
Polydisperse Aerosol Transport and Deposition in Upper Airways of Age-Specific Lung

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Methods
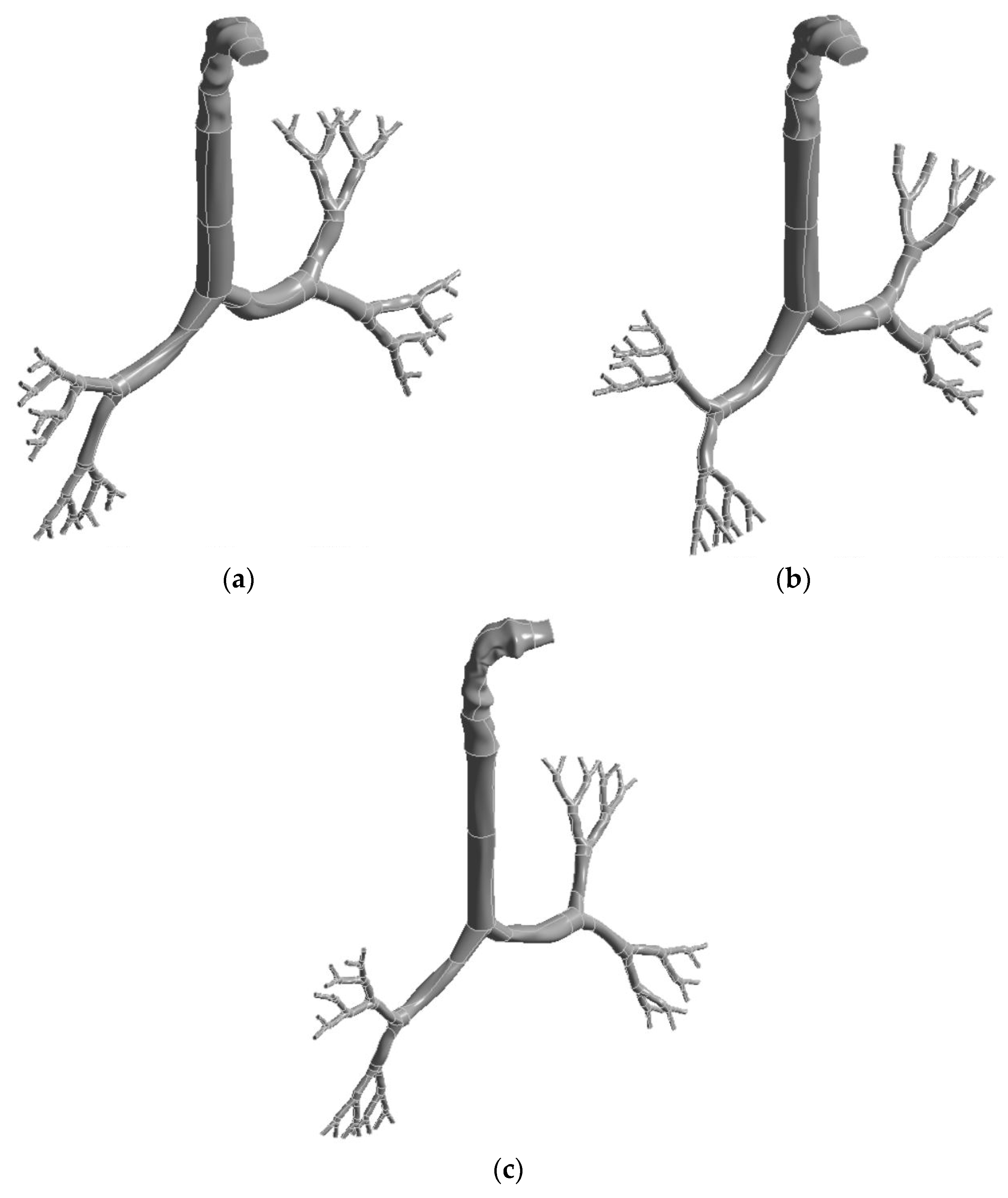
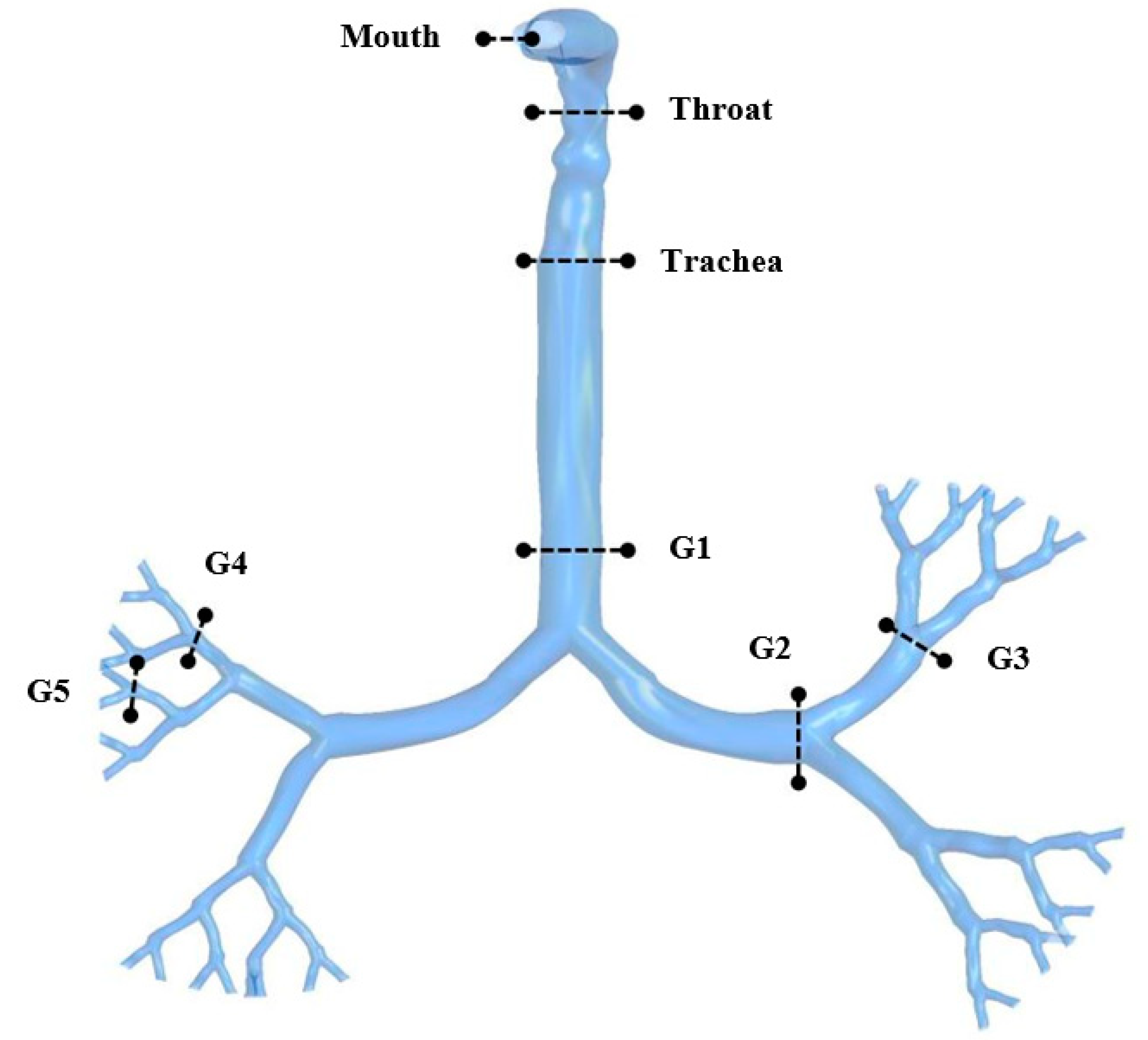
2.1. Geometrical Development
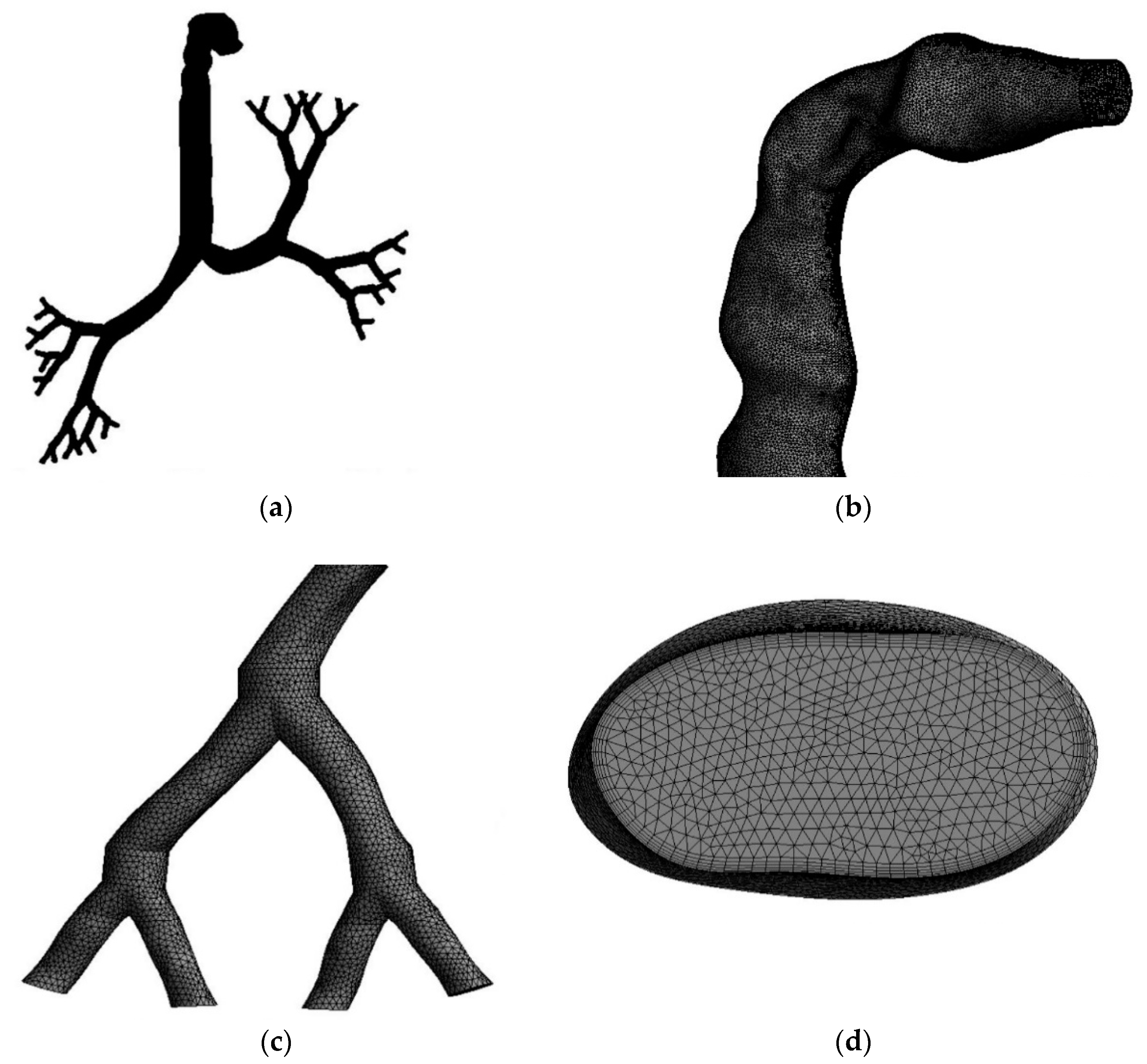
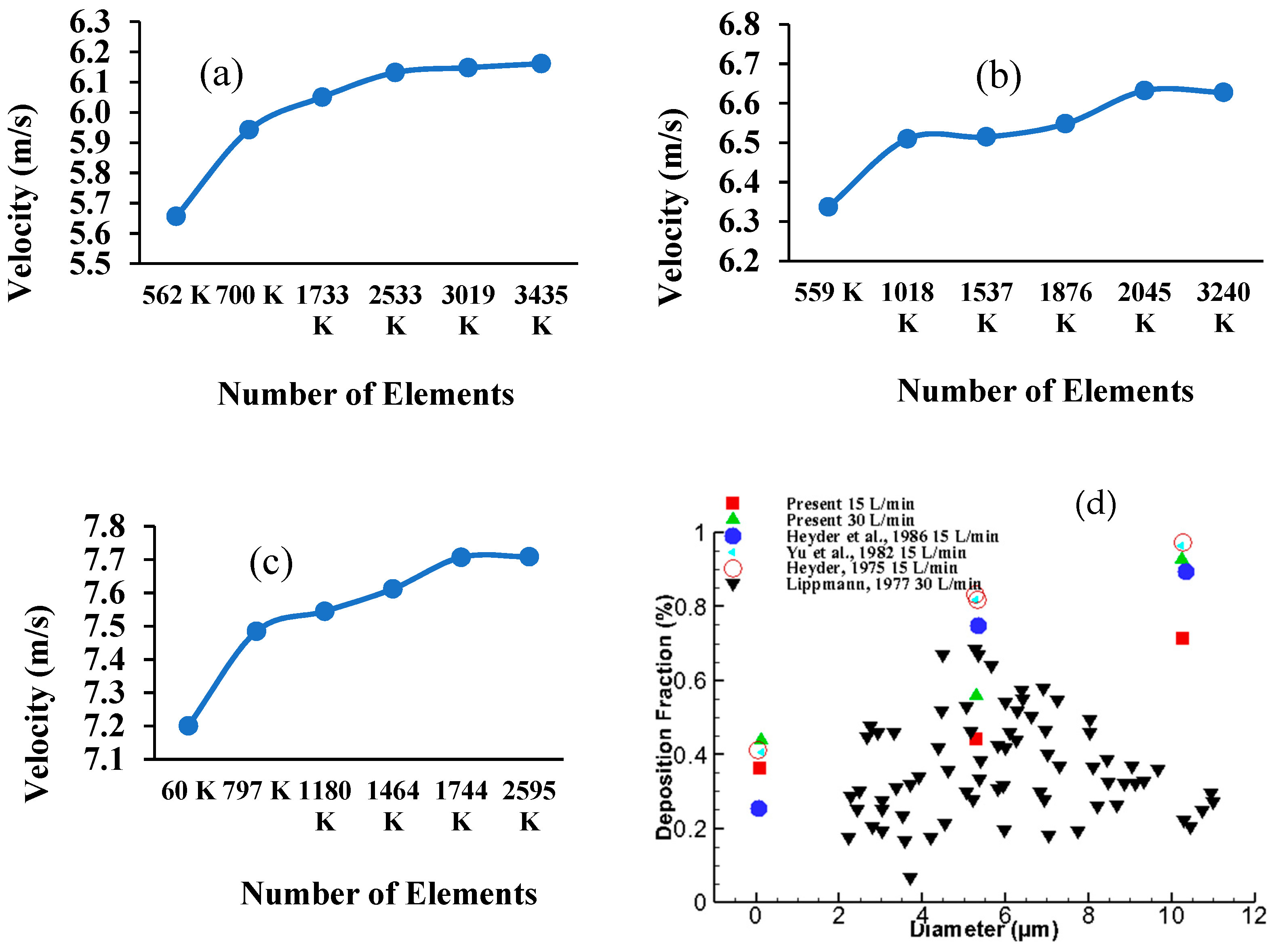
2.2. Grid Generation and Model Validation
2.3. Numerical Methods
3. Results
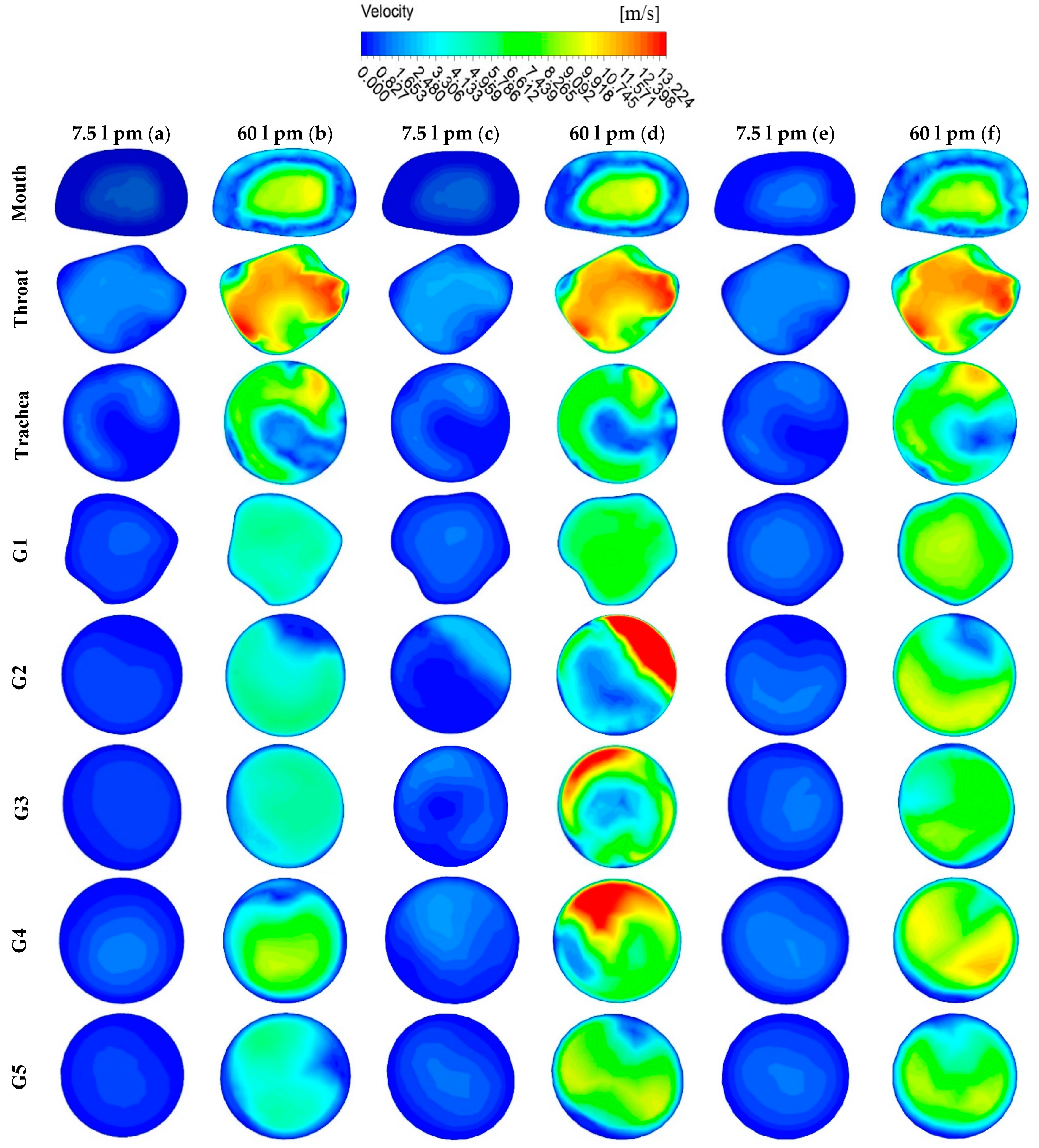
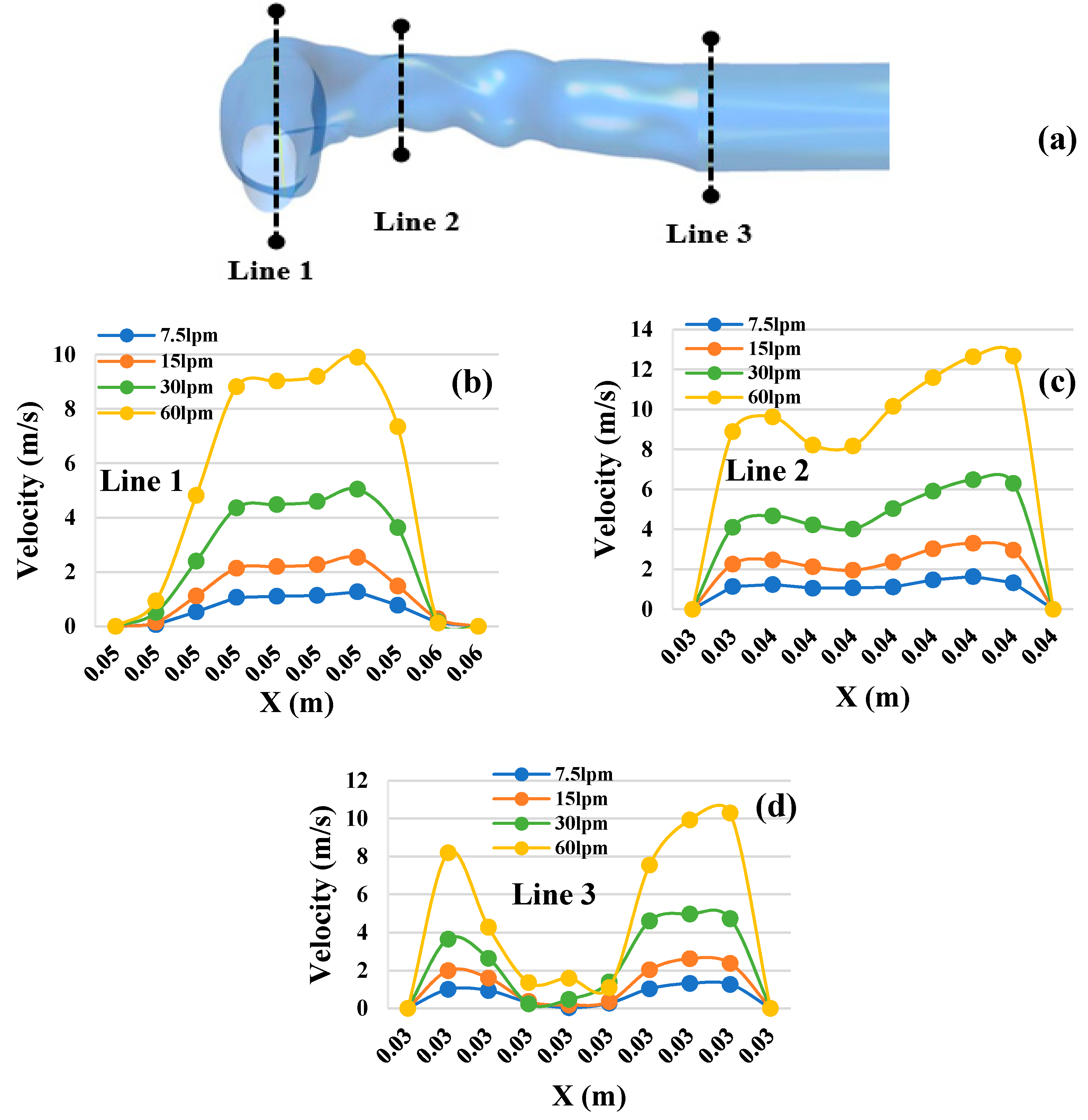
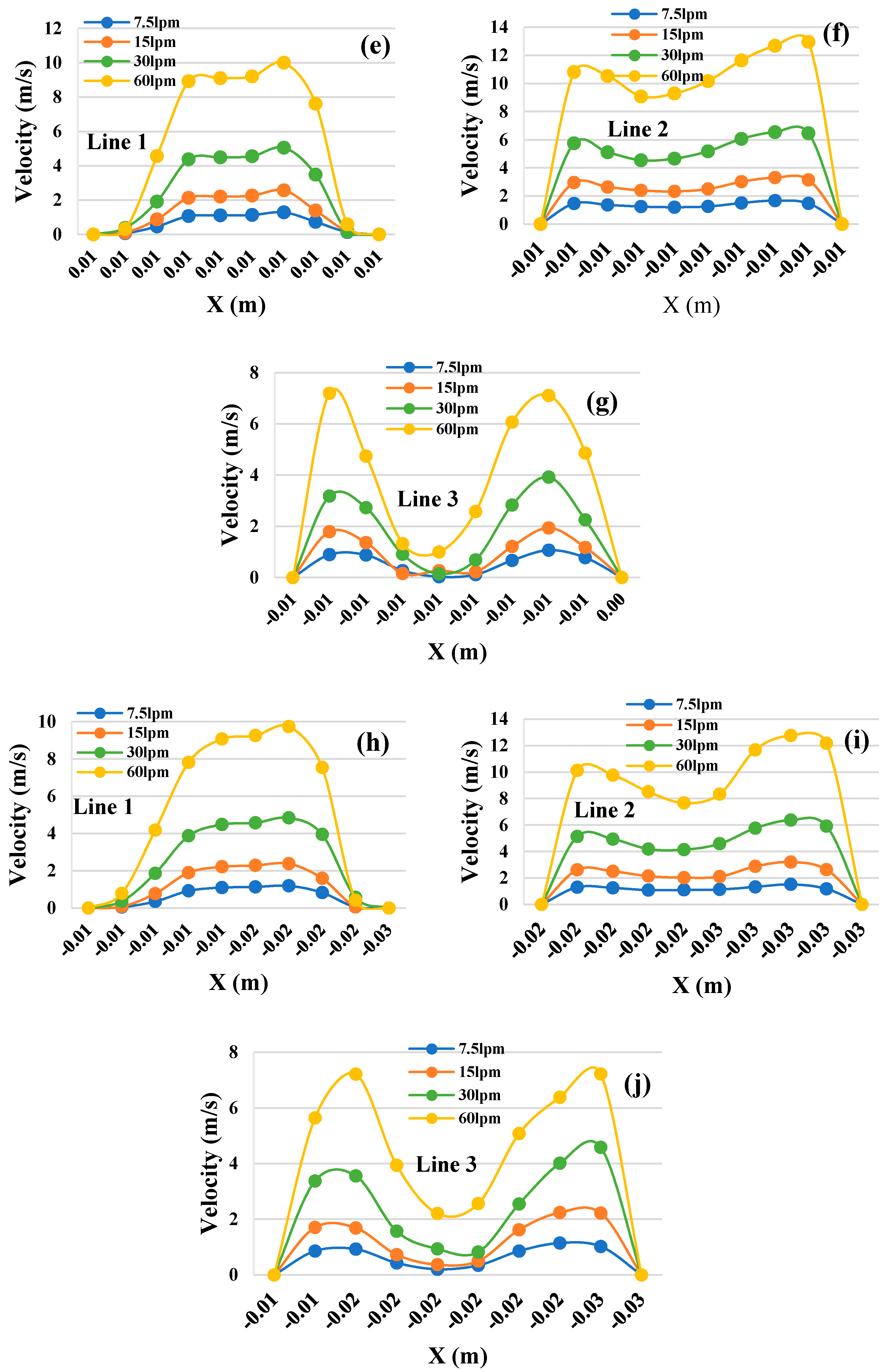
3.1. Velocity Contours
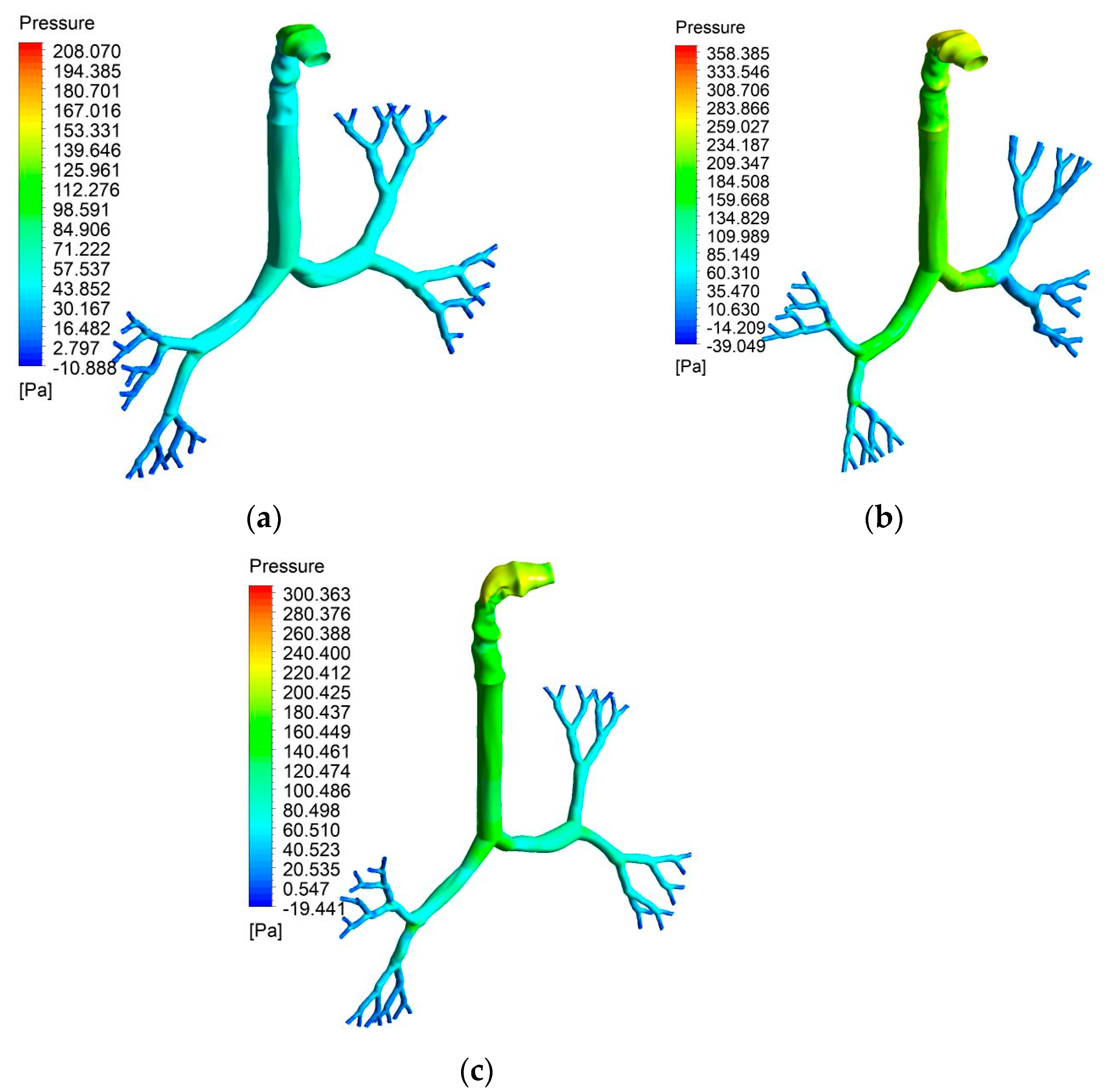
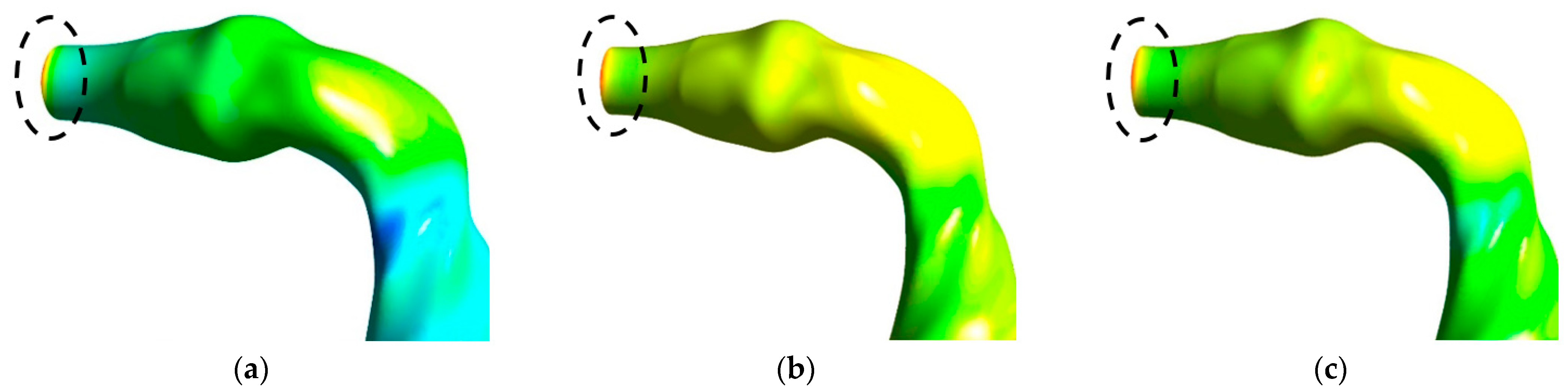
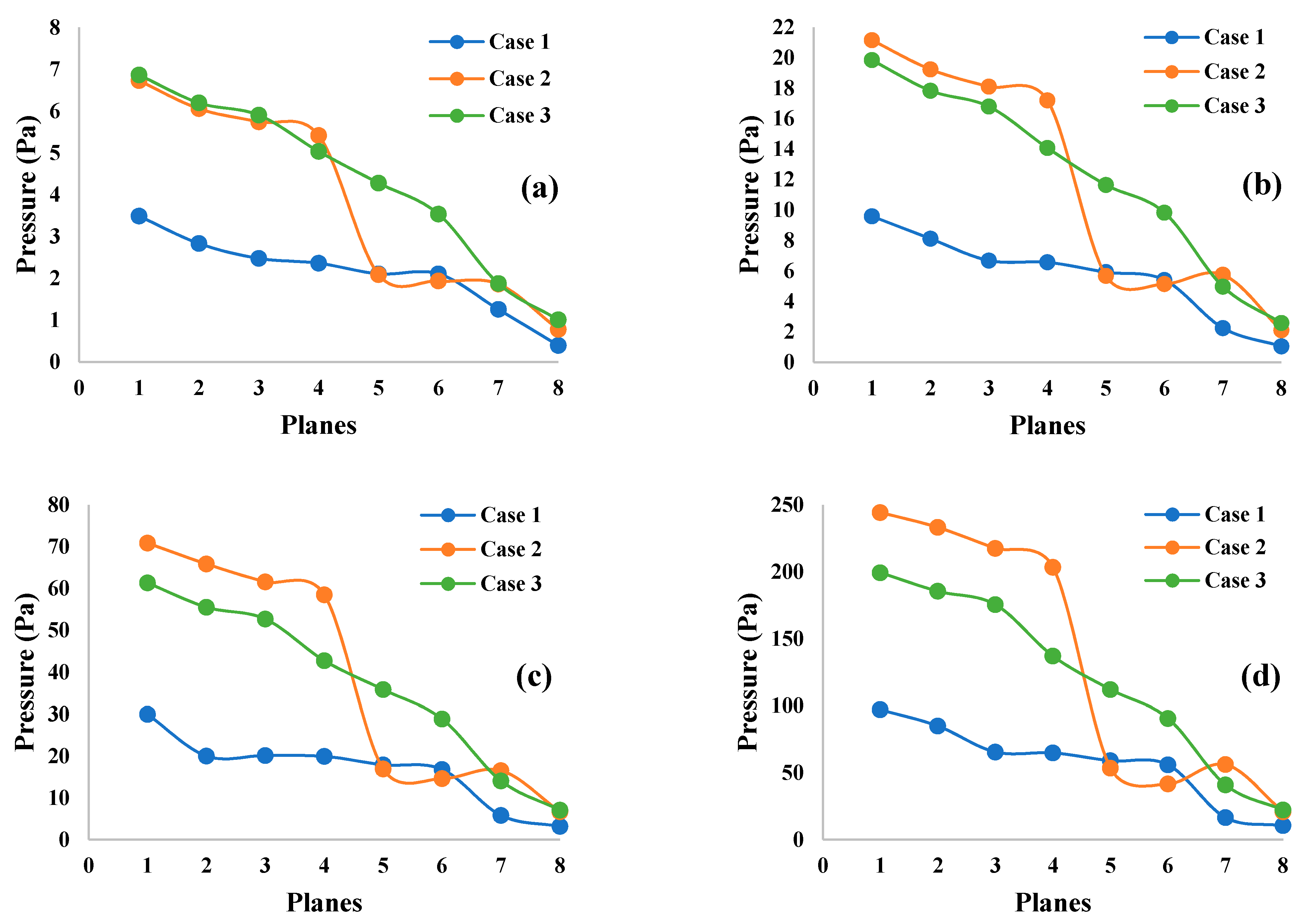
3.2. Pressure Contours
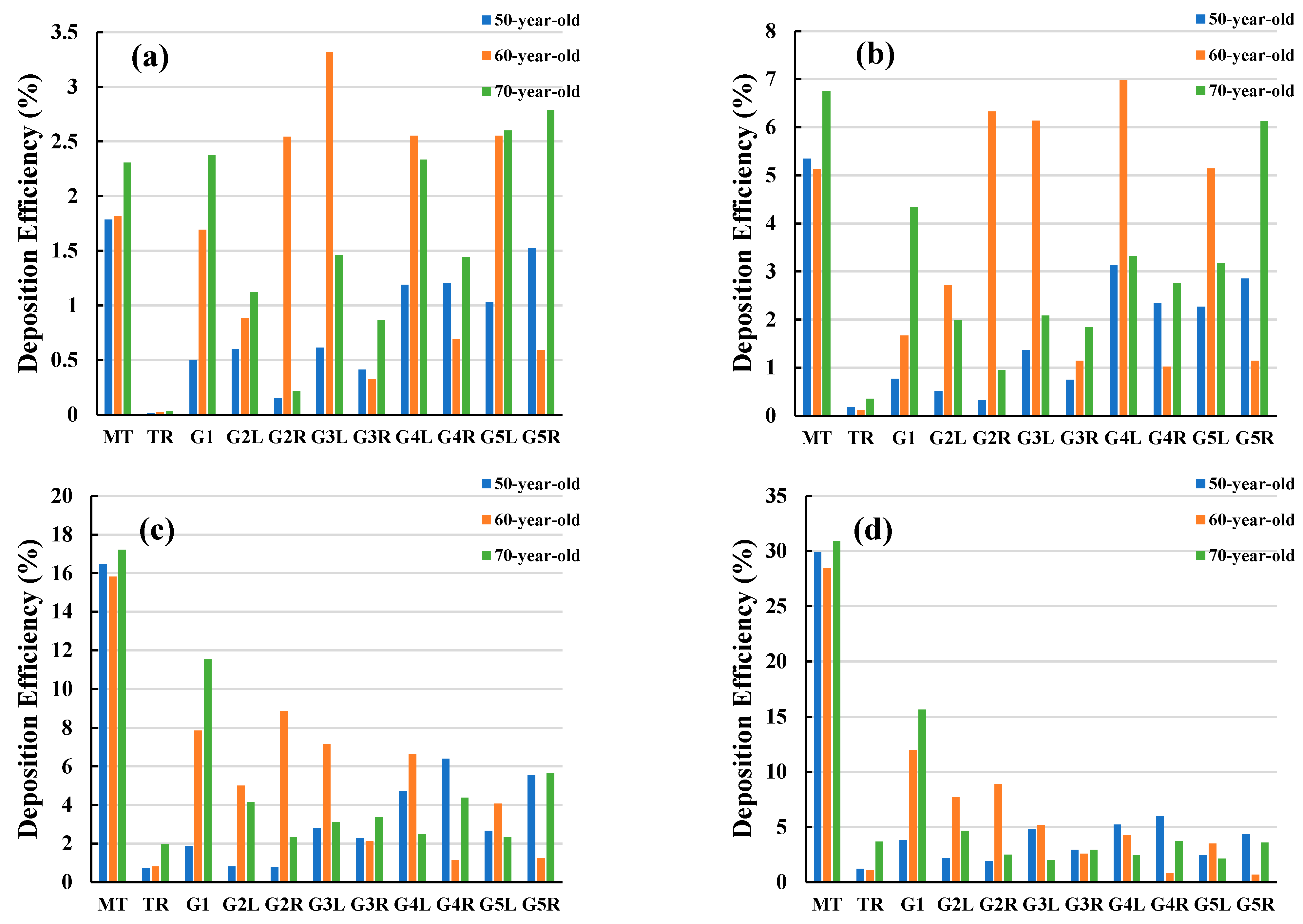
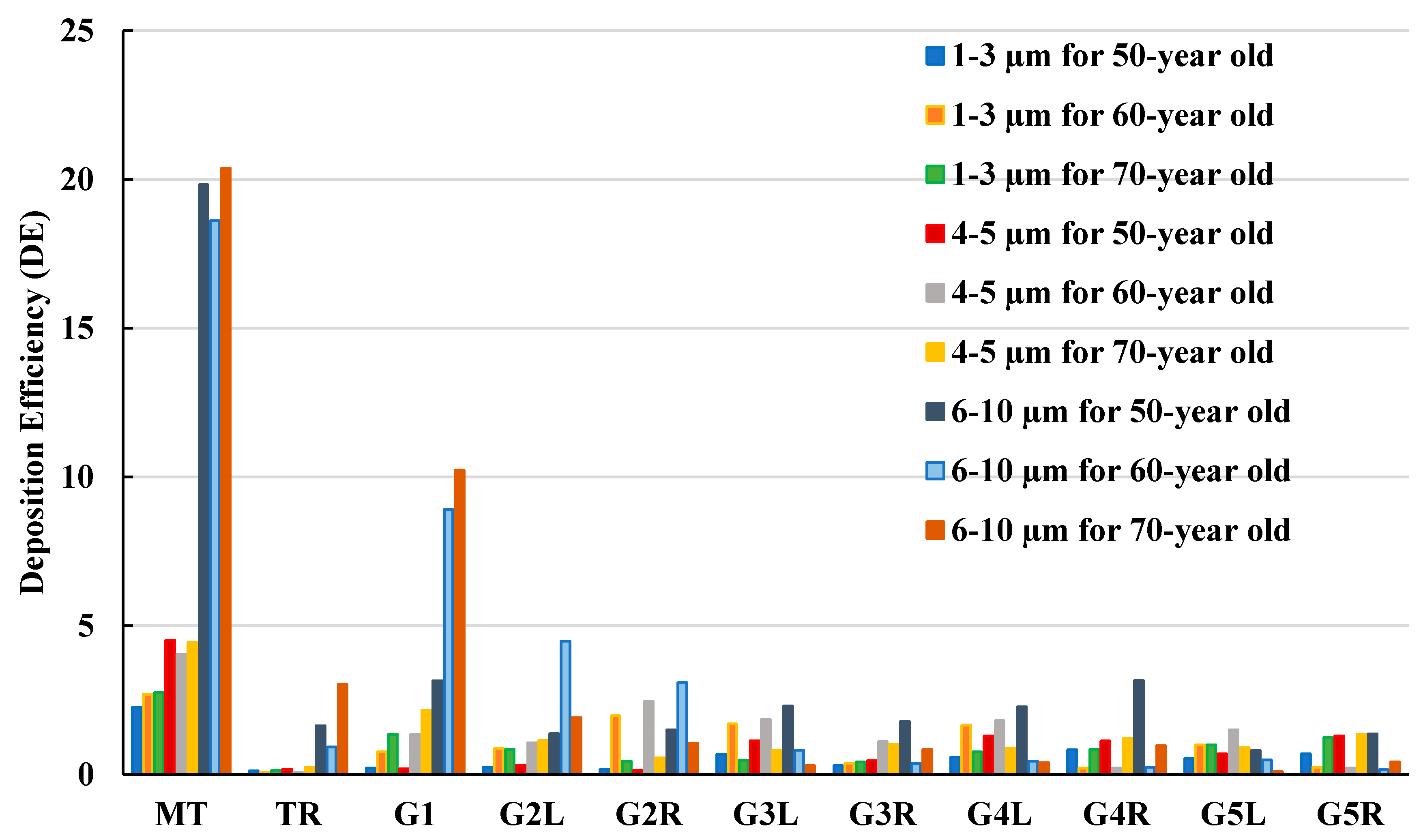
3.3. Particle Deposition Efficiency
4. Discussion
5. Conclusions
Limitations of the Study
- This study focused on airflow and particle transport in human lungs for an inhalation scenario;
- The model used only a small number of lung generations, where the end of generation 5 was set to be the outlet;
- The airway size for elderly patient-specific lung can increase, and this study did not consider this effect;
- The upper lobe was not considered for the airway model to make the similar geometry for all cases and minimise the reconstruction complexity;
- This study did not consider any dynamic wall motion or airway deformation;
- Open outlet conditions and constant pressure were used at the outlets.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Islam, M.S.; Saha, S.C.; Sauret, E.; Gemci, T.; Yang, I.A.; Gu, Y. Ultrafine particle transport and deposition in a large scale 17-generation lung model. J. Biomech. 2017, 64, 16–25. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Li, C.; Ristovski, Z.; Milic, A.; Gu, Y.; Islam, M.S.; Wang, S.; Hao, J.; Zhang, H.; He, C. A review of biomass burning: Emissions and impacts on air quality, health and climate in China. Sci. Total Environ. 