1. Introduction
Degenerative disc disease (DDD) is one of the main causes of low back pain and contributes to the socioeconomic problems [
1,
2]. It is caused by damage to the tissue forming the intervertebral disc. Despite little to no innervation of the intervertebral disc, its pathology negatively affects many other structures in its proximity, such as the highly innervated posterior longitudinal ligament, spinal dura mater and nerve roots, which can cause a number of pathological conditions leading to pain [
3].
Degenerative disc disease is a progressive condition. Depending on the reason for dysfunction, various classifications are used to describe the level of advancement [
4]. The scientific literature on DDD commonly distinguishes between two types of the disease, protrusion and extrusion of the intervertebral disc, as approved by the American Society of Neuroradiology (ASNR). The clinical parameters of individuals with symptoms of a protruded or extruded lumbar disc are known to vary depending on the progression level of the disease and are usually recognized as acute, subacute and chronic phases depending on the symptoms, such as pain, functional outcome and ability to work [
5].
Contemporary methods for imaging and assessment of the activation of desired muscle groups, such as ultrasonography or electromyography (surface EMG, SEMG; intramuscular EMG, IEMG), make it possible to determine the involvement of certain muscles in the given movement sections or their exclusion from certain activities [
6]. Thus, it is possible to determine the exact function of a particular muscle group and administer targeted therapy, which contributes to achieving maximum recovery of the patient. Spinal stability is achieved through cooperation of the neural, muscular and skeletal systems. The main muscle structures responsible for stabilization of the lower back are the lumbar multifidus muscle and the deep abdominal muscles, particularly the transverse abdominal muscle; thus, targeted training of these groups is implemented in case of their dysfunction [
7].
Stabilizing training is a form of conservative treatment for lumbar pain alongside manual treatment or techniques in the fields of chiropractic and physiotherapy [
8,
9]. Conservative treatment methods usually constitute the first-line therapy for low back pain. In case of no improvement, those might also be a decisive tool within the need and timing of the surgery in the light of poor correlation between the radiological and clinical outcomes [
10,
11]. It is thought that proper stabilization of this region of the body is crucial for coping with pain [
12,
13,
14]. Although studies continue to examine the effectiveness of stabilization training, they primarily relate to chronic nonspecific low back pain [
14,
15]. Moreover, there is a lack of studies in the literature that attempted assessing the efficiency of physiotherapeutic treatment with regard to stabilization of the deep core muscles in young people with a protruded or extruded disc. We hypothesized that the core stabilizing training would have an effect on both types of the disease within the functional outcome but the time of the patient reaction can be different. Therefore, the aim of the study was to assess the effectiveness of core stability exercise in young patients with lumbar disc protrusion or extrusion.
2. Materials and Methods
2.1. Participants
The study included 42 experimental subjects (21 men and 21 women) with DDD and was designed as a non-randomized before-and-after study without a control group. The participants were recruited from Wroclaw Medical University and a private physiotherapy clinic. The recruitment was took place from January to December 2016. All the subjects underwent an imaging examination in the form of MRI, the results of which were interpreted by a radiologist. All the procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Declaration of Helsinki 1975 as revised in 2008. The research study protocol was approved by the IRB of the authors’ affiliated institutions and was registered at
ClinicalTrials.gov (accessed on 25 February 2021) (NCT04119466) in June 2019. All the subjects received detailed information about the research project and gave written consent to participate in the study. They were also informed about the possibility of withdrawal from the study at any time without any consequences.
The inclusion criteria included age between 20 and 35 years, DDD in the lumbar region of the spine confirmed by MRI and subacute stage of the disease. The exclusion criteria included advanced deformation changes of the spine, previous fracture of the spine, neurological deficits in the lower limbs or pelvis, tumors, spondylolisthesis, transitional vertebra, rheumatic disease or mental health disorders.
After enrollment, the damage to the intervertebral disc was classified as protrusion or extrusion based on the recommendations of the ASNR, with 21 patients included in the group with intervertebral disc protrusion (PRO) and 21—in the group with intervertebral disc extrusion (EXT).
