
Incidence, Risk Factors, and Outcomes of Preterm and Early Term Births: A Population-Based Register Study

 , ,
, ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Neonatal Factors
2.3. Maternal Factors
2.4. Statistical Analysis
3. Results
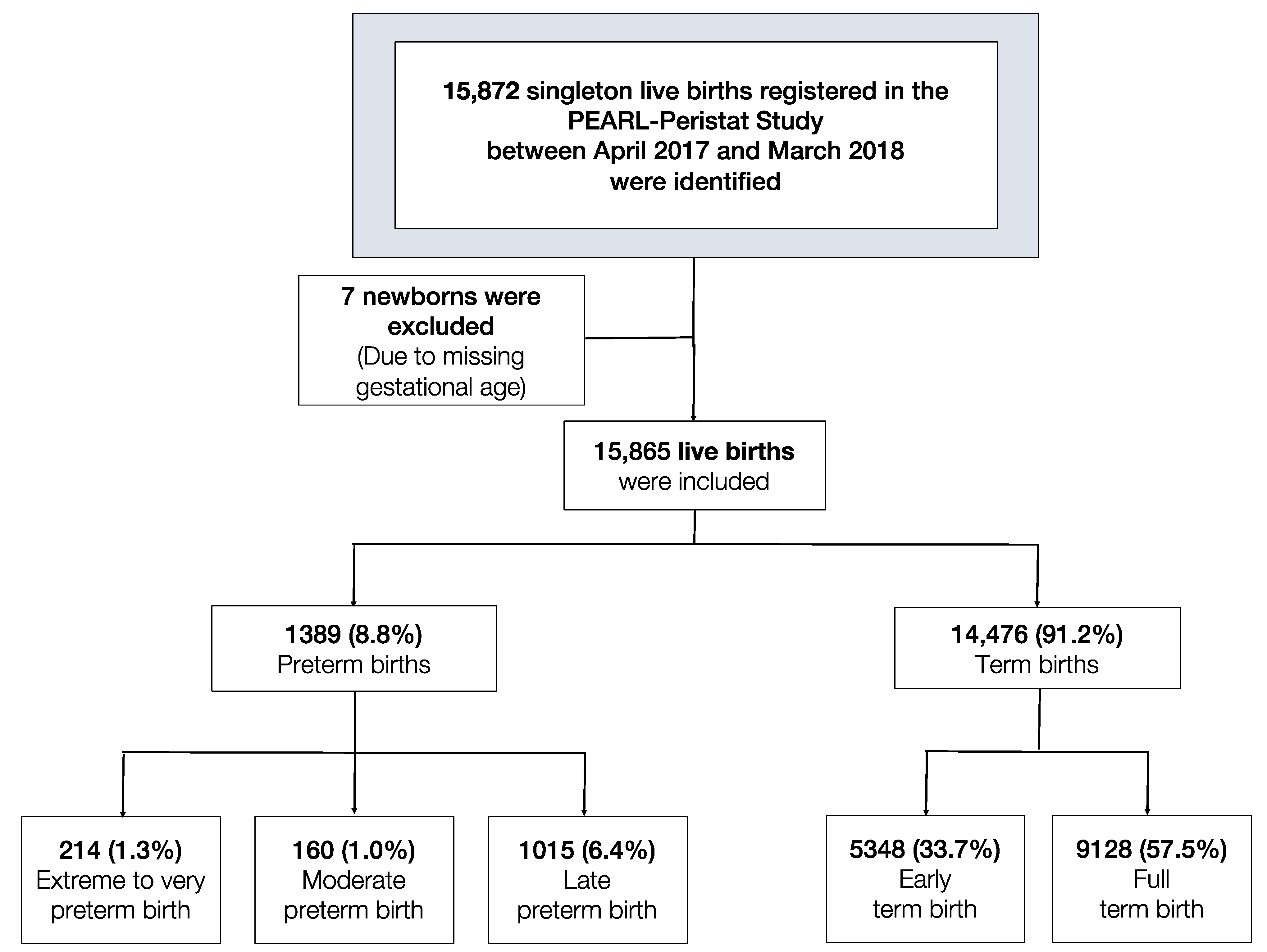
3.1. Characteristics of the Study Population and Differences between Pre and Early Term Groups in Comparison to Full Term Group
3.2. Risk Factors Associated with PTB and ETB
3.3. Adverse Outcomes Associated with PTB and ETB
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- March of Dimes, PMNCH, Save the Children, WHO. Born Too Soon: The Global Action Report on Preterm Birth. Available online: https://www.marchofdimes.org/materials/born-too-soon-the-global-action-report-on-preterm-.pdf (accessed on 18 October 2020).
