
Clinical Effectiveness and Safety of Once-Weekly GLP-1 Receptor Agonist Dulaglutide as Add-On to Metformin or Metformin Plus Insulin Secretagogues in Obesity and Type 2 Diabetes

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
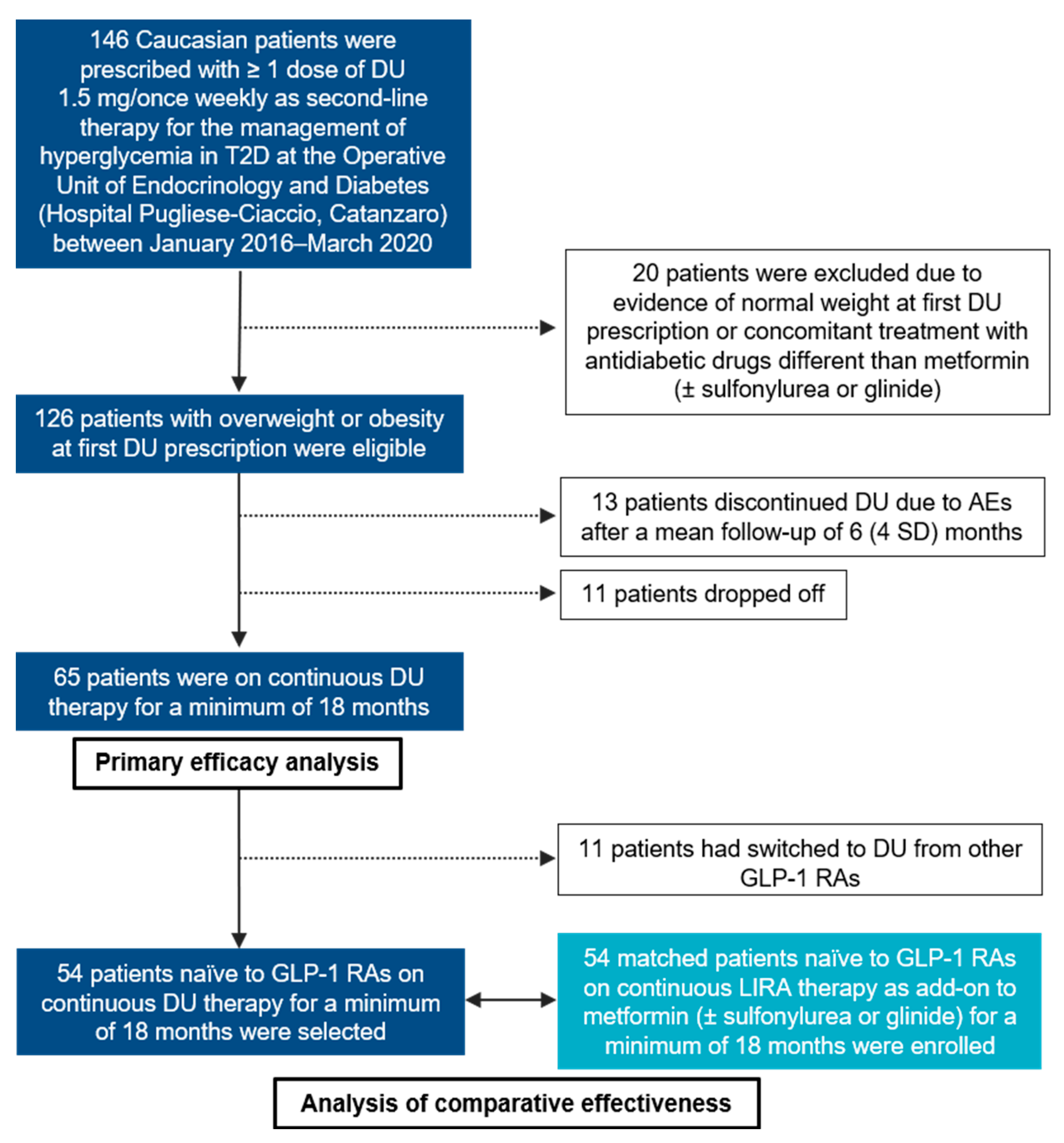
2.1. Study Participants
2.2. Assessments
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Cohort
3.2. Safety Outcomes
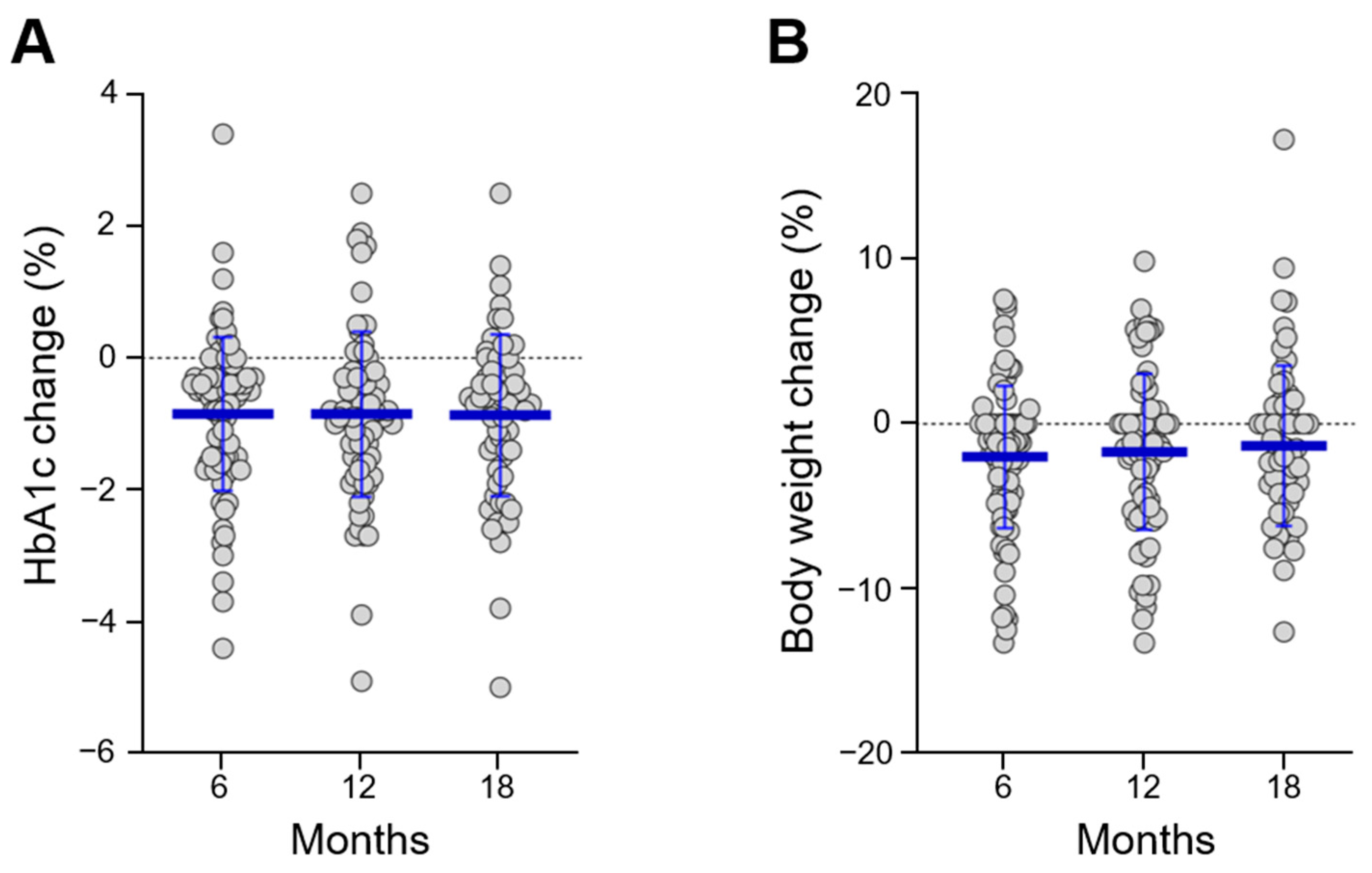
3.3. Efficacy Outcomes and Predictors of Response
3.4. Comparative Efficacy versus Liraglutide
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43 (Suppl. 1), S98–S110. [Google Scholar] [CrossRef] [Green Version]
- Madsen, K.S.; Kähler, P.; Kähler, L.K.; Madsbad, S.; Gnesin, F.; Metzendorf, M.I.; Richter, B.; Hemmingsen, B. Metformin and second- or third-generation sulphonylurea combination therapy for adults with type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2019, 4, CD012368. [Google Scholar] [CrossRef]