2.2. Intervention
All the subjects underwent core stability exercise sessions over a period of four weeks (20 sessions in total) based on the protocol proposed by Richardson [
16]. The exercise was conducted from Monday to Friday and included activation of the lumbar multifidus muscle (m. multifidus) and the transverse abdominal muscle (m. transversus abdominis). One session comprised four exercises in which the patient was instructed to perform pelvic tilts (draw-in) with simultaneous full exhalation, thus activating the aforementioned muscle groups in different positions: (a) prone, (b) supine with lower extremities flexed, (c) quadruped and (d) standing with the back against the wall. The subjects performed three sets consisting of 10 repetitions, each of which lasted approximately 10 s. After this treatment period, the subjects were asked to refrain from any other form of exercise until the third examination (follow-up).
2.3. Outcome Measures
Clinical outcome assessment was performed at three timepoints during the study: prior to initiation of the exercise (pre-intervention, week 0), following the conclusion of the 20 exercise sessions (post-intervention, week 4), and four weeks after the completion of all exercise sessions (follow-up, week 8). An outcome assessor who was unaware of group allocation performed all outcome measurements.
The participants’ spinal range of motion (ROM) was assessed with a SpinalMouse
® device (Idiag AG, Fehraltorf, Sweden). This non-invasive device is used to assess spinal mobility, the reliability of which has been confirmed by other researchers [
17,
18,
19]. Within the scope of this study, the lumbar spine was measured in the sagittal plane. The device measured flexion and extension ROM, comprising the total mobility from maximum flexion to maximum extension. Three measurements were taken, and the mean value was used for statistical analyses. During the test, each subject was asked to stand with their feet placed on marked spots so that the distance between the feet was slightly smaller than the width of the pelvis. Then, the subject made an active movement over a range deemed by them to be maximal while keeping their balance and not using their upper limbs for support.
To quantify disability associated with low back pain, the Oswestry Disability Index (ODI) was used. The ODI is a validated and reliable assessment tool that is suited for use in clinical practice. The results are measured on a 100-point scale (range, 0–100), with higher scores indicating greater dysfunction [
20].
The straight leg raise (SLR) test is considered by researchers to be sensitive and specific in diagnosing damage to the peripheral nervous system [
21]. The subject’s lower limb was passively raised with the knee extended until potential symptoms were triggered, although not to an angle greater than 60° of flexion in the hip joint, which, according to Kapandji, causes maximum stretching of nerve structures. This test was considered to be positive (1) when it replicated the participant’s symptoms or provoked pain.
The passive lumbar extension (PLE) test was used as a tool for assessing the instability in the lumbar section of the spine [
22]. Ferrari et al. suggest that the PLE test is the most suitable test for detecting lumbar instability thanks to its excellent diagnostic accuracy and good reliability [
22]. This test was scored as positive (1) when it replicated the symptoms or provoked pain. The procedure was as follows: patient was in the prone position, both legs were then elevated concurrently to a height of about 30 cm from the bed while maintaining the knees extended and pulling the legs [
23].
The subjective level of pain associated with the patient’s current condition was assessed based on a numeric rating scale (NRS). The intraclass correlation coefficient of the NRS is 0.95 [
24].
2.4. Data Analysis
All statistical calculations were performed using the Statistica 12.5 software (StatSoft, Palo Alto, CA, USA). The data were presented as the means and standard deviations (SD) or the medians and interquartile ranges (IQR). The groups were compared at the baseline using a t-test for independent samples (unpaired) for continuous variables and the chi-squared test for categorical data. The results of therapy were analyzed using Friedman’s ANOVA with the Wilcoxon post-hoc test. The Friedman’s ANOVA effect size was calculated using Kendall’s W and with interpretation guidelines of 0.1 ≥ x < 0.3 (small effect), 0.3 ≥ x < 0.5 (moderate effect) and x ≥ 0.5 (large effect). For dichotomous values, (SLR/PLE), the Cochran’s Q test was used. Values of α < 0.05 were considered to be statistically significant.
