
Non-Invasive Risk Prediction Based on Right Ventricular Function in Patients with Pulmonary Arterial Hypertension

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Echocardiography
2.3. Outcome
2.4. Statistical Methods
3. Results
3.1. Patient Characteristics
3.2. Echocardiographic Parameters
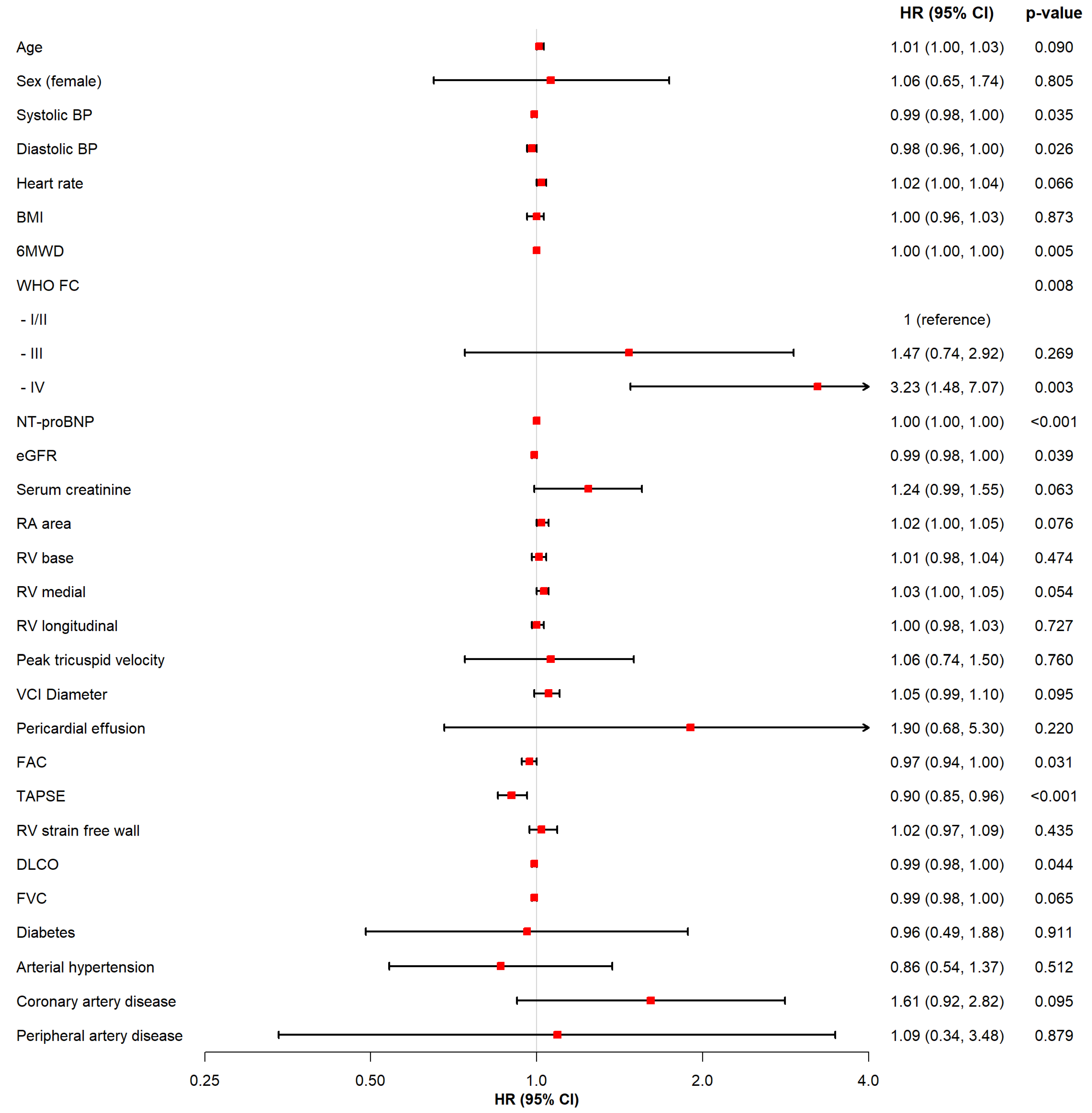
3.3. Regression Analysis
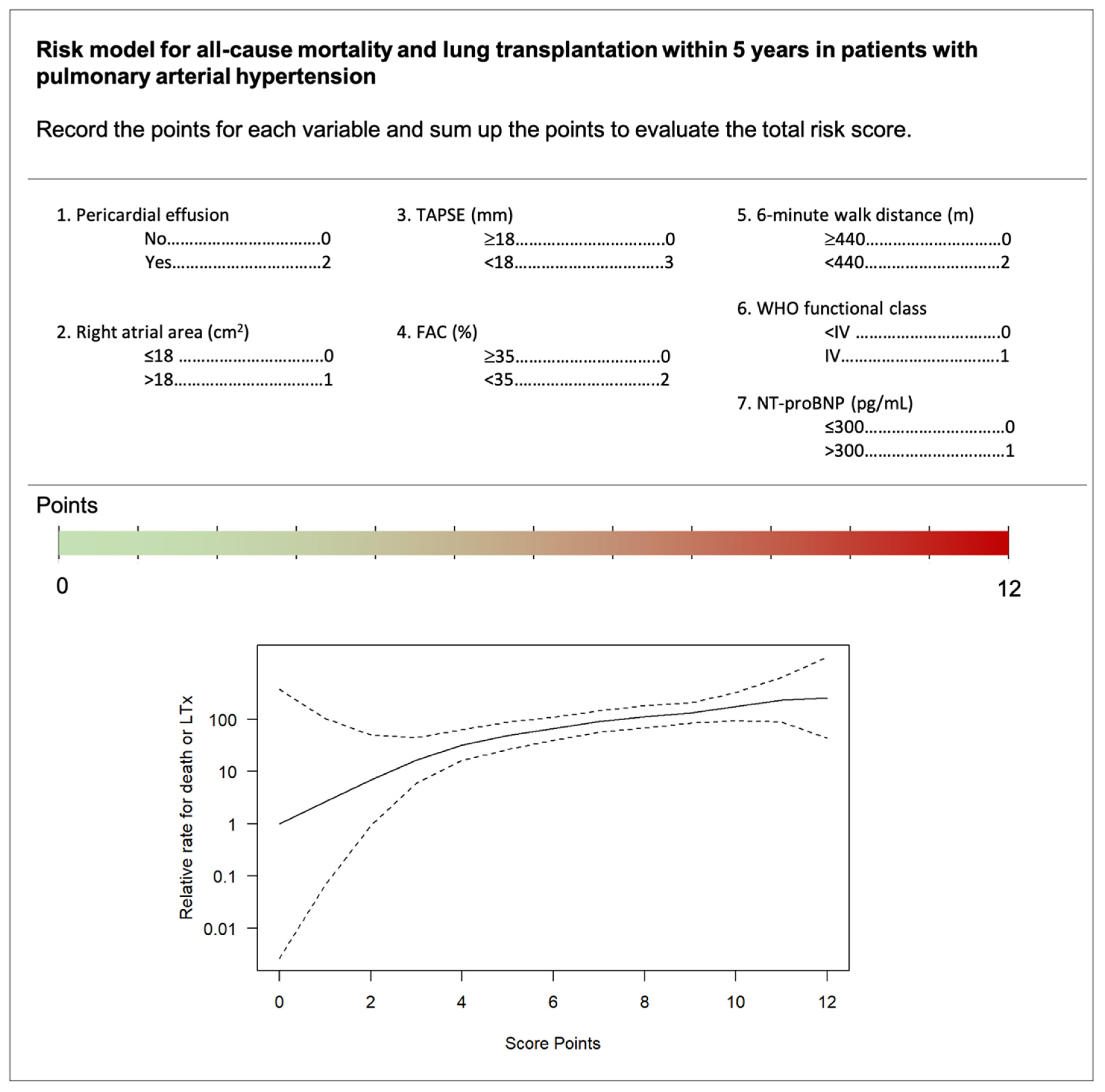
3.4. Non-Invasive Risk Score
4. Discussion
4.1. Cohort and Clinical Risk Parameters
4.2. Echocardiographic Parameters
4.3. Point-Based Risk Score
4.4. Strengths and Limitations
4.5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galiè, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [PubMed]
- Humbert, M.; Sitbon, O.; Simonneau, G. Treatment of pulmonary arterial hypertension. N. Engl. J. Med. 2004, 351, 1425–1436. [Google Scholar] [CrossRef]
- Galiè, N.; Palazzini, M.; Manes, A. Pulmonary arterial hypertension: From the kingdom of the near-dead to multiple clinical trial meta-analyses. Eur. Heart J. 2010, 31, 2080–2086. [Google Scholar] [CrossRef] [PubMed]
- D’Alonzo, G.E.; Barst, R.J.; Ayres, S.M.; Bergofsky, E.H.; Brundage, B.H.; Detre, K.M.; Fishman, A.P.; Goldring, R.M.; Groves, B.M.; Kernis, J.T.; et al. Survival in Patients with Primary Pulmonary Hypertension. Results from a national prospective registry. Ann. Intern. Med. 1991, 115, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Benza, R.L.; Miller, D.; Barst, R.J.; Badesch, D.B.; Frost, A.E.; McGoon, M.D. An Evaluation of Long-term Survival from Time of Diagnosis in Pulmonary Arterial Hypertension from the REVEAL Registry. Chest 2012, 142, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Benza, R.L.; Gomberg-Maitland, M.; Miller, D.; Frost, A.; Frantz, R.; Foreman, A.J.; Badesch, D.B.; McGoon, M.D. The REVEAL Registry Risk Score Calculator in Patients Newly Diagnosed With Pulmonary Arterial Hypertension. Chest 2012, 141, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Boucly, A.; Weatherald, J.; Savale, L.; Jais, X.; Cottin, V.; Prevot, G.; Picard, F.; de Groote, P.; Jevnikar, M.; Bergot, E.; et al. Risk assessment, prognosis and guideline implementation in pulmonary arterial hypertension. Eur. Respir. J. 2017, 50, 1700889. [Google Scholar] [CrossRef] [Green Version]
