
Nailfold Capillaroscopy in Systemic Sclerosis Patients with and without Pulmonary Arterial Hypertension: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection and Eligibility Criteria
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Statistical Analysis
3. Results
3.1. Search Results, Study Characteristics and Quality Assessment
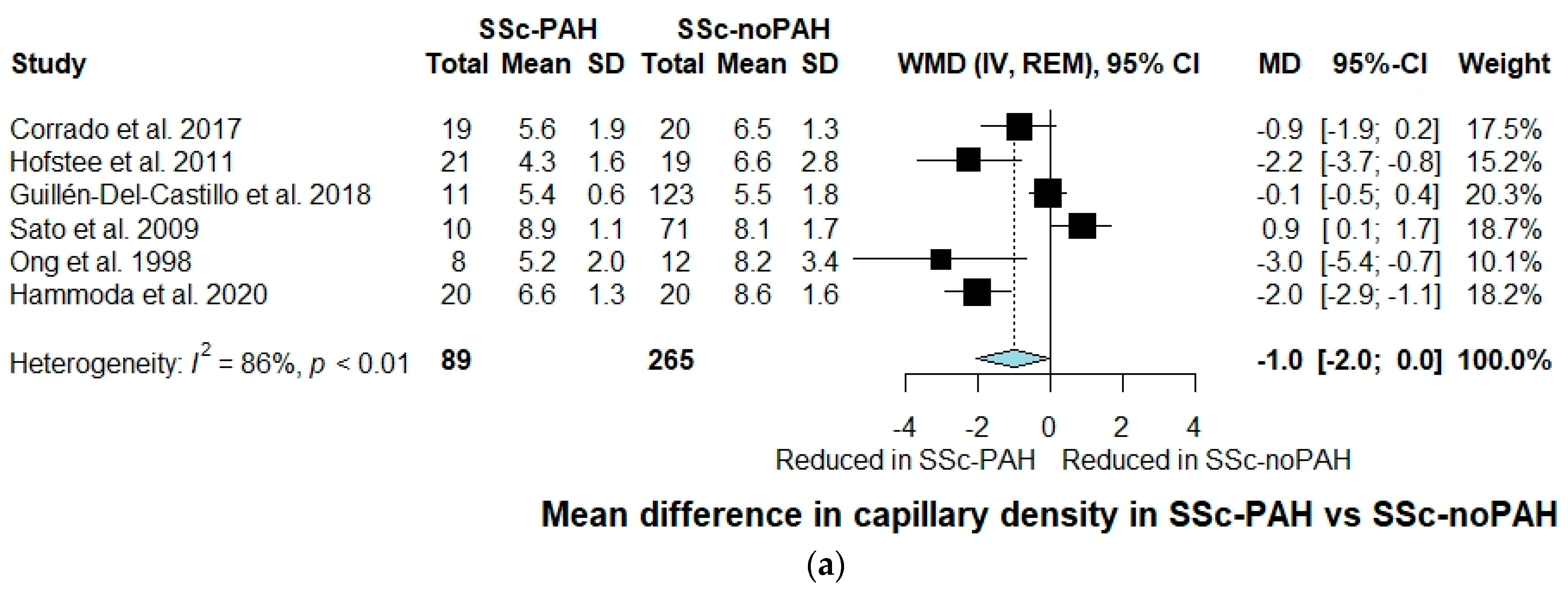
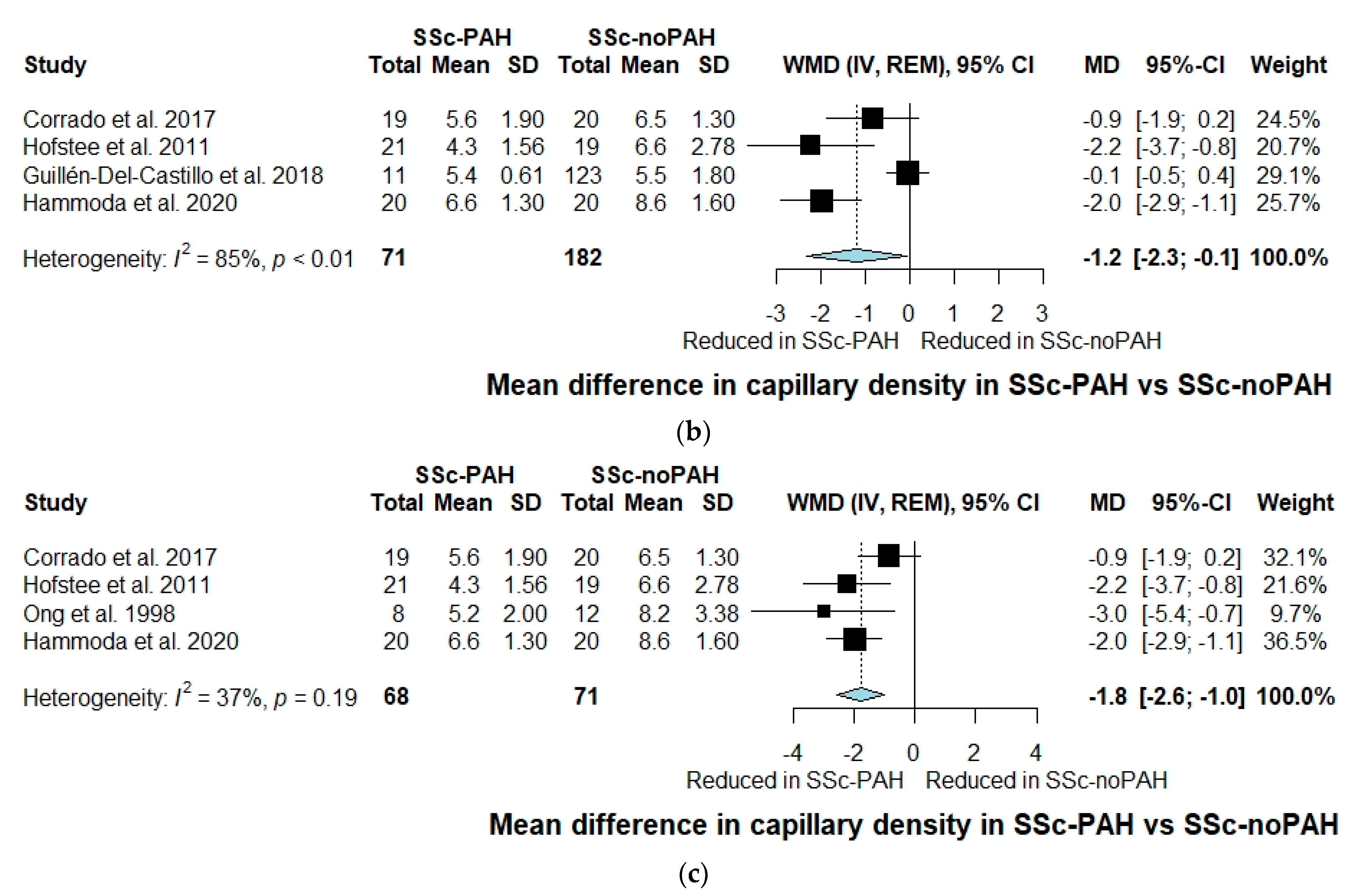
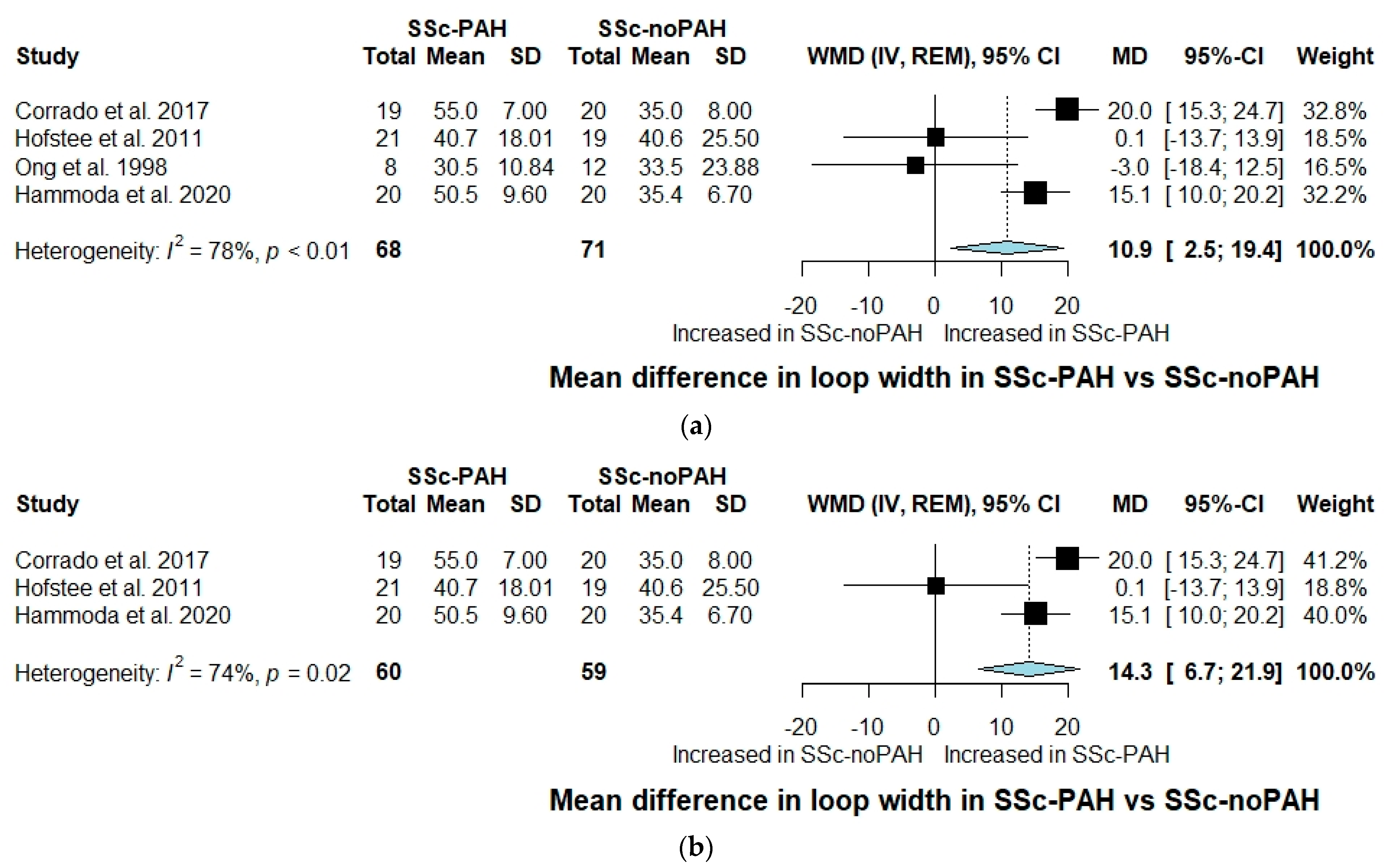
3.2. Quantitative Assessment
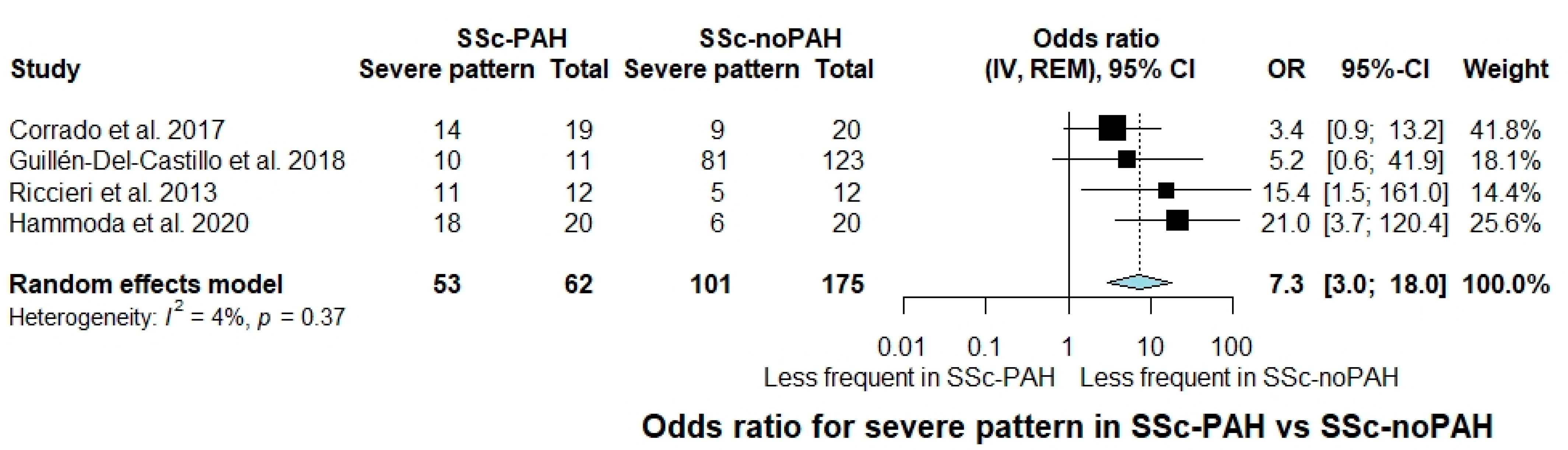
3.3. Semi-Quantitative and Qualitative Assessment
4. Discussion
4.1. Strengths and Limitations
4.2. Future Perspectives and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- LeRoy, E.C. Systemic Sclerosis. A Vascular Perspective. Rheum. Dis. Clin. N. Am. 1996, 22, 675–694. [Google Scholar] [CrossRef]
- Elhai, M.; Meune, C.; Avouac, J.; Kahan, A.; Allanore, Y. Trends in Mortality in Patients with Systemic Sclerosis over 40 Years: A Systematic Review and Meta-Analysis of Cohort Studies. Rheumatology 2012, 51, 1017–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nihtyanova, S.I.; Tang, E.C.; Coghlan, J.G.; Wells, A.U.; Black, C.M.; Denton, C.P. Improved Survival in Systemic Sclerosis Is Associated with Better Ascertainment of Internal Organ Disease: A Retrospective Cohort Study. QJM Int. J. Med. 2010, 103, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Tyndall, A.J.; Bannert, B.; Vonk, M.; Airò, P.; Cozzi, F.; Carreira, P.E.; Bancel, D.F.; Allanore, Y.; Müller-Ladner, U.; Distler, O.; et al. Causes and Risk Factors for Death in Systemic Sclerosis: A Study from the EULAR Scleroderma Trials and Research (EUSTAR) Database. Ann. Rheum. Dis. 2010, 69, 1809–1815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukerjee, D.; St, G.; Coleiro, B.; Knight, C.; Denton, C.; Davar, J.; Black, C.; Coghlan, J. Prevalence and Outcome in Systemic Sclerosis Associated Pulmonary Arterial Hypertension: Application of a Registry Approach. Ann. Rheum. Dis. 2003, 62, 1088–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phung, S.; Strange, G.; Chung, L.P.; Leong, J.; Dalton, B.; Roddy, J.; Deague, J.; Playford, D.; Musk, M.; Gabbay, E. Prevalence of Pulmonary Arterial Hypertension in an Australian Scleroderma Population: Screening Allows for Earlier Diagnosis. Intern. Med. J. 2009, 39, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Weatherald, J.; Montani, D.; Jevnikar, M.; Jaïs, X.; Savale, L.; Humbert, M. Screening for Pulmonary Arterial Hypertension in Systemic Sclerosis. Eur. Respir. Rev. 2019, 28, 190023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demerouti, E.; Tsangaris, I.; Dimitroulas, T.; Giannakoulas, G.; Katsimpri, P.; Mitrouska, I.; Orfanos, S.; Skoularigkis, I.; Voulgari, P.; Sfikakis, P. Pulmonary Arterial Hypertension in Connective Tissue Disorders: The Emerging Role of Screening and Early Diagnosis. A Position Paper for Greek Rheumatologists. Mediterr. J. Rheumatol. 