- Samara, M.; Wolke, D.; Marlow, N. Pervasive Behaviour problems at six years of age in a whole population sample of children born at 25 weeks of gestation or less. Pediatrics 2008, 122, 562–573. [Google Scholar] [CrossRef]
- Wolke, D.; Samara, M.; Bracewell, M.; Marlow, N. Specific language difficulties and school achievement in a whole population sample of children born at 25 weeks of gestation or less. J. Pediatr. 2008, 152, 256–262.e1. [Google Scholar] [CrossRef] [Green Version]
- Wolke, D.; Chernova, J.; Eryigit Madzwamuse, S.; Samara, M.; Zwierzynska, K.; Petrou, S. Self and Parent Perspectives on Health Related Quality of Life of Adolescents born Very Preterm. J. Pediatr. 2013. [Google Scholar] [CrossRef] [PubMed]
- Samara, M.; Neil, M.; Johnson, S.; Lamberts, K.; Wolke, D. Eating problems at six years of age in a whole population sample of children born at 25 weeks of gestation or less. Dev. Med. Child Neurol. 2010, 52, e16–e22. [Google Scholar] [CrossRef] [Green Version]
- Muhe, L.M.; McClure, E.M.; Nigussie, A.K.; Mekasha, A.; Worku, B.; Worku, A.; Demtse, A.; Eshetu, B.; Tigabu, Z.; Gizaw, M.A.; et al. Major causes of death in preterm infants in selected hospitals in Ethiopia (SIP): A prospective, cross-sectional, observational study. Lancet Glob. Health 2019, 7, e1130–e1138. [Google Scholar] [CrossRef] [Green Version]
- Allin, M.; Rooney, M.; Griffiths, T.; Cuddy, M.; Wyatt, J.; Rifkin, L.; Murray, R. Neurological abnormalities in young adults born preterm. J. Neurol. Neurosurg. Psychiatry 2006, 77, 495. [Google Scholar] [CrossRef] [Green Version]
- Luu, T.M.; Katz, S.L.; Leeson, P.; Thébaud, B.; Nuyt, A.-M. Preterm birth: Risk factor for early-onset chronic diseases. Can. Med. Assoc. J. 2016, 188, 736. [Google Scholar] [CrossRef] [Green Version]
- Fleischman, A.R.; Oinuma, M.; Clark, S.L. Rethinking the Definition of “Term Pregnancy”. Obstet. Gynecol. 2010, 116, 136–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). ICD-10: International Statistical Classification of Diseases and Related Health Problems; 10th Revision; World Health Organization: Geneva, Switzerland; Volume 2, Available online: http://www.who.int/classifications/icd/ICD-10_2nd_ed_volume2.pdf (accessed on 12 February 2021).
