
Pancreatic Ductal Adenocarcinoma: The Dawn of the Era of Nuclear Medicine?

 ,
,  , and
, and {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Radiotracers Clinically Available for PDAC Diagnosis, Staging and Monitoring
2.1. 18F-FDG
2.2. 18F-FLT
2.3. 18F-FMISO and 18F-FAZA
2.4. 68Ga-FAPI
3. Recent Developments in Nuclear Medicine for PDAC Imaging and Treatment
3.1. Radiotracers in Development Dedicated to Stroma Imaging
3.1.1. Fibronectin-Targeting Agents
3.1.2. MT1-MMP Imaging
3.1.3. CAFs
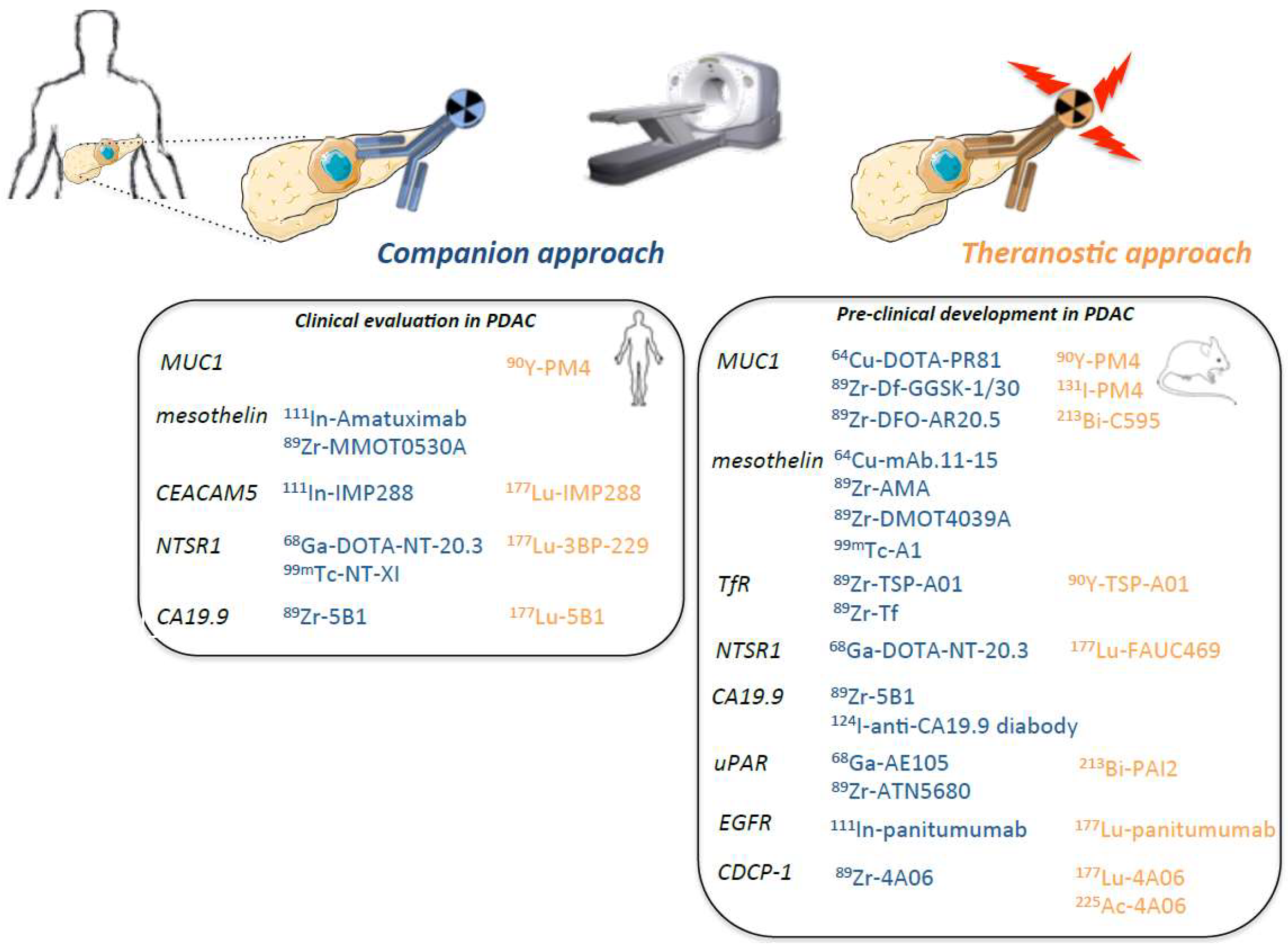
3.2. Radiotracers Targeting Tumor Antigen: Companion and Theranostic Approaches
3.2.1. MUC1-Targeting
3.2.2. Mesothelin-Targeting with Antibody-Derived Radiotracers
3.2.3. Transferrin Receptor (TfR)-Targeting Agents
3.2.4. CEACAM5-Targeting Agents
3.2.5. Neurotensin Receptor-Targeting Agents
3.2.6. CA19.9-Targeting Agents
3.2.7. uPA/uPAR System
3.2.8. EGFR
3.2.9. CDCP-1
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
Abbreviations
| CAF | Cancer-associated fibroblast |
| CA19.9 | Carbohydrate antigen19.9 |
| CDCP1 | CUB domain-containing protein1 |
| CEACAM5 | Carcinoembryonic antigen-related cell adhesion |
| EGFR | Epidermoid growth factor receptor |
| FAP | Fibroblast activating protein |
| FAPI | Fibroblast activating protein inhibitor |
| FAZA | Fluoroazomycin arabinoside |
| FDG | Fluorodeoxyglucose |
| FLT | Fluorothymidine |
| FMISO | Fluoromisonidazole |
| mAb | Monoclonal antibody |
| MMP | Matrix metalloproteinase |
| MRI | Magnetic resonance imaging |
| MUC1 | Mucin-1 |
| NTS | Neurotensin |
| OS | Overall survival |
| PAI2 | Plasminogen activator inhibitor-2 |
| PDAC | Pancreatic ductal adenocarcinoma |
| PET | Positron emission tomography |
| PFS | Progression-free survival |
| SdAb | Single-domain antibody |
| SPECT | Single-photon emission computed tomography |
| SUV | Standardized uptake value |
| TfR | Transferrin receptor |
| uPa | Urokinase-type plasminogen activator |
References
- Haeberle, L.; Esposito, I. Pathology of Pancreatic Cancer. Transl. Gastroenterol. Hepatol. 2019, 4. [Google Scholar] [CrossRef] [PubMed]
- Kleeff, J.; Korc, M.; Apte, M.; La Vecchia, C.; Johnson, C.D.; Biankin, A.V.; Neale, R.E.; Tempero, M.; Tuveson, D.A.; Hruban, R.H.; et al. Pancreatic Cancer. Nat. Rev. Dis. Primers 2016, 2, 16022. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef]
- Quante, A.S.; Ming, C.; Rottmann, M.; Engel, J.; Boeck, S.; Heinemann, V.; Westphalen, C.B.; Strauch, K. Projections of Cancer Incidence and Cancer-Related Deaths in Germany by 2020 and 2030. Cancer Med. 2016, 5, 2649–2656. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orth, M.; Metzger, P.; Gerum, S.; Mayerle, J.; Schneider, G.; Belka, C.; Schnurr, M.; Lauber, K. Pancreatic Ductal Adenocarcinoma: Biological Hallmarks, Current Status, and Future Perspectives of Combined Modality Treatment Approaches. Radiat. Oncol. 2019, 14, 141. [Google Scholar] [CrossRef] [PubMed]
- Manji, G.A.; Olive, K.P.; Saenger, Y.M.; Oberstein, P. Current and Emerging Therapies in Metastatic Pancreatic Cancer. Clin. Cancer Res. 2017, 23, 1670–1678. [Google Scholar] [CrossRef] [Green Version]
- Winter, K.; Talar-Wojnarowska, R.; Dąbrowski, A.; Degowska, M.; Durlik, M.; Gąsiorowska, A.; Głuszek, S.; Jurkowska, G.; Kaczka, A.; Lampe, P.; et al. Diagnostic and Therapeutic Recommendations in Pancreatic Ductal Adenocarcinoma. Recommendations of the Working Group of the Polish Pancreatic Club. Prz. Gastroenterol. 2019, 14, 1–18. [Google Scholar] [CrossRef]
- Bengtsson, A.; Andersson, R.; Ansari, D. The Actual 5-Year Survivors of Pancreatic Ductal Adenocarcinoma Based on Real-World Data. Sci. Rep. 2020, 10, 16425. [Google Scholar] [CrossRef] [PubMed]
- Michelassi, F.; Erroi, F.; Dawson, P.J.; Pietrabissa, A.; Noda, S.; Handcock, M.; Block, G.E. Experience with 647 Consecutive Tumors of the Duodenum, Ampulla, Head of the Pancreas, and Distal Common Bile Duct. Ann. Surg. 1989, 210, 544–556. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.-L.; Choné, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; Psarelli, E.E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; O’Reilly, D.A.; Cunningham, D.; Wadsley, J.; et al. Comparison of Adjuvant Gemcitabine and Capecitabine with Gemcitabine Monotherapy in Patients with Resected Pancreatic Cancer (ESPAC-4): A Multicentre, Open-Label, Randomised, Phase 3 Trial. Lancet 2017, 389, 1011–1024. [Google Scholar] [CrossRef]
- Adamska, A.; Domenichini, A.; Falasca, M. Pancreatic Ductal Adenocarcinoma: Current and Evolving Therapies. Int. J. Mol. Sci. 2017, 18, 1338. [Google Scholar] [CrossRef]
- Rhim, A.D.; Mirek, E.T.; Aiello, N.M.; Maitra, A.; Bailey, J.M.; McAllister, F.; Reichert, M.; Beatty, G.L.; Rustgi, A.K.; Vonderheide, R.H.; et al. EMT and Dissemination Precede Pancreatic Tumor Formation. Cell 2012, 148, 349–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yordanova, A.; Eppard, E.; Kürpig, S.; Bundschuh, R.A.; Schönberger, S.; Gonzalez-Carmona, M.; Feldmann, G.; Ahmadzadehfar, H.; Essler, M. Theranostics in Nuclear Medicine Practice. Onco Targets 2017, 10, 4821–4828. [Google Scholar] [CrossRef] [Green Version]
- Gomes Marin, J.F.; Nunes, R.F.; Coutinho, A.M.; Zaniboni, E.C.; Costa, L.B.; Barbosa, F.G.; Queiroz, M.A.; Cerri, G.G.; Buchpiguel, C.A. Theranostics in Nuclear Medicine: Emerging and Re-Emerging Integrated Imaging and Therapies in the Era of Precision Oncology. RadioGraphics 2020, 40, 1715–1740. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Emmett, L.; Violet, J.; Y Zhang, A.; Lawrence, N.J.; Stockler, M.; Francis, R.J.; Iravani, A.; Williams, S.; Azad, A.; et al. TheraP: A Randomized Phase 2 Trial of 177 Lu-PSMA-617 Theranostic Treatment vs Cabazitaxel in Progressive Metastatic Castration-Resistant Prostate Cancer (Clinical Trial Protocol ANZUP 1603). BJU Int. 2019, 124 (Suppl. 1), 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elbanna, K.Y.; Jang, H.-J.; Kim, T.K. Imaging Diagnosis and Staging of Pancreatic Ductal Adenocarcinoma: A Comprehensive Review. Insights Imaging 2020, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halbrook, C.J.; Lyssiotis, C.A. Employing Metabolism to Improve the Diagnosis and Treatment of Pancreatic Cancer. Cancer Cell 2017, 31, 5–19. [Google Scholar] [CrossRef] [Green Version]
