Multimodality Imaging of the Anatomy of Tricuspid Valve

 , , and
, , and
Abstract
:1. Introduction
1.1. Prevalence of TR
1.2. Therapeutic Options
- (a)
- Which is the best noninvasive imaging technique to visualize TV?
- (b)
- Does the tricuspid annulus exist?
- (c)
- How many leaflets has the valve?
- (d)
- Which are the similarities and differences between tricuspid and mitral valve?
2. Which Is the Best Noninvasive Imaging Technique to Visualize TV?
2.1. CT Scan
2.2. CMR
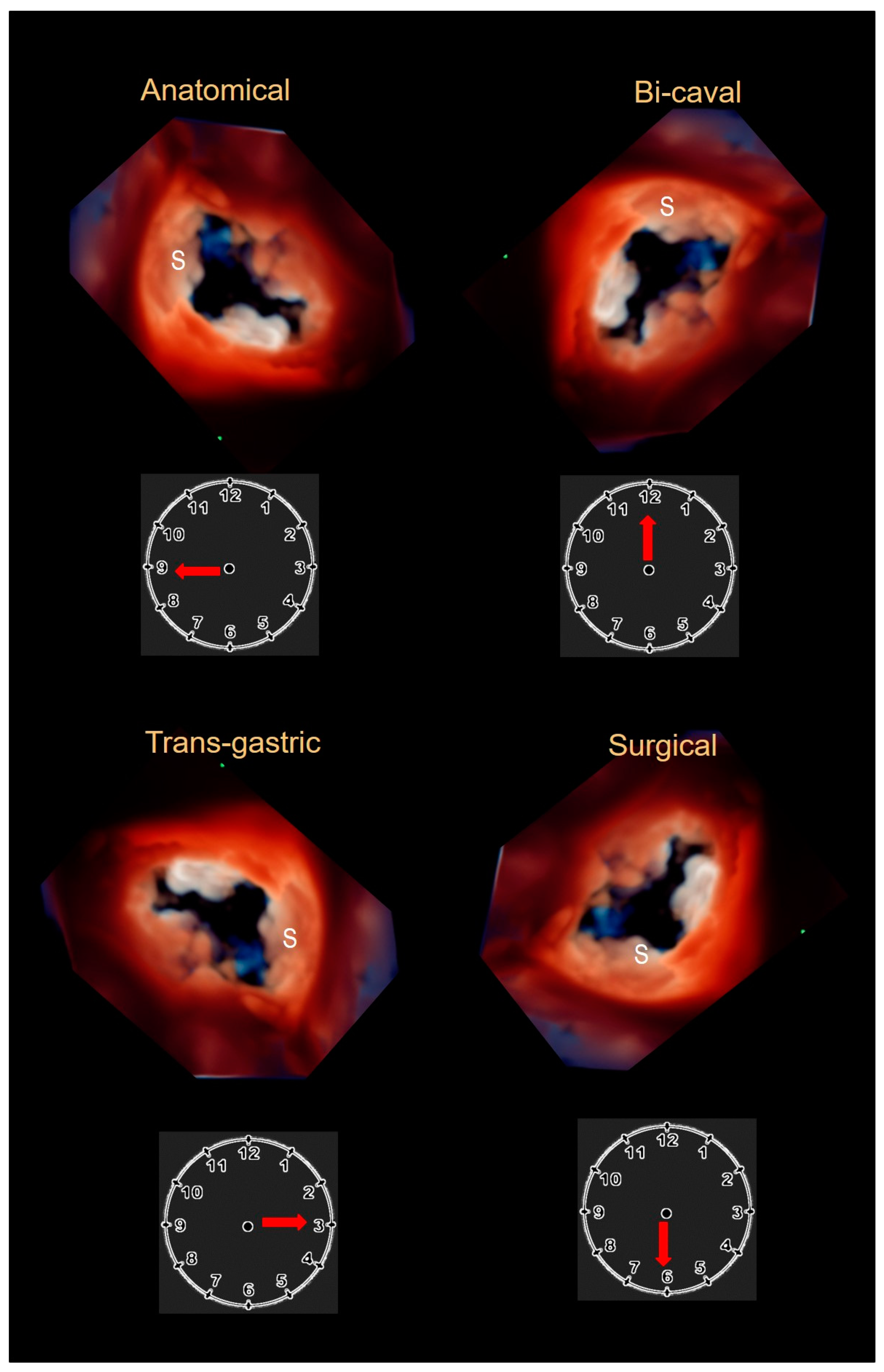
2.3. Echocardiography
3. Does the Tricuspid Annulus Exist?
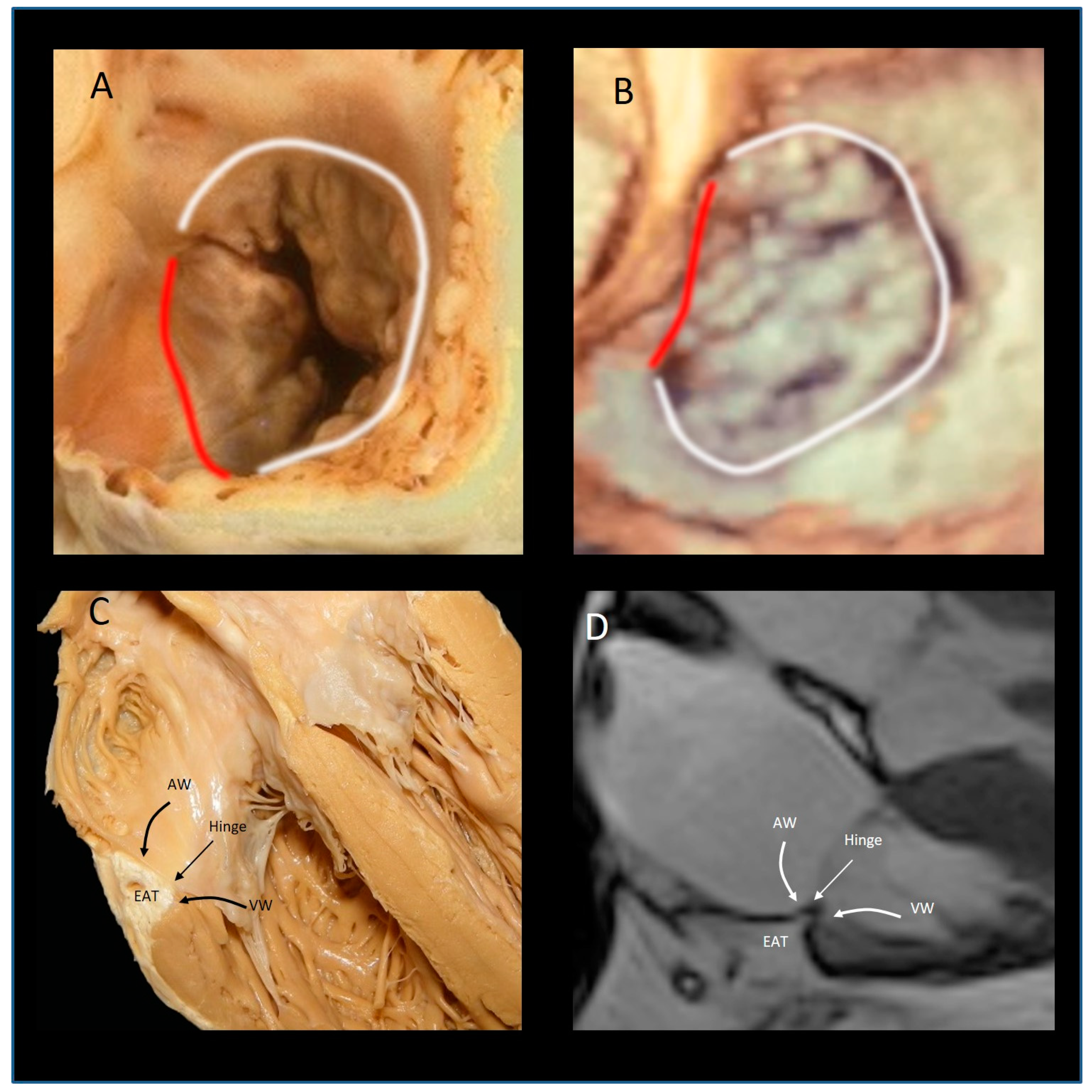
The “Mural” Annulus
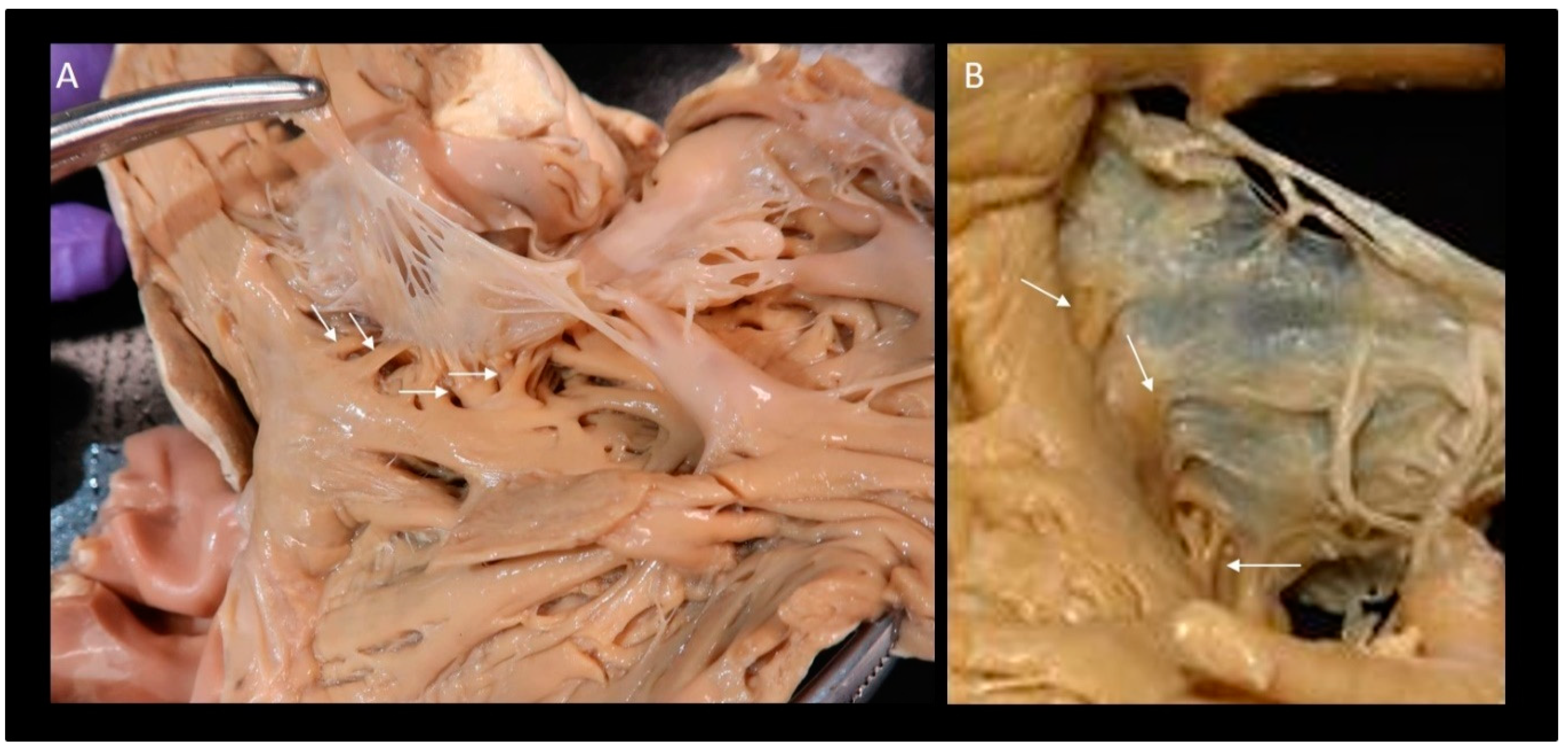
4. The “Septal” Annulus
5. Physiological and Physiopathologic Consequences of the Annular Structure
6. How Many Leaflets Has the Valve?
7. What Are the Similarities and Differences between the Tricuspid and Mitral Valve
8. Conclusions
Funding
Conflicts of Interest
References
- Braunwald, N.S.; Ross, J.; Morrow, A.G. Conservative Management of Tricuspid Regurgitation in Patients Undergoing Mitral Valve Replacement. Circulation 1967, 35, I63–I69. [Google Scholar] [CrossRef]
- Nath, J.; Foster, E.; Heidenreich, P.A. Impact of tricuspid regurgitation on long-term survival. J. Am. Coll. Cardiol. 2004, 43, 405–409. [Google Scholar] [CrossRef] [Green Version]
- Prihadi, E.A.; Delgado, V.; Leon, M.B.; Enriquez-Sarano, M.; Topilsky, Y.; Bax, J.J. Morphologic Types of Tricuspid Regurgitation: Characteristics and Prognostic Implications. JACC Cardiovasc. Imaging 2019, 12, 491–499. [Google Scholar] [CrossRef]
- Bohbot, Y.; Chadha, G.; Delabre, J.; Landemaine, T.; Beyls, C.; Tribouilloy, C. Characteristics and prognosis of patients with sig-nificant tricuspid regurgitation. Arch Cardiovasc. Dis. 2019, 112, 604–614. [Google Scholar] [CrossRef]
- Benfari, G.; Antoine, C.; Miller, W.L.; Thapa, P.; Topilsky, Y.; Rossi, A.; Michelena, H.I.; Pislaru, S.; Enriquez-Sarano, M. Excess Mortality Associated with Functional Tricuspid Regurgitation Complicating Heart Failure with Reduced Ejection Fraction. Circulation 2019, 140, 196–206. [Google Scholar] [CrossRef]
- Chorin, E.; Rozenbaum, Z.; Topilsky, Y.; Konigstein, M.; Ziv-Baran, T.; Richert, E.; Keren, G.; Banai, S. Tricuspid regurgitation and long-term clinical outcomes. Eur. Heart J. Cardiovasc. Imaging 2019. [Google Scholar] [CrossRef] [PubMed]
