
The Role of Very Low Calorie Ketogenic Diet in Sympathetic Activation through Cortisol Secretion in Male Obese Population

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects, and Anthropometric and Biochemical Measurements
2.2. Study Protocol
2.3. Diet Protocol
2.4. Hormonal Secretion Assay
2.5. Galvanic Skin Response
2.6. Applied Mathematics Analysis
3. Results
3.1. Anthropometric and Biochemical Characteristics of VLCKD Obese Patients
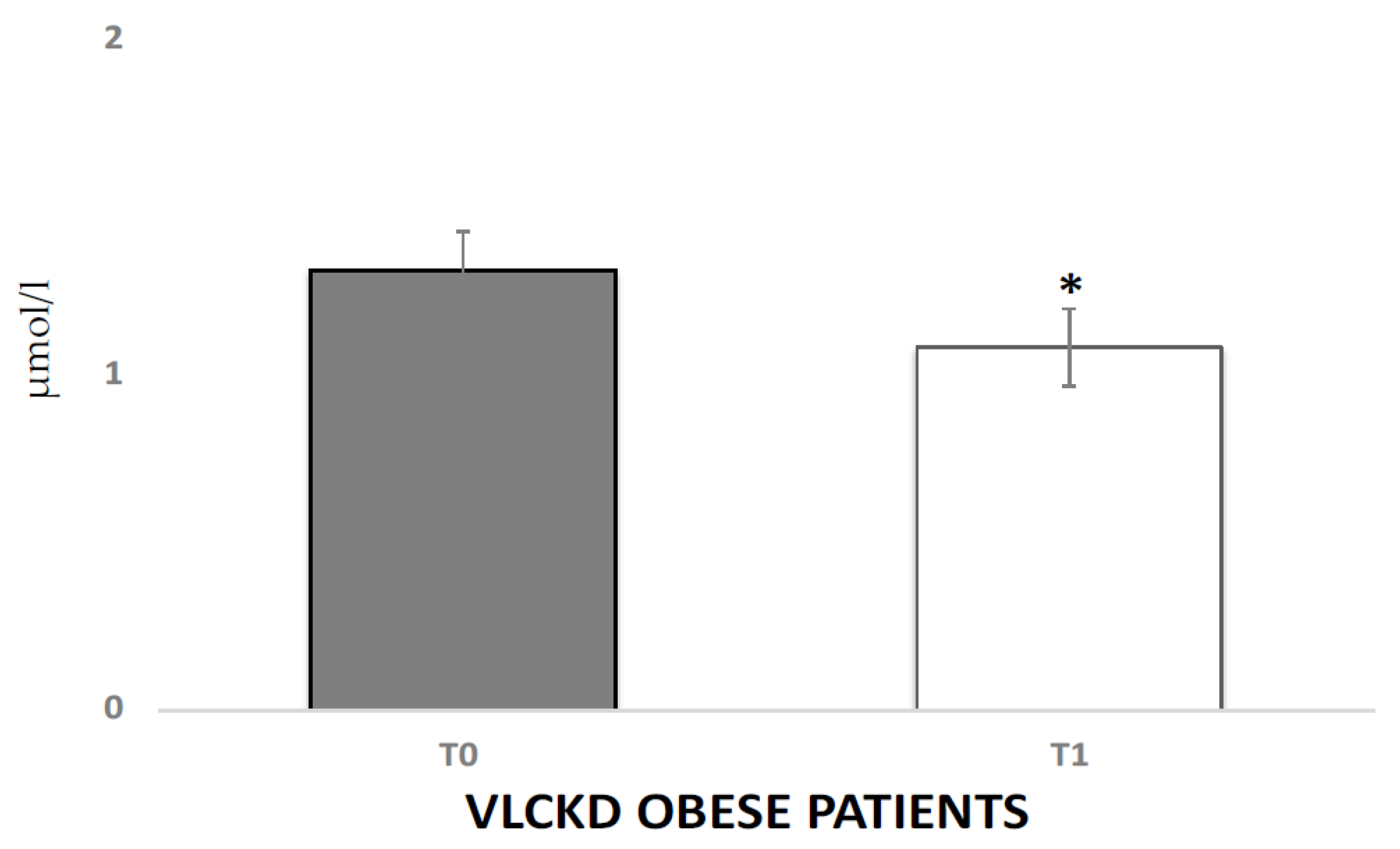
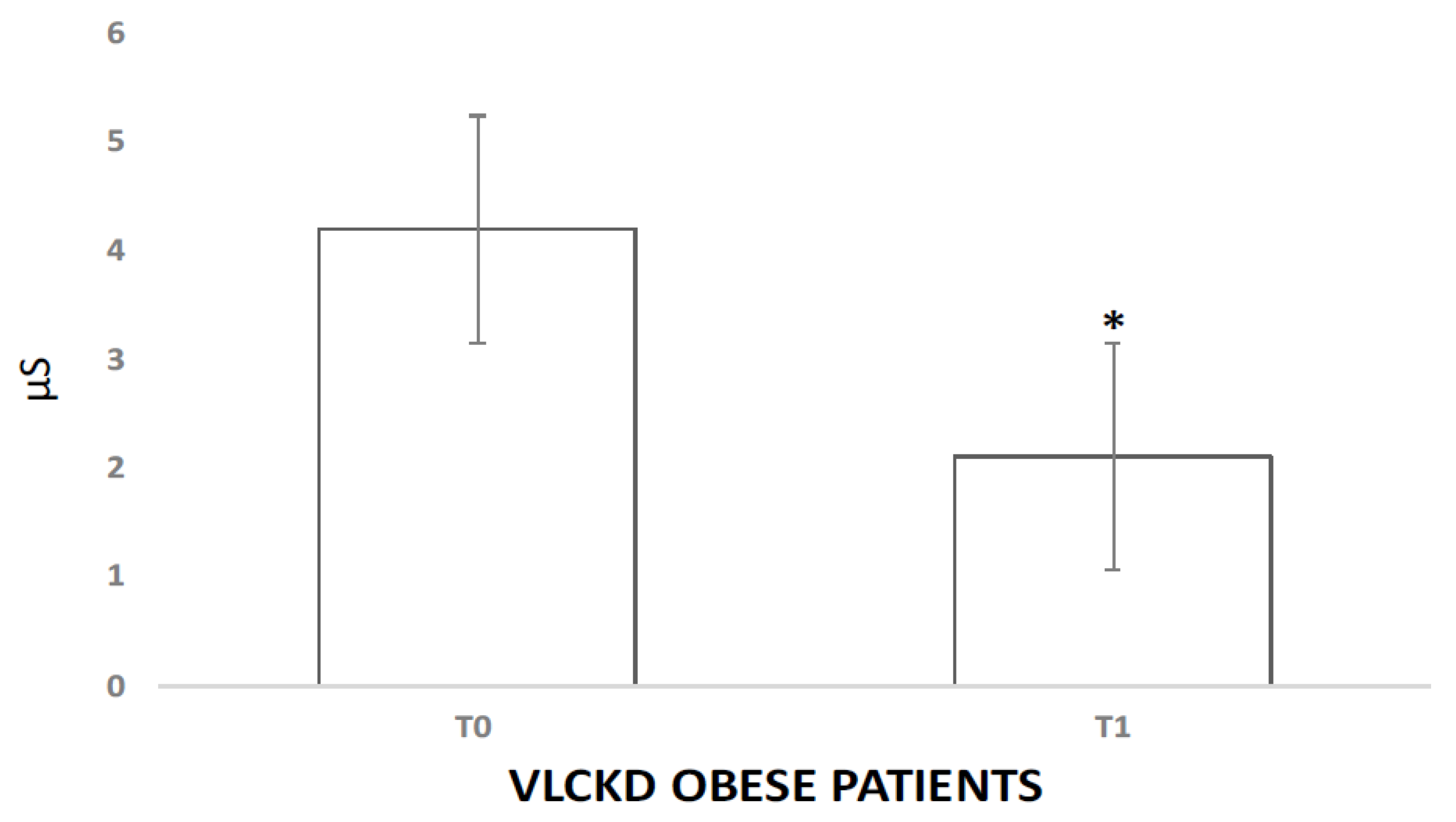
3.2. Physiological Responses to VLCKD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kiessl, G.R.R.; Laessle, R.G. Stress inhibits PYY secretion in obese and normal weight women. Eat. Weight. Disord.-Stud. Anorexia Bulim. Obes. 2016, 21, 245–249. [Google Scholar] [CrossRef]
- Orban, G.; Bombardi, C.; Marino Gammazza, A.; Colangeli, R.; Pierucci, M.; Pomara, C.; Pessia, M.; Bucchieri, F.; Arcangelo, B.; Smolders, I.; et al. Role(s) of the 5-HT2C Receptor in the Development of Maximal Dentate Activation in the Hippocampus of Anesthetized Rats. CNS Neurosci. Ther. 2014, 20, 651–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrowski, K.; Wintermann, G.B.; Joraschky, P.; Päßler, S. Chewing after stress: Psychosocial stress influences chewing fre-quency, chewing efficacy, and appetite. Psychoneuroendocrinology 2014, 48, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Schiavone, S.; Neri, M.; Trabace, L.; Turillazzi, E. The NADPH oxidase NOX2 mediates loss of parvalbumin interneurons in traumatic brain injury: Human autoptic immunohistochemical evidence. Sci. Rep. 2017, 7, 8752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messina, G.; Chieffi, S.; Viggiano, A.; Tafuri, D.; Cibelli, G.; Valenzano, A.; Triggiani, A.I.; Messina, A.; De Luca, V.; Monda, M. Parachute jumping induces more sympathetic activation than cortisol secretion in first-time parachutists. Asian J. Sports Med. 2016, 7, 26841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herhaus, B.; Päßler, S.; Petrowski, K. Stress-related laboratory eating behavior in adults with obesity and healthy weight. Physiol. Behav. 2018, 196, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Masih, T.; Dimmock, J.A.; Epel, E.S.; Guelfi, K.J. Stress-induced eating and the relaxation response as a potential antidote: A review and hypothesis. Appetite 2017, 118, 136–143. [Google Scholar] [CrossRef]
