
Autologous Micro-Fragmented Adipose Tissue (MFAT) to Treat Symptomatic Knee Osteoarthritis: Early Outcomes of a Consecutive Case Series

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Lipo-Aspiration and MFAT Processing
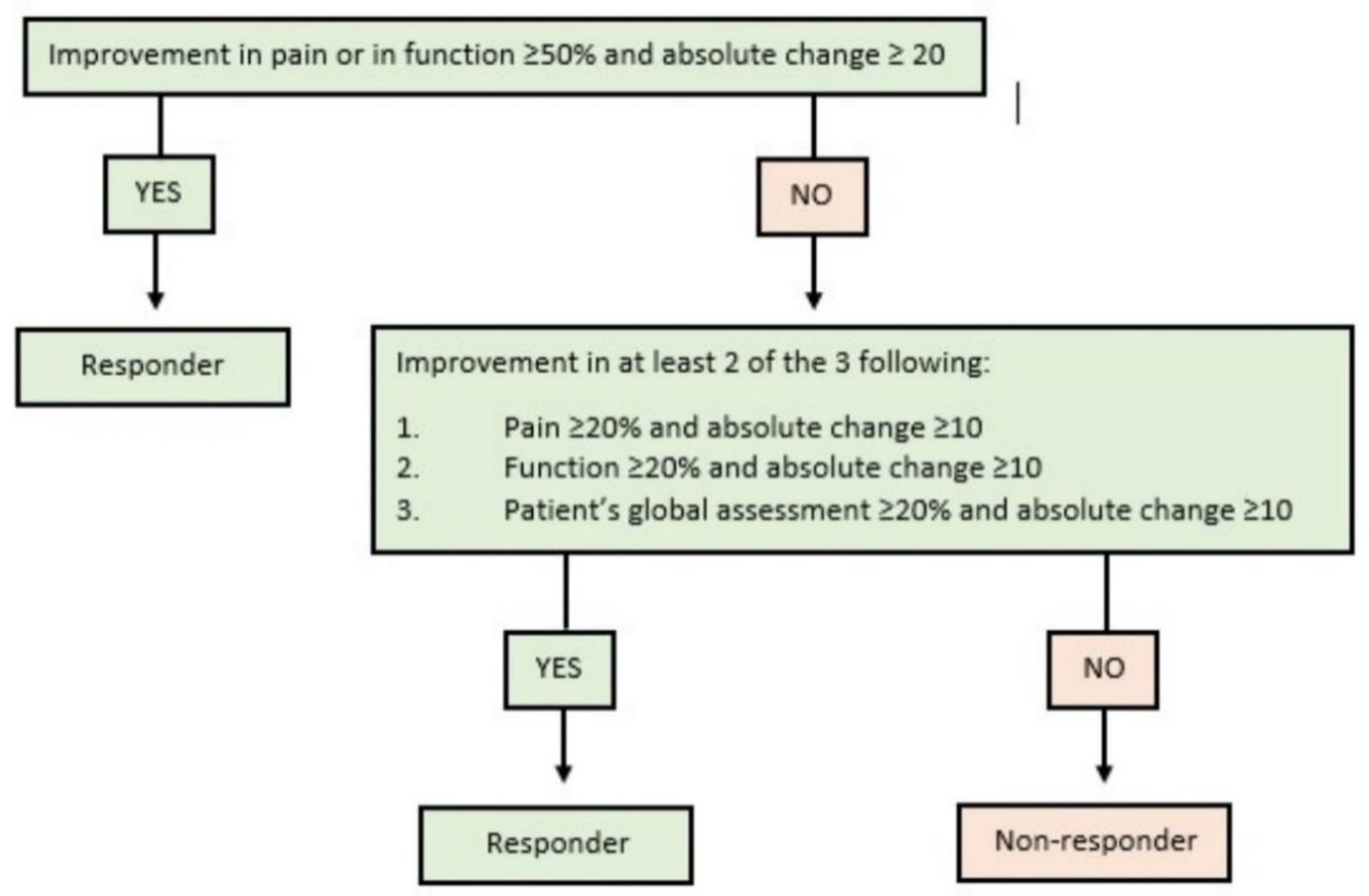
2.2. Clinical and Safety Assessment
2.3. Imaging
2.4. Statistics
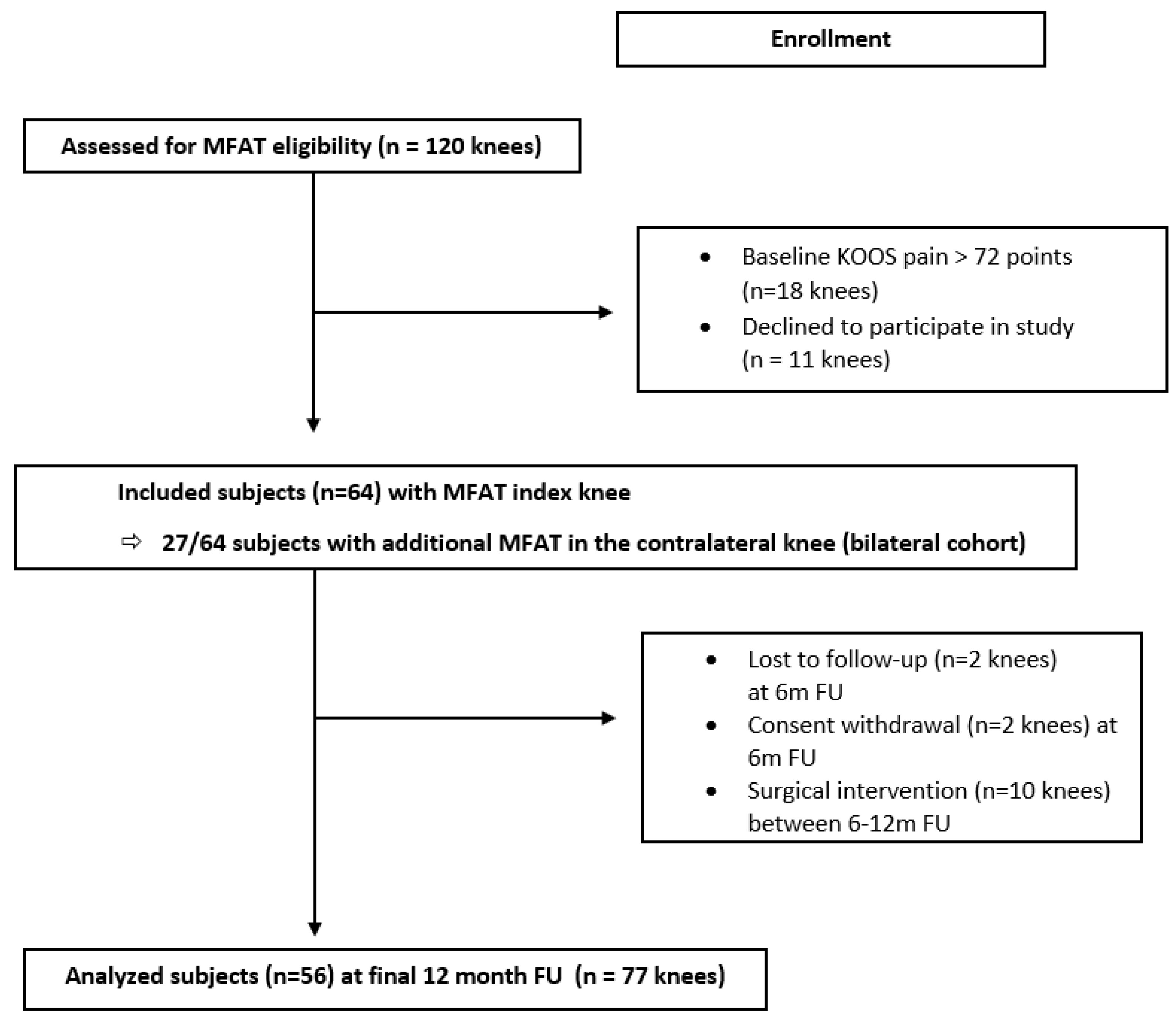
3. Results
3.1. Safety
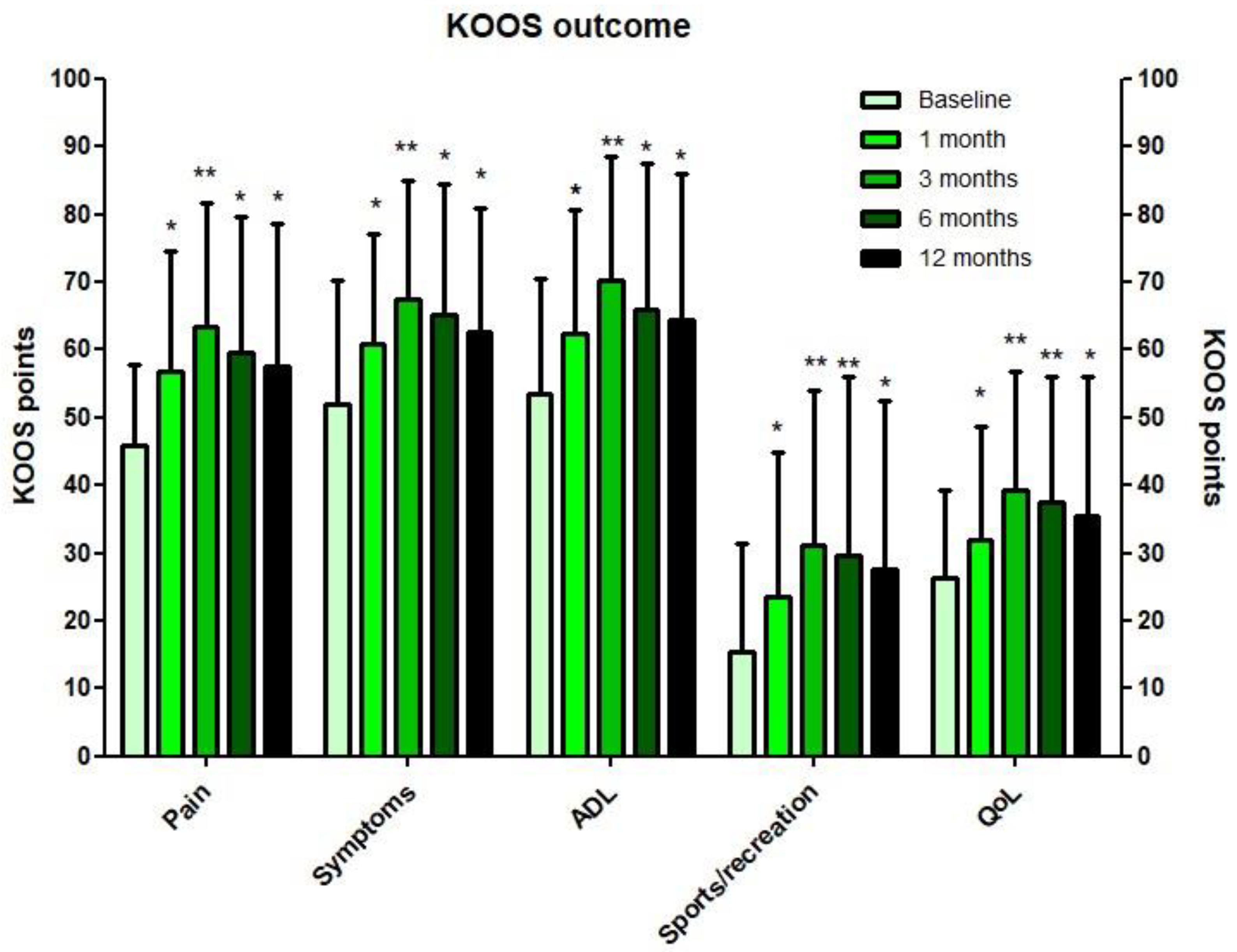
3.2. Clinical Outcomes Index Knee
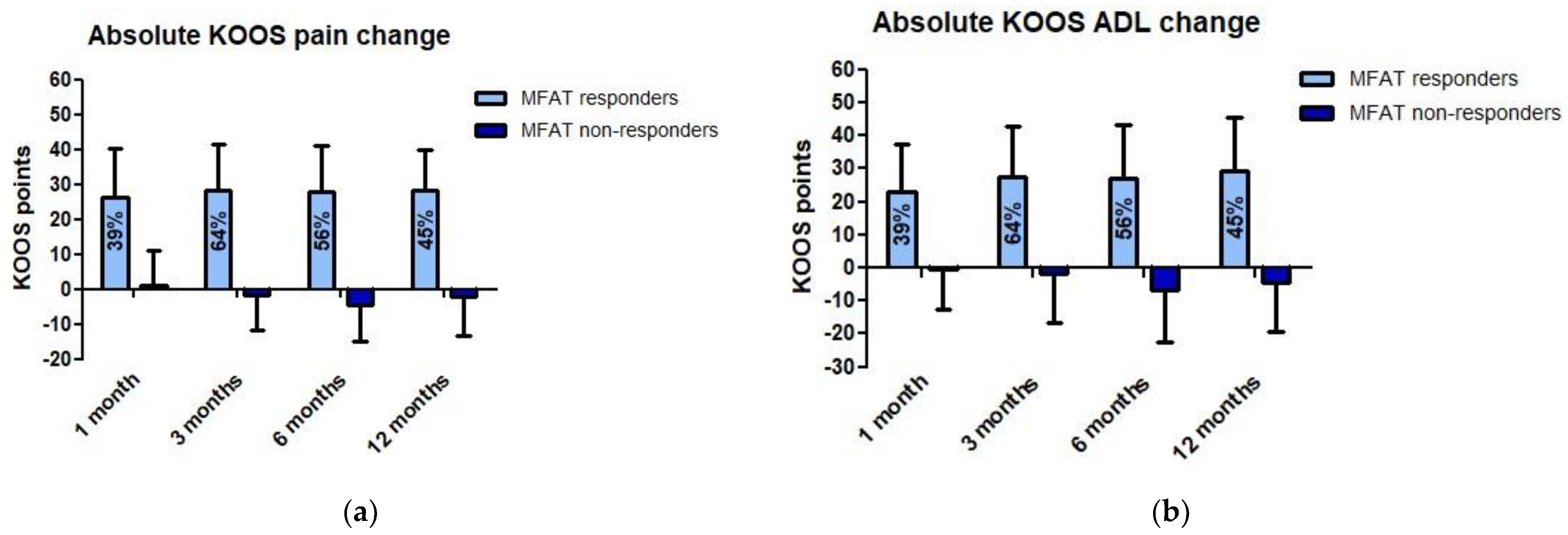
3.3. Subgroup Analysis
3.3.1. Bilateral Cohort
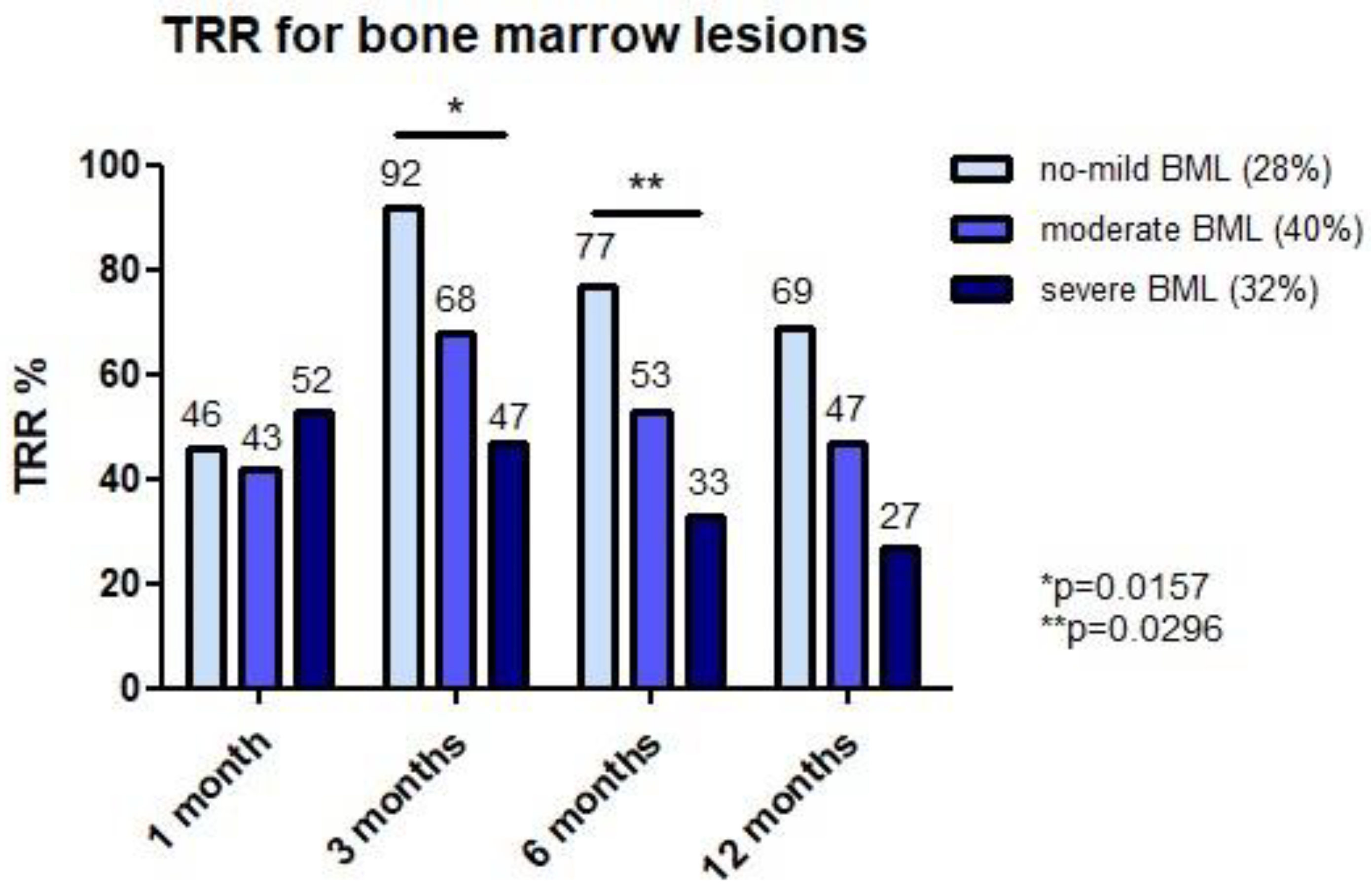
3.3.2. Subject- and Pathology-Specific Factors and Clinical Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, Y.; Jordan, J.M. Epidemiology of Osteoarthritis. Clin. Geriatr. Med. 2011, 26, 355–369. [Google Scholar] [CrossRef] [Green Version]
- Levy, D.M.; Petersen, K.A.; Vaught, M.S.; Christian, D.R.; Cole, B.J. Injections for Knee Osteoarthritis: Corticosteroids, Viscosupplementation, Platelet-Rich Plasma, and Autologous Stem Cells. Arthrosc. J. Arthrosc. Relat. Surg. 2018, 34, 1730–1743. [Google Scholar] [CrossRef]
- Deshpande, B.R.; Katz, J.N.; Solomon, D.H.; Yelin, E.H.; Hunter, D.J.; Messier, S.P.; Suter, L.G.; Losina, E. The number of persons with symptomatic knee osteoarthritis in the United States: Impact of race/ethnicity, age, sex, and obesity. Arthritis Care Res. 2016, 68, 1743–1750. [Google Scholar] [CrossRef]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, M. Prevalence of Childhood and Adult Obesity in the United States. JAMA 2016, 311, 806–814. [Google Scholar] [CrossRef] [Green Version]
