. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, C.; Zou, L.; Liu, X.; Song, W. The effects of mind-body exercise on cognitive performance in elderly: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2018, 15, 2791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, A.L.; Bird, M.-L.; Talevski, J. Effect of Pilates exercise for improving balance in older adults: A systematic review with meta-analysis. Arch. Phys. Med. Rehabil. 2015, 96, 715–723. [Google Scholar] [CrossRef]
- D’Silva, S.; Poscablo, C.; Habousha, R.; Kogan, M.; Kligler, B. Mind-body medicine therapies for a range of depression severity: A systematic review. Psychosomatics 2012, 53, 407–423. [Google Scholar] [CrossRef] [PubMed]
- Kwok, J.Y.Y.; Choi, K.C.; Chan, H.Y.L. Effects of mind-body exercises on the physiological and psychosocial well-being of individuals with Parkinson’s disease: A systematic review and meta-analysis. Complement. Ther. Med. 2016, 29, 121–131. [Google Scholar] [CrossRef]
- Laird, K.T.; Paholpak, P.; Roman, M.; Rahi, B.; Lavretsky, H. Mind-body therapies for late-life mental and cognitive health. Curr. Psychiatry Rep. 2018, 20, 2. [Google Scholar] [CrossRef]
- Gouw, V.X.H.; Jiang, Y.; Seah, B.; He, H.; Hong, J.; Wang, W. Effectiveness of internal Qigong on quality of life, depressive symptoms and self-efficacy among community-dwelling older adults with chronic disease: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2019, 99, 103378. [Google Scholar] [CrossRef]
- Samad, Z.; Brealey, S.; Gilbody, S. The effectiveness of behavioural therapy for the treatment of depression in older adults: A meta-analysis. Int. J. Geriatr. Psychiatry 2011, 26, 1211–1220. [Google Scholar] [CrossRef]
- Chi, I.; Jordan-Marsh, M.; Guo, M.; Xie, B.; Bai, Z. Tai chi and reduction of depressive symptoms for older adults: A meta-analysis of randomized trials. Geriatr. Gerontol. Int. 2013, 13, 3–12. [Google Scholar] [CrossRef]
- Bo, A.; Mao, W.; Lindsey, M.A. Effects of mind–body interventions on depressive symptoms among older Chinese adults: A systematic review and meta-analysis. Int. J. Geriatr. Psychiatry 2017, 32, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Williams, C.S. Falls, injuries due to falls, and the risk of admission to a nursing home. N. Engl. J. Med. 1997, 337, 1279–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, A.; Delbaere, K.; Zijlstra, G.A.R.; Carpenter, H.; Iliffe, S.; Masud, T.; Skelton, D.; Morris, R.; Kendrick, D. Exercise for reducing fear of falling in older people living in the community: Cochrane systematic review and meta-analysis. Age Ageing 2016, 45, 345–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delbaere, K.; Close, J.C.T.; Brodaty, H.; Sachdev, P.; Lord, S.R. Determinants of disparities between perceived and physiological risk of falling among elderly people: Cohort study. BMJ 2010, 341, c4165. [Google Scholar] [CrossRef] [PubMed]
- Harling, A.; Simpson, J.P. A systematic review to determine the effectiveness of Tai Chi in reducing falls and fear of falling in older adults. Phys. Ther. Rev. 2008, 13, 237–248. [Google Scholar] [CrossRef]
- Logghe, I.H.J.; Verhagen, A.P.; Rademaker, A.C.H.J.; Bierma-Zeinstra, S.M.A.; van Rossum, E.; Faber, M.J.; Koes, B.W. The effects of Tai Chi on fall prevention, fear of falling and balance in older people: A meta-analysis. Prev. Med. (Baltim) 2010, 51, 222–227. [Google Scholar] [CrossRef]
- Jahnke, R.; Larkey, L.; Rogers, C.; Etnier, J.; Lin, F. A comprehensive review of health benefits of Qigong and Tai Chi. Am. J. Health Promot. 2010, 24. [Google Scholar] [CrossRef]
- Wu, W.; Kwong, E.; Lan, X.; Jiang, X. The effect of a meditative movement intervention on quality of sleep in the elderly: A systematic review and meta-analysis. J. Altern. Complement. Med. 2015, 21, 509–519. [Google Scholar] [CrossRef]
- Ju, Y.E.S.; Lucey, B.P.; Holtzman, D.M. Sleep and Alzheimer disease pathology-a bidirectional relationship. Nat. Rev. Neurol. 2014, 10, 115–119. [Google Scholar] [CrossRef]
