
Understanding Period Poverty: Socio-Economic Inequalities in Menstrual Hygiene Management in Eight Low- and Middle-Income Countries


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Menstrual Hygiene Management Data and Measures
2.3. Wealth Measure
2.4. Concentration Index
2.5. Decomposition Analysis
- Beta: Firstly, we report on the Beta from Equation (3). The beta indicates the direction of the relationship between variable and the MHM measure. It therefore does not illustrate inequality, but the point change in the probability of the MHM measure associated with a unit change of each variable .
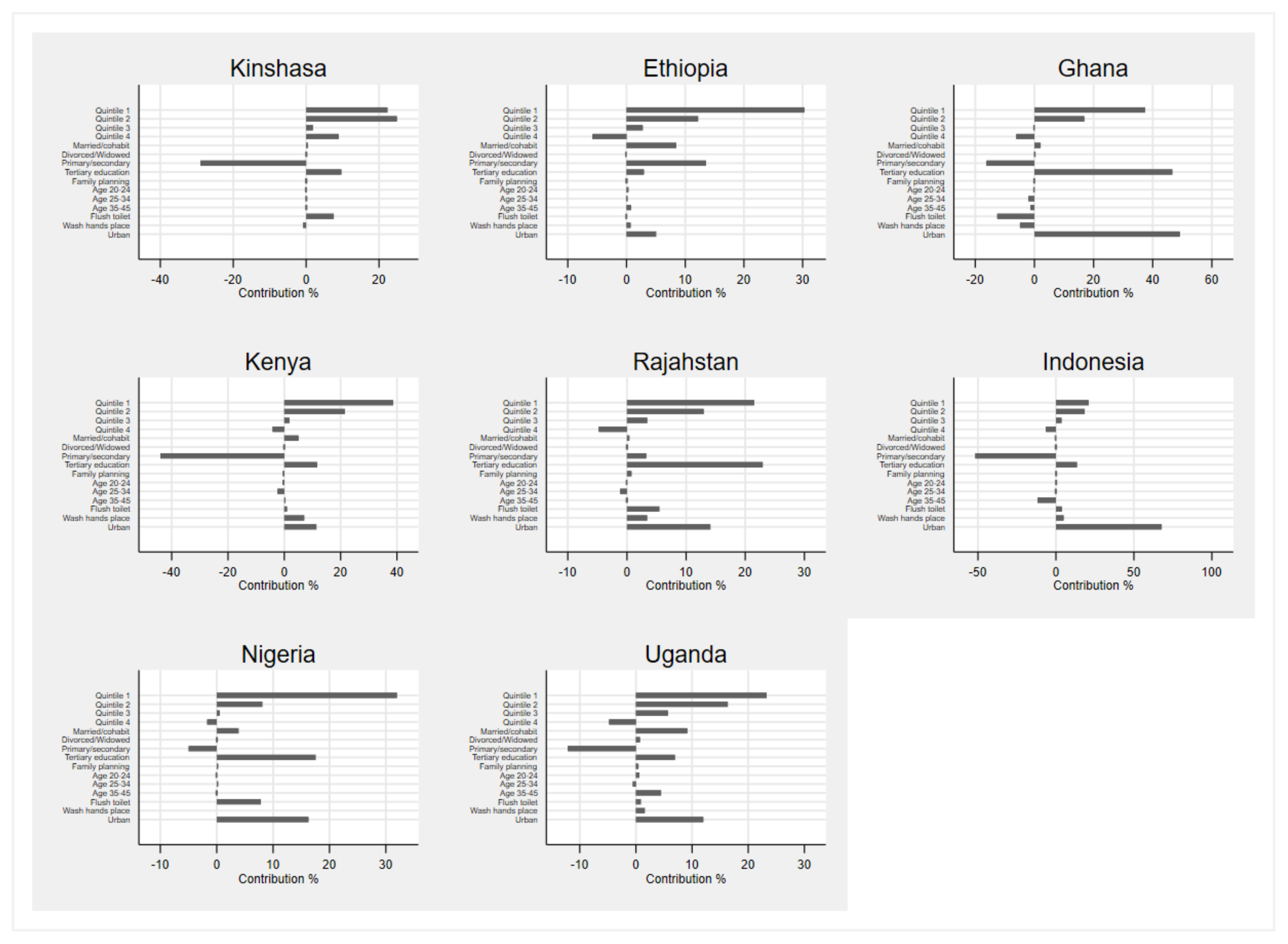
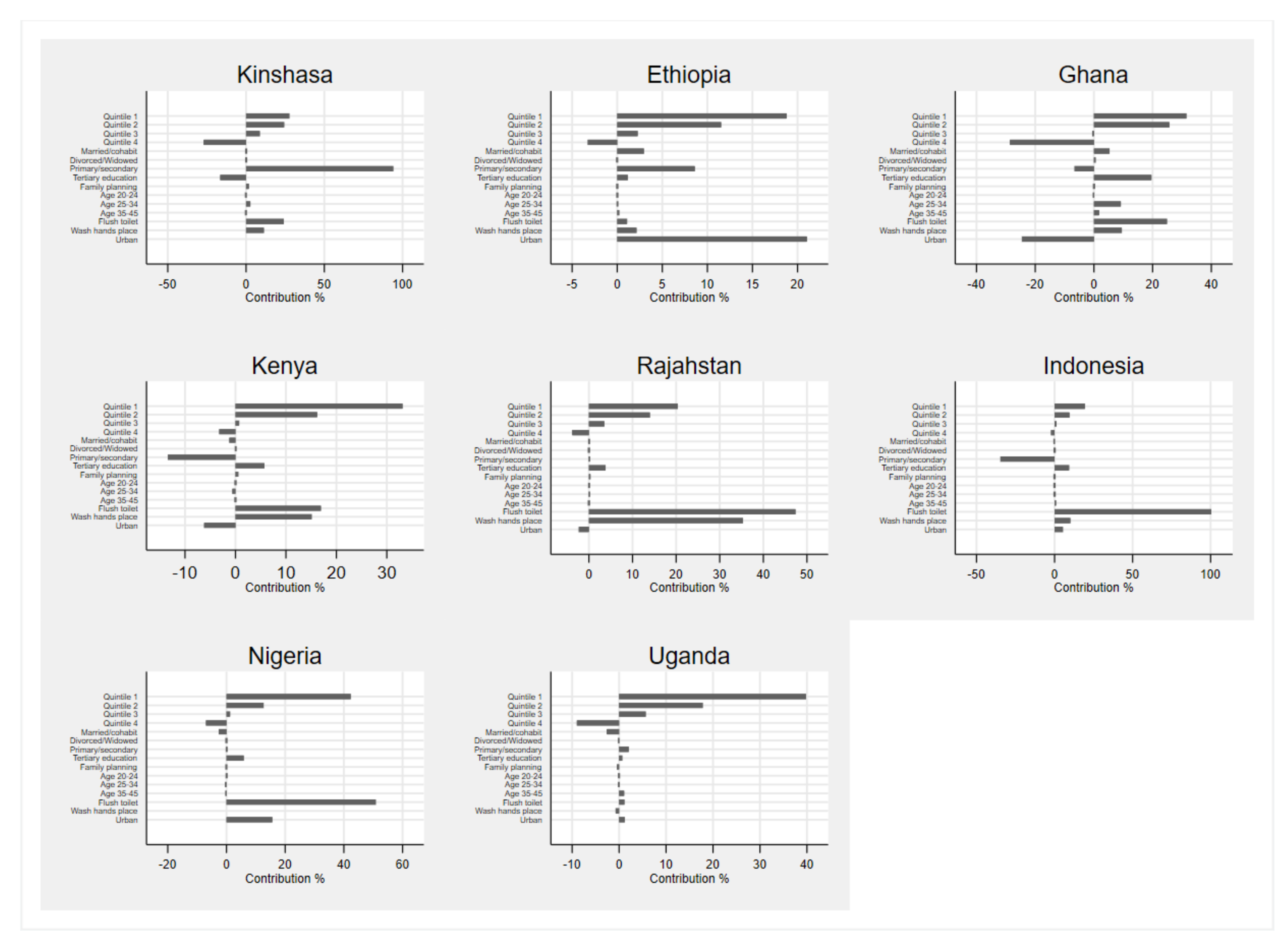
- The Contribution rows show the absolute contribution of each explanatory variable to the overall wealth-related inequality in MHM measure m. This contribution is calculated as the product of the explanatory variable’s elasticity and own concentration index to the wealth index. The Contribution is greater if the explanatory variable’s own concentration index is larger, it has a higher mean or a greater Beta.