- Giorda, C.B.; Orsi, E.; De Cosmo, S.; Bossi, A.C.; Guerzoni, C.; Cercone, S.; Gilio, B.; Cavalot, F. Prescription of Sulphonylureas among Patients with Type 2 Diabetes Mellitus in Italy: Results from the Retrospective, Observational Multicentre Cross-Sectional SUSCIPE (Sulphonyl_UreaS_Correct_Internal_Prescription_Evaluation) Study. Diabetes Ther. 2020, 11, 2105–2119. [Google Scholar] [CrossRef]
- Apovian, C.M.; Okemah, J.; O’Neil, P.M. Body Weight Considerations in the Management of Type 2 Diabetes. Adv. Ther. 2019, 36, 44–58. [Google Scholar] [CrossRef] [Green Version]
- Potts, J.E.; Gray, L.J.; Brady, E.M.; Khunti, K.; Davies, M.J.; Bodicoat, D.H. The effect of glucagon-like peptide 1 receptor agonists on weight Loss in type 2 diabetes: A systematic review and mixed treatment comparison meta-analysis. PLoS ONE 2015, 10, e0126769. [Google Scholar] [CrossRef] [Green Version]
- Greco, M.; Chiefari, E.; Montalcini, T.; Accattato, F.; Costanzo, F.S.; Pujia, A.; Foti, D.; Brunetti, A.; Gulletta, E. Early effects of a hypocaloric, Mediterranean diet on laboratory parameters in obese individuals. Mediators Inflamm. 2014, 2014, 750860. [Google Scholar] [CrossRef] [Green Version]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.; Peters, A.; Wagenknecht, L. Look AHEAD Research Group. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar] [CrossRef] [Green Version]
- Hermansen, K.; Mortensen, L.S. Bodyweight changes associated with antihyperglycaemic agents in Type 2 diabetes mellitus. Drug Safe 2007, 30, 1127–1142. [Google Scholar] [CrossRef]
- Mirabelli, M.; Chiefari, E.; Caroleo, P.; Arcidiacono, B.; Corigliano, D.M.; Giuliano, S.; Brunetti, F.S.; Tanyolaç, S.; Foti, D.P.; Puccio, L.; et al. Long-Term Effectiveness of Liraglutide for Weight Management and Glycemic Control in Type 2 Diabetes. Int. J. Environ. Res. Public Health 2019, 17, 207. [Google Scholar] [CrossRef] [Green Version]
- Nauck, M.A.; Quast, D.R.; Wefers, J.; Meier, J.J. GLP-1 receptor agonists in the treatment of type 2 diabetes—State-of-the-art. Mol. Metab. 2020, 101102. [Google Scholar] [CrossRef]
- European Medicines Agency. TRULICITY, INN-Dulaglutide, Product Information. Available online: https://www.ema.europa.eu/en/documents/product-information/trulicity-epar-product-information_en.pdf (accessed on 8 January 2021).