3. Results
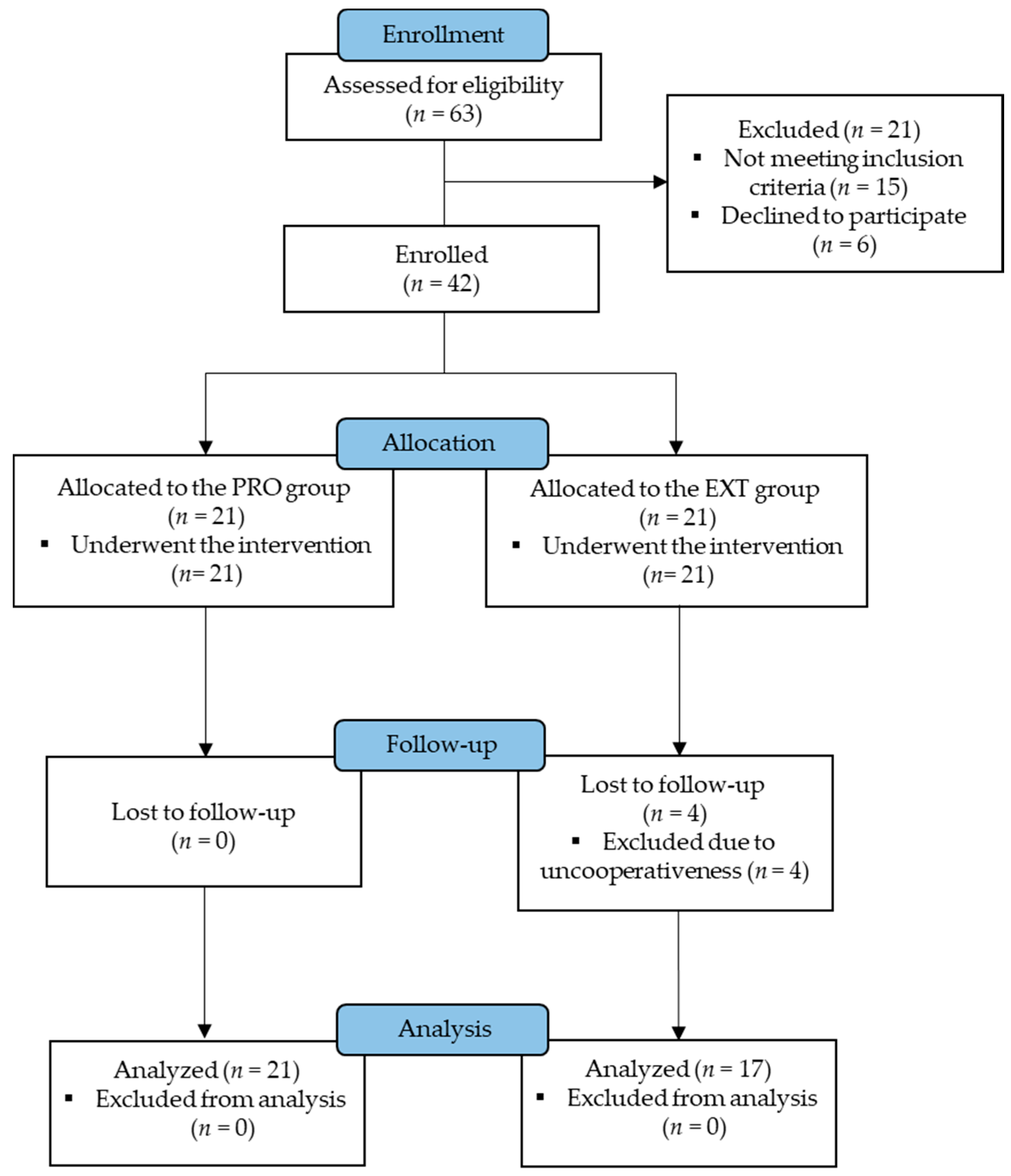
Four participants from the EXT group did not complete the intervention program. The sample size at each assessment timepoint is presented in
Figure 1. In total, the study comprised 21 subjects with protrusion (PRO) and 17 subjects with extrusion (EXT) with the average age of 28.24 (SD, 3.88) and 30.17 (SD, 3.30) years, respectively (
Table 1). The pre-intervention, post-intervention and follow-up scores for clinical outcomes and tests are presented in
Table 2.
In the PRO group, the total range of motion in the sagittal plane from before the intervention to after the intervention and from before the intervention to the follow-up was reduced by 6% in both tests, with values of 88.52° (SD, 6.93), 83.33° (SD, 5.64) and 82.85° (SD, 3.69) measured in the pre-intervention, post-intervention and follow-up assessments, respectively (Kendall’s W = 0.26; p = 0.01). The ODI results revealed a reduction post-intervention by 59%, from 16.14 (SD, 6.71) to 6.57 (SD, 0.58) points, and a reduction by 42% (to 9.42 points, SD, 7.15) at the follow-up examination (Kendall’s W = 0.60; p < 0.01). The subjective level of pain reported by the participants was reduced by 47% and 65% at the post-intervention and follow-up examinations, respectively (Kendall’s W = 0.86; p < 0.01).
