
Stereolithography vs. Direct Light Processing for Rapid Manufacturing of Complete Denture Bases: An In Vitro Accuracy Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Experimental Section
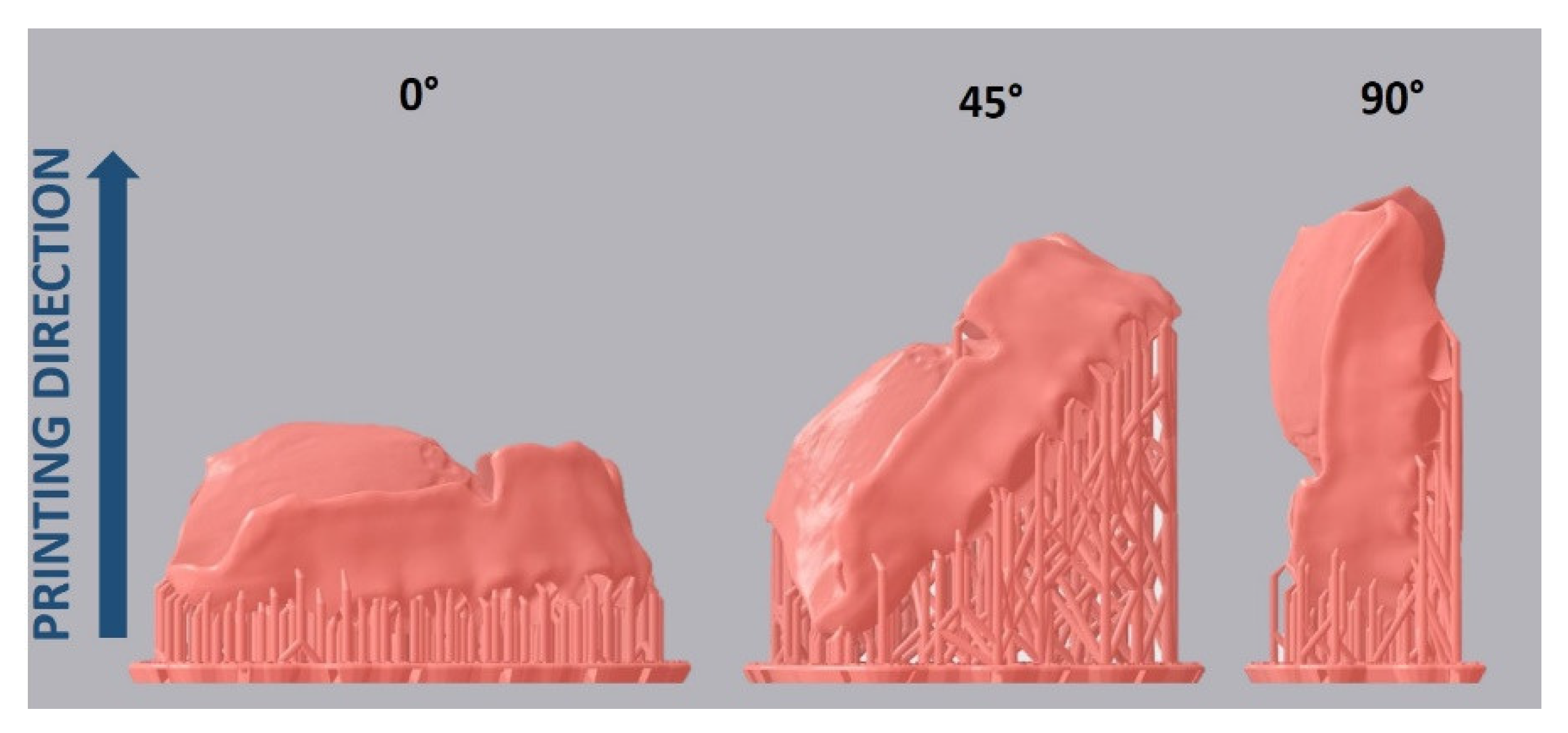
2.1. Specimen Design and Fabrication
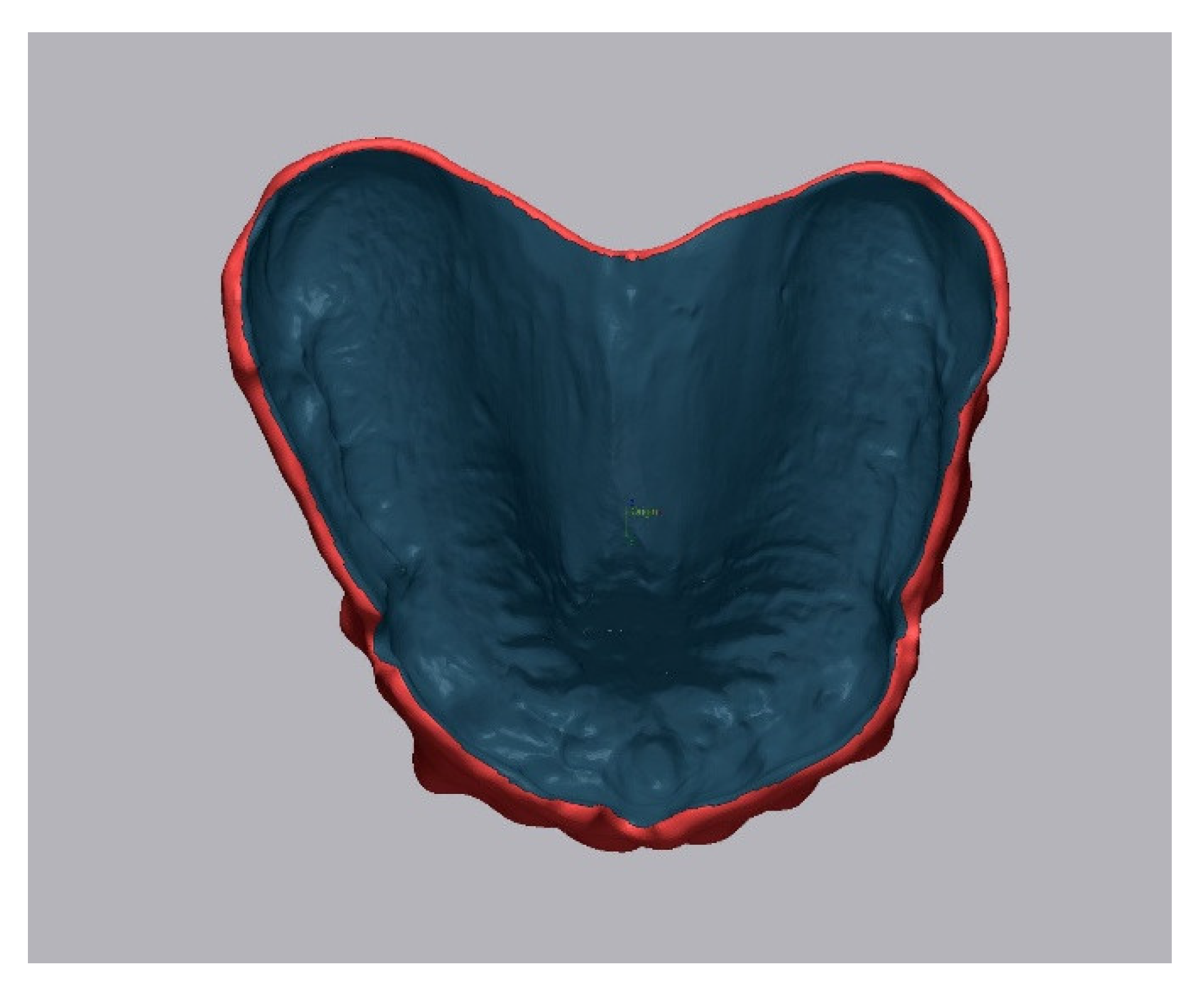
2.2. Accuracy Analysis
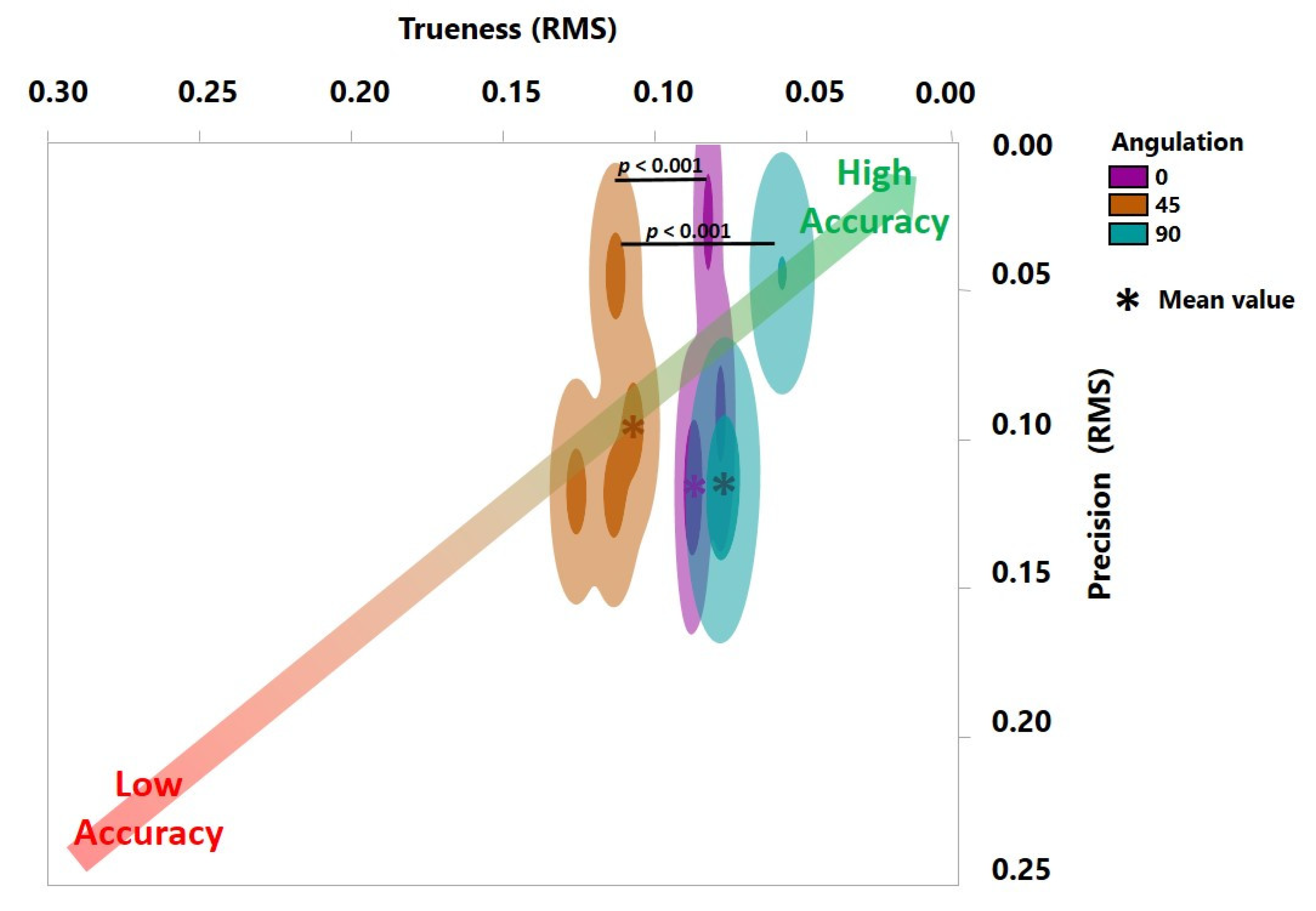
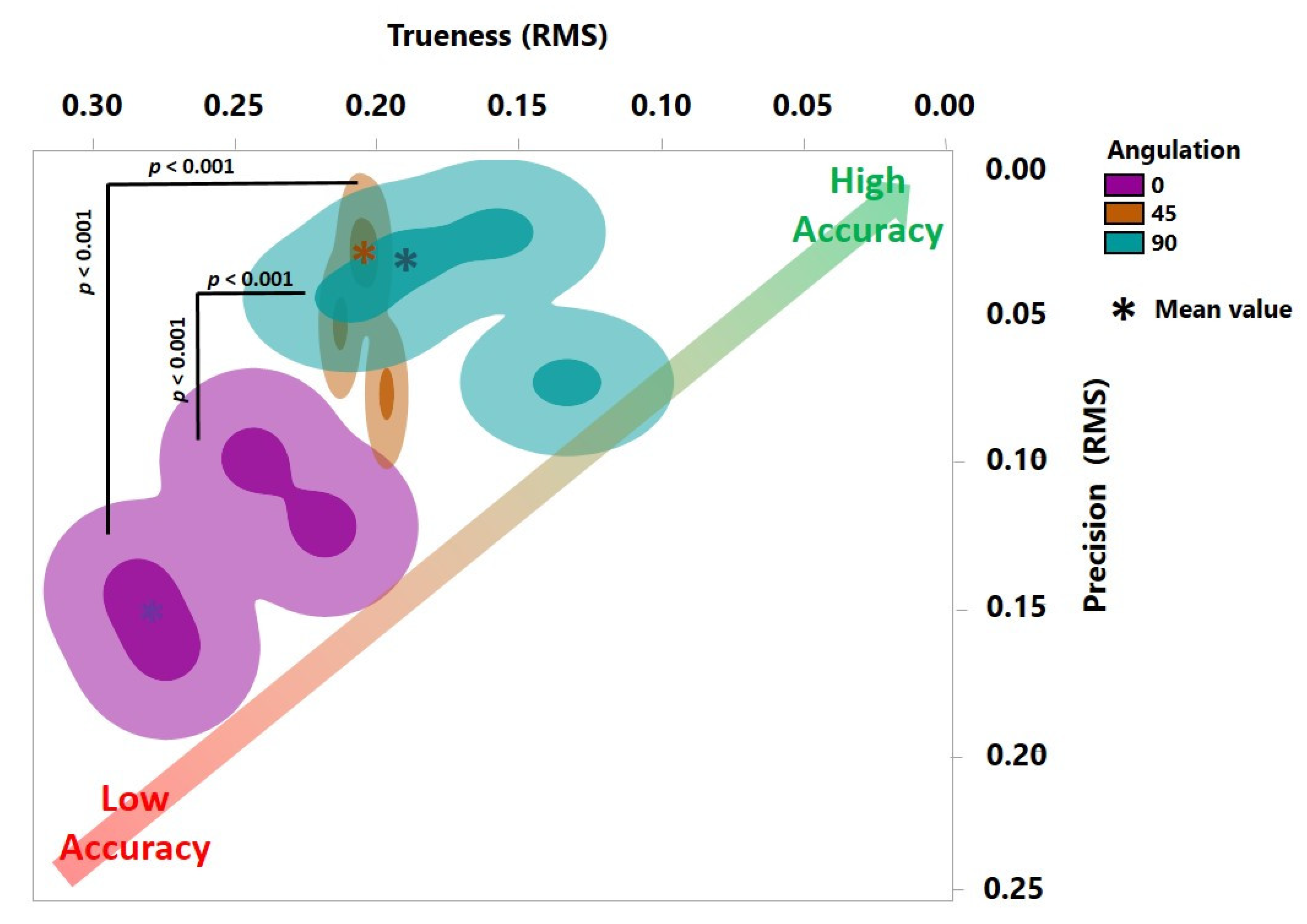
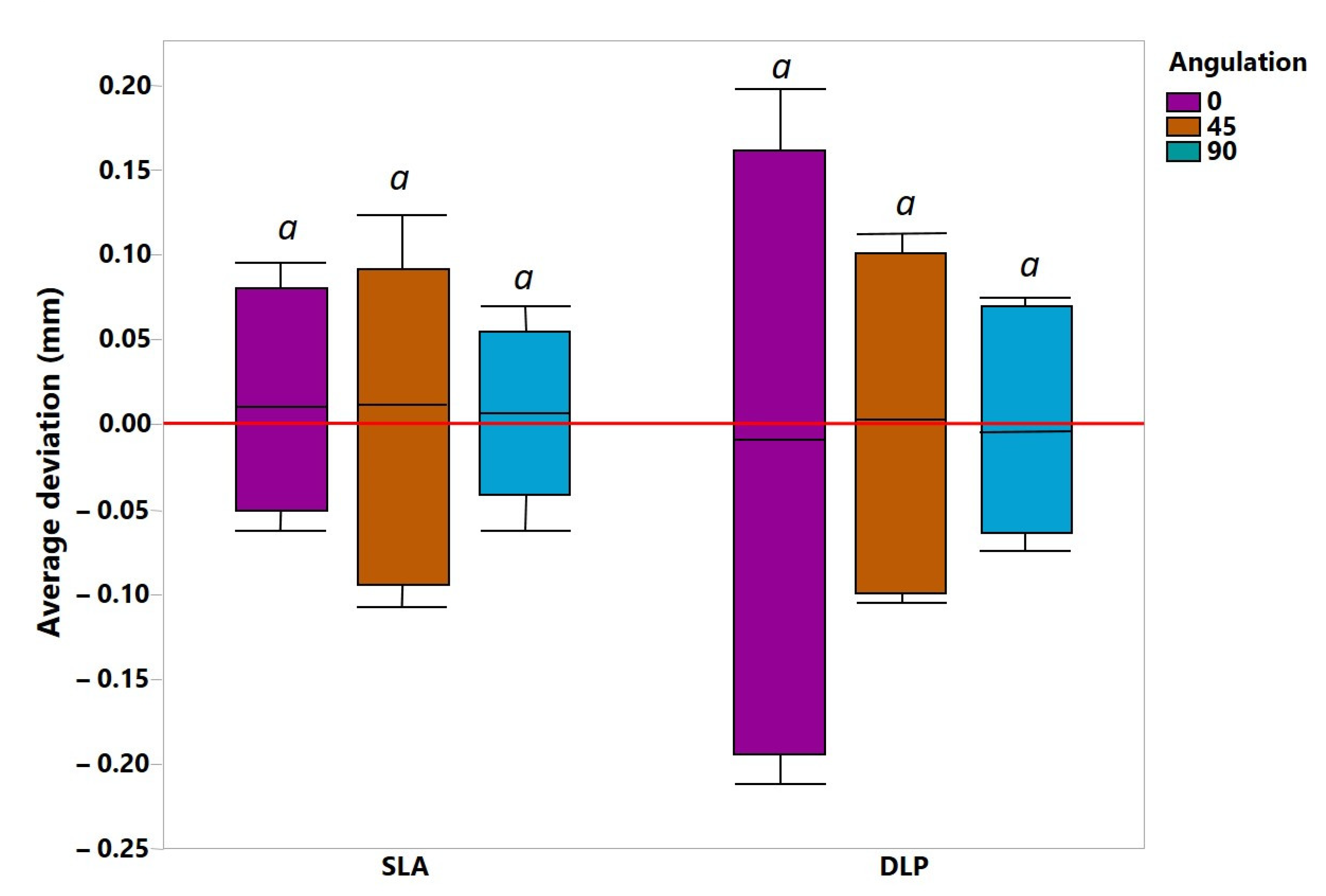
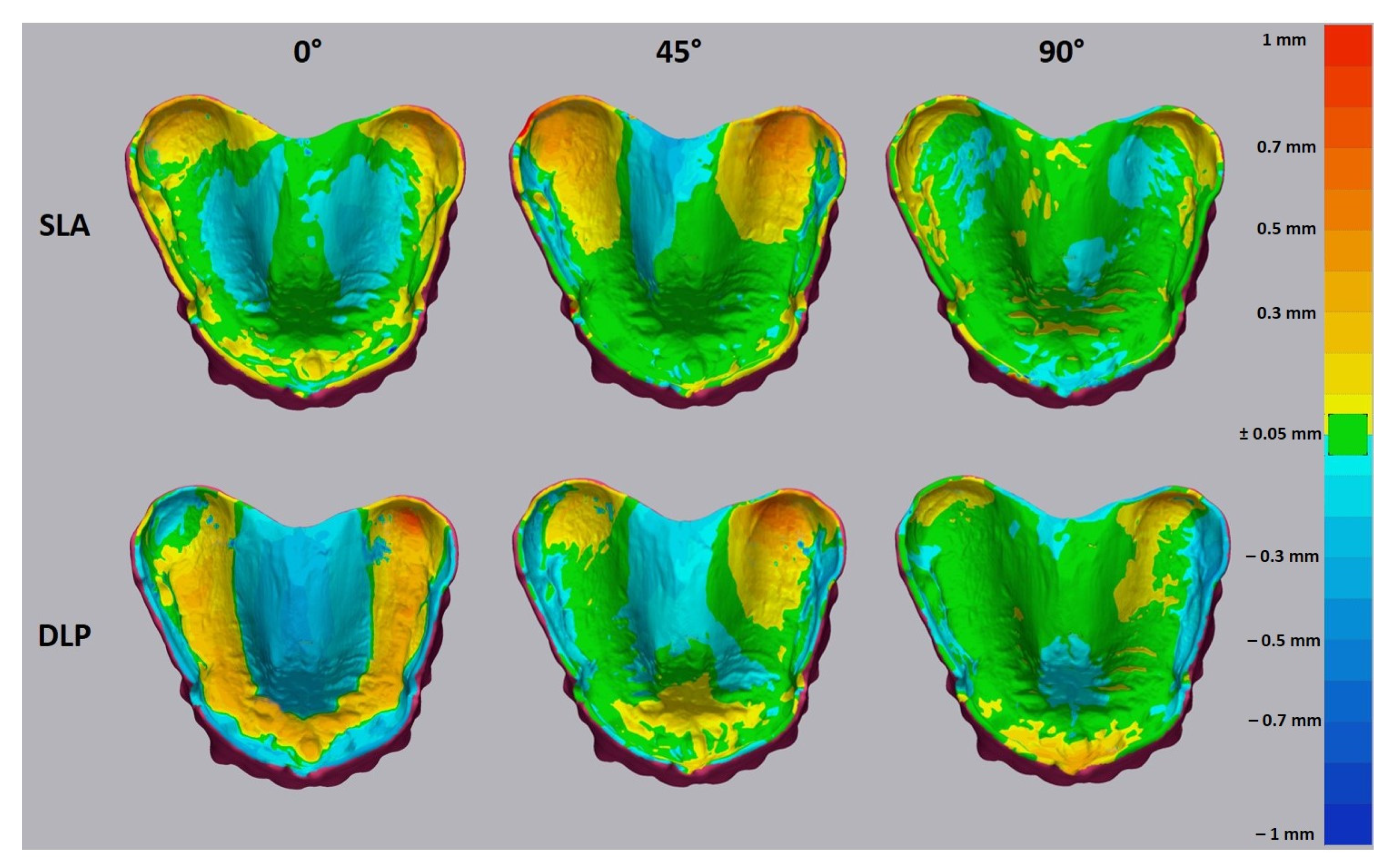
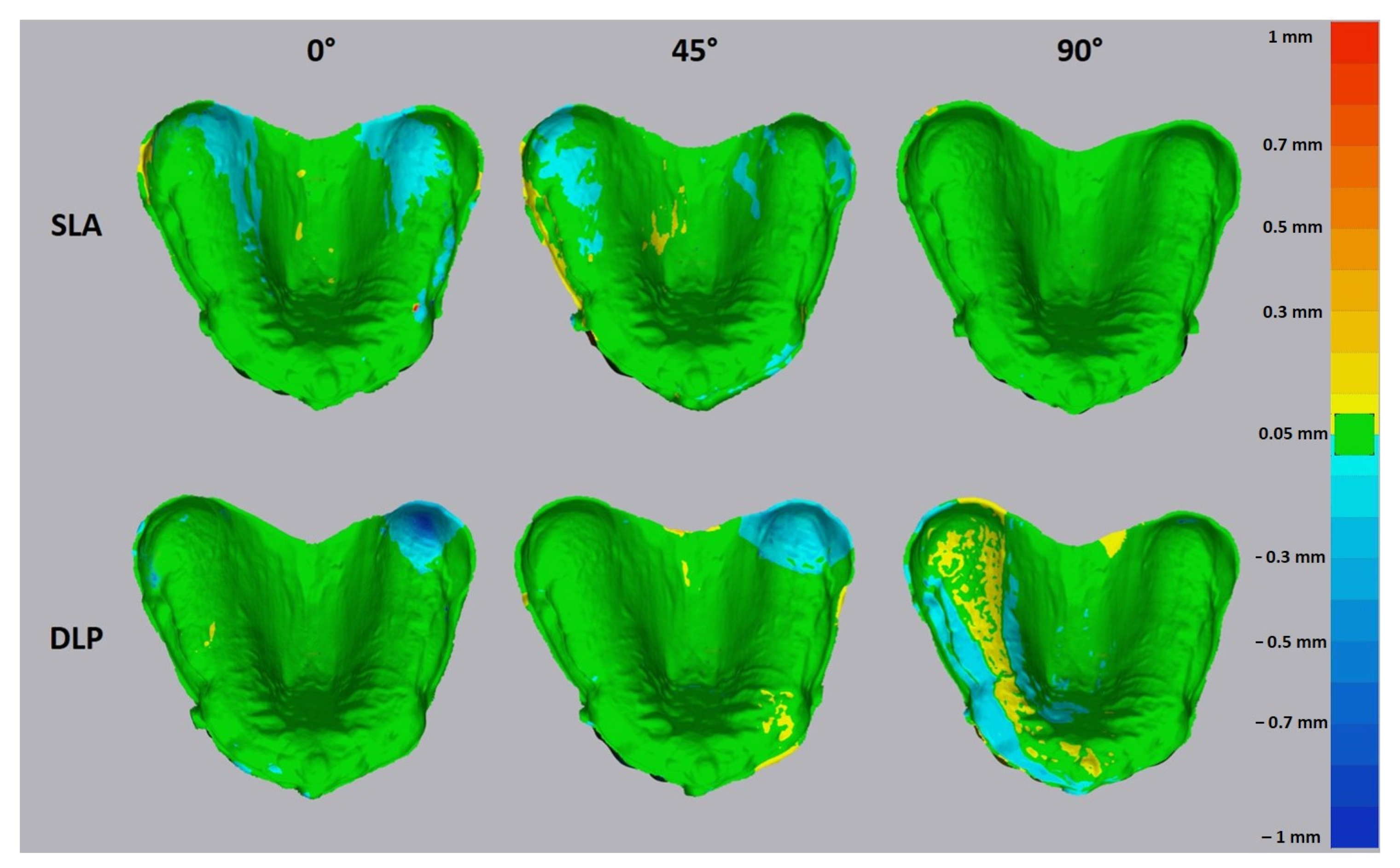
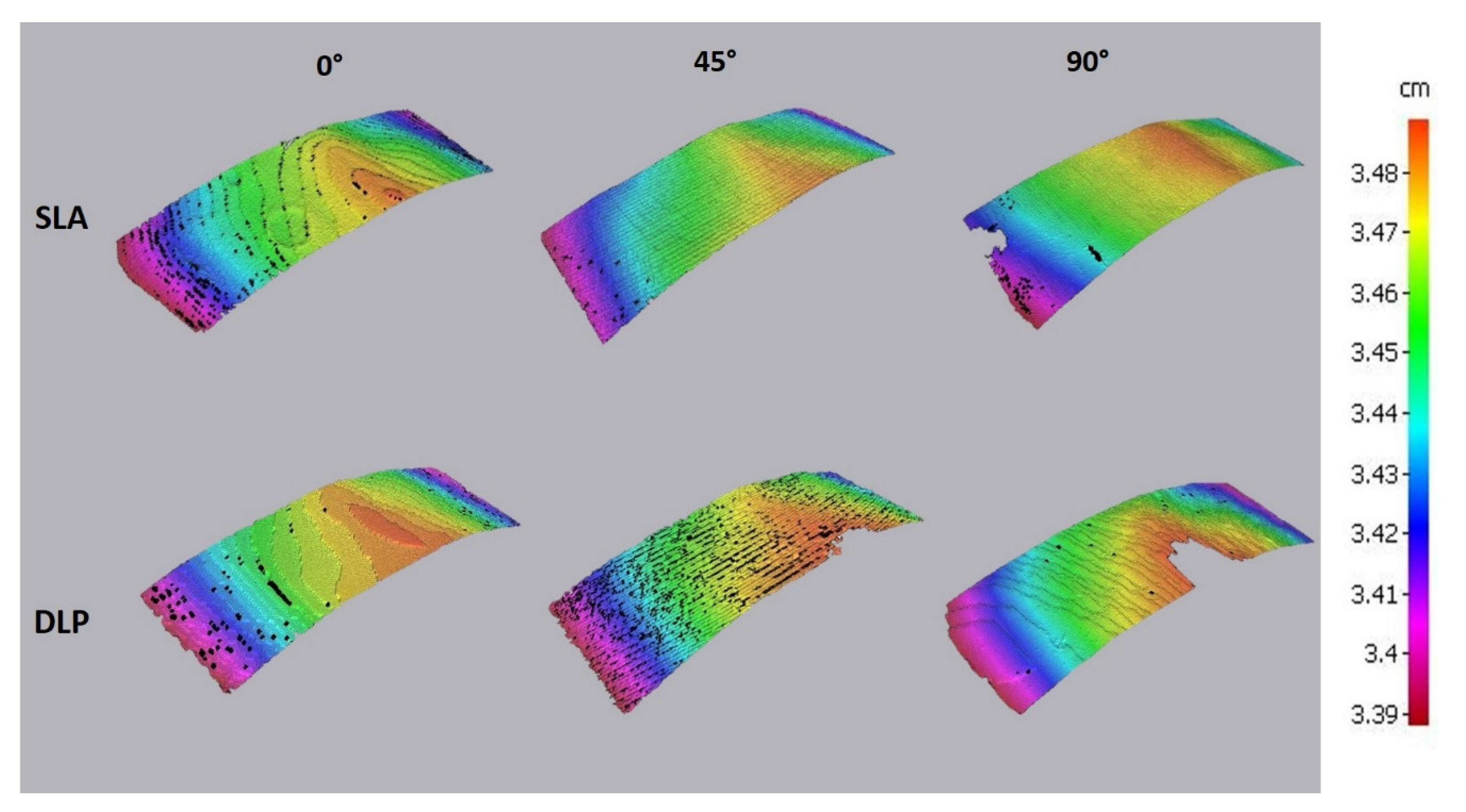
3. Results
4. Discussion
4.1. Outcomes of the Accuracy Test
4.2. Clinical Interpretation
5. Conclusions
- SLA may produce an intaglio denture surface with a better trueness than DLP;
- SLA and DLP demonstrated nearly the same precision for 3D printing of denture bases;
- The build orientation of 90° may provide the best trueness for both SLA and DLP;
- Besides the illumination source of a 3D printing hardware (SLA, DLP, LCD), the geometrical accuracy may be presumably influenced by part geometry and material type.