- Nauck, M.; Weinstock, R.S.; Umpierrez, G.E.; Guerci, B.; Skrivanek, Z.; Milicevic, Z. Efficacy and safety of dulaglutide versus sitagliptin after 52 weeks in type 2 diabetes in a randomized controlled trial (AWARD-5). Diabetes Care 2014, 37, 2149–2158. [Google Scholar] [CrossRef] [Green Version]
- Giorgino, F.; Benroubi, M.; Sun, J.H.; Zimmermann, A.G.; Pechtner, V. Efficacy and Safety of Once-Weekly Dulaglutide Versus Insulin Glargine in Patients With Type 2 Diabetes on Metformin and Glimepiride (AWARD-2). Diabetes Care 2015, 38, 2241–2249. [Google Scholar] [CrossRef] [Green Version]
- Chang, K.C.; Shao, S.C.; Kuo, S.; Yang, C.Y.; Chen, H.Y.; Chan, Y.Y.; Ou, H.T. Comparative effectiveness of dulaglutide versus liraglutide in Asian type 2 diabetes patients: A multi-institutional cohort study and meta-analysis. Cardiovasc. Diabetol. 2020, 19, 172. [Google Scholar] [CrossRef]
- Wasir, J.S.; Mithal, A.; Agarwal, P.; Mittal, A. Once Weekly Dulaglutide Therapy in Type 2 Diabetic Subjects, Real-world Evidence from a Tertiary Care Diabetes Center in India. Indian J. Endocrinol. Metab. 2018, 22, 728–734. [Google Scholar] [CrossRef]
- Mody, R.; Grabner, M.; Yu, M.; Turner, R.; Kwan, A.Y.; York, W.; Fernández Landó, L. Real-world effectiveness, adherence and persistence among patients with type 2 diabetes mellitus initiating dulaglutide treatment. Curr. Med. Res. Opin. 2018, 34, 995–1003. [Google Scholar] [CrossRef] [Green Version]
- Yoo, J.H.; Cho, Y.K.; Lee, J.; Kim, H.S.; Kang, Y.M.; Jung, C.H.; Park, J.Y.; Lee, W.J. Clinical Efficacy and Parameters Affecting the Response to Dulaglutide Treatment in Patients with Type 2 Diabetes: A Retrospective, Real-World Data Study. Diabetes Ther. 2019, 10, 1453–1463. [Google Scholar] [CrossRef] [Green Version]
- Obregón, F.M.; Miramontes-González, J.P.; Guajardo-Fajardo, C.R.; Nieto-Sánchez, Á.; López-Suárez, J.M.; Martín-Vallejo, J.; Arco-Prados, Y.; de Lucas, M.D.; León-Jiménez, D. Real-life experience with Dulaglutide: Analysis of clinical effectiveness to 24 months. Diabetes Res. Clin. Pract. 2019, 158, 107916. [Google Scholar] [CrossRef]
- Lee, J.; Cho, Y.K.; Kim, H.S.; Jung, C.H.; Park, J.Y.; Lee, W.J. Dulaglutide as an Add-on to Insulin in Type 2 Diabetes; Clinical Efficacy and Parameters Affecting the Response in Real-World Practice. Diabetes Metab. Syndr. Obes. 2019, 12, 2745–2753. [Google Scholar] [CrossRef] [Green Version]
- Berra, C.C.; Resi, V.; Mirani, M.; Folini, L.; Rossi, A.; Solerte, S.B.; Fiorina, P. Clinical efficacy and predictors of response to dulaglutide in type-2 diabetes. Pharmacol. Res. 2020, 159, 104996. [Google Scholar] [CrossRef]
- Mirabelli, M.; Chiefari, E.; Caroleo, P.; Vero, R.; Brunetti, F.S.; Corigliano, D.M.; Arcidiacono, B.; Foti, D.P.; Puccio, L.; Brunetti, A. Long-Term Effectiveness and Safety of SGLT-2 Inhibitors in an Italian Cohort of Patients with Type 2 Diabetes Mellitus. J. Diabetes Res. 2019, 2019, 3971060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiefari, E.; Capula, C.; Vero, A.; Oliverio, R.; Puccio, L.; Liguori, R.; Pullano, V.; Greco, M.; Foti, D.; Tirinato, D.; et al. Add-On Treatment with Liraglutide Improves Glycemic Control in Patients with Type 2 Diabetes on Metformin Therapy. Diabetes Technol. Ther. 2015, 17, 468–474. [Google Scholar] [CrossRef]
- Associazione Medici Diabetologi, Società Italiana di Diabetologia. Standard di cura del Diabete Mellito AMD-SID 2018. Available online: http://www.siditalia.it/pdf/Standard%20di%20Cura%20AMD%20-%20SID%202018_protetto2.pdf (accessed on 8 January 2021).
