Correlation between Transthoracic Lung Ultrasound Score and HRCT Features in Patients with Interstitial Lung Diseases

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Protocol
2.3. Clinical Assessment
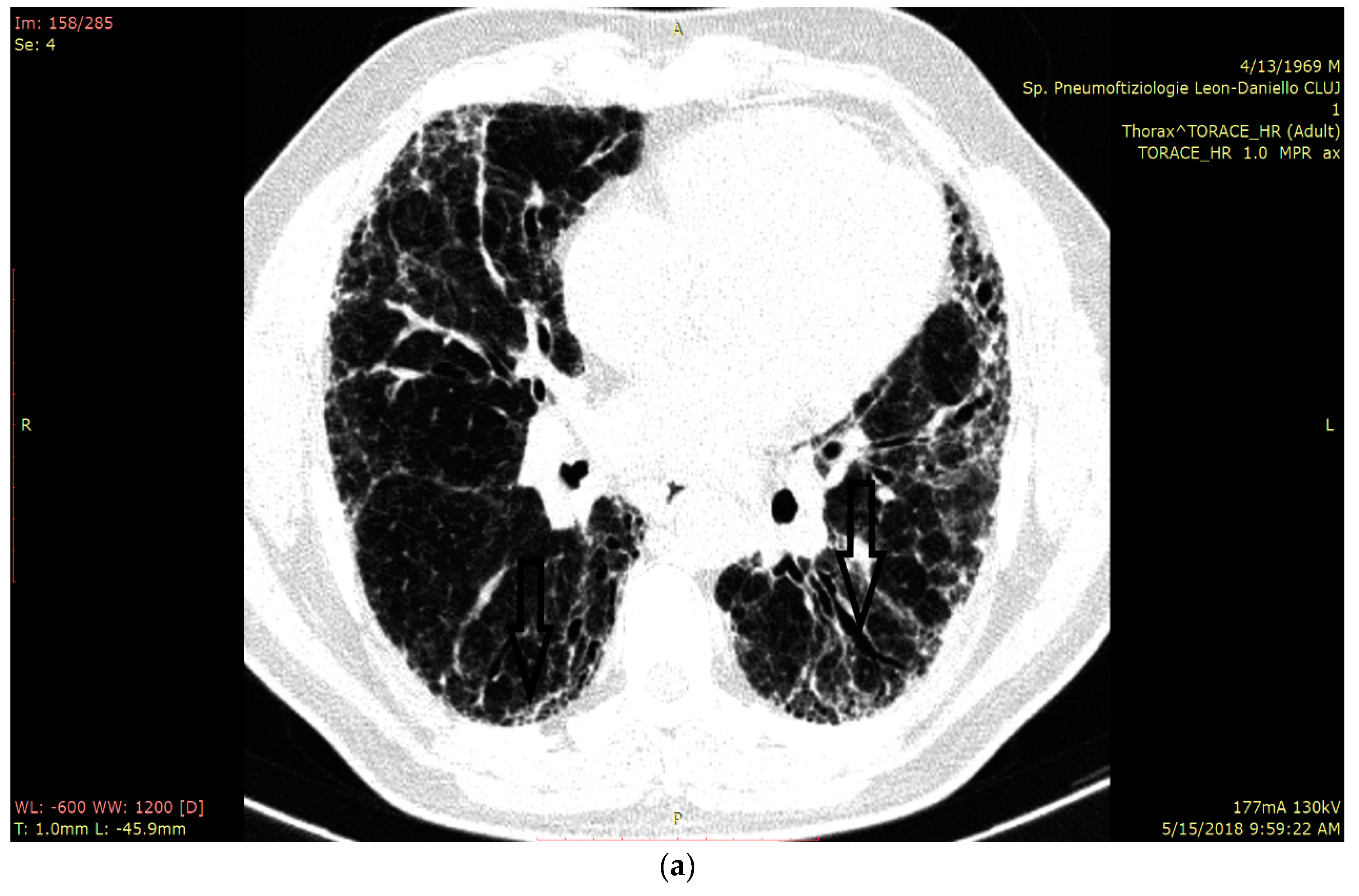
2.4. HRCT Assessment and Disease Quantification
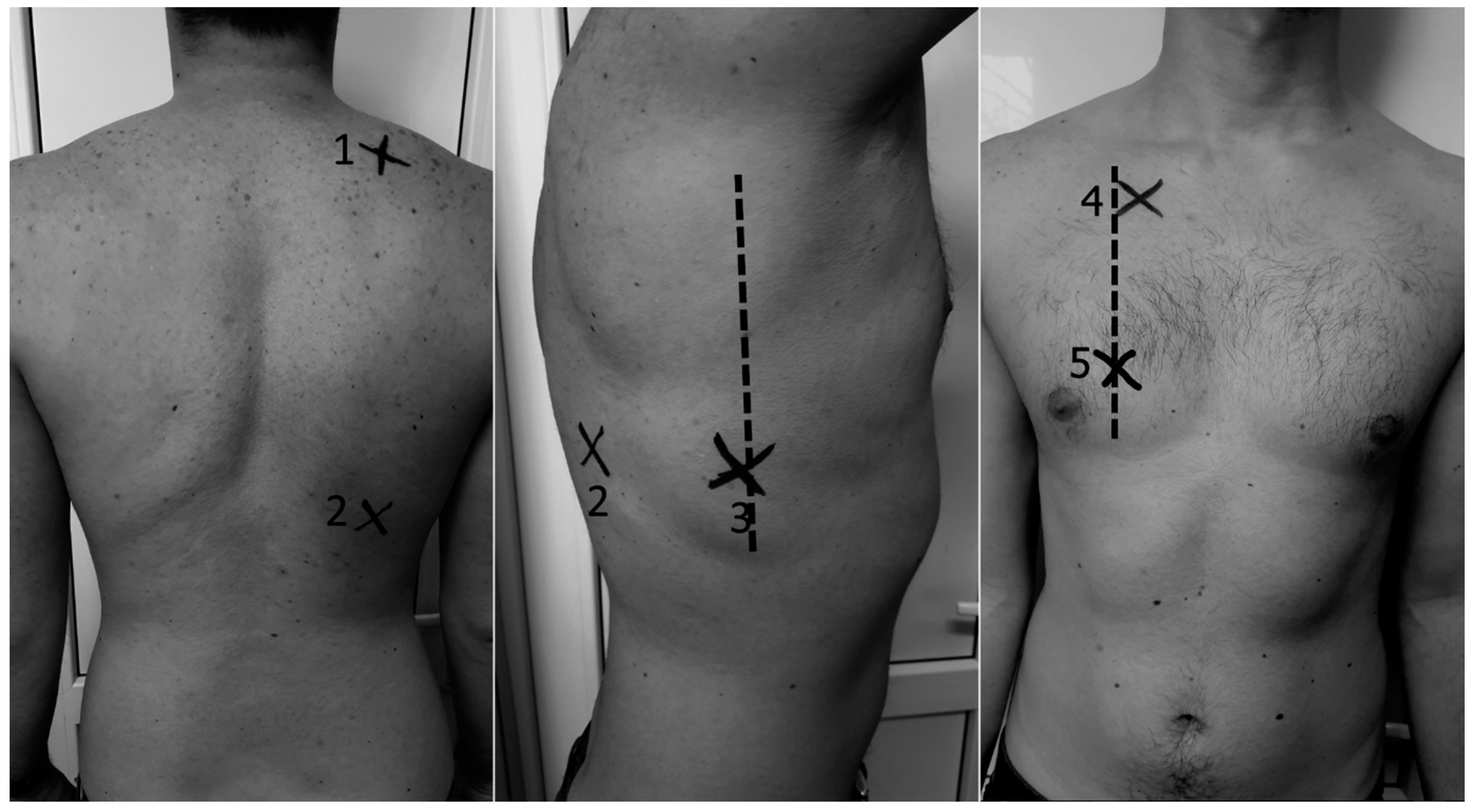
2.5. LUS Assessment and Quantification
2.6. Pulmonary Function Tests (PFTs)
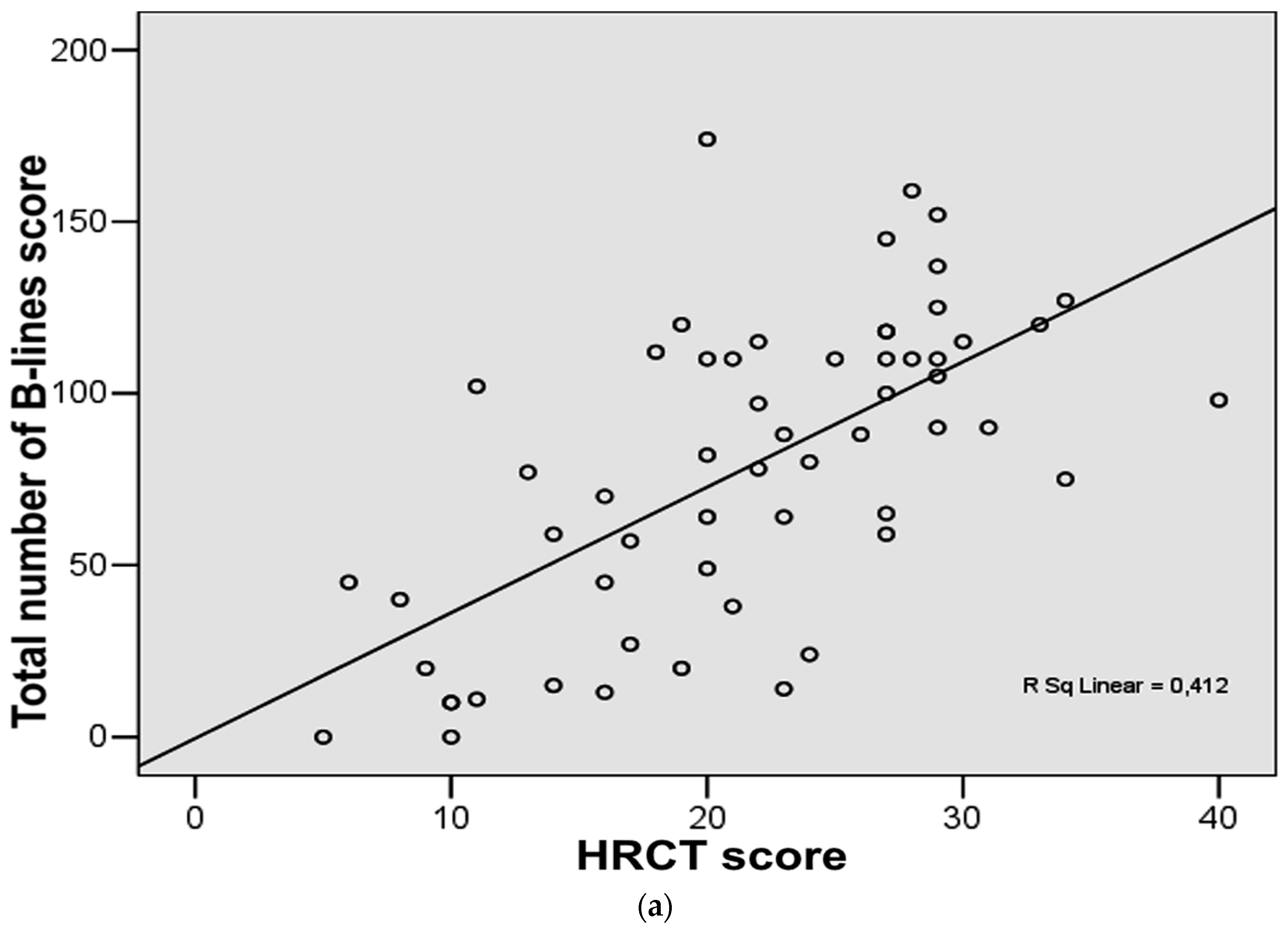
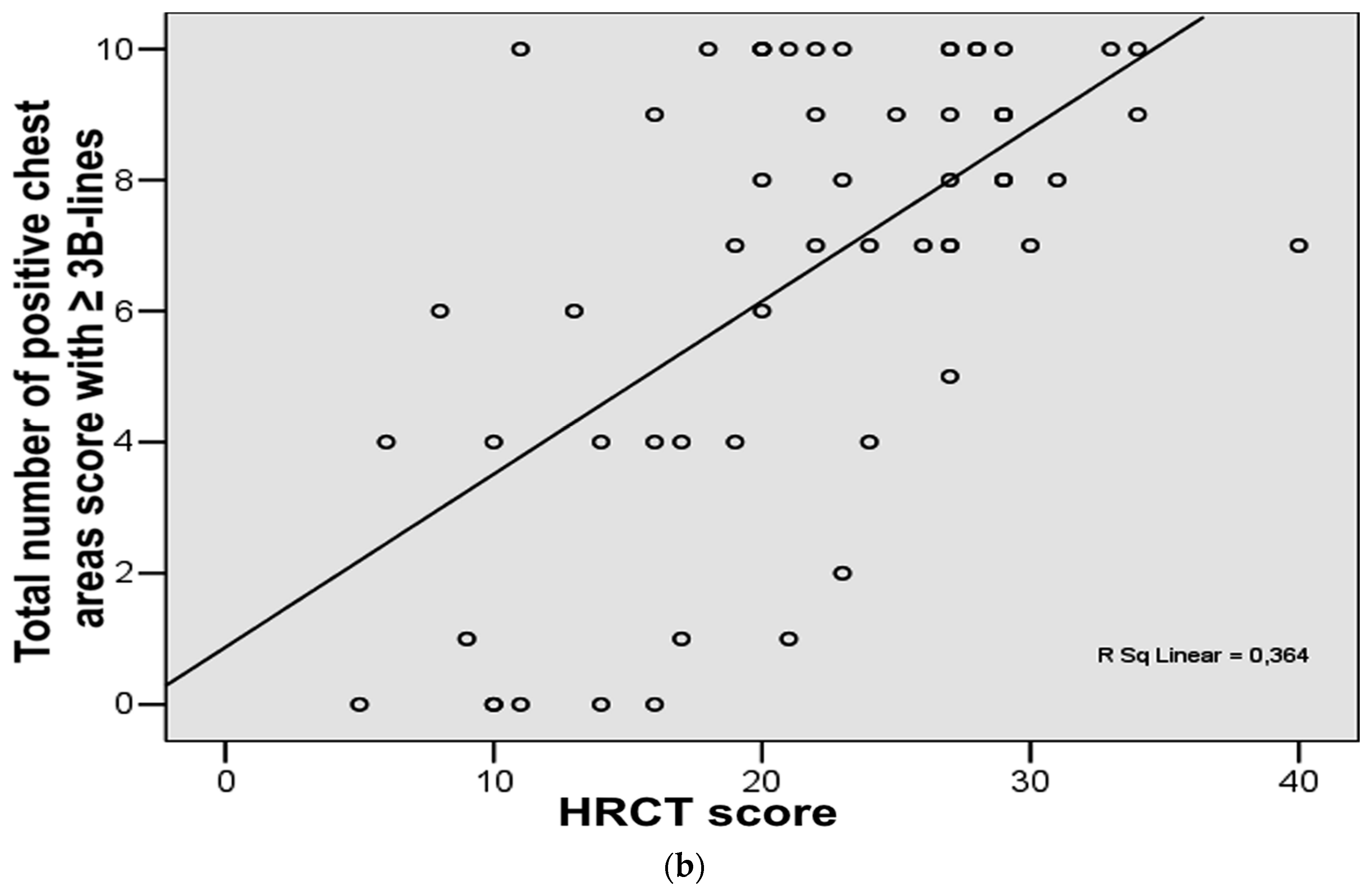
2.7. Statistical Analysis
3. Results
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Dhooria, S.; Agarwal, R.; Sehgal, I.S.; Prasad, K.T.; Garg, M.; Bal, A.; Aggarwal, A.N.; Behera, D. Spectrum of interstitial lung diseases at a tertiary center in a developing country: A study of 803 subjects. PLoS ONE 2018, 13, e0191938. [Google Scholar] [CrossRef] [PubMed]
- Arghir, O.C.; Niţu, M.; Trenchea, M.; Ciobotaru, C. Progressive intraparenchymal lung nodules dissemination in a heavy smoker and seropositive rheumatoid arthritis suspected of tuberculosis relapse. Rom. J. Morphol. Embryol. 2013, 54, 659–663. [Google Scholar] [PubMed]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Update of the International Multidisciplinary Classification of the Idiopathic Interstitial Pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Arghir, O.C.; Rascu, A.; Leonte, D.G.; Jimborean, G.; Mihailov, C. Romanian Asbestos Industry, Occupational Exposure and Delayed Diagnosis of a Malignant Pleural Mesothelioma—Case Report and Literature Review. J. Environ. Prot. Ecol. 2016, 17, 1354–1542. [Google Scholar]