- Neuendorf, R.; Wahbeh, H.; Chamine, I.; Yu, J.; Hutchison, K.; Oken, B.S. The effects of mind-body interventions on sleep quality: A systematic review. Evidence-based Complement. Altern. Med. 2015, 1–17. [Google Scholar] [CrossRef]
- Fleming, K.M.; Herring, M.P. The effects of Pilates on mental health outcomes: A meta-analysis of controlled trials. Complement. Ther. Med. 2018, 37, 80–95. [Google Scholar] [CrossRef] [PubMed]
- Schure, M.B.; Christopher, J.; Christopher, S. Mind-Body medicine and the art of self-care: Teaching mindfulness to counseling students through Yoga, meditation, and Qigong. J. Couns. Dev. 2008, 86, 47–56. [Google Scholar] [CrossRef]
- Zhang, S.; Zou, L.; Chen, L.-Z.; Yao, Y.; Loprinzi, P.D.; Siu, P.M.; Wei, G.-X. The Effect of Tai Chi Chuan on negative emotions in non-clinical populations: A meta-analysis and systematic review. Int. J. Environ. Res. Public Health 2019, 16, 3033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Leeuwen, K.M.; Van Loon, M.S.; Van Nes, F.A.; Bosmans, J.E.; De Veti, H.C.W.; Ket, J.C.F.; Widdershoven, G.A.M.; Ostelo, R.W.J.G. What does quality of life mean to older adults? A thematic synthesis. PLoS ONE 2019, 14, 1–39. [Google Scholar] [CrossRef] [Green Version]
- Bulamu, N.B.; Kaambwa, B.; Ratcliffe, J. A systematic review of instruments for measuring outcomes in economic evaluation within aged care. Health Qual. Life Outcomes 2015, 13, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Makai, P.; Brouwer, W.B.F.; Koopmanschap, M.A.; Stolk, E.A.; Nieboer, A.P. Quality of life instruments for economic evaluations in health and social care for older people: A systematic review. Soc. Sci. Med. 2014, 102, 83–93. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Osypiuk, K.; Thompson, E.; Wayne, P.M. Can Tai Chi and Qigong postures shape our mood? Toward an embodied cognition framework for mind-body research. Front. Hum. Neurosci. 2018, 12. [Google Scholar] [CrossRef]
- Irez, G.B.; Ozdemir, R.A.; Evin, R.; Irez, S.G.; Korkusuz, F. Integrating Pilates exercise into an exercise program for 65+ year-old women to reduce falls. J. Sports Sci. Med. 2011, 10, 105–111. [Google Scholar]
- Deeks, J.J.; Higgins, J.P. Statistical algorithms in Review Manager 5; The Cochrane Collaboration: London, UK, 2016. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawerence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Aibar-Almazán, A.; Hita-Contreras, F.; Cruz-Díaz, D.; de la Torre-Cruz, M.; Jiménez-García, J.D.; Martínez-Amat, A. Effects of Pilates training on sleep quality, anxiety, depression and fatigue in postmenopausal women: A randomized controlled trial. Maturitas 2019, 124, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Aibar-Almazán, A.; Martínez-Amat, A.; Cruz-Díaz, D.; De la Torre-Cruz, M.J.; Jiménez-García, J.D.; Zagalaz-Anula, N.; Pérez-Herrezuelo, I.; Hita-Contreras, F. Effects of Pilates on fall risk factors in community-dwelling elderly women: A randomized, controlled trial. Eur. J. Sport Sci. 2019, 19, 1386–1394. [Google Scholar] [CrossRef]
- Fransen, M.; Nairn, L.; Winstanley, J.; Lam, P.; Edmonds, J. Physical activity for osteoarthritis management: A randomized controlled clinical trial evaluating hydrotherapy or Tai Chi classes. Arthritis Care Res. (Hoboken). 2007, 57, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Gabizon, H.; Press, Y.; Volkov, I.; Melzer, I. The effects of Pilates training on balance control and self-reported health status in community-dwelling older adults: A randomized controlled trial. J. Aging Phys. Act. 2016, 24, 376–383. [Google Scholar] [CrossRef]
- Greendale, G.A.; Huang, M.-H.; Karlamangla, A.S.; Seeger, L.; Crawford, S. Yoga decreases kyphosis in senior women and men with adult onset hyperkyphosis: Results of a randomized controlled trial. J. Am. Geriatr. Soc. 2009, 57, 1569–1579. [Google Scholar] [CrossRef] [Green Version]
