
Association of C-Reactive Protein Velocity with Early Left Ventricular Dysfunction in Patients with First ST-Elevation Myocardial Infarction

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design, Patient Population and Endpoint Definition
2.2. Cardiac Magnetic Resonance Imaging
2.3. Statistical Analyses
3. Results
3.1. Baseline Patient Characteristics
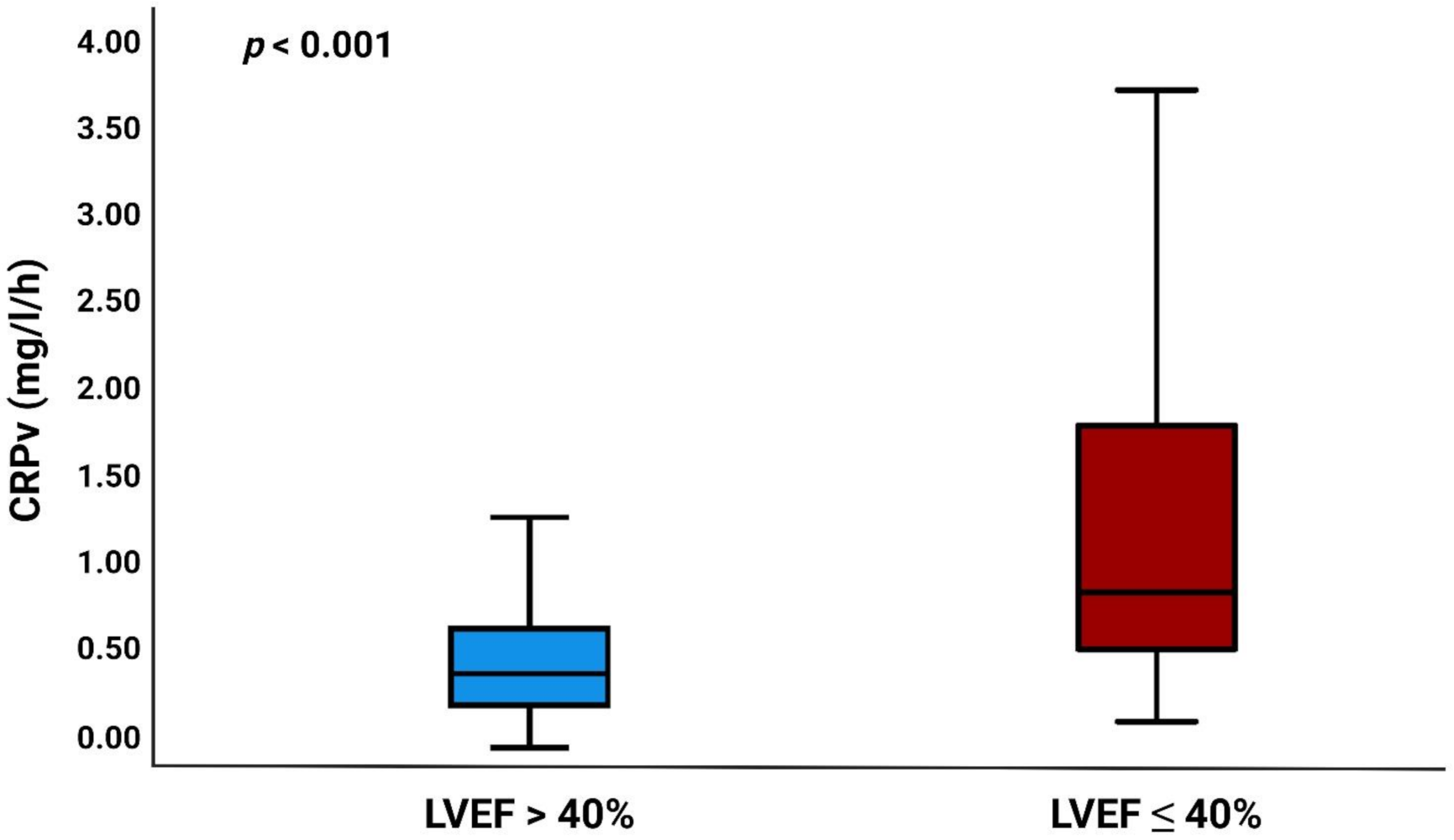
3.2. CRPv as a Marker of LV Dysfunction
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Desta, L.; Jernberg, T.; Lofman, I.; Hofman-Bang, C.; Hagerman, I.; Spaak, J.; Persson, H. Incidence, temporal trends, and prognostic impact of heart failure complicating acute myocardial infarction. The SWEDEHEART Registry (Swedish Web-System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies): A study of 199,851 patients admitted with index acute myocardial infarctions, 1996 to 2008. JACC Heart Fail. 2015, 3, 234–242. [Google Scholar] [PubMed]
- Sutton, N.R.; Li, S.; Thomas, L.; Wang, T.Y.; de Lemos, J.A.; Enriquez, J.R.; Shah, R.U.; Fonarow, G.C. The association of left ventricular ejection fraction with clinical outcomes after myocardial infarction: Findings from the Acute Coronary Treatment and Intervention Outcomes Network (ACTION) Registry-Get With the Guidelines (GWTG) Medicare-linked database. Am. Heart J. 2016, 178, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Ng, V.G.; Lansky, A.J.; Meller, S.; Witzenbichler, B.; Guagliumi, G.; Peruga, J.Z.; Brodie, B.; Shah, R.; Mehran, R.; Stone, G.W. The prognostic importance of left ventricular function in patients with ST-segment elevation myocardial infarction: The HORIZONS-AMI trial. Eur. Heart J. Acute Cardiovasc. Care 2014, 3, 67–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Stumpf, C.; Sheriff, A.; Zimmermann, S.; Schaefauer, L.; Schlundt, C.; Raaz, D.; Garlichs, C.D.; Achenbach, S. C-reactive protein levels predict systolic heart failure and outcome in patients with first ST-elevation myocardial infarction treated with coronary angioplasty. Arch. Med. Sci. 2017, 13, 1086–1093. [Google Scholar] [CrossRef] [Green Version]
- Reindl, M.; Reinstadler, S.J.; Feistritzer, H.J.; Klug, G.; Tiller, C.; Mair, J.; Mayr, A.; Jaschke, W.; Metzler, B. Relation of inflammatory markers with myocardial and microvascular injury in patients with reperfused ST-elevation myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2017, 6, 640–649. [Google Scholar] [CrossRef]
