Impact of COVID-19Quarantine on Low Back Pain Intensity, Prevalence, and Associated Risk Factors among Adult Citizens Residing in Riyadh (Saudi Arabia): A Cross-Sectional Study


 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
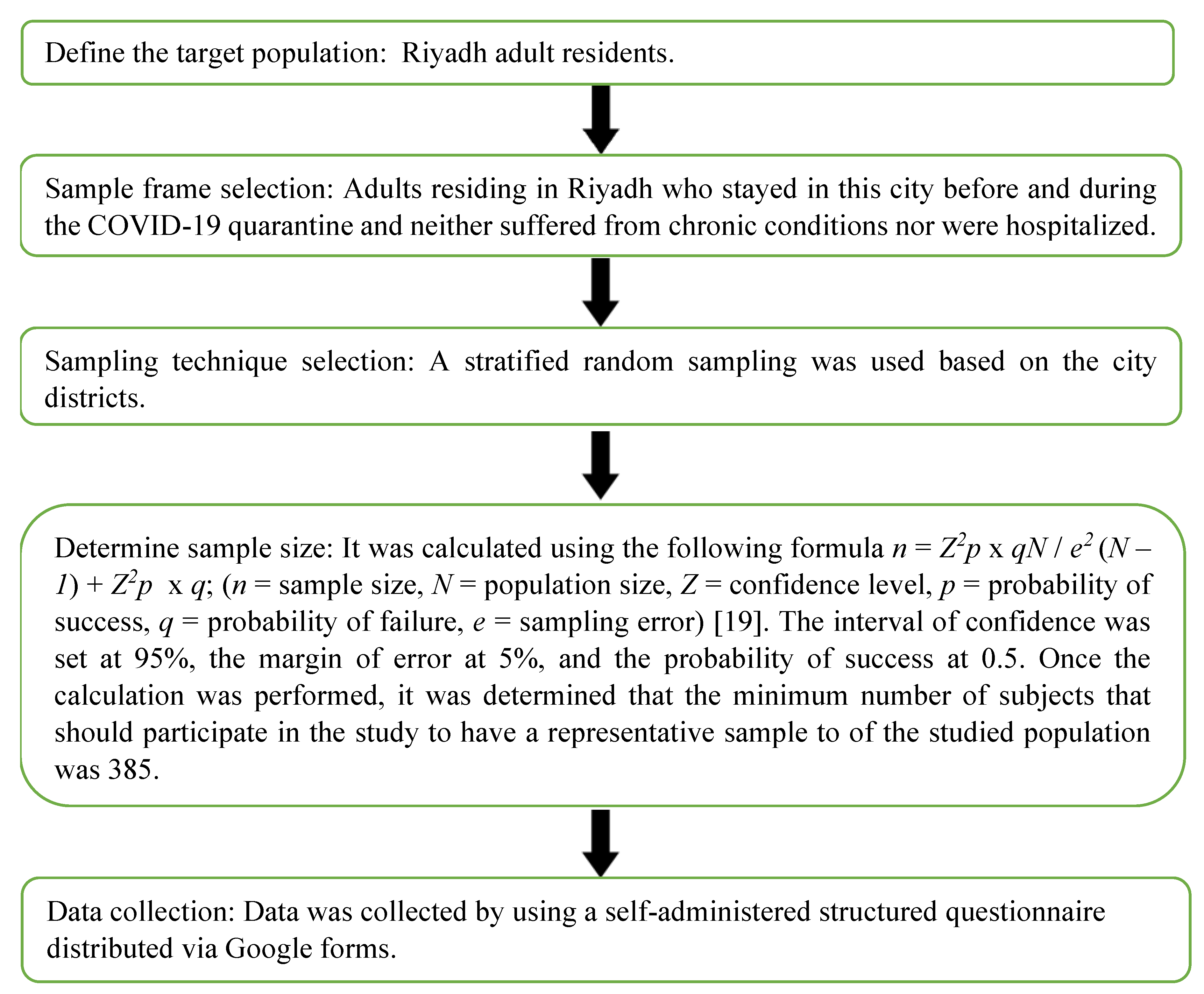
2.1. Subjects
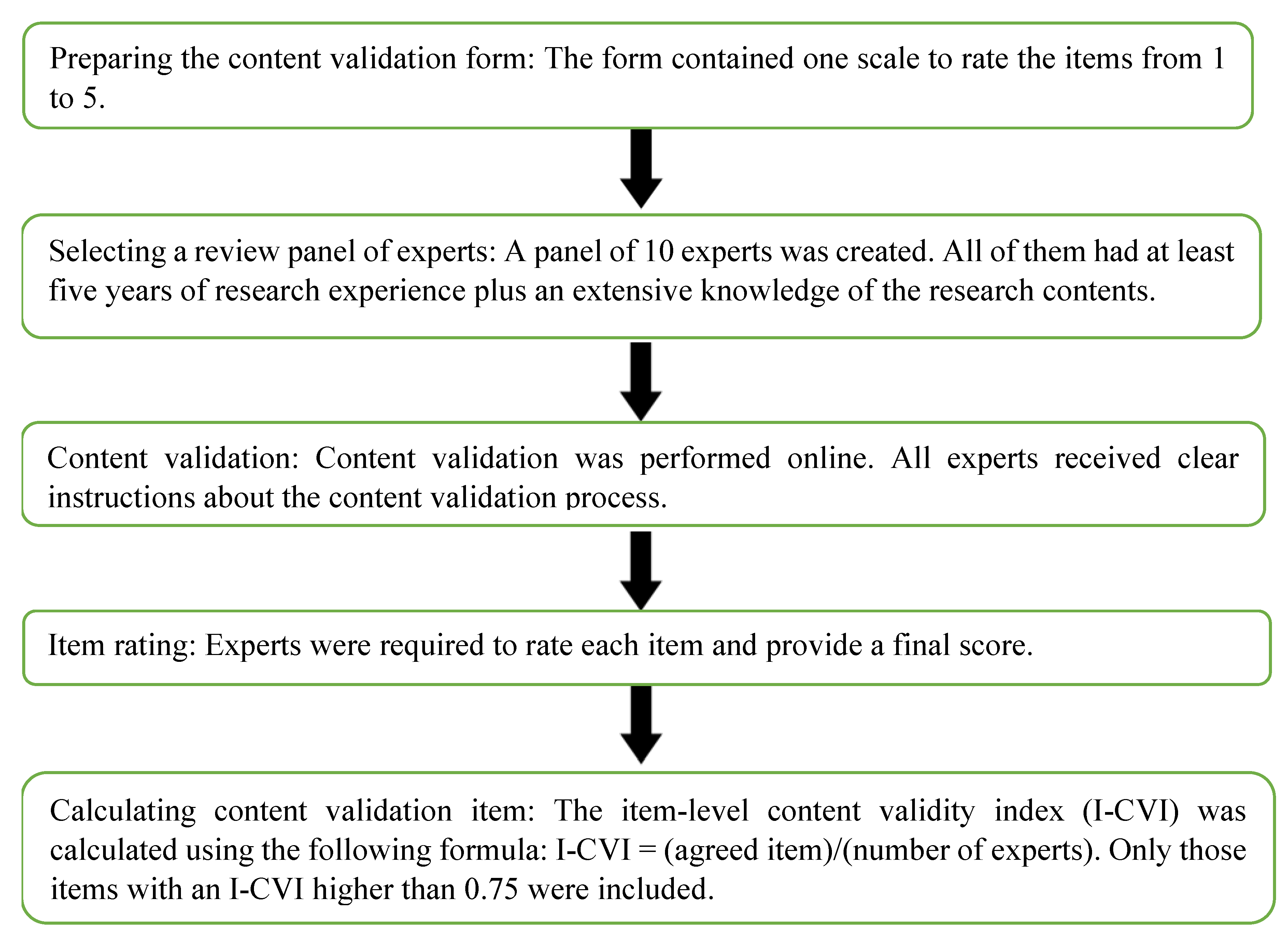
2.2. Questionnaire Application
2.3. Ethical Clearance
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 Diseases and Injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Fatoye, F.; Gebrye, T.; Odeyemi, I. Real-world incidence and prevalence of low back pain using routinely collected data. Rheumatol. Int. 2019, 39, 619–626. [Google Scholar] [CrossRef] [Green Version]
- Meisha, D.E.; Alsharqawi, N.S.; Samarah, A.A.; Al-Ghamdi, M.Y. Prevalence of work-related musculoskeletal disorders and ergonomic practice among dentists in Jeddah, Saudi Arabia. Clin. Cosmet. Investig. Dent. 2019, 11, 171–179. [Google Scholar] [CrossRef] [Green Version]
- Şimşek, Ş. Prevalence and Risk Factors of Low Back Pain among Health-care Workers in Denizli. Ağrı - J. Turkish Soc. Algol. 2017, 29, 71–78. [Google Scholar]
- Dutmer, A.L.; Schiphorst Preuper, H.R.; Soer, R.; Brouwer, S.; Bültmann, U.; Dijkstra, P.U.; Coppes, M.H.; Stegeman, P.; Buskens, E.; Van Asselt, A.D.I.; et al. Personal and Societal Impact of Low Back Pain: The Groningen Spine Cohort. Spine 2019, 44, E1443–E1451. [Google Scholar] [PubMed]
- Crow, W.T.; Willis, D.R. Estimating cost of care for patients with acute low back pain: A retrospective review of patient records. J. Am. Osteopath. Assoc. 2009, 109, 229–233. [Google Scholar]
- Coenen, P. On the Origin of Back Pain; VU University Amsterdam: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Brady, S.R.E.; Hussain, S.M.; Brown, W.J.; Heritier, S.; Billah, B.; Wang, Y.; Teede, H.; Urquhart, D.M.; Cicuttini, F.M. Relationships Between Weight, Physical Activity, and Back Pain in Young Adult Women. Medicine (Baltimore) 2016, 95, e3368. [Google Scholar]
- Bento, T.P.F.; dos Santos Genebra, C.V.; Maciel, N.M.; Cornelio, G.P.; Simeão, S.F.; de Vitta, A. Low back pain and some associated factors: Is there any difference between genders? Brazilian J. Phys. Ther. 2020, 24, 79–87. [Google Scholar]