- Hoeper, M.M.; Kramer, T.; Pan, Z.; Eichstaedt, C.A.; Spiesshoefer, J.; Benjamin, N.; Olsson, K.M.; Meyer, K.; Vizza, C.D.; Vonk-Noordegraaf, A.; et al. Mortality in pulmonary arterial hypertension: Prediction by the 2015 European pulmonary hypertension guidelines risk stratification model. Eur. Respir. J. 2017, 50, 1700740. [Google Scholar] [CrossRef] [Green Version]
- Kylhammar, D.; Kjellström, B.; Hjalmarsson, C.; Jansson, K.; Nisell, M.; Söderberg, S.; Wikström, G.; Rådegran, G. A comprehensive risk stratification at early follow-up determines prognosis in pulmonary arterial hypertension. Eur. Heart J. 2017, 39, 4175–4181. [Google Scholar] [CrossRef]
- Chin, K.; Kim, N.H.S.; Rubin, L.J. The right ventricle in pulmonary hypertension. Coron. Artery Dis. 2005, 16, 13–18. [Google Scholar] [CrossRef]
- Humbert, M.J.; Sitbon, O.; Chaouat, A.; Bertocchi, M.; Habib, G.; Gressin, V.; Yaïci, A.; Weitzenblum, E.; Cordier, J.-F.; Chabot, F.; et al. Survival In Patients With Idiopathic, Familial, And Anorexigen-associated Pulmonary Arterial Hypertension In The Modern Management Era. Circulation 2010, 122, 156–163. [Google Scholar] [CrossRef] [Green Version]
- Ghio, S.; Klersy, C.; Magrini, G.; D’Armini, A.M.; Scelsi, L.; Raineri, C.; Pasotti, M.; Serio, A.; Campana, C.; Viganò, M. Prognostic relevance of the echocardiographic assessment of right ventricular function in patients with idiopathic pulmonary arterial hypertension. Int. J. Cardiol. 2010, 140, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Ghio, S.; Pica, S.; Klersy, C.; Guzzafame, E.; Scelsi, L.; Raineri, C.; Turco, A.; Schirinzi, S.; Visconti, L.O. Prognostic value of TAPSE after therapy optimisation in patients with pulmonary arterial hypertension is independent of the haemodynamic effects of therapy. Open Heart 2016, 3, e000408. [Google Scholar] [CrossRef] [Green Version]