- Cassim, S.; Raymond, V.-A.; Dehbidi-Assadzadeh, L.; Lapierre, P.; Bilodeau, M. Metabolic Reprogramming Enables Hepatocarcinoma Cells to Efficiently Adapt and Survive to a Nutrient-Restricted Microenvironment. Cell Cycle 2018, 17, 903–916. [Google Scholar] [CrossRef]
- Cassim, S.; Vučetić, M.; Ždralević, M.; Pouyssegur, J. Warburg and Beyond: The Power of Mitochondrial Metabolism to Collaborate or Replace Fermentative Glycolysis in Cancer. Cancers 2020, 12, 1119. [Google Scholar] [CrossRef]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM Procedure Guidelines for Tumour Imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Bryant, K.L.; Mancias, J.D.; Kimmelman, A.C.; Der, C.J. KRAS: Feeding Pancreatic Cancer Proliferation. Trends Biochem. Sci. 2014, 39, 91–100. [Google Scholar] [CrossRef] [Green Version]
- Pupo, E.; Avanzato, D.; Middonti, E.; Bussolino, F.; Lanzetti, L. KRAS-Driven Metabolic Rewiring Reveals Novel Actionable Targets in Cancer. Front. Oncol. 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Serrao, E.M.; Kettunen, M.I.; Rodrigues, T.B.; Dzien, P.; Wright, A.J.; Gopinathan, A.; Gallagher, F.A.; Lewis, D.Y.; Frese, K.K.; Almeida, J.; et al. MRI with Hyperpolarised [1-13C]Pyruvate Detects Advanced Pancreatic Preneoplasia Prior to Invasive Disease in a Mouse Model. Gut 2015, 65, 465–475. [Google Scholar] [CrossRef] [Green Version]
- Seufferlein, T.; Bachet, J.B.; Van Cutsem, E.; Rougier, P.; ESMO Guidelines Working Group. Pancreatic Adenocarcinoma: ESMO-ESDO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2012, 23 (Suppl. 7), vii33–vii40. [Google Scholar] [CrossRef]
- Yeh, R.; Dercle, L.; Garg, I.; Wang, Z.J.; Hough, D.M.; Goenka, A.H. The Role of 18F-FDG PET/CT and PET/MRI in Pancreatic Ductal Adenocarcinoma. Abdom. Radiol. 2018, 43, 415–434. [Google Scholar] [CrossRef]
- Best, L.M.; Rawji, V.; Pereira, S.P.; Davidson, B.R.; Gurusamy, K.S. Imaging Modalities for Characterising Focal Pancreatic Lesions. Cochrane Database Syst. Rev. 2017, 4, CD010213. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, I.; Shirakawa, S.; Shinzeki, M.; Asari, S.; Goto, T.; Ajiki, T.; Fukumoto, T.; Kitajima, K.; Ku, Y. 18-Fluorodeoxyglucose Positron Emission Tomography Does Not Aid in Diagnosis of Pancreatic Ductal Adenocarcinoma. Clin. Gastroenterol. Hepatol. 2013, 11, 712–718. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; O, J.H.; Choi, M.; Choi, J.Y. Impact of F-18 Fluorodeoxyglucose PET/CT and PET/MRI on Initial Staging and Changes in Management of Pancreatic Ductal Adenocarcinoma: A Systemic Review and Meta-Analysis. Diagnostics 2020, 10, 952. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, M.; Sato, T.; Furuya, T.; Shibata, S.; Andoh, H.; Asanuma, Y.; Hatazawa, J.; Shimosegawa, E.; Koyama, K.; Yamamoto, Y. Role of Positron Emission Tomography with 2-Deoxy-2-[18F]Fluoro-D-Glucose in Evaluating the Effects of Arterial Infusion Chemotherapy and Radiotherapy on Pancreatic Cancer. J. Gastroenterol. 2004, 39, 50–55. [Google Scholar] [CrossRef]
- Jain, R.K.; Lee, J.J.; Ng, C.; Hong, D.; Gong, J.; Naing, A.; Wheler, J.; Kurzrock, R. Change in Tumor Size by RECIST Correlates Linearly With Overall Survival in Phase I Oncology Studies. J. Clin. Oncol. 2012, 30, 2684–2690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokose, T.; Kitago, M.; Matsusaka, Y.; Masugi, Y.; Shinoda, M.; Yagi, H.; Abe, Y.; Oshima, G.; Hori, S.; Endo, Y.; et al. Usefulness of 18F-fluorodeoxyglucose Positron Emission Tomography/Computed Tomography for Predicting the Prognosis and Treatment Response of Neoadjuvant Therapy for Pancreatic Ductal Adenocarcinoma. Cancer Med. 2020, 9, 4059–4068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperti, C.; Pasquali, C.; Bissoli, S.; Chierichetti, F.; Liessi, G.; Pedrazzoli, S. Tumor Relapse after Pancreatic Cancer Resection Is Detected Earlier by 18-FDG PET than by CT. J. Gastrointest. Surg. 2010, 14, 131–140. [Google Scholar] [CrossRef]
- Wang, L.; Dong, P.; Wang, W.; Li, M.; Hu, W.; Liu, X.; Tian, B. Early Recurrence Detected by 18F-FDG PET/CT in Patients with Resected Pancreatic Ductal Adenocarcinoma. Medicine 2020, 99, e19504. [Google Scholar] [CrossRef]
- Javery, O.; Shyn, P.; Mortele, K. FDG PET or PET/CT in Patients with Pancreatic Cancer: When Does it Add to Diagnostic CT or MRI? Clin. Imaging 2013, 37, 295–301. [Google Scholar] [CrossRef]
- Yamamoto, T.; Sugiura, T.; Mizuno, T.; Okamura, Y.; Aramaki, T.; Endo, M.; Uesaka, K. Preoperative FDG-PET Predicts Early Recurrence and a Poor Prognosis after Resection of Pancreatic Adenocarcinoma. Ann. Surg. Oncol. 2015, 22, 677–684. [Google Scholar] [CrossRef]
- Moon, S.Y.; Joo, K.R.; So, Y.R.; Lim, J.U.; Cha, J.M.; Shin, H.P.; Yang, Y.-J. Predictive Value of Maximum Standardized Uptake Value (SUVmax) on 18F-FDG PET/CT in Patients with Locally Advanced or Metastatic Pancreatic Cancer. Clin. Nucl. Med. 2013, 38, 778–783. [Google Scholar] [CrossRef]
- Pimiento, J.M.; Davis-Yadley, A.H.; Kim, R.D.; Chen, D.-T.; Eikman, E.A.; Berman, C.G.; Malafa, M.P. Metabolic Activity by (18)F-FDG-PET/CT Is Prognostic for Stage I and II Pancreatic Cancer. Clin. Nucl. Med. 2016, 41, 177–181. [Google Scholar] [CrossRef] [Green Version]
- Bollineni, V.R.; Kramer, G.M.; Jansma, E.P.; Liu, Y.; Oyen, W.J.G. A Systematic Review on [18F]FLT-PET Uptake as a Measure of Treatment Response in Cancer Patients. Eur. J. Cancer 2016, 55, 81–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Forstner, C.; Egberts, J.H.; Ammerpohl, O.; Niedzielska, D.; Buchert, R.; Mikecz, P.; Schumacher, U.; Peldschus, K.; Adam, G.; Pilarsky, C.; et al. Gene Expression Patterns and Tumor Uptake of 18F-FDG, 18F-FLT, and 18F-FEC in PET/MRI of an Orthotopic Mouse Xenotransplantation Model of Pancreatic Cancer. J. Nucl. Med. 2008, 49, 1362–1370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrmann, K.; Eckel, F.; Schmidt, S.; Scheidhauer, K.; Krause, B.J.; Kleeff, J.; Schuster, T.; Wester, H.-J.; Friess, H.; Schmid, R.M.; et al. In Vivo Characterization of Proliferation for Discriminating Cancer from Pancreatic Pseudotumors. J. Nucl. Med. 2008, 49, 1437–1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quon, A.; Chang, S.T.; Chin, F.; Kamaya, A.; Dick, D.W.; Loo, B.W.; Gambhir, S.S.; Koong, A.C. Initial Evaluation of 18F-Fluorothymidine (FLT) PET/CT Scanning for Primary Pancreatic Cancer. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 527–531. [Google Scholar] [CrossRef] [Green Version]