- ACOG Committee Opinion No. 579: Definition of term pregnancy; American College of Obstetricians and Gynecologists. Obstet. Gynecol. 2013, 122, 1139–1140. [CrossRef] [PubMed]
- Zhang, X.; Kramer, M.S. Variations in mortality and morbidity by gestational age among infants born at term. J. Pediatr. 2009, 154, 358–362. [Google Scholar] [CrossRef]
- Sengupta, S.; Carrion, V.; Shelton, J.; Wynn, R.J.; Ryan, R.M.; Singhal, K.; Lakshminrusimha, S. Adverse neonatal outcomes associated with early-term birth. JAMA Pediatr. 2013, 167, 1053–1059. [Google Scholar] [CrossRef] [Green Version]
- Helle, E.; Andersson, S.; Häkkinen, U.; Järvelin, J.; Eskelinen, J.; Kajantie, E. Morbidity and health care costs after early term birth. Paediatr. Perinat Epidemiol. 2016, 30, 533–540. [Google Scholar] [CrossRef]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, R.L.; McClure, E.M. The epidemiology of preterm birth. Preterm Birth 2010, 22. [Google Scholar] [CrossRef]
- Lumley, J. Defining the problem: The epidemiology of preterm birth. BJOG Int. J. Obstet. Gynaecol. 2003, 110, 3–7. [Google Scholar] [CrossRef]
- Richards, J.L.; Kramer, M.S.; Deb-Rinker, P.; Rouleau, J.; Mortensen, L.; Gissler, M.; Morken, N.H.; Skjærven, R.; Cnattingius, S.; Johansson, S.; et al. Temporal Trends in Late Preterm and Early Term Birth Rates in 6 High-Income Countries in North America and Europe and Association with Clinician-Initiated Obstetric Interventions. JAMA 2016, 316, 410–419. [Google Scholar] [CrossRef] [Green Version]
- Delnord, M.; Mortensen, L.; Hindori-Mohangoo, A.D.; Blondel, B.; Gissler, M.; Kramer, M.R.; Richards, J.L.; Deb-Rinker, P.; Rouleau, J.; Morisaki, N.; et al. International variations in the gestational age distribution of births: An ecological study in 34 high-income countries. Eur. J. Public Health 2018, 28, 303–309. [Google Scholar] [CrossRef]
- Romero, R.; Espinoza, J.; Kusanovic, J.P.; Gotsch, F.; Hassan, S.; Erez, O.; Chaiworapongsa, T.; Mazor, M. The preterm parturition syndrome. BJOG Int. J. Obstet. Gynaecol. 2006, 113, 17–42. [Google Scholar] [CrossRef]
- Anum, E.A.; Springel, E.H.; Shriver, M.D.; Strauss, J.F., 3rd. Genetic contributions to disparities in preterm birth. Pediatr. Res. 2009, 65, 1–9. [Google Scholar] [CrossRef]
- DeFranco, E.; Teramo, K.; Muglia, L. Genetic influences on preterm birth. Semin. Reprod. Med. 2007, 25, 40–51. [Google Scholar] [CrossRef] [Green Version]
- Varner, M.W.; Esplin, M.S. Current understanding of genetic factors in preterm birth. BJOG Int. J. Obstet. Gynaecol. 2005, 112 (Suppl. 1), 28–31. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Understanding Premature Birth and Assuring Healthy Outcomes; Behrman, R.E.; Butler, A.S. (Eds.) Chapter 8—The Role of Environmental Toxicants in Preterm Birth. In Preterm Birth: Causes, Consequences, and Prevention; National Academies Press: Washington, DC, USA, 2007. Available online: https://www.ncbi.nlm.nih.gov/books/NBK11368/ (accessed on 13 February 2021).