- Forfia, P.R.; Fisher, M.R.; Mathai, S.C.; Housten-Harris, T.; Hemnes, A.R.; Borlaug, B.A.; Chamera, E.; Corretti, M.C.; Champion, H.C.; Abraham, T.P.; et al. Tricuspid Annular Displacement Predicts Survival in Pulmonary Hypertension. Am. J. Respir. Crit. Care Med. 2006, 174, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Ghio, S.; Mercurio, V.; Fortuni, F.; Forfia, P.R.; Gall, H.; Ghofrani, A.; Mathai, S.C.; Mazurek, J.A.; Mukherjee, M.; Richter, M.; et al. A comprehensive echocardiographic method for risk stratification in pulmonary arterial hypertension. Eur. Respir. J. 2020, 56, 2000513. [Google Scholar] [CrossRef]
- Raymond, R.J.; Hinderliter, A.L.; Willis, P.W.; Ralph, D.; Caldwell, E.J.; Williams, W.; A Ettinger, N.; Hill, N.S.; Summer, W.R.; de Boisblanc, B.; et al. Echocardiographic predictors of adverse outcomes in primary pulmonary hypertension. J. Am. Coll. Cardiol. 2002, 39, 1214–1219. [Google Scholar] [CrossRef] [Green Version]
- Bustamante-Labarta, M.; Perrone, S.; de la Fuente, R.L.; Stutzbach, P.; de la Hoz, R.P.; Torino, A.; Favaloro, R. Right atrial size and tricuspid regurgitation severity predict mortality or transplantation in primary pulmonary hypertension. J. Am. Soc. Echocardiogr. 2002, 15, 1160–1164. [Google Scholar] [CrossRef] [Green Version]
- Haeck, M.L.; Scherptong, R.W.; Marsan, N.A.; Holman, E.R.; Schalij, M.J.; Bax, J.J.; Vliegen, H.W.; Delgado, V. Prognostic Value of Right Ventricular Longitudinal Peak Systolic Strain in Patients With Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2012, 5, 628–636. [Google Scholar] [CrossRef] [Green Version]
- Fine, N.M.; Chen, L.; Bastiansen, P.M.; Frantz, R.; Pellikka, P.A.; Oh, J.K.; Kane, G.C. Outcome Prediction by Quantitative Right Ventricular Function Assessment in 575 Subjects Evaluated for Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2013, 6, 711–721. [Google Scholar] [CrossRef] [Green Version]
- Farber, H.W.; Benza, R.L. Risk Assessment Tools in Pulmonary Arterial Hypertension. Prognosis for Prospective Trials? Am. J. Respir. Crit. Care Med. 2018, 197, 843–845. [Google Scholar] [CrossRef] [PubMed]
- Badagliacca, R.; Papa, S.; Matsubara, H.; Lang, I.M.; Poscia, R.; Manzi, G.; Vizza, C.D. The importance of right ventricular evaluation in risk assessment and therapeutic strategies: Raising the bar in pulmonary arterial hypertension. Int. J. Cardiol. 2020, 301, 183–189. [Google Scholar] [CrossRef]