2017, 579, 1000–1034. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Hu, D.; Chen, J.; Ye, X.; Wang, S.X.; Hao, J.M.; Wang, L.; Zhang, R.; An, Z. Particle size distribution and polycyclic aromatic hydrocarbons emissions from agricultural crop residue burning. J. Environ. Sci. 2011, 45, 5477–5482. [Google Scholar] [CrossRef]
- ACGIH. 2005 TLVs and BEIs: Based on the Documentation of the Threshold Limit Values for Chemical Substances and Physical Agents & Biological Exposure Indices; American Conference of Governmental Industrial Hygienists: Cincinnati, OH, USA, 2005. [Google Scholar]
- Islam, M.S.; Saha, S.C.; Sauret, E.; Ong, H.; Young, P.; Gu, Y. Euler–Lagrange approach to investigate respiratory anatomical shape effects on aerosol particle transport and deposition. J. Toxicol. Res. 2019, 3, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Hu, L.-W.; Qian, Z.M.; Chang, J.-J.; King, C.; Paul, G.; Lin, S.; Chen, P.-C.; Lee, Y.L.; Dong, G.-H. Association of perfluoroalkyl substances exposure with reproductive hormone levels in adolescents: By sex status. J. Environ. Int. 2016, 94, 189–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, M.; Slezakova, K.; Delerue-Matos, C.; Pereira, M.C.; Morais, S. Children environmental exposure to particulate matter and polycyclic aromatic hydrocarbons and biomonitoring in school environments: A review on indoor and outdoor exposure levels, major sources and health impacts. J. Environ. Int. 2019, 124, 180–204. [Google Scholar] [CrossRef]
- Gehring, U.; Koppelman, H.G. Improvements in air quality: Whose lungs benefit? Eur. Respir. Soc. 2019, 53, 1900365. [Google Scholar] [CrossRef]
- Gehr, P.; Heyder, J. Particle-Lung Interactions; CRC Press: Boca Raton, FL, USA, 2000. [Google Scholar]
- Diat-Sanchez, D. The role of diesel exhaust particles and their associated polyaromatic hydrocarbons in the induction of allergic airway disease. Allergy 1997, 52, 52–56. [Google Scholar] [CrossRef]