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wemken, G.; Spies, B.C.; Pieralli, S.; Adali, U.; Beuer, F.; Wesemann, C. Do hydrothermal aging and microwave sterilization affect the trueness of milled, additive manufactured and injection molded denture bases? J. Mech. Behav. Biomed. Mater. 2020, 111, 103975. [Google Scholar] [CrossRef]
- Schweiger, J.; Stumbaum, J.; Edelhoff, D.; Güth, J.-F. Systematics and concepts for the digital production of complete dentures: Risks and opportunities. Int. J. Comput. Dent. 2018, 21, 41–56. [Google Scholar]
- Schweiger, J.; Güth, J.-F.; Edelhoff, D.; Stumbaum, J. Virtual evaluation for CAD-CAM-fabricated complete dentures. J. Prosthet. Dent. 2017, 117, 28–33. [Google Scholar] [CrossRef]
- Lin, W.-S.; Harris, B.T.; Pellerito, J.; Morton, D. Fabrication of an interim complete removable dental prosthesis with an in-office digital light processing three-dimensional printer: A proof-of-concept technique. J. Prosthet. Dent. 2018, 120, 331–334. [Google Scholar] [CrossRef]
- Unkovskiy, A.; Wahl, E.; Zander, A.T.; Huettig, F.; Spintzyk, S. Intraoral scanning to fabricate complete dentures with functional borders: A proof-of-concept case report. BMC Oral Health 2019, 19, 46. [Google Scholar] [CrossRef] [Green Version]