- Wieder, H.; Beer, A.J.; Siveke, J.; Schuster, T.; Buck, A.K.; Herrmann, K.; Stollfuss, J.C. 18F-Fluorothymidine PET for Predicting Survival in Patients with Resectable Pancreatic Cancer. Oncotarget 2018, 9, 10128–10134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muz, B.; de la Puente, P.; Azab, F.; Azab, A.K. The Role of Hypoxia in Cancer Progression, Angiogenesis, Metastasis, and Resistance to Therapy. Hypoxia 2015, 3, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Gaustad, J.-V.; Simonsen, T.G.; Wegner, C.S.; Rofstad, E.K. Vascularization, Oxygenation, and the Effect of Sunitinib Treatment in Pancreatic Ductal Adenocarcinoma Xenografts. Front. Oncol. 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.; Gao, S.; Ren, H.; Sun, W.; Zhang, H.; Sun, J.; Yang, S.; Hao, J. Hypoxia-Inducible Factor-1 Promotes Pancreatic Ductal Adenocarcinoma Invasion and Metastasis by Activating Transcription of the Actin-Bundling Protein Fascin. Cancer Res. 2014, 74, 2455–2464. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, Y.; Ding, Q.; Desaki, R.; Maemura, K.; Mataki, Y.; Shinchi, H.; Natsugoe, S.; Takao, S. Hypoxia Inducible Factor-1 Alpha Plays a Pivotal Role in Hepatic Metastasis of Pancreatic Cancer: An Immunohistochemical Study. J. Hepatobiliary Pancreat Sci. 2014, 21, 105–112. [Google Scholar] [CrossRef]
- Metran-Nascente, C.; Yeung, I.; Vines, D.C.; Metser, U.; Dhani, N.C.; Green, D.; Milosevic, M.; Jaffray, D.; Hedley, D.W. Measurement of Tumor Hypoxia in Patients with Advanced Pancreatic Cancer Based on 18F-Fluoroazomyin Arabinoside Uptake. J. Nucl. Med. 2016, 57, 361–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segard, T.; Robins, P.D.; Yusoff, I.F.; Ee, H.; Morandeau, L.; Campbell, E.M.; Francis, R.J. Detection of Hypoxia with 18F-Fluoromisonidazole (18F-FMISO) PET/CT in Suspected or Proven Pancreatic Cancer. Clin. Nucl. Med. 2013, 38, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Yamane, T.; Aikawa, M.; Yasuda, M.; Fukushima, K.; Seto, A.; Okamoto, K.; Koyama, I.; Kuji, I. [18F]FMISO PET/CT as a Preoperative Prognostic Factor in Patients with Pancreatic Cancer. EJNMMI Res. 2019, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siveke, J.T. Fibroblast-Activating Protein: Targeting the Roots of the Tumor Microenvironment. J. Nucl. Med. 2018, 59, 1412–1414. [Google Scholar] [CrossRef]
- Loktev, A.; Lindner, T.; Mier, W.; Debus, J.; Altmann, A.; Jäger, D.; Giesel, F.; Kratochwil, C.; Barthe, P.; Roumestand, C.; et al. A Tumor-Imaging Method Targeting Cancer-Associated Fibroblasts. J. Nucl. Med. 2018, 59, 1423–1429. [Google Scholar] [CrossRef]
- Kratochwil, C.; Flechsig, P.; Lindner, T.; Abderrahim, L.; Altmann, A.; Mier, W.; Adeberg, S.; Rathke, H.; Röhrich, M.; Winter, H.; et al. 68Ga-FAPI PET/CT: Tracer Uptake in 28 Different Kinds of Cancer. J. Nucl. Med. 2019, 60, 801–805. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Zhao, L.; Hao, B.; Sun, L.; Jacobson, O.; Wu, H. Comparison of 68Ga-FAPI and 18F-FDG PET/CT for Detection, Staging, and Restaging of Various Kinds of Cancer. J. Nucl. Med. 2020, 61, 625. [Google Scholar]
- Röhrich, M.; Naumann, P.; Giesel, F.L.; Choyke, P.; Staudinger, F.; Wefers, A.; Liew, D.P.; Kratochwil, C.; Rathke, H.; Liermann, J.; et al. Impact of 68Ga-FAPI-PET/CT Imaging on the Therapeutic Management of Primary and Recurrent Pancreatic Ductal Adenocarcinomas. J. Nucl. Med. 2020. [Google Scholar] [CrossRef]
- Liermann, J.; Syed, M.; Ben-Josef, E.; Schubert, K.; Schlampp, I.; Sprengel, S.D.; Ristau, J.; Weykamp, F.; Röhrich, M.; Koerber, S.A.; et al. Impact of FAPI-PET/CT on Target Volume Definition in Radiation Therapy of Locally Recurrent Pancreatic Cancer. Cancers 2021, 13, 796. [Google Scholar] [CrossRef]
- Loktev, A.; Lindner, T.; Burger, E.-M.; Altmann, A.; Giesel, F.; Kratochwil, C.; Debus, J.; Marme, F.; Jaeger, D.; Mier, W.; et al. Development of Novel FAP-Targeted Radiotracers with Improved Tumor Retention. J. Nucl. Med. 2019. [Google Scholar] [CrossRef]
- Sperb, N.; Tsesmelis, M.; Wirth, T. Crosstalk between Tumor and Stromal Cells in Pancreatic Ductal Adenocarcinoma. Int. J. Mol. Sci. 2020, 21, 5486. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Ansari, D.; Zhou, Q.; Sasor, A.; Said Hilmersson, K.; Andersson, R. Stromal Fibronectin Expression in Patients with Resected Pancreatic Ductal Adenocarcinoma. World J. Surg. Oncol. 2019, 17. [Google Scholar] [CrossRef] [PubMed]
- Jailkhani, N.; Ingram, J.R.; Rashidian, M.; Rickelt, S.; Tian, C.; Mak, H.; Jiang, Z.; Ploegh, H.L.; Hynes, R.O. Noninvasive Imaging of Tumor Progression, Metastasis, and Fibrosis Using a Nanobody Targeting the Extracellular Matrix. Proc. Natl. Acad. Sci. USA 2019, 116, 14181–14190. [Google Scholar] [CrossRef] [Green Version]
- Slapak, E.J.; Duitman, J.; Tekin, C.; Bijlsma, M.F.; Spek, C.A. Matrix Metalloproteases in Pancreatic Ductal Adenocarcinoma: Key Drivers of Disease Progression? Biology 2020, 9, 80. [Google Scholar] [CrossRef] [Green Version]
- Dangi-Garimella, S.; Krantz, S.B.; Barron, M.R.; Shields, M.A.; Heiferman, M.J.; Grippo, P.J.; Bentrem, D.J.; Munshi, H.G. Three-Dimensional Collagen I Promotes Gemcitabine Resistance in Pancreatic Cancer through MT1-MMP-Mediated Expression of HMGA2. Cancer Res. 2011, 71, 1019–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morcillo, M.Á.; García de Lucas, Á.; Oteo, M.; Romero, E.; Magro, N.; Ibáñez, M.; Martínez, A.; Garaulet, G.; Arroyo, A.G.; López-Casas, P.P.; et al. MT1-MMP as a PET Imaging Biomarker for Pancreas Cancer Management. Contrast Media Mol. Imaging 2018, 2018, 8382148. [Google Scholar] [CrossRef] [PubMed]
- Koustoulidou, S.; Hoorens, M.W.H.; Dalm, S.U.; Mahajan, S.; Debets, R.; Seimbille, Y.; de Jong, M. Cancer-Associated Fibroblasts as Players in Cancer Development and Progression and Their Role in Targeted Radionuclide Imaging and Therapy. Cancers 2021, 13, 1100. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.J.; Alpaugh, R.K.; Palazzo, I.; Meropol, N.J.; Rogatko, A.; Xu, Z.; Hoffman, J.P.; Weiner, L.M.; Cheng, J.D. Fibroblast Activation Protein and Its Relationship to Clinical Outcome in Pancreatic Adenocarcinoma. Pancreas 2008, 37, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Watabe, T.; Liu, Y.; Kaneda-Nakashima, K.; Shirakami, Y.; Lindner, T.; Ooe, K.; Toyoshima, A.; Nagata, K.; Shimosegawa, E.; Haberkorn, U.; et al. Theranostics Targeting Fibroblast Activation Protein in the Tumor Stroma: 64Cu- and 225Ac-Labeled FAPI-04 in Pancreatic Cancer Xenograft Mouse Models. J. Nucl. Med. 2020, 61, 563–569. [Google Scholar] [CrossRef]