- Cahill, T.J.; Prothero, A.; Wilson, J.; Kennedy, A.; Brubert, J.; Masters, M.; Newton, J.D.; Dawkins, S.; Enriquez-Sarano, M.; Prendergast, B.D.; et al. Community prevalence, mechanisms and outcome of mitral or tricuspid regurgitation. Heart 2021, 107, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Topilsky, Y.; Maltais, S.; Medina Inojosa, J.; Oguz, D.; Michelena, H.; Maalouf, J.; Mahoney, D.W.; Enriquez-Sarano, M. Burden of Tri-cuspid Regurgitation in Patients Diagnosed in the Community Setting. JACC Cardiovasc. Imaging 2019, 12, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Vieitez, J.M.; Monteagudo, J.M.; Mahia, P.; Perez, L.; Lopez, T.; Marco, I.; Perone, F.; González, T.; Sitges, M.; Bouzas-Mosquera, A.; et al. New insights of tricuspid regurgitation: A large-scale prospective cohort study. Eur. Heart J. Cardiovasc. Imaging 2020, 22, 196–202. [Google Scholar] [CrossRef]
- Fender, E.A.; Zack, C.J.; Nishimura, R.A. Isolated tricuspid regurgitation: Outcomes and therapeutic interventions. Heart 2017, 104, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Hahn, R.T.; Asch, F.; Weissman, N.J.; Grayburn, P.; Kar, S.; Lim, S.; Ben-Yehuda, O.; Shahim, B.; Chen, S.; Liu, M.; et al. Impact of Tricuspid Regurgitation on Clinical Outcomes: The COAPT Trial. J. Am. Coll. Cardiol. 2020, 76, 1305–1314. [Google Scholar] [CrossRef] [PubMed]
- Asmarats, L.; Taramasso, M.; Rodés-Cabau, J. Tricuspid valve disease: Diagnosis, prognosis and management of a rapidly evolving field. Nat. Rev. Cardiol. 2019, 16, 538–554. [Google Scholar] [CrossRef]
- Lankeit, M.; Keller, K.; Tschöpe, C.; Pieske, B. Medikamentöse Therapie der Trikuspidalklappeninsuffizienz [Medicinal treatment of tricuspid valve regurgitation]. Herz 2017, 42, 634–643. [Google Scholar] [CrossRef]
- Antunes, M.J.; Rodríguez-Palomares, J.; Prendergast, B.; De Bonis, M.; Rosenhek, R.; Al-Attar, N.; Barili, F.; Casselman, F.; Folliguet, T.; et al.; ESC Working Groups of Cardiovascular Surgery and Valvular Heart Disease Management of tricuspid valve regurgitation: Position statement of the European Society of Cardiology Working Groups of Cardiovascular Surgery and Valvular Heart Disease. Eur. J. Cardiothorac. Surg. 2017, 52, 1022–1030. [Google Scholar] [CrossRef] [Green Version]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar]
- Dreyfus, G.D.; Martin, R.P.; Chan, K.M.; Dulguerov, F.; Alexandrescu, C. Functional tricuspid regurgitation: A need to revise our understanding. J. Am. Coll. Cardiol. 2015, 65, 2331–2336. [Google Scholar] [CrossRef] [Green Version]
- Zack, C.J.; Fender, E.A.; Chandrashekar, P.; Reddy, Y.N.; Bennett, C.E.; Stulak, J.M.; Miller, V.M.; Nishimura, R.A. National Trends and Outcomes in Isolated Tricuspid Valve Surgery. J. Am. Coll. Cardiol. 2017, 70, 2953–2960. [Google Scholar] [CrossRef]
- Asmarats, L.; Puri, R.; Latib, A.; Navia, J.L.; Rodés-Cabau, J. Transcatheter Tricuspid Valve Interventions: Landscape, Challenges, and Future Directions. J. Am. Coll. Cardiol. 2018, 71, 2935–2956. [Google Scholar] [CrossRef] [PubMed]