- Bilgin, M.S.; Erdem, A.; Aglarci, O.S.; Dilber, E. Fabricating Complete Dentures with CAD/CAM and RP Technologies. J. Prosthodont. 2015, 24, 576–579. [Google Scholar] [CrossRef] [PubMed]
- Cristache, C.M.; Totu, E.E.; Iorgulescu, G.; Pantazi, A.; Dorobantu, D.; Nechifor, A.C.; Isildak, I.; Burlibasa, M.; Nechifor, G.; Enachescu, M. Eighteen Months Follow-Up with Patient-Centered Outcomes Assessment of Complete Dentures Manufactured Using a Hybrid Nanocomposite and Additive CAD/CAM Protocol. J. Clin. Med. 2020, 9, 324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inokoshi, M.; Kanazawa, M.; Minakuchi, S. Evaluation of a complete denture trial method applying rapid prototyping. Dent. Mater. J. 2012, 31, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berman, B. 3-D printing: The new industial revolution. Bus. Horiz. 2012, 55, 155–162. [Google Scholar] [CrossRef]
- Yoon, H.-I.; Hwang, H.-J.; Ohkubo, C.; Han, J.-S.; Park, E.-J. Evaluation of the trueness and tissue surface adaptation of CAD-CAM mandibular denture bases manufactured using digital light processing. J. Prosthet. Dent. 2018, 120, 919–926. [Google Scholar] [CrossRef]