- Groessl, E.J.; Maiya, M.; Schmalzl, L.; Wing, D.; Jeste, D.V. Yoga to prevent mobility limitations in older adults: Feasibility of a randomized controlled trial. BMC Geriatr. 2018, 18. [Google Scholar] [CrossRef]
- Hosseini, H.; Esfirizi, M.F.; Marandi, S.M.; Rezaei, A. The effect of Tai Chi exercise on the sleep quality of the elderly residents in Isfahan, Sadeghieh elderly home. Iran. J. Nurs. Midwifery Res. 2011, 16, 55–60. [Google Scholar]
- Hosseini, L.; Kargozar, E.; Sharifi, F.; Negarandeh, R.; Memari, A.H.; Navab, E. Tai Chi Chuan can improve balance and reduce fear of falling in community dwelling older adults: A randomized control trial. J. Exerc. Rehabil. 2018, 14, 1024–1031. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Moyle, W.; Cooke, M.; Jones, C. Seated Tai Chi versus usual activities in older people using wheelchairs: A randomized controlled trial. Complement. Ther. Med. 2016, 24, 1–6. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Moyle, W.; Cooke, M.; Jones, C. Seated T’ai Chi in older Taiwanese people using wheelchairs: A randomized controlled trial investigating mood states and self-efficacy. J. Altern. Complement. Med. 2016, 22, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.T.; Yang, L.H.; Liu, C.Y. Reducing the fear of falling among community-dwelling elderly adults through cognitive-behavioural strategies and intense Tai Chi exercise: A randomized controlled trial. J. Adv. Nurs. 2011, 67, 961–971. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R.; Olmstead, R.; Motivala, S.J. Improving sleep quality in older adults with moderate sleep complaints: A randomized controlled trial of Tai Chi Chih. Sleep 2008, 31, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Alp, A.; Cansever, Ş.; Görgeç, N.; Yurtkuran, M.; Topsaç, T. Effects of Tai Chi exercise on functional and life quality assessments in senile osteoporosis. Turkiye Klin. J. Med. Sci. 2009, 29, 687–695. [Google Scholar]
- Li, F.; Harmer, P.; McAuley, E.; John Fisher, K.; Duncan, T.E.; Duncan, S.C. Tai Chi, self-efficacy, and physical function in the elderly. Prev. Sci. 2001, 2, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Lipsitz, L.A.; Macklin, E.A.; Travison, T.G.; Manor, B.; Gagnon, P.; Tsai, T.; Aizpurua, I.I.; Lo, O.-Y.; Wayne, P.M. A cluster randomized trial of Tai Chi vs. health education in subsidized housing: The MI-WiSH study. J. Am. Geriatr. Soc. 2019, 67, 1812–1819. [Google Scholar] [CrossRef] [PubMed]
- Logghe, I.H.J.; Zeeuwe, P.E.M.; Verhagen, A.P.; Wijnen-Sponselee, R.M.T.; Willemsen, S.P.; Bierma-Zeinstra, S.M.A.; van Rossum, E.; Faber, M.J.; Koes, B.W. Lack of Effect of Tai Chi Chuan in preventing falls in elderly people living at home: A randomized clinical trial. J. Am. Geriatr. Soc. 2009, 57, 70–75. [Google Scholar] [CrossRef]
- Lü, J.; Huang, L.; Wu, X.; Fu, W.; Liu, Y. Effect of Tai Ji Quan training on self-reported sleep quality in elderly Chinese women with knee osteoarthritis: A randomized controlled trail. Sleep Med. 2017, 33, 70–75. [Google Scholar] [CrossRef]
- Mortazavi, H.; Tabatabaeicher, M.; Golestani, A.; Armat, M.; Yousefi, M. The effect of Tai Chi exercise on the risk and fear of falling in older adults: A randomized clinical trial. Mater. Socio Medica 2018, 30, 38. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, M.H.; Kruse, A. A randomized controlled trial of Tai Chi for balance, sleep quality and cognitive performance in elderly Vietnamese. Clin. Interv. Aging 2012, 7, 185–189. [Google Scholar] [CrossRef] [Green Version]
- Nick, N.; Petramfar, P.; Ghodsbin, F.; Keshavarzi, S.; Jahanbin, I. The effect of Yoga on balance and fear of falling in older adults. PM R 2016, 8, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Noradechanunt, C.; Worsley, A.; Groeller, H. Thai Yoga improves physical function and well-being in older adults: A randomised controlled trial. J. Sci. Med. Sport 2017, 20, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Oh, C.; Kang, H. Effects of Tai Chi exercise on the body composition, self-efficacy and life satisfaction of older adults in Korean local community. Int. J. Gerontol. 2019, 13, 134–138. [Google Scholar] [CrossRef]