- Taramasso, M.; Pozzoli, A.; Guidotti, A.; Nietlispach, F.; Inderbitzin, D.T.; Benussi, S.; Alfieri, O.; Maisano, F. Percutaneous tricuspid valve therapies: The new frontier. Eur. Heart J. 2016, 38, 639–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orban, M.; Rommel, K.P.; Ho, E.C.; Unterhuber, M.; Pozzoli, A.; Connelly, K.A.; Deseive, S.; Besler, C.; Ong, G.; Braun, D.; et al. Transcatheter Edge-to-Edge Tricuspid Repair for Severe Tricuspid Regurgitation Reduces Hospitalizations for Heart Failure. JACC Heart Fail. 2020, 8, 265–276. [Google Scholar] [CrossRef]
- Orban, M.; Besler, C.; Braun, D.; Nabauer, M.; Zimmer, M.; Orban, M.; Noack, T.; Mehilli, J.; Hagl, C.; Seeburger, J.; et al. Six-month outcome after transcatheter edge-to-edge repair of severe tricuspid regurgitation in patients with heart failure. Eur. J. Heart Fail. 2018, 20, 1055–1062. [Google Scholar] [CrossRef] [Green Version]
- Dahou, A.; Levin, D.; Reisman, M.; Hahn, R.T. Anatomy and Physiology of the Tricuspid Valve. JACC Cardiovasc. Imaging 2019, 12, 458–468. [Google Scholar] [CrossRef]
- Khalique, O.K.; Cavalcante, J.L.; Shah, D.; Guta, A.C.; Zhan, Y.; Piazza, N.; Muraru, D. Multimodality Imaging of the Tricuspid Valve and Right Heart Anatomy. JACC Cardiovasc. Imaging 2019, 12, 2611–2612. [Google Scholar] [CrossRef]
- Muraru, D.; Hahn, R.T.; Soliman, O.I.; Faletra, F.F.; Basso, C.; Badano, L.P. 3-Dimensional Echocardiography in Imaging the Tricuspid Valve. JACC Cardiovasc. Imaging 2019, 12, 500–515. [Google Scholar] [CrossRef]
- Ancona, F.; Stella, S.; Capogrosso, C.; Marini, C.; Fisicaro, A.; Margonato, A.; Denti, P.; Agricola, E. Tricuspid valve imaging. Minerva Cardioangiol. 2018, 66, 680–690. [Google Scholar] [CrossRef]
- Ancona, F.; Agricola, E.; Stella, S.; Capogrosso, C.; Marini, C.; Margonato, A.; Hahn, R.T. Interventional Imaging of the Tricuspid Valve. Interv. Cardiol. Clin. 2018, 7, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Huttin, O.; Voilliot, D.; Mandry, D.; Venner, C.; Juillière, Y.; Selton-Suty, C. All you need to know about the tricuspid valve: Tricuspid valve imaging and tricuspid regurgitation analysis. Arch. Cardiovasc. Dis. 2016, 109, 67–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ancona, F.; Stella, S.; Taramasso, M.; Marini, C.; Latib, A.; Denti, P.; Grigioni, F.; Enriquez-Sarano, M.; Alfieri, O.; Colombo, A.; et al. Multimodality imaging of the tricuspid valve with implication for percutaneous repair approaches. Heart 2017, 103, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Faletra, F.F.; Leo, L.A.; Paiocchi, V.L.; Schlossbauer, S.A.; Borruso, M.G.; Pedrazzini, G.; Moccetti, T.; Ho, S.Y. Imaging-based