- Mather, A.N.; Fairbairn, T.A.; Artis, N.J.; Greenwood, J.P.; Plein, S. Relationship of cardiac biomarkers and reversible and irreversible myocardial injury following acute myocardial infarction as determined by cardiovascular magnetic resonance. Int J. Cardiol. 2013, 166, 458–464. [Google Scholar] [CrossRef]
- Orn, S.; Manhenke, C.; Ueland, T.; Damas, J.K.; Mollnes, T.E.; Edvardsen, T.; Aukrust, P.; Dickstein, K. C-reactive protein, infarct size, microvascular obstruction, and left-ventricular remodelling following acute myocardial infarction. Eur. Heart J. 2009, 30, 1180–1186. [Google Scholar] [CrossRef] [Green Version]
- Yip, H.K.; Hang, C.L.; Fang, C.Y.; Hsieh, Y.K.; Yang, C.H.; Hung, W.C.; Wu, C.J. Level of high-sensitivity C-reactive protein is predictive of 30-day outcomes in patients with acute myocardial infarction undergoing primary coronary intervention. Chest 2005, 127, 803–808. [Google Scholar] [CrossRef]
- Theroux, P.; Armstrong, P.W.; Mahaffey, K.W.; Hochman, J.S.; Malloy, K.J.; Rollins, S.; Nicolau, J.C.; Lavoie, J.; Luong, T.M.; Burchenal, J.; et al. Prognostic significance of blood markers of inflammation in patients with ST-segment elevation myocardial infarction undergoing primary angioplasty and effects of pexelizumab, a C5 inhibitor: A substudy of the COMMA trial. Eur. Heart J. 2005, 26, 1964–1970. [Google Scholar] [CrossRef] [Green Version]
- Ortolani, P.; Marzocchi, A.; Marrozzini, C.; Palmerini, T.; Saia, F.; Taglieri, N.; Baldazzi, F.; Silenzi, S.; Bacchi-Reggiani, M.L.; Guastaroba, P.; et al. Predictive value of high sensitivity C-reactive protein in patients with ST-elevation myocardial infarction treated with percutaneous coronary intervention. Eur. Heart J. 2008, 29, 1241–1249. [Google Scholar] [CrossRef] [Green Version]
- Kushner, I.; Broder, M.L.; Karp, D. Control of the acute phase response. Serum C-reactive protein kinetics after acute myocardial infarction. J. Clin. Investig. 1978, 61, 235–242. [Google Scholar] [CrossRef]
- Mani, P.; Puri, R.; Schwartz, G.G.; Nissen, S.E.; Shao, M.; Kastelein, J.J.P.; Menon, V.; Lincoff, A.M.; Nicholls, S.J. Association of Initial and Serial C-Reactive Protein Levels With Adverse Cardiovascular Events and Death After Acute Coronary Syndrome: A Secondary Analysis of the VISTA-16 Trial. JAMA Cardiol. 2019, 4, 314–320. [Google Scholar] [CrossRef] [Green Version]
- Swiatkiewicz, I.; Magielski, P.; Kubica, J. C-Reactive Protein as a Risk Marker for Post-Infarct Heart Failure over a Multi-Year Period. Int. J. Mol. Sci. 2021, 22, 3169. [Google Scholar] [CrossRef]
- Swiatkiewicz, I.; Taub, P.R. The usefulness of C-reactive protein for the prediction of post-infarct left ventricular systolic dysfunction and heart failure. Kardiol. Pol. 2018, 76, 821–829. [Google Scholar] [CrossRef] [Green Version]
