
The Impact of the COVID-19 Emergency on Life Activities and Delivery of Healthcare Services in the Elderly Population

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Explanatory Variables
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
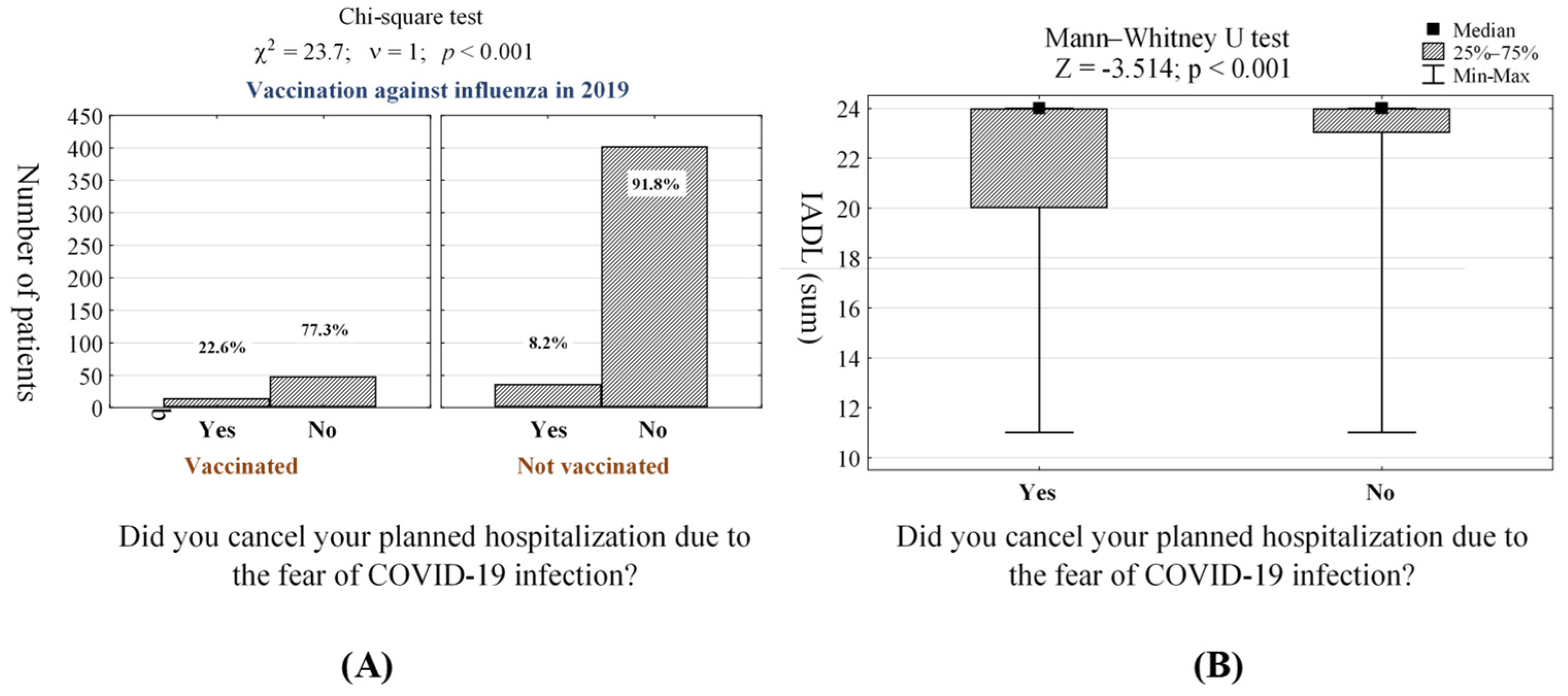
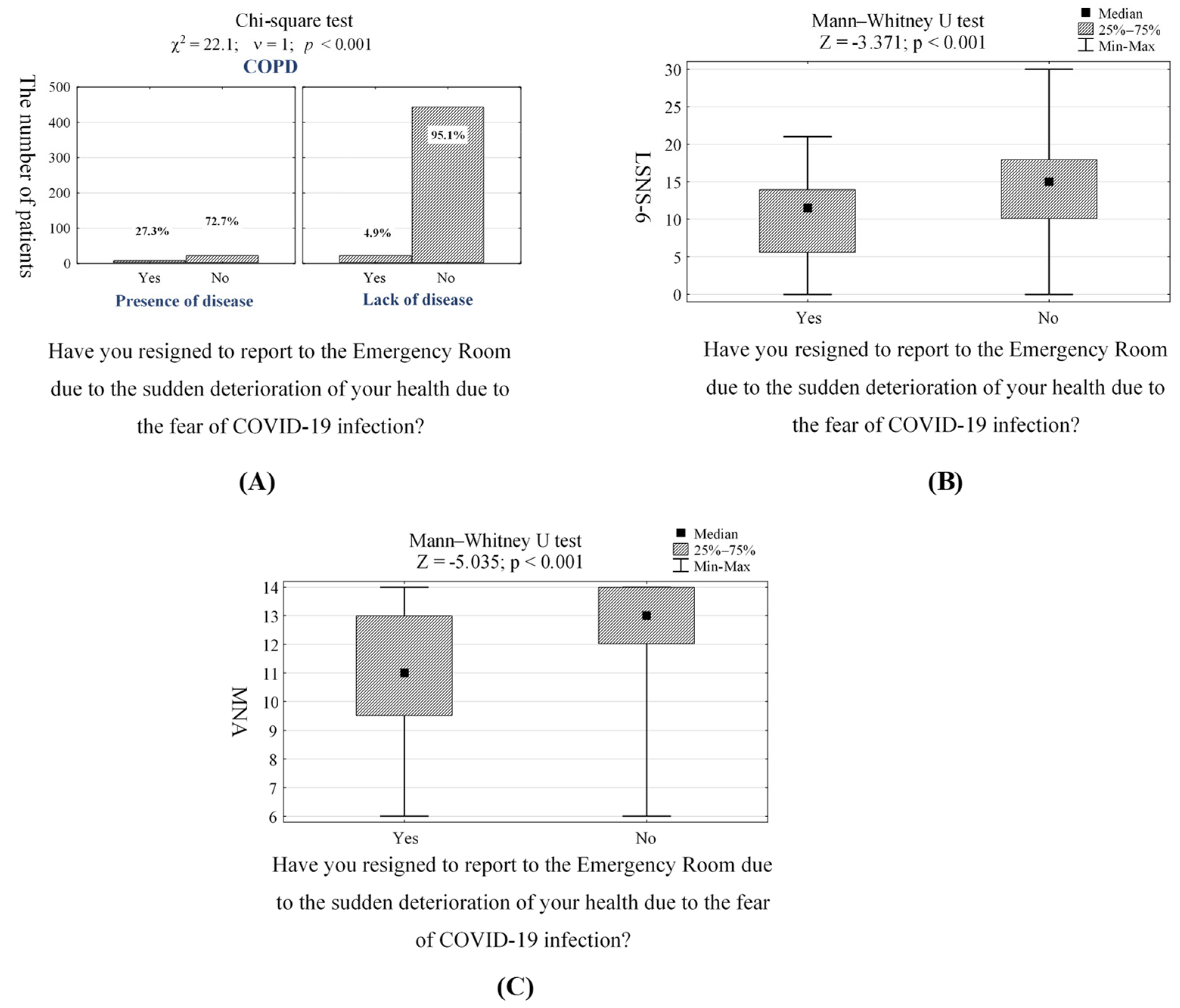
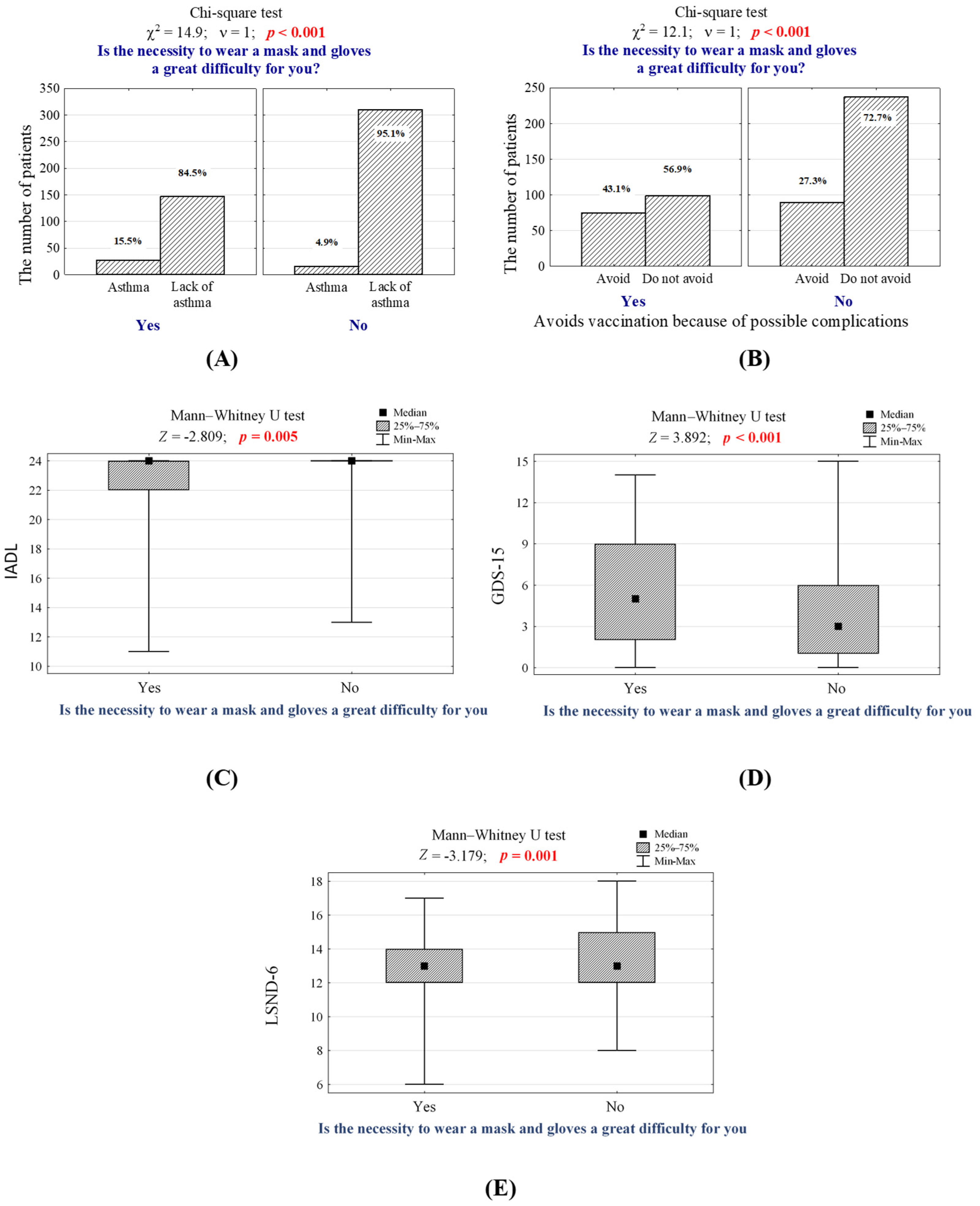
3.2. Reactions (Limitations) Related to the Fear of COVID-19 Infection
4. Discussion
4.1. The Impact of COVID-19 Pandemic on Everyday Activities of Elderly Population
4.2. The Most Significant Findings of the Study
4.3. Telemedicine as a Proposed Strategy against SARS-CoV-2
4.4. The Importance of COVID-19 Safety Measures
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meisner, B.A.; Boscart, V.; Gaudreau, P.; Stolee, P.; Ebert, P.; Heyer, M.; Kadowaki, L.; Kelly, C.; Levasseur, M.; Massie, A.S.; et al. Interdisciplinary and Collaborative Approaches Needed to Determine Impact of COVID-19 on Older Adults and Aging: CAG/ACG and CJA/RCV Joint Statement. Can. J. Aging 2020, 39, 333–343. [Google Scholar] [CrossRef]
- Niu, S.; Tian, S.; Lou, J.; Kang, X.; Zhang, L.; Lian, H.; Zhang, J. Clinical characteristics of older patients infected with COVID-19: A descriptive study. Arch. Gerontol. Geriatr. 2020, 89, 104058. [Google Scholar] [CrossRef]
- Lian, J.; Jin, X.; Hao, S.; Cai, H.; Zhang, S.; Zheng, L.; Jia, H.; Hu, J.; Gao, J.; Zhang, Y.; et al. Analysis of epidemiological and clinical features in older patients with coronavirus disease 2019 (COVID-19) outside Wuhan. Clin. Infect. Dis. 2020, 71, 740–747. [Google Scholar] [CrossRef] [Green Version]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Liu, J.; Zhao, X.; Liu, C.; Wang, W.; Wang, D.; Xu, W.; Zhang, C.; Yu, J.; Jiang, B.; et al. Clinical characteristics of imported cases of coronavirus disease 2019 (COVID-19) in Jiangsu Province: A multicenter descriptive study. Clin. Infect. Dis. 2020, 71, 706–712. [Google Scholar] [CrossRef]