- The Contribution % row translates the absolute contribution into a percentage contribution.
2.6. Independent Variables
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sommer, M.; Sahin, M. Overcoming the Taboo: Advancing the Global Agenda for Menstrual Hygiene Management for Schoolgirls. Am. J. Public Health 2013, 103, 1556–1559. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D.; Muli, A.; Schwab, K.J.; Hennegan, J. National Monitoring for Menstrual Health and Hygiene: Is the Type of Menstrual Material Used Indicative of Needs Across 10 Countries? Int. J. Environ. Res. Public Health 2020, 17, 2633. [Google Scholar] [CrossRef]
- Mishra, V.K. Social and psychological impact of limited access to sanitation: MHM and reproductive tract infections. In Water, Sanitation and Hygiene Services Beyond; Shaw, R.J., Ed.; Loughborough University: Loughborough, UK, 2015. [Google Scholar]
- Baker, K.K.; Padhi, B.; Torondel, B.; Das, P.; Dutta, A.; Sahoo, K.C.; Das, B.; Dreibelbis, R.; Caruso, B.; Freeman, M.C.; et al. From menarche to menopause: A population-based assessment of water, sanitation, and hygiene risk factors for reproductive tract infection symptoms over life stages in rural girls and women in India. PLoS ONE 2017, 12, e0188234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips-Howard, P.A.; Otieno, G.; Burmen, B.; Otieno, F.; Odongo, F.; Odour, C.; Nyothach, E.; Amek, N.; Zielinski-Gutierrez, E.; Odhiambo, F.; et al. Menstrual Needs and Associations with Sexual and Reproductive Risks in Rural Kenyan Females: A Cross-Sectional Behavioral Survey Linked with HIV Prevalence. J. Women’s Health 2015, 24, 801–811. [Google Scholar] [CrossRef] [PubMed]
- Oruko, K.; Nyothach, E.; Zielinski-Gutierrez, E.; Mason, L.; Alexander, K.; Vulule, J.; Laserson, K.F.; Phillips-Howard, P.A. ’He is the one who is providing you with everything so whatever he says is what you do’: A Qualitative Study on Factors Affecting Secondary Schoolgirls’ Dropout in Rural Western Kenya. PLoS ONE 2015, 10, e0144321. [Google Scholar] [CrossRef] [PubMed]
- Sumpter, C.; Torondel, B. A Systematic Review of the Health and Social Effects of Menstrual Hygiene Management. PLoS ONE 2013, 8, e62004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miiro, G.; Rutakumwa, R.; Nakiyingi-Miiro, J.; Nakuya, K.; Musoke, S.; Namakula, J.; Francis, S.; Torondel, B.; Gibson, L.J.; Ross, D.A.; et al. Menstrual health and school absenteeism among adolescent girls in Uganda (MENISCUS): A feasibility study. BMC Women’s Health 2018, 18, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrmann, M.A.; Rockoff, J.E. Do menstrual problems explain gender gaps in absenteeism and earnings? Evidence from the national health interview survey. Labour Econ. 2013, 24, 12–22. [Google Scholar] [CrossRef]
- Ichino, A.; Moretti, E. Biological Gender Differences, Absenteeism, and the Earnings Gap. Am. Econ. J. Appl. Econ. 2009, 1, 183–218. [Google Scholar] [CrossRef]
- Oster, E.; Thornton, R. Menstruation, Sanitary Products, and School Attendance: Evidence from a Randomized Evaluation. Am. Econ. J. Appl. Econ. 2011, 3, 91–100. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, P.; Hennegan, J.; Dolan, C.; Wu, M.; Steinfield, L.; Scott, L. Menstruation and the Cycle of Poverty: A Cluster Quasi-Randomised Control Trial of Sanitary Pad and Puberty Education Provision in Uganda. PLoS ONE 2016, 11, e0166122. [Google Scholar] [CrossRef]