- Jradi, H.; Alanazi, H.; Mohammad, Y. Psychosocial and occupational factors associated with low back pain among nurses in Saudi Arabia. J. Occup. Health 2020, 62, e12126. [Google Scholar] [CrossRef]
- Alnaami, I.; Awadalla, N.J.; Alkhairy, M.; Alburidy, S.; Alqarni, A.; Algarni, A.; Alshehri, R.; Amrah, B.; Alasmari, M.; Mahfouz, A.A. Prevalence and factors associated with low back pain among health care workers in southwestern Saudi Arabia. BMC Musculoskelet. Disord. 2019, 20, 56. [Google Scholar]
- Abdel-Salam, D.M.; Almuhaisen, A.S.; Alsubiti, R.A.; Aldhuwayhi, N.F.; Almotairi, F.S.; Alzayed, S.M.; Bakri, F.F. Musculoskeletal pain and its correlates among secondary school female teachers in Aljouf region, Saudi Arabia. J. Public Heal. 2019, 1–8. [Google Scholar] [CrossRef]
- Badawood, M.A.; Obaid, H.; Mohammed, M.E.; Alrogi, A.J. Impact of Low Back Pain on the work performance of male high school Saudi Teachers in Taif City. J. Health Inform. Dev. Ctries. 2017, 11, 1–18. [Google Scholar]
- Awaji, M.A. Epidemiology of Low Back Pain in Saudi Arabia. J. Adv. Med. Pharm. Sci. 2016, 6, 1–9. [Google Scholar]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar]
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel Med. 2020, 27, taaa020. [Google Scholar]
- Mattioli, A.V.; Ballerini Puviani, M.; Nasi, M.; Farinetti, A. COVID-19 pandemic: The effects of quarantine on cardiovascular risk. Eur. J. Clin. Nutr. 2020, 74, 852–855. [Google Scholar]
- Taherdoost, H. Sampling Methods in Research Methodology; How to Choose a Sampling Technique for Research. SSRN Electron. J. 2018, 5, 18–27. [Google Scholar]
- Naing, L.; Winn, T.; Rusli, B.N. Practical Issues in Calculating the Sample Size for Prevalence Studies. Arch. Orofac. Sci. 2006, 1, 9–14. [Google Scholar]
- Tsang, S.; Royse, C.; Terkawi, A. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaesth. 2017, 11, 80. [Google Scholar]
- González-Alonso, J.; Santacruz, P. Cálculo e interpretación del Alfa de Cronbach para el caso de validación de la consistencia interna de un cuestionario, con dos posibles escalas tipo Likert. Rev. Publicando 2015, 2, 62–77. [Google Scholar]