- Rosenkranz, S.; Preston, I.R. Right heart catheterisation: Best practice and pitfalls in pulmonary hypertension. Eur. Respir. Rev. 2015, 24, 642–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voigt, J.-U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J.-Cardiovasc. Imaging 2014, 16, 1–11. [Google Scholar] [CrossRef]
- Lancellotti, P.; Cosyns, B. The EACVI Echo Handbook; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Quanjer, P.H.; Brazzale, D.J.; Boros, P.W.; Pretto, J.J. Implications of adopting the Global Lungs Initiative 2012 all-age reference equations for spirometry. Eur. Respir. J. 2013, 42, 1046–1054. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, L.M.; Massaro, J.M.; D’Agostino, R.B., Sr. Presentation of multivariate data for clinical use: The Framingham Study risk score functions. Stat. Med. 2004, 23, 1631–1660. [Google Scholar] [CrossRef]
- Eilers, P.H.C.; Marx, B.D. Flexible smoothing with B-splines and penalties. Stat. Sci. 1996, 11, 89–121. [Google Scholar] [CrossRef]
- Hoeper, M.M.; Simon, R.G.J. The changing landscape of pulmonary arterial hypertension and implications for patient care. Eur. Respir. Rev. 2014, 23, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Rothbard, N.; Agrawal, A.; Fischer, C.; Talwar, A.; Sahni, S. Pulmonary arterial hypertension in the elderly: Clinical perspectives. Cardiol. J. 2020, 27, 184–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montani, D.; Girerd, B.; Jaïs, X.; Laveneziana, P.; Lau, E.M.; Bouchachi, A.; Hascoët, S.; Günther, S.; Godinas, L.; Parent, F.; et al. Screening for pulmonary arterial hypertension in adults carrying a BMPR2 mutation. Eur. Respir. J. 2020, 58, 2004229. [Google Scholar] [CrossRef]
- Coghlan, J.G.; Denton, C.P.; Grünig, E.; Bonderman, D.; Distler, O.; Khanna, D.; Müller-Ladner, U.; E Pope, J.; Vonk, M.C.; Doelberg, M.; et al. Evidence-based detection of pulmonary arterial hypertension in systemic sclerosis: The DETECT study. Ann. Rheum. Dis. 2014, 73, 1340–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benza, R.L.; Gomberg-Maitland, M.; Elliott, C.G.; Farber, H.W.; Foreman, A.J.; Frost, A.E.; McGoon, M.D.; Pasta, D.J.; Selej, M.; Burger, C.D.; et