- Evans, J.T.; Walker, R.W.; Evans, J.P.; Blom, A.W.; Sayers, A.; Whitehouse, M.R. How long does a knee replacement last? A systematic review and meta-analysis of case series and national registry reports with more than 15 years of follow-up. Lancet 2019, 393, 655–663. [Google Scholar] [CrossRef] [Green Version]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [Green Version]
- Tremolada, C.; Colombo, V.; Ventura, C. Adipose Tissue and Mesenchymal Stem Cells: State of the Art and Lipogems® Technology Development. Curr. Stem Cell Rep. 2016, 2, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Damia, E.; Chicharro, D.; Lopez, S.; Cuervo, B.; Rubio, M.; Sopena, J.J.; Vilar, J.M.; Carrillo, J.M. Adipose-derived mesenchymal stem cells: Are they a good therapeutic strategy for osteoarthritis? Int. J. Mol. Sci. 2018, 19, 1926. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, F.; Maioli, M.; Leonardi, E.; Olivi, E.; Pasquinelli, G.; Valente, S.; Mendez, A.J.; Ricordi, C.; Raffaini, M.; Tremolada, C.; et al. A new nonenzymatic method and device to obtain a fat tissue derivative highly enriched in pericyte-like elements by mild mechanical forces from human lipoaspirates. Cell Transplant. 2013, 22, 2063–2077. [Google Scholar] [CrossRef]
- Kakudo, N. Potential of Adipose-Derived Stem Cells for Regeneration Medicine: Clinical Application and Usefulness of Fat Grafting. J. Stem Cell Res. Ther. 2014, 4, 358–361. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Contreras, M.; Messaggio, F.; Jimenez, O.; Mendez, A. Differences in exosome content of human adipose tissue processed by non-enzymatic and enzymatic methods. CellR4 2015, 3, e1423. [Google Scholar]