- Gu, Q.; Qi, S.; Yue, Y.; Shen, J.; Zhang, B.; Sun, W.; Qian, W.; Islam, M.S.; Saha, S.C.; Wu, J. Structural and functional alterations of the tracheobronchial tree after left upper pulmonary lobectomy for lung cancer. Biomed. Eng. Online 2019, 18, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Saha, S.; Islam, M.; Rahimi-Gorji, M.; Molla, M. Aerosol Particle Transport and Deposition in a CT-Scan Based Mouth-Throat Model. In AIP Conference Proceedings; AIP Publishing: Melville, NY, USA, 2019. [Google Scholar]
- Yousefi, M.; Pourmehran, O.; Gorji-Bandpy, M.; Inthavong, K.; Yeo, L.; Tu, J. CFD simulation of aerosol delivery to a human lung via surface acoustic wave nebulization. Biomech. Modeling Mechanobiol. 2017, 16, 2035–2050. [Google Scholar] [CrossRef]
- Ghosh, A.; Islam, M.S.; Saha, S.C. Targeted drug delivery of magnetic nano-particle in the specific lung region. Computation 2020, 8, 10. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.S.; Gu, Y.; Farkas, A.; Paul, G.; Saha, S.C. Helium–Oxygen Mixture Model for Particle Transport in CT-Based Upper Airways. Int. J. Environ. Res. Public Health 2020, 17, 3574. [Google Scholar] [CrossRef]
- Xu, G.; Yu, C. Effects of age on deposition of inhaled aerosols in the human lung. Aerosol Sci. Technol. 1986, 5, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Hendryx, M.; Islam, M.S.; Dong, G.-H.; Paul, G. Air pollution emissions 2008–2018 from australian coal mining: Implications for public and occupational health. Int. J. Environ. Res. Public Health 2020, 17, 1570. [Google Scholar] [CrossRef] [Green Version]
- Thurlbeck, W.M. Postnatal growth and development of the lung. Am. Rev. Respir. Dis. 1975, 111, 803–844. [Google Scholar]
- Horsfield, K.; Gordon, W.; Kemp, W.; Phillips, S. Growth of the bronchial tree in man. Thorax 1987, 42, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Storey-Bishoff, J.; Noga, M.; Finlay, W. Deposition of micrometer-sized aerosol particles in infant nasal airway replicas. J. Aerosol Sci. 2008, 39, 1055–1065. [Google Scholar] [CrossRef]
- Janssens, H.M.; de Jongste, J.C.; Fokkens, W.J.; Robben, S.G.; Wouters, K.; Tiddens, H.A. The Sophia Anatomical Infant Nose-Throat (Saint) model: A valuable tool to study aerosol deposition in infants. J. Aerosol Med. 2001, 14, 433–441. [Google Scholar] [CrossRef]
- Cheng, Y.-S.; Smith, S.M.; Yeh, H.-C.; Kim, D.-B.; Cheng, K.-H.; Swift, D.L. Deposition of ultrafine aerosols and thoron progeny in replicas of nasal airways of young children. Aerosol Sci. Technol. 1995, 23, 541–552. [Google Scholar] [CrossRef]
- Swift, D. Inspiratory inertial deposition of aerosols in human nasal airway replicate casts: Implication for the proposed NCRP lung model. Radiat. Prot. Dosim. 1991, 38, 29–34. [Google Scholar] [CrossRef]
- Cheng, K.-H.; Cheng, Y.-S.; Yeh, H.-C.; Swift, D. Measurements of airway dimensions and calculation of mass transfer characteristics of the human oral passage. J. Biomech. Eng. 1997, 119, 479–482. [Google Scholar] [CrossRef]
- Grgic, B.; Finlay, W.H.; Burnell, P.; Heenan, A. In vitro intersubject and intrasubject deposition measurements in realistic mouth–throat geometries. J. Aerosol Sci. 2004, 35, 1025–1040. [Google Scholar] [CrossRef]
- Koullapis, P.; Nicolaou, L.; Kassinos, S.C. In silico assessment of mouth-throat effects on regional deposition in the upper tracheobronchial airways. J. Aerosol Sci. 2018, 117, 164–188. [Google Scholar] [CrossRef]
- Nicolaou, L.; Zaki, T. Direct numerical simulations of flow in realistic mouth–throat geometries. J. Aerosol Sci. 2013, 57, 71–87. [Google Scholar] [CrossRef] [Green Version]
- Hofmann, W. Dose calculations for the respiratory tract from inhaled natural radioactive nuclides as a function of age--II. Basal cell dose distributions and associated lung cancer risk. Health Phys. 1982, 43, 31–44. [Google Scholar] [CrossRef]
- Islam, M.S.; Saha, S.; Sauret, E.; Gu, Y.; Ristovski, Z. Numerical investigation of aerosol particle transport and deposition in realistic lung airway. In Proceedings of the 6th International Conference on Computational Methods, Auckland, New Zealand, 14–17 July 2015; Volume 2. [Google Scholar]
- Islam, M.S.; Saha, S.C.; Gemci, T.; Yang, I.A.; Sauret, E.; Gu, Y. Polydisperse microparticle transport and deposition to the terminal bronchioles in a heterogeneous vasculature tree. Sci. Rep. 2018, 8, 1–9. [Google Scholar]
- Islam, M.S.; Saha, S.C.; Gemci, T.; Yang, I.A.; Sauret, E.; Ristovski, Z.; Gu, Y. Euler-Lagrange prediction of Diesel-exhaust polydisperse particle transport and Deposition in Lung: Anatomy and turbulence Effects. Sci. Rep. 2019, 9, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.S.; Saha, S.C.; Sauret, E.; Gemci, T.; Gu, Y. Pulmonary aerosol transport and deposition analysis in upper 17 generations of the human respiratory tract. J. Aerosol Sci. 2017, 108, 29–43. [Google Scholar] [CrossRef] [Green Version]
- Oakes, J.M.; Roth, S.C.; Shadden, S.C. Airflow simulations in infant, child, and adult pulmonary conducting airways. Ann. Biomed. Eng. 2018, 46, 498–512. [Google Scholar] [CrossRef] [PubMed]
- Crawford, D. Identifying critical human subpopulations by age groups: Radioactivity and the lung. Phys. Med. Biol. 1982, 27, 539. [Google Scholar] [CrossRef]
- Hofmann, W.; Steinhausler, F.; Pohl, E. Dose Calculations For the Respiratory Tract From Inhaled Natural Radioactive Nuclides As a Function of Age-I: Compartmental Deposition, Retention and Resulting Dose. Health Phys. 1979, 37, 517–532. [Google Scholar] [CrossRef]
- Oldham, M.J.; Mannix, R.C.; Phalen, R.F. Deposition of monodisperse particles in hollow models representing adult and child-size tracheobronchial airways. Health Phys. 1997, 72, 827–834. [Google Scholar] [CrossRef] [Green Version]