- Lindner, T.; Loktev, A.; Altmann, A.; Giesel, F.; Kratochwil, C.; Debus, J.; Jäger, D.; Mier, W.; Haberkorn, U. Development of Quinoline-Based Theranostic Ligands for the Targeting of Fibroblast Activation Protein. J. Nucl. Med. 2018, 59, 1415–1422. [Google Scholar] [CrossRef] [Green Version]
- Suh, H.; Pillai, K.; Morris, D.L. Mucins in Pancreatic Cancer: Biological Role, Implications in Carcinogenesis and Applications in Diagnosis and Therapy. Am. J. Cancer Res. 2017, 7, 1372–1383. [Google Scholar]
- Wang, S.; You, L.; Dai, M.; Zhao, Y. Mucins in Pancreatic Cancer: A Well-Established but Promising Family for Diagnosis, Prognosis and Therapy. J. Cell. Mol. Med. 2020, 24, 10279–10289. [Google Scholar] [CrossRef] [PubMed]
- Tréhoux, S.; Duchêne, B.; Jonckheere, N.; Van Seuningen, I. The MUC1 Oncomucin Regulates Pancreatic Cancer Cell Biological Properties and Chemoresistance. Implication of P42-44 MAPK, Akt, Bcl-2 and MMP13 Pathways. Biochem. Biophys. Res. Commun. 2015, 456, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Nath, S.; Roy, L.D.; Grover, P.; Rao, S.; Mukherjee, P. Mucin 1 Regulates Cox-2 Gene in Pancreatic Cancer. Pancreas 2015, 44, 909–917. [Google Scholar] [CrossRef] [Green Version]
- Nath, S.; Daneshvar, K.; Roy, L.D.; Grover, P.; Kidiyoor, A.; Mosley, L.; Sahraei, M.; Mukherjee, P. MUC1 Induces Drug Resistance in Pancreatic Cancer Cells via Upregulation of Multidrug Resistance Genes. Oncogenesis 2013, 2, e51. [Google Scholar] [CrossRef] [Green Version]
- Yokoyama, S.; Hamada, T.; Higashi, M.; Matsuo, K.; Maemura, K.; Kurahara, H.; Horinouchi, M.; Hiraki, T.; Sugimoto, T.; Akahane, T.; et al. Predicted Prognosis of Patients with Pancreatic Cancer by Machine Learning. Clin. Cancer Res. 2020, 26, 2411–2421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alirezapour, B.; Rasaee, M.J.; Jalilian, A.R.; Rajabifar, S.; Mohammadnejad, J.; Paknejad, M.; Maadi, E.; Moradkhani, S. Development of [64Cu]-DOTA-PR81 Radioimmunoconjugate for MUC-1 Positive PET Imaging. Nucl. Med. Biol 2016, 43, 73–80. [Google Scholar] [CrossRef]
- Stergiou, N.; Nagel, J.; Pektor, S.; Heimes, A.-S.; Jäkel, J.; Brenner, W.; Schmidt, M.; Miederer, M.; Kunz, H.; Roesch, F.; et al. Evaluation of a Novel Monoclonal Antibody against Tumor-Associated MUC1 for Diagnosis and Prognosis of Breast Cancer. Int. J. Med. Sci. 2019, 16, 1188–1198. [Google Scholar] [CrossRef] [Green Version]
- Fung, K.; Vivier, D.; Keinänen, O.; Sarbisheh, E.K.; Price, E.W.; Zeglis, B.M. 89Zr-Labeled AR20.5: A MUC1-Targeting ImmunoPET Probe. Molecules 2020, 25, 2315. [Google Scholar] [CrossRef]
- Hull, A.; Li, Y.; Bartholomeusz, D.; Hsieh, W.; Allen, B.; Bezak, E. Radioimmunotherapy of Pancreatic Ductal Adenocarcinoma: A Review of the Current Status of Literature. Cancers 2020, 12, 481. [Google Scholar] [CrossRef] [Green Version]
- Cardillo, T.M.; Ying, Z.; Gold, D.V. Therapeutic Advantage of (90)Yttrium- versus (131)Iodine-Labeled PAM4 Antibody in Experimental Pancreatic Cancer. Clin. Cancer Res. 2001, 7, 3186–3192. [Google Scholar]
- Gold, D.V.; Modrak, D.E.; Schutsky, K.; Cardillo, T.M. Combined 90Yttrium-DOTA-Labeled PAM4 Antibody Radioimmunotherapy and Gemcitabine Radiosensitization for the Treatment of a Human Pancreatic Cancer Xenograft. Int. J. Cancer 2004, 109, 618–626. [Google Scholar] [CrossRef]
- Gulec, S.A.; Cohen, S.J.; Pennington, K.L.; Zuckier, L.S.; Hauke, R.J.; Horne, H.; Wegener, W.A.; Teoh, N.; Gold, D.V.; Sharkey, R.M.; et al. Treatment of Advanced Pancreatic Carcinoma with 90Y-Clivatuzumab Tetraxetan: A Phase I Single-Dose Escalation Trial. Clin. Cancer Res. 2011, 17, 4091–4100. [Google Scholar] [CrossRef] [Green Version]
- Ocean, A.J.; Pennington, K.L.; Guarino, M.J.; Sheikh, A.; Bekaii-Saab, T.; Serafini, A.N.; Lee, D.; Sung, M.W.; Gulec, S.A.; Goldsmith, S.J.; et al. Fractionated Radioimmunotherapy with (90) Y-Clivatuzumab Tetraxetan and Low-Dose Gemcitabine Is Active in Advanced Pancreatic Cancer: A Phase 1 Trial. Cancer 2012, 118, 5497–5506. [Google Scholar] [CrossRef] [Green Version]
- Marcu, L.; Bezak, E.; Allen, B.J. Global Comparison of Targeted Alpha vs Targeted Beta Therapy for Cancer: In Vitro, in Vivo and Clinical Trials. Crit. Rev. Oncol. Hematol. 2018, 123, 7–20. [Google Scholar] [CrossRef]
- Qu, C.F.; Li, Y.; Song, Y.J.; Rizvi, S.M.A.; Raja, C.; Zhang, D.; Samra, J.; Smith, R.; Perkins, A.C.; Apostolidis, C.; et al. MUC1 Expression in Primary and Metastatic Pancreatic Cancer Cells for in Vitro Treatment by (213)Bi-C595 Radioimmunoconjugate. Br. J. Cancer 2004, 91, 2086–2093. [Google Scholar] [CrossRef] [Green Version]
- Song, E.Y.; Qu, C.F.; Rizvi, S.M.A.; Raja, C.; Beretov, J.; Morgenstern, A.; Apostolidis, C.; Bruchertseifer, F.; Perkins, A.; Allen, B.J. Bismuth-213 Radioimmunotherapy with C595 Anti-MUC1 Monoclonal Antibody in an Ovarian Cancer Ascites Model. Cancer Biol. 2008, 7, 76–80. [Google Scholar] [CrossRef] [Green Version]
- Nichetti, F.; Marra, A.; Corti, F.; Guidi, A.; Raimondi, A.; Prinzi, N.; de Braud, F.; Pusceddu, S. The Role of Mesothelin as a Diagnostic and Therapeutic Target in Pancreatic Ductal Adenocarcinoma: A Comprehensive Review. Target. Oncol. 2018, 13, 333–351. [Google Scholar] [CrossRef]
- Montemagno, C.; Cassim, S.; Trichanh, D.; Savary, C.; Pouyssegur, J.; Pagès, G.; Fagret, D.; Broisat, A.; Ghezzi, C. 99mTc-A1 as a Novel Imaging Agent Targeting Mesothelin-Expressing Pancreatic Ductal Adenocarcinoma. Cancers 2019, 11, 1531. [Google Scholar] [CrossRef] [Green Version]
- Hassan, R.; Thomas, A.; Alewine, C.; Le, D.T.; Jaffee, E.M.; Pastan, I. Mesothelin Immunotherapy for Cancer: Ready for Prime Time? J. Clin. Oncol. 2016, 34, 4171–4179. [Google Scholar] [CrossRef] [Green Version]
- Montemagno, C.; Cassim, S.; Pouyssegur, J.; Broisat, A.; Pagès, G. From Malignant Progression to Therapeutic Targeting: Current Insights of Mesothelin in Pancreatic Ductal Adenocarcinoma. Int. J. Mol. Sci. 2020, 21, 4067. [Google Scholar] [CrossRef]
- Kobayashi, K.; Sasaki, T.; Takenaka, F.; Yakushiji, H.; Fujii, Y.; Kishi, Y.; Kita, S.; Shen, L.; Kumon, H.; Matsuura, E. A Novel PET Imaging Using 64Cu-Labeled Monoclonal Antibody against Mesothelin Commonly Expressed on Cancer Cells. J. Immunol. Res. 2015, 2015, 268172. [Google Scholar] [CrossRef] [Green Version]