- Ceserani, V.; Ferri, A.; Berenzi, A.; Benetti, A.; Ciusani, E.; Pascucci, L.; Bazzucchi, C.; Coccè, V.; Bonomi, A.; Pessina, A.; et al. Angiogenic and anti-inflammatory properties of micro-fragmented fat tissue and its derived mesenchymal stromal cells. Vasc. Cell 2016, 8, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Vezzani, B.; Shaw, I.; Lesme, H.; Yong, L.; Khan, N.; Tremolada, C.; Péault, B. Higher Pericyte Content and Secretory Activity of Microfragmented Human Adipose Tissue Compared to Enzymatically Derived Stromal Vascular Fraction. Stem Cells Transl. Med. 2018, 7, 876–886. [Google Scholar] [CrossRef] [Green Version]
- Cattaneo, G.; De Caro, A.; Napoli, F.; Chiapale, D.; Trada, P.; Camera, A. Micro-fragmented adipose tissue injection associated with arthroscopic procedures in patients with symptomatic knee osteoarthritis. BMC Musculoskelet. Disord. 2018, 19, 1–7. [Google Scholar] [CrossRef]
- Panni, A.S.; Vasso, M.; Braile, A.; Toro, G.; De Cicco, A.; Viggiano, D.; Lepore, F. Preliminary results of autologous adipose-derived stem cells in early knee osteoarthritis: Identification of a subpopulation with greater response. Int. Orthop. 2019, 43, 7–13. [Google Scholar] [CrossRef]
- Panchal, J.; Malanga, G.; Sheinkop, M. Safety and Efficacy of Percutaneous Injection of Lipogems Micro-Fractured Adipose Tissue for Osteoarthritic Knees. Am. J. Orthop. 2018, 47, 1–11. [Google Scholar] [CrossRef]
- Borić, I.; Hudetz, D.; Rod, E.; Jeleč, Ž.; Vrdoljak, T.; Skelin, A.; Polašek, O.; Plečko, M.; Trbojević-Akmačić, I.; Lauc, G.; et al. A 24-month follow-up study of the effect of intra-articular injection of autologous microfragmented fat tissue on proteoglycan synthesis in patients with knee osteoarthritis. Genes 2019, 10, 1051. [Google Scholar] [CrossRef] [Green Version]
- Barfod, K.W.; Blønd, L. Treatment of osteoarthritis with autologous and microfragmented adipose tissue. Dan Med. J. 2019, 66, 1–5. [Google Scholar]