- Ferguson, K.K.; Meeker, J.D. The Role of Environmental Exposures in Preterm Birth. In Translational Toxicology. Molecular and Integrative Toxicology; Hughes, C., Waters, M., Eds.; Humana Press: Cham, Switzerland, 2016. [Google Scholar] [CrossRef]
- Filicori, M.; Cognigni, G.E.; Gamberini, E.; Troilo, E.; Parmegiani, L.; Bernardi, S. Impact of medically assisted fertility on preterm birth. BJOG Int. J. Obstet. Gynaecol. 2005, 112 (Suppl. 1), 113–117. [Google Scholar] [CrossRef]
- Wang, J.X.; Norman, R.J.; Kristiansson, P. The effect of various infertility treatments on the risk of preterm birth. Hum. Reprod. 2002, 17, 945–949. [Google Scholar] [CrossRef] [Green Version]
- Ibrahimou, B.; Kodali, S.; Salihu, H. Survival of Preterm Singleton Deliveries: A Population-Based Retrospective Study. Adv. Epidemiol. 2015, 2015, 858274. [Google Scholar] [CrossRef] [Green Version]
- Joseph, K.S.; Fahey, J.; Shankardass, K.; Allen, V.M.; O’Campo, P.; Dodds, L.; Liston, R.M.; Allen, A.C. Effects of socioeconomic position and clinical risk factors on spontaneous and iatrogenic preterm birth. BMC Pregnancy Childbirth 2014, 14, 117. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Marlow, N.; Wolke, D.; Bracewell, M.A.; Samara, M. Neurologic and developmental disability at six years of age after extremely preterm birth. N. Engl. J. Med. 2005, 352, 9–19. [Google Scholar] [CrossRef]
- Van Wassenaer-Leemhuis, A.G.; Marlow, N.; Lees, C.; Wolf, H. The association of neonatal morbidity with long-term neurological outcome in infants who were growth restricted and preterm at birth: Secondary analyses from TRUFFLE (Trial of Randomized Umbilical and Fetal Flow in Europe). BJOG Int. J. Obstet. Gynaecol. 2017, 124, 1072–1078. [Google Scholar] [CrossRef]
- Shah, P.S.; Kusuda, S.; Håkansson, S.; Reichman, B.; Lui, K.; Lehtonen, L.; Modi, N.; Vento, M.; Adams, M.; Rusconi, F.; et al. Neonatal Outcomes of Very Preterm or Very Low Birth Weight Triplets. Pediatrics 2018, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, L.V.; Hashmi, M.F.; Bragg, B.N. APGAR Score; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- NHLBI Obesity Education Initiative Expert Panel on the Identification, Evaluation, and Treatment of Obesity in Adults (US). Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report; National Heart, Lung, and Blood Institute: Bethesda, MD, USA, 1998. Available online: https://www.ncbi.nlm.nih.gov/books/NBK2003/ (accessed on 14 February 2021).
- World Health Organization (WHO). Obesity—Preventing and Managing the Global Epidemic; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Delnord, M.; Zeitlin, J. Epidemiology of late preterm and early term births—An international perspective. Semin. Fetal Neonat. Med. 2019, 24, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Baer, R.J.; Berghella, V.; Chambers, C.; Chung, P.; Coker, T.; Currier, R.J.; Druzin, M.L.; Kuppermann, M.; Muglia, L.J. Recurrence of preterm birth and early term birth. Obstet. Gynecol. 2016, 128, 364. [Google Scholar] [CrossRef] [Green Version]