- Swiatkiewicz, I.; Magielski, P.; Kubica, J.; Zadourian, A.; DeMaria, A.N.; Taub, P.R. Enhanced Inflammation is a Marker for Risk of Post-Infarct Ventricular Dysfunction and Heart Failure. Int. J. Mol. Sci. 2020, 21, 807. [Google Scholar] [CrossRef] [Green Version]
- Swiatkiewicz, I.; Kozinski, M.; Magielski, P.; Fabiszak, T.; Sukiennik, A.; Navarese, E.P.; Odrowaz-Sypniewska, G.; Kubica, J. Value of C-reactive protein in predicting left ventricular remodelling in patients with a first ST-segment elevation myocardial infarction. Mediat. Inflamm. 2012, 2012, 250867. [Google Scholar] [CrossRef]
- Ries, W.; Torzewski, J.; Heigl, F.; Pfluecke, C.; Kelle, S.; Darius, H.; Ince, H.; Mitzner, S.; Nordbeck, P.; Butter, C.; et al. C-Reactive Protein Apheresis as Anti-inflammatory Therapy in Acute Myocardial Infarction: Results of the CAMI-1 Study. Front. Cardiovasc. Med. 2021, 8, 591714. [Google Scholar] [CrossRef]
- Holzknecht, M.; Tiller, C.; Reindl, M.; Lechner, I.; Troger, F.; Hosp, M.; Mayr, A.; Brenner, C.; Klug, G.; Bauer, A.; et al. C-reactive protein velocity predicts microvascular pathology after acute ST-elevation myocardial infarction. Int. J. Cardiol. 2021. [Google Scholar] [CrossRef]
- Zahler, D.; Merdler, I.; Rozenfeld, K.L.; Shenberg, G.; Milwidsky, A.; Berliner, S.; Banai, S.; Arbel, Y.; Shacham, Y. C-Reactive Protein Velocity and the Risk of New Onset Atrial Fibrillation among ST Elevation Myocardial Infarction Patients. Isr. Med. Assoc. J. 2021, 23, 169–173. [Google Scholar]
- Milwidsky, A.; Ziv-Baran, T.; Letourneau-Shesaf, S.; Keren, G.; Taieb, P.; Berliner, S.; Shacham, Y. CRP velocity and short-term mortality in ST segment elevation myocardial infarction. Biomarkers 2017, 22, 383–386. [Google Scholar] [CrossRef]
- Zahler, D.; Rozenfeld, K.L.; Stein, M.; Milwidsky, A.; Berliner, S.; Banai, S.; Arbel, Y.; Shacham, Y. C-reactive protein velocity and the risk of acute kidney injury among ST elevation myocardial infarction patients undergoing primary percutaneous intervention. J. Nephrol. 2019, 32, 437–443. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Group, E.S.C.S.D. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2019, 40, 237–269. [Google Scholar] [CrossRef] [Green Version]
- Reinstadler, S.J.; Feistritzer, H.J.; Klug, G.; Mair, J.; Tu, A.M.; Kofler, M.; Henninger, B.; Franz, W.M.; Metzler, B. High-sensitivity troponin T for prediction of left ventricular function and infarct size one year following ST-elevation myocardial infarction. Int. J. Cardiol. 2016, 202, 188–193. [Google Scholar] [CrossRef]
