1. Introduction
In the last days of December 2019, coronavirus disease 2019 (COVID-19), which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), broke out in the Huabei region (China). Since then, SARS-CoV-2 has continued to spread worldwide leading the WHO, on March 11th, to declare COVID-19 a pandemic [
1]. Patients affected by COVID-19 gave rise to high rates of hospitalization and intensive care unit (ICU) admissions [
2], with in-hospital mortality as high as 28% in severe COVID-19 [
3].
Several studies investigated the possible correlation between markers of cardiac disease and the worsening of COVID-19 severity [
4,
5]. Diffuse inflammation is the hallmark of the disease and could possibly lead to atherosclerosis-based cardiovascular disease, as previously demonstrated for other infectious diseases [
6]. Increased concentrations of markers for cardiac disease were detected early in patients suffering from COVID-19, and in particular high concentrations of high-sensitive cardiac troponin I (HsTnI) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) were associated with the worst prognosis for hospitalized patients [
7,
8,
9]. NT-proBNP is currently known as an independent risk factor for in-hospital death of patients with severe COVID-19 [
10]. B-type natriuretic peptide (BNP) was recently reported as a possible predictive marker for survival of COVID-19 patients [
11]. HsTnI is significantly increased at admission in patients with severe COVID-19 compared to those affected by milder forms of COVID-19 [
12], and has been recently described as a possible predictor of in-hospital mortality [
13].
The aim of this study was to evaluate which of BNP, NT-proBNP and HsTnI could be considered the best prognostic predictor in COVID-19 patients.
2. Materials and Methods
This prospective observational study was performed according to the current version of the Helsinki Declaration and was approved by the Ethical Committee of the University of Naples “Federico II”, Italy (Number 156/20, 22 April 2020). Informed consent was obtained from all subjects involved in the study.
Patients were hospitalized in two units of the University of Naples “Federico II” (infectious disease unit and ICU) directly from the emergency room or following general practitioner indications. In order to be selected, all patients admitted to those wards from 10 March 2020 to 30 April 2020, and from 8 December 2020 to 25 January 2021 had to match the following inclusion criteria: intention to participate in the study and signature of informed consent, age > 18 years, and rhino-oropharyngeal swab positivity for SARS-CoV-2 RNA. Exclusion criteria included inability to understand or sign informed consent, age < 18 years, absence of positivity for SARS-CoV-2 RNA test, positivity for serological tests only, as well as any other condition that in the investigator’s opinion could make the patient non-eligible to participate in the study or could interfere with the patient’s participation in the study and its completion.
BNP, NT-proBNP and HsTnI were analyzed at admission. Data on the clinical course of COVID-19 before hospitalization and its related complications were also acquired. In particular, the presence of pre-existing diseases related to cardiac and pulmonary functions was recorded and included in data analysis, alongside with diabetes and hypertension.
BNP and HsTnI plasma concentrations were measured by chemiluminescent microparticle immunoassay on the ARCHITECT i2000SR system (Abbott Laboratories, Wiesbaden, Germany). NT-proBNP was also measured on the ARCHITECT i2000SR system by using the Alere assay (Roche Diagnostics GmbH, Mannheim, Germany). BNP and NT-proBNP were collected in tubes with EDTA, while HsTnI was collected in tubes with sodium heparin.
Upper reference ranges for BNP were: 89 ng/L for patients under 45 years, 111 ng/L for 45–54 years-old patients, 155 ng/L for 54–64 years-old patients, 159 ng/L for 64–74 years-old patients and 266 ng/L for patients > 74 years. Upper reference ranges for NT-proBNP were 125 ng/L for patients < 75 years and 450 ng/L for patients > 75 years. The decision level (99th percentile) for HsTnI was 34 ng/L for men and 16 ng/L for women.
Data analysis was performed comparing the level of all the markers between in-hospital survivors who were successfully discharged and in-hospital non-survivors, for both critical patients (ICU) and non-critical patients (infectious disease unit).