2019, 30, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Humbert, M.; Yaici, A.; de Groote, P.; Montani, D.; Sitbon, O.; Launay, D.; Gressin, V.; Guillevin, L.; Clerson, P.; Simonneau, G.; et al. Screening for Pulmonary Arterial Hypertension in Patients with Systemic Sclerosis: Clinical Characteristics at Diagnosis and Long-Term Survival. Arthritis Rheum. 2011, 63, 3522–3530. [Google Scholar] [CrossRef]
- Lambova, S.N.; Muller-Ladner, U. Nailfold Capillaroscopy Within and Beyond the Scope of Connective Tissue Diseases. Curr. Rheumatol. Rev. 2018, 14, 12–21. [Google Scholar] [CrossRef] [PubMed]
- van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.; Riemekasten, G.; Carreira, P.; et al. Classification Criteria for Systemic Sclerosis: An ACR-EULAR Collaborative Initiative. Arthritis Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasile, M.; Avouac, J.; Sciarra, I.; Stefanantoni, K.; Iannace, N.; Cravotto, E.; Valesini, G.; Allanore, Y.; Riccieri, V. From VEDOSS to Established Systemic Sclerosis Diagnosis According to ACR/EULAR 2013 Classification Criteria: A French-Italian Capillaroscopic Survey. Clin. Exp. Rheumatol. 2018, 36, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Ingegnoli, F.; Ardoino, I.; Boracchi, P.; Cutolo, M.; Airò, P.; Ananieva, L.P.; Ancuta, C.; Andrade, L.E.; Becvar, R.; Benenati, A.; et al. Nailfold Capillaroscopy in Systemic Sclerosis: Data from the EULAR Scleroderma Trials and Research (EUSTAR) Database. Microvasc. Res. 2013, 89, 122–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caramaschi, P.; Canestrini, S.; Martinelli, N.; Volpe, A.; Pieropan, S.; Ferrari, M.; Bambara, L.M.; Carletto, A.; Biasi, D. Scleroderma Patients Nailfold Videocapillaroscopic Patterns Are Associated with Disease Subset and Disease Severity. Rheumatology 2007, 46, 1566–1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanatta, E.; Famoso, G.; Boscain, F.; Montisci, R.; Pigatto, E.; Polito, P.; Schiavon, F.; Iliceto, S.; Cozzi, F.; Doria, A.; et al. Nailfold Avascular Score and Coronary Microvascular Dysfunction in Systemic Sclerosis: A Newsworthy Association. Autoimmun. Rev. 2019, 18, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Emrani, Z.; Karbalaie, A.; Fatemi, A.; Etehadtavakol, M.; Erlandsson, B.