- Ministry of Interior: Change to the Times Allowed during the Curfew in All Regions, Except MAKKAH 3 Riyadh The Official Saudi Press Agency. Available online: https://www.spa.gov.sa/viewfullstory.php?lang=en&newsid=2091631 (accessed on 2 August 2020).
- Custodian of the Two Holy Mosques Issues Curfew Order to Limit Spread of Novel Coronavirus from Seven in the Evening Until Six in the Morning for 21 Days Starting in the Evening of Monday 23 March The Official Saudi Press Agency. Available online: https://www.spa.gov.sa/viewfullstory.php?lang=en&newsid=2050402 (accessed on 2 August 2020).
- Kornacki, A.; Bochniak, A.; Kubik-Komar, A. Sample size determination in the Mann–Whitney test. Biom. Lett. 2017, 54, 175–186. [Google Scholar]
- Alanzi, M.S.Z.; Almuhawwis, A.G.A.; Abo El-Fetoh, N.M. Low Back Pain in Population of Arar City, Northern Saudi Arabia: An Epidemiological Study. Egypt. J. Hosp. Med. 2017, 69, 2839–2845. [Google Scholar]
- Population of Cities in Saudi Arabia. 2020. Available online: https://worldpopulationreview.com/countries/cities/saudi-arabia (accessed on 2 August 2020).
- Freburger, J.K.; Holmes, G.M.; Agans, R.P.; Jackman, A.M.; Darter, J.D.; Wallace, A.S.; Castel, L.D.; Kalsbeek, W.D.; Carey, T.S. The rising prevalence of chronic low back pain. Arch. Intern. Med. 2009, 169, 251–258. [Google Scholar] [PubMed] [Green Version]
- Al-Arfaj, A.S.; Al-Saleh, S.S.; Alballa, S.R.; Al-Dalaan, A.N.; Bahabri, S.A.; Al-Sekeit, M.A.; Mousa, M.A. How common is back pain in Al-Qaseem region. Saudi Med. J. 2003, 24, 170–173. [Google Scholar]
- Sirajudeen, M.S.; Alaidarous, M.; Waly, M.; Alqahtani, M. Work-related musculoskeletal disorders among faculty members of college of Applied Medical Sciences, Majmaah University, Saudi Arabia: A cross-sectional study. Int. J. Health Sci. (Qassim) 2018, 12, 18–25. [Google Scholar]
- Algarni, A.D.; Al-Saran, Y.; Al-Moawi, A.; Bin Dous, A.; Al-Ahaideb, A.; Kachanathu, S.J. The Prevalence of and Factors Associated with Neck, Shoulder, and Low-Back Pains among Medical Students at University Hospitals in Central Saudi Arabia. Pain Res. Treat. 2017, 2017, 1235706. [Google Scholar]
- Ahmad, I.; Balkhyour, M.A.; Abokhashabah, T.M.; Ismail, I.M.; Rehan, M. Occupational Musculoskeletal Disorders among Taxi Industry Workers in Jeddah, Saudi Arabia. Biosci. Biotechnol. Res. Asia 2017, 14, 593–606. [Google Scholar]