The normal distribution of variables was evaluated by the Kolmogorov–Smirnov test and the chi-square test to compare frequencies between groups, with the use of the Fisher exact test when comparing dichotomic variables. Categorical variables are reported as number of subjects and percentages, and continuous non-parametric variables are reported as interquartile range, respectively. Differences between two groups were assessed by the Mann–Whitney test.
Analysis of receiver operating characteristic (ROC) curves and dot diagrams was performed with the MedCalc software Version 11.5.1 (Medcalc Software Ltd., 8400 Ostend, Belgium). Statistical significance of the area under the ROC curves (AUC) was calculated against the null hypothesis AUC = 0.5 as recommended by DeLong et al. [
14]. Threshold values were determined by the farthest point from the bisector of the ROC curve.
Binary logistic regression was performed, including gender (encoded as 1 = male and 2 = female), age in years, NT-proBNP and HsTnI. Kaplan–Meier analysis (log-rank test) was used to compare the survival experience of the participants. Statistical analyses were carried out using the statistical Predictive Analytics Software version 21.0 (SPSS Inc., Chicago, IL, USA). A p-value of p < 0.05 was considered statistically significant.
3. Results
One hundred and seventy-four patients were enrolled in this study: eighteen critical patients were admitted to the ICU while 156 non-critical patients were hospitalized in the infectious disease unit. Thirteen patients showed in-hospital fatal outcome, ten from the ICU and three from the infectious disease unit. The direct causes of death were respiratory failure (