- Toma, C.L.; Danteş, E.L.E.N.A.; Leonte, D.G.; Fildan, A.P. Respiratory bronchiolitis-associated interstitial lung disease—An unexpected form of idiopathic interstitial pneumonia in a young male. Rom. J. Morphol. Embryol. 2017, 58, 261–265. [Google Scholar] [PubMed]
- Vizioli, L.; Ciccarese, F.; Forti, P.; Chiesa, A.M.; Giovagnoli, M.; Mughetti, M.; Zompatori, M.; Zoli, M. Integrated Use of Lung Ultrasound and Chest X-Ray in the Detection of Interstitial Lung Disease. Respiration 2017, 93, 15–22. [Google Scholar] [CrossRef]
- Trăilă, D.; Mlădinescu, O.F.; Oancea, C.; Tudorache, V. Short telomeres in pulmonary fibrosis: From genetics to clinical significance. Pneumologia 2015, 64, 8–11. [Google Scholar]
- Domokos-Hancu, B.; Man, M.A.; Liana, H.; Pop, C.M. Lung response after subchronic glass fiber intratracheal instillation—an experimental study on rats. Exp. Lung Res. 2014, 40, 51–58. [Google Scholar] [CrossRef]
- Manolescu, D.; Davidescu, L.; Trăilă, D.; Oancea, C.; Tudorache, V. The reliability of lung ultrasound in assessment of idiopathic pulmonary fibrosis. Clin. Interv. Aging 2018, 13, 437–449. [Google Scholar] [CrossRef]
- Gargani, L.; Doveri, M.; D’Errico, L.; Frassi, F.; Bazzichi, M.L.; Sedie, A.D.; Scali, M.C.; Monti, S.; Mondillo, S.; Bombardieri, S.; et al. Ultrasound lung comets in systemic sclerosis: A chest sonography hallmark of pulmonary interstitial fibrosis. Rheumatology 2009, 48, 1382–1387. [Google Scholar] [CrossRef]