- ter Weele, E.J.; Terwisscha van Scheltinga, A.G.T.; Kosterink, J.G.W.; Pot, L.; Vedelaar, S.R.; Lamberts, L.E.; Williams, S.P.; Lub-de Hooge, M.N.; de Vries, E.G.E. Imaging the Distribution of an Antibody-Drug Conjugate Constituent Targeting Mesothelin with 89Zr and IRDye 800CW in Mice Bearing Human Pancreatic Tumor Xenografts. Oncotarget 2015, 6, 42081–42090. [Google Scholar] [CrossRef] [Green Version]
- van Scheltinga, A.G.T.T.; Ogasawara, A.; Pacheco, G.; Vanderbilt, A.N.; Tinianow, J.N.; Gupta, N.; Li, D.; Firestein, R.; Marik, J.; Scales, S.J.; et al. Preclinical Efficacy of an Antibody-Drug Conjugate Targeting Mesothelin Correlates with Quantitative89 Zr-ImmunoPET. Mol. Cancer Ther. 2017, 16, 134–142. [Google Scholar] [CrossRef] [Green Version]
- Lamberts, T.E.; Menke-van der Houven, C.W.; Weele, E.J.T.; Bensch, F.; Smeenk, M.M.; Voortman, J.; Hoekstra, O.S.; Williams, S.P.; Fine, B.M.; Maslyar, D.; et al. ImmunoPET with Anti-Mesothelin Antibody in Patients with Pancreatic and Ovarian Cancer before Anti-Mesothelin Antibody-Drug Conjugate Treatment. Clin. Cancer Res. 2015, 22, 1642–1652. [Google Scholar] [CrossRef] [Green Version]
- Lindenberg, L.; Thomas, A.; Adler, S.; Mena, E.; Kurdziel, K.; Maltzman, J.; Wallin, B.; Hoffman, K.; Pastan, I.; Paik, C.H.; et al. Safety and Biodistribution of 111In-Amatuximab in Patients with Mesothelin Expressing Cancers Using Single Photon Emission Computed Tomography-Computed Tomography (SPECT-CT) Imaging. Oncotarget 2015, 6, 4496–4504. [Google Scholar] [CrossRef] [Green Version]
- Montemagno, C.; Bacot, S.; Ahmadi, M.; Kerfelec, B.; Baty, D.; Debiossat, M.; Soubies, A.; Perret, P.; Riou, L.; Fagret, D.; et al. Preclinical Evaluation of Mesothelin-Specific Ligands for SPECT Imaging of Triple-Negative Breast Cancer. J. Nucl. Med. 2018, 59, 1056–1062. [Google Scholar] [CrossRef]
- Yakushiji, H.; Kobayashi, K.; Takenaka, F.; Kishi, Y.; Shinohara, M.; Akehi, M.; Sasaki, T.; Ohno, E.; Matsuura, E. Novel Single-chain Variant of Antibody against Mesothelin Established by Phage Library. Cancer Sci. 2019, 110, 2722–2733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wickstroem, K.; Hagemann, U.B.; Cruciani, V.; Wengner, A.M.; Kristian, A.; Ellingsen, C.; Siemeister, G.; Bjerke, R.M.; Karlsson, J.; Ryan, O.B.; et al. Synergistic Effect of a Mesothelin-Targeted 227Th Conjugate in Combination with DNA Damage Response Inhibitors in Ovarian Cancer Xenograft Models. J. Nucl. Med. 2019, 60, 1293–1300. [Google Scholar] [CrossRef] [Green Version]
- Torti, S.V.; Torti, F.M. Iron: The Cancer Connection. Mol. Asp. Med. 2020, 75, 100860. [Google Scholar] [CrossRef]
- Basuli, D.; Tesfay, L.; Deng, Z.; Paul, B.; Yamamoto, Y.; Ning, G.; Xian, W.; McKeon, F.; Lynch, M.; Crum, C.P.; et al. Iron Addiction: A Novel Therapeutic Target in Ovarian Cancer. Oncogene 2017, 36, 4089–4099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatter, K.C.; Brown, G.; Trowbridge, I.S.; Woolston, R.E.; Mason, D.Y. Transferrin Receptors in Human Tissues: Their Distribution and Possible Clinical Relevance. J. Clin. Pathol 1983, 36, 539–545. [Google Scholar] [CrossRef] [Green Version]
- Shen, Y.; Li, X.; Dong, D.; Zhang, B.; Xue, Y.; Shang, P. Transferrin Receptor 1 in Cancer: A New Sight for Cancer Therapy. Am. J. Cancer Res. 2018, 8, 916–931. [Google Scholar]
- Daniels-Wells, T.R.; Penichet, M.L. Transferrin Receptor 1: A Target for Antibody-Mediated Cancer Therapy. Immunotherapy 2016, 8, 991–994. [Google Scholar] [CrossRef] [Green Version]
- Luria-Pérez, R.; Helguera, G.; Rodríguez, J.A. Antibody-Mediated Targeting of the Transferrin Receptor in Cancer Cells. Boletín Médico Hosp. Infant. México 2016, 73, 372–379. [Google Scholar] [CrossRef]
- Pirollo, K.F.; Nemunaitis, J.; Leung, P.K.; Nunan, R.; Adams, J.; Chang, E.H. Safety and Efficacy in Advanced Solid Tumors of a Targeted Nanocomplex Carrying the P53 Gene Used in Combination with Docetaxel: A Phase 1b Study. Mol. Ther. 2016, 24, 1697–1706. [Google Scholar] [CrossRef] [Green Version]
- Sugyo, A.; Tsuji, A.B.; Sudo, H.; Nagatsu, K.; Koizumi, M.; Ukai, Y.; Kurosawa, G.; Zhang, M.R.; Kurosawa, Y.; Saga, T. Preclinical Evaluation of 89Zr-Labeled Human Antitransferrin Receptor Monoclonal Antibody as a PET Probe Using a Pancreatic Cancer Mouse Model. Nucl. Med. Commun. 2015, 36, 286–294. [Google Scholar] [CrossRef]
- Sugyo, A.; Tsuji, A.B.; Sudo, H.; Okada, M.; Koizumi, M.; Satoh, H.; Kurosawa, G.; Kurosawa, Y.; Saga, T. Evaluation of Efficacy of Radioimmunotherapy with 90Y-Labeled Fully Human Anti-Transferrin Receptor Monoclonal Antibody in Pancreatic Cancer Mouse Models. PLloS ONE 2015, 10, e0123761. [Google Scholar] [CrossRef] [Green Version]
- Henry, K.; Dacek, M.; Dilling, T.; Caen, J.; Evans, M.; Lewis, J. Interrogating KRAS, ERK, and MYC Signaling in Pancreatic Cancer with Endogenous PET Imaging. J. Nucl. Med. 2018, 59, 72. [Google Scholar]
- Henry, K.E.; Dacek, M.M.; Dilling, T.R.; Caen, J.D.; Fox, I.L.; Evans, M.J.; Lewis, J.S. A PET Imaging Strategy for Interrogating Target Engagement and Oncogene Status in Pancreatic Cancer. Clin. Cancer Res. 2019, 25, 166–176. [Google Scholar] [CrossRef] [Green Version]
- Zhou, G.; Liu, X.; Wang, X.; Jin, D.; Chen, Y.; Li, G.; Li, C.; Fu, D.; Xu, W.; Wang, X. Combination of Preoperative CEA and CA19-9 Improves Prediction Outcomes in Patients with Resectable Pancreatic Adenocarcinoma: Results from a Large Follow-up Cohort. OncoTargets Ther. 2017, 10, 1199–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni, X.G.; Bai, X.F.; Mao, Y.L.; Shao, Y.F.; Wu, J.X.; Shan, Y.; Wang, C.F.; Wang, J.; Tian, Y.T.; Liu, Q.; et al. The Clinical Value of Serum CEA, CA19-9, and CA242 in the Diagnosis and Prognosis of Pancreatic Cancer. Eur. J. Surg. Oncol. 2005, 31, 164–169. [Google Scholar] [CrossRef]
- Vuijk, F.A.; de Muynck, L.D.A.N.; Franken, L.C.; Busch, O.R.; Wilmink, J.W.; Besselink, M.G.; Bonsing, B.A.; Bhairosingh, S.S.; Kuppen, P.J.K.; Mieog, J.S.D.; et al. Molecular Targets for Diagnostic and Intraoperative Imaging of Pancreatic Ductal Adenocarcinoma after Neoadjuvant FOLFIRINOX Treatment. Sci. Rep. 2020, 10, 16211. [Google Scholar] [CrossRef]