n = 3), septic complications (
n = 4), neurological complications (
n = 2) and cardiogenic shock (
n = 4). Population characteristics, biochemical baseline values and differences between surviving and non-surviving groups are depicted in
Table 1.
Comorbidities, smoking and oxygen saturation at admission were not statistically different between surviving and non-surviving patients. In detail, cardiac pathologies reported were ischemic heart disease (n = 14), heart failure (n = 6) and atrial fibrillation (n = 4). Older age, a higher percentage of male gender, and higher concentrations of BNP, NT-proBNP and HsTnI were present in the non-surviving group. Only 17 patients showed baseline values higher than the appropriate upper reference ranges for age and sex for BNP (9,8%) and 20 for HsTnI (11.5%), whereas higher baseline values for NT-proBNP were reported in 87 patients (50.0%).
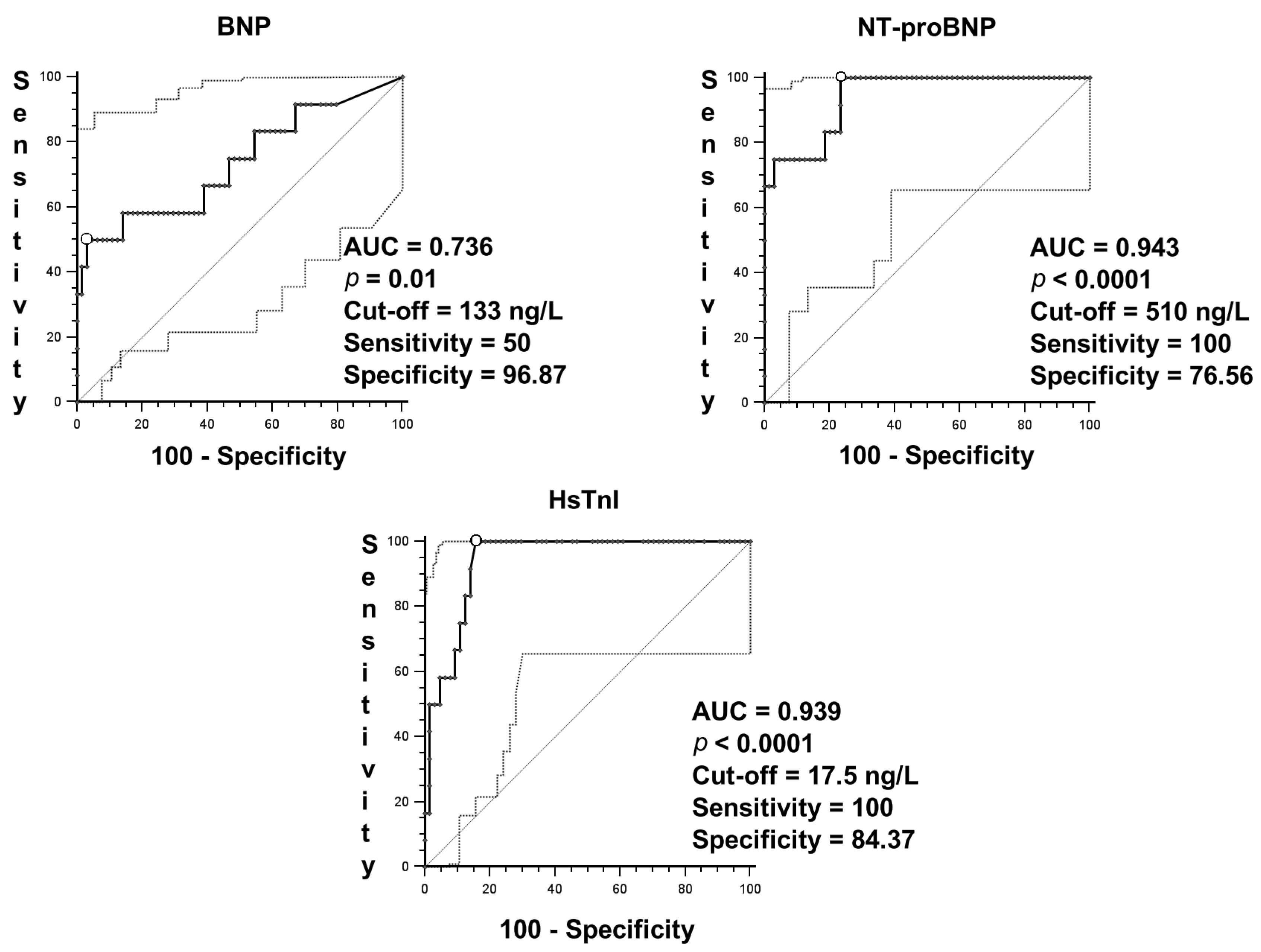
ROC curves were performed (
Figure 1) for BNP (AUC = 0.777,
p < 0.001), NT-proBNP (AUC = 0.951,
p < 0.001) and HsTnI (AUC = 0.974,
p < 0.001), with both NT-proBNP and HsTnI ROC curves performing better than the BNP ROC curve (
p = 0.01). There were no statistical differences between NT-proBNP and HsTnI ROC curves.
Logistic regression was then performed with age, gender, NT-proBNP and HsTnI as covariates and in-hospital death as the dependent variable, with only NT-proBNP showing a significant odds ratio (OR = 1.002, 95%CI 1.001–1.003, p = 0.04).
