Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Degenerative Disc Disease
3. Prolapsed Intervertebral Disc
4. Clinical Findings
5. Natural History: Degenerative Cascade
6. Current Diagnostic Imaging
6.1. Role of Roentgenogram and Magnetic Resonance Imaging
6.2. Recent Developments in Diagnostic Tool Imaging
6.2.1. Contouring of Modic Changes
6.2.2. Assessment of Bone Marrow Lesion Composition
6.2.3. Diffusion Tensor Imaging
6.2.4. Multi-Detector Computed Tomography Scan
7. Development of Biomarkers
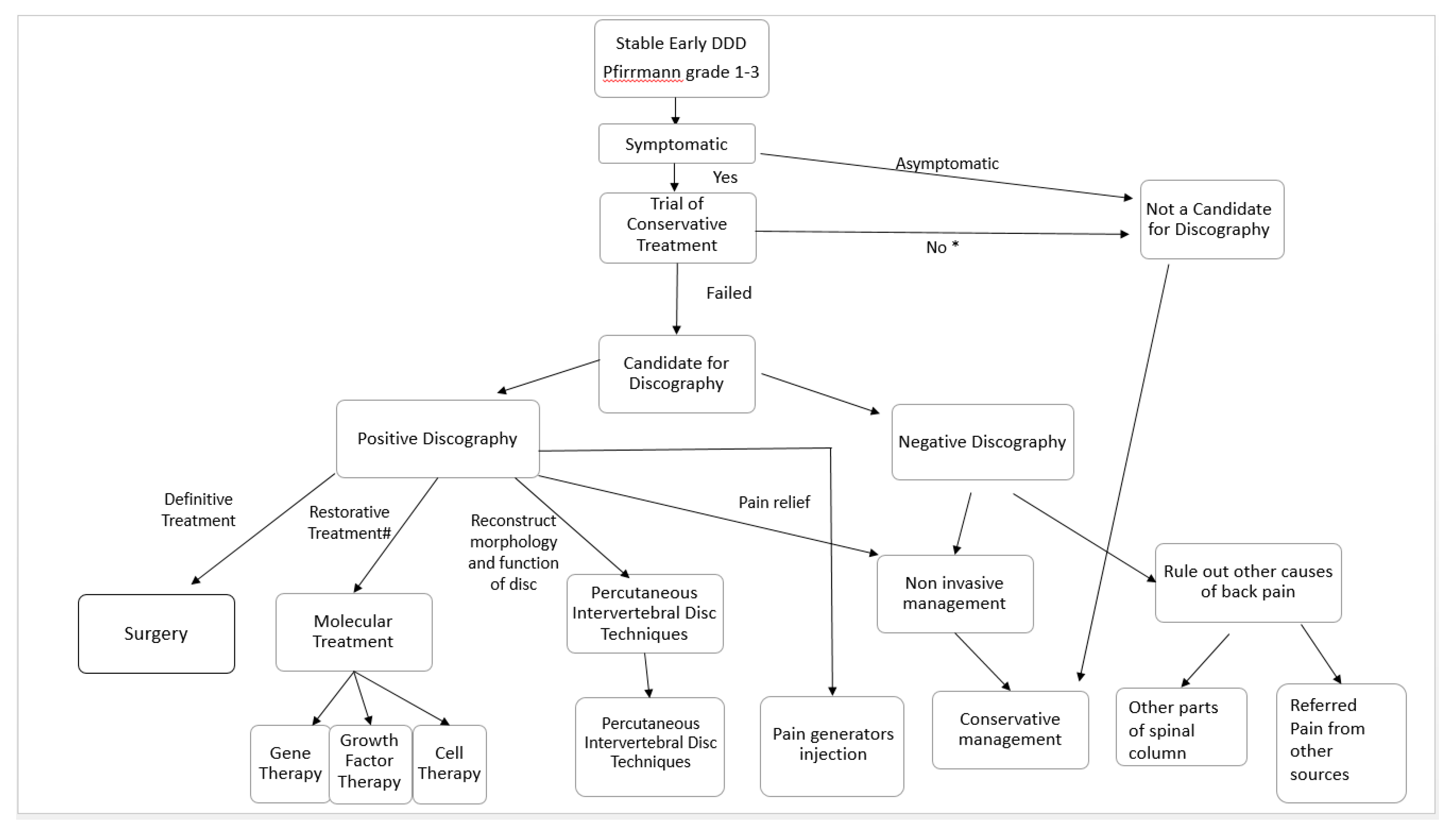
8. Standard Confirmatory Tests
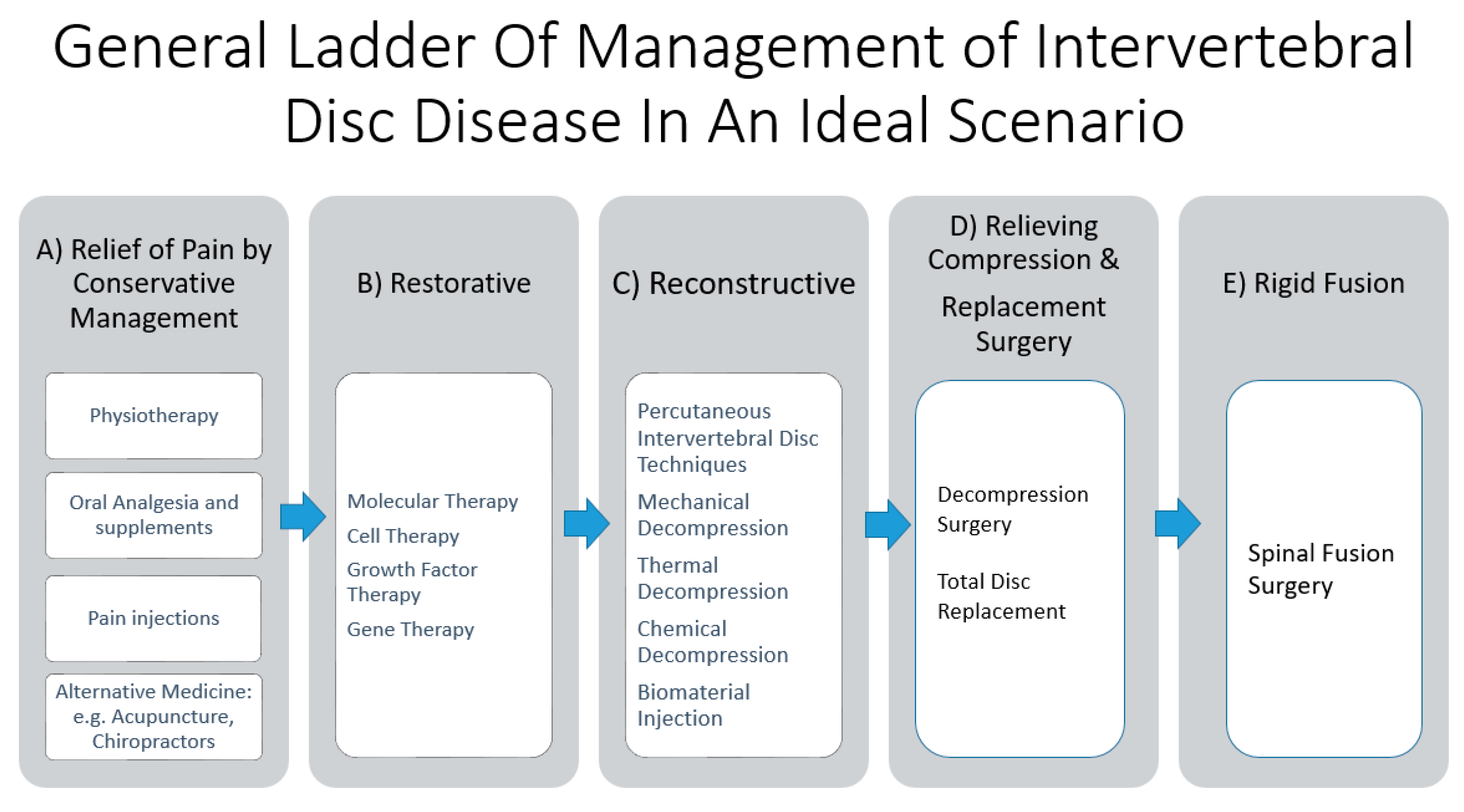
9. Current Treatment Strategies for Degenerative Disc Disease
9.1. Treatment Options for Relief of Pain in Conservative Therapy
9.1.1. Physical Strengthening and Physiotherapy
9.1.2. Oral Medications
9.1.3. Pain-Relieving Injection
9.2. Treatment with Aims of Restoration, Repair, and Regeneration of Intervertebral Disc Diseases: Molecular Therapy
9.2.1. Cell Therapy
9.2.2. Growth Factor Therapy
9.2.3. Gene Therapy
10. Reconstructive Strategies: Percutaneous Intervertebral Disc Techniques
10.1. Mechanical Decompression
10.2. Thermal Decompression
10.3. Chemical Percutaneous Decompression Techniques
10.4. Biomaterial Implantation
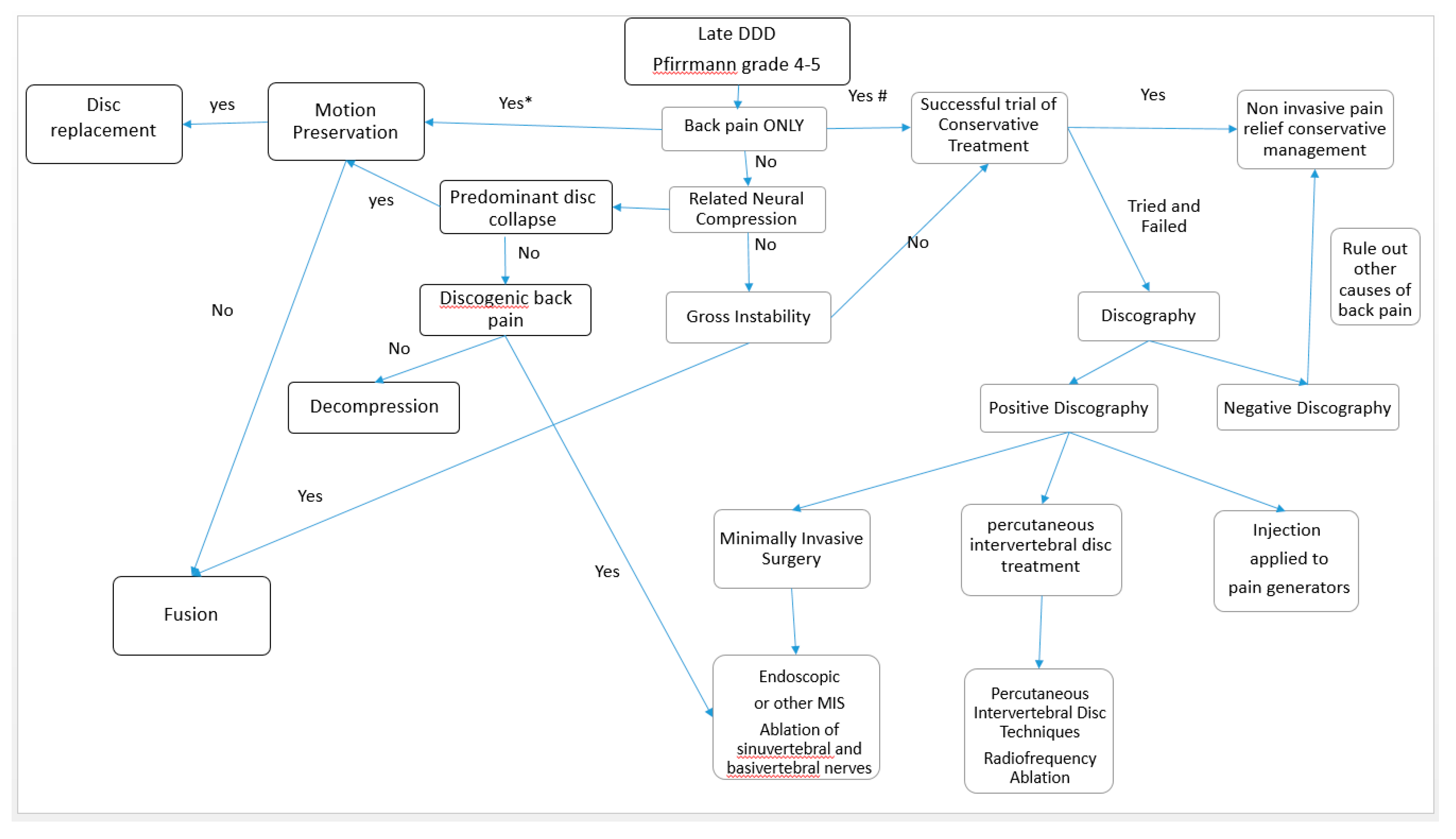
11. Definitive Treatment for Intervertebral Disc Diseases
11.1. Surgical Management
11.2. Clinical and Radiological Factors Predictive of Conservative Failure
11.3. Surgical Options for IVD Diseases
11.3.1. Disc Herniation
11.3.2. Degenerative Disc Disease with or without Spinal Stenosis
11.4. Recent Development of Endoscopic Spine Surgery and Its Role in Degenerative Disc Diseases
11.5. Summary of Surgical Techniques
12. Limitations
13. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| IVD | Intervertebral Disc |
| DDD | Degenerative Disc Disease |
| ODI | Oswestry Disability Index |
| VAS | Visual Analogue Scale |
| AF | Annulus Fibrosus |
| NP | Nucleus Pulposus |
| PLL | Posterior Longitudinal Ligament |
| TELD | Transforaminal Endoscopic Lumbar Discectomy |
| IELD | Interlaminar Endoscopic Lumbar Discectomy |
| SVN | Sinuvertebral Nerve |
| BVN | Basivertebral Nerve |
References
- Vos, T.P.; Flaxman, A.D.P.; Naghavi, M.P.; Lozano, R.P.; Michaud, C.M.D.; Ezzati, M.P.; Shibuya, K.P.; Salomon, J.A.P.; Abdalla, S.M.; Aboyans, V.P.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Walker, B.F. The prevalence of low back pain: A systematic review of the literature from 1966 to 1998. J. Spinal Disord. 2000, 13, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Sargar, K. Temporal evolution of disc in young patients with low back pain and stress reaction in lumbar vertebrae. Am. J. Neuroradiol. 2017, 38, 1647–1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerhardt, J.; Bette, S.; Janssen, I.; Gempt, J.; Meyer, B.; Ryang, Y.M. Is eighty the new sixty? Outcomes and complications after lumbar decompression surgery in elderly patients over 80 years of age. World Neurosurg. 2018, 112, e555–e560. [Google Scholar] [CrossRef] [PubMed]
- Boden, S.D.; Davis, D.O.; Dina, T.S.; Patronas, N.J.; Wiesel, S.W. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J. Bone Jt. Surg. Am. 1990, 72, 403–408. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, H.; Kettler, A.; Rohlmann, A.; Claes, L.; Wilke, H.J. The risk of disc prolapses with complex loading in different degrees of disc degeneration—A finite element analysis. Clin. Biomech. (Bristol Avon) 2007, 22, 988–998. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.A.; Roughley, P.J. What is intervertebral disc degeneration, and what causes it? Spine (Phila Pa 1976) 2006, 31, 2151–2161. [Google Scholar] [CrossRef] [Green Version]
- Ito, K.; Creemers, L. Mechanisms of intervertebral disk degeneration/injury and pain: A review. Glob. Spine J. 2013, 3, 145–152. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Adsul, N.; Yudoyono, F.; Paudel, B.; Kim, K.J.; Choi, S.H.; Kim, J.H.; Chung, S.K.; Choi, J.-H.; Jang, J.-S.; et al. Transforaminal epiduroscopic basivertebral nerve laser ablation for chronic low back pain associated with modic changes: A preliminary open-label study. Pain Res. Manag. 2018, 2018, 6857983. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Paudel, B.; Chung, S.K.; Jang, J.S.; Oh, S.H.; Jang, I.T. Transforaminal epiduroscopic laser ablation of sinuvertebral nerve in patients with chronic diskogenic back pain: Technical note and preliminary result. J. Neurol. Surg. Part. A Cent. Eur. Neurosurg. 2017, 78, 529–534. [Google Scholar] [CrossRef]
- Shayota, B.; Wong, T.L.; Fru, D.; David, G.; Iwanaga, J.; Loukas, M.; Tubbs, R.S. A comprehensive review of the sinuvertebral nerve with clinical applications. Anat. Cell Biol. 2019, 52, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Wu, P.H.; Jang, I.-T. Lumbar degenerative disease part 1: Anatomy and pathophysiology of intervertebral discogenic pain and radiofrequency ablation of basivertebral and sinuvertebral nerve treatment for chronic discogenic back pain: A prospective case series and review of literature. Int. J. Mol. Sci. 2020, 21, 1483. [Google Scholar]
- Olmarker, K.; Blomquist, J.; Stromberg, J.; Nannmark, U.; Thomsen, P.; Rydevik, B. Inflammatogenic properties of nucleus pulposus. Spine (Phila Pa 1976) 1995, 20, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Byrod, G.; Otani, K.; Brisby, H.; Rydevik, B.; Olmarker, K. Methylprednisolone reduces the early vascular permeability increase in spinal nerve roots induced by epidural nucleus pulposus application. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2000, 18, 983–987. [Google Scholar] [CrossRef]
- Kelsey, J.L.; Golden, A.L.; Mundt, D.J. Low back pain/prolapsed lumbar intervertebral disc. Rheum. Dis. Clin. N. Am. 1990, 16, 699–716. [Google Scholar]
- Corniola, M.V.; Stienen, M.N.; Joswig, H.; Smoll, N.R.; Schaller, K.; Hildebrandt, G.; Gautschi, O.P. Correlation of pain, functional impairment, and health-related quality of life with radiological grading scales of lumbar degenerative disc disease. Acta Neurochir. (Wien) 2016, 158, 499–505. [Google Scholar] [CrossRef]
- Sethi, G.; Aljawadi, A.; Choudhry, M.N.; Fischer, B.; Divecha, H.M.; Leach, J.; Arnall, F.; Verma, R.; Yasin, N.; Mohammad, S.; et al. Concomitant back pain as a predictor of outcome after single level lumbar micro-decompressive surgery—A study of 995 patients. J. Orthop. 2019, 16, 478–482. [Google Scholar] [CrossRef]