tricuspid valve anatomy by computed tomography, magnetic resonance imaging, two and three-dimensional echocardiography: Correlation with anatomic specimen. Eur. Heart J. Cardiovasc. Imaging 2018, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Leo, L.; Paiocchi, V.; Schlossbauer, S.; Gherbesi, E.; Faletra, F. Anatomy of Mitral Valve Complex as Revealed by Non-Invasive Imaging: Pathological, Surgical and Interventional Implications. J. Cardiovasc. Dev. Dis. 2020, 7, 49. [Google Scholar] [CrossRef] [PubMed]
- Paiocchi, V.; Faletra, F.; Ferrari, E.; Schlossbauer, S.; Leo, L.; Maisano, F. Multimodality Imaging of the Anatomy of the Aortic Root. J. Cardiovasc. Dev. Dis. 2021, 8, 51. [Google Scholar] [CrossRef]
- Abdelrahman, K.M.; Chen, M.Y.; Dey, A.K.; Virmani, R.; Finn, A.V.; Khamis, R.Y.; Choi, A.D.; Min, J.K.; Williams, M.C.; Buckler, A.J.; et al. Coronary Computed Tomography Angiography From Clinical Uses to Emerging Technologies: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Francone, M.; Budde, R.P.J.; Bremerich, J.; Dacher, J.N.; Loewe, C.; Wolf, F.; Natale, L.; Pontone, G.; Redheuil, A.; Vliegenthart, R.; et al. CT and MR imaging prior to transcatheter aortic valve implantation: Standardization of scanning protocols, measurements and reporting—A consensus document by the European Society of Cardiovascular Radiology (ESCR). Eur. Radiol. 2020, 30, 2627–2650. [Google Scholar] [CrossRef] [Green Version]
- Rajwani, A.; Nelson, A.J.; Shirazi, M.G.; Disney, P.J.S.; Teo, K.S.L.; Wong, D.T.L.; Young, G.D.; Worthley, S.G. CT sizing for left atrial ap-pendage closure is associated with favourable outcomes for procedural safety. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1361–1368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulerwitz, T.C.; Khalique, O.K.; Leb, J.; Hahn, R.T.; Nazif, T.; Leon, M.B.; George, I.; Vahl, T.P.; D’Souza, B.; Bapat, V.N.; et al. Optimizing Cardiac CT Protocols for Comprehensive Acquisition Prior to Percutaneous MV and TV Repair/Replacement. JACC Cardiovasc. Imaging 2020, 13, 836–850. [Google Scholar] [CrossRef]
- Weir-McCall, J.R.; Blanke, P.; Naoum, C.; Delgado, V.; Bax, J.J.; Leipsic, J. Mitral Valve Imaging with CT: Relationship with Transcatheter Mitral Valve Interventions. Radiology 2018, 288, 638–655. [Google Scholar] [CrossRef] [PubMed]
- Kochav, J.; Simprini, L.; Weinsaft, J.W. Imaging of the Right Heart-CT and CMR. Echocardiography 2014, 32, S53–S68. [Google Scholar] [CrossRef]
- Lell, M.M.; Kachelrieß, M. Recent and Upcoming Technological Developments in Computed Tomography: High Speed, Low Dose, Deep Learning, Multienergy. Investig. Radiol. 2020, 55, 8–19. [Google Scholar] [CrossRef]