- Feistritzer, H.J.; Reinstadler, S.J.; Klug, G.; Reindl, M.; Wohrer, S.; Brenner, C.; Mayr, A.; Mair, J.; Metzler, B. Multimarker approach for the prediction of microvascular obstruction after acute ST-segment elevation myocardial infarction: A prospective, observational study. BMC Cardiovasc. Disord. 2016, 16, 239. [Google Scholar] [CrossRef] [Green Version]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Gavara, J.; Marcos-Garces, V.; Lopez-Lereu, M.P.; Monmeneu, J.V.; Rios-Navarro, C.; de Dios, E.; Perez, N.; Merenciano, H.; Gabaldon, A.; Canoves, J.; et al. Magnetic Resonance Assessment of Left Ventricular Ejection Fraction at Any Time Post-Infarction for Prediction of Subsequent Events in a Large Multicenter STEMI Registry. J. Magn. Reson. Imaging 2021. [Google Scholar] [CrossRef] [PubMed]
- Reinstadler, S.J.; Klug, G.; Feistritzer, H.J.; Mayr, A.; Harrasser, B.; Mair, J.; Bader, K.; Streil, K.; Hammerer-Lercher, A.; Esterhammer, R.; et al. Association of copeptin with myocardial infarct size and myocardial function after ST segment elevation myocardial infarction. Heart 2013, 99, 1525–1529. [Google Scholar] [CrossRef] [PubMed]
- Holzknecht, M.; Reindl, M.; Tiller, C.; Reinstadler, S.J.; Lechner, I.; Pamminger, M.; Schwaiger, J.P.; Klug, G.; Bauer, A.; Metzler, B.; et al. Global longitudinal strain improves risk assessment after ST-segment elevation myocardial infarction: A comparative prognostic evaluation of left ventricular functional parameters. Clin. Res. Cardiol. 2021, 110, 1599–1611. [Google Scholar] [CrossRef] [PubMed]
- Lechner, I.; Reindl, M.; Tiller, C.; Holzknecht, M.; Troger, F.; Fink, P.; Mayr, A.; Klug, G.; Bauer, A.; Metzler, B.; et al. Impact of COVID-19 pandemic restrictions on ST-segment elevation myocardial infarction: A cardiac MRI study. Eur. Heart J. 2021, ehab621. [Google Scholar] [CrossRef] [PubMed]
- Reindl, M.; Reinstadler, S.J.; Feistritzer, H.J.; Theurl, M.; Basic, D.; Eigler, C.; Holzknecht, M.; Mair, J.; Mayr, A.; Klug, G.; et al. Relation of Low-Density Lipoprotein Cholesterol with Microvascular Injury and Clinical Outcome in Revascularized ST-Elevation Myocardial Infarction. J. Am. Heart Assoc. 2017, 6, e006957. [Google Scholar] [CrossRef] [Green Version]
- Bondarenko, O.; Beek, A.M.; Hofman, M.B.; Kuhl, H.P.; Twisk, J.W.; van Dockum, W.G.; Visser, C.A.; van Rossum, A.C. Standardizing the definition of hyperenhancement in the quantitative assessment of infarct size and myocardial viability using delayed contrast-enhanced CMR. J. Cardiovasc. Magn. Reson. 2005, 7, 481–485. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Rice, M.E.; Harris, G.T. Comparing effect sizes in follow-up studies: ROC Area, Cohen’s d, and r. Law Hum. Behav. 2005, 29, 615–620. [Google Scholar] [CrossRef]