- Franceschini, M.; Castellaneta, C.; Mineo, G. Injection of autologous micro-fragmented adipose tissue for the treatment of post-traumatic degenerative lesion of knee cartilage: A case report. CellR4 2016, 4, 1–6. [Google Scholar]
- Pham, T.; van der Heijde, D.M.F.M.; Altman, R.D.; Anderson, J.J.; Bellamy, N.; Hochberg, M.; Simon, L.; Strand, V.; Woodworth, T.; Dougados, M. OMERACT-OARSI initiative: Osteoarthritis research society international set of responder criteria for osteoarthritis clinical trials revisited. Osteoarthr. Cartil. 2004, 12, 389–399. [Google Scholar] [CrossRef] [Green Version]
- Hunter, D.J.; Guermazi, A.; Lo, G.H.; Grainger, A.J.; Conaghan, P.G.; Boudreau, R.M.; Roemer, F.W. Evolution of semi-quantitative whole joint assessment of knee OA: MOAKS (MRI Osteoarthritis Knee Score). Osteoarthr. Cartil. 2011, 19, 990–1002. [Google Scholar] [CrossRef] [Green Version]
- Rutjes, A.W.; Jüni, P.; da Costa, B.R.; Trelle, S.; Nüesch, E.; Reichenbach, S. Viscosupplementation for osteoarthritis of the knee: A systematic review and meta-analysis. Ann. Intern. Med. 2012, 157, 180–191. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Ruiz, M.T.P.; Vaccaro, F.; Guitaldi, R.; Di Martino, A.; Cenacchi, A.; Fornasari, P.M.; Marcacci, M. Platelet-rich plasma intra-articular injections for cartilage degeneration and osteoarthritis: Single- versus double-spinning approach. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 2082–2091. [Google Scholar] [CrossRef]
- Hudetz, D.; Borić, I.; Rod, E.; Jeleč, Ž.; Radić, A.; Vrdoljak, T.; Skelin, A.; Lauc, G.; Trbojević-Akmačić, I.; Plečko, M.; et al. The effect of intra-articular injection of autologous microfragmented fat tissue on proteoglycan synthesis in patients with knee osteoarthritis. Genes 2017, 8, 270. [Google Scholar] [CrossRef] [Green Version]