- Phillips-Howard, P.A.; Caruso, B.; Torondel, B.; Zulaika, G.; Sahin, M.; Sommer, M. Menstrual hygiene management among adolescent schoolgirls in low- and middle-income countries: Research priorities. Glob. Health Action 2016, 9, 33032. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, T. Imperfect Information in Menstrual Health and the Role of Informed Choice. Indian J. Gend. Stud. 2019, 26, 59–78. [Google Scholar] [CrossRef]
- Van Eijk, A.M.; Sivakami, M.; Thakkar, M.B.; Bauman, A.; Laserson, K.F.; Coates, S.; Phillips-Howard, P.A. Menstrual hygiene management among adolescent girls in India: A systematic review and meta-analysis. BMJ Open 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Sommer, M.; Kjellén, M.; Pensulo, C. Girls’ and women’s unmet needs for menstrual hygiene management (MHM): The interactions between MHM and sanitation systems in low-income countries. J. Water Sanit. Hyg. Dev. 2013, 3, 283–297. [Google Scholar] [CrossRef]
- Mason, L.; Nyothach, E.; Van Eijk, A.M.; Obor, D.; Alexander, K.T.; Ngere, I.; Laserson, K.; Phillips-Howard, P. Comparing use and acceptability of menstrual cups and sanitary pads by schoolgirls in rural Western Kenya. Int. J. Reprod. Contraception Obstet. Gynecol. 2019, 8, 2974. [Google Scholar] [CrossRef] [Green Version]
- PMA 2020. Survey Methodology 2020. Available online: https://www.pmadata.org/data/survey-methodology (accessed on 6 March 2020).
- Tulane University School of Public Health, University of Kinshasa School of Public Health, The Bill & Melinda Gates Institute for Population and Reproductive Health at The Johns Hopkins Bloomberg School of Public Health. Performance Monitoring and Accountability 2020 (PMA2020) Survey Round 5, PMA2017/DRC-R6 (Kinshasa & Kongo Central); The Johns Hopkins Bloomberg School of Public Health: Baltimore, MD, USA, 2017. [Google Scholar]
- Addis Ababa University School of Public Health, The Bill & Melinda Gates Institute for Population and Reproductive Health at The Johns Hopkins Bloomberg School of Public Health. Performance Monitoring and Accountability 2020 (PMA2020) Survey Round 5, PMA2017/Ethiopia-R5; The Johns Hopkins Bloomberg School of Public Health: Baltimore, MD, USA, 2017. [Google Scholar]
- Kwame Nkrumah University of Science & Technology School of Medicine, The Bill & Melinda Gates Institute for Population and Reproductive Health at The Johns Hopkins Bloomberg School of Public Health. Performance Monitoring and Accountability 2020 (PMA2020) Survey Round 5, PMA2016/Ghana-R5. 2016; The Johns Hopkins Bloomberg School of Public Health: Baltimore, MD, USA, 2016. [Google Scholar]
- International Centre for Reproductive Health Kenya (ICRHK), and The Bill & Melinda Gates Institute for Population and Reproductive Health at The Johns Hopkins Bloomberg School of Public Health. Performance Monitoring and Accountability 2020 (PMA2020) Survey Round 5, PMA2016/Kenya-R5; The Johns Hopkins Bloomberg School of Public Health: Baltimore, MD, USA, 2016. [Google Scholar]
- Indian Institute of Health Management Research (IIHMR) University in Jaipur, The Bill & Melinda Gates Institute for Population and Reproductive Health at The Johns Hopkins Bloomberg School of Public Health. Performance Monitoring and Accountability 2020 (PMA2020) Survey Round 2, PMA2017/India-R2 (Rajasthan); The Johns Hopkins Bloomberg School of Public Health: Baltimore, MD, USA, 2017. [Google Scholar]