In the EXT group, the ROM decreased by 5% and 4% at the post-intervention and follow-up examinations, respectively (pre-intervention, 88.52°; SD, 6.93; post-intervention, 83.33°; SD, 5.64; follow-up, 82.85°; SD, 3.69; Kendall’s W = 0.20; p = 0.01). The ODI results were 32% lower after the intervention and 35% lower at the follow-up examination (Kendall’s W = 0.48; p < 0.001). The subjective pain level measured using the NRS was decreased by 46% (to 4.85 points, SD, 1.01 vs. to 2.57 points, SD, 1.32) post-intervention and by 55% at the follow-up examination (Kendall’s W = 0.78; p < 0.001).
4. Discussion
Despite an abundance of previous research, the treatment of DDD still raises considerable uncertainties concerning the course of rehabilitation [
25]. The literature comprises numerous publications on the influence and effectiveness of stabilizing exercises for the lumbar multifidus muscle and the transverse abdominal muscle in patients with low back pain [
7,
26,
27,
28,
29]; however, there is little scientific evidence to support this form of exercise for treating people under 35 years of age. The present study examined another criterion for the division of patients, namely, the type of damage to the intervertebral disc (disc protrusion or extrusion in the subacute stage of the disease according to the ASNR classification). Although Rasmussen–Barr et al. demonstrated the effectiveness of stabilizing exercise in people suffering from subacute DDD, they did not explicitly divide subjects by the type of damage to the intervertebral disc [
30]. Preliminary research suggests that the patients’ functional condition varies depending on the progression of the disease. Thus, there are important differences concerning the types of everyday activities and the level of associated pain, where patients with an extruded disc experience greater levels of pain [
5].
After four weeks of therapy, the ROM decreased in both groups. During the follow-up period, the tendency for reduced lumbar spine mobility was sustained, although the patients were instructed not to perform any other form of treatment except for the previously administered intervention. This reduced ROM also affected the PLE test results and was probably due to improved neuromuscular control in the area of the muscles stabilizing the lower spine and the general influence of being aware of participating in a research study [
31]. When attempting to characterize the biomechanics of the lumbar spine in patients with DDD, Hueng et al. observed a decrease in mobility in the sagittal plane as the pathology progresses [
32]. It is also worth bearing in mind that the degeneration of the intervertebral disc could trigger a pathological cycle, the progression of which leads to increasingly limited mobility of vertebral segments [
33].
The experience of pain in people suffering from DDD is the main reason for the commencement of treatment, and pain usually accompanies the patient throughout the course of the disease. In the presented research, pain relief was observed in patients both with protruded and extruded discs. Many studies have demonstrated the effectiveness of stabilizing exercise in terms of the level of pain and assessment of the degree of disability [
8,
34,
35], but none have assessed participants based on the progression of disc disease, and the available scientific evidence is often insufficient [
25]. The ODI analysis performed in the current study demonstrated the overall effectiveness of stabilizing exercise in both groups. However, because the initial parameters showed statistically significant differences between the groups, interpretation of subsequent stages of the study with the Oswestry questionnaire was not performed due to the non-homogenous nature of the groups. In spite of this, significant differences were observed between the pre-intervention and the post-intervention examinations in both groups. Similar conclusions have been drawn by other researchers, although the clinical condition of subjects was often not determined on the basis of medical imaging [
35,
36].
When studying subjects with DDD, it is recommended that the irritation of nerve structures be assessed. In this study, we used the SLR. The initial values differed significantly between the two groups. In the PRO group, the results deteriorated; therefore, the therapy did not prove to be successful with respect to the SLR test. However, in the EXT group, a decrease in irritability of nerve structures was observed. In that group, the effect was observed across all stages of the study, although the follow-up results did not differ significantly from the post-intervention examination.