- Schoffelen, R.; Boerman, O.C.; Goldenberg, D.M.; Sharkey, R.M.; van Herpen, C.M.L.; Franssen, G.M.; McBride, W.J.; Chang, C.-H.; Rossi, E.A.; van der Graaf, W.T.A.; et al. Development of an Imaging-Guided CEA-Pretargeted Radionuclide Treatment of Advanced Colorectal Cancer: First Clinical Results. Br. J. Cancer 2013, 109, 934–942. [Google Scholar] [CrossRef] [Green Version]
- Reubi, J.; Waser, B.; Friess, H.; Buchler, M.; Laissue, J. Neurotensin Receptors: A New Marker for Human Ductal Pancreatic Adenocarcinoma. Gut 1998, 42, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-G.; Li, N.-N.; Li, H.-N.; Cui, L.; Wang, P. Pancreatic Cancer Bears Overexpression of Neurotensin and Neurotensin Receptor Subtype-1 and SR 48692 Counteracts Neurotensin Induced Cell Proliferation in Human Pancreatic Ductal Carcinoma Cell Line PANC-1. Neuropeptides 2011, 45, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Körner, M.; Waser, B.; Strobel, O.; Büchler, M.; Reubi, J.C. Neurotensin Receptors in Pancreatic Ductal Carcinomas. EJNMMI Res. 2015, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christou, N.; Blondy, S.; David, V.; Verdier, M.; Lalloué, F.; Jauberteau, M.-O.; Mathonnet, M.; Perraud, A. Neurotensin Pathway in Digestive Cancers and Clinical Applications: An Overview. Cell Death Dis. 2020, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, Q.; Zhou, J.; Yang, W.; Cui, H.; Xu, M.; Yi, L. Oncogenic Role of Neurotensin and Neurotensin Receptors in Various Cancers. Clin. Exp. Pharmacol. Physiol. 2017, 44, 841–846. [Google Scholar] [CrossRef] [Green Version]
- El Masri, R.; Delon, J. RHO GTPases: From New Partners to Complex Immune Syndromes. Nat. Rev. Immunol. 2021. [Google Scholar] [CrossRef]
- Megrelis, L.; El Ghoul, E.; Moalli, F.; Versapuech, M.; Cassim, S.; Ruef, N.; Stein, J.V.; Mangeney, M.; Delon, J. Fam65b Phosphorylation Relieves Tonic RhoA Inhibition During T Cell Migration. Front. Immunol. 2018, 9, 2001. [Google Scholar] [CrossRef]
- Takahashi, K.; Ehata, S.; Miyauchi, K.; Morishita, Y.; Miyazawa, K.; Miyazono, K. Neurotensin Receptor 1 Signaling Promotes Pancreatic Cancer Progression. Mol. Oncol. 2021, 15, 151–166. [Google Scholar] [CrossRef]
- Hodolic, M.; Ambrosini, V.; Fanti, S. Potential Use of Radiolabelled Neurotensin in PET Imaging and Therapy of Patients with Pancreatic Cancer. Nucl. Med. Commun. 2020, 41, 411–415. [Google Scholar] [CrossRef]
- Marenco, M.; Lodola, L.; Persico, M.G.; Frangipane, V.; Facoetti, A.; Aprile, C.; Hodolič, M. Evidence of 68Ga-DOTA-NT-20.3 Uptake in Pancreatic Adenocarcinoma AsPC-1 Cell Line—in Vitro Study. Curr. Pharm. Biotechnol. 2018, 19, 754–759. [Google Scholar] [CrossRef]
- Prignon, A.; Provost, C.; Alshoukr, F.; Wendum, D.; Couvelard, A.; Barbet, J.; Forgez, P.; Talbot, J.-N.; Gruaz-Guyon, A. Preclinical Evaluation of 68Ga-DOTA-NT-20.3: A Promising PET Imaging Probe To Discriminate Human Pancreatic Ductal Adenocarcinoma from Pancreatitis. Mol. Pharm. 2019, 16, 2776–2784. [Google Scholar] [CrossRef]
- Hodolic, M.; Wu, W.-Y.; Zhao, Z.; Yu, F.; Virgolini, I.; Wang, F. Safety and Tolerability of 68Ga-NT-20.3, a Radiopharmaceutical for Targeting Neurotensin Receptors, in Patients with Pancreatic Ductal Adenocarcinoma: The First in-Human Use. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1229–1234. [Google Scholar] [CrossRef]
- Buchegger, F.; Bonvin, F.; Kosinski, M.; Schaffland, A.O.; Prior, J.; Reubi, J.C.; Bläuenstein, P.; Tourwé, D.; García Garayoa, E.; Bischof Delaloye, A. Radiolabeled Neurotensin Analog, 99mTc-NT-XI, Evaluated in Ductal Pancreatic Adenocarcinoma Patients. J. Nucl. Med. 2003, 44, 1649–1654. [Google Scholar]
- Deng, H.; Wang, H.; Zhang, H.; Wang, M.; Giglio, B.; Ma, X.; Jiang, G.; Yuan, H.; Wu, Z.; Li, Z. Imaging Neurotensin Receptor in Prostate Cancer With 64Cu-Labeled Neurotensin Analogs. Mol. Imaging 2017, 16. [Google Scholar] [CrossRef]
- Chavatte, K.; Wong, E.; Fauconnier, T.K.; Lu, L.; Nguyen, T.; Roe, D.; Pollak, A.; Eshima, D.; Terriere, D.; Mertens, J.; et al. Rhenium (Re) and Technetium (Tc)-99M Oxocomplexes of Neurotensin(8-13). J. Label. Compd. Radiopharm. 1999, 42, 415–421. [Google Scholar] [CrossRef]
- Baum, R.P.; Singh, A.; Schuchardt, C.; Kulkarni, H.R.; Klette, I.; Wiessalla, S.; Osterkamp, F.; Reineke, U.; Smerling, C. 177Lu-3BP-227 for Neurotensin Receptor 1-Targeted Therapy of Metastatic Pancreatic Adenocarcinoma: First Clinical Results. J. Nucl. Med. 2018, 59, 809–814. [Google Scholar] [CrossRef]
- Azizian, A.; Rühlmann, F.; Krause, T.; Bernhardt, M.; Jo, P.; König, A.; Kleiß, M.; Leha, A.; Ghadimi, M.; Gaedcke, J. CA19-9 for Detecting Recurrence of Pancreatic Cancer. Sci. Rep. 2020, 10, 1332. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, D.P.; Sandanayake, N.S.; Jenkinson, C.; Gentry-Maharaj, A.; Apostolidou, S.; Fourkala, E.-O.; Camuzeaux, S.; Blyuss, O.; Gunu, R.; Dawnay, A.; et al. Serum CA19-9 Is Significantly Upregulated up to 2 Years before Diagnosis with Pancreatic Cancer: Implications for Early Disease Detection. Clin. Cancer Res. 2015, 21, 622–631. [Google Scholar] [CrossRef] [Green Version]
- Marchegiani, G.; Andrianello, S.; Malleo, G.; De Gregorio, L.; Scarpa, A.; Mino-Kenudson, M.; Maggino, L.; Ferrone, C.R.; Lillemoe, K.D.; Bassi, C.; et al. Does Size Matter in Pancreatic Cancer?: Reappraisal of Tumour Dimension as a Predictor of Outcome Beyond the TNM. Ann. Surg. 2017, 266, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Imaoka, H.; Shimizu, Y.; Senda, Y.; Natsume, S.; Mizuno, N.; Hara, K.; Hijioka, S.; Hieda, N.; Tajika, M.; Tanaka, T.; et al. Post-Adjuvant Chemotherapy CA19-9 Levels Predict Prognosis in Patients with Pancreatic Ductal Adenocarcinoma: A Retrospective Cohort Study. Pancreatology 2016, 16, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Goh, S.K.; Gold, G.; Christophi, C.; Muralidharan, V. Serum Carbohydrate Antigen 19-9 in Pancreatic Adenocarcinoma: A Mini Review for Surgeons. ANZ J. Surg. 2017, 87, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Houghton, J.L.; Zeglis, B.M.; Abdel-Atti, D.; Aggeler, R.; Sawada, R.; Agnew, B.J.; Scholz, W.W.; Lewis, J.S. Site-Specifically Labeled CA19.9-Targeted Immunoconjugates for the PET, NIRF, and Multimodal PET/NIRF Imaging of Pancreatic Cancer. Proc. Natl. Acad. Sci. USA 2015, 112, 15850–15855. [Google Scholar] [CrossRef] [Green Version]
- Houghton, J.L.; Abdel-Atti, D.; Scholz, W.W.; Lewis, J.S. Preloading with Unlabeled CA19.9 Targeted Human Monoclonal Antibody Leads to Improved PET Imaging with 89Zr-5B1. Mol. Pharm. 2017, 14, 908–915. [Google Scholar] [CrossRef]