al. Predicting Survival in Patients With Pulmonary Arterial Hypertension: The REVEAL Risk Score Calculator 2.0 and Comparison With ESC/ERS-Based Risk Assessment Strategies. Chest 2019, 156, 323–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, J.J.; Lau, E.M.; Lavender, M.; Benza, R.; Celermajer, D.S.; Collins, N.; Corrigan, C.; Dwyer, N.; Feenstra, J.; Horrigan, M.; et al. Retrospective Validation of the REVEAL 2.0 Risk Score With the Australian and New Zealand Pulmonary Hypertension Registry Cohort. Chest 2020, 157, 162–172. [Google Scholar] [CrossRef] [Green Version]
- Marra, A.M.; Halank, M.; Benjamin, N.; Bossone, E.; Cittadini, A.; Eichstaedt, C.A.; Egenlauf, B.; Harutyunova, S.; Fischer, C.; Gall, H.; et al. Right ventricular size and function under riociguat in pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension (the RIVER study). Respir. Res. 2018, 19, 258. [Google Scholar] [CrossRef]
- Kaul, S.; Tei, C.; Hopkins, J.M.; Shah, P.M. Assessment of right ventricular function using two-dimensional echocardiography. Am. Heart J. 1984, 107, 526–531. [Google Scholar] [CrossRef]
- Brierre, G.; Blot-Souletie, N.; Degano, B.; Têtu, L.; Bongard, V.; Carrié, D. New echocardiographic prognostic factors for mortality in pulmonary arterial hypertension. Eur. J. Echocardiogr. 2010, 11, 516–522. [Google Scholar] [CrossRef] [Green Version]
- Simonneau, G.; Galie, N.; Rubin, L.J.; Langleben, D.; Seeger, W.; Domenighetti, G.; Gibbs, S.; Lebrec, D.; Speich, R.; Beghetti, M.; et al. Clinical classification of pulmonary hypertension. J. Am. Coll. Cardiol. 2004, 43, S5–S12. [Google Scholar] [CrossRef]
- Simonneau, G.; Gatzoulis, M.A.; Adatia, I.; Celermajer, D.; Denton, C.; Ghofrani, A.; Sanchez, M.A.G.; Kumar, R.K.; Landzberg, M.; Machado, R.; et al. Updated Clinical Classification of Pulmonary Hypertension. J. Am. Coll. Cardiol. 2013, 62, D34–D41. [Google Scholar] [CrossRef] [Green Version]