- Shahid, Z.; Kalayanamitra, R.; McClafferty, B.; Kepko, D.; Ramgobin, D.; Patel, R.; Aggarwal, C.S.; Vunnam, R.; Sahu, N.; Bhatt, D.; et al. COVID-19 and Older Adults: What We Know. J. Am. Geriatr. Soc. 2020, 68, 926–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lithander, F.E.; Neumann, S.; Tenison, E.; Lloyd, K.; Welsh, T.J.; Rodrigues, J.C.L.; Higgins, J.P.T.; Scourfield, L.; Christensen, H.; Haunton, V.J.; et al. COVID-19 in older people: A rapid clinical review. Age Ageing 2020, 49, 501–515. [Google Scholar] [CrossRef] [PubMed]
- Nanda, A.; Vura, N.V.R.K.; Gravenstein, S. COVID-19 in older adults. Aging Clin. Exp. Res. 2020, 32, 1199–1202. [Google Scholar] [CrossRef] [PubMed]
- Wańkowicz, P.; Szylińska, A.; Rotter, I. The Impact of the COVID-19 Pandemic on Psychological Health and Insomnia among People with Chronic Diseases. J. Clin. Med. 2021, 10, 1206. [Google Scholar] [CrossRef] [PubMed]
- Mistry, S.K.; Ali, A.M.; Yadav, U.N.; Ghimire, S.; Hossain, M.B.; Das Shuvo, S.; Saha, M.; Sarwar, S.; Nirob, M.M.H.; Sekaran, V.C.; et al. Older adults with non-communicable chronic conditions and their health care access amid COVID-19 pandemic in Bangladesh: Findings from a cross-sectional study. PLoS ONE 2021, 16, e0255534. [Google Scholar] [CrossRef]
- Addis, S.G.; Nega, A.D.; Miretu, D.G. Psychological impact of COVID-19 pandemic on chronic disease patients in Dessie town government and private hospitals, Northeast Ethiopia. Diabetes Metab. Syndr. 2021, 15, 129. [Google Scholar] [CrossRef]
- Mills, J.P.; Kaye, K.S.; Mody, L. COVID-19 in older adults: Clinical, psychosocial, and public health considerations. JCI Insight 2020, 5, e139292. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Chen, S.; Liu, M.; Nie, H.; Lu, H. Comorbid Chronic Diseases are Strongly Correlated with Disease Severity among COVID-19 Patients: A Systematic Review and Meta-Analysis. Aging Dis. 2020, 11, 668. [Google Scholar] [CrossRef]
- Agrawal, S.; Gołębiowska, J.; Bartoszewicz, B.; Makuch, S.; Mazur, G. Clinical preventive services to reduce pandemic deaths. Prev. Med. Rep. 2020, 20, 101249. [Google Scholar] [CrossRef]
- de Oliveira, L.D.S.S.C.B.; Souza, E.C.; Rodrigues, R.A.S.; Fett, C.A.; Piva, A.B. The effects of physical activity on anxiety, depression, and quality of life in elderly people living in the community. Trends Psychiatry Psychother. 2019, 41, 36–42. [Google Scholar] [CrossRef]