- Hahn, R.T.; Abraham, T.; Adams, M.S.; Bruce, C.J.; Glas, K.E.; Lang, R.M.; Reeves, S.T.; Shanewise, J.S.; Siu, S.; Stewart, W.; et al. Guidelines for Performing a Comprehensive Transesophageal Echocardiographic Examination: Recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J. Am. Soc. Echocardiogr. 2013, 26, 921–964. [Google Scholar] [CrossRef]
- Hahn, R.T. State-of-the-Art Review of Echocardiographic Imaging in the Evaluation and Treatment of Functional Tricuspid Regurgitation. Circ. Cardiovasc. Imaging 2016, 9, e005332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahn, R.T.; Thomas, J.D.; Khalique, O.K.; Cavalcante, J.L.; Praz, F.; Zoghbi, W.A. Imaging Assessment of Tricuspid Regurgitation Severity. JACC Cardiovasc. Imaging 2019, 12, 469–490. [Google Scholar] [CrossRef]
- Faletra, F.F.; Ramamurthi, A.; Dequarti, M.C.; Leo, L.A.; Moccetti, T.; Pandian, N. Artifacts in Three-Dimensional Transesophageal Echocardiography. J. Am. Soc. Echocardiogr. 2014, 27, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Hahn, R.T.; Nabauer, M.; Zuber, M.; Nazif, T.; Hausleiter, J.; Taramasso, M.; Pozzoli, A.; George, I.; Kodali, S.; Bapat, V.; et al. Intraprocedural Imaging of Transcatheter Tricuspid Valve Interventions. JACC Cardiovasc. Imaging 2019, 12, 532–553. [Google Scholar] [CrossRef] [PubMed]
- Addetia, K.; Muraru, D.; Veronesi, F.; Jenei, C.; Cavalli, G.; Besser, S.A.; Mor-Avi, V.; Lang, R.M.; Badano, L. 3-Dimensional Echocardiographic Analysis of the Tricuspid Annulus Provides New Insights Into Tricuspid Valve Geometry and Dynamics. JACC Cardiovasc. Imaging 2019, 12, 401–412. [Google Scholar] [CrossRef]
- Fukuda, S.; Saracino, G.; Matsumura, Y.; Daimon, M.; Tran, H.; Greenberg, N.L.; Hozumi, T.; Yoshikawa, J.; Thomas, J.D.; Shiota, T. Three-dimensional geometry of the tricuspid annulus in healthy subjects and in patients with functional tricuspid regurgitation: A real-time, 3-dimensional echocardiographic study. Circulation. 2006, 114 (Suppl. 1), I492–I498. [Google Scholar] [CrossRef] [Green Version]
- Salgo, I.S.; Gorman, J.H.; Gorman, R.C.; Jackson, B.M.; Bowen, F.W.; Plappert, T.; Sutton, M.G.S.J.; Edmunds, L.H. Effect of Annular Shape on Leaflet Curvature in Reducing Mitral Leaflet Stress. Circulation 2002, 106, 711–717. [Google Scholar] [CrossRef] [Green Version]
- Messer, S.; Moseley, E.; Marinescu, M.; Freeman, C.; Goddard, M.; Nair, S. Histologic analysis of the right atrioventricular junction in the adult human heart. J. Heart Valve Dis. 2012, 21, 368–373. [Google Scholar]