- Phalen, R.F.; Oldham, M.J.; Beaucage, C.B.; Crocker, T.T.; Mortensen, J. Postnatal enlargement of human tracheobronchial airways and implications for particle deposition. Anat. Rec. 1985, 212, 368–380. [Google Scholar] [CrossRef] [Green Version]
- Schum, G.M.; Phalen, R.F.; Oldham, M.J. The effect of dead space on inhaled particle deposition. J. Aerosol Med. 1991, 4, 297–311. [Google Scholar] [CrossRef]
- Asgharian, B.; Menache, M.; Miller, F. Modeling age-related particle deposition in humans. J. Aerosol Med. 2004, 17, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Sturm, R. Bioaerosols in the lungs of subjects with different ages-part 1: Deposition modeling. Ann. Transl. Med. 2016, 4, 211. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Heise, R.L.; Reynolds, A.M.; Pidaparti, R.M. Aging effects on airflow dynamics and lung function in human bronchioles. PLoS ONE 2017, 12, e0183654. [Google Scholar] [CrossRef]
- Tsega, E.G. Computational fluid dynamics modeling of respiratory airflow in tracheobronchial airways of infant, child, and adult. Comput. Math. Methods Med. 2018, 2018, 9603451. [Google Scholar] [CrossRef]
- Bass, K.; Farkas, D.; Hassan, A.; Bonasera, S.; Hindle, M.; Longest, W. High-efficiency dry powder aerosol delivery to children: Review and application of new technologies. J. Aerosol Sci. 2020, 153, 105692. [Google Scholar] [CrossRef]
- Vinchurkar, S.; de Backer, L.; Vos, W.; van Holsbeke, C.; de Backer, J.; de Backer, W. A case series on lung deposition analysis of inhaled medication using functional imaging based computational fluid dynamics in asthmatic patients: Effect of upper airway morphology and comparison with in vivo data. Inhal. Toxicol. 2012, 24, 81–88. [Google Scholar] [CrossRef]
- Katan, J.T.; Hofemeier, P.; Sznitman, J. Computational models of inhalation therapy in early childhood: Therapeutic aerosols in the developing acinus. J. Aerosol Med. Pulm. Drug Deliv. 2016, 29, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; Ou, C.; Chen, J.; Xiang, Y. Particle deposition in tracheobronchial airways of an infant, child and adult. Sci. Total Environ. 2018, 612, 339–346. [Google Scholar] [CrossRef]