- Jo, C.H.; Lee, Y.G.; Shin, W.H.; Kim, H.; Chai, J.W.; Jeong, E.C.; Kim, J.E.; Shim, H.; Shin, J.S.; Shin, I.S.; et al. Intra-Articular Injection of Mesenchymal Stem Cells for the Treatment of Osteoarthritis of the Knee: A Proof-of-Concept Clinical Trial. Stem Cells Transl. Med. 2014, 32, 1254–1266. [Google Scholar] [CrossRef]
- Pers, Y.-M.M.; Rackwitz, L.; Ferreira, R. Adipose Mesenchymal Stromal Cell-Based Therapy for Severe Osteoarthritis of the Knee. Stem Cells Transl. Med. 2016, 5, 847–856. [Google Scholar]
- Comella, K.; Parlo, M.; Daly, R.; Depasquale, V.; Edgerton, E.; Mallory, P.; Schmidt, R.; Drake, W.P. Safety Analysis of Autologous Stem Cell Therapy in a Variety of Degenerative Diseases and Injuries Using the Stromal Vascular Fraction. J. Clin. Med. Res. 2017, 9, 935–942. [Google Scholar] [CrossRef] [Green Version]
- Kon, E.; Engebretsen, L.; Verdonk, P.; Nehrer, S.; Filardo, G. Clinical Outcomes of Knee Osteoarthritis Treated With an Autologous Protein Solution Injection: A 1-Year Pilot Double-Blinded Randomized Controlled Trial. Am. J. Sports Med. 2018, 46, 171–180. [Google Scholar] [CrossRef]
- Russo, A.; Condello, V.; Madonna, V.; Guerriero, M.; Zorzi, C. Autologous and micro-fragmented adipose tissue for the treatment of diffuse degenerative knee osteoarthritis. J. Exp. Orthop. 2017, 5, 1–7. [Google Scholar] [CrossRef]
- Guillibert, C.; Charpin, C.; Raffray, M.; Benmenni, A.; Dehaut, F.X.; El Ghobeira, G.; Giorgi, R.; Magalon, J.; Arniaud, D. Single injection of high volume of autologous pure PRP provides a significant improvement in knee osteoarthritis: A prospective routine care study. Int. J. Mol. Sci. 2019, 20, 1327. [Google Scholar] [CrossRef] [Green Version]