- Turillazzi, E.; Baroldi, G.; Silver, M.D.; Parolini, M.; Pomara, C.; Fineschi, V. A systematic study of a myocardial lesion: Colliquative myocytolysis. Int. J. Cardiol. 2005, 104, 152–157. [Google Scholar] [CrossRef]
- Appelhans, B.M.; Pagoto, S.L.; Peters, E.N.; Spring, B.J. HPA axis response to stress predicts short-term snack intake in obese women. Appetite 2010, 54, 217–220. [Google Scholar] [CrossRef] [Green Version]
- Buren, J.; Bergstrom, S.A.; Loh, E.; Soderstrom, I.; Olsson, T.; Mattsson, C. Hippocampal 11beta-hydroxysteroid dehydrogenase type 1 messenger ribonucleic acid expression has a diurnal variability that is lost in the obese Zucker rat. Endocrinology 2007, 148, 2716–2722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steptoe, A.; Kunz-Ebrecht, S.R.; Brydon, L.; Wardle, J. Central adiposity and cortisol responses to waking in middle-aged men and women. Int. J. Obes. 2004, 28, 1168–1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, S.B.; Rubino, D.; Sinaii, N.; Ramsey, S.; Nieman, L.K. Cortisol, obesity, and the metabolic syndrome: A cross-sectional study of obese subjects and review of the literature. Obesity 2013, 21, E105–E117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Valk, E.S.; Savas, M.; van Rossum, E.F.C. Stress and obesity: Are there more susceptible individuals? Curr. Obes. Rep. 2018, 7, 193–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fardet, L.; Fève, B. Systemic Glucocorticoid Therapy: A Review of its Metabolic and Cardiovascular Adverse Events. Drugs 2014, 74, 1731–1745. [Google Scholar] [CrossRef]
- Stalder, T.; Steudte-Schmiedgen, S.; Alexander, N.; Klucken, T.; Vater, A.; Wichmann, S.; Kirschbaum, C.; Miller, R. Stress-related and basic de-terminants of hair cortisol in humans: A meta-analysis. Psychoneuroendocrinology 2017, 77, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Noppe, G.; Van Den Akker, E.L.T.; De Rijke, Y.B.; Koper, J.W.; Jaddoe, V.W.; Van Rossum, E.F.C. Long-term glucocorticoid concentrations as a risk factor for childhood obesity and adverse body-fat distribution. Int. J. Obes. 2016, 40, 1503–1509. [Google Scholar] [CrossRef]