- Ferrero, D.M.; Larson, J.; Jacobsson, B.; Di Renzo, G.C.; Norman, J.E.; Martin, J.N., Jr.; D’Alton, M.; Castelazo, E.; Howson, C.P.; Sengpiel, V. Cross-country individual participant analysis of 4.1 million singleton births in 5 countries with very high human development index confirms known associations but provides no biologic explanation for 2/3 of all preterm births. PLoS ONE 2016, 11, e0162506. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Preterm Birth—Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 14 December 2020).
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef] [Green Version]
- Ray, J.G.; Park, A.L.; Fell, D.B. Mortality in Infants Affected by Preterm Birth and Severe Small-for-Gestational Age Birth Weight. Pediatrics 2017, 140, e20171881. [Google Scholar] [CrossRef] [Green Version]
- Jensen, E.A.; Foglia, E.E.; Dysart, K.C.; Simmons, R.A.; Aghai, Z.H.; Cook, A.; Greenspan, J.S.; DeMauro, S.B. Adverse effects of small for gestational age differ by gestational week among very preterm infants. Arch. Dis. Child. Fetal Neonat. Ed. 2019, 104, F192. [Google Scholar] [CrossRef]
- Saigal, S.; Doyle, L.W. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 2008, 371, 261–269. [Google Scholar] [CrossRef]
- Lawn, J.E.; Davidge, R.; Paul, V.K.; von Xylander, S.; de Graft Johnson, J.; Costello, A.; Kinney, M.V.; Segre, J.; Molyneux, L. Born too soon: Care for the preterm baby. Reprod. Health 2013, 10 (Suppl. 1), S5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simões, R.; Cavalli, R.C.; Bernardo, W.M.; Salomão, A.J.; Baracat, E.C. Cesarean delivery and prematurity. Rev. Assoc. Med. Bras. 2015, 61, 489–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, S.; Al Rifai, H.; El Ansari, W.; Nimeri, N.; El Tinay, S.; Salameh, K.; Abbas, T.; Jarir, R.A.; Said, N.; Taha, S. A PEARL Study Analysis of National Neonatal, Early Neonatal, Late Neonatal, and Corrected Neonatal Mortality Rates in the State of Qatar during 2011: A Comparison with World Health Statistics 2011 and Qatar’s Historic Data over a Period of 36 Years (1975–2011). J. Clin. Neonatol. 2012, 1, 195–201. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Extreme to Very PTB (n = 214) | Moderate PTB (n = 160) | Late PTB (n = 1015) | ETB (n = 5348) | FTB (n = 9128) (Ref.) | |||||
|---|---|---|---|---|---|---|---|---|---|
| n (%) | p Value | n (%) | p Value | n (%) | p Value | n (%) | p Value | n (%) | |
| Maternal age | <0.001 | <0.001 | <0.001 | <0.001 | |||||
| Normal (20–34 yr) | 149 (69.6) | 107 (66.9) | 718 (70.7) | 3973 (74.3) | 7402 (81.1) | ||||
| Young (<20 yr) | 5 (2.3) | 7 (4.4) | 20 (2) | 99 (1.9) | 219 (2.4) | ||||
| Advanced (35–39 yr) | 46 (21.5) | 36 (22.5) | 217 (21.4) | 937 (17.5) | 1209 (13.2) | ||||
| Very advanced (40–44 yr) | 14 (6.5) | 9 (5.6) | 53 (5.2) | 310 (5.8) | 285 (3.1) | ||||
| Extremely advanced (≥45 yr) | 0 (0) | 1 (0.6) | 7 (0.7) | 29 (0.5) | 13 (0.1) | ||||
| Parity | 0.001 | 0.283 | 0.105 | <0.001 | |||||
| Nulliparous | 85 (39.7) | 53 (33.1) | 272 (26.8) | 1232 (23) | 2668 (29.2) | ||||