-E. Capillary Density: An Important Parameter in Nailfold Capillaroscopy. Microvasc. Res. 2017, 109, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Soulaidopoulos, S.; Triantafyllidou, E.; Garyfallos, A.; Kitas, G.D.; Dimitroulas, T. The Role of Nailfold Capillaroscopy in the Assessment of Internal Organ Involvement in Systemic Sclerosis: A Critical Review. Autoimmun. Rev. 2017, 16, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z.; Wang, G.; Xiao, H.; Guo, S.; Liu, Y.; Meng, F.; Liu, D.; Li, G.; Zong, L. Diagnostic Value of Nailfold Videocapillaroscopy in Systemic Sclerosis Secondary Pulmonary Arterial Hypertension: A Meta-Analysis. Intern. Med. J. 2018, 48, 1355–1359. [Google Scholar] [CrossRef] [PubMed]
- Smith, V.; Vanhaecke, A.; Vandecasteele, E.; Guerra, M.; Paolino, S.; Melsens, K.; Cutolo, M. Nailfold Videocapillaroscopy in Systemic Sclerosis-Related Pulmonary Arterial Hypertension: A Systematic Literature Review. J. Rheumatol. 2020, 47, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galiè, N.; Humbert, M.; Vachiery, J.-L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Noordegraaf, A.V.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS)Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [CrossRef] [PubMed]
- Smith, V.; Herrick, A.L.; Ingegnoli, F.; Damjanov, N.; de Angelis, R.; Denton, C.P.; Distler, O.; Espejo, K.; Foeldvari, I.; Frech, T.; et al. Standardisation of Nailfold Capillaroscopy for the Assessment of Patients with Raynaud’s Phenomenon and Systemic Sclerosis. Autoimmun. Rev. 2020, 19, 102458. [Google Scholar] [CrossRef] [PubMed]
- Smith, V.; Pizzorni, C.; de Keyser, F.; Decuman, S.; van Praet, J.T.; Deschepper, E.; Sulli, A.; Cutolo, M. Reliability of the Qualitative and Semiquantitative Nailfold Videocapillaroscopy Assessment in a Systemic Sclerosis Cohort: A Two-Centre Study. Ann. Rheum. Dis. 2010, 69, 1092–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, P.; Leung, F.Y.; Alderdice, C.; Armstrong, S.K. Nailfold Capillary Microscopy in the Connective Tissue Diseases: A Semiquantitative Assessment. J. Rheumatol. 1983, 10, 930–938. [Google Scholar] [PubMed]
- Riccieri, V.; Vasile, M.; Iannace, N.; Stefanantoni, K.; Sciarra, I.; Vizza, C.D.; Badagliacca, R.; Poscia, R.; Papa, S.; Mezzapesa, M.; et al. Systemic Sclerosis Patients with and without Pulmonary Arterial Hypertension: A Nailfold Capillaroscopy Study. Rheumatology 2013, 52, 1525–1528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maricq, H.R.; Harper, F.E.; Khan, M.M.; Tan, E.M.; LeRoy, E.C. Microvascular Abnormalities as Possible Predictors of Disease Subsets in Raynaud Phenomenon and Early Connective Tissue Disease. Clin. Exp. Rheumatol. 1983, 1, 195–205. [Google Scholar] [PubMed]