- Chu, L.; Sheng, K.; Liu, P.; Ye, K.; Wang, Y.; Li, C.; Kang, X.; Song, Y. Increased Cortisol and Cortisone Levels in Overweight Children. Med. Sci. Monit. Basic Res. 2017, 23, 25–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boison, D. New insights into the mechanisms of the ketogenic diet. Curr. Opin. Neurol. 2017, 30, 187–192. [Google Scholar] [CrossRef] [Green Version]
- Adam-Perrot, A.; Clifton, P.; Brouns, F. Low-carbohydrate diets: Nutritional and physiological aspects. Obes. Rev. 2006, 7, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Salminen, A.; Kaarniranta, K.; Kauppinen, A. Crosstalk between Oxidative Stress and SIRT1: Impact on the Aging Process. Int. J. Mol. Sci. 2013, 14, 3834. [Google Scholar] [CrossRef] [Green Version]
- Valenzano, A.; Polito, R.; Trimigno, V.; Di Palma, A.; Moscatelli, F.; Corso, G.; Sessa, F.; Salerno, M.; Montana, A.; Di Nunno, N.; et al. Effects of very low calorie ketogenic diet on the orexinergic system, visceral adipose tissue, and ROS production. Antioxidants 2019, 8, 643. [Google Scholar] [CrossRef] [Green Version]
- Monda, V.; Polito, R.; Lovino, A.; Finaldi, A.; Valenzano, A.; Nigro, E.; Corso, G.; Sessa, F.; Asmundo, A.; Di Nunno, N.; et al. Short-term physiological effects of a very low-calorie ketogenic diet: Effects on adiponectin levels and inflammatory states. Int. J. Mol. Sci. 2020, 21, 3228. [Google Scholar] [CrossRef] [PubMed]
- Rask, E.; Olsson, T.; Soderberg, S.; Andrew, R.; Livingstone, D.E.; Johnson, O.; Walker, B.R. Tissue-specific dysregulation of cortisol metabolism in human obesity. J. Clin. Endocrinol. Metab. 2001, 86, 1418–1421. [Google Scholar] [CrossRef]
- Pasquali, R.; Vicennati, V.; Cacciari, M.; Pagotto, U. The Hypothalamic-Pituitary-Adrenal Axis Activity in Obesity and the Metabolic Syndrome. Ann.-N. Y. Acad. Sci. 2006, 1083, 111–128. [Google Scholar] [CrossRef] [PubMed]