- Hoette, S.; Creuzé, N.; Günther, S.; Montani, D.; Savale, L.; Jais, X.; Parent, F.; Sitbon, O.; Rochitte, C.E.; Simonneau, G.; et al. RV Fractional Area Change and TAPSE as Predictors of Severe Right Ventricular Dysfunction in Pulmonary Hypertension: A CMR Study. Lung 2018, 196, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, A.; Villarraga, H.R.; Frantz, R.; McGoon, M.D.; Hsiao, J.-F.; Maalouf, J.F.; Ammash, N.M.; McCully, R.B.; Miller, F.A.; Pellikka, P.A.; et al. Right Ventricular Strain for Prediction of Survival in Patients with Pulmonary Arterial Hypertension. Chest 2011, 139, 1299–1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marwick, T.H. Can we Justify the Cost of Echocardiography? Lessons from Outcomes Research. Eur. J. Echocardiogr. 2005, 6, 155–163. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| All (N = 254) | Females (N = 86) | Males (N = 168) | p-Value | |
|---|---|---|---|---|
| Clinical parameters | ||||
| Age (years) | 65.5 (49.9, 74.0) | 66.0 (55.9, 75.0) | 65.0 (48.0, 74.0) | 0.24 |
| Sex (females) No. (%) | 86 (33.9) | |||
| PAH etiology No. (%) | ||||
| Idopathic | 160 (63.7) | 57 (66.3) | 103 (62.4) | 0.64 |
| Heritable | 5 (2.0) | 1 (1.2) | 4 (2.4) | 0.84 |
| Drug/toxin induced | 2 (0.8) | 1 (1.2) | 1 (0.6) | 1.00 |
| Associated | 84 (33.5) | 27 (31.4) | 57 (34.5) | 0.72 |
| Systolic BP (mmHg) | 128.0 ± 22.8 | 127.2 ± 22.9 | 128.4 ± 22.7 | 0.70 |
| Diastolic BP (mmHg) | 75.5 ± 14.3 | 75.7 ± 15.9 | 75.3 ± 13.5 | 0.85 |
| Heart rate (bpm) | 77.3 ± 13.8 | 75.9 ± 13.0 | 78.1 ± 14.1 | 0.22 |
| BMI (kg/m2) | 27.3 ± 6.1 | 27.2 ± 5.0 | 27.4 ± 6.6 | 0.80 |
| WHO FC: I/II No. (%) | 54 (21.3) | 22 (25.6) | 32 (19.2) | 0.31 |
| WHO FC: III No. (%) | 162 (64.0) | 51 (59.3) | 111 (66.5) | 0.32 |
| WHO FC: IV No. (%) | 37 (14.6) | 13 (15.1) | 24 (14.4) | 1.00 |
| Functional and laboratory parameters | ||||
| 6MWD (m) | 269.2 ± 183.9 | 255.5 ± 203.4 | 276.2 ± 173.4 | 0.40 |
| 6MWD < 440 m No. (%) | 209 (84.3) | 67 (80.7) | 142 (86.1) | 0.37 |
| FVC (%) | 75.0 (58.0, 86.0) | 77.0 (59.4, 83.0) | 73.5 (58.0, 88.0) | 0.78 |
| DLCO (%) | 58.0 (38.9, 77.0) | 53.5 (31.0, 74.2) | 60.0 (42.4, 77.0) | 0.12 |
| DLCO < 40% No.(%) | 50 (25.8) | 23 (32.9) | 27 (21.8) | 0.13 |
| Laboratory parameter | ||||
| NT-proBNP (pg/mL) | 1570.0 (437.3, 4099.8) | 1732.0 (461.3, 4464.7) | 1509.0 (434.2, 3462.2) | 0.56 |
| NT-proBNP > 300 pg/mL No. (%) | 201 (80.1) | 67 (78.8) | 134 (80.7) | 0.85 |