- Parker, S.L.; Mendenhall, S.K.; Godil, S.S.; Sivasubramanian, P.; Cahill, K.; Ziewacz, J.; McGirt, M.J. Incidence of low back pain after lumbar discectomy for herniated disc and its effect on patient-reported outcomes. Clin. Orthop. Relat. Res. 2015, 473, 1988–1999. [Google Scholar] [CrossRef] [Green Version]
- Kapetanakis, S.; Chaniotakis, C.; Kazakos, C.; Papathanasiou, J.V. Cauda equina syndrome due to lumbar disc herniation: A review of literature. Folia Med. 2017, 59, 377–386. [Google Scholar] [CrossRef]
- Spector, L.R.; Madigan, L.; Rhyne, A.; Darden, B.; Kim, D. Cauda equina syndrome. J. Am. Acad. Orthop. Surg. 2008, 16, 471–479. [Google Scholar] [CrossRef] [Green Version]
- Yong-Hing, K.; Kirkaldy-Willis, W.H. The pathophysiology of degenerative disease of the lumbar spine. Orthop. Clin. N. Am. 1983, 14, 491–504. [Google Scholar]
- Suthar, P.; Patel, R.; Mehta, C.; Patel, N. MRI evaluation of lumbar disc degenerative disease. J. Clin. Diagn. Res. 2015, 9, TC04. [Google Scholar] [CrossRef] [PubMed]
- Pfirrmann, C.W.; Metzdorf, A.; Zanetti, M.; Hodler, J.; Boos, N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine (Phila Pa 1976) 2001, 26, 1873–1878. [Google Scholar] [CrossRef] [PubMed]
- Modic, M.T.; Steinberg, P.M.; Ross, J.S.; Masaryk, T.J.; Carter, J.R. Degenerative disk disease: Assessment of changes in vertebral body marrow with MR imaging. Radiology 1988, 166, 193–199. [Google Scholar] [CrossRef]
- Jensen, R.K.; Leboeuf-Yde, C. Is the presence of modic changes associated with the outcomes of different treatments? A systematic critical review. BMC Musculoskelet. Disord. 2011, 12, 183. [Google Scholar] [CrossRef] [Green Version]
- Jensen, T.S.; Karppinen, J.; Sorensen, J.S.; Niinimaki, J.; Leboeuf-Yde, C. Vertebral endplate signal changes (Modic change): A systematic literature review of prevalence and association with non-specific low back pain. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2008, 17, 1407–1422. [Google Scholar] [CrossRef] [Green Version]
- Griffith, J.F.; Wang, Y.X.; Antonio, G.E.; Choi, K.C.; Yu, A.; Ahuja, A.T.; Leung, P.C. Modified Pfirrmann grading system for lumbar intervertebral disc degeneration. Spine (Phila Pa 1976) 2007, 32, E708–E712. [Google Scholar] [CrossRef]
- Wang, Y.; Videman, T.; Niemelainen, R.; Battie, M.C. Quantitative measures of modic changes in lumbar spine magnetic resonance imaging: Intra- and inter-rater reliability. Spine (Phila Pa 1976) 2011, 36, 1236–1243. [Google Scholar] [CrossRef]
- Fields, A.J.; Battie, M.C.; Herzog, R.J.; Jarvik, J.G.; Krug, R.; Link, T.M.; Lotz, J.C.; O’Neill, C.W.; Sharma, A. Measuring and reporting of vertebral endplate bone marrow lesions as seen on MRI (Modic changes): Recommendations from the ISSLS Degenerative Spinal Phenotypes Group. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2019, 28, 2266–2274. [Google Scholar] [CrossRef] [Green Version]
- Karampinos, D.C.; Melkus, G.; Baum, T.; Bauer, J.S.; Rummeny, E.J.; Krug, R. Bone marrow fat quantification in the presence of trabecular bone: Initial comparison between water-fat imaging and single-voxel MRS. Magn. Reson. Med. 2014, 71, 1158–1165. [Google Scholar] [CrossRef] [Green Version]
- Karampinos, D.C.; Ruschke, S. Quantitative MRI and spectroscopy of bone marrow. J. Magn. Reson. Imaging 2018, 47, 332–353. [Google Scholar] [CrossRef] [Green Version]
- Patel, K.B.; Poplawski, M.M.; Pawha, P.S.; Naidich, T.P.; Tanenbaum, L.N. Diffusion-weighted MRI “claw sign” improves differentiation of infectious from degenerative modic type 1 signal changes of the spine. Ajnr. Am. J. Neuroradiol. 2014, 35, 1647–1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalil, C.; Hancart, C.; Le Thuc, V.; Chantelot, C.; Chechin, D.; Cotten, A. Diffusion tensor imaging and tractography of the median nerve in carpal tunnel syndrome: Preliminary results. Eur. Radiol. 2008, 18, 2283–2291. [Google Scholar] [CrossRef] [PubMed]
- Takagi, T.; Nakamura, M.; Yamada, M.; Hikishima, K.; Momoshima, S.; Fujiyoshi, K.; Shibata, S.; Okano, H.J.; Toyama, Y.; Okano, H. Visualization of peripheral nerve degeneration and regeneration: Monitoring with diffusion tensor tractography. NeuroImage 2009, 44, 884–892. [Google Scholar] [CrossRef] [PubMed]
- Oikawa, Y.; Eguchi, Y.; Inoue, G.; Yamauchi, K.; Orita, S.; Kamoda, H.; Ishikawa, T.; Miyagi, M.; Suzuki, M.; Sakuma, Y.; et al. Diffusion tensor imaging of lumbar spinal nerve in subjects with degenerative lumbar disorders. Magn. Reson. Imaging 2015, 33, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Akeda, K. Morphology of intervertebral disc ruptures evaluated by vacuum phenomenon using multi-detector computed tomography: Association with lumbar disc degeneration and canal stenosis. BMC Musculoskelet. Disord. 2018, 19, 164. [Google Scholar] [CrossRef] [PubMed]
- Park, M.-S.; Lee, H.-M.; Hahn, S.-B.; Moon, S.-H.; Kim, Y.-T.; Lee, C.-S.; Jung, H.-W.; Kwon, B.-S.; Riew, K.D. The association of the activation-inducible tumor necrosis factor receptor and ligand with lumbar disc herniation. Yonsei Med. J. 2007, 48, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Kraychete, D.C.; Sakata, R.K.; Issy, A.M.; Bacellar, O.; Santos-Jesus, R.; Carvalho, E.M. Serum cytokine levels in patients with chronic low back pain due to herniated disc: Analytical cross-sectional study. Sao Paulo Med. J. Rev. Paul. Med. 2010, 128, 259–262. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, L.M.; Schistad, E.; Jacobsen, L.M.; Roe, C.; Gjerstad, J. Serum levels of the pro-inflammatory interleukins 6 (IL-6) and -8 (IL-8) in patients with lumbar radicular pain due to disc herniation: A 12-month prospective study. Brain Behav. Immun. 2015, 46, 132–136. [Google Scholar] [CrossRef]
- Cheng, L.; Fan, W.; Liu, B.; Wang, X.; Nie, L. Th17 lymphocyte levels are higher in patients with ruptured than non-ruptured lumbar discs, and are correlated with pain intensity. Injury 2013, 44, 1805–1810. [Google Scholar] [CrossRef]
- Xue, H.; Yao, Y.; Wang, X.; Zhang, F.; Jiang, X.; Liu, J.; Wang, H.; Li, Y.; Wang, X.; Li, H.; et al. Interleukin-21 Is Associated with the Pathogenesis of Lumbar Disc Herniation. Iran. J. Allergy Asthma Immunol. 2015, 14, 509–518. [Google Scholar] [PubMed]