- Tuttle, K.R.; Lakshmanan, M.C.; Rayner, B.; Busch, R.S.; Zimmermann, A.G.; Woodward, D.B.; Botros, F.T. Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7): A multicentre, open-label, randomised trial. Lancet Diabetes Endocrinol. 2018, 6, 605–617. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet 2019, 394, 121–130. [Google Scholar] [CrossRef]
- Frison, V.; Simioni, N.; Marangoni, A.; Balzano, S.; Vinci, C.; Zenari, L.; De Moliner, L.; Tadiotto, F.; D’Ambrosio, M.; Confortin, L.; et al. Clinical Impact of 5 Years of Liraglutide Treatment on Cardiovascular Risk Factors in Patients with Type 2 Diabetes Mellitus in a Real-Life Setting in Italy: An Observational Study. Diabetes Ther. 2018, 9, 2201–2208. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.C.; Dekoven, M.; Bouchard, J.; Massoudi, M.; Langer, J. Improved real-world glycaemic outcomes with liraglutide versus other incretin-based therapies in type 2 diabetes. Diabetes Obes. Metab. 2014, 16, 819–826. [Google Scholar] [CrossRef]
- Gail, M.H. Frequency Matching. In Encyclopedia of Biostatistics; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2005. [Google Scholar] [CrossRef]
- Morieri, M.L.; Rigato, M.; Frison, V.; Simioni, N.; D’Ambrosio, M.; Tadiotto, F.; Paccagnella, A.; Lapolla, A.; Avogaro, A.; Fadini, G.P. Effectiveness of dulaglutide vs liraglutide and exenatide once-weekly. A real-world study and meta-analysis of observational studies. Metabolism 2020, 106, 154190. [Google Scholar] [CrossRef] [Green Version]
- Wysham, C.; Blevins, T.; Arakaki, R.; Colon, G.; Garcia, P.; Atisso, C.; Kuhstoss, D.; Lakshmanan, M. Efficacy and safety of dulaglutide added onto pioglitazone and metformin versus exenatide in type 2 diabetes in a randomized controlled trial (AWARD-1). Diabetes Care 2014, 37, 2159–2167. [Google Scholar] [CrossRef] [Green Version]
- Blonde, L.; Jendle, J.; Gross, J.; Woo, V.; Jiang, H.; Fahrbach, J.L.; Milicevic, Z. Once-weekly dulaglutide versus bedtime insulin glargine, both in combination with prandial insulin lispro, in patients with type 2 diabetes (AWARD-4): A randomised, open-label, phase 3, non-inferiority study. Lancet 2015, 385, 2057–2066. [Google Scholar] [CrossRef]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef] [Green Version]