- Oken, B.S.; Zajdel, D.; Kishiyama, S.; Flegal, K.; Dehen, C.; Haas, M.; Kraemer, D.F.; Lawrence, J.; Leyva, J. Randomized, controlled, six-month trial of Yoga in healthy seniors: Effects on cognition and quality of life. Altern. Ther. Health Med. 2006, 12, 40–47. [Google Scholar]
- Chan, A.W.K.; Lee, A.; Lee, D.T.F.; Sit, J.W.H.; Chair, S.Y. Evaluation of the sustaining effects of Tai Chi Qigong in the sixth month in promoting psychosocial health in COPD patients: A single-blind, randomized controlled trial. Sci. World J. 2013. [Google Scholar] [CrossRef] [Green Version]
- Tajik, A.; Rejeh, N.; Heravi-Karimooi, M.; Kia, P.S.; Tadrisi, S.D.; Watts, T.E.; Griffiths, P.; Vaismoradi, M. The effect of Tai Chi on quality of life in male older people: A randomized controlled clinical trial. Complement. Ther. Clin. Pract. 2018, 33, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Teut, M.; Knilli, J.; Daus, D.; Roll, S.; Witt, C.M. Qigong or Yoga versus no intervention in older adults with chronic low back pain—A randomized controlled trial. J. Pain 2016, 17, 796–805. [Google Scholar] [CrossRef]
- Tew, G.A.; Howsam, J.; Hardy, M.; Bissell, L. Adapted Yoga to improve physical function and health-related quality of life in physically-inactive older adults: A randomised controlled pilot trial. BMC Geriatr. 2017, 17. [Google Scholar] [CrossRef]
- Tiedemann, A.; O’Rourke, S.; Sesto, R.; Sherrington, C. A 12-week Iyengar Yoga program improved balance and mobility in older community-dwelling people: A pilot randomized controlled trial. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 68, 1068–1075. [Google Scholar] [CrossRef]
- Tsang, H.W.H.; Lee, J.L.C.; Au, D.W.H.; Wong, K.K.W.; Lai, K.W. Developing and testing the effectiveness of a novel health Qigong for frail elders in Hong Kong: A preliminary study. Evid. Based Complement. Altern. Med. 2013, 2013, 827392. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.S. Feasibility of a Yoga intervention for enhancing the mental well-being and physical functioning of older adults living in the community. Act. Adapt. Aging 2010, 34, 85–97. [Google Scholar] [CrossRef]
- Zhao, Y.; Chung, P.K.; Tong, T.K. Effectiveness of a community-based exercise program on balance performance and fear of falling in older nonfallers at risk for falling: A randomized, controlled study. J. Aging Phys. Act. 2016, 24, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.K.; Yu, D.S.F.; Choi, K.C. Effects of Tai Chi Qigong on psychosocial well-being among hidden elderly, using elderly neighborhood volunteer approach: A pilot randomized controlled trial. Clin. Interv. Aging 2017, 12, 85–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.M.; Chen, M.H.; Chao, H.C.; Hung, H.M.; Lin, H.S.; Li, C.H. Sleep quality, depression state, and health status of older adults after silver Yoga exercises: Cluster randomized trial. Int. J. Nurs. Stud. 2009, 46, 154–163. [Google Scholar] [CrossRef]
- Chyu, M.C.; James, C.R.; Sawyer, S.F.; Brismée, J.M.; Xu, K.T.; Poklikuha, G.; Dunn, D.M.; Shen, C.L. Effects of Tai Chi exercise on posturography, gait, physical function and quality of life in postmenopausal women with osteopaenia: A randomized clinical study. Clin. Rehabil. 2010, 24, 1080–1090. [Google Scholar] [CrossRef]
- Dong, L.; Lee, J.-B.; Kim, Y.-K.; Kim, Y.-S. The effects of health Qigong training of elderly single women on pain consciousness and depression. Int. J. Appl. Sport. Sci. 2013, 25, 118–126. [Google Scholar] [CrossRef]
- Fakhari, M. Effects of Tai Chi exercise on depression in older adults: A randomized controlled trial. Bali Med. J. 2017, 6, 679. [Google Scholar] [CrossRef]