Three factors limit the generalizability of this study. The first is the lack of a control group that received no intervention for disc protrusion and extrusion. For this reason, we could not perform randomization, which severely limits our ability to draw conclusions. Second, as this was a pilot study, the sample size was relatively small. Third, our study did not examine the longitudinal effects of the interventions used; therefore, future research should include follow-up outcome measures. Lastly, in our research, we did not meet the assumptions for parametric tests; therefore, nonparametric tests were used, which are statistically weaker. However, our results may aid in the design of future studies with regard to the study protocol or the generation of effect sizes, which can be used to power a larger randomized clinical trial.
5. Conclusions
To date, this study is one of the few to examine the effects of core stability exercise in individuals with DDD, with a distinction between the degree of progression into protrusion and extrusion. Our research showed that stabilization training can reduce pain, improve the clinical condition and daily living activities of people with DDD. However, due to the limitations of our study, the generalizability is limited. Based on the obtained results, we are unable to unambiguously state whether the type of damage to the intervertebral disc significantly affects the results of a stabilizing exercise-based treatment.
Author Contributions
Conceptualization, T.K. and A.S.; methodology, T.K. and B.C.; formal analysis, A.D.-B. and B.C.; investigation, T.K.; resources, N.K.; data curation, A.D.-B.; writing—original draft preparation, T.K., B.C. and N.K.; writing—review and editing, A.D.-B. and A.S.; supervision, A.S.; project administration, T.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the University School of Physical Education in Wroclaw, Poland (No. 11/2015; May 2015).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Genevay, S.; Courvoisier, D.S.; Konstantinou, K.; Kovacs, F.M.; Marty, M.; Rainville, J.; Norberg, M.; Kaux, J.F.; Cha, T.D.; Katz, J.N.; et al. Clinical Classification Criteria for Neurogenic Claudication Caused by Lumbar Spinal Stenosis. The N-CLASS Criteria. Spine J. 2018, 18, 941–947. [Google Scholar] [CrossRef] [Green Version]
- Baek, S.O.; Cho, H.K.; Jung, G.S.; Son, S.M.; Cho, Y.W.; Ahn, S.H. Verification of an Optimized Stimulation Point on the Abdominal Wall for Transcutaneous Neuromuscular Electrical Stimulation for Activation of Deep Lumbar Stabilizing Muscles. Spine J. 2014, 14, 2178–2183. [Google Scholar] [CrossRef] [PubMed]
- Daghighi, M.H.; Pouriesa, M.; Maleki, M.; Fouladi, D.F.; Pezeshki, M.Z.; Mazaheri Khameneh, R.; Bazzazi, A.M. Migration Patterns of Herniated Disc Fragments: A Study on 1,020 Patients with Extruded Lumbar Disc Herniation. Spine J. 2014, 14, 1970–1977. [Google Scholar] [CrossRef]
- Williams, A.L.; Murtagh, F.R.; Rothman, S.L.G.; Sze, G.K. Lumbar Disc Nomenclature: Version 2.0. Am. J. Neuroradiol. 2014, 35, 2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuligowski, T.; Cieślik, B.; Nowicka, Z. Functional Outcomes in Relation with the Progression Level in Young Degenerative Disc Disease Patients. Fizjoterapia 2017, 24. [Google Scholar] [CrossRef]
- Kim, C.Y.; Choi, J.D.; Kim, S.Y.; Oh, D.W.; Kim, J.K.; Park, J.W. Comparison between Muscle Activation Measured by Electromyography and Muscle Thickness Measured Using Ultrasonography for Effective Muscle Assessment. J. Electromyogr. Kinesiol. 2014, 24, 614–620. [Google Scholar] [CrossRef]