| Serum creatinine (mg/dL) | 1.0 (0.8, 1.2) | 1.2 (1.0, 1.5) | 1.0 (0.8, 1.2) | <0.001 |
| eGFR (mL/min/1.73 m2) | 67.7 (47.3, 93.3) | 50.3 (36.5, 63.1) | 83.3 (61.4, 101.9) | <0.001 |
| eGFR < 60 mL/min/1.73 m2 No. (%) | 97 (39.0) | 60 (69.8) | 37 (22.7) | <0.001 |
| Medication | ||||
| PAH drugs ≥ 2 No. (%) | 73 (28.7) | 23 (26.7) | 50 (29.8) | 0.72 |
| Phosphodiestarase 5 inhibitor No. (%) | 136 (53.5) | 45 (52.3) | 91 (54.2) | 0.88 |
| Endothelin receptor antagonist No. (%) | 113 (44.5) | 38 (44.2) | 75 (44.6) | 1.00 |
| Prostacyclin agonist No. (%) | 31 (12.2) | 8 (9.3) | 23 (13.7) | 0.42 |
| Pre-existing diseases | ||||
| Arterial hypertension No. (%) | 112 (45.0) | 41 (47.7) | 71 (43.6) | 0.63 |
| Diabetes No. (%) | 41 (16.5) | 19 (22.1) | 22 (13.5) | 0.12 |
| Coronary artery disease No. (%) | 51 (20.5) | 26 (30.2) | 25 (15.3) | 0.009 |
| Peripheral artery disease No. (%) | 9 (3.6) | 4 (4.7) | 5 (3.1) | 0.78 |
| Echocardiographic Parameters | All (N = 254) | Females (N = 86) | Males (N = 168) | p-Value |
|---|---|---|---|---|
| RA area (cm2) | 24.0 (19.0, 29.0) | 26.0 (21.0, 31.3) | 23.0 (19.0, 29.0) | 0.049 |
| RA area > 18 cm2 No. (%) | 190 (79.5) | 67 (82.7) | 123 (77.8) | 0.48 |
| RV base (mm) | 46.5 (41.0, 52.0) | 49.0 (43.7, 54.0) | 45.0 (40.0, 51.0) | 0.003 |
| RV medial (mm) | 37.0 (30.0, 43.0) | 38.0 (30.4, 43.0) | 36.5 (30.0, 42.1) | 0.32 |
| RV longitudinal (mm) | 70.0 (64.0, 77.0) | 74.0 (68.0, 82.0) | 68.0 (61.0, 74.1) | <0.001 |
| Peak tricuspid velocity (m/s) | 4.0 (3.0, 4.0) | 4.0 (3.0, 4.0) | 4.0 (3.0, 4.0) | 0.28 |
| VCI diameter (mm) | 18.0 (15.0, 21.0) | 20.0 (17.0, 22.8) | 17.0 (14.0, 21.0) | 0.001 |
| Pericardial effusion No. (%) | 14 (5.8) | 5 (6.1) | 9 (5.7) | 1.00 |
| FAC (%) | 26.0 (20.0, 33.1) | 26.0 (19.4, 31.6) | 27.0 (20.0, 35.0) | 0.43 |
| FAC < 35 No. (%) | 159 (77.2) | 56 (82.4) | 103 (74.6) | 0.29 |
| TAPSE (mm) | 17.0 (14.0, 21.0) | 17.0 (14.0, 21.0) | 17.0 (14.0, 21.0) | 0.69 |
| TAPSE < 18 mm No. (%) | 124 (53.7) | 46 (57.5) | 78 (51.7) | 0.48 |
| RV strain free wall (%) | −14.0 (−18.0, −10.0) | −13.5 (−18.0, −10.0) | −14.0 (−17.3, −10.7) | 1.00 |