- Cutolo, M.; Sulli, A.; Pizzorni, C.; Accardo, S. Nailfold Videocapillaroscopy Assessment of Microvascular Damage in Systemic Sclerosis. J. Rheumatol. 2000, 27, 155–160. [Google Scholar]
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G.; Settings, E.W.G.; ESH Working Group on CV Risk in Low Resource Settings. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for Examining and Interpreting Funnel Plot Asymmetry in Meta-Analyses of Randomised Controlled Trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ioannidis, J.P.A.; Trikalinos, T.A. The Appropriateness of Asymmetry Tests for Publication Bias in Meta-Analyses: A Large Survey. Can. Med. Assoc. J. 2007, 176, 1091–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meier, F.; Geyer, M.; Tiede, H.; Rieth, A.; Ghofrani, H.A.; Müller-Ladner, U.; Dinser, R.; Hermann, W. Is Nailfold Videocapillaroscopy a Valuable Diagnostic Tool in Pulmonary Hypertension? [Abstract]. Eur. Respir. J. 2012, 40, 972. [Google Scholar]
- Bredemeier, M.; Xavier, R.M.; Capobianco, K.G.; Restelli, V.G.; Rohde, L.E.P.; Pinotti, A.F.F.; Pitrez, E.H.; Vieira, M.V.; Fontoura, M.A.; Ludwig, D.H.D.C.; et al. Nailfold Capillary Microscopy Can Suggest Pulmonary Disease Activity in Systemic Sclerosis. J. Rheumatol. 2004, 31, 286–294. [Google Scholar] [PubMed]
- Greidinger, E.L.; Gaine, S.P.; Wise, R.A.; Boling, C.; Housten-Harris, T.; Wigley, F.M. Primary Pulmonary Hypertension Is Not Associated with Scleroderma-Like Changes in Nailfold Capillaries. Chest 2001, 120, 796–800. [Google Scholar] [CrossRef] [PubMed]
- Hofstee, H.; Noordegraaf, A.V.; E Voskuyl, A.; Dijkmans, B.; Postmus, P.; Smulders, Y.; Serne, E. Nailfold Capillary Density Is Associated with the Presence and Severity of Pulmonary Arterial Hypertension in Systemic Sclerosis. Ann. Rheum. Dis. 2009, 68, 191–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrado, A.; Correale, M.; Mansueto, N.; Monaco, I.; Carriero, A.; Mele, A.; Colia, R.; Di Biase, M.; Cantatore, F.P. Nailfold Capillaroscopic Changes in Patients with Idiopathic Pulmonary Arterial Hypertension and Systemic Sclerosis-Related Pulmonary Arterial Hypertension. Microvasc. Res. 2017, 114, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Hammoda, R.M.; Ali, Y.A.; Samy, N. Value of Nailfold Capillaroscopy as A Screening Method for Pulmonary Arterial Hypertension in Patients with Systemic Sclerosis. Egypt. J. Hosp. Med. 2020, 80, 920–927. [Google Scholar] [CrossRef]
- Ong, Y.Y.; Nikoloutsopoulos, T.; Bond, C.P.; Smith, M.D.; Ahern, M.J.; Roberts-Thomson, P.J. Decreased Nailfold Capillary Density in Limited Scleroderma with Pulmonary Hypertension. Asian Pac. J. Allergy Immunol. 1998, 16, 81–86. [Google Scholar] [PubMed]