- Das, P.; Nof, E.; Amirav, I.; Kassinos, S.C.; Sznitman, J. Targeting inhaled aerosol delivery to upper airways in children: Insight from computational fluid dynamics (CFD). PLoS ONE 2018, 13, e0207711. [Google Scholar] [CrossRef]
- Manojkumar, N.; Srimuruganandam, B.; Nagendra, S.S. Application of multiple-path particle dosimetry model for quantifying age specified deposition of particulate matter in human airway. Ecotoxicol. Environ. Saf. 2019, 168, 241–248. [Google Scholar] [CrossRef]
- Haddrell, A.E.; Lewis, D.; Church, T.; Vehring, R.; Murnane, D.; Reid, J.P. Pulmonary aerosol delivery and the importance of growth dynamics. Ther. Deliv. 2017, 8, 1051–1061. [Google Scholar] [CrossRef] [Green Version]
- Niewoehner, D.E.; Kleinerman, J. Morphologic basis of pulmonary resistance in the human lung and effects of aging. J. Appl. Physiol. 1974, 36, 412–418. [Google Scholar] [CrossRef]
- Heyder, J.; Gebhart, J.; Rudolf, G.; Schiller, C.F.; Stahlhofen, W. Deposition of particles in the human respiratory tract in the size range 0.005–15 μm. J. Aerosol Sci. 1986, 17, 811–825. [Google Scholar] [CrossRef]
- Lippmann, M. Regional deposition of particles in the human respiratory tract. Compr. Physiol. 1977, 213–232. [Google Scholar]
- Yu, C.; Diu, C. A comparative study of aerosol deposition in different lung models. Am. Ind. Hyg. Assoc. J. 1982, 43, 54–65. [Google Scholar] [CrossRef]
- Heyder, J.; Armbruster, L.; Gebhart, J.; Grein, E.; Stahlhofen, W. Total deposition of aerosol particles in the human respiratory tract for nose and mouth breathing. J. Aerosol Sci. 1975, 6, 311–328. [Google Scholar] [CrossRef]
- Gemci, T.; Ponyavin, V.; Chen, Y.; Chen, H.; Collins, R. Computational model of airflow in upper 17 generations of human respiratory tract. J. Biomech. 2008, 41, 2047–2054. [Google Scholar] [CrossRef]