- Mann, J.F.; Ørsted, D.D.; Brown-Frandsen, K.; Marso, S.P.; Poulter, N.R.; Rasmussen, S.; Tornøe, K.; Zinman, B.; Buse, J.B. Liraglutide and Renal Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 839–848. [Google Scholar] [CrossRef] [Green Version]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Botros, F.T.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and renal outcomes in type 2 diabetes: An exploratory analysis of the REWIND randomised, placebo-controlled trial. Lancet 2019, 394, 131–138. [Google Scholar] [CrossRef]
- Shaw, J.E.; Botros, F.T.; Malik, R.; Atisso, C.; Colhoun, H.M.; Gerstein, H.C. 356-OR: Effect of Dulaglutide on Kidney Function–Related Outcomes in Type 2 Diabetes: Post Hoc Analysis from the REWIND Trial. Diabetes 2020, 69 (Suppl. 1). [Google Scholar] [CrossRef]
- Greco, E.V.; Russo, G.; Giandalia, A.; Viazzi, F.; Pontremoli, R.; De Cosmo, S. GLP-1 Receptor Agonists and Kidney Protection. Medicina 2019, 55, 233. [Google Scholar] [CrossRef] [Green Version]
- Brunetti, A. Endocrines: A Passion for Endocrinology. Endocrines 2020, 1, 46–48. [Google Scholar] [CrossRef]
- Gallwitz, B.; Dagogo-Jack, S.; Thieu, V.; Garcia-Perez, L.E.; Pavo, I.; Yu, M.; Robertson, K.E.; Zhang, N.; Giorgino, F. Effect of once-weekly dulaglutide on glycated haemoglobin (HbA1c) and fasting blood glucose in patient subpopulations by gender, duration of diabetes and baseline HbA1c. Diabetes Obes. Metab. 2018, 20, 409–418. [Google Scholar] [CrossRef] [Green Version]
- Anichini, R.; Cosimi, S.; Di Carlo, A.; Orsini, P.; De Bellis, A.; Seghieri, G.; Franconi, F.; Baccetti, F. Gender difference in response predictors after 1-year exenatide therapy twice daily in type 2 diabetic patients: A real world experience. Diabetes Metab. Syndr. Obes. 2013, 6, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Wilding, J.P.; Overgaard, R.V.; Jacobsen, L.V.; Jensen, C.B.; le Roux, C.W. Exposure-response analyses of liraglutide 3.0 mg for weight management. Diabetes Obes. Metab. 2016, 18, 491–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franconi, F.; Campesi, I.; Occhioni, S.; Tonolo, G. Sex-gender differences in diabetes vascular complications and treatment. Endocr. Metab. Immune Disord. Drug Targets 2012, 12, 179–196. [Google Scholar] [CrossRef]
- Khera, R.; Murad, M.H.; Chandar, A.K.; Dulai, P.S.; Wang, Z.; Prokop, L.J.; Loomba, R.; Camilleri, M.; Singh, S. Association of Pharmacological Treatments for Obesity With Weight Loss and Adverse Events: A Systematic Review and Meta-analysis. JAMA 2016, 315, 2424–2434. [Google Scholar] [CrossRef]
- U.S. Food and Drugs Administration. Highlights of Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/125469s036lbl.pdf (accessed on 8 January 2021).