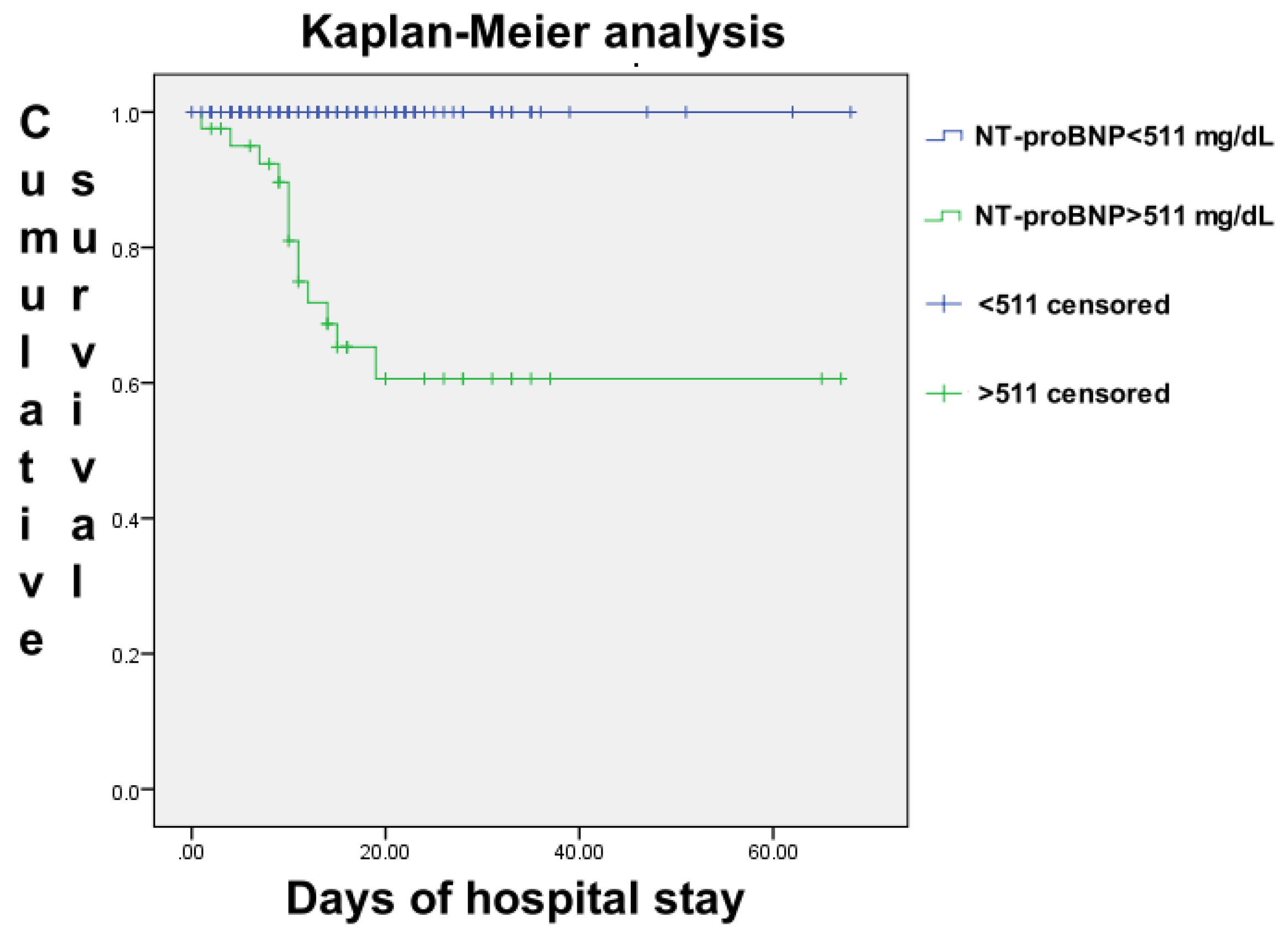
The population was then divided into two groups based on whether patients had higher values than the cut-off point of the NT-proBNP ROC curve (511 ng/L) or not. The Kaplan–Meier analysis was performed (
Figure 2) and logarithmic rank analysis showed a statistical difference in terms of survival between the two groups (
p < 0.001), with an absence of fatal outcome in the group of patients with NT-proBNP values lower than 511 ng/L at admission.
4. Discussion
This prospective observational study highlighted that NT-proBNP may be the most useful predictor of fatal outcome in COVID-19 patients. There was no fatal outcome in patients with a value of NT-proBNP below the 511 ng/L cut-off resulting from the ROC curve at admission. Moreover, a large number of patients in both surviving and non-surviving groups showed pathological values of NT-proBNP above the upper reference interval, although this reference interval was age adjusted [
15,
16]. HsTnI, nonetheless, seems to be a good mortality predictor as well.