- Hame, S.L.; Alexander, R.A. Knee osteoarthritis in women. Curr. Rev. Musculoskelet. Med. 2013, 6, 182–187. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, T.W.; Felson, D.T. Mechanisms of Osteoarthritis (OA) Pain. Curr. Osteoporos. Rep. 2018, 16, 611–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spaková, T.; Rosocha, J.; Lacko, M.; Harvanová, D.; Gharaibeh, A. Treatment of knee joint osteoarthritis with autologous platelet-rich plasma in comparison with hyaluronic acid. Am. J. Phys. Med. Rehabil. 2012, 91, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Kon, E.; Mandelbaum, B.; Buda, R.; Filardo, G.; Delcogliano, M.; Timoncini, A.; Fornasari, P.M.; Giannini, S.; Marcacci, M. Platelet-rich plasma intra-articular injection versus hyaluronic acid viscosupplementation as treatments for cartilage pathology: From early degeneration to osteoarthritis. Arthrosc. J. Arthrosc. Relat. Surg. 2011, 27, 1490–1501. [Google Scholar] [CrossRef]
- Campbell, K.A.; Saltzman, B.M.; Mascarenhas, R.; Khair, M.M.; Verma, N.N.; Bach Jr, B.R.; Cole, B.J. Does Intra-articular Platelet-Rich Plasma Injection Provide Clinically Superior Outcomes Compared with Other Therapies in the Treatment of Knee Osteoarthritis? A Systematic Review of Overlapping Meta-analyses. Arthrosc. J. Arthrosc. Relat. Surg. 2015, 31, 2213–2221. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Buda, R.; Timoncini, A.; Di Martino, A.; Cenacchi, A.; Fornasari, P.M.; Giannini, S.; Marcacci, M. Platelet-rich plasma intra-articular knee injections for the treatment of degenerative cartilage lesions and osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Heidari, N.; Noorani, A.; Slevin, M.; Cullen, A.; Stark, L.; Olgiati, S.; Zerbi, A.; Wilson, A. Patient-Centered Outcomes of Microfragmented Adipose Tissue Treatments of Knee Osteoarthritis: An Observational, Intention-to-Treat Study at Twelve Months. Stem Cells Int. 2020, 2020. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Severity | Definition | Additional Medication Required? | Physicians Advice Required? |