- National Population and Family Planning Board of Indonesia (BkkbN), Universitas Gadjah Mada (UGM) UHU, Universitas Sumatera Utara (USU), Health. TBMGIfPaRHaTJHBSoP. Performance Monitoring and Accountability 2020 (PMA2020) Survey Round 2, PMA2016/Indonesia-R2; The Johns Hopkins Bloomberg School of Public Health: Baltimore, MD, USA, 2016. [Google Scholar]
- Centre for Research ERaDC, Bayero University Kano (BUK), The Bill & Melinda Gates Institute for Population and Reproductive Health at The Johns Hopkins Bloomberg School of Public Health. Performance Monitoring and Accountability 2020 (PMA2020) Survey Round 5, PMA2018/Nigeria-R5 (National); The Johns Hopkins Bloomberg School of Public Health: Baltimore, MD, USA, 2018. [Google Scholar]
- Makerere University SoPHatCoHS, Health. TBMGIfPaRHaTJHBSoP. Performance Monitoring and Accountability 2020 (PMA2020) Survey Round 5, PMA2017/Uganda-R5; The Johns Hopkins Bloomberg School of Public Health: Baltimore, MD, USA, 2017. [Google Scholar]
- Hennegan, J.; Shannon, A.K.; Schwab, K.J.; PMA2020 investigators. Wealthy, urban, educated. Who is represented in population surveys of women’s menstrual hygiene management? Reprod. Health Matters 2018, 26, 81–91. [Google Scholar] [CrossRef] [Green Version]
- Kakwani, N.C. Measurement of Tax Progressivity: An International Comparison. Econ. J. 1977, 87, 71. [Google Scholar] [CrossRef]
- Wagstaff, A.; Paci, P.; van Doorslaer, E. On the measurement of inequalities in health. Soc. Sci. Med. 1991, 33, 545–557. [Google Scholar] [CrossRef] [Green Version]
- Wagstaff, A.; van Doorslaer, E.; Watanabe, N. On decomposing the causes of health sector inequalities with an application to malnutrition inequalities in Vietnam. J. Econ. 2003, 112, 207–223. [Google Scholar] [CrossRef] [Green Version]
- Kakwani, N.; Wagstaff, A.; van Doorslaer, E. Socioeconomic inequalities in health: Measurement, computation, and statistical inference. J. Econ. 1997, 77, 87–103. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, O.; O’Neill, S.; Van Ourti, T.; Walsh, B. Conindex: Estimation of Concentration Indices. Stata J. Promot. Commun. Stat. Stata 2016, 16, 112–138. [Google Scholar] [CrossRef] [Green Version]
- Wagstaff, A. The bounds of the concentration index when the variable of interest is binary, with an application to immunization inequality. Health Econ. 2005, 14, 429–432. [Google Scholar] [CrossRef] [PubMed]
- Erreygers, G. Correcting the concentration index. J. Health Econ. 2009, 28, 504–515. [Google Scholar] [CrossRef] [Green Version]
- Wagstaff, A. Correcting the concentration index: A comment. J. Health Econ. 2009, 28, 516–520. [Google Scholar] [CrossRef]
- Gordon, T.; Booysen, F.; Mbonigaba, J. Socio-economic inequalities in the multiple dimensions of access to healthcare: The case of South Africa. BMC Public Health 2020, 20, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Mutyambizi, C.; Booysen, F.; Stokes, A.; Pavlova, M.; Groot, W. Lifestyle and socio-economic inequalities in diabetes prevalence in South Africa: A decomposition analysis. PLoS ONE 2019, 14, e0211208. [Google Scholar] [CrossRef]
- Heckley, G.; Gerdtham, U.-G.; Kjellsson, G. A general method for decomposing the causes of socioeconomic inequality in health. J. Health Econ. 2016, 48, 89–106. [Google Scholar] [CrossRef] [Green Version]