| Parity ≥ 1 | 129 (60.3) | 107 (66.9) | 743 (73.2) | 4116 (77) | 6460 (70.8) | ||||
| Nationality | <0.05 | <0.05 | <0.001 | 0.001 | |||||
| Qatari | 61 (28.5) | 57 (35.6) | 343 (33.8) | 1730 (32.4) | 2750 (30.1) | ||||
| Other Arabs | 75 (35) | 48 (30) | 349 (34.4) | 2048 (38.3) | 3786 (41.5) | ||||
| Other Nationalities | 78 (36.4) | 55 (34.4) | 323 (31.8) | 1569 (29.3) | 2589 (28.4) | ||||
| Consanguineous | 0.161 | 0.651 | 0.163 | 0.634 | |||||
| No | 42 (75) | 27 (62.8) | 217 (62.4) | 1435 (66.7) | 2444 (66.1) | ||||
| Yes | 14 (25) | 16 (37.2) | 131 (37.6) | 717 (33.3) | 1255 (33.9) | ||||
| Education | 0.570 | 0.168 | <0.05 | 0.248 | |||||
| Elementary and below | 4 (6.5) | 1 (2.2) | 47 (12.4) | 205 (9) | 355 (8.9) | ||||
| Secondary/Highschool | 23 (37.1) | 12 (26.7) | 130 (34.3) | 673 (29.5) | 1254 (31.5) | ||||
| University or above | 35 (56.5) | 32 (71.1) | 202 (53.3) | 1404 (61.5) | 2373 (59.6) | ||||
| Diabetes status | <0.001 | <0.001 | <0.001 | <0.001 | |||||
| No DM | 161 (75.2) | 103 (64.4) | 613 (60.4) | 3259 (60.9) | 6981 (76.5) | ||||
| GDM | 43 (20.1) | 48 (30) | 348 (34.3) | 1829 (34.2) | 2099 (23) | ||||
| PGDM | 10 (4.7) | 9 (5.6) | 54 (5.3) | 260 (4.9) | 48 (0.5) | ||||
| Chronic hypertension | <0.001 | <0.001 | <0.001 | <0.001 | |||||
| No | 205 (95.8) | 149 (93.1) | 982 (96.7) | 5243 (98) | 9078 (99.5) | ||||
| Yes | 9 (4.2) | 11 (6.9) | 33 (3.3) | 105 (2) | 50 (0.5) | ||||
| PP obesity | <0.05 | 0.529 | <0.001 | <0.001 | |||||
| No | 43 (58.9) | 33 (67.3) | 262 (62.7) | 1403 (63.4) | 2369 (71.4) | ||||
| Yes | 30 (41.1) | 16 (32.7) | 156 (37.3) | 811 (36.6) | 947 (28.6) | ||||
| Baby gender | <0.01 | <0.05 | <0.001 | <0.001 | |||||
| Male | 125 (58.4) | 95 (59.4) | 557 (54.9) | 2843 (53.2) | 4482 (49.1) | ||||
| Female | 89 (41.6) | 65 (40.6) | 457 (45) | 2503 (46.8) | 4646 (50.9) | ||||
| Ambiguous | 0 (0) | 0 (0) | 1 (0.1) | 1 (0) | 0 (0) | ||||
| Chromosomal/congenital abnormality | <0.001 | <0.001 | <0.001 | <0.05 | |||||
| No | 185 (86.4) | 148 (92.5) | 968 (95.4) | 5271 (98.6) | 9032 (98.9) | ||||
| Yes | 29 (13.6) | 12 (7.5) | 47 (4.6) | 77 (1.4) | 96 (1.1) | ||||
| Smoking | <0.05 | 0.308 | 0.452 | 0.862 | |||||
| No | 148 (97.4) | 120 (98.4) | 745 (98.9) | 4117 (99.2) | 6932 (99.2) | ||||
| Yes | 4 (2.6) | 2 (1.6) | 8 (1.1) | 32 (0.8) | 56 (0.8) | ||||
| Preterm history | <0.001 | <0.001 | <0.001 | <0.001 | |||||
| No | 172 (80.4) | 130 (81.3) | 860 (84.7) | 4895 (91.5) | 8758 (95.9) | ||||
| Yes | 42 (19.6) | 30 (18.8) | 155 (15.3) | 453 (8.5) | 370 (4.1) | ||||
| Employment status | 0.477 | 0.346 | 0.357 | 0.151 | |||||
| Employed | 54 (100) | 42 (97.7) | 344 (98.6) | 2159 (98.7) | 3737 (99.1) | ||||
| Unemployed | 0 (0) | 1 (2.3) | 5 (1.4) | 29 (1.3) | 35 (0.9) | ||||
| Birth weight | <0.001 | <0.001 | <0.001 | <0.001 | |||||
| ≤2499 g | 210 (98.6) | 148 (92.5) | 432 (42.6) | 375 (7) | 127 (1.4) | ||||
| ≥2500 g | 3 (1.4) | 12 (7.5) | 583 (57.4) | 4972 (93) | 8996 (98.6) | ||||
| Fetal weight by GA | <0.001 | <0.001 | <0.001 | <0.001 | |||||