- Lohrmann, C.; O’Reilly, E.M.; O’Donoghue, J.; Pandit-Taskar, N.; Carrasquillo, J.A.; Lyashchenko, S.K.; Ruan, S.; Teng, R.; Scholz, W.; Maffuid, P.W.; et al. Retooling a Blood-Based Biomarker: Phase I Assessment of the High-Affinity CA19-9 Antibody HuMab-5B1 for Immuno-PET Imaging of Pancreatic Cancer. Clin. Cancer Res. 2019, 25, 7014–7023. [Google Scholar] [CrossRef] [Green Version]
- Girgis, M.D.; Federman, N.; Rochefort, M.M.; McCabe, K.E.; Wu, A.M.; Nagy, J.O.; Denny, C.; Tomlinson, J.S. An Engineered Anti-CA19-9 Cys-Diabody for Positron Emission Tomography Imaging of Pancreatic Cancer and Targeting of Polymerized Liposomal Nanoparticles. J. Surg. Res. 2013, 185, 45–55. [Google Scholar] [CrossRef] [Green Version]
- Girgis, M.D.; Kenanova, V.; Olafsen, T.; McCabe, K.E.; Wu, A.M.; Tomlinson, J.S. Anti-CA19-9 Diabody as a PET Imaging Probe for Pancreas Cancer. J. Surg. Res. 2011, 170, 169–178. [Google Scholar] [CrossRef]
- Mauro, C.D.; Pesapane, A.; Formisano, L.; Rosa, R.; D’Amato, V.; Ciciola, P.; Servetto, A.; Marciano, R.; Orsini, R.C.; Monteleone, F.; et al. Urokinase-Type Plasminogen Activator Receptor (UPAR) Expression Enhances Invasion and Metastasis in RAS Mutated Tumors. Sci. Rep. 2017, 7, 9388. [Google Scholar] [CrossRef]
- Jaiswal, R.K.; Varshney, A.K.; Yadava, P.K. Diversity and Functional Evolution of the Plasminogen Activator System. Biomed. Pharmacother. 2018, 98, 886–898. [Google Scholar] [CrossRef] [PubMed]
- Li Santi, A.; Napolitano, F.; Montuori, N.; Ragno, P. The Urokinase Receptor: A Multifunctional Receptor in Cancer Cell Biology. Therapeutic Implications. Int. J. Mol. Sci. 2021, 22, 4111. [Google Scholar] [CrossRef] [PubMed]
- Dass, K.; Ahmad, A.; Azmi, A.S.; Sarkar, S.H.; Sarkar, F.H. Evolving Role of UPA/UPAR System in Human Cancers. Cancer Treat. Rev. 2008, 34, 122–136. [Google Scholar] [CrossRef]
- de Geus, S.W.; Baart, V.M.; Boonstra, M.C.; Kuppen, P.J.; Prevoo, H.A.; Mazar, A.P.; Bonsing, B.A.; Morreau, H.; van de Velde, C.J.; Vahrmeijer, A.L.; et al. Prognostic Impact of Urokinase Plasminogen Activator Receptor Expression in Pancreatic Cancer: Malignant Versus Stromal Cells. Biomark Insights 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Harris, N.L.E.; Vennin, C.; Conway, J.R.W.; Vine, K.L.; Pinese, M.; Cowley, M.J.; Shearer, R.F.; Lucas, M.C.; Herrmann, D.; Allam, A.H.; et al. SerpinB2 Regulates Stromal Remodelling and Local Invasion in Pancreatic Cancer. Oncogene 2017, 36, 4288–4298. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Zheng, B.; Robbins, D.H.; Lewin, D.N.; Mikhitarian, K.; Graham, A.; Rumpp, L.; Glenn, T.; Gillanders, W.E.; Cole, D.J.; et al. Accurate Discrimination of Pancreatic Ductal Adenocarcinoma and Chronic Pancreatitis Using Multimarker Expression Data and Samples Obtained by Minimally Invasive Fine Needle Aspiration. Int. J. Cancer 2007, 120, 1511–1517. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Liu, S.; Shan, H.; Conti, P.; Li, Z. Urokinase Plasminogen Activator Receptor (UPAR) Targeted Nuclear Imaging and Radionuclide Therapy. Theranostics 2013, 3, 507–515. [Google Scholar] [CrossRef] [Green Version]
- Yang, D.; Severin, G.W.; Dougherty, C.A.; Lombardi, R.; Chen, D.; Van Dort, M.E.; Barnhart, T.E.; Ross, B.D.; Mazar, A.P.; Hong, H. Antibody-Based PET of UPA/UPAR Signaling with Broad Applicability for Cancer Imaging. Oncotarget 2016, 7, 73912–73924. [Google Scholar] [CrossRef] [Green Version]
- Persson, M.; Skovgaard, D.; Brandt-Larsen, M.; Christensen, C.; Madsen, J.; Nielsen, C.H.; Thurison, T.; Klausen, T.L.; Holm, S.; Loft, A.; et al. First-in-Human UPAR PET: Imaging of Cancer Aggressiveness. Theranostics 2015, 5, 1303–1316. [Google Scholar] [CrossRef] [Green Version]
- Skovgaard, D.; Persson, M.; Brandt-Larsen, M.; Christensen, C.; Madsen, J.; Klausen, T.L.; Holm, S.; Andersen, F.L.; Loft, A.; Berthelsen, A.K.; et al. Safety, Dosimetry, and Tumor Detection Ability of 68Ga-NOTA-AE105: First-in-Human Study of a Novel Radioligand for UPAR PET Imaging. J. Nucl. Med. 2017, 58, 379–386. [Google Scholar] [CrossRef] [Green Version]
- Persson, M.; Juhl, K.; Rasmussen, P.; Brandt-Larsen, M.; Madsen, J.; Ploug, M.; Kjaer, A. UPAR Targeted Radionuclide Therapy with (177)Lu-DOTA-AE105 Inhibits Dissemination of Metastatic Prostate Cancer. Mol. Pharm. 2014, 11, 2796–2806. [Google Scholar] [CrossRef] [PubMed]
- Qu, C.F.; Song, E.Y.; Li, Y.; Rizvi, S.M.A.; Raja, C.; Smith, R.; Morgenstern, A.; Apostolidis, C.; Allen, B.J. Pre-Clinical Study of 213Bi Labeled PAI2 for the Control of Micrometastatic Pancreatic Cancer. Clin. Exp. Metastasis 2005, 22, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Ciardiello, F.; Tortora, G. EGFR Antagonists in Cancer Treatment. N. Engl. J. Med. 2008, 358, 1160–1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modjtahedi, H.; Dean, C. The Receptor for EGF and Its Ligands—Expression, Prognostic Value and Target for Therapy in Cancer (Review). Int. J. Oncol. 1994, 4, 277–296. [Google Scholar] [CrossRef] [PubMed]
- Tobita, K.; Kijima, H.; Dowaki, S.; Kashiwagi, H.; Ohtani, Y.; Oida, Y.; Yamazaki, H.; Nakamura, M.; Ueyama, Y.; Tanaka, M.; et al. Epidermal Growth Factor Receptor Expression in Human Pancreatic Cancer: Significance for Liver Metastasis. Int. J. Mol. Med. 2003, 11, 305–309. [Google Scholar] [CrossRef]
- Bloomston, M.; Bhardwaj, A.; Ellison, E.C.; Frankel, W.L. Epidermal Growth Factor Receptor Expression in Pancreatic Carcinoma Using Tissue Microarray Technique. Dig. Surg. 2006, 23, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; Luo, G.; Liu, C.; Cheng, H.; Lu, Y.; Jin, K.; Liu, Z.; Long, J.; Liu, L.; Xu, J.; et al. The Prognostic and Predictive Role of Epidermal Growth Factor Receptor in Surgical Resected Pancreatic Cancer. Int. J. Mol. Sci. 2016, 17, 1090. [Google Scholar] [CrossRef] [Green Version]
- Ueda, S.; Ogata, S.; Tsuda, H.; Kawarabayashi, N.; Kimura, M.; Sugiura, Y.; Tamai, S.; Matsubara, O.; Hatsuse, K.; Mochizuki, H. The Correlation between Cytoplasmic Overexpression of Epidermal Growth Factor Receptor and Tumor Aggressiveness: Poor Prognosis in Patients with Pancreatic Ductal Adenocarcinoma. Pancreas 2004, 29, e1–e8. [Google Scholar] [CrossRef]
- Fagman, J.B.; Ljungman, D.; Falk, P.; Iresjö, B.-M.; Engström, C.; Naredi, P.; Lundholm, K. EGFR, but Not COX-2, Protein in Resected Pancreatic Ductal Adenocarcinoma Is Associated with Poor Survival. Oncol. Lett. 2019, 17, 5361–5368. [Google Scholar] [CrossRef] [Green Version]