- Wong, A.Y.L.; Parent, E.C.; Funabashi, M.; Kawchuk, G.N. Do Changes in Transversus Abdominis and Lumbar Multifidus During Conservative Treatment Explain Changes in Clinical Outcomes Related to Nonspecific Low Back Pain? A Systematic Review. J. Pain 2014, 15, 377.e1–377.e35. [Google Scholar] [CrossRef] [PubMed]
- Aluko, A.; DeSouza, L.; Peacock, J. The Effect of Core Stability Exercises on Variations in Acceleration of Trunk Movement, Pain, and Disability during an Episode of Acute Nonspecific Low Back Pain: A Pilot Clinical Trial. J. Manip. Physiol. Ther. 2013, 36, 497–504.e3. [Google Scholar] [CrossRef]
- Park, S.; Choi, B. Effects of Lumbar Stabilization Exercises on the Flexion-Relaxation Phenomenon of the Erector Spinae. J. Phys. Ther. Sci. 2016, 28, 1709–1711. [Google Scholar] [CrossRef] [Green Version]
- Andersen, J.C. Is Immediate Imaging Important in Managing Low Back Pain? J. Athl. Train. 2011, 46, 99–102. [Google Scholar] [CrossRef] [Green Version]
- Chou, R.; Fu, R.; Carrino, J.A.; Deyo, R.A. Imaging Strategies for Low-Back Pain: Systematic Review and Meta-Analysis. Lancet 2009, 373, 463–472. [Google Scholar] [CrossRef]
- Dagenais, S.; Mayer, J.; Haldeman, S.; Borg-Stein, J. Evidence-Informed Management of Chronic Low Back Pain with Prolotherapy. Spine J. 2008, 8, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Owen, P.J.; Miller, C.T.; Mundell, N.L.; Verswijveren, S.J.J.M.; Tagliaferri, S.D.; Brisby, H.; Bowe, S.J.; Belavy, D.L. Which Specific Modes of Exercise Training Are Most Effective for Treating Low Back Pain? Network Meta-Analysis. Br. J. Sports Med. 2020, 54, 1279–1287. [Google Scholar] [CrossRef]
- Coulombe, B.J.; Games, K.E.; Neil, E.R.; Eberman, L.E. Core Stability Exercise Versus General Exercise for Chronic Low Back Pain. J. Athl. Train. 2017, 52, 71–72. [Google Scholar] [CrossRef]
- Niederer, D.; Mueller, J. Sustainability Effects of Motor Control Stabilisation Exercises on Pain and Function in Chronic Nonspecific Low Back Pain Patients: A Systematic Review with Meta-Analysis and Meta-Regression. PLoS ONE 2020, 15, e0227423. [Google Scholar] [CrossRef]
- Richardson, C.A.; Jull, G.A. Muscle Control-Pain Control. What Exercises Would You Prescribe? Man. Ther. 1995, 1, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Post, R.B.; Leferink, V.J.M. Spinal Mobility: Sagittal Range of Motion Measured with the SpinalMouse, a New Non-Invasive Device. Arch. Orthop. Trauma Surg. 2004, 124, 187–192. [Google Scholar] [CrossRef]
- Mannion, A.F.; Knecht, K.; Balaban, G.; Dvorak, J.; Grob, D. A New Skin-Surface Device for Measuring the Curvature and Global and Segmental Ranges of Motion of the Spine: Reliability of Measurements and Comparison with Data Reviewed from the Literature. Eur. Spine J. 2004, 13, 122–136. [Google Scholar] [CrossRef] [Green Version]
- Livanelioglu, A.; Kaya, F.; Nabiyev, V.; Demirkiran, G.; Fırat, T. The Validity and Reliability of “Spinal Mouse” Assessment of Spinal Curvatures in the Frontal Plane in Pediatric Adolescent Idiopathic Thoraco-Lumbar Curves. Eur. Spine J. 2016, 25, 476–482. [Google Scholar] [CrossRef]
- Vianin, M. Psychometric Properties and Clinical Usefulness of the Oswestry Disability Index. J. Chiropr. Med. 2008, 7, 161–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capra, F.; Vanti, C.; Donati, R.; Tombetti, S.; O’Reilly, C.; Pillastrini, P. Validity of the Straight-Leg Raise Test for Patients with Sciatic Pain with or without Lumbar Pain Using Magnetic Resonance Imaging Results as a Reference Standard. J. Manip. Physiol. Ther. 2011, 34, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, S.; Manni, T.; Bonetti, F.; Villafañe, J.H.; Vanti, C. A Literature Review of Clinical Tests for Lumbar Instability in Low Back Pain: Validity and Applicability in Clinical Practice. Chiropr. Man. Ther. 2015, 23, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasai, Y.; Morishita, K.; Kawakita, E.; Kondo, T.; Uchida, A. A New Evaluation Method for Lumbar Spinal Instability: Passive Lumbar Extension Test. Phys. Ther. 2006, 86, 1661–1667. [Google Scholar] [CrossRef] [PubMed]