- Dohrn, I.M.; Hagströmer, M.; Hellénius, M.L.; Ståhle, A. Short- and long-term effects of balance training on physical activity in older adults with osteoporosis: A randomized controlled trial. J. Geriatr. Phys. Ther. 2017, 40, 102–111. [Google Scholar] [CrossRef] [Green Version]
- Steffl, M.; Bohannon, R.W.; Sontakova, L.; Tufano, J.J.; Shiells, K.; Holmerova, I. Relationship between sarcopenia and physical activity in older people: A systematic review and meta-analysis. Clin. Interv. Aging 2017, 12, 835–845. [Google Scholar] [CrossRef] [Green Version]
- An, H.Y.; Chen, W.; Wang, C.W.; Yang, H.F.; Huang, W.T.; Fan, S.Y. The relationships between physical activity and life satisfaction and happiness among young, middle-aged, and older adults. Int. J. Environ. Res. Public Health 2020, 17, 4817. [Google Scholar] [CrossRef] [PubMed]
- Lindsay Smith, G.; Banting, L.; Eime, R.; O’Sullivan, G.; van Uffelen, J.G.Z. The association between social support and physical activity in older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 56. [Google Scholar] [CrossRef] [PubMed]
- De Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J.C. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials Physical functioning, physical health and activity. BMC Geriatr. 2015, 15, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, F.; Norman, I.J.; While, A.E. Physical activity in older people: A systematic review. BMC Public Health 2013, 13, 449. [Google Scholar] [CrossRef] [Green Version]
- Gallardo-Alfaro, L.; Bibiloni, M.D.M.; Mateos, D.; Ugarriza, L.; Tur, J.A. Leisure-time physical activity and metabolic syndrome in older adults. Int. J. Environ. Res. Public Health 2019, 16, 3358. [Google Scholar] [CrossRef] [Green Version]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Moccia, F.; Gerbino, A.; Lionetti, V.; Miragoli, M.; Munaron, L.M.; Pagliaro, P.; Pasqua, T.; Penna, C.; Rocca, C.; Samaja, M.; et al. COVID-19-associated cardiovascular morbidity in older adults: A position paper from the Italian Society of Cardiovascular Researches. GeroScience 2020, 42, 1021–1049. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ma, Z.F. Impact of the COVID-19 pandemic on mental health and quality of life among local residents in Liaoning Province, China: A cross-sectional study. Int. J. Environ. Res. Public Health 2020, 17, 2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takashima, R.; Onishi, R.; Saeki, K.; Hirano, M. Perception of COVID-19 restrictions on daily life among japanese older adults: A qualitative focus group study. Healthcare 2020, 8, 450. [Google Scholar] [CrossRef] [PubMed]
- Goethals, L.; Barth, N.; Guyot, J.; Hupin, D.; Celarier, T.; Bongue, B. Impact of home quarantine on physical activity among older adults living at home during the COVID-19 pandemic: Qualitative interview study. JMIR Aging 2020, 3, e19007. [Google Scholar] [CrossRef]
- Briguglio, M.; Giorgino, R.; Dell’Osso, B.; Cesari, M.; Porta, M.; Lattanzio, F.; Banfi, G.; Peretti, G.M. Consequences for the Elderly After COVID-19 Isolation: FEaR (Frail Elderly amid Restrictions). Front. Psychol. 2020, 11, 565052. [Google Scholar] [CrossRef]
- Iorga, M.; Soponaru, C.; Socolov, R.V.; Cărăuleanu, A.; Socolov, D.G. How the sars-cov-2 pandemic period influenced the health status and determined changes in professional practice among obstetrics and gynecology doctors in Romania. Medicina 2021, 57, 325. [Google Scholar] [CrossRef] [PubMed]
- Awick, E.A.; Ehlers, D.K.; Aguiñaga, S.; Daugherty, A.M.; Kramer, A.F.; McAuley, E. Effects of a randomized exercise trial on physical activity, psychological distress and quality of life in older adults. Gen. Hosp. Psychiatry 2017, 49, 44–50. [Google Scholar] [CrossRef]
- Puciato, D.; Borysiuk, Z.; Rozpara, M. Quality of life and physical activity in an older working-age population. Clin. Interv. Aging 2017, 12, 1627–1634. [Google Scholar] [CrossRef] [Green Version]
- Groessl, E.J.; Kaplan, R.M.; Rejeski, W.J.; Katula, J.A.; Glynn, N.W.; King, A.C.; Anton, S.D.; Walkup, M.; Lu, C.J.; Reid, K.; et al. Physical Activity and Performance Impact Long-term Quality of Life in Older Adults at Risk for Major Mobility Disability. Am. J. Prev. Med. 2019, 56, 141–146. [Google Scholar] [CrossRef] [PubMed]
- OECD Evaluating the initial impact of COVID-19 containment measures on economic activity. In Tackling Coronavirus (COVID-19) Contributing to a Global Effort; OECD: Paris, France, 2020; pp. 1–5.