- AlShayhan, F.A.; Saadeddin, M. Prevalence of low back pain among health sciences students. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 165–170. [Google Scholar]
- Wami, S.D.; Abere, G.; Dessie, A.; Getachew, D. Work-related risk factors and the prevalence of low back pain among low wage workers: Results from a cross-sectional study. BMC Public Health 2019, 19, 1072. [Google Scholar]
- Al Shammari, M.; Hassan, A.; Al Dandan, O.; Al Gadeeb, M.; Bubshait, D. Musculoskeletal symptoms among radiologists in Saudi Arabia: A multi-center cross-sectional study. BMC Musculoskelet. Disord. 2019, 20, 541. [Google Scholar]
- Ferguson, S.A.; Merryweather, A.; Thiese, M.S.; Hegmann, K.T.; Lu, M.L.; Kapellusch, J.M.; Marras, W.S. Prevalence of low back pain, seeking medical care, and lost time due to low back pain among manual material handling workers in the United States. BMC Musculoskelet. Disord. 2019, 20, 243. [Google Scholar]
- Alzahrani, H.; Mackey, M.; Stamatakis, E.; Zadro, J.R.; Shirley, D. The association between physical activity and low back pain: A systematic review and meta-analysis of observational studies. Sci. Rep. 2019, 9, 1–10. [Google Scholar]
- Taulaniemi, A.; Kankaanpää, M.; Tokola, K.; Parkkari, J.; Suni, J.H. Neuromuscular exercise reduces low back pain intensity and improves physical functioning in nursing duties among female healthcare workers; Secondary analysis of a randomised controlled trial. BMC Musculoskelet. Disord. 2019, 20, 328. [Google Scholar]
- Mörl, F.; Bradl, I. Lumbar posture and muscular activity while sitting during office work. J. Electromyogr. Kinesiol. 2013, 23, 362–368. [Google Scholar]
- Alias, A.N.; Karuppiah, K.; How, V.; Perumal, V. Prevalence of musculoskeletal disorders (MSDS) among primary school female teachers in Terengganu, Malaysia. Int. J. Ind. Ergon. 2020, 77, 102957. [Google Scholar]
- Sheng, B.; Feng, C.; Zhang, D.; Spitler, H.; Shi, L. Associations between Obesity and Spinal Diseases: A Medical Expenditure Panel Study Analysis. Int. J. Environ. Res. Public Health 2017, 14, 183. [Google Scholar]
- Zaletel-Kragelj, L.; Pahor, M.; Bilban, M. Identification of population groups at very high risk for frequent perception of stress in slovenia. Croat. Med. J. 2005, 46, 137–145. [Google Scholar] [PubMed]