- Fanola, C.L.; Morrow, D.A.; Cannon, C.P.; Jarolim, P.; Lukas, M.A.; Bode, C.; Hochman, J.S.; Goodrich, E.L.; Braunwald, E.; O’Donoghue, M.L. Interleukin-6 and the Risk of Adverse Outcomes in Patients After an Acute Coronary Syndrome: Observations From the SOLID-TIMI 52 (Stabilization of Plaque Using Darapladib-Thrombolysis in Myocardial Infarction 52) Trial. J. Am. Heart Assoc. 2017, 6, e005637. [Google Scholar] [CrossRef] [Green Version]
- Sheriff, A.; Kayser, S.; Brunner, P.; Vogt, B. C-Reactive Protein Triggers Cell Death in Ischemic Cells. Front. Immunol. 2021, 12, 630430. [Google Scholar] [CrossRef]
- Vanhaverbeke, M.; Veltman, D.; Pattyn, N.; De Crem, N.; Gillijns, H.; Cornelissen, V.; Janssens, S.; Sinnaeve, P.R. C-reactive protein during and after myocardial infarction in relation to cardiac injury and left ventricular function at follow-up. Clin. Cardiol. 2018, 41, 1201–1206. [Google Scholar] [CrossRef]
- Tiller, C.; Reindl, M.; Holzknecht, M.; Lechner, I.; Simma, F.; Schwaiger, J.; Mayr, A.; Klug, G.; Bauer, A.; Reinstadler, S.J.; et al. High sensitivity C-reactive protein is associated with worse infarct healing after revascularized ST-elevation myocardial infarction. Int. J. Cardiol. 2020, 328, 191–196. [Google Scholar] [CrossRef]
- de Waha, S.; Patel, M.R.; Granger, C.B.; Ohman, E.M.; Maehara, A.; Eitel, I.; Ben-Yehuda, O.; Jenkins, P.; Thiele, H.; Stone, G.W. Relationship between microvascular obstruction and adverse events following primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: An individual patient data pooled analysis from seven randomized trials. Eur. Heart J. 2017, 38, 3502–3510. [Google Scholar] [CrossRef]
- Reinstadler, S.J.; Stiermaier, T.; Eitel, C.; Fuernau, G.; Saad, M.; Poss, J.; de Waha, S.; Mende, M.; Desch, S.; Metzler, B.; et al. Impact of Atrial Fibrillation During ST-Segment-Elevation Myocardial Infarction on Infarct Characteristics and Prognosis. Circ. Cardiovasc. Imaging 2018, 11, e006955. [Google Scholar] [CrossRef] [Green Version]
- Montone, R.A.; La Vecchia, G. Interplay between inflammation and microvascular obstruction in ST-segment elevation myocardial infarction: The importance of velocity. Int J. Cardiol. 2021, 339, 7–9. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. CRP Apheresis in STEMI. Available online: https://clinicaltrials.gov/ct2/show/NCT04939805 (accessed on 27 September 2021).