BNP and NT-proBNP are secreted in response to increased myocardial wall stress [
17]. Quite surprisingly, despite BNP values being higher in non-surviving patients, the NT-proBNP ROC curve showed that NT-proBNP was a more effective prognostic tool than BNP, although these two markers may be considered as equal diagnostic tools for heart failure [
18]. This discordance may be due to extrarenal clearance in the context of renal failure, since neutral endopeptidases seem to accumulate, whereas up-regulation of the type-C natriuretic peptide receptor seems to occur in critical states [
19]. Another explanation may be related to the presence of NT-proBNP glycosylation, a process which may be inhibited during critical status; NT-proBNP is often miscalculated due to its preponderant undetectable glycosylated quota [
20], showing much higher values when tubes are pre-treated with de-glycosylation enzymes [
21]. Further studies are needed to support this hypothesis. Finally, this result may be caused by a proBNP cross-reaction occurring during NT-proBNP detection without affecting the BNP measurement [
22], leading to NT-proBNP values higher than BNP values.
BNP was recently described in the meta-analysis by Wungu et al. [
11] as a possible predictive marker for survival of COVID-19 patients. A significant difference between surviving and non-surviving patients was reported in our study as well, but BNP was eventually outperformed by NT-proBNP and HsTnI ROC curves.
Elevated NT-proBNP concentrations were associated to a significant risk of mortality in septic patients even without a clear cardiac depression [
23]. Several mechanisms are likely to account for increased NT-proBNP in septic patients, including acute renal injury and proinflammatory molecules such as lipopolysaccharides, interleukin 1, C-reactive protein, and cardiotrophin I, which are independent of ventricular function [
24,
25].
The angiotensin-converting enzyme 2 (ACE2) is likely to play a role, being a major binding site for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [
26]. As an indirect mechanism, the down-regulation of ACE2 and the subsequent activation of the renin–angiotensin–aldosterone system induced by the viral infection may contribute to the local and systemic inflammatory response, which damages the tissue and triggers the release of biomarkers [
26]. As a direct mechanism, SARS-CoV-2, binding ACE2, prevents the angiotensin II clearance, by reducing the concentrations of angiotensin-(1–7); thus, resulting in an increase in NT-proBNP concentrations and kidney podocytes dysfunction [
26,
27].
HsTnI concentrations were higher in non-surviving patients, and its ROC curve was comparable to the NT-proBNP one. When age and sex were considered, though, the still significant variable was only NT-proBNP. HsTnI, in fact, is highly influenced by gender [
28], thus, making NT-proBNP a highly, very reliable independent prognostic factor at admission for fatal outcome in COVID-19 patients.
This is the first study to effectively compare BNP and NT-proBNP, which—as previously stated—are known as equal diagnostic tools for heart failure.
The study has a few limitations: only 18 patients were hospitalized in the ICU, whereas 156 patients were hospitalized in the infectious disease unit, leading to a heterogeneity in our population. Moreover, only six ICU patients showed in-hospital survival, as most of them were non-surviving patients. A greater number of patients discharged from the ICU might have been useful in order to compare these two different population subgroups.
If confirmed by larger population studies, our findings may provide clinicians with the most appropriate tools to gain relevant insight into COVID-19 prognosis and survival rate.
5. Conclusions
In conclusion, NT-proBNP turned out to be a better prognostic marker than BNP and HsTnI in COVID-19 disease. In particular, our study highlighted that a value of NT-proBNP below the cut-off of 511 ng/L at admission led to no in-hospital mortality in our population.
Author Contributions
Conceptualization, G.F., I.G. and G.S.; Methodology, R.d.F., M.V. (Maria Vargas) and B.P.; Validation, M.S.; Formal Analysis, R.d.F. and M.V. (Maria Vargas); Investigation, A.M., D.P. and M.V. (Martina Vano); Writing—Original Draft Preparation, G.F. and R.d.F.; Writing—Review and Editing, G.F., I.G. and G.S.; Project Administration, G.F., I.G. and G.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the University of Naples “Federico II” (Number 156/20, 22 April 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from the patients to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
I.G. acted as a consultant for Gilead, MSD, Abbvie, Pfizer, Nordic, Angelini, Correvio. All of the other authors declare no conflict of interest.