- Messina, A.; Bitetti, I.; Precenzano, F.; Iacono, D.; Messina, G.; Roccella, M.; Parisi, L.; Salerno, M.; Valenzano, A.; Maltese, A.; et al. Non-rapid eye movement sleep parasomnias and migraine: A role of orexinergic projections. Front. Neurol. 2018, 9, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Precenzano, F.; Ruberto, M.; Parisi, L.; Salerno, M.; Maltese, A.; Vagliano, C.; Messina, G.; Di Folco, A.; Di Filippo, T.; Roccella, M. Executive functioning in preschool children affected by autismspectrum dis-order: A pilot study. Acta Med. 2017, 33, 35. [Google Scholar]
- Viggiano, E.; Monda, V.; Messina, A.; Moscatelli, F.; Valenzano, A.; Tafuri, D.; Cibelli, G.; De Luca, B.; Messina, G.; Monda, M. Cortical spreading depression produces a neuroprotective effect activating mitochondrial uncoupling protein-5. Neuropsychiatr. Dis. Treat. 2016, 12, 1705–1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monda, M.; Viggiano, A.; Mondola, R.; Viggiano, E.; Messina, G.; Tafuri, D.; De Luca, V. Olanzapine blocks the sympathetic and hyperthermic reactions due to cerebral injection of orexin A. Peptides 2008, 29, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Viggiano, A.; Nicodemo, U.; Viggiano, E.; Messina, G.; Viggiano, A.; Monda, M.; De Luca, B. Mastication overload causes an increase in O2- production into the subnucleus oralis of the spinal trigeminal nucleus. Neuroscience 2010, 166, 416–421. [Google Scholar] [CrossRef]
- Viggiano, A.; Vicidomini, C.; Monda, M.; Carleo, D.; Carleo, R.; Messina, G.; Viggiano, A.; Viggiano, E.; De Luca, B. Fast and low-cost analysis of heart rate variability reveals vegetative alterations in noncomplicated diabetic patients. J. Diabetes its Complicat. 2009, 23, 119–123. [Google Scholar] [CrossRef]
- Esposito, M.; Serpe, F.P.; Diletti, G.; Messina, G.; Scortichini, G.; La Rocca, C.; Baldi, L.; Amorena, M.; Monda, M. Serum levels of polychlorinated dibenzo-p-dioxins, polychlorinated dibenzofurans and polychlorinated biphenyls in a population living in the Naples area, southern Italy. Chemosphere 2014, 94, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Wake, D.J.; Rask, E.; Livingstone, D.E.; Soderberg, S.; Olsson, T.; Walker, B.R. Local and systemic impact of transcriptional up-regulation of 11beta-hydroxy-steroid dehydrogenase type 1 in adipose tissue in human obesity. J. Clin. Endocrinol. Metab. 2003, 88, 3983–3988. [Google Scholar] [CrossRef]