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| HR (95% CI) | HR per SD (95% CI) | p-Value | HR (95% CI) | HR per SD (95% CI) | p-Value | |
| WHO FC I/II | 1 (reference) | 1 (reference) | ||||
| WHO FC III | 1.01 (0.46, 2.23) | 1.00 (0.69, 1.46) | 0.983 | 0.91 (0.36, 2.28) | 0.96 (0.62, 1.47) | 0.836 |
| WHO FC IV | 1.74 (0.68, 4.43) | 1.21 (0.88, 1.68) | 0.244 | 1.54 (0.52, 4.58) | 1.16 (0.80, 1.69) | 0.437 |
| NT-proBNP > 300 pg/mL | 1.69 (0.77, 3.71) | 1.24 (0.90, 1.70) | 0.188 | 1.38 (0.59, 3.21) | 1.14 (0.80, 1.63) | 0.461 |
| 6MWD < 440 m | 2.08 (0.86, 5.02) | 1.31 (0.95, 1.82) | 0.103 | 1.77 (0.73, 4.31) | 1.24 (0.89, 1.73) | 0.210 |
| RA area > 18 cm2 | 1.68 (0.81, 3.48) | 1.23 (0.92, 1.66) | 0.160 | 1.33 (0.57, 3.10) | 1.13 (0.79, 1.60) | 0.508 |
| Pericardial effusion | 1.53 (0.54, 4.36) | 1.11 (0.86, 1.43) | 0.425 | 1.82 (0.63, 5.31) | 1.15 (0.90, 1.48) | 0.271 |
| TAPSE < 18 mm | 2.36 (1.28, 4.35) | 1.54 (1.13, 2.09) | 0.006 | |||
| FAC < 35% | 1.56 (0.67, 3.64) | 1.21 (0.84, 1.73) | 0.301 | |||
| N | 225 | 189 | ||||
| N events | 62 | 52 | ||||
| C-Index | 0.539 (0.446, 0.632) | 0.639 * (0.550, 0.729) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qaderi, V.; Weimann, J.; Harbaum, L.; Schrage, B.N.; Knappe, D.; Hennigs, J.K.; Sinning, C.; Schnabel, R.B.; Blankenberg, S.; Kirchhof, P.; et al. Non-Invasive Risk Prediction Based on Right Ventricular Function in Patients with Pulmonary Arterial Hypertension. J. Clin. Med. 2021, 10, 5130. https://doi.org/10.3390/jcm10215130
Qaderi V, Weimann J, Harbaum L, Schrage BN, Knappe D, Hennigs JK, Sinning C, Schnabel RB, Blankenberg S, Kirchhof P, et al. Non-Invasive Risk Prediction Based on Right Ventricular Function in Patients with Pulmonary Arterial Hypertension. Journal of Clinical Medicine. 2021; 10(21):5130. https://doi.org/10.3390/jcm10215130
Chicago/Turabian StyleQaderi, Vazhma, Jessica Weimann, Lars Harbaum, Benedikt N. Schrage, Dorit Knappe, Jan K. Hennigs, Christoph Sinning, Renate B. Schnabel, Stefan Blankenberg, Paulus Kirchhof, and et al. 2021. "Non-Invasive Risk Prediction Based on Right Ventricular Function in Patients with Pulmonary Arterial Hypertension" Journal of Clinical Medicine 10, no. 21: 5130. https://doi.org/10.3390/jcm10215130