- Goode, A.P.; Marshall, S.W.; Kraus, V.B.; Renner, J.B.; Sturmer, T.; Carey, T.S.; Irwin, D.E.; Jordan, J.M. Association between serum and urine biomarkers and lumbar spine individual radiographic features: The Johnston County Osteoarthritis Project. Osteoarthr. Cartil. 2012, 20, 1286–1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grad, S.; Bow, C.; Karppinen, J.; Luk, K.D.; Cheung, K.M.; Alini, M.; Samartzis, D. Systemic blood plasma CCL5 and CXCL6: Potential biomarkers for human lumbar disc degeneration. Eur. Cells Mater. 2016, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ye, S.; Ju, B.; Wang, H.; Lee, K.B. Bone morphogenetic protein-2 provokes interleukin-18-induced human intervertebral disc degeneration. Bone Jt. Res. 2016, 5, 412–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.N.; Jacobsen, H.E.; Khan, J.; Filippi, C.G.; Levine, M.; Lehman, R.A., Jr.; Riew, K.D.; Lenke, L.G.; Chahine, N.O. Inflammatory biomarkers of low back pain and disc degeneration: A review. Ann. N. Y. Acad. Sci. 2017, 1410, 68–84. [Google Scholar] [CrossRef] [PubMed]
- Willems, P. Decision making in surgical treatment of chronic low back pain: The performance of prognostic tests to select patients for lumbar spinal fusion. Acta Orthop. Suppl. 2013, 84, 1–35. [Google Scholar] [CrossRef]
- Pneumaticos, S.G.; Reitman, C.A.; Lindsey, R.W. Diskography in the evaluation of low back pain. J. Am. Acad. Orthop. Surg. 2006, 14, 46–55. [Google Scholar] [CrossRef]
- Maus, T.P.; Aprill, C.N. Lumbar diskogenic pain, provocation diskography, and imaging correlates. Radiol. Clin. N. Am. 2012, 50, 681–704. [Google Scholar] [CrossRef]
- Sigmundsson, F.G.; Kang, X.P.; Jonsson, B.; Stromqvist, B. Correlation between disability and MRI findings in lumbar spinal stenosis: A prospective study of 109 patients operated on by decompression. Acta Orthop. 2011, 82, 204–210. [Google Scholar] [CrossRef] [Green Version]
- Quattrocchi, C.C.; Alexandre, A.M.; Della Pepa, G.M.; Altavilla, R.; Zobel, B.B. Modic changes: Anatomy, pathophysiology and clinical correlation. Acta Neurochir. Suppl. 2011, 108, 49–53. [Google Scholar] [CrossRef]
- Hestbaek, L.; Leboeuf-Yde, C.; Manniche, C. Low back pain: What is the long-term course? A review of studies of general patient populations. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2003, 12, 149–165. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Atlas, S.J.; Stanos, S.P.; Rosenquist, R.W. Nonsurgical interventional therapies for low back pain: A review of the evidence for an American Pain Society clinical practice guideline. Spine (Phila Pa 1976) 2009, 34, 1078–1093. [Google Scholar] [CrossRef] [PubMed]
- Luan, S.; Wan, Q.; Luo, H.; Li, X.; Ke, S.; Lin, C.; Wu, Y.; Wu, S.; Ma, C. Running exercise alleviates pain and promotes cell proliferation in a rat model of intervertebral disc degeneration. Int. J. Mol. Sci. 2015, 16, 2130–2144. [Google Scholar] [CrossRef] [PubMed]
- Steele, J.; Bruce-Low, S.; Smith, D.; Osborne, N.; Thorkeldsen, A. Can specific loading through exercise impart healing or regeneration of the intervertebral disc? Spine J. Off. J. N. Am. Spine Soc. 2015, 15, 2117–2121. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kim, H.; Chung, J. Effects of spinal stabilization exercise on the cross-sectional areas of the lumbar multifidus and psoas major muscles, pain intensity, and lumbar muscle strength of patients with degenerative disc disease. J. Phys. Ther. Sci. 2014, 26, 579–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofstee, D.J.; Gijtenbeek, J.M.; Hoogland, P.H.; van Houwelingen, H.C.; Kloet, A.; Lotters, F.; Tans, J.T. Westeinde sciatica trial: Randomized controlled study of bed rest and physiotherapy for acute sciatica. J. Neurosurg. 2002, 96, 45–49. [Google Scholar] [CrossRef]
- Weber, H.; Holme, I.; Amlie, E. The natural course of acute sciatica with nerve root symptoms in a double-blind placebo-controlled trial evaluating the effect of piroxicam. Spine (Phila Pa 1976) 1993, 18, 1433–1438. [Google Scholar] [CrossRef]
- Kjaer, P.; Tunset, A.; Boyle, E.; Jensen, T.S. Progression of lumbar disc herniations over an eight-year period in a group of adult Danes from the general population—A longitudinal MRI study using quantitative measures. BMC Musculoskelet. Disord. 2016, 17, 26. [Google Scholar] [CrossRef] [Green Version]
- Wong, J.J.; Cote, P.; Sutton, D.A.; Randhawa, K.; Yu, H.; Varatharajan, S.; Goldgrub, R.; Nordin, M.; Gross, D.P.; Shearer, H.M.; et al. Clinical practice guidelines for the noninvasive management of low back pain: A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Eur. J. Pain (Lond. Engl. ) 2017, 21, 201–216. [Google Scholar] [CrossRef]
- Risbud, M.V.; Shapiro, I.M. Role of cytokines in intervertebral disc degeneration: Pain and disc content. Nat. Rev. Rheumatol. 2014, 10, 44–56. [Google Scholar] [CrossRef]
- Stuber, K.; Sajko, S.; Kristmanson, K. Efficacy of glucosamine, chondroitin, and methylsulfonylmethane for spinal degenerative joint disease and degenerative disc disease: A systematic review. J. Can. Chiropr. Assoc. 2011, 55, 47–55. [Google Scholar] [PubMed]
- Maroon, J.C.; Bost, J.W. Omega-3 fatty acids (fish oil) as an anti-inflammatory: An alternative to nonsteroidal anti-inflammatory drugs for discogenic pain. Surg. Neurol. 2006, 65, 326–331. [Google Scholar] [CrossRef] [PubMed]
- NaPier, Z.; Kanim, L.E.A.; Arabi, Y.; Salehi, K.; Sears, B.; Perry, M.; Kim, S.; Sheyn, D.; Bae, H.W.; Glaeser, J.D. Omega-3 fatty acid supplementation reduces intervertebral disc degeneration. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2019, 25, 9531–9537. [Google Scholar] [CrossRef] [PubMed]
- Benyamin, R.M.; Manchikanti, L.; Parr, A.T.; Diwan, S.; Singh, V.; Falco, F.J.; Datta, S.; Abdi, S.; Hirsch, J.A. The effectiveness of lumbar interlaminar epidural injections in managing chronic low back and lower extremity pain. Pain Physician 2012, 15, E363–E404. [Google Scholar] [PubMed]
- Parr, A.T.; Diwan, S.; Abdi, S. Lumbar interlaminar epidural injections in managing chronic low back and lower extremity pain: A systematic review. Pain Physician 2009, 12, 163–188. [Google Scholar]
- Manchikanti, L.; Buenaventura, R.M.; Manchikanti, K.N.; Ruan, X.; Gupta, S.; Smith, H.S.; Christo, P.J.; Ward, S.P. Effectiveness of therapeutic lumbar transforaminal epidural steroid injections in managing lumbar spinal pain. Pain Physician 2012, 15, E199–E245. [Google Scholar]
- Parr, A.T.; Manchikanti, L.; Hameed, H.; Conn, A.; Manchikanti, K.N.; Benyamin, R.M.; Diwan, S.; Singh, V.; Abdi, S. Caudal epidural injections in the management of chronic low back pain: A systematic appraisal of the literature. Pain Physician 2012, 15, E159–E198. [Google Scholar]
- Helm Ii, S.; Benyamin, R.M.; Chopra, P.; Deer, T.R.; Justiz, R. Percutaneous adhesiolysis in the management of chronic low back pain in post lumbar surgery syndrome and spinal stenosis: A systematic review. Pain Physician 2012, 15, E435–E462. [Google Scholar]
- Lee, J.H.; Lee, S.H. Clinical effectiveness of percutaneous adhesiolysis using Navicath for the management of chronic pain due to lumbosacral disc herniation. Pain Physician 2012, 15, 213–221. [Google Scholar]
- Kanayama, M.; Oha, F.; Hashimoto, T. What types of degenerative lumbar pathologies respond to nerve root injection? A retrospective review of six hundred and forty one cases. Int. Orthop. 2015, 39, 1379–1382. [Google Scholar] [CrossRef]
- Chou, R.; Hashimoto, R.; Friedly, J.; Fu, R.; Dana, T.; Sullivan, S.; Bougatsos, C.; Jarvik, J. AHRQ technology assessments. In Pain Management Injection Therapies for Low Back Pain; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2015. [Google Scholar]
- Huang, Y.C.; Leung, V.Y.; Lu, W.W.; Luk, K.D. The effects of microenvironment in mesenchymal stem cell-based regeneration of intervertebral disc. Spine J. Off. J. N. Am. Spine Soc. 2013, 13, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Sakai, D.; Schol, J. Cell therapy for intervertebral disc repair: Clinical perspective. J. Orthop. Transl. 2017, 9, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Chakravarthy, K.; Chen, Y.; He, C.; Christo, P.J. Stem Cell Therapy for Chronic Pain Management: Review of Uses, Advances, and Adverse Effects. Pain Physician 2017, 20, 293–305. [Google Scholar] [CrossRef] [PubMed]
- Atesok, K.; Fu, F.H.; Sekiya, I.; Stolzing, A.; Ochi, M.; Rodeo, S.A. Stem cells in degenerative orthopaedic pathologies: Effects of aging on therapeutic potential. Knee Surg. Sports Traumatol. Arthrosc. Off. J. Esska 2017, 25, 626–636. [Google Scholar] [CrossRef]
- Wuertz, K.; Godburn, K.; Neidlinger-Wilke, C.; Urban, J.; Iatridis, J.C. Behavior of mesenchymal stem cells in the chemical microenvironment of the intervertebral disc. Spine (Phila Pa 1976) 2008, 33, 1843–1849. [Google Scholar] [CrossRef] [Green Version]
- Arpinar, V.E.; Rand, S.D.; Klein, A.P.; Maiman, D.J.; Muftuler, L.T. Changes in perfusion and diffusion in the endplate regions of degenerating intervertebral discs: A DCE-MRI study. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2017, 26, 1416. [Google Scholar] [CrossRef] [Green Version]
- Muftuler, L.T.; Jarman, J.P.; Yu, H.J.; Gardner, V.O.; Maiman, D.J.; Arpinar, V.E. Association between intervertebral disc degeneration and endplate perfusion studied by DCE-MRI. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2015, 24, 679–685. [Google Scholar] [CrossRef]
- Clarke, L.E.; McConnell, J.C.; Sherratt, M.J.; Derby, B.; Richardson, S.M.; Hoyland, J.A. Growth differentiation factor 6 and transforming growth factor-beta differentially mediate mesenchymal stem cell differentiation, composition, and micromechanical properties of nucleus pulposus constructs. Arthritis Res. Ther. 2014, 16, R67. [Google Scholar] [CrossRef] [Green Version]
- Stoyanov, J.V.; Gantenbein-Ritter, B.; Bertolo, A.; Aebli, N.; Baur, M.; Alini, M.; Grad, S. Role of hypoxia and growth and differentiation factor-5 on differentiation of human mesenchymal stem cells towards intervertebral nucleus pulposus-like cells. Eur. Cells Mater. 2011, 21, 533–547. [Google Scholar] [CrossRef]
- Mouw, J.K.; Connelly, J.T.; Wilson, C.G.; Michael, K.E.; Levenston, M.E. Dynamic compression regulates the expression and synthesis of chondrocyte-specific matrix molecules in bone marrow stromal cells. Stem Cells (Dayt. OH) 2007, 25, 655–663. [Google Scholar] [CrossRef]
- James, G.; Blomster, L.; Hall, L.; Schmid, A.B.; Shu, C.C.; Little, C.B.; Melrose, J.; Hodges, P.W. Mesenchymal stem cell treatment of intervertebral disc lesion prevents fatty infiltration and fibrosis of the multifidus muscle, but not cytokine and muscle fiber changes. Spine (Phila Pa 1976) 2016, 41, 1208–1217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, W.; Lu, Z.; Qin, L.; Mauck, R.L.; Smith, H.E.; Smith, L.J.; Malhotra, N.R.; Heyworth, M.F.; Caldera, F.; Enomoto-Iwamoto, M.; et al. Cell therapy for the degenerating intervertebral disc. Transl. Res. J. Lab. Clin. Med. 2017, 181, 49–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccirilli, M.; Delfinis, C.P.; Santoro, A.; Salvati, M. Mesenchymal stem cells in lumbar spine surgery: A single institution experience about red bone marrow and fat tissue derived MSCs. J. Neurosurg. Sci. 2017, 61, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Centeno, C.; Markle, J.; Dodson, E. Treatment of lumbar degenerative disc disease-associated radicular pain with culture-expanded autologous mesenchymal stem cells: A pilot study on safety and efficacy. J. Transl. Med. 2017, 15, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comella, K.; Silbert, R.; Parlo, M. Effects of the intradiscal implantation of stromal vascular fraction plus platelet rich plasma in patients with degenerative disc disease. J. Transl. Med. 2017, 15, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coric, D.; Pettine, K.; Sumich, A.; Boltes, M.O. Prospective study of disc repair with allogeneic chondrocytes presented at the 2012 Joint Spine Section Meeting. J. Neurosurg. Spine 2013, 18, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Elabd, C.; Centeno, C.J.; Schultz, J.R.; Lutz, G.; Ichim, T.; Silva, F.J. Intra-discal injection of autologous, hypoxic cultured bone marrow-derived mesenchymal stem cells in five patients with chronic lower back pain: A long-term safety and feasibility study. J. Transl. Med. 2016, 14, 253. [Google Scholar] [CrossRef] [Green Version]
- Haufe, S.M.; Mork, A.R. Intradiscal injection of hematopoietic stem cells in an attempt to rejuvenate the intervertebral discs. Stem Cells Dev. 2006, 15, 136–137. [Google Scholar] [CrossRef]
- Kumar, H.; Ha, D.H.; Lee, E.J.; Park, J.H.; Shim, J.H.; Ahn, T.K.; Kim, K.T.; Ropper, A.E.; Sohn, S.; Kim, C.H.; et al. Safety and tolerability of intradiscal implantation of combined autologous adipose-derived mesenchymal stem cells and hyaluronic acid in patients with chronic discogenic low back pain: 1-year follow-up of a phase I study. Stem Cell Res. Ther. 2017, 8, 262. [Google Scholar] [CrossRef] [Green Version]
- Mochida, J.; Sakai, D.; Nakamura, Y.; Watanabe, T.; Yamamoto, Y.; Kato, S. Intervertebral disc repair with activated nucleus pulposus cell transplantation: A three-year, prospective clinical study of its safety. Eur. Cells Mater. 2015, 29, 202–212, discussion 212. [Google Scholar] [CrossRef]
- Noriega, D.C.; Ardura, F.; Hernandez-Ramajo, R.; Martin-Ferrero, M.A.; Sanchez-Lite, I.; Toribio, B.; Alberca, M.; Garcia, V.; Moraleda, J.M.; Sanchez, A.; et al. Intervertebral Disc Repair by Allogeneic Mesenchymal Bone Marrow Cells: A Randomized Controlled Trial. Transplantation 2017, 101, 1945–1951. [Google Scholar] [CrossRef] [PubMed]
- Pang, X.; Yang, H.; Peng, B. Human umbilical cord mesenchymal stem cell transplantation for the treatment of chronic discogenic low back pain. Pain Physician 2014, 17, E525–E530. [Google Scholar] [PubMed]
- Masuda, K.; An, H.S. Growth factors and the intervertebral disc. Spine J. Off. J. N. Am. Spine Soc. 2004, 4, 330s–340s. [Google Scholar] [CrossRef] [PubMed]
- Dowdell, J.; Erwin, M.; Choma, T.; Vaccaro, A.; Iatridis, J.; Cho, S.K. Intervertebral Disk Degeneration and Repair. Neurosurgery 2017, 80, S46–S54. [Google Scholar] [CrossRef]
- Thompson, J.P.; Oegema, T.R., Jr.; Bradford, D.S. Stimulation of mature canine intervertebral disc by growth factors. Spine (Phila Pa 1976) 1991, 16, 253–260. [Google Scholar] [CrossRef]
- Huang, K.Y.; Yan, J.J.; Hsieh, C.C.; Chang, M.S.; Lin, R.M. The in vivo biological effects of intradiscal recombinant human bone morphogenetic protein-2 on the injured intervertebral disc: An animal experiment. Spine (Phila Pa 1976) 2007, 32, 1174–1180. [Google Scholar] [CrossRef]
- Chujo, T.; An, H.S.; Akeda, K.; Miyamoto, K.; Muehleman, C.; Attawia, M.; Andersson, G.; Masuda, K. Effects of growth differentiation factor-5 on the intervertebral disc—In Vitro bovine study and in vivo rabbit disc degeneration model study. Spine (Phila Pa 1976) 2006, 31, 2909–2917. [Google Scholar] [CrossRef]
- Hayes, A.J.; Ralphs, J.R. The response of foetal annulus fibrosus cells to growth factors: Modulation of matrix synthesis by TGF-beta1 and IGF-1. Histochem. Cell Biol. 2011, 136, 163–175. [Google Scholar] [CrossRef]
- Takegami, K.; An, H.S.; Kumano, F.; Chiba, K.; Thonar, E.J.; Singh, K.; Masuda, K. Osteogenic protein-1 is most effective in stimulating nucleus pulposus and annulus fibrosus cells to repair their matrix after chondroitinase ABC-induced in vitro chemonucleolysis. Spine J. Off. J. N. Am. Spine Soc. 2005, 5, 231–238. [Google Scholar] [CrossRef]
- Lee, K.I.; Moon, S.H.; Kim, H.; Kwon, U.H.; Kim, H.J.; Park, S.N.; Suh, H.; Lee, H.M.; Kim, H.S.; Chun, H.J.; et al. Tissue engineering of the intervertebral disc with cultured nucleus pulposus cells using atelocollagen scaffold and growth factors. Spine (Phila Pa 1976) 2012, 37, 452–458. [Google Scholar] [CrossRef]
- Gilbertson, L.; Ahn, S.H.; Teng, P.N.; Studer, R.K.; Niyibizi, C.; Kang, J.D. The effects of recombinant human bone morphogenetic protein-2, recombinant human bone morphogenetic protein-12, and adenoviral bone morphogenetic protein-12 on matrix synthesis in human annulus fibrosis and nucleus pulposus cells. Spine J. Off. J. N. Am. Spine Soc. 2008, 8, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.J.; Wu, Y.C.; Tu, Y.K.; Cheng, J.W.; Tsai, W.C.; Yu, T.Y. Autologous blood-derived products compared with corticosteroids for treatment of plantar fasciopathy: A systematic review and meta-analysis. Am. J. Phys. Med. Rehabil. 2019, 98, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.L.; Hunter, D.J.; Paterson, K.L. Platelet-rich plasma for the management of hip and knee osteoarthritis. Curr. Rheumatol. Rep. 2017, 19, 24. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.H.; Lo, W.C.; Lee, J.J.; Su, C.H.; Lin, C.T.; Liu, H.Y.; Lin, T.W.; Lin, W.C.; Huang, T.Y.; Deng, W.P. Tissue-engineered intervertebral disc and chondrogenesis using human nucleus pulposus regulated through TGF-beta1 in platelet-rich plasma. J. Cell. Physiol. 2006, 209, 744–754. [Google Scholar] [CrossRef] [PubMed]
- Monfett, M.; Harrison, J.; Boachie-Adjei, K.; Lutz, G. Intradiscal platelet-rich plasma (PRP) injections for discogenic low back pain: An update. Int. Orthop. 2016, 40, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Friedmann, T.; Roblin, R. Gene therapy for human genetic disease? Science (N. Y.) 1972, 175, 949–955. [Google Scholar] [CrossRef]
- Li, W.; Wang, P.; Zhang, Z.; Wang, W.; Liu, Y.; Qi, Q. MiR-184 regulates proliferation in nucleus pulposus cells by targeting GAS1. World Neurosurg. 2017, 97, 710–715. [Google Scholar] [CrossRef]
- Sampara, P.; Banala, R.R.; Vemuri, S.K.; Av, G.R.; Gpv, S. Understanding the molecular biology of intervertebral disc degeneration and potential gene therapy strategies for regeneration: A review. Gene Ther. 2018, 25, 67–82. [Google Scholar] [CrossRef]
- Cooney, A.L.; McCray, P.B., Jr.; Sinn, P.L. Cystic fibrosis gene therapy: Looking back, looking forward. Genes 2018, 9, 538. [Google Scholar] [CrossRef] [Green Version]
- Olowoyeye, A.; Okwundu, C.I. Gene therapy for sickle cell disease. Cochrane Database Syst. Rev. 2018, 11, CD007652. [Google Scholar] [CrossRef]
- Kelekis, A.D.; Filippiadis, D.K.; Martin, J.B.; Brountzos, E. Standards of practice: Quality assurance guidelines for percutaneous treatments of intervertebral discs. Cardiovasc. Interv. Radiol. 2010, 33, 909–913. [Google Scholar] [CrossRef] [PubMed]
- Buy, X.; Gangi, A. Percutaneous treatment of intervertebral disc herniation. Semin. Interv. Radiol. 2010, 27, 148–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.; Kim, H.S.; Oh, S.W.; Adsul, N.M.; Singh, R.; Kashlan, O.N.; Noh, J.H.; Jang, I.T.; Oh, S.H. Evolution of spinal endoscopic surgery. Neurospine 2019, 16, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Kambin, P.; Sampson, S. Posterolateral percutaneous suction-excision of herniated lumbar intervertebral discs. Report of interim results. Clin. Orthop. Relat. Res. 1986, 207, 37–43. [Google Scholar]
- Kim, H.S.; Paudel, B.; Jang, J.S.; Lee, K.; Oh, S.H.; Jang, I.T. Percutaneous endoscopic lumbar discectomy for all types of Lumbar Disc Herniations (LDH) Including severely difficult and extremely difficult LDH cases. Pain Physician 2018, 21, E401–E408. [Google Scholar] [PubMed]
- Duarte, R.; Costa, J.C. Percutaneous laser disc decompression for lumbar discogenic radicular pain. Radiologia 2012, 54, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Fukui, S.; Rohof, O. Results of pulsed radiofrequency technique with two laterally placed electrodes in the annulus in patients with chronic lumbar discogenic pain. J. Anesth. 2012, 26, 606–609. [Google Scholar] [CrossRef]
- Gerszten, P.C.; Smuck, M.; Rathmell, J.P.; Simopoulos, T.T.; Bhagia, S.M.; Mocek, C.K.; Crabtree, T.; Bloch, D.A. Plasma disc decompression compared with fluoroscopy-guided transforaminal epidural steroid injections for symptomatic contained lumbar disc herniation: A prospective, randomized, controlled trial. J. Neurosurg. Spine 2010, 12, 357–371. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.; Kumar, A.; Siddharth, M.S.; Sambhav, P.S.; Tan, J. Annulo-nucleoplasty using Disc-FX in the management of lumbar disc pathology: Early results. Int. J. Spine Surg. 2014, 8. [Google Scholar] [CrossRef] [Green Version]
- Einarson, T.R.; Bootman, J.L.; Smith, G.H. Chymopapain. Drug Intell. Clin. Pharm. 1984, 18, 560–568. [Google Scholar] [CrossRef]
- Wardlaw, D. Sciatica caused by disc herniation: Why is Chymopapain Chemonucleolysis denied to our patients? Int. J. Spine Surg. 2016, 10, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, K.; Elias, G.; Steppan, J.; Boxley, C.; Balagurunathan, K.; Victor, X.; Meaders, T.; Muto, M. Percutaneous treatment of herniated lumbar discs with ozone: Investigation of the mechanisms of action. J. Vasc. Interv. Radiol. 2016, 27, 1242–1250. [Google Scholar] [CrossRef] [PubMed]
- Ezeldin, M.; Leonardi, M.; Princiotta, C.; Dall’olio, M.; Tharwat, M.; Zaki, M.; Abdel-Wanis, M.E.; Cirillo, L. Percutaneous ozone nucleolysis for lumbar disc herniation. Neuroradiology 2018, 60, 1231–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giurazza, F.; Guarnieri, G.; Murphy, K.J.; Muto, M. Intradiscal O2O3: Rationale, injection technique, short- and long-term outcomes for the treatment of low back pain due to disc herniation. Can. Assoc. Radiol. J. 2017, 68, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Stagni, S.; de Santis, F.; Cirillo, L.; Dall’olio, M.; Princiotta, C.; Simonetti, L.; Stafa, A.; Leonardi, M. A minimally invasive treatment for lumbar disc herniation: DiscoGel(R) chemonucleolysis in patients unresponsive to chemonucleolysis with oxygen-ozone. Interv. Neuroradiol. J. Perither. Neuroradiol. Surg. Proced. Relat. Neurosci. 2012, 18, 97–104. [Google Scholar] [CrossRef]
- Marcia, S.; Bellini, M.; Hirsch, J.A.; Chandra, R.V.; Piras, E.; Marras, M.; Sanna, A.M.; Saba, L. Efficacy of an ethyl alcohol gel in symptomatic disc herniation. Eur. J. Radiol. 2018, 109, 101–107. [Google Scholar] [CrossRef]
- Huang, Y.C.; Hu, Y.; Li, Z. Biomaterials for intervertebral disc regeneration: Current status and looming challenges. J. Tissue Eng. Regen. Med. 2018, 12, 2188–2202. [Google Scholar] [CrossRef]
- Bowles, R.D.; Setton, L.A. Biomaterials for intervertebral disc regeneration and repair. Biomaterials 2017, 129, 54–67. [Google Scholar] [CrossRef]
- Benneker, L.M.; Andersson, G.; Iatridis, J.C.; Sakai, D.; Hartl, R.; Ito, K.; Grad, S. Cell therapy for intervertebral disc repair: Advancing cell therapy from bench to clinics. Eur. Cells Mater. 2014, 27, 5–11. [Google Scholar] [CrossRef]
- Wang, B.H.; Campbell, G. Formulations of polyvinyl alcohol cryogel that mimic the biomechanical properties of soft tissues in the natural lumbar intervertebral disc. Spine (Phila Pa 1976) 2009, 34, 2745–2753. [Google Scholar] [CrossRef]
- Likhitpanichkul, M.; Dreischarf, M.; Illien-Junger, S.; Walter, B.A.; Nukaga, T.; Long, R.G.; Sakai, D.; Hecht, A.C.; Iatridis, J.C. Fibrin-genipin adhesive hydrogel for annulus fibrosus repair: Performance evaluation with large animal organ culture, in situ biomechanics, and in vivo degradation tests. Eur. Cells Mater. 2014, 28, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Borem, R.; Madeline, A.; Walters, J.; Mayo, H.; Gill, S.; Mercuri, J. Angle-ply biomaterial scaffold for annulus fibrosus repair replicates native tissue mechanical properties, restores spinal kinematics, and supports cell viability. Acta Biomater. 2017, 58, 254–268. [Google Scholar] [CrossRef] [PubMed]
- Gloria, A.; Russo, T.; D’Amora, U.; Santin, M.; De Santis, R.; Ambrosio, L. Customised multiphasic nucleus/annulus scaffold for intervertebral disc repair/regeneration. Connect. Tissue Res. 2020, 61, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Du, L.; Yang, Q.; Zhang, J.; Zhu, M.; Ma, X.; Zhang, Y.; Wang, L.; Xu, B. Engineering a biomimetic integrated scaffold for intervertebral disc replacement. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 96, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Huang, D.; Li, J.; Liu, S.; Qing, X.; Shao, Z. Genipin-crosslinked decellularized annulus fibrosus hydrogels induces tissue-specific differentiation of bone mesenchymal stem cells and intervertebral disc regeneration. J. Tissue Eng. Regen. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Gebhard, H.; Bowles, R.; Dyke, J.; Saleh, T.; Doty, S.; Bonassar, L.; Hartl, R. Total disc replacement using a tissue-engineered intervertebral disc in vivo: New animal model and initial results. Evid. Based Spine Care J. 2010, 1, 62–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohd Isa, I.L.; Abbah, S.A. Implantation of hyaluronic acid hydrogel prevents the pain phenotype in a rat model of intervertebral disc injury. Sci. Adv. 2018, 4, eaaq0597. [Google Scholar] [CrossRef] [Green Version]
- Xu, B.; Xu, H.; Wu, Y.; Li, X.; Zhang, Y.; Ma, X.; Yang, Q. Intervertebral disc tissue engineering with natural extracellular matrix-derived biphasic composite scaffolds. PLoS ONE 2015, 10, e0124774. [Google Scholar] [CrossRef] [Green Version]
- Guterl, C.C.; See, E.Y.; Blanquer, S.B.; Pandit, A.; Ferguson, S.J.; Benneker, L.M.; Grijpma, D.W.; Sakai, D.; Eglin, D.; Alini, M.; et al. Challenges and strategies in the repair of ruptured annulus fibrosus. Eur. Cells Mater. 2013, 25, 1–21. [Google Scholar] [CrossRef]
- Bailey, A.; Araghi, A.; Blumenthal, S.; Huffmon, G.V. Prospective, multicenter, randomized, controlled study of anular repair in lumbar discectomy: Two-year follow-up. Spine (Phila Pa 1976) 2013, 38, 1161–1169. [Google Scholar] [CrossRef]
- Martin, J.T.; Milby, A.H.; Ikuta, K.; Poudel, S.; Pfeifer, C.G.; Elliott, D.M.; Smith, H.E.; Mauck, R.L. A radiopaque electrospun scaffold for engineering fibrous musculoskeletal tissues: Scaffold characterization and in vivo applications. Acta Biomater. 2015, 26, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reitmaier, S.; Graichen, F.; Shirazi-Adl, A.; Schmidt, H. Separate the Sheep from the Goats: Use and Limitations of Large Animal Models in Intervertebral Disc Research. J. Bone Jt. Surg. Am. 2017, 99, e102. [Google Scholar] [CrossRef] [PubMed]
- Newell, N.; Little, J.P.; Christou, A.; Adams, M.A.; Adam, C.J.; Masouros, S.D. Biomechanics of the human intervertebral disc: A review of testing techniques and results. J. Mech. Behav. Biomed. Mater. 2017, 69, 420–434. [Google Scholar] [CrossRef] [PubMed]
- Fritzell, P.; Hagg, O.; Wessberg, P.; Nordwall, A. 2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: A multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine (Phila Pa 1976) 2001, 26, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Fritzell, P.; Hagg, O.; Jonsson, D.; Nordwall, A. Cost-effectiveness of lumbar fusion and nonsurgical treatment for chronic low back pain in the Swedish Lumbar Spine Study: A multicenter, randomized, controlled trial from the Swedish Lumbar Spine Study Group. Spine (Phila Pa 1976) 2004, 29, 421–434. [Google Scholar] [CrossRef]
- Brox, J.I.; Sorensen, R.; Friis, A.; Nygaard, O.; Indahl, A.; Keller, A.; Ingebrigtsen, T.; Eriksen, H.R.; Holm, I.; Koller, A.K.; et al. Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine (Phila Pa 1976) 2003, 28, 1913–1921. [Google Scholar] [CrossRef] [Green Version]
- Fairbank, J.; Frost, H.; Wilson-MacDonald, J.; Yu, L.M.; Barker, K.; Collins, R. Randomised controlled trial to compare surgical stabilisation of the lumbar spine with an intensive rehabilitation programme for patients with chronic low back pain: The MRC spine stabilisation trial. BMJ (Clin. Res. Ed.) 2005, 330, 1233. [Google Scholar] [CrossRef] [Green Version]
- Storm, P.B.; Chou, D.; Tamargo, R.J. Surgical management of cervical and lumbosacral radiculopathies: Indications and outcomes. Phys. Med. Rehabil. Clin. N. Am. 2002, 13, 735–759. [Google Scholar] [CrossRef]
- Motiei-Langroudi, R.; Sadeghian, H.; Seddighi, A.S. Clinical and magnetic resonance imaging factors which may predict the need for surgery in lumbar disc herniation. Asian Spine J. 2014, 8, 446–452. [Google Scholar] [CrossRef] [Green Version]
- Hara, M.; Takahashi, H.; Yokoyama, Y.; Wada, A.; Hasegawa, K.; Iida, Y. Comparison of the invasiveness of conventional discectomy and microendoscopic discectomy for lumbar disc herniation: Differences in the methods of approach. Asian J. Endosc. Surg. 2015, 8, 40–47. [Google Scholar] [CrossRef]
- Mobbs, R.J.; Phan, K.; Malham, G.; Seex, K.; Rao, P.J. Lumbar interbody fusion: Techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J. Spine Surg. (Hong Kong) 2015, 1, 2–18. [Google Scholar] [CrossRef]
- Quaglietta, P.; Cassitto, D.; Corriero, A.S.; Corriero, G. Paraspinal approach to the far lateral disc herniations: Retrospective study on 42 cases. Acta Neurochir. Suppl. 2005, 92, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Yorukoglu, A.G.; Goker, B.; Tahta, A.; Akcakaya, M.O.; Aydoseli, A.; Sabanci, P.A.; Aras, Y.; Alkir, G.; Sencer, A.; Imer, M.; et al. Fully endoscopic interlaminar and transforaminal lumbar discectomy: Analysis of 47 complications encountered in a series of 835 patients. Neurocirugía (Asturias Spain) 2017, 28, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Alvi, M.A.; Kerezoudis, P.; Wahood, W.; Goyal, A.; Bydon, M. Operative approaches for lumbar disc herniation: A systematic review and multiple treatment meta-analysis of conventional and minimally invasive surgeries. World Neurosurg. 2018, 114, 391–407. [Google Scholar] [CrossRef] [PubMed]
- Feng, F.; Xu, Q.; Yan, F.; Xie, Y.; Deng, Z.; Hu, C.; Zhu, X.; Cai, L. Comparison of 7 surgical interventions for lumbar disc herniation: A network Meta-analysis. Pain Physician 2017, 20, E863. [Google Scholar] [PubMed]
- Wu, P.H.; Kim, H.S.; Jang, I.-T. How I do it? Uniportal full endoscopic contralateral approach for lumbar foraminal stenosis with double crush syndrome. Acta Neurochir. 2019. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Zhang, C.; Wang, J.; Chu, T.W.; Li, C.Q.; Zhang, Z.F.; Zheng, W.J. Endoscopic transforaminal lumbar decompression, interbody fusion and pedicle screw fixation-a report of 42 cases. Chin. J. Traumatol. 2008, 11, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Choi, G.; Lee, S.H.; Bhanot, A.; Raiturker, P.P.; Chae, Y.S. Percutaneous endoscopic discectomy for extraforaminal lumbar disc herniations: Extraforaminal targeted fragmentectomy technique using working channel endoscope. Spine (Phila Pa 1976) 2007, 32, E93–E99. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.H.; Choi, M.; Ryu, D.S.; Choi, I.; Kim, C.H.; Kim, H.S.; Sohn, M.J. Efficacy and safety of full-endoscopic decompression via interlaminar approach for central or lateral recess spinal stenosis of the lumbar spine: A meta-analysis. Spine (Phila Pa 1976) 2018, 43, 1756–1764. [Google Scholar] [CrossRef]
- Heo, D.H.; Lee, D.C.; Park, C.K. Comparative analysis of three types of minimally invasive decompressive surgery for lumbar central stenosis: Biportal endoscopy, uniportal endoscopy, and microsurgery. Neurosurg. Focus 2019, 46, E9. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.-W.; Yoon, K.-J.; Ha, S.-S. Comparative analysis between three different lumbar decompression techniques (Microscopic, Tubular, and Endoscopic) in lumbar canal and lateral recess stenosis: Preliminary report. Biomed. Res. Int. 2019, 2019, 6078469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.J.; Wang, C.; Choi, K.H.; Kim, H.N. Use of a life-size three-dimensional-printed spine model for pedicle screw instrumentation training. J. Orthop. Surg. Res. 2018, 13, 86. [Google Scholar] [CrossRef] [PubMed]
- Gornet, M.; Buttermann, G.; Guyer, R.; Yue, J.; Ferko, N.; Hollmann, S. Defining the ideal lumbar total disc replacement patient and standard of care. Spine (Phila Pa 1976) 2017, 42 (Suppl. 24), S103–S107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, M.; Garcia, R.; Miller, L.; Reed, W.; Zigler, J.; Ferko, N.; Hollmann, S. Challenges and solutions for lumbar total disc replacement implantation. Spine (Phila Pa 1976) 2017, 42 (Suppl. 24), S108–S111. [Google Scholar] [CrossRef] [PubMed]