- Attenhofer Jost, C.H.; Connolly, H.M.; Dearani, J.A.; Edwards, W.D.; Danielson, G.K. Ebstein’s anomaly. Circulation 2007, 115, 277–285. [Google Scholar] [CrossRef] [Green Version]
- Agricola, E.; Ancona, F.; Stella, S.; Rosa, I.; Marini, C.; Spartera, M.; Denti, P.; Margonato, A.; Hahn, R.T.; Alfieri, O.; et al. Use of Echocardiography for Guiding Percutaneous Tricuspid Valve Procedures. JACC Cardiovasc. Imaging 2017, 10, 1194–1198. [Google Scholar] [CrossRef]
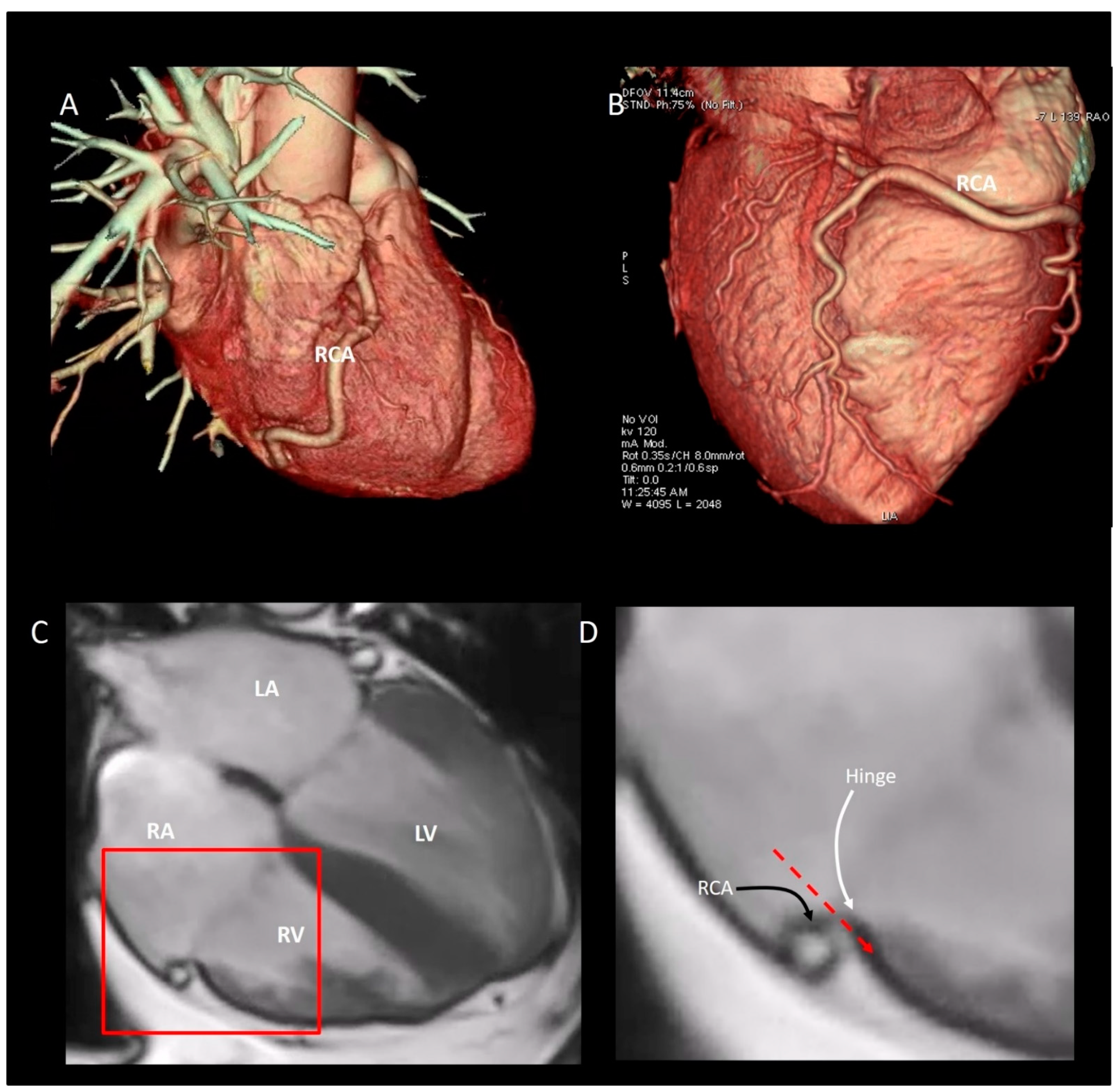
- Hinzpeter, R.; Eberhard, M.; Pozzoli, A.; Manka, R.; Tanner, F.C.; Taramasso, M.; Maisano, F.; Alkadhi, H. Dynamic anatomic relationship of coronary arteries to the valves. Part 2: Tricuspid annulus and right coronary artery. EuroIntervention 2019, 15, 935–938. [Google Scholar] [CrossRef]
- Muraru, D.; Caravita, S.; Guta, A.C.; Mihalcea, D.; Branzi, G.; Parati, G.; Badano, L.P. Functional Tricuspid Regurgitation and Atrial Fibrillation: Which Comes First, the Chicken or the Egg? CASE 2020, 4, 458–463. [Google Scholar] [CrossRef]
- Silver, M.D.; Lam, J.H.C.; Ranganathan, N.; Wigle, E.D. Morphology of the Human Tricuspid Valve. Circulation 1971, 43, 333–348. [Google Scholar] [CrossRef] [Green Version]
- Kocak, A.; Govsa, F.; Aktas, E.O.; Boydak, B.; Yavuz, I.C. Structure of the human tricuspid valve leaflets and its chordae tendineae in unexpected death. A forensic autopsy study of 400 cases. Saudi Med. J. 2004, 25, 1051–1059. [Google Scholar] [PubMed]
- Skwarek, M.; Hreczecha, J.; Dudziak, M.; Grzybiak, M. The morphology of the right atrioventricular valve in the adult human heart. Folia Morphol. 2006, 65, 200–208. [Google Scholar]
- Lama, P.; Tamang, B.K.; Kulkarni, J. Morphometry and aberrant morphology of the adult human tricuspid valve leaflets. Anat. Sci. Int. 2015, 91, 143–150. [Google Scholar] [CrossRef]
- Hołda, M.K.; Zhingre Sanchez, J.D.; Bateman, M.G.; Iaizzo, P.A. Right Atrioventricular Valve Leaflet Morphology Redefined: Implications for Transcatheter Repair Procedures. JACC Cardiovasc Interv. 2019, 12, 169–178. [Google Scholar] [CrossRef]
- Sakon, Y.; Murakami, T.; Fujii, H.; Takahashi, Y.; Morisaki, A.; Yamane, K.; Ohsawa, M.; Shintani, A.; Seki, T.; Shibata, T. New insight into tricuspid valve anatomy from 100 hearts to reappraise annuloplasty methodology. Gen. Thorac. Cardiovasc. Surg. 2019, 67, 758–764. [Google Scholar] [CrossRef]
- Kujur, B.; Thakur, N.; Prasad, R. Morphological Study of Tricuspid Valve And Its Variations in Adult Human Hearts. IOSR J. Dent. Med. Sci. 2016, 15, 72–78. [Google Scholar] [CrossRef]
- Hahn, R.T.; Weckbach, L.T.; Noack, T.; Hamid, N.; Kitamura, M.; Bae, R.; Lurz, P.; Kodali, S.K.; Sorajja, P.; Hausleiter, J.; et al. Proposal for a Standard Echocardiographic Tricuspid Valve Nomenclature. JACC Cardiovasc. Imaging 2021. [Google Scholar] [CrossRef]