- Roberts, M.H.; Ferguson, G.T. Real-World Evidence: Bridging Gaps in Evidence to Guide Payer Decisions. Pharm. Open 2020. [Google Scholar] [CrossRef]
- Chiefari, E.; Tanyolac, S.; Iiritano, S.; Sciacqua, A.; Capula, C.; Arcidiacono, B.; Nocera, A.; Possidente, K.; Baudi, F.; Ventura, V.; et al. A polymorphism of HMGA1 is associated with increased risk of metabolic syndrome and related components. Sci. Rep. 2013, 3, 1491. [Google Scholar] [CrossRef] [PubMed]
- Brunetti, A.; Chiefari, E.; Foti, D.P. Pharmacogenetics in type 2 diabetes: Still a conundrum in clinical practice. Expert Rev. Endocrinol. Metab. 2017, 12, 155–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Clinical and Demographic Characteristics | N or Means % or (SD) | |
|---|---|---|
| Female gender, N | 61 | 48.4% |
| Age, yr | 59.8 | (9.4) |
| T2D duration, yr | 8.0 | (6.0) |
| T2D duration >10 yr | 41 | 32.5% |
| Hypertension, N | 97 | 77.0% |
| CHD, N | 11 | 8.7% |
| History of stroke/TIA, N | 4 | 3.2% |
| Peripheral arterial disease, N | 2 | 1.6% |
| Overweight (BMI 25–29.9 kg/m2), N | 46 | 36.5% |
| Obesity (BMI ≥ 30 kg/m2), N | 80 | 63.5% |
| Dyslipidemia, N | 76 | 60.3% |
| Other comorbidities, N | 86 | 68.3% |
| Microvascular diabetic complications, N | 23 | 18.3% |
| Diabetic retinopathy, N | 9 | 7.1% |
| Early-stage DKD, N | 8 | 6.4% |
| Advanced stage DKD, N | 1 | 0.8% |
| Diabetic neuropathy, N | 9 | 7.1% |
| Background Medications | ||
| ACE inhibitors, N | 34 | 27.0% |
| ARB, N | 42 | 33.3% |
| Calcium blockers, N | 15 | 11.9% |
| Beta-blockers, N | 37 | 29.4% |
| Diuretics, N | 46 | 36.5% |
| Alpha1 blockers, N | 7 | 5.6% |
| Statin, N | 59 | 46.8% |
| Ezetimibe, N | 6 | 4.8% |
| Cardioaspirin, N | 23 | 18.3% |
| Other medications, N | 45 | 35.7% |
| MET, N | 126 | 100% |
| MET plus sulfonylurea, N | 18 | 14.2% |
| MET plus glinide, N | 9 | 7.1% |
| Naïve to GLP-1 RAs, N | 109 | 86.5% |
| Parameter | Baseline (N = 126) | 6 Months (N = 89) | 12 Months (N = 77) | 18 Months (N = 65) | p Value (0 vs. 6 Months) | p Value (0 vs. 12 Months) | p Value (0 vs. 18 Months) |
|---|---|---|---|---|---|---|---|
| Creatinine, mg/dL | 0.85 (0.19) | 0.90 (0.18) | 0.85 (0.22) | 0.94 (0.19) | 0.624 | 0.906 | 0.097 |
| eGFR, mL/min | 90.1 (25.1) | 82.1 (15.0) | 91.1 (21.9) | 84.1 (20.7) | 0.461 | 1.000 | 0.049 |
| AST, U/L | 26.9 (11.8) | 29.6 (19.4) | 25.7 (9.0) | 29.3 (10.9) | 0.819 | 0.716 | 0.442 |
| ALT, U/L | 31.4 (18.4) | 26.0 (11.9) | 25.8 (13.2) | 24.3 (7.0) | 0.041 | 0.166 | 0.451 |
| Parameter | Baseline (N = 126) | 6 Months (N = 89) | 12 Months (N = 77) | 18 Months (N = 65) | p Value (0 vs. 6 Months) | p Value (0 vs. 12 Months) | p Value (0 vs. 18 Months) |
|---|---|---|---|---|---|---|---|
| HbA1c, % | 7.8 (1.0) | 7.0 (1.0) | 7.0 (1.2) | 6.9 (1.0) | <0.001 | <0.001 | <0.001 |