- Fan, B.; Song, W.; Zhang, J.; Er, Y.; Xie, B.; Zhang, H.; Liao, Y.; Wang, C.; Hu, X.; Mcintyre, R.; et al. The efficacy of mind-body (Baduanjin) exercise on self-reported sleep quality and quality of life in elderly subjects with sleep disturbances: A randomized controlled trial. Sleep Breath. 2020. [Google Scholar] [CrossRef]
- Mortimer, J.A.; Ding, D.; Borenstein, A.R.; DeCarli, C.; Guo, Q.; Wu, Y.; Zhao, Q.; Chu, S. Changes in brain volume and cognition in a randomized trial of exercise and social interaction in a community-based sample of non-demented Chinese elders. J. Alzheimer’s Dis. 2012, 30, 757–766. [Google Scholar] [CrossRef] [Green Version]
- Blake, H.; Hawley, H. Effects of Tai Chi exercise on physical and psychological health of older people. Curr. Aging Sci. 2012, 5, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Nebiker, L.; Lichtenstein, E.; Minghetti, A.; Zahner, L.; Gerber, M.; Faude, O.; Donath, L. Moderating effects of exercise duration and intensity in neuromuscular vs. endurance exercise interventions for the treatment of depression: A meta-analytical review. Front. Psychiatry 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, P.; Bergmark, A. Compared with what? An analysis of control-group types in Cochrane and Campbell reviews of psychosocial treatment efficacy with substance use disorders. Addiction 2015, 110, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Andresen, E.M.; Malmgren, J.A.; Carter, W.B.; Patrick, D.L. Screening for depression in well older adults: Evaluation of a short form of the CES-D. Am. J. Prev. Med. 1994, 10, 77–84. [Google Scholar] [CrossRef]
- Barrera, M.; Sandler, I.N.; Ramsay, T.B. Preliminary development of a scale of social support: Studies on college students. Am. J. Community Psychol. 1981, 9, 435–447. [Google Scholar] [CrossRef]
- Beck, A.; Ward, C.; Mendelson, H.; Mock, M.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- De Leo, D.; Diekstra, R.F.W.; Lonnqvist, J.; Lonnqvist, J.; Cleiren, M.H.P.D.; Frisoni, G.B.; Buono, M.D.; Haltunen, A.; Zucchetto, M.; Rozzini, R.; et al. Leipad, an internationally applicable instrument to assess quality of life in the elderly. Behav. Med. 1998, 24, 17–27. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Gierveld, J.D.J.; Van Tilburg, T. A 6-item scale for overall, emotional, and social loneliness: Confirmatory tests on survey data. Res. Aging 2006, 28, 582–598. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.T. Geriatric fear of falling measure: Development and psychometric testing. Int. J. Nurs. Stud. 2006, 43, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Cacioppo, J.T. A short scale for measuring loneliness in large surveys: Results from two population-based studies. Res. Aging 2004, 26, 655–672. [Google Scholar] [CrossRef] [PubMed]
- Hunt, S.M.; McEwen, J.; McKenna, S.P. Measuring health status: A new tool for clinicians and epidemiologists. J. R. Coll. Gen. Pract. 1985, 35, 185–188. [Google Scholar] [PubMed]
- Jones, P.W.; Quirk, F.H.; Baveystock, C.M. The St. George’s respiratory questionnaire. Respir. Med. 1991, 85, 25–31. [Google Scholar] [CrossRef]
- Kempen, G.; Yardley, L.; van Haastregt, J.; Zijlstra, G.; Beyer, N.; Hauer, K.; Todd, C. The short FES-I: A shortened version of the falls efficacy scale-international to assess fear of falling. Age Ageing 2008, 37, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Yang, M.J.; Lai, T.J.; Chiu, N.M.; Chau, T.T. Development of the Taiwanese depression questionnaire. Chang Gung Med. J. 2000, 23, 688–694. [Google Scholar]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Lubben, J.E. Assessing social networks among elderly populations. Fam. Community Heal. J. Heal. Promot. Maint. 1988, 11, 42–52. [Google Scholar] [CrossRef]
- McNair, D.M.; Lorr, M. An analysis of mood in neurotics. J. Abnorm. Soc. Psychol. 1964, 69, 620–627. [Google Scholar] [CrossRef]