- Ardito, C.M.; Grüner, B.M.; Takeuchi, K.K.; Lubeseder-Martellato, C.; Teichmann, N.; Mazur, P.K.; Delgiorno, K.E.; Carpenter, E.S.; Halbrook, C.J.; Hall, J.C.; et al. EGF Receptor Is Required for KRAS-Induced Pancreatic Tumorigenesis. Cancer Cell 2012, 22, 304–317. [Google Scholar] [CrossRef] [Green Version]
- Moore, M.J.; Goldstein, D.; Hamm, J.; Figer, A.; Hecht, J.R.; Gallinger, S.; Au, H.J.; Murawa, P.; Walde, D.; Wolff, R.A.; et al. Erlotinib plus Gemcitabine Compared with Gemcitabine Alone in Patients with Advanced Pancreatic Cancer: A Phase III Trial of the National Cancer Institute of Canada Clinical Trials Group. J. Clin. Oncol. 2007, 25, 1960–1966. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, R.; Goel, S.; Cai, W. Nanobody: The “Magic Bullet” for Molecular Imaging? Theranostics 2014, 4, 386–398. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Gainkam, L.O.T.; Caveliers, V.; Vanhove, C.; Keyaerts, M.; De Baetselier, P.; Bossuyt, A.; Revets, H.; Lahoutte, T. SPECT Imaging with 99mTc-Labeled EGFR-Specific Nanobody for in Vivo Monitoring of EGFR Expression. Mol. Imaging Biol. 2008, 10, 167–175. [Google Scholar] [CrossRef]
- Vosjan, M.J.W.D.; Perk, L.R.; Roovers, R.C.; Visser, G.W.M.; Stigter-van Walsum, M.; van Bergen En Henegouwen, P.M.P.; van Dongen, G.A.M.S. Facile Labelling of an Anti-Epidermal Growth Factor Receptor Nanobody with 68Ga via a Novel Bifunctional Desferal Chelate for Immuno-PET. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 753–763. [Google Scholar] [CrossRef] [Green Version]
- Gainkam, L.O.T.; Keyaerts, M.; Caveliers, V.; Devoogdt, N.; Vanhove, C.; Van Grunsven, L.; Muyldermans, S.; Lahoutte, T. Correlation between Epidermal Growth Factor Receptor-Specific Nanobody Uptake and Tumor Burden: A Tool for Noninvasive Monitoring of Tumor Response to Therapy. Mol. Imaging Biol. 2011, 13, 940–948. [Google Scholar] [CrossRef]
- Garousi, J.; Andersson, K.G.; Mitran, B.; Pichl, M.-L.; Ståhl, S.; Orlova, A.; Löfblom, J.; Tolmachev, V. PET Imaging of Epidermal Growth Factor Receptor Expression in Tumours Using 89Zr-Labelled ZEGFR:2377 Affibody Molecules. Int. J. Oncol. 2016, 48, 1325–1332. [Google Scholar] [CrossRef] [Green Version]
- Menke-van der Houven van Oordt, C.W.; Gootjes, E.C.; Huisman, M.C.; Vugts, D.J.; Roth, C.; Luik, A.M.; Mulder, E.R.; Schuit, R.C.; Boellaard, R.; Hoekstra, O.S.; et al. 89Zr-Cetuximab PET Imaging in Patients with Advanced Colorectal Cancer. Oncotarget 2015, 6, 30384–30393. [Google Scholar] [CrossRef] [Green Version]
- Aghevlian, S.; Lu, Y.; Winnik, M.A.; Hedley, D.W.; Reilly, R.M. Panitumumab Modified with Metal-Chelating Polymers (MCP) Complexed to 111In and 177Lu-An EGFR-Targeted Theranostic for Pancreatic Cancer. Mol. Pharm. 2018, 15, 1150–1159. [Google Scholar] [CrossRef]
- Aghevlian, S.; Cai, Z.; Lu, Y.; Hedley, D.W.; Winnik, M.A.; Reilly, R.M. Radioimmunotherapy of PANC-1 Human Pancreatic Cancer Xenografts in NRG Mice with Panitumumab Modified with Metal-Chelating Polymers Complexed to 177Lu. Mol. Pharm. 2019, 16, 768–778. [Google Scholar] [CrossRef]
- Scherl-Mostageer, M.; Sommergruber, W.; Abseher, R.; Hauptmann, R.; Ambros, P.; Schweifer, N. Identification of a Novel Gene, CDCP1, Overexpressed in Human Colorectal Cancer. Oncogene 2001, 20, 4402–4408. [Google Scholar] [CrossRef] [Green Version]
- Spassov, D.S.; Baehner, F.L.; Wong, C.H.; McDonough, S.; Moasser, M.M. The Transmembrane Src Substrate Trask Is an Epithelial Protein That Signals during Anchorage Deprivation. Am. J. Pathol. 2009, 174, 1756–1765. [Google Scholar] [CrossRef] [Green Version]
- Khan, T.; Kryza, T.; Lyons, N.J.; He, Y.; Hooper, J.D. The CDCP1 Signaling Hub: A Target for Cancer Detection and Therapeutic Intervention. Cancer Res. 2021. [Google Scholar] [CrossRef]
- Uekita, T.; Jia, L.; Narisawa-Saito, M.; Yokota, J.; Kiyono, T.; Sakai, R. CUB Domain-Containing Protein 1 Is a Novel Regulator of Anoikis Resistance in Lung Adenocarcinoma. Mol. Cell Biol. 2007, 27, 7649–7660. [Google Scholar] [CrossRef] [Green Version]
- Miyazawa, Y.; Uekita, T.; Hiraoka, N.; Fujii, S.; Kosuge, T.; Kanai, Y.; Nojima, Y.; Sakai, R. CUB Domain-Containing Protein 1, a Prognostic Factor for Human Pancreatic Cancers, Promotes Cell Migration and Extracellular Matrix Degradation. Cancer Res. 2010, 70, 5136–5146. [Google Scholar] [CrossRef] [Green Version]
- Nakashima, K.; Uekita, T.; Yano, S.; Kikuchi, J.-I.; Nakanishi, R.; Sakamoto, N.; Fukumoto, K.; Nomoto, A.; Kawamoto, K.; Shibahara, T.; et al. Novel Small Molecule Inhibiting CDCP1-PKCδ Pathway Reduces Tumor Metastasis and Proliferation. Cancer Sci. 2017, 108, 1049–1057. [Google Scholar] [CrossRef]
- Harrington, B.S.; He, Y.; Khan, T.; Puttick, S.; Conroy, P.J.; Kryza, T.; Cuda, T.; Sokolowski, K.A.; Tse, B.W.; Robbins, K.K.; et al. Anti-CDCP1 Immuno-Conjugates for Detection and Inhibition of Ovarian Cancer. Theranostics 2020, 10, 2095–2114. [Google Scholar] [CrossRef]
- Kryza, T.; Khan, T.; Puttick, S.; Li, C.; Sokolowski, K.A.; Tse, B.W.; Cuda, T.; Lyons, N.; Gough, M.; Yin, J.; et al. Effective Targeting of Intact and Proteolysed CDCP1 for Imaging and Treatment of Pancreatic Ductal Adenocarcinoma. Theranostics 2020, 10, 4116–4133. [Google Scholar] [CrossRef]
- Moroz, A.; Wang, Y.-H.; Sharib, J.M.; Wei, J.; Zhao, N.; Huang, Y.; Chen, Z.; Martinko, A.J.; Zhuo, J.; Lim, S.A.; et al. Theranostic Targeting of CUB Domain Containing Protein 1 (CDCP1) in Pancreatic Cancer. Clin. Cancer Res. 2020, 26, 3608–3615. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montemagno, C.; Cassim, S.; De Leiris, N.; Durivault, J.; Faraggi, M.; Pagès, G. Pancreatic Ductal Adenocarcinoma: The Dawn of the Era of Nuclear Medicine? Int. J. Mol. Sci. 2021, 22, 6413. https://doi.org/10.3390/ijms22126413
Montemagno C, Cassim S, De Leiris N, Durivault J, Faraggi M, Pagès G. Pancreatic Ductal Adenocarcinoma: The Dawn of the Era of Nuclear Medicine? International Journal of Molecular Sciences. 2021; 22(12):6413. https://doi.org/10.3390/ijms22126413
Chicago/Turabian StyleMontemagno, Christopher, Shamir Cassim, Nicolas De Leiris, Jérôme Durivault, Marc Faraggi, and Gilles Pagès. 2021. "Pancreatic Ductal Adenocarcinoma: The Dawn of the Era of Nuclear Medicine?" International Journal of Molecular Sciences 22, no. 12: 6413. https://doi.org/10.3390/ijms22126413