| AGA | 120 (56.3) | 96 (60) | 682 (67.2) | 4126 (77.2) | 6453 (81.6) | ||||
| SGA | 41 (19.2) | 28 (17.5) | 112 (11) | 250 (4.7) | 451 (5.7) | ||||
| LGA | 52 (24.4) | 36 (22.5) | 221 (21.8) | 971 (18.2) | 1002 (12.7) | ||||
| Pregnancy mode | <0.001 | <0.01 | <0.001 | <0.001 | |||||
| Spontaneous | 202 (94.4) | 150 (94.3) | 961 (95.1) | 5159 (97) | 8906 (98.1) | ||||
| Assisted | 12 (5.6) | 9 (5.7) | 49 (4.9) | 157 (3) | 169 (1.9) | ||||
| Delivery mode | <0.001 | <0.001 | <0.001 | <0.001 | |||||
| Vaginal | 77 (36) | 63 (39.4) | 502 (49.5) | 3236 (60.5) | 7169 (78.5) | ||||
| Caesarean | 137 (64) | 97 (60.6) | 513 (50.5) | 2112 (39.5) | 1959 (21.5) | ||||
| Apgar < 7 at 1 min | <0.001 | <0.001 | <0.001 | <0.05 | |||||
| No | 112 (53.1) | 137 (87.3) | 956 (94.5) | 5280 (99) | 8975 (98.6) | ||||
| Yes | 99 (46.9) | 20 (12.7) | 56 (5.5) | 56 (1) | 131 (1.4) | ||||
| Apgar < 7 at 5 min | <0.001 | <0.001 | <0.001 | 0.251 | |||||
| No | 196 (92.9) | 154 (98.1) | 1003 (99) | 5328 (99.8) | 9102 (99.9) | ||||
| Yes | 15 (7.1) | 3 (1.9) | 10 (1) | 9 (0.2) | 9 (0.1) | ||||
| Baby outcome | <0.001 | <0.001 | <0.001 | 0.052 | |||||
| Discharged alive | 190 (88.8) | 153 (95.6) | 1002 (98.7) | 5335 (99.8) | 9118 (99.9) | ||||
| In-hospital mortality | 24 (11.2) | 7 (4.4) | 13 (1.3) | 13 (0.2) | 10 (0.1) | ||||
| Baby disposition | <0.001 | <0.001 | <0.001 | <0.001 | |||||
| Postnatal ward | 1 (0.5) | 8 (5) | 640 (63.1) | 4853 (90.8) | 8528 (93.4) | ||||
| NICU or death in LR/OT | 213 (99.5) | 152 (95) | 375 (36.9) | 494 (9.2) | 600 (6.6) | ||||
| Risk Factors | Extreme to Very PTB (n = 214) | Moderate PTB (n = 160) | Late PTB (n = 1015) | ETB (n = 5348) |
|---|---|---|---|---|
| aOR a (95% CI) | aOR b (95% CI) | aOR c (95% CI) | aOR d (95% CI) | |
| Maternal age | ||||
| Normal (20–34 yr) | ref | ref | ref | ref |
| Young (<20 yr) | 0.96 (0.34–2.72) | 2.76 (1.26–6.07) ‡ | 1.01 (0.48–2.13) | 1.02 (0.8–1.31) |
| Advanced (35–39 yr) | 1.81 (1.15–2.83) ‡ | 1.48 (0.98–2.23) | 1.39 (1.05–1.86) ‡ | 1.18 (1.07–1.31) * |
| Very advanced (40–44 yr) | 2.39 (1.12–5.11) ‡ | 1.77 (0.87–3.63) | 1.57 (0.91–2.71) | 1.53 (1.28–1.82) * |
| Extremely advanced (≥45 yr) | NA | 1.64 (0.16–16.9) | 4.97 (0.79–31.38) | 2.36 (1.18–4.71) ‡ |
| Parity | ||||
| Nulliparous | ref | ref | ||
| Parity ≥ 1 | 0.34 (0.23–0.51) * | 1.21 (1.11–1.32) * | ||
| Nationality | ||||
| Qataris | 0.78 (0.51–1.2) | 0.87 (0.59–1.28) | 0.8 (0.61–1.05) | 0.99 (0.9–1.08) |
| Other Arabs | 0.73 (0.48–1.09) | 0.6 (0.4–0.89) ‡ | 0.64 (0.49–0.83) * | 0.89 (0.81–0.96) † |
| Other Nationalities | ref | ref | ref | ref |
| Education | ||||
| Elementary and below | 1.46 (1.02–2.08) ‡ | |||
| Secondary/Highschool | 1.25 (0.98–1.59) | |||
| University or above | ref | |||
| Diabetes status | ||||
| No DM | ref | ref | ref | ref |
| GDM | 0.88 (0.58–1.33) | 1.47 (1.03–2.1) ‡ | 1.61 (1.27–2.05) * | 1.8 (1.67–1.94) * |
| PGDM | 7.37 (2.97–18.31) * | 5.03 (2.08–12.17) * | 6.55 (3.17–13.52) * | 9.72 (7.07–13.35) * |
| Chronic hypertension | ||||