- Silverman, N.H.; Schiller, N.B. Apex echocardiography. A two-dimensional technique for evaluating congenital heart disease. Circulation 1978, 57, 503–511. [Google Scholar] [CrossRef] [Green Version]
- Anderson, R.H.; Ho, S.Y.; Becker, A.E. Anatomy of the human atrioventricular junctions revisited. Anat. Rec. Adv. Integr. Anat. Evol. Biol. 2000, 260, 81–91. [Google Scholar] [CrossRef]
- Faletra, F.F.; Leo, L.A.; Paiocchi, V.L.; Schlossbauer, S.A.; Pedrazzini, G.; Moccetti, T.; Ho, S.Y. Revisiting Anatomy of the Interatrial Septum and its Adjoining Atrioventricular Junction Using Noninvasive Imaging Techniques. J. Am. Soc. Echocardiogr. 2019, 32, 580–592. [Google Scholar] [CrossRef]
- Mori, S.; Nishii, T.; Takaya, T.; Kashio, K.; Kasamatsu, A.; Takamine, S.; Ito, T.; Fujiwara, S.; Kono, A.K.; Hirata, K. Clinical structural anatomy of the inferior pyramidal space reconstructed from the living heart: Three-dimensional visualization using multidetector-row computed tomography. Clin. Anat. 2015, 28, 878–887. [Google Scholar] [CrossRef]
- Victor, S.; Nayak, V.M. The tricuspid valve is bicuspid. J. Heart Valve Dis. 1994, 3, 27–36. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tricuspid Valve | Mitral Valve | ||
|---|---|---|---|
| Annulus | Two components: septal annulus and C-shaped mural annulus. | Annulus | Two components: anterior annulus and C-shaped posterior annulus |
| Mural annulus | C-shaped configuration. Made up of convergence of four tissues: atrial myocardium, ventricular myocardium, hinge line of leaflets and adipose tissue. No fibrous ring. Asymmetric sphincteric contraction of the annulus depending almost exclusively on the mural annulus. The dilation of the annulus mainly affects the mural annulus. No calcifications | Posterior annulus | C-shaped configuration. Made up of convergence of four tissues: atrial myocardium, ventricular myocardium, hinge line of leaflets and adipose tissue. An incomplete fibrous semi-ring glues these components. Asymmetric sphincteric contraction of the annulus depends almost exclusively on the posterior annulus. The dilation of the annulus mainly affects the posterior annulus. Prone to calcification |
| Septal annulus | Made up of the insertion of septal leaflet with collagen fibers. The hinge line of septal leaflet divides the membranous septum into two parts (see text) | Anterior annulus | Hinge line of anterior leaflet is in continuity with the mitral-aortic curtain. Reinforced by two fibrous nodules (trigons) at the extremities of the mitral-aortic curtain |