- Kessels, R.; Erreygers, G. Structural equation modeling for decomposing rank-dependent indicators of socioeconomic inequality of health: An empirical study. Health Econ. Rev. 2016, 6, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Kessels, R.; Erreygers, G. A direct regression approach to decomposing socioeconomic inequality of health. Health Econ. 2019, 28, 884–905. [Google Scholar] [CrossRef]
- Efron, B.; Tibshirani, R. Bootstrap methods for standard errors, confidence intervals, and other measures of statistical accuracy. Stat. Sci. 1986, 1, 54–75. [Google Scholar] [CrossRef]
- Efron, B. Better Bootstrap Confidence Intervals. J. Am. Stat. Assoc. 1987, 82, 171. [Google Scholar] [CrossRef]
- Ataguba, J.E.; Ojo, K.O.; Ichoku, H.E. Explaining socio-economic inequalities in immunization coverage in Nigeria. Health Policy Plan. 2016, 31, 1212–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yiengprugsawan, V.; Lim, L.L.; Carmichael, G.A.; Dear, K.B.; Sleigh, A.C. Decomposing socioeconomic inequality for binary health outcomes: An improved estimation that does not vary by choice of reference group. BMC Res. Notes 2010, 3, 57. [Google Scholar] [CrossRef] [Green Version]
- O’donnell, O.; Van Doorslaer, E.; Wagstaff, A.; Lindelow, M. Analyzing Health Equity Using Household Survey Data: A Guide to Techniques and Their Implementation; The World Bank: Washington, DC, USA, 2007. [Google Scholar]
- Chisha, Z.; Nwosu, C.O.; Ataguba, J.E.-O. Decomposition of socioeconomic inequalities in cigarette smoking: The case of Namibia. Int. J. Equity Health 2019, 18, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nwosu, C.O.; Oyenubi, A. Income-related health inequalities associated with the coronavirus pandemic in South Africa: A decomposition analysis. Int. J. Equity Health 2021, 20, 1–12. [Google Scholar] [CrossRef]
- Beyene, A.; Hailu, T.; Faris, K.; Kloos, H. Current state and trends of access to sanitation in Ethiopia and the need to revise indicators to monitor progress in the Post-2015 era. BMC Public Health 2015, 15, 1–8. [Google Scholar] [CrossRef]
- The World Bank. People Using At Least Basic Sanitation Services (% of Population) 2020. Available online: https://data.worldbank.org/indicator/SH.STA.BASS.ZS?locations=UG-ET (accessed on 15 December 2020).
- Budlender, D.; Casale, D.; Valodia, I. Gender equality and taxation in South Africa. In Taxation and Gender Equity; Routledge: London, UK, 2010; pp. 234–260. [Google Scholar]
- Cotropia, C.A.; Rozema, K. Who Would Benefit from Repealing Tampon Taxes? Empirical Evidence from New Jersey. SSRN Electron. J. 2017, 15, 620–647. [Google Scholar] [CrossRef] [Green Version]
- Rossouw, L.; Ross, H.; Bill & Melinda Gates Foundation. An economic assessment of menstrual hygiene Product Tax cuts. Gates Open Res. 2020, 4. [Google Scholar] [CrossRef]
- Fox, S. Advocating for Affordability: The Story of Menstrual Hygiene Product Tax Advocacy in Four Countries. Gates Open Res. 2020, 4. [Google Scholar] [CrossRef]
- Independent Panel of Experts for the Review of Zero Rating in South Africa. Recommendations on Zero Ratings in the Value-Added Tax System; South African Treasury: Pretoria, South Africa, 2018. [Google Scholar]
- Hennegan, J. Interventions to Improve Menstrual Health in Low-and Middle-Income Countries: Do We Know What Works? In The Palgrave Handbook of Critical Menstruation Studies; Palgrave Macmillan: Singapore, 2020; pp. 637–652. [Google Scholar]



{kind=link}
{kind=link}
| MHM Sample | Analytical Sample | Date Collected | |