- Gokcek, E.; Kaydu, A. Assessment of relationship between Vitamin D deficiency and pain severity in patients with low back pain: A retrospective, observational study. Anesth. Essays Res. 2018, 12, 680. [Google Scholar] [PubMed]
- van den Berg, R.; Jongbloed, E.M.; de Schepper, E.I.T.; Bierma-Zeinstra, S.M.A.; Koes, B.W.; Luijsterburg, P.A.J. The association between pro-inflammatory biomarkers and nonspecific low back pain: A systematic review. Spine J. 2018, 18, 2140–2151. [Google Scholar] [PubMed]
- Trajković, N.; Sporiš, G.; Krističević, T.; Bogataj, Š. Effects of Small-Sided Recreational Volleyball on Health Markers and Physical Fitness in Middle-Aged Men. Int. J. Environ. Res. Public Health 2020, 17, 3021. [Google Scholar]
- Bogataj, Š.; Pajek, J.; Buturović Ponikvar, J.; Hadžić, V.; Pajek, M. Kinesiologist-guided functional exercise in addition to intradialytic cycling program in end-stage kidney disease patients: A randomised controlled trial. Sci. Rep. 2020, 10, 5717. [Google Scholar]
- Daoust, R.; Sirois, M.J.; Lee, J.S.; Perry, J.J.; Griffith, L.E.; Worster, A.; Lang, E.; Paquet, J.; Chauny, J.M.; Émond, M.; et al. Painful memories: Reliability of pain intensity recall at 3 months in senior patients. Pain Res. Manag. 2017, 2017, 5983721. [Google Scholar]
- Bolton, J.E. Accuracy of recall of usual pain intensity in back pain patients. Pain 1999, 83, 533–539. [Google Scholar]



{kind=link}
{kind=link}
| Subjects | Body Area | Before the Quarantine * (%) | During the Quarantine # (%) | Percentage Change (%) | Significance Level (p) |
|---|---|---|---|---|---|
| Percentage of subjects who reported having pain in different body areas | Nowhere | 35.2(F: 34.09, M: 36.31) | 33(F: 33.33, M: 32.83) | −6.25 | 0.92 |
| Neck | 25.8(F: 29.11, M: 21.89) | 30.3(F: 32.56, M: 27.86) | 17.44 | 0.17 | |
| Shoulder(s) | 18.5(F: 19.15, M: 17.91) | 23.2(F: 23.37, M: 30.35) | 25.41 | 0.21 | |
| Thoracic area | 9(F: 9.96, M: 7.96) | 15.7(F: 15.32, M: 15.42) | 74.44 | 0.02 | |
| Low back | 38.8(F: 35.25, M: 43.28) | 43.8(F: 42.52, M: 44.7) | 11.41 | 0.001 | |
| Leg(s) | 9.9(F: 10.34, M: 9.45) | 13.9(F: 14.56, M: 13.43) | 40.40 | 0.07 | |
| Percentage of subjects who did telework or distance learning | 3.9(F: 47.14, M: 52.86) | 48.3(F: 46.36, M: 51.25) | 1138 | <0.001 | |