| Saddle shape configuration | Less accentuated both in systole and diastole. The saddle-shaped configuration disappears (the annulus become flat) in annular dilation | Saddle shape configuration | More accentuated both in systole and in diastole. The saddle-shaped configuration disappears (the annulus become flat) in annular dilation |
| Leaflets | Leaflets | ||
| Three main leaflets and three main commissures. Thin and fragile. The commissures do not reach the hinge line, leaving a strip of tissue between leaflets. Two or more leaflets inserted on mural annulus. Each leaflet presents with a basal, a clear and a rough zone. On the atrial side the rough zone corresponds to the coaptation zone. Additional leaflets especially on mural annulus. Three layers (atrialis, spongiosa and fibrosa) thinner that the corresponding mitral leaflets | Two main leaflets and two main commissures. Thick and robust. The commissures do not reach the hinge line, leaving a strip of tissue between leaflets. Three or more scallops on posterior leaflet Each leaflet presents with a clear and a rough zone. On the atrial side the rough zone corresponds to the coaptation zone. Three layers (atrialis, spongiosa and fibrosa) thicker than the corresponding tricuspid leaflets | ||
| Papillary muscles | Three papillary muscles. Anterior, inferior and septal. The anterior is the dominant arising from the moderator band. Usually the inferior papillary muscles have multiple and thin heads originating from the inferior wall. The septally located papillary muscle, may have multiple heads originating directly from the septum. | Papillary muscles | Two groups of papillary muscles: antero-medial and postero-lateral. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schlossbauer, S.A.; Faletra, F.F.; Paiocchi, V.L.; Leo, L.A.; Franciosi, G.; Bonanni, M.; Angelini, G.; Pavon, A.G.; Ferrari, E.; Ho, S.Y.; et al. Multimodality Imaging of the Anatomy of Tricuspid Valve. J. Cardiovasc. Dev. Dis. 2021, 8, 107. https://doi.org/10.3390/jcdd8090107
Schlossbauer SA, Faletra FF, Paiocchi VL, Leo LA, Franciosi G, Bonanni M, Angelini G, Pavon AG, Ferrari E, Ho SY, et al. Multimodality Imaging of the Anatomy of Tricuspid Valve. Journal of Cardiovascular Development and Disease. 2021; 8(9):107. https://doi.org/10.3390/jcdd8090107
Chicago/Turabian StyleSchlossbauer, Susanne Anna, Francesco Fulvio Faletra, Vera Lucia Paiocchi, Laura Anna Leo, Giorgio Franciosi, Michela Bonanni, Gianmarco Angelini, Anna Giulia Pavon, Enrico Ferrari, Siew Yen Ho, and et al. 2021. "Multimodality Imaging of the Anatomy of Tricuspid Valve" Journal of Cardiovascular Development and Disease 8, no. 9: 107. https://doi.org/10.3390/jcdd8090107