- Alghadir, A.H.; Anwer, S.; Iqbal, A.; Iqbal, Z.A. Test–Retest Reliability, Validity, and Minimum Detectable Change of Visual Analog, Numerical Rating, and Verbal Rating Scales for Measurement of Osteoarthritic Knee Pain. J. Pain Res. 2018, 11, 851–856. [Google Scholar] [CrossRef] [Green Version]
- Hahne, A.J.; Ford, J.J.; Hinman, R.S.; Richards, M.C.; Surkitt, L.D.; Chan, A.Y.P.; Slater, S.L.; Taylor, N.F. Individualized Functional Restoration as an Adjunct to Advice for Lumbar Disc Herniation with Associated Radiculopathy. A Preplanned Subgroup Analysis of a Randomized Controlled Trial. Spine J. 2017, 17, 346–359. [Google Scholar] [CrossRef]
- Altinkaya, N.; Cekinmez, M. Lumbar Multifidus Muscle Changes in Unilateral Lumbar Disc Herniation Using Magnetic Resonance Imaging. Skelet. Radiol. 2016, 45, 73–77. [Google Scholar] [CrossRef]
- Hebert, J.J.; Koppenhaver, S.L.; Magel, J.S.; Fritz, J.M. The Relationship of Transversus Abdominis and Lumbar Multifidus Activation and Prognostic Factors for Clinical Success With a Stabilization Exercise Program: A Cross-Sectional Study. Arch. Phys. Med. Rehabil. 2010, 91, 78–85. [Google Scholar] [CrossRef]
- Hides, J.; Stanton, W.; Dilani Mendis, M.; Sexton, M. The Relationship of Transversus Abdominis and Lumbar Multifidus Clinical Muscle Tests in Patients with Chronic Low Back Pain. Man. Ther. 2011, 16, 573–577. [Google Scholar] [CrossRef]
- Wang-Price, S.; Zafereo, J.; Brizzolara, K.; Sokolowski, L.; Turner, D. Effects of Different Verbal Instructions on Change of Lumbar Multifidus Muscle Thickness in Asymptomatic Adults and in Patients with Low Back Pain. J. Man. Manip. Ther. 2017, 25, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen-Barr, E.; Nilsson-Wikmar, L.; Arvidsson, I. Stabilizing Training Compared with Manual Treatment in Sub-Acute and Chronic Low-Back Pain. Man. Ther. 2003, 8, 233–241. [Google Scholar] [CrossRef]
- Antonio, L.; Guglielmi, G.; Cassar-Pullicino, V.N.; Bonomo, L. Lumbar Intervertebral Instability: A Review. Radiology 2007, 245, 62–77. [Google Scholar] [CrossRef]
- Hueng, D.Y.; Chung, T.T.; Chuang, W.H.; Hsu, C.P.; Chou, K.N.; Lin, S.C. Biomechanical Effects of Cage Positions and Facet Fixation on Initial Stability of the Anterior Lumbar Interbody Fusion Motion Segment. Spine 2014, 39, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Jaumard, N.V.; Welch, W.C.; Winkelstein, B.A. Spinal Facet Joint Biomechanics and Mechanotransduction in Normal, Injury and Degenerative Conditions. J. Biomech. Eng. 2011, 133, 071010. [Google Scholar] [CrossRef] [Green Version]
- França, F.R.; Burke, T.N.; Caffaro, R.R.; Ramos, L.A.; Marques, A.P. Effects of Muscular Stretching and Segmental Stabilization on Functional Disability and Pain in Patients with Chronic Low Back Pain: A Randomized, Controlled Trial. J. Manip. Physiol. Ther. 2012, 35, 279–285. [Google Scholar] [CrossRef]
- Heo, M.-Y.; Kim, K.; Hur, B.-Y.; Nam, C.-W. The Effect of Lumbar Stabilization Exercises and Thoracic Mobilization and Exercises on Chronic Low Back Pain Patients. J. Phys. Ther. Sci. 2015, 27, 3843–3846. [Google Scholar] [CrossRef] [Green Version]
- Hosseinifar, M.; Akbari, M.; Behtash, H.; Amiri, M.; Sarrafzadeh, J. The Effects of Stabilization and Mckenzie Exercises on Transverse Abdominis and Multifidus Muscle Thickness, Pain, and Disability: A Randomized Controlled Trial in NonSpecific Chronic Low Back Pain. J. Phys. Ther. Sci. 2013, 25, 1541–1545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}