- Hwang, H.-J.; Lee, S.J.; Park, E.-J.; Yoon, H.-I. Assessment of the trueness and tissue surface adaptation of CAD-CAM maxillary denture bases manufactured using digital light processing. J. Prosthet. Dent. 2019, 121, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.-C.; Yoon, H.-I.; Yeo, I.-S.; Kim, S.-H.; Han, J.-S. The effect of build angle on the tissue surface adaptation of maxillary and mandibular complete denture bases manufactured by digital light processing. J. Prosthet. Dent. 2020, 123, 473–482. [Google Scholar] [CrossRef]
- Yoon, S.-N.; Oh, K.C.; Lee, S.J.; Han, J.-S.; Yoon, H.-I. Tissue surface adaptation of CAD-CAM maxillary and mandibular complete denture bases manufactured by digital light processing: A clinical study. J. Prosthet. Dent. 2020, 124, 682–689. [Google Scholar] [CrossRef]
- Stansbury, J.W.; Idacavage, M.J. 3D printing with polymers: Challenges among expanding options and opportunities. Dent. Mater. 2016, 32, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Gibson, I.; Rosen, D.W.; Stucker, B. Additive Manufacturing Technologies, 2nd ed.; Springer: Boston, MA, USA, 2015; pp. 63–106. [Google Scholar]