References
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef]
- Vargas, M.; De Marco, G.; De Simone, S.; Servillo, G. Logistic and organizational aspects of a dedicated intensive care unit for COVID-19 patients. Crit Care 2020, 24, 237. [Google Scholar] [CrossRef]
- Weiss, P.; Murdoch, D.R. Clinical course and mortality risk of severe COVID-19. Lancet 2020, 395, 1014–1015. [Google Scholar] [CrossRef]
- Mueller, C.; Giannitsis, E.; Jaffe, A.S.; Huber, K.; Mair, J.; Cullen, L.; Hammarsten, O.; Mills, N.L.; Mockel, M.; Krychtiuk, K.; et al. Cardiovascular biomarkers in patients with COVID-19. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 310–319. [Google Scholar] [CrossRef]
- Dawson, D.; Dominic, P.; Sheth, A.; Modi, M. Prognostic value of Cardiac Biomarkers in COVID-19 Infection: A Meta-analysis. Res. Sq. 2020, 11, 4930. [Google Scholar] [CrossRef]
- Musher, D.M.; Abers, M.S.; Corrales-Medina, V.F. Acute Infection and Myocardial Infarction. N. Engl. J. Med. 2019, 380, 171–176. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Wibowo, A.; Pranata, R.; Akbar, M.R.; Purnomowati, A.; Martha, J.W. Prognostic performance of troponin in COVID-19: A diagnostic meta-analysis and meta-regression. Int. J. Infect.Dis. 2021, 105, 312–318. [Google Scholar] [CrossRef]
- Pranata, R.; Huang, I.; Lukito, A.A.; Raharjo, S.B. Elevated N-terminal pro-brain natriuretic peptide is associated with increased mortality in patients with COVID-19: Systematic review and meta-analysis. Postgrad. Med. J. 2020, 96, 387–391. [Google Scholar] [CrossRef]
- Wungu, C.D.K.; Khaerunnisa, S.; Putri, E.A.C.; Hidayati, H.B.; Qurnianingsih, E.; Lukitasari, L.; Humairah, I.; Soetjipto. Meta-analysis of cardiac markers for predictive factors on severity and mortality of COVID-19. Int. J. Infect. Dis. 2021, 105, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Lavie, C.J.; Sanchis-Gomar, F. Cardiac troponin I in patients with coronavirus disease 2019 (COVID-19): Evidence from a meta-analysis. Prog. Cardiovasc. Dis. 2020, 63, 390–391. [Google Scholar] [CrossRef] [PubMed]
- Tahtasakal, C.A.; Oncul, A.; Sevgi, D.Y.; Celik, E.; Ocal, M.; Turkkan, H.M.; Bayraktar, B.; Oba, S.; Dokmetas, I. Could we predict the prognosis of the COVID-19 disease? J. Med. Virol. 2021, 93, 2420–2430. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Hogenhuis, J.; Voors, A.A.; Jaarsma, T.; Hillege, H.L.; Boomsma, F.; van Veldhuisen, D.J. Influence of age on natriuretic peptides in patients with chronic heart failure: A comparison between ANP/NT-ANP and BNP/NT-proBNP. Eur. J. Heart Fail. 2005, 7, 81–86. [Google Scholar] [CrossRef] [Green Version]
- Fortunato, G.; Carandente Giarrusso, P.; Martinelli, P.; Sglavo, G.; Vassallo, M.; Tomeo, L.; Rea, M.; Paladini, D. Cardiac troponin T and amino-terminal pro-natriuretic peptide concentrations in fetuses in the second trimester and in healthy neonates. Clin. Chem. Lab. Med. 2006, 44, 834–836. [Google Scholar] [CrossRef]