- Yu, T.; Zhou, W.; Wu, S.; Liu, Q.; Li, X. Evidence for disruption of diurnal salivary cortisol rhythm in childhood obesity: Relationships with anthropometry, puberty and physical activity. BMC Pediatr. 2020, 20, 381. [Google Scholar] [CrossRef]
- Sessa, F.; Messina, G.; Russo, R.; Salerno, M.; Castruccio Castracani, C.; Distefano, A.; Li Volti, G.; Calogero, A.E.; Cannarella, R.; Mongioi’, L.M.; et al. Consequences on aging process and human wellness of generation of nitrogen and oxygen species during strenuous exercise. Aging Male 2020, 23, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Tirabassi, G.; Boscaro, M.; Arnaldi, G. Harmful effects of functional hypercortisolism: A working hypothesis. Endocrine 2014, 46, 370–386. [Google Scholar] [CrossRef] [PubMed]
- Dube, S.; Slama, M.Q.; Basu, A.; Rizza, R.A.; Basu, R. Glucocorticoid excess increases hepatic 11β-HSD-1 activity in humans: Implications in steroid-induced diabetes. J. Clin. Endocrinol. Metab. 2015, 100, 4155–4162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stimson, R.H.; Johnstone, A.M.; Homer, N.Z.M.; Wake, D.J.; Morton, N.M.; Andrew, R.; Lobley, G.E.; Walker, B.R. Dietary regulation of 11-HSD1 in humans. J. Clin. Endocrinol. Metab. 2007, 92, 4480–4484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herhaus, B.; Ullmann, E.; Chrousos, G.; Petrowski, K. High/low cortisol reactivity and food intake in people with obesity and healthy weight. Transl. Psychiatry 2020, 10, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertozzi, G.; Salerno, M.; Pomara, C.; Sessa, F. Neuropsychiatric and Behavioral Involvement in AAS Abusers. A Literature Review. Medicina 2019, 55, 396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monda, V.; Salerno, M.; Fiorenzo, M.; Villano, I.; Viggiano, A.; Sessa, F.; Triggiani, A.I.; Cibelli, G.; Valenzano, A.; Marsala, G.; et al. Role of Sex Hormones in the Control of Vegetative and Metabolic Functions of Middle-Aged Women. Front. Physiol. 2017, 8, 773. [Google Scholar] [CrossRef] [Green Version]