- Islam, M.S.; Paul, G.; Ong, H.X.; Young, P.M.; Gu, Y.; Saha, S.C. A Review of Respiratory Anatomical Development, Air Flow Characterization and Particle Deposition. Int. J. Environ. Res. Public Health 2020, 17, 380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loring, S.H.; Topulos, G.P.; Hubmayr, R.D. Transpulmonary pressure: The importance of precise definitions and limiting assumptions. Am. J. Respir. Crit. Care Med. 2016, 194, 1452–1457. [Google Scholar] [CrossRef]
- Kim, K.-H.; Kabir, E.; Kabir, S.J.E.I. A review on the human health impact of airborne particulate matter. Environ. Int. 2015, 74, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Maynard, R.L. The effects on health of ambient particles: Time for an agonizing reappraisal? J. Cell Biol. 2015, 31, 131–147. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Properties | Air | Aerosol |
|---|---|---|
| Density (kg/m3) | 1.225 | 1100 |
| Viscosity (kg/m-s) | 1.7893 × 105 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.S.; Larpruenrudee, P.; Hossain, S.I.; Rahimi-Gorji, M.; Gu, Y.; Saha, S.C.; Paul, G. Polydisperse Aerosol Transport and Deposition in Upper Airways of Age-Specific Lung. Int. J. Environ. Res. Public Health 2021, 18, 6239. https://doi.org/10.3390/ijerph18126239
Islam MS, Larpruenrudee P, Hossain SI, Rahimi-Gorji M, Gu Y, Saha SC, Paul G. Polydisperse Aerosol Transport and Deposition in Upper Airways of Age-Specific Lung. International Journal of Environmental Research and Public Health. 2021; 18(12):6239. https://doi.org/10.3390/ijerph18126239
Chicago/Turabian StyleIslam, Mohammad S., Puchanee Larpruenrudee, Sheikh I. Hossain, Mohammad Rahimi-Gorji, Yuantong Gu, Suvash C. Saha, and Gunther Paul. 2021. "Polydisperse Aerosol Transport and Deposition in Upper Airways of Age-Specific Lung" International Journal of Environmental Research and Public Health 18, no. 12: 6239. https://doi.org/10.3390/ijerph18126239