- Wang, F.; Wu, Y.; Tang, L.; Zhu, W.; Chen, F.; Xu, T.; Bo, L.; Li, J.; Deng, X. Brain natriuretic peptide for prediction of mortality in patients with sepsis: A systematic review and meta-analysis. Crit. Care 2012, 16, R74. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Van Kimmenade, R.R.; Januzzi, J.L., Jr.; Bakker, J.A.; Houben, A.J.; Rennenberg, R.; Kroon, A.A.; Crijns, H.J.; van Dieijen-Visser, M.P.; de Leeuw, P.W.; Pinto, Y.M. Renal clearance of B-type natriuretic peptide and amino terminal pro-B-type natriuretic peptide a mechanistic study in hypertensive subjects. J. Am. Coll. Cardiol. 2009, 53, 884–890. [Google Scholar] [CrossRef] [Green Version]
- Nishikimi, T.; Ikeda, M.; Takeda, Y.; Ishimitsu, T.; Shibasaki, I.; Fukuda, H.; Kinoshita, H.; Nakagawa, Y.; Kuwahara, K.; Nakao, K. The effect of glycosylation on plasma N-terminal proBNP-76 levels in patients with heart or renal failure. Heart 2012, 98, 152–161. [Google Scholar] [CrossRef]
- Rosjo, H.; Dahl, M.B.; Jorgensen, M.; Roysland, R.; Brynildsen, J.; Cataliotti, A.; Christensen, G.; Hoiseth, A.D.; Hagve, T.A.; Omland, T. Influence of glycosylation on diagnostic and prognostic accuracy of N-terminal pro-B-type natriuretic peptide in acute dyspnea: Data from the Akershus Cardiac Examination 2 Study. Clin. Chem. 2015, 61, 1087–1097. [Google Scholar] [CrossRef] [Green Version]
- Luckenbill, K.N.; Christenson, R.H.; Jaffe, A.S.; Mair, J.; Ordonez-Llanos, J.; Pagani, F.; Tate, J.; Wu, A.H.; Ler, R.; Apple, F.S. Cross-reactivity of BNP, NT-proBNP, and proBNP in commercial BNP and NT-proBNP assays: Preliminary observations from the IFCC Committee for Standardization of Markers of Cardiac Damage. Clin. Chem. 2008, 54, 619–621. [Google Scholar] [CrossRef]
- Shor, R.; Rozenman, Y.; Bolshinsky, A.; Harpaz, D.; Tilis, Y.; Matas, Z.; Fux, A.; Boaz, M.; Halabe, A. BNP in septic patients without systolic myocardial dysfunction. Eur. J. Intern. Med. 2006, 17, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Vallabhajosyula, S.; Wang, Z.; Murad, M.H.; Sundaragiri, P.R.; Kashani, K.; Miller, W.L.; Jaffe, A.S. Natriuretic Peptides to Predict Short-Term Mortality in Patients with Sepsis: A Systematic Review and Meta-analysis. Mayo Clin.Proc. Innov. Qual. Outcomes 2020, 4, 50–64. [Google Scholar] [CrossRef]
- Han, H.; Xie, L.; Liu, R.; Yang, J.; Liu, F.; Wu, K.; Chen, L.; Hou, W.; Feng, Y.; Zhu, C. Analysis of heart injury laboratory parameters in 273 COVID-19 patients in one hospital in Wuhan, China. J. Med. Virol. 2020, 92, 819–823. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Vardeny, O.; Michel, T.; McMurray, J.J.V.; Pfeffer, M.A.; Solomon, S.D. Renin-Angiotensin-Aldosterone System Inhibitors in Patients with Covid-19. N. Engl. J. Med. 2020, 382, 1653–1659. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Rojas, M.A.; Vega-Vega, O.; Bobadilla, N.A. Is the kidney a target of SARS-CoV-2? Am. J. Physiol. Ren. Physiol. 2020, 318, F1454–F1462. [Google Scholar] [CrossRef]
- Giannitsis, E.; Mueller-Hennessen, M.; Zeller, T.; Schuebler, A.; Aurich, M.; Biener, M.; Vafaie, M.; Stoyanov, K.M.; Ochs, M.; Riffel, J.; et al. Gender-specific reference values for high-sensitivity cardiac troponin T and I in well-phenotyped healthy individuals and validity of high-sensitivity assay designation. Clin. Biochem. 2020, 78, 18–24. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 


{kind=link}
{kind=link}