| Percentage of subjects who were sitting always or most of the time | 30.51(F: 32.43, M: 27.63) | 50.9(F: 52.71, M: 50.02) | 71.38 | <0.001 | |
| Percentage of subjects who were sitting and moving equally | 27.9(F: 23.94, M: 31.5) | 24.2(F: 19.37, M: 28.57) | −13.26 | 0.24 | |
| Percentage who were moving always or most of the time | 42.4(F:43.63, M: 40.5) | 24.9(F: 27.92, M: 20.41) | −41.27 | <0.001 | |
| Percentage of subjects who did not practice PA | 7.3(F: 4.98, M: 9.41) | 20(F: 22.23, M: 18.81) | 173.97 | 0.001 | |
| Percentage of subjects who practiced PA once a week | 10.3(F: 11.49, M: 8.49) | 15.2(F: 14.50, M: 16.42) | 47.57 | 0.02 | |
| Percentage of subjects who practiced PA two or three times a week | 35.6(F: 39.84, M: 30.19) | 25.1(F: 26.33, M: 23.38) | −29.49 | 0.001 | |
| Percentage of subjects who practiced PA four or five times a week | 24.1(F: 24.52, M: 23.21) | 25.8(F: 25.57, M: 25.94) | 7.05 | 0.97 | |
| Percentage of subjects who practiced PA six or seven times a week | 22.7(F: 19.17, M: 28.71) | 13.9(F: 11.37, M: 15.65) | −38.76 | <0.001 | |
| Percentage of subjects who reported a higher level of perceived stress | 22.41(F: 52.99, M: 47.01) | 50.43(F: 56.86, M: 43.13) | N/A | <0.001 | |
| Factor | Cohort | Pain Intensity before the Quarantine * | Pain Intensity during the Quarantine ▲ |
|---|---|---|---|
| Time | Whole sample (n = 463) | 1.95(2) | 2.44(2) § |
| Gender | Male (n = 259) | 1.96(2) | 2.39(2) |
| Female (n = 204) | 1.95(2) | 2.46(2) | |
| Age group (years) | 18–34 (n = 252) | 1.90(2) + | 2.35(2) + |
| 35–49 (n = 166) | 2.04(2) | 2.58(2) | |
| 50–64 (n = 45) | 1.93(2) + | 2.44(2) + | |
| Body mass index (BMI) category | Normal weight (n = 224) | 1.93(2) | 2.40(2) |
| Overweight (n = 160) | 1.97(2) † | 2.44(2) † | |
| Obese (n = 71) | 2.06(2) †, †† | 2.64(2) †, †† | |
| Perceived stress | Mild or no stress (n = 104) | 1.94(2) | 2.14(2) |
| Moderate or severe (n = 234) | 1.96(2) | 2.73(2) ¥ | |
| Ergonomic recommendations compliance | Subjects who complied with the ergonomic recommendations (n = 63) | 1.90(2) | 2.27(2) |
| Subjects who did not comply with the ergonomic recommendations (n = 223) | 2.02(2) ■ | 2.63(2) ■ | |