|---|---|---|---|
| Kinshasa (DRC) [19] | 2125 | 2102 | 2017 |
| Ethiopia [20] | 4954 | 4814 | 2017 |
| Ghana [21] | 2935 | 2861 | 2016 |
| Kenya [22] | 4573 | 4478 | 2017 |
| Rajasthan (India) [23] | 5133 | 5018 | 2017 |
| Indonesia [24] | 8274 | 8122 | 2016 |
| Nigeria [25] | 8469 | 8121 | 2018 |
| Uganda [26] | 2798 | 2736 | 2017 |
| DRC (Kinshasa) | Ethiopia | Ghana | Kenya | India (Rajasthan) | Indonesia | Nigeria | Uganda | ||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Mean | Mean | Mean | Mean | Mean | Mean | Mean | ||
| Condition of main place for managing menstrual hygiene | Not clean | 0.158 | 0.511 | 0.137 | 0.125 | 0.187 | 0.054 | 0.134 | 0.091 |
| No private | 0.565 | 0.306 | 0.152 | 0.128 | 0.112 | 0.073 | 0.171 | 0.142 | |
| Not safe | 0.348 | 0.512 | 0.183 | 0.149 | 0.202 | 0.089 | 0.187 | 0.218 | |
| Cannot lock | 0.745 | 0.727 | 0.352 | 0.314 | 0.493 | 0.183 | 0.348 | 0.465 | |
| No water | 0.826 | 0.549 | 0.583 | 0.608 | 0.353 | 0.083 | 0.59 | 0.418 | |
| No soap | 0.838 | 0.631 | 0.561 | 0.674 | 0.39 | 0.135 | 0.618 | 0.425 | |
| Does not have all six conditions | 0.961 | 0.883 | 0.733 | 0.752 | 0.629 | 0.294 | 0.738 | 0.701 | |
| Materials used | No pads used | 0.168 | 0.41 | 0.103 | 0.136 | 0.535 | 0.087 | 0.367 | 0.357 |
| N | 2102 | 4814 | 2861 | 4478 | 5018 | 8122 | 8121 | 2736 |
| Kinshasa | Ethiopia | Ghana | Kenya | Rajasthan | Indonesia | Nigeria | Uganda | ||
|---|---|---|---|---|---|---|---|---|---|
| CCI | CCI | CCI | CCI | CCI | CCI | CCI | CCI | ||
| Condition of main place for managing menstrual hygiene | Not clean | −0.06 *** | −0.334 *** | −0.075 *** | −0.138 *** | −0.238 *** | −0.091 *** | −0.268 *** | −0.117 *** |
| No private | −0.028 | −0.176 *** | −0.156 *** | −0.095 *** | −0.1 *** | −0.138 *** | −0.283 *** | −0.105 *** | |
| Not safe | −0.147 *** | −0.35 *** | −0.133 *** | −0.135 *** | −0.251 *** | −0.13 *** | −0.317 *** | −0.158 *** | |
| Cannot lock | −0.221 *** | −0.307 *** | −0.191 *** | −0.405 *** | −0.529 *** | −0.276 *** | −0.544 *** | −0.467 *** | |
| No water | −0.05 *** | −0.23 *** | −0.092 *** | −0.25 *** | −0.338 *** | −0.104 *** | −0.285 *** | −0.293 *** | |
| No soap | −0.032 * | −0.168 *** | 0.021 | −0.184 *** | −0.308 *** | −0.124 *** | −0.249 *** | −0.246 *** | |
| Does not have all six conditions | −0.037 *** | −0.16 *** | −0.127 *** | −0.235 *** | −0.513 *** | −0.312 *** | −0.385 *** | −0.403 *** | |
| Materials used | No pads used | −0.15 *** | −0.627 *** | −0.18 *** | −0.198 *** | −0.447 *** | −0.093 *** | −0.586 *** | −0.303 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossouw, L.; Ross, H. Understanding Period Poverty: Socio-Economic Inequalities in Menstrual Hygiene Management in Eight Low- and Middle-Income Countries. Int. J. Environ. Res. Public Health 2021, 18, 2571. https://doi.org/10.3390/ijerph18052571
Rossouw L, Ross H. Understanding Period Poverty: Socio-Economic Inequalities in Menstrual Hygiene Management in Eight Low- and Middle-Income Countries. International Journal of Environmental Research and Public Health. 2021; 18(5):2571. https://doi.org/10.3390/ijerph18052571
Chicago/Turabian StyleRossouw, Laura, and Hana Ross. 2021. "Understanding Period Poverty: Socio-Economic Inequalities in Menstrual Hygiene Management in Eight Low- and Middle-Income Countries" International Journal of Environmental Research and Public Health 18, no. 5: 2571. https://doi.org/10.3390/ijerph18052571