| FPG, mg/dL | 169.4 (37.9) | 140.5 (27.1) | 145.0 (38.4) | 141.4 (28.3) | <0.001 | <0.001 | <0.001 |
| Body weight, kg | 92.1 (16.9) | 89.9 (17.2) | 91.8 (17.6) | 91.4 (18.5) | <0.001 | 0.002 | 0.007 |
| BMI, kg/m2 | 33.2 (5.7) | 32.8 (6.0) | 33.2 (6.0) | 32.8 (6.0) | <0.001 | 0.003 | 0.006 |
| Systolic BP, mmHg | 129.8 (14.5) | 130.9 (14.7) | 128.6 (14.6) | 131.5 (12.6) | 0.407 | 0.758 | 0.758 |
| Diastolic BP, mmHg | 76.3 (10.5) | 77.2 (11.1) | 77.3 (10.4) | 76.5 (8.2) | 0.279 | 0.084 | 0.084 |
| Total chol., mg/dL | 175.8 (35.6) | 164.8 (30.2) | 161.7 (32.4) | 166.6 (35.5) | 0.022 | 0.005 | 0.017 |
| LDL-chol., mg/dL | 98.9 (31.1) | 89.3 (23.7) | 87.2 (28.2) | 82.8 (28.3) | 0.030 | 0.040 | 0.065 |
| HDL-chol., mg/dL | 47.8 (10.7) | 47.4 (11.5) | 49.2 (10.7) | 49.1 (11.7) | 0.786 | 0.274 | 0.820 |
| TG, mg/dL | 155.9 (110.6) | 143.3 (67.0) | 140.1 (82.3) | 152.9 (61.3) | 0.200 | 0.011 | 0.763 |
| Outcome | Predictor | OR | (95% CI) | p Value |
|---|---|---|---|---|
| Drug discontinuation due to AEs * | Baseline BMI ≥ 30 kg/m2 | 0.211 | (0.058–0.771) | 0.019 |
| HbA1c reduction ≥ 0.5% | Baseline HbA1c % | 2.961 | (1.394–6.290) | 0.005 |
| Body weight loss ≥ 5% | Baseline HbA1c % | 2.571 | (1.171–5.644) | 0.019 |
| Outcomes | LIRA (N = 54) | DU (N = 54) | p Value |
|---|---|---|---|
| Body weight reduction ≥ 5% | 15 (27.8%) | 13 (24.1%) | 0.827 |
| HbA1c reduction ≥ 0.5% | 32 (59.3%) | 34 (63.0%) | 0.987 |
| HbA1c ≤ 7% | 23 (42.6%) | 35 (64.8%) | 0.033 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mirabelli, M.; Chiefari, E.; Tocci, V.; Caroleo, P.; Giuliano, S.; Greco, E.; Luque, R.M.; Puccio, L.; Foti, D.P.; Aversa, A.; et al. Clinical Effectiveness and Safety of Once-Weekly GLP-1 Receptor Agonist Dulaglutide as Add-On to Metformin or Metformin Plus Insulin Secretagogues in Obesity and Type 2 Diabetes. J. Clin. Med. 2021, 10, 985. https://doi.org/10.3390/jcm10050985
Mirabelli M, Chiefari E, Tocci V, Caroleo P, Giuliano S, Greco E, Luque RM, Puccio L, Foti DP, Aversa A, et al. Clinical Effectiveness and Safety of Once-Weekly GLP-1 Receptor Agonist Dulaglutide as Add-On to Metformin or Metformin Plus Insulin Secretagogues in Obesity and Type 2 Diabetes. Journal of Clinical Medicine. 2021; 10(5):985. https://doi.org/10.3390/jcm10050985
Chicago/Turabian StyleMirabelli, Maria, Eusebio Chiefari, Vera Tocci, Patrizia Caroleo, Stefania Giuliano, Emanuela Greco, Raul Miguel Luque, Luigi Puccio, Daniela Patrizia Foti, Antonio Aversa, and et al. 2021. "Clinical Effectiveness and Safety of Once-Weekly GLP-1 Receptor Agonist Dulaglutide as Add-On to Metformin or Metformin Plus Insulin Secretagogues in Obesity and Type 2 Diabetes" Journal of Clinical Medicine 10, no. 5: 985. https://doi.org/10.3390/jcm10050985