- Baldi, G.; Gargani, L.; Abramo, A.; D’Errico, L.; Caramella, D.; Picano, E.; Giunta, F.; Forfori, F. Lung water assessment by lung ultrasonography in intensive care: Apilot study. Intensive Care Med. 2013, 39, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Chiumello, D.; Mongodi, S.; Algieri, I.; Vergani, G.L.; Orlando, A.; Via, G.; Crimella, F.; Cressoni, M.; Mojoli, F. Assessment of Lung Aeration and Recruitment by CT scan and Ultrasound in Acute Respiratory Distress Syndrome Patients. Crit. Care Med. 2018, 46, 1761–1768. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Gargani, L.; Barskova, T.; Furst, D.E.; Cerinic, M.M. Usefulness of lung ultrasound B-lines in connective tissue disease-associated interstitial lung disease: A literature review. Arthritis Res. Ther. 2017, 19, 206. [Google Scholar] [CrossRef] [PubMed]
- Hasan, A.A.; Makhlouf, H.A. B-lines: Transthoracic chest ultrasound signs useful in assessment of interstitial lung diseases. Ann. Thorac. Med. 2014, 9, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Soldati, G.; Demi, M. The use of lung ultrasound images for the differential diagnosis of pulmonary and cardiac interstitial pathology. J. Ultrasound 2017, 20, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [Green Version]
- Zawada, T.; Wieczorek, A.; Garba, P. Point of care ultrasound-a way to reduce radiation exposure of patients and medical staff. Intensive Care Med. Exp. 2015, 3, A273. [Google Scholar] [CrossRef]
- Gutierrez, M.; Tardella, M.; Rodriguez, L.; Mendoza, J.; Clavijo-Cornejo, D.; García, A.; Bertolazzi, C. Ultrasound as a potential tool for the assessment of interstitial lung disease in rheumatic patients. Where are we now? Radiol. Med. 2019, 1–11. [Google Scholar] [CrossRef]