- Kohler, H.; Bäuerle, A.; Schweda, A.; Weismüller, B.; Fink, M.; Musche, V.; Robitzsch, A.; Pfeiffer, C.; Benecke, A.V.; Dörrie, N.; et al. Increased COVID-19-related fear and subjective risk perception regarding COVID-19 affects behavior in individuals with internal high-risk diseases. J. Prim. Care Community Health 2021, 12, 2150132721996898. [Google Scholar] [CrossRef]
- Liang, C.; Zhang, W.; Li, S.; Qin, G. Coronary heart disease and COVID-19: A meta-analysis. Med. Clin. 2021, 156, 547–554. [Google Scholar] [CrossRef]
- Gerayeli, F.V.; Milne, S.; Cheung, C.; Li, X.; Yang, C.W.T.; Tam, A.; Choi, L.H.; Bae, A.; Sin, D.D. COPD and the risk of poor outcomes in COVID-19: A systematic review and meta-analysis. EClinicalMedicine 2021, 33, 100789. [Google Scholar] [CrossRef]
- Nan, J.; Jia, R.; Meng, S.; Jin, Y.; Chen, W.; Hu, H. The Impact of the COVID-19 Pandemic and the Importance of Telemedicine in Managing Acute ST Segment Elevation Myocardial Infarction Patients: Preliminary Experience and Literature Review. J. Med. Syst. 2021, 45, 9. [Google Scholar] [CrossRef]
- Gazibara, T.; Kovacevic, N.; Kisic-Tepavcevic, D.; Nurkovic, S.; Kurtagic, I.; Gazibara, T.; Pekmezovic, T. Flu vaccination among older persons: Study of knowledge and practices. J. Health Popul. Nutr. 2019, 38, 2. [Google Scholar] [CrossRef] [Green Version]
- Demicheli, V.; Jefferson, T.; Di Pietrantonj, C.; Ferroni, E.; Thorning, S.; Thomas, R.E.; Rivetti, A. Vaccines for preventing influenza in the elderly. Cochrane Database Syst. Rev. 2018, 2, CD004876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massoudi, N.; Mohit, B. A Case–Control Study of the 2019 Influenza Vaccine and Incidence of COVID-19 Among Healthcare Workers. J. Clin. Immunol. 2021, 41, 324–334. [Google Scholar] [CrossRef] [PubMed]
- Zanettini, C.; Omar, M.; Dinalankara, W.; Imada, E.L.; Colantuoni, E.; Parmigiani, G.; Marchionni, L. Influenza vaccination and covid-19 mortality in the usa: An ecological study. Vaccines 2021, 9, 427. [Google Scholar] [CrossRef] [PubMed]
- Conlon, A.; Ashur, C.; Washer, L.; Eagle, K.A.; Hofmann Bowman, M.A. Impact of the influenza vaccine on COVID-19 infection rates and severity. Am. J. Infect. Control 2021, 49, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Pedote, P.D.; Termite, S.; Gigliobianco, A.; Lopalco, P.L.; Bianchi, F.P. Influenza vaccination and health outcomes in COVID-19 patients: A retrospective cohort study. Vaccines 2021, 9, 358. [Google Scholar] [CrossRef] [PubMed]
- Chow, N.; Fleming-Dutra, K.; Gierke, R.; Hall, A.; Hughes, M.; Pilishvili, T.; Ritchey, M.; Roguski, K.; Skoff, T.; Ussery, E. Preliminary Estimates of the Prevalence of Selected Underlying Health Conditions Among Patients with Coronavirus Disease 2019—United States, February 12–March 28, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 382–386. [Google Scholar]
- Han, M.F.Y.; Mahendran, R.; Yu, J. Associations Between Fear of COVID-19, Affective Symptoms and Risk Perception Among Community-Dwelling Older Adults During a COVID-19 Lockdown. Front. Psychol. 2021, 12, 961. [Google Scholar] [CrossRef]
- Zhu, S.; Gao, Q.; Yang, L.; Yang, Y.; Xia, W.; Cai, X.; Hui, Y.; Zhu, D.; Zhang, Y.; Zhang, G.; et al. Prevalence and risk factors of disability and anxiety in a retrospective cohort of 432 survivors of Coronavirus Disease-2019 (COVID-19) from China. PLoS ONE 2020, 15, e0243883. [Google Scholar] [CrossRef]
- International Labour Organization Global impact and policy recommendations. In COVID-19 and the World of Work, 1st ed.; ILO Monitor: Geneva, Switzerland, 2020; pp. 1–15.
- Vanni, G.; Materazzo, M.; Pellicciaro, M.; Ingallinella, S.; Rho, M.; Santori, F.; Cotesta, M.; Caspi, J.; Makarova, A.; Pistolese, C.A.; et al. Breast cancer and COVID-19: The effect of fear on patients’ decision-making process. In Vivo 2020, 34, 1651–1659. [Google Scholar] [CrossRef]
- Lee, Y.R.; Lee, J.Y.; Park, I.H.; Kim, M.; Jhon, M.; Kim, J.W.; Ryu, S.; Kim, J.M.; Kim, S.W. The Relationships among Media Usage Regarding COVID-19, Knowledge about Infection, and Anxiety: Structural Model Analysis. J. Korean Med. Sci. 2020, 35, e426. [Google Scholar] [CrossRef]
- De Bonis, S.; Salerno, N.; Bisignani, A.; Capristo, A.; Sosto, G.; Verta, A.; Borselli, R.; Capristo, C.; Bisignani, G. COVID-19 and STEMI: The role of telecardiology in the management of STEMI diagnosis during COVID 19 pandemic. Int. J. Cardiol. Hear. Vasc. 2021, 32, 100720. [Google Scholar]
- Franklin, G.; Martin, C.; Ruszaj, M.; Matin, M.; Kataria, A.; Hu, J.; Brickman, A.; Elkin, P.L. How the COVID-19 pandemic impacted medical education during the last year of medical school: A class survey. Life 2021, 11, 294. [Google Scholar] [CrossRef]
- Hau, Y.S.; Kim, J.K.; Hur, J.; Chang, M.C. How about actively using telemedicine during the COVID-19 pandemic? J. Med. Syst. 2020, 44, 108. [Google Scholar] [CrossRef] [PubMed]
- Tourkmani, M.A.; Harbi, J.A.L.T.; Rsheed, A.M.B.; Alrasheedy, A.A.; ALMadani, W.; ALJuraisi, F.; AlOtaibi, A.F.; AlHarbi, M.; AlAbood, A.F.; Alshaikh, A.A.I. The impact of telemedicine on patients with uncontrolled type 2 diabetes mellitus during the COVID-19 pandemic in Saudi Arabia: Findings and implications. J. Telemed. Telecare 2021. [Google Scholar] [CrossRef]
- Tolone, S.; Gambardella, C.; Brusciano, L.; del Genio, G.; Lucido, F.S.; Docimo, L. Telephonic triage before surgical ward admission and telemedicine during COVID-19 outbreak in Italy. Effective and easy procedures to reduce in-hospital positivity. Int. J. Surg. 2020, 78, 123. [Google Scholar] [CrossRef]
- Difficulty Breathing in a Face Mask? Advice for Asthma and Lung Disease. Available online: https://creakyjoints.org/living-with-arthritis/coronavirus/managing-symptoms/difficulty-breathing-face-mask-asthma-lung-disease/ (accessed on 1 September 2021).
- AAAAI|American Academy of Allergy, Asthma & Immunology. Available online: https://www.aaaai.org/ (accessed on 1 September 2021).
- Latkin, C.A.; Dayton, L.; Yi, G.; Colon, B.; Kong, X. Mask usage, social distancing, racial, and gender correlates of COVID-19 vaccine intentions among adults in the US. PLoS ONE 2021, 16, e0246970. [Google Scholar] [CrossRef]
- Su, Z.; Wen, J.; McDonnell, D.; Goh, E.; Li, X.; Šegalo, S.; Ahmad, J.; Cheshmehzangi, A.; Xiang, Y.-T. Vaccines are not yet a silver bullet: The imperative of continued communication about the importance of COVID-19 safety measures. Brain Behav. Immun.-Health 2021, 12, 100204. [Google Scholar] [CrossRef] [PubMed]
- SARS-CoV-2 Variant Classifications and Definitions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-info.html (accessed on 1 September 2021).




{kind=link}
{kind=link}
{kind=link}
| Feature (Variable) | Statistics |
|---|---|
| Gender | |
| Female | 290 (58.0%) |
| Male | 210 (42.0%) |
| Age | |
| 60–64 | 141 (28.2%) |
| 65–69 | 128 (25.6%) |
| 70 and more | 231 (46.2%) |
| Place of residence | |
| Village | 110 (22.0%) |
| Town, less than 20,000 inhabitants | 56 (11.2%) |
| Town, between 20,000 to 100,000 inhabitants | 136 (27.2%) |
| Town, between 100,000 to 200,000 inhabitants | 62 (12.4%) |
| Town, between 200,000 to 400,000 inhabitants | 39 (7.8%) |
| Town, more than 400,000 inhabitants | 97 (19.4%) |
| Housing situation | |
| Lives alone | 108 (21.6%) |
| Lives with partner | 202 (40.4%) |
| Lives with partner and children | 117 (23.4%) |
| Lives alone with children | 35 (7.0%) |
| Lives with family | 29 (5.8%) |
| Other situation | 9 (1.8%) |
| Education | |
| Primary | 8 (1.6%) |
| Vocational | 105 (21.0%) |
| Secondary | 245 (49.0%) |
| Higher | 142 (28.4%) |
| Body mass (kg) | |
| M ± SD | 78.5 ± 15.7 |
| Me (Q1–Q3) | 76 (67–88) |
| Min–Max | 48–140 |
| Body height (cm) | |
| M ± SD | 169 ± 9 |
| Me (Q1–Q3) | 168 (163–175) |
| Min–Max | 141–210 |
| BMI (kg/m2) | |
| M ± SD | 27.4 ± 4.6 |
| Me (Q1–Q3) | 27 (24–30) |
| Min–Max | 19–46 |
| Household income per person per month | |
| Less than 500 PLN | 5 (1.0%) |
| 501–1000 PLN | 24 (4.8%) |
| 1001–2000 PLN | 188 (37.6%) |
| 2001–3000 PLN | 158 (31.6%) |
| More than 3000 PLN | 110 (2.0%) |
| Refusal to answer | 15 (3.0%) |
| Chronic diseases | |
| Coronary Heart Disease | 63 (12.6%) |
| Diabetes Mellitus | 74 (14.8%) |
| Asthma | 43 (8.6%) |
| COPD | 33 (6.6%) |
| Heart Failure | 71 (14.2%) |
| Kidney Failure | 20 (4.0%) |
| Gastroesophageal Reflux Disease | 68 (13.6%) |
| Was vaccinated against influenza in 2019 | 62 (12.4%) |
| Was vaccinated against influenza in 2020 | 51 (10.2%) |
| Avoids vaccination because of possible complications | 164 (32.8%) |
| Wants to be vaccinated against influenza but was unable due to lack of availability of vaccines | 104 (20.8%) |
| The GP doctor recommended vaccination against influenza and pneumococci | 81 (16.2%) |
| Number of drugs taken | |
| 1 to 3 | 301 (60.2%) |
| 4 to 6 | 151 (30.2%) |
| 7 to 10 | 40 (8.0%) |
| More than 10 | 8 (1.6%) |
| Cardiac drugs | 132 (26.4%) |
| Antihypertensive drugs | 255 (51.0%) |
| Diuretics | 78 (15.6%) |
| Analgesics | 230 (46.0%) |
| Digestive ailments drugs | 131 (26.2%) |
| Anticoagulants | 87 (17.4%) |
| Antidepressants | 78 (15.6%) |
| Nootropics | 54 (10.8%) |
| All drugs are prescribed by the same doctor | 352 (70.4%) |
| How many different doctors have prescribed your medications? | n = 148 |
| 2 | 82 (55.4%) |
| 3 | 52 (35.1%) |
| 4 and more | 14 (9.4%) |
| Informs the GP about all new medications | 391 (78.2%) |
| Buys drugs and/or supplements without a prescription | 378 (75.6%) |
| Analgesics | 305 (61.0%) |
| For heartburn | 132 (26.4%) |
| Herbal | 155 (31.0%) |
| Vitamins (C, B, D) | 345 (69.0%) |
| Other | 96 (19.2%) |
| Activities of Daily Living (ADL) | |
| M ± SD | 5.9 ± 0.4 |
| Me (Q1–Q3) | 6 (6–6) |
| Min–Max | 2–6 |
| Fit people (5–6 pts.) | 493 (98.6%) |
| Moderately disabled people (3–4 pts.) | 6 (1.2%) |
| Disabled people (0–2 pts.) | 1 (0.2%) |
| The Lawton Instrumental Activities of Daily Living (IADL) | |
| M ± SD | 22.9 ± 2.3 |
| Me (Q1–Q3) | 24 (23–24) |
| Min–Max | 11–24 |
| Abbreviated Mental Test Score (AMTS) | |
| M ± SD | 9.1 ± 1.0 |
| Me (Q1–Q3) | 9 (9–10) |
| Min–Max | 5–10 |
| Normal condition (7–10 pts.) | 9.1 ± 1.0 |
| Moderate disorder (4–6 pts.) | 9 (9–10) |
| Geriatric depression scale (GDS-15) | |
| M ± SD | 4.8 ± 4.0 |
| Me (Q1–Q3) | 4 (2–8) |
| Min–Max | 0–15 |
| Lack of depression (0–5 pts.) | 324 (64.8%) |
| Depression (6–15 pts.) | 176 (35.2%) |
| Gastric Anxiety Scale (GAS-10) | |
| M ± SD | 7.2 ± 4.6 |
| Me (Q1–Q3) | 6 (4–10) |
| Min–Max | 0–25 |
| Lubben Social Network Scale (LSNS-6) | |
| M ± SD | 14.2 ± 5.9 |
| Me (Q1–Q3) | 15 (10–18) |
| Min–Max | 0–30 |
| Social loneliness scale (Gierveld Scale) | |
| M ± SD | 13.1 ± 1.8 |
| Me (Q1–Q3) | 13 (12–14) |
| Min–Max | 6–18 |
| Mini Nutritional Assessment (MNA) | |
| M ± SD | 12.8 ± 1.5 |
| Me (Q1–Q3) | 13 (12–14) |
| Min–Max | 6–14 |
| Proper nutritional status (12–14 pts.) | 418 (83.6%) |
| The danger of malnutrition (8–11 pts.) | 78 (15.6%) |
| Malnutrition (0–7 pts.) | 4 (0.8%) |
| Questionnaire Question, n (%) | Statistics |
|---|---|
| 1. Have you limited your professional activity due to the fear of COVID-19 infection? (Yes = 1 pts., No = 0 pts.) | 133 (26.6%) |
| 2. Have you limited your social activities (family meetings, family and cultural events, meetings with friends) due to the fear of COVID-19 infection? (Yes = 1 pts., No = 0 pts.) | 381 (76.2%) |
| 3. Have you limited your recreational activities (walking, cycling, Nordic walking, swimming, etc.) due to the fear of COVID-19 infection? (Yes = 1 pts., No = 0 pts.) | 277 (55.4%) |
| 4. Have you limited shopping due to the fear of COVID-19 infection? (Yes = 1 pts., No = 0 pts.) | 162 (32.4%) |
| If yes, how did you supply yourself with food? | n = 162 |
| Through internet orders | 17 (10.5%) |
| With the help of family | 98 (60.5%) |
| With the help of neighbors | 8 (4.9%) |
| I ate less | 39 (24.1%) |
| 5. Did you cancel your planned hospitalization due to the fear of COVID-19 infection? (Yes = 1 pts., No = 0 pts.) | 50 (10.0%) |
| 6. Have you resigned to report to the Emergency Room due to the sudden deterioration of your health due to the fear of COVID-19 infection? (Yes = 1 pts., No = 0 pts.) | 32 (6.4%) |
| Total points: | |
| M ± SD | 2.1 ± 1.4 |
| Me (Q1–Q3) | 2 (1–3) |
| Min–Max | 0–6 |
| Feature (Variable) | b | p | β | p | OR (95% CI) |
|---|---|---|---|---|---|
| Coronary Heart Disease | 1.274 | <0.001 | - | >0.05 | - |
| Asthma | 0.988 | 0.016 | - | >0.05 | - |
| COPD | 2.022 | <0.001 | - | >0.05 | - |
| Heart Failure | 1.546 | <0.001 | - | >0.05 | - |
| Was vaccinated against influenza in 2019 | 1.181 | 0.001 | 1.099 | 0.003 | 3.00 (1.46–6.16) |
| Was vaccinated against influenza in 2020 | 1.062 | 0.005 | - | >0.05 | - |
| The GP doctor recommended vaccination against influenza and pneumococci | 1.447 | <0.001 | - | >0.05 | - |
| Number of drugs currently taken | 0.764 | <0.001 | 0.652 | 0.001 | 1.92 (1.33–2.78) |
| Cardiac drugs | 1.073 | <0.001 | - | >0.05 | - |
| Nootropics | 0.982 | 0.009 | - | >0.05 | - |
| The number of different doctors prescribing currently taken drugs | 0.567 | 0.023 | - | >0.05 | - |
| The Lawton Instrumental Activities of Daily Living (IADL) | 0.189 | <0.001 | −0.138 | 0.007 | 0.87 (0.79–0.96) |
| Gastric Anxiety Scale (GAS-10) | 0.089 | 0.003 | - | >0.05 | - |
| Lubben Social Network Scale (LSNS-6) | 0.069 | 0.008 | - | >0.05 | - |
| Mini Nutritional Assessment (MNA) | 0.311 | <0.001 | - | >0.05 | - |
| Feature (Variable) | b | p | β | p | OR (95% CI) |
|---|---|---|---|---|---|
| Coronary heart disease | 1.099 | 0.009 | - | >0.05 | - |
| COPD | 1.980 | <0.001 | 1.753 | <0.001 | 5.77 (2.16–15.4) |
| Heart Failure | 1.109 | 0.006 | - | >0.05 | - |
| The GP doctor recommended vaccination against influenza and pneumococci | 0.933 | 0.020 | - | >0.05 | - |
| Number of drugs currently taken | 0.528 | 0.015 | - | >0.05 | - |
| Cardiac drugs | 0.973 | 0.009 | - | >0.05 | - |
| The Lawton Instrumental Activities of Daily Living (IADL) | −0.202 | <0.001 | - | >0.05 | - |
| Depression assessment (GDS-15) | 0.197 | <0.001 | - | >0.05 | - |
| Gastric Anxiety Scale (GAS-10) | 0.137 | <0.001 | - | >0.05 | - |
| Lubben Social Network Scale (LSNS-6) | −0.118 | <0.001 | −0.094 | 0.014 | 0.91 (0.84–0.98) |
| Mini Nutritional Assessment (MNA) | −0.602 | <0.001 | −0.553 | <0.001 | 0.58 (0.47–0.71) |
| Feature (Variable) | b | p | β | p | OR (95% CI) |
|---|---|---|---|---|---|
| Asthma | 1.269 | <0.001 | 1.025 | 0.003 | 2.79 (1.40–5.54) |
| COPD | 1.005 | 0.006 | - | >0.05 | - |
| Heart failure | 0.640 | 0.013 | - | >0.05 | - |
| Avoiding vaccination because of possible complications | 0.702 | <0.001 | 0.692 | 0.001 | 2.00 (1.33–2.99) |
| Willingness to be vaccinated against influenza, but it is difficult because there is no vaccine in pharmacies | −0.645 | 0.010 | - | >0.05 | - |
| Cardiac drugs | 0.445 | 0.033 | - | >0.05 | - |
| Painkillers | 0.460 | 0.015 | - | >0.05 | - |
| All medicines prescribed by the same doctor | −0.435 | 0.031 | - | >0.05 | - |
| The Lawton Instrumental Activities of Daily Living (IADL) | −0.124 | 0.002 | −0.091 | 0.033 | 0.91 (0.84–0.99) |
| Depression assessment (GDS-15) | 0.099 | <0.001 | 0.071 | 0.006 | 1.07 (1.02–1.13) |
| Gastric Anxiety Scale (GAS-10) | 0.083 | <0.001 | - | >0.05 | - |
| Lubben Social Network Scale (LSNS-6) | −0.196 | <0.001 | −0.150 | 0.009 | 0.86 (0.77–0.96) |
| Status assessment nutrition (MNA) | −0.125 | 0.046 | - | >0.05 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agrawal, S.; Makuch, S.; Dróżdż, M.; Strzelec, B.; Sobieszczańska, M.; Mazur, G. The Impact of the COVID-19 Emergency on Life Activities and Delivery of Healthcare Services in the Elderly Population. J. Clin. Med. 2021, 10, 4089. https://doi.org/10.3390/jcm10184089
Agrawal S, Makuch S, Dróżdż M, Strzelec B, Sobieszczańska M, Mazur G. The Impact of the COVID-19 Emergency on Life Activities and Delivery of Healthcare Services in the Elderly Population. Journal of Clinical Medicine. 2021; 10(18):4089. https://doi.org/10.3390/jcm10184089
Chicago/Turabian StyleAgrawal, Siddarth, Sebastian Makuch, Mateusz Dróżdż, Bartłomiej Strzelec, Małgorzata Sobieszczańska, and Grzegorz Mazur. 2021. "The Impact of the COVID-19 Emergency on Life Activities and Delivery of Healthcare Services in the Elderly Population" Journal of Clinical Medicine 10, no. 18: 4089. https://doi.org/10.3390/jcm10184089