- Taormina, G.; Sciancalepore, C.; Messori, M.; Bondioli, F. 3D printing processes for photocurable polymeric materials: Technologies, materials, and future trends. J. Appl. Biomater. Funct. Mater. 2018, 16, 151–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unkovskiy, A.; Roehler, A.; Huettig, F.; Geis-Gerstorfer, J.; Brom, J.; Keutel, C.; Spintzyk, S. Simplifying the digital workflow of facial prostheses manufacturing using a three-dimensional (3D) database: Setup, development, and aspects of virtual data validation for reproduction. J. Prosthodont. Res. 2019, 63, 313–320. [Google Scholar] [CrossRef]
- Unkovskiy, A.; Bui, P.H.-B.; Schille, C.; Geis-Gerstorfer, J.; Huettig, F.; Spintzyk, S. Objects build orientation, positioning, and curing influence dimensional accuracy and flexural properties of stereolithographically printed resin. Dent. Mater. 2018, 34, e324–e333. [Google Scholar] [CrossRef] [PubMed]
- Ollison, T.; Berisso, K. Three-dimensional printing build variables that impact cylindricity. J. Ind. Technol. 2010, 26, 1–10. [Google Scholar]
- Aretxabaleta, M.; Xepapadeas, A.B.; Poets, C.F.; Koos, B.; Spintzyk, S. Comparison of additive and subtractive CAD/CAM materials for their potential use as Tübingen Palatal Plate: An in-vitro study on flexural strength. Addit. Manuf. 2021, 37, 101693. [Google Scholar] [CrossRef]
- Choi, J.-W.; Ahn, J.-J.; Son, K.; Huh, J.-B. Three-Dimensional Evaluation on Accuracy of Conventional and Milled Gypsum Models and 3D Printed Photopolymer Models. Materials 2019, 12, 3499. [Google Scholar] [CrossRef] [Green Version]
- Rubayo, D.D.; Phasuk, K.; Vickery, J.M.; Morton, D.; Lin, W.-S. Influences of build angle on the accuracy, printing time, and material consumption of additively manufactured surgical templates. J. Prosthet. Dent. 2020. [Google Scholar] [CrossRef] [PubMed]
- Dalal, N.; Ammoun, R.; Abdulmajeed, A.A.; Deeb, G.R.; Bencharit, S. Intaglio Surface Dimension and Guide Tube Deviations of Implant Surgical Guides Influenced by Printing Layer Thickness and Angulation Setting. J. Prosthodont. 2020, 29, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Hada, T.; Kanazawa, M.; Iwaki, M.; Arakida, T.; Soeda, Y.; Katheng, A.; Otake, R.; Minakuchi, S. Effect of Printing Direction on the Accuracy of 3D-Printed Dentures Using Stereolithography Technology. Materials 2020, 13, 3405. [Google Scholar] [CrossRef] [PubMed]
- You, S.-G.; Kang, S.-Y.; Bae, S.-Y.; Kim, J.-H. Evaluation of the adaptation of complete denture metal bases fabricated with dental CAD-CAM systems: An in vitro study. J. Prosthet. Dent. 2020. [Google Scholar] [CrossRef]
- You, S.-M.; Kang, S.-Y.; Bae, S.-Y.; Kim, J.-H. Evaluation of the accuracy (trueness and precision) of a maxillary trial denture according to the layer thickness: An in vitro study. J. Prosthet. Dent. 2021, 125, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Patzelt, S.B.; Bishti, S.; Stampf, S.; Att, W. Accuracy of computer-aided design/computer-aided manufacturing–generated dental casts based on intraoral scanner data. J. Am. Dent. Assoc. 2014, 145, 1133–1140. [Google Scholar] [CrossRef]
- Choi, S.; Chan, A. A virtual prototyping system for rapid product development. Comput. Des. 2004, 36, 401–412. [Google Scholar] [CrossRef]
- Formlabs. SLA vs. DLP: Guide to Resin 3D Printers. Available online: https://formlabs.com/blog/resin-3d-printer-comparison-sla-vs-dlp/ (accessed on 24 January 2021).