| Carrying out teleworking or distance learning | No (n = 239) | 1.94(2) | 2.26(2) |
| Yes (n = 224) | 1.97(2) | 2.64(2) ⅏ | |
| Time spent moving or sitting | Subjects who were sitting always or most of the time (n = 238) | 2.11(2) | 2.75(2) |
| Subjects who were moving always or most of the time (n = 212) | 1.92(2) # | 2.23(2) # | |
| Weekly practice of PA (times) | None (n = 91) | 2.23(2) | 2.98(2) |
| 1 (n = 71) | 2.01(2) | 2.75(2) & | |
| 2–3 (n = 117) | 1.93(2) | 2.25(2) &, && | |
| 4–5 (n = 119) | 1.87(2) &, &&, &&& | 2.20(2) &, && | |
| 6–7 (n = 66) | 1.81(2) &, &&, &&& | 2.12(2) &, &&, &&&, &&&& |
| Factor | Back Pain Intensity before the Quarantine | Back Pain Intensity during the Quarantine | ||
|---|---|---|---|---|
| Time spent sitting | r = 0.054 | p = 0.216 | r = 0.124 | p = 0.008 |
| Weekly frequency of PA | r = −0.023 | p = 0.621 | r = −0.198 | p < 0.001 |
| Perceived stress | r = 0.129 | p = 0.014 | r = 0.186 | p < 0.001 |
| Compliance with ergonomic recommendations | r = 0.030 | p = 0.521 | r = −0.059 | p = 0.207 |
| Age | r = 0.068 | p = 0.147 | r = −0.008 | p = 0.869 |
| BMI | r = 0.106 | p = 0.029 | r = 0.190 | p = 0.009 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šagát, P.; Bartík, P.; Prieto González, P.; Tohănean, D.I.; Knjaz, D. Impact of COVID-19Quarantine on Low Back Pain Intensity, Prevalence, and Associated Risk Factors among Adult Citizens Residing in Riyadh (Saudi Arabia): A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 7302. https://doi.org/10.3390/ijerph17197302
Šagát P, Bartík P, Prieto González P, Tohănean DI, Knjaz D. Impact of COVID-19Quarantine on Low Back Pain Intensity, Prevalence, and Associated Risk Factors among Adult Citizens Residing in Riyadh (Saudi Arabia): A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(19):7302. https://doi.org/10.3390/ijerph17197302
Chicago/Turabian StyleŠagát, Peter, Peter Bartík, Pablo Prieto González, Dragoș Ioan Tohănean, and Damir Knjaz. 2020. "Impact of COVID-19Quarantine on Low Back Pain Intensity, Prevalence, and Associated Risk Factors among Adult Citizens Residing in Riyadh (Saudi Arabia): A Cross-Sectional Study" International Journal of Environmental Research and Public Health 17, no. 19: 7302. https://doi.org/10.3390/ijerph17197302