|---|---|---|---|
| Mild | Minor discomfort noticed but does not interfere with normal daily activity | No | No |
| Moderate | Discomfort reducing or affecting normal daily activity | Yes | Potentially |
| Severe | Incapacitating with inability to work or perform normal daily activity | Yes | Yes |
| Serious | Permanent damage, life-threatening or death | Yes | Yes |
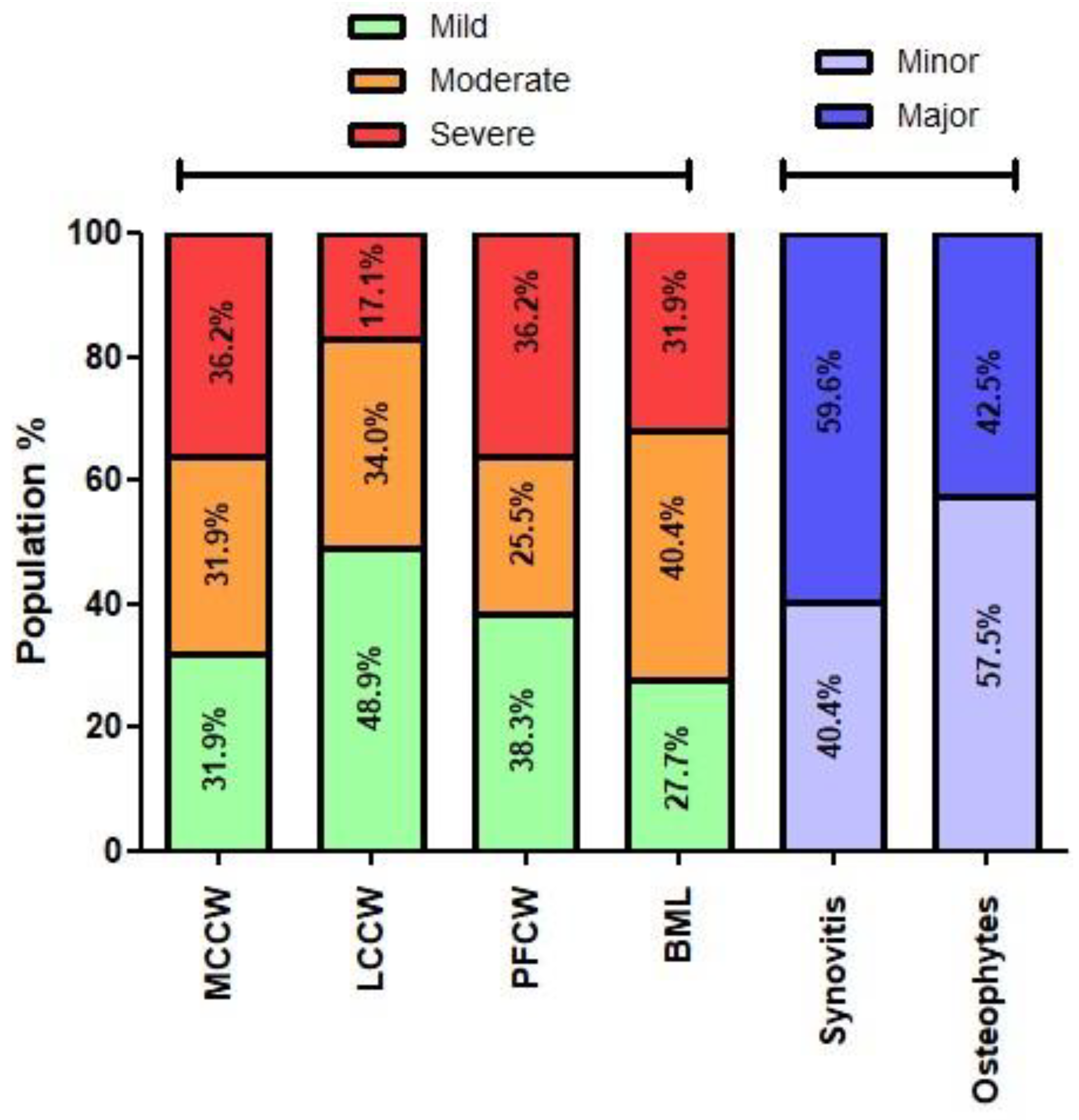
| Pathology-Specific Parameters (Maximum Points on MOAKS) | Gradation (Points on MOAKS) |
|---|---|
| MCCW (15) | Mild (0–5) Moderate (6–10) Severe (11–15) |
| LCCW (15) | Mild (0–5) Moderate (6–10) Severe (11–15) |
| PFCW (12) | Mild (0–6) Moderate (7–9) Severe (10–12) |
| BML (45) | Mild (0–3) Moderate (4–10) Severe (>10) |
| Patellar synovitis (3) | Minor (0–1) Major (2–3) |
| Osteophytes (36) | Minor (0–14) Major (15–36) |
| PHL (yes/no) | MM LM |
| (1) | ||
| All MFAT Subjects (n = 64) | ||
| Age (mean ± SD) | 54.2 ± 9.1 | |
| Sex (%female) | 51.6% | |
| BMI (mean ± SD) | 27.2 ± 4.5 | |
| Bilateral injection n (%) | 27 subjects (42%) | |
| Smoking (%) | 12.9% | |
| Baseline KOOS (mean ± SD) | ||
| Pain | 45.9 ± 12.0 | |
| Symptoms | 52.0 ± 18.2 | |
| ADL | 53.6 ± 16.9 | |
| Sports | 15.4 ± 15.9 | |
| QoL | 26.3 ± 13.0 | |
| Baseline NRS (mean ± SD) | 5.5 ± 2.2 | |
| Baseline UCLA (mean ± SD) | 6.1 ± 2.1 | |
| Baseline EQ-5D index (mean ± SD) | 0.809 ± 0.052 | |
| (2) | ||
| Bilateral Cohort (n = 27) | Index Knee | Contralateral Knee |
| Age (mean ± SD) | 55.6 ± 10.1 | |