- Monda, V.; Salerno, M.; Sessa, F.; Bernardini, R.; Valenzano, A.; Marsala, G.; Zammit, C.; Avola, R.; Carotenuto, M.; Messina, G.; et al. Functional Changes of Orexinergic Reaction to Psychoactive Substances. Mol. Neurobiol. 2018, 55, 6362–6368. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| VLCKD Obese Subjects | |||
|---|---|---|---|
| T0 | T1 | p-Value | |
| Age | 57 ± 8 | ns | |
| Height (m) | 1.65 ± 0.2 | ns | |
| Weight (kg) | 90.73 ± 11 | 83.33 ± 12 | <0.05 |
| BMI (kg/m²) | 33 ± 4.5 | 30.5 ± 3.22 | <0.05 |
| Total cholesterol (mg/dL) | 220.13 ± 50.77 | 173.91 ± 32.93 | <0.05 |
| Triglycerides (mg/dL) | 126.54 ± 11 | 90.25 ± 14 | <0.05 |
| AST-GOT (U/L) | 22.17 ± 5.98 | 20.31 ± 4.7 | <0.05 |
| ALT-GPT (U/L) | 26.01 ± 14.89 | 24.06 ± 16.27 | <0.05 |
| Gamma GT (U/L) | 30 ± 8.8 | 15.31 ± 5.41 | <0.05 |
| Azotemia (mg/dL) | 36.7 ± 8.43 | 35.01 ± 5.16 | ns |
| Calcemia (mg/dL) | 9.7 ± 0.33 | 9.52 ± 0.35 | ns |
| Sodium (mmol/L) | 139.19 ± 2.48 | 139.18 ± 2 | ns |
| CRP (mg/mL) | 0.89 ± 0.1 | 0.48 ± 0.07 | <0.05 |
| Adiponectin (μg/mL) | 9.96 ± 0.7 | 23.56 ± 2.33 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polito, R.; Messina, G.; Valenzano, A.; Scarinci, A.; Villano, I.; Monda, M.; Cibelli, G.; Porro, C.; Pisanelli, D.; Monda, V.; et al. The Role of Very Low Calorie Ketogenic Diet in Sympathetic Activation through Cortisol Secretion in Male Obese Population. J. Clin. Med. 2021, 10, 4230. https://doi.org/10.3390/jcm10184230
Polito R, Messina G, Valenzano A, Scarinci A, Villano I, Monda M, Cibelli G, Porro C, Pisanelli D, Monda V, et al. The Role of Very Low Calorie Ketogenic Diet in Sympathetic Activation through Cortisol Secretion in Male Obese Population. Journal of Clinical Medicine. 2021; 10(18):4230. https://doi.org/10.3390/jcm10184230
Chicago/Turabian StylePolito, Rita, Giovanni Messina, Anna Valenzano, Alessia Scarinci, Ines Villano, Marcellino Monda, Giuseppe Cibelli, Chiara Porro, Daniela Pisanelli, Vincenzo Monda, and et al. 2021. "The Role of Very Low Calorie Ketogenic Diet in Sympathetic Activation through Cortisol Secretion in Male Obese Population" Journal of Clinical Medicine 10, no. 18: 4230. https://doi.org/10.3390/jcm10184230