| No | ref | ref | ref | ref |
| Yes | 2.97 (0.96–9.18) | 6.5 (2.92–14.46) * | 1.14 (0.37–3.49) | 2.39 (1.67–3.43) * |
| Baby gender | ||||
| Female | ref | ref | ref | ref |
| Male | 1.39 (0.99–1.95) | 1.46 (1.06–2.03) ‡ | 1.12 (0.9–1.39) | 1.2 (1.11–1.28) * |
| Chromosomal/Congenital abnormalities | ||||
| No | ref | ref | ref | ref |
| Yes | 15.52 (8.91–27.02) * | 7.9 (4.14–15.04) * | 3.9 (1.97–7.7) * | 1.26 (0.92–1.72) |
| Smoking | ||||
| No | ref | |||
| Yes | 3.01 (0.99–9.13) | |||
| Preterm history | ||||
| No | ref | ref | ref | ref |
| Yes | 7.23 (4.44–11.77) * | 4.7 (3.04–7.28) * | 3.5 (2.48–4.94) * | 1.95 (1.68–2.26) * |
| Pregnancy mode | ||||
| Spontanious pregnancy | ref | ref | ref | ref |
| Assisted pregnancy | 2.49 (1.19–5.21) ‡ | 2.82 (1.38–5.79) † | 3.11 (1.9–5.08) * | 1.61 (1.28–2.02) * |
| LBW | SGA | LGA | Caesarean Delivery | Apgar < 7 at 1 Min | Apgar < 7 at 5 Min | In-Hospital Mortality | NICU/Death in LR/OT | |
|---|---|---|---|---|---|---|---|---|
| aOR (95%CI) | aOR (95%CI) | aOR (95%CI) | aOR (95%CI) | aOR (95%CI) | aOR (95%CI) | aOR (95%CI) | aOR (95%CI) | |
| Extreme to very PTB a | 5669.36 (1317.88–24,388.98) * | 4.11 (2.55–6.64) * | 3.8 (2.5–5.79) * | 5.26 (3.71–7.47) * | 52.3 (33.89–80.71) * | 69.2 (20.54–233.09) * | 84.73 (28.87–248.69) * | 2417.24 (332.79–17,557.67) * |
| Moderate PTB b | 1021.64 (520.79–2004.19) * | 3.78 (2.38–6.00) * | 2.44 (1.63–3.64) * | 4.54 (3.26–6.34) * | 7.73 (4.43–13.50) * | 9.81 (2.01–47.91) † | 27.76 (7.52–102.48) * | 274.38 (132.59–567.78) * |
| Late PTB c | 57.41 (40.1–82.19) * | 1.9 (1.28–2.82) * | 1.87 (1.39–2.5) * | 2.47 (1.96–3.12) * | 1.64 (0.73–3.69) | NA | NA | 8.48 (6.37–11.28) * |
| ETB d | 5.96 (4.83–7.35) * | 0.9 (0.77–1.07) | 1.37 (1.24–1.52) * | 2.14 (1.98–2.32) * | 0.71 (0.51–0.99) ‡ | 1.2 (0.45–3.19) | 2.11 (0.84–5.32) | 1.31 (1.15–1.51) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Younes, S.; Samara, M.; Al-Jurf, R.; Nasrallah, G.; Al-Obaidly, S.; Salama, H.; Olukade, T.; Hammuda, S.; Ismail, M.A.; Abdoh, G.; et al. Incidence, Risk Factors, and Outcomes of Preterm and Early Term Births: A Population-Based Register Study. Int. J. Environ. Res. Public Health 2021, 18, 5865. https://doi.org/10.3390/ijerph18115865
Younes S, Samara M, Al-Jurf R, Nasrallah G, Al-Obaidly S, Salama H, Olukade T, Hammuda S, Ismail MA, Abdoh G, et al. Incidence, Risk Factors, and Outcomes of Preterm and Early Term Births: A Population-Based Register Study. International Journal of Environmental Research and Public Health. 2021; 18(11):5865. https://doi.org/10.3390/ijerph18115865
Chicago/Turabian StyleYounes, Salma, Muthanna Samara, Rana Al-Jurf, Gheyath Nasrallah, Sawsan Al-Obaidly, Husam Salama, Tawa Olukade, Sara Hammuda, Mohamed A. Ismail, Ghassan Abdoh, and et al. 2021. "Incidence, Risk Factors, and Outcomes of Preterm and Early Term Births: A Population-Based Register Study" International Journal of Environmental Research and Public Health 18, no. 11: 5865. https://doi.org/10.3390/ijerph18115865