- Xu, Y.; Xepapadeas, A.B.; Koos, B.; Geis-Gerstorfer, J.; Li, P.; Spintzyk, S. Effect of post-rinsing time on the mechanical strength and cytotoxicity of a 3D printed orthodontic splint material. Dent. Mater. 2021. [Google Scholar] [CrossRef] [PubMed]
- Reymus, M.; Stawarczyk, B. Influence of Different Postpolymerization Strategies and Artificial Aging on Hardness of 3D-Printed Resin Materials: An In Vitro Study. Int. J. Prosthodont. 2020, 33, 634–640. [Google Scholar] [CrossRef]
- Reymus, M.; Lümkemann, N.; Stawarczyk, B. 3D-printed material for temporary restorations: Impact of print layer thickness and post-curing method on degree of conversion. Int. J. Comput. Dent. 2019, 22, 231–237. [Google Scholar] [PubMed]
- You, S.-M.; Lee, B.-I.; Kim, J.-H. Evaluation of trueness in a denture base fabricated by using CAD-CAM systems and adaptation to the socketed surface of denture base: An in vitro study. J. Prosthet. Dent. 2020. [Google Scholar] [CrossRef]
- Kulkarni, P.; Marsan, A.; Dutta, D. A review of process planning techniques in layered manufacturing. Rapid Prototyp. J. 2000, 6, 18–35. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SLA (Stereolithography) | DLP (Direct Light Processing) | ||||||
|---|---|---|---|---|---|---|---|
| 0° | 45° | 90° | 0° | 45° | 90° | ||
| Trueness (RMS) | Mean | 0.094 | 0.132 | 0.083 | 0.256 | 0.211 | 0.163 |
| SD | 0.004 | 0.016 | 0.009 | 0.031 | 0.031 | 0.030 | |
| Precision (RMS) | Mean | 0.087 | 0.094 | 0.098 | 0.134 | 0.048 | 0.044 |
| SD | 0.042 | 0.034 | 0.037 | 0.028 | 0.023 | 0.023 | |
| Average + (mm) | Mean | 0.082 | 0.099 | 0.055 | 0.166 | 0.101 | 0.066 |
| SD | 0.011 | 0.015 | 0.009 | 0.027 | 0.010 | 0.010 | |
| Average − (mm) | Mean | −0.054 | −0.089 | −0.045 | −0.187 | −0.097 | −0.065 |
| SD | 0.006 | 0.018 | 0.010 | 0.024 | 0.008 | 0.006 | |
| Max + (mm) | Mean | 0.613 | 0.630 | 0.533 | 0.547 | 0.573 | 0.500 |
| SD | 0.136 | 0.119 | 0.030 | 0.169 | 0.163 | 0.071 | |
| Max − (mm) | Mean | −0.168 | −0.294 | −0.132 | −0.366 | −0.402 | −0.416 |
| SD | 0.005 | 0.143 | 0.020 | 0.058 | 0.027 | 0.048 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Unkovskiy, A.; Schmidt, F.; Beuer, F.; Li, P.; Spintzyk, S.; Kraemer Fernandez, P. Stereolithography vs. Direct Light Processing for Rapid Manufacturing of Complete Denture Bases: An In Vitro Accuracy Analysis. J. Clin. Med. 2021, 10, 1070. https://doi.org/10.3390/jcm10051070
Unkovskiy A, Schmidt F, Beuer F, Li P, Spintzyk S, Kraemer Fernandez P. Stereolithography vs. Direct Light Processing for Rapid Manufacturing of Complete Denture Bases: An In Vitro Accuracy Analysis. Journal of Clinical Medicine. 2021; 10(5):1070. https://doi.org/10.3390/jcm10051070
Chicago/Turabian StyleUnkovskiy, Alexey, Franziska Schmidt, Florian Beuer, Ping Li, Sebastian Spintzyk, and Pablo Kraemer Fernandez. 2021. "Stereolithography vs. Direct Light Processing for Rapid Manufacturing of Complete Denture Bases: An In Vitro Accuracy Analysis" Journal of Clinical Medicine 10, no. 5: 1070. https://doi.org/10.3390/jcm10051070