- Powell, L.; Myers, A. The activities-specific balance confidence (ABC) scale. J. Gerontol. 1995, 50A, 28–34. [Google Scholar] [CrossRef]
- Riggs, M.L.; Knight, P.A. The impact of perceived group success-failure on motivational beliefs and attitudes: A causal model. J. Appl. Psychol. 1994, 79, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M. Self esteem and the adolescent self-image. Science. 1965, 148, 804. [Google Scholar] [CrossRef]
- Sarason, I.G.; Sarason, B.R.; Shearin, E.N.; Pierce, G.R. A brief measure of social support: Practical and theoretical implications. J. Soc. Pers. Relat. 1987, 4, 497–510. [Google Scholar] [CrossRef]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial a report from the WHOQOL Group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Smets, E.M.A.; Garssen, B.; Bonke, B.; de Haes, J. The multidimensional fatigue inventory (MFI) psychometric qualities of an instrument to assess fatigue. J. Psychosom. Res. 1995, 39, 315–325. [Google Scholar] [CrossRef] [Green Version]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Dinburgh mental well-being scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [Green Version]
- Tinetti, M.E.; Richman, D.; Powell, L. Falls efficacy as a measure of fear of falling. J. Gerontol. 1990, 45, 239–243. [Google Scholar] [CrossRef]
- Veit, C.T.; Ware, J.E. The structure of psychological distress and well-being in general populations. J. Consult. Clin. Psychol. 1983, 51, 730–742. [Google Scholar] [CrossRef]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health urvey (SF-36). Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snalth, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Gordon, K.; Farley, G.K. The multidimensional scale of perceived social support. J. Pers. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Levels | Search Terms with Boolean Operators |
|---|---|
| Search #1 | ((psychological AND (well-being OR health)) OR well-being OR wellness OR quality of life OR mindful* OR self-efficacy OR self-esteem OR fear of falling OR balance confidence OR depression OR depressive symptoms OR sleep quality OR ((emotional OR mental) AND health)) |
| Search #2 | AND (mind body OR tai chi OR qigong OR yoga OR pilates OR feldenkrais) |
| Search #3 | AND (old* OR elder* OR senior* OR aged) |
| Subscales of Questionnaires | |||
|---|---|---|---|
| Questionnaires | Physical Functioning | Psychological Functioning | Social Functioning |
| SF-36/12 | Physical functioning Role—physical Body pain General health | Mental health Role—emotional Vitality | Social functioning |
| LEIPAD | Physical functioning Self-care | Mental functioning | Social functioning |
| MFI | Physical fatigue Reduced activity | Mental fatigue Reduced motivation | --- |
| NHP | Physical abilities | Tiredness Emotional reaction | Social isolation |
| WHOQOL-BREF | Physical health | Psychological health | Social relations |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weber, M.; Schnorr, T.; Morat, M.; Morat, T.; Donath, L. Effects of Mind–Body Interventions Involving Meditative Movements on Quality of Life, Depressive Symptoms, Fear of Falling and Sleep Quality in Older Adults: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6556. https://doi.org/10.3390/ijerph17186556
Weber M, Schnorr T, Morat M, Morat T, Donath L. Effects of Mind–Body Interventions Involving Meditative Movements on Quality of Life, Depressive Symptoms, Fear of Falling and Sleep Quality in Older Adults: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(18):6556. https://doi.org/10.3390/ijerph17186556
Chicago/Turabian StyleWeber, Manuel, Thiemo Schnorr, Mareike Morat, Tobias Morat, and Lars Donath. 2020. "Effects of Mind–Body Interventions Involving Meditative Movements on Quality of Life, Depressive Symptoms, Fear of Falling and Sleep Quality in Older Adults: A Systematic Review with Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 18: 6556. https://doi.org/10.3390/ijerph17186556