| Sex (%female) | 51.9% | |
| BMI (mean ± SD) | 28.2 ± 4.5 | |
| Baseline KOOS (mean ± SD) | ||
| Pain | 45.2 ± 12.1 | 46.5 ± 14.1 |
| Symptoms | 52.0 ± 19.0 | 56.6 ± 21.7 |
| ADL | 50.2 ± 16.2 | 53.4 ± 15.3 |
| Sports | 14.6 ± 14.8 | 17.6 ± 16.7 |
| QoL | 27.1 ± 12.9 | 29.9 ± 12.3 |
| Baseline NRS (mean ± SD) | 5.4 ± 2.2 | 4.6 ± 1.9 |
| Location | Injury | Tear Type |
|---|---|---|
| Medial meniscus | Tear | Vertical: 6% (3/47) |
| Horizontal: 30% (14/47) | ||
| Complex: 32% (15/47) | ||
| PHL: 40% (19/47) | ||
| Maceration | Partial: 55% (26/47) | |
| Complete: 32% (15/47) | ||
| Lateral meniscus | Tear | Vertical: 11% (5/47) |
| Horizontal: 23% (11/47) | ||
| Complex: 13% (6/47) | ||
| PHL: 30% (14/47) | ||
| Maceration | Partial: 45% (21/47) | |
| Complete: 11% (5/47) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Genechten, W.; Vuylsteke, K.; Martinez, P.R.; Swinnen, L.; Sas, K.; Verdonk, P. Autologous Micro-Fragmented Adipose Tissue (MFAT) to Treat Symptomatic Knee Osteoarthritis: Early Outcomes of a Consecutive Case Series. J. Clin. Med. 2021, 10, 2231. https://doi.org/10.3390/jcm10112231
Van Genechten W, Vuylsteke K, Martinez PR, Swinnen L, Sas K, Verdonk P. Autologous Micro-Fragmented Adipose Tissue (MFAT) to Treat Symptomatic Knee Osteoarthritis: Early Outcomes of a Consecutive Case Series. Journal of Clinical Medicine. 2021; 10(11):2231. https://doi.org/10.3390/jcm10112231
Chicago/Turabian StyleVan Genechten, Wouter, Kristien Vuylsteke, Pedro Rojas Martinez, Linus Swinnen, Kristof Sas, and Peter Verdonk. 2021. "Autologous Micro-Fragmented Adipose Tissue (MFAT) to Treat Symptomatic Knee Osteoarthritis: Early Outcomes of a Consecutive Case Series" Journal of Clinical Medicine 10, no. 11: 2231. https://doi.org/10.3390/jcm10112231