- Zigler, J.; Gornet, M.F.; Ferko, N.; Cameron, C.; Schranck, F.W.; Patel, L. Comparison of lumbar total disc replacement with surgical spinal fusion for the treatment of single-level degenerative disc disease: A meta-analysis of 5-year outcomes from randomized controlled trials. Glob. Spine J. 2018, 8, 413–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nie, H.; Chen, G.; Wang, X.; Zeng, J. Comparison of Total Disc Replacement with lumbar fusion: A meta-analysis of randomized controlled trials. J. Coll. Physicians Surg. Pak. 2015, 25, 60–67. [Google Scholar]
- Mu, X.; Wei, J.; A, J.; Li, Z.; Ou, Y. The short-term efficacy and safety of artificial total disc replacement for selected patients with lumbar degenerative disc disease compared with anterior lumbar interbody fusion: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0209660. [Google Scholar] [CrossRef]
- Kurd, M.; Cohick, S.; Park, A.; Ahmadinia, K.; Lee, J.; An, H. Fusion in degenerative spondylolisthesis: Comparison of osteoconductive and osteoinductive bone graft substitutes. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2015, 24, 1066–1073. [Google Scholar] [CrossRef]
- Vaccaro, A.R.; Patel, T.; Fischgrund, J.; Anderson, D.G.; Truumees, E.; Herkowitz, H.N.; Phillips, F.; Hilibrand, A.; Albert, T.J.; Wetzel, T.; et al. A pilot study evaluating the safety and efficacy of OP-1 Putty (rhBMP-7) as a replacement for iliac crest autograft in posterolateral lumbar arthrodesis for degenerative spondylolisthesis. Spine (Phila Pa 1976) 2004, 29, 1885–1892. [Google Scholar] [CrossRef]
- Rihn, J.A.; Kirkpatrick, K.; Albert, T.J. Graft options in posterolateral and posterior interbody lumbar fusion. Spine (Phila Pa 1976) 2010, 35, 1629–1639. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Zhu, Y.; Zhang, H.; Wang, C.; He, S.; Gu, G. Comparison of bilateral versus unilateral decompression incision of minimally invasive transforaminal lumbar interbody fusion in two-level degenerative lumbar diseases. Int. Orthop. 2018, 42, 2835–2842. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.J.; Han, Y.C.; Liu, X.M.; Ma, B.; Zhao, W.D.; Wu, D.S.; Tan, J. Fusion techniques for adult isthmic spondylolisthesis: A systematic review. Arch. Orthop. Trauma Surg. 2014, 134, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.T.; Yeung, C.A. Advances in endoscopic disc and spine surgery: Foraminal approach. Surg. Technol. Int. 2003, 11, 255–263. [Google Scholar] [PubMed]
- Wu, R.H.; Fraser, J.F.; Hartl, R. Minimal access versus open transforaminal lumbar interbody fusion: Meta-analysis of fusion rates. Spine (Phila Pa 1976) 2010, 35, 2273–2281. [Google Scholar] [CrossRef] [PubMed]
- Schonauer, C.; Stienen, M.N.; Gautschi, O.P.; Schaller, K.; Tessitore, E. Endoscope-assisted extreme-lateral interbody fusion: Preliminary experience and technical note. World Neurosurg. 2017, 103, 869–875. [Google Scholar] [CrossRef]
- Heo, D.H.; Kim, J.S. Clinical and radiological outcomes of spinal endoscopic discectomy-assisted oblique lumbar interbody fusion: Preliminary results. Neurosurg. Focus 2017, 43, E13. [Google Scholar] [CrossRef]
- Machado, G.C.; Ferreira, P.H.; Yoo, R.I.; Harris, I.A.; Pinheiro, M.B.; Koes, B.W.; van Tulder, M.W.; Rzewuska, M.; Maher, C.G.; Ferreira, M.L. Surgical options for lumbar spinal stenosis. Cochrane Database Syst. Rev. 2016, 11, CD012421. [Google Scholar] [CrossRef]
- Li, Y.; Sun, P.; Chen, D.; Tang, L.; Chen, C.; Wu, A. Artificial total disc replacement versus fusion for lumbar degenerative disc disease: An update systematic review and meta-analysis. Turk. Neurosurg. 2018. [Google Scholar] [CrossRef] [Green Version]
- Ding, F.; Jia, Z.; Zhao, Z.; Xie, L.; Gao, X.; Ma, D.; Liu, M. Total disc replacement versus fusion for lumbar degenerative disc disease: A systematic review of overlapping meta-analyses. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2017, 26, 806–815. [Google Scholar] [CrossRef]
- Vorhies, J.S.; Hernandez-Boussard, T.; Alamin, T. Treatment of degenerative lumbar spondylolisthesis with fusion or decompression alone results in similar rates of reoperation at 5 years. Clin. Spine Surg. 2018, 31, E74–E79. [Google Scholar] [CrossRef]
- Noshchenko, A.; Hoffecker, L.; Lindley, E.M.; Burger, E.L.; Cain, C.M.; Patel, V.V. Long-term treatment effects of lumbar arthrodeses in degenerative disk disease: A systematic review with meta-analysis. J. Spinal Disord. Tech. 2015, 28, E493–E521. [Google Scholar] [CrossRef] [PubMed]
- Harris, E.B.; Sayadipour, A.; Massey, P.; Duplantier, N.L.; Anderson, D.G. Mini-open versus open decompression and fusion for lumbar degenerative spondylolisthesis with stenosis. Am. J. Orthop. (Belle Mead NJ) 2011, 40, E257–E261. [Google Scholar] [PubMed]
- Heo, D.H.; Son, S.K.; Eum, J.H.; Park, C.K. Fully endoscopic lumbar interbody fusion using a percutaneous unilateral biportal endoscopic technique: Technical note and preliminary clinical results. Biomed. Res. Int. 2017, 43, E8. [Google Scholar] [CrossRef] [PubMed]
- McGrath, L.B.; White-Dzuro, G.A.; Hofstetter, C.P. Comparison of clinical outcomes following minimally invasive or lumbar endoscopic unilateral laminotomy for bilateral decompression. J. Neurosurg. Spine 2019, 30, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Kang, T.; Park, S.Y.; Kang, C.H.; Lee, S.H.; Park, J.H.; Suh, S.W. Is biportal technique/endoscopic spinal surgery satisfactory for lumbar spinal stenosis patients? A prospective randomized comparative study. Medicine (Baltim) 2019, 98, e15451. [Google Scholar] [CrossRef]








© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, P.H.; Kim, H.S.; Jang, I.-T. Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease. Int. J. Mol. Sci. 2020, 21, 2135. https://doi.org/10.3390/ijms21062135
Wu PH, Kim HS, Jang I-T. Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease. International Journal of Molecular Sciences. 2020; 21(6):2135. https://doi.org/10.3390/ijms21062135
Chicago/Turabian StyleWu, Pang Hung, Hyeun Sung Kim, and Il-Tae Jang. 2020. "Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease" International Journal of Molecular Sciences 21, no. 6: 2135. https://doi.org/10.3390/ijms21062135