- Broch, K.; Anstensrud, A.K.; Woxholt, S.; Sharma, K.; Tollefsen, I.M.; Bendz, B.; Aakhus, S.; Ueland, T.; Amundsen, B.H.; Damas, J.K.; et al. Randomized Trial of Interleukin-6 Receptor Inhibition in Patients with Acute ST-Segment Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2021, 77, 1845–1855. [Google Scholar] [CrossRef]
- Toldo, S.; Abbate, A. The NLRP3 inflammasome in acute myocardial infarction. Nat. Rev. Cardiol. 2018, 15, 203–214. [Google Scholar] [CrossRef]
- Abbate, A.; Toldo, S.; Marchetti, C.; Kron, J.; Van Tassell, B.W.; Dinarello, C.A. Interleukin-1 and the Inflammasome as Therapeutic Targets in Cardiovascular Disease. Circ. Res. 2020, 126, 1260–1280. [Google Scholar] [CrossRef]
- Abbate, A.; Kontos, M.C.; Grizzard, J.D.; Biondi-Zoccai, G.G.; Van Tassell, B.W.; Robati, R.; Roach, L.M.; Arena, R.A.; Roberts, C.S.; Varma, A.; et al. Interleukin-1 blockade with anakinra to prevent adverse cardiac remodeling after acute myocardial infarction (Virginia Commonwealth University Anakinra Remodeling Trial [VCU-ART] Pilot study). Am. J. Cardiol. 2010, 105, 1371–1377.e1. [Google Scholar] [CrossRef] [Green Version]
- Everett, B.M.; Cornel, J.H.; Lainscak, M.; Anker, S.D.; Abbate, A.; Thuren, T.; Libby, P.; Glynn, R.J.; Ridker, P.M. Anti-Inflammatory Therapy with Canakinumab for the Prevention of Hospitalization for Heart Failure. Circulation 2019, 139, 1289–1299. [Google Scholar] [CrossRef]
- El-Menyar, A.; Zubaid, M.; AlMahmeed, W.; Sulaiman, K.; AlNabti, A.; Singh, R.; Al Suwaidi, J. Killip classification in patients with acute coronary syndrome: Insight from a multicenter registry. Am. J. Emerg. Med. 2012, 30, 97–103. [Google Scholar] [CrossRef]
- Overtchouk, P.; Barthelemy, O.; Hauguel-Moreau, M.; Guedeney, P.; Rouanet, S.; Zeitouni, M.; Silvain, J.; Collet, J.P.; Vicaut, E.; Zeymer, U.; et al. Angiographic predictors of outcome in myocardial infarction patients presenting with cardiogenic shock: A CULPRIT-SHOCK angiographic substudy. EuroIntervention 2021, 16, e1237–e1244. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.M.; Schomig, A. Coronary and myocardial angiography: Angiographic assessment of both epicardial and myocardial perfusion. Circulation 2004, 109, 3096–3105. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Total Population (n = 432) | LVEF > 40% (n = 335, 78%) | LVEF ≤ 40% (n = 97, 22%) | p-Value | |
|---|---|---|---|---|
| Age, years | 57 [51–65] | 56 [50–64] | 58 [53–69] | 0.010 |
| Female, n (%) | 81(19) | 68 (20) | 13 (13) | 0.125 |
| Body mass index, kg/m2 | 26.1 [24.4–28.7] | 26.0 [24.4–28.7] | 26.2 [24.7–28.7] | 0.622 |
| Current smoker, n (%) | 247 (57) | 205 (61) | 42 (43) | 0.002 |
| Hyperlipidemia, n (%) | 230 (53) | 176 (53) | 54 (56) | 0.586 |
| Diabetes mellitus, n (%) | 35 (8) | 25 (8) | 10 (10) | 0.366 |
| Family history, n (%) | 135 (31) | 112 (33) | 23 (24) | 0.160 |
| Hypertension, n (%) | 191 (44) | 148 (44) | 43 (44) | 0.979 |
| Systolic blood pressure, mmHg | 137 [117–154] | 136 [117–154] | 137 [118–152] | 0.827 |
| Diastolic blood pressure, mmHg | 82 [72–95] | 80 [72–94] | 85 [76–100] | 0.039 |
| Symptomatic heart failure before STEMI, n (%) | 0 (0) | 0 (0) | 0 (0) | - |
| Killip class, n (%) | <0.001 | |||
| I | 296 (69) | 247 (74) | 49 (50) | |
| II | 136 (32) | 88 (26) | 48 (50) | |
| Total ischemia time, min | 178 [120–262] | 171 [120–260] | 188 [129–267] | 0.407 |
| Culprit lesion, n (%) | <0.001 | |||
| RCA | 183 (42) | 165 (49) | 18 (19) | |
| LAD | 189 (44) | 124 (37) | 65 (67) | |
| LCX | 57 (13) | 45 (13) | 12 (12) | |
| RI | 3 (1) | 1 (1) | 2 (2) | |
| Anterior infarction, n (%) | 190 (44) | 126 (38) | 64 (66) | <0.001 |
| Number of affected vessels, n (%) | 0.656 | |||
| 1 | 260 (60) | 201 (60) | 59 (61) | |
| 2 | 119 (28) | 95 (28) | 24 (25) | |
| 3 | 53 (12) | 39 (12) | 14 (14) | |
| TIMI flow pre-PCI, n (%) | 0.018 | |||
| 0 | 273 (63) | 200 (60) | 73 (75) | |
| 1 | 55 (13) | 43 (13) | 12 (13) | |
| 2 | 75 (17) | 67 (20) | 8 (8) | |
| 3 | 29 (7) | 25 (7) | 4 (4) | |
| TIMI flow post-PCI, n (%) | 0.006 | |||
| 0 | 4 (1) | 2 (1) | 2 (2) | |
| 1 | 6 (1) | 3 (1) | 3 (3) | |
| 2 | 34 (8) | 20 (6) | 14 (14) | |
| 3 | 388 (90) | 310 (92) | 78 (81) | |
| CRP, mg/L | ||||
| Admission | 2.1 [1.0–4.2] | 2.0 [1.0–4.2] | 2.3 [1.0–4.7] | 0.383 |
| 24 h | 12.4 [6.9–20.1] | 11.0 [6.0–17.1] | 20.9 [10.9–45.7] | <0.001 |
| Peak | 22.5 [11.7–45.5] | 19.0 [10.3–34.4] | 54.6 [25.9–94.7] | <0.001 |
| Admission to 24 h CRP, h | 21 [19–25] | 21 [19–25] | 21 [19–25] | 0.640 |
| Admission to peak CRP, h | 46 [35–56] | 45 [31–55] | 47 [42–58] | 0.028 |
| CRPv (admission to 24 h), mg/L/h | 0.42 [0.21–0.76] | 0.34 [0.16–0.61] | 0.81 [0.47–1.78] | <0.001 |
| cTnT, ng/L | ||||
| Peak | 4646 [2187–8430] | 3902 [1718–6676] | 9065 [5014–14877] | <0.001 |
| Admission to peak cTnT, h | 11 [7–16] | 11 [7–16] | 9 [6–13] | 0.014 |
| Total Population (n = 432) | LVEF > 40% (n = 335, 78%) | LVEF ≤ 40% (n = 97, 22%) | p-Value | |
|---|---|---|---|---|
| LVEDV, mL | 167 [137–189] | 162 [134–187] | 182 [154–204] | <0.001 |
| LVESV, mL | 83 [64–94] | 75 [60–92] | 118 [99–131] | <0.001 |
| LVEF, % | 49 [42–55] | - | - | - |
| LVSV, mL | 79 [65–94] | 84 [70–97] | 60 [50–75] | <0.001 |
| CO, L/min | 5.3 [4.4–6.2] | 5.5 [4.7–6.3] | 4.6 [3.8–5.7] | <0.001 |
| IS, % of LVMM | 14.5 [7.5–24.3] | 13.0 [6.2–20.6] | 26.1 [16.0–34.2] | <0.001 |
| MVO, n (%) | 241 (56) | 160 (48) | 81 (84) | <0.001 |
| MVO, % of LVMM | 0.4 [0.0–2.5] | 0.0 [0.0–1.5] | 2.5 [0.6–6.4] | <0.001 |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| β | p-Value | β | p-Value | |
| CRPv | −0.397 | <0.001 | −0.161 | 0.004 |
| Peak CRP | −0.378 | <0.001 | −0.098 | 0.082 |
| Peak cTnT | −0.498 | <0.001 | −0.343 | <0.001 |
| Anterior infarction | −0.222 | <0.001 | −0.047 | 0.253 |
| TIMI flow pre-PCI | 0.264 | <0.001 | 0.085 | 0.045 |
| TIMI flow post-PCI | 0.204 | <0.001 | 0.105 | 0.010 |
| Current smoker | 0.173 | <0.001 | 0.104 | 0.015 |
| Age | −0.133 | 0.006 | 0.011 | 0.806 |
| Diastolic blood pressure | 0.000 | 0.999 | - | - |
| Killip class | −0.210 | <0.001 | −0.053 | 0.197 |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| CRPv | 2.69 (2.01–3.60) | <0.001 | 1.71(1.19–2.45) | 0.004 |
| Peak CRP | 2.55 (1.92–3.39) | <0.001 | 1.28 (0.92–1.79) | 0.146 |
| Peak cTnT | 2.82 (2.15–3.71) | <0.001 | 2.09 (1.54–2.85) | <0.001 |
| Anterior infarction | 1.78 (1.41–2.26) | <0.001 | 1.28 (0.97–1.71) | 0.079 |
| TIMI flow pre-PCI | 0.67 (0.51–0.88) | 0.003 | 1.04 (0.75–1.44) | 0.828 |
| TIMI flow post-PCI | 0.73 (0.60–0.89) | 0.002 | 0.83 (0.65–1.05) | 0.112 |
| Current smoker | 0.70 (0.56–0.88) | 0.002 | 0.76 (0.56–1.03) | 0.079 |
| Age | 1.38 (1.09–1.72) | 0.006 | 1.03 (0.75–1.37) | 0.914 |
| Diastolic blood pressure | 1.27 (1.02–1.59) | 0.037 | 1.18 (0.89–1.55) | 0.258 |
| Killip class | 2.75 (1.72–4.38) | <0.001 | 1.54 (0.87–2.76) | 0.142 |
| Variables | AUC | 95% CI | p-Value | AUC Increment | ROC Comparison |
|---|---|---|---|---|---|
| Admission CRP | 0.53 | 0.48–0.58 | 0.383 | - | - |
| 24 h CRP | 0.73 | 0.69–0.77 | <0.001 | 0.20 | <0.001 |
| CRPv | 0.77 | 0.72–0.81 | <0.001 | 0.04 | <0.001 |
| Peak CRP | 0.77 | 0.73–0.81 | <0.001 | <0.01 | 0.807 |
| Peak cTnT | 0.77 | 0.73–0.81 | <0.001 | <0.01 | 0.905 |
| CRPv and peak cTnT | 0.81 | 0.77–0.85 | <0.001 | 0.04 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holzknecht, M.; Tiller, C.; Reindl, M.; Lechner, I.; Fink, P.; Lunger, P.; Mayr, A.; Henninger, B.; Brenner, C.; Klug, G.; et al. Association of C-Reactive Protein Velocity with Early Left Ventricular Dysfunction in Patients with First ST-Elevation Myocardial Infarction. J. Clin. Med. 2021, 10, 5494. https://doi.org/10.3390/jcm10235494
Holzknecht M, Tiller C, Reindl M, Lechner I, Fink P, Lunger P, Mayr A, Henninger B, Brenner C, Klug G, et al. Association of C-Reactive Protein Velocity with Early Left Ventricular Dysfunction in Patients with First ST-Elevation Myocardial Infarction. Journal of Clinical Medicine. 2021; 10(23):5494. https://doi.org/10.3390/jcm10235494
Chicago/Turabian StyleHolzknecht, Magdalena, Christina Tiller, Martin Reindl, Ivan Lechner, Priscilla Fink, Patrick Lunger, Agnes Mayr, Benjamin Henninger, Christoph Brenner, Gert Klug, and et al. 2021. "Association of C-Reactive Protein Velocity with Early Left Ventricular Dysfunction in Patients with First ST-Elevation Myocardial Infarction" Journal of Clinical Medicine 10, no. 23: 5494. https://doi.org/10.3390/jcm10235494