- Sato, L.T.; Kayser, C.; Andrade, L.E.C. Nailfold Capillaroscopy Abnormalities Correlate with Cutaneous and Visceral Involvement in Systemic Sclerosis Patients. Acta Reumatol. Port. 2009, 34, 219–227. [Google Scholar] [PubMed]
- Guillén-Del-Castillo, A.; Simeón-Aznar, C.P.; Callejas-Moraga, E.L.; Tolosa-Vilella, C.; Alonso-Vila, S.; Fonollosa-Pla, V.; Selva-O’Callaghan, A. Quantitative Videocapillaroscopy Correlates with Functional Respiratory Parameters: A Clue for Vasculopathy as a Pathogenic Mechanism for Lung Injury in Systemic Sclerosis. Arthritis Res. Ther. 2018, 20, 281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sulli, A.; Pizzorni, C.; Smith, V.; Zampogna, G.; Ravera, F.; Cutolo, M. Timing of Transition between Capillaroscopic Patterns in Systemic Sclerosis. Arthritis Rheum. 2012, 64, 821–825. [Google Scholar] [CrossRef] [PubMed]
- Avouac, J.; Lepri, G.; Smith, V.; Toniolo, E.; Hurabielle, C.; Vallet, A.; Amrouche, F.; Kahan, A.; Cutolo, M.; Allanore, Y. Sequential Nailfold Videocapillaroscopy Examinations Have Responsiveness to Detect Organ Progression in Systemic Sclerosis. Semin. Arthritis Rheum. 2017, 47, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Preliminary Criteria for the Classification of Systemic Sclerosis (Scleroderma). Subcommittee for Scleroderma Criteria of the American Rheumatism Association Diagnostic and Therapeutic Criteria Committee. Arthritis Rheum. 1980, 23, 581–590. [Google Scholar] [CrossRef]
- LeRoy, E.C.; Medsger, T.A. Criteria for the Classification of Early Systemic Sclerosis. J. Rheumatol. 2001, 28, 1573–1576. [Google Scholar] [PubMed]
- Allanore, Y.; Simms, R.; Distler, O.; Trojanowska, M.; Pope, J.; Denton, C.P.; Varga, J. Systemic Sclerosis. Nat. Rev. Dis. Prim. 2015, 1, 15002. [Google Scholar] [CrossRef] [PubMed]
- Sulli, A.; Paolino, S.; Pizzorni, C.; Ferrari, G.; Pacini, G.; Pesce, G.; Carmisciano, L.; Smith, V.; Cutolo, M. Progression of Nailfold Capillaroscopic Patterns and Correlation with Organ Involvement in Systemic Sclerosis: A 12 Year Study. Rheumatology 2020, 59, 1051–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arvanitaki, A.; Giannakoulas, G.; Triantafyllidou, E.; Feloukidis, C.; Boutou, A.K.; Garyfallos, A.; Karvounis, H.; Dimitroulas, T. Peripheral Microangiopathy in Precapillary Pulmonary Hypertension: A Nailfold Video Capillaroscopy Prospective Study. Respir. Res. 2021, 22, 27. [Google Scholar] [CrossRef] [PubMed]
- Arvanitaki, A.; Giannakoulas, G.; Triantafyllidou, E.; Karvounis, H.; Garyfallos, A.; Kitas, G.; Dimitroulas, T. Nailfold Videocapillaroscopy: A Novel Possible Surrogate Marker for the Evaluation of Peripheral Microangiopathy in Pulmonary Arterial Hypertension. Scand. J. Rheumatol. 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Donnarumma, J.F.S.; Ferreira, E.V.M.; Ota-Arakaki, J.; Kayser, C. Nailfold Capillaroscopy as a Risk Factor for Pulmonary Arterial Hypertension in Systemic Lupus Erythematosus Patients. Adv. Rheumatol. 2019, 59, 1. [Google Scholar] [CrossRef] [PubMed]
- Arvanitaki, A.; Giannakoulas, G.; Triantafyllidou, E.; Feloukidis, C.; Boutou, A.; Garyfallos, A.; Karvounis, H.; Diller, G.-P.; Gatzoulis, M.A.; Dimitroulas, T. Peripheral Microangiopathy in Eisenmenger Syndrome: A Nailfold Video Capillaroscopy Study. Int. J. Cardiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hoeper, M.M.; Kramer, T.; Pan, Z.; Eichstaedt, C.A.; Spiesshoefer, J.; Benjamin, N.; Olsson, K.M.; Meyer, K.; Vizza, C.D.; Vonk-Noordegraaf, A.; et al. Mortality in Pulmonary Arterial Hypertension: Prediction by the 2015 European Pulmonary Hypertension Guidelines Risk Stratification Model. Eur. Respir. J. 2017, 50, 1700740. [Google Scholar] [CrossRef] [Green Version]
- Weatherald, J.; Boucly, A.; Launay, D.; Cottin, V.; Prévot, G.; Bourlier, D.; Dauphin, C.; Chaouat, A.; Savale, L.; Jaïs, X.; et al. Haemodynamics and Serial Risk Assessment in Systemic Sclerosis Associated Pulmonary Arterial Hypertension. Eur. Respir. J. 2018, 52, 1800678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rich, S.; Dantzker, D.R.; Ayres, S.M.; Bergofsky, E.H.; Brundage, B.H.; Detre, K.M.; Fishman, A.P.; Goldring, R.M.; Groves, B.M.; Koerner, S.K. Primary Pulmonary Hypertension. A National Prospective Study. Ann. Intern. Med. 1987, 107, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Coghlan, J.G.; Denton, C.P.; Grünig, E.; Bonderman, D.; Distler, O.; Khanna, D.; Müller-Ladner, U.; Pope, J.E.; Vonk, M.C.; Doelberg, M.; et al. Evidence-Based Detection of Pulmonary Arterial Hypertension in Systemic Sclerosis: The DETECT Study. Ann. Rheum. Dis. 2014, 73, 1340–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrisroe, K.; Stevens, W.; Sahhar, J.; Rabusa, C.; Nikpour, M.; Proudman, S.; Hill, C.; Lester, S.; Nash, P.; Ngian, G.; et al. Epidemiology and Disease Characteristics of Systemic Sclerosis-Related Pulmonary Arterial Hypertension: Results from a Real-Life Screening Programme. Arthritis Res. Ther. 2017, 19, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hao, Y.; Thakkar, V.; Stevens, W.; Morrisroe, K.; Prior, D.; Rabusa, C.; Youssef, P.; Gabbay, E.; Roddy, J.; Walker, J.; et al. A Comparison of the Predictive Accuracy of Three Screening Models for Pulmonary Arterial Hypertension in Systemic Sclerosis. Arthritis Res. Ther. 2015, 17, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillén-Del Castillo, A.; Callejas-Moraga, E.L.; García, G.; Rodríguez-Palomares, J.F.; Román, A.; Berastegui, C.; López-Meseguer, M.; Domingo, E.; Fonollosa-Plá, V.; Simeón-Aznar, C.P. High Sensitivity and Negative Predictive Value of the DETECT Algorithm for an Early Diagnosis of Pulmonary Arterial Hypertension in Systemic Sclerosis: Application in a Single Center. Arthritis Res. Ther. 2017, 19, 135. [Google Scholar] [CrossRef] [Green Version]
- Vandecasteele, E.; Drieghe, B.; Melsens, K.; Thevissen, K.; de Pauw, M.; Deschepper, E.; Decuman, S.; Bonroy, C.; Piette, Y.; de Keyser, F.; et al. Screening for Pulmonary Arterial Hypertension in an Unselected Prospective Systemic Sclerosis Cohort. Eur. Respir. J. 2017, 49, 1602275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauling, J.D.; McHugh, N.J. Evaluating Factors Influencing Screening for Pulmonary Hypertension in Systemic Sclerosis: Does Disparity between Available Guidelines Influence Clinical Practice? Clin. Rheumatol. 2012, 31, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, M.; Trombetta, A.C.; Melsens, K.; Pizzorni, C.; Sulli, A.; Ruaro, B.; Paolino, S.; Deschepper, E.; Smith, V. Automated Assessment of Absolute Nailfold Capillary Number on Videocapillaroscopic Images: Proof of Principle and Validation in Systemic Sclerosis. Microcirculation 2018, 25, e12447. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | SSc Criteria | Population | Mean Disease Duration (Years) | Method of PAH Diagnosis | Nailfold Capillaroscopy Method | Capillaroscopy Parameters | ||
|---|---|---|---|---|---|---|---|---|---|
| SSc- PAH | SSc-noPAH | SSc- PAH | SSc-noPAH | ||||||
| Corrado et al. 2017 [36] | Cross-sectional | ACR/EULAR 2013 diagnostic criteria for SSc [11] | 19 | 20 | 15.3 ± 3.9 | 18.4 ± 4.1 | RHC | NVC, 200× magnification | Capillary density Capillary dimensions Neoangiogenesis Pattern |
| Hofstee et al. 2009 [35] | Cross-sectional | preliminary criteria for the classification of SSc 1980 [43] | 21 | 19 | 3.7 ± 12.3 | 3.7 ± 9.8 | RHC | computer-based panorama mosaic NVC | Capillary density Capillary dimensions |
| Guillén-Del-Castillo et al. 2018 [40] | Cross-sectional | ACR/EULAR 2013 diagnostic criteria for SSc [11] | 11 | 123 | N/A | RHC | NVC, 200× magnification | Capillary density Capillary dimensions Microhemorrhages Neoangiogenesis Pattern | |
| Sato et al. 2009 [39] | Cross-sectional | preliminary criteria for the classification of SSc 1980 [43] | 10 | 71 | N/A | TTE | microscopy 10–20× magnification | Capillary density Capillary dimensions VDS | |
| Ong et al. 1998 [38] | Cross-sectional | Not defined | 8 | 12 | 22.9 ± 16.6 | 18.1 ± 10.2 | TTE and/or RHC | microscopy 60× magnification | Capillary density Capillary dimensions |
| Riccieri et al. 2013 [25] | Cross-sectional | preliminary criteria for the classification of SSc 1980 [43] | 12 | 12 | 24.4 ± 17.6 | 18.9 ± 10.7 | RHC | NVC, 200× magnification | Pattern VDS NFC |
| Hammoda et al. 2020 [37] | Cross-sectional | ACR/EULAR 2013 diagnostic criteria for SSc [11] | 20 | 20 | 21.4 ± 10.4 | 9.3 ± 6.5 | RHC | NVC, 200× magnification | Capillary density Capillary dimensions VDS Microhemorrhages Pattern NFC |
| Meier et al. 2012 [32] | Cross-sectional | Not defined | 10 | 37 | N/A | Not defined | NVC | Capillary density Capillary dimensions | |
| Bredemeier et al. 2004 [33] | Cross-sectional | preliminary criteria for the classification of SSc 1980 [43] | 11 | 75 | N/A | TTE | microscopy 6.5–65× magnification | Capillary dimensions VDS Microhemorrhages | |
| Greidinger et al. 2001 [34] | Cross-sectional | Not defined | 8 | 7 | N/A | TTE and/or RHC | microscopy | Capillary density Neoangiogenesis | |
| Avouac et al. 2017 [42] | Longitudinal | ACR/EULAR 2013 diagnostic criteria for SSc [11] | 8 | 132 | 9 ± 8 | 9 ± 8 | RHC | NVC, 200× magnification | Capillary density Capillary dimensions Microhemorrhages Neoangiogenesis |
| Sulli et al. 2012 [41] | Longitudinal | preliminary criteria for the classification of SSc 1980 [43] or LeRoy criteria for the classification of early SSc [44] | 4 | 34 | N/A | RHC | NVC, 200× magnification | Capillary dimensions Microhemorrhages Capillary ramifications Pattern NFC | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minopoulou, I.; Theodorakopoulou, M.; Boutou, A.; Arvanitaki, A.; Pitsiou, G.; Doumas, M.; Sarafidis, P.; Dimitroulas, T. Nailfold Capillaroscopy in Systemic Sclerosis Patients with and without Pulmonary Arterial Hypertension: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 1528. https://doi.org/10.3390/jcm10071528
Minopoulou I, Theodorakopoulou M, Boutou A, Arvanitaki A, Pitsiou G, Doumas M, Sarafidis P, Dimitroulas T. Nailfold Capillaroscopy in Systemic Sclerosis Patients with and without Pulmonary Arterial Hypertension: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(7):1528. https://doi.org/10.3390/jcm10071528
Chicago/Turabian StyleMinopoulou, Ioanna, Marieta Theodorakopoulou, Afroditi Boutou, Alexandra Arvanitaki, Georgia Pitsiou, Michael Doumas, Pantelis Sarafidis, and Theodoros Dimitroulas. 2021. "Nailfold Capillaroscopy in Systemic Sclerosis Patients with and without Pulmonary Arterial Hypertension: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 7: 1528. https://doi.org/10.3390/jcm10071528