- Buda, N.; Kosiak, W.; Radzikowska, E.; Olszewski, R.; Jassem, E.; Grabczak, E.M.; Pomiecko, A.; Piotrkowski, J.; Piskunowicz, M.; Sołtysiak, M.; et al. Polish recommendations for lung ultrasound in internal medicine (POLLUS-IM). J. Ultrason. 2018, 18, 198–206. [Google Scholar] [CrossRef]
- Anile, A.; Russo, J.; Castiglione, G.; Volpicelli, G. A simplified lung ultrasound approach to detect incrased exatravascular lung water in critically ill patients. Crit. Ultrasound J. 2017, 9, 13. [Google Scholar] [CrossRef]
- Bouhemad, B.; Liu, Z.-H.; Arbelot, C.; Zhang, M.; Ferarri, F.; Le-Guen, M.; Girard, M.; Lu, Q.; Rouby, J.-J. Ultrasound assessment of antibiotic-induced pulmonary reaeration in ventilator-associated pneumonia. Crit. Care Med. 2010, 38, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Bouhemad, B.; Brisson, H.; Le-Guen, M.; Arbelot, C.; Lu, Q.; Rouby, J.-J. Bedside ultrasound assessment of positive end-expiratory pressure-induced lung recruitment. Am. J. Respir. Crit. Care Med. 2011, 183, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Yin, W.; Zou, T.; Qin, Y.; Yang, J.; Li, Y.; Zeng, X.; Kang, Y. Poor lung ultrasound score in shock patients admitted to the ICU is associated with worse outcome. BMC Pulm. Med. 2019, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Mongodi, S.; Pozzi, M.; Orlando, A.; Bouhemad, B.; Stella, A.; Tavazzi, G.; Via, G.; Iotti, G.A.; Mojoli, F. Lung ultrasound for daily monitoring of ARDS patients on extracorporeal membrane oxygenation: Preliminary experience. Intensive Care Med. 2018, 44, 123–124. [Google Scholar] [CrossRef] [PubMed]
- Soummer, A.; Perbet, S.; Brisson, H.; Arbelot, C.; Constantin, J.-M.; Lu, Q.; Rouby, J.-J. Ultrasound assessment of lung aeration loss during a successful weaning trial predicts postextubation distress. Crit. Care Med. 2012, 40, 2064–2072. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Jiang, L.; Xi, X.; Jiang, Q.; Zhu, B.; Wang, M.; Xing, J.; Zhang, D. Prognostic value of extravascular lung water assessed with lung ultrasound score by chest sonography in patients with acute respiratory distress syndrome. BMC Pulm. Med. 2015, 15, 98. [Google Scholar] [CrossRef] [PubMed]
- Dexheimer Neto, F.L.; Andrade, J.M.S.D.; Raupp, A.C.T.; Townsend, R.D.S.; Beltrami, F.G.; Brisson, H.; Lu, Q.; Dalcin, P.D.T.R. Diagnostic accuracy of the Bedside Lung Ultrasound in Emergency protocol for the diagnosis of acute respiratory failure in spontaneously breathing patients. J. Bras. Pneumol. 2015, 41, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, G.S.; Weeratunga, D.; Baker, K. Point-of Care Lung Ultrasound in Critically ill Patients. Rev. Recent. Clin. Trials 2018, 13, 15–26. [Google Scholar] [CrossRef]
- Wangkaew, S.; Euathrongchit, J.; Wattanawittawas, P.; Kasitanon, N. Correlation of delta high-resolution computed tomography (HRCT) score with delta clinical variables in early systemic sclerosis (SSc) patients. Quant. Imaging Med. Surg. 2016, 6, 381–390. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez, M.; Salaffi, F.; Carotti, M.; Tardella, M.; Pineda, C.; Bertolazzi, C.; Bichisecchi, E.; Filippucci, E.; Grassi, W. Utility of a simplified ultrasound assessment to assess interstitial pulmonary fibrosis in connective tissue disorders—Preliminary results. Arthritis Res. Ther. 2011, 13, 134. [Google Scholar] [CrossRef]
- Mohammadi, A.; Oshnoei, S.; Ghasemi-rad, M. Comparison of a new, modified lung ultrasonography technique with high-resolution CT in the diagnosis of the alveolar-interstitial syndrome of systemic scleroderma. Med. Ultrason. 2014, 16, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Tardella, M.; Di Carlo, M.; Carotti, M.; Filippucci, E.; Grassi, W.; Salaffi, F. Ultrasound B-lines in the evaluation of interstitial lung disease in patients with systemic sclerosis: Cut-off point definition for the presence of significant pulmonary fibrosis. Medicine 2018, 97, e0566. [Google Scholar] [CrossRef] [PubMed]
- Mongodi, S.; Bouhemad, B.; Orlando, A.; Stella, A.; Tavazzi, G.; Via, G.; Iotti, G.A.; Braschi, A.; Mojoli, F. Modified Lung Ultrasound Score for Assessing and Monitoring Pulmonary Aeration. Ultraschall Med. 2017, 38, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Bujang, M.A.; Baharum, N. Sample Size Guideline for Correlation Analysis. World 2016, 3. [Google Scholar] [CrossRef]
- Gigante, A.; Fanelli, F.R.; Lucci, S.; Barilaro, G.; Quarta, S.; Barbano, B.; Giovannetti, A.; Amoroso, A.; Rosato, E. Lung ultrasound in systemic sclerosis: Correlation with high-resolution computed tomography, pulmonary function tests and clinical variables of disease. Intern. Emerg. Med. 2016, 11, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Asano, M.; Watanabe, H.; Sato, K.; Okuda, Y.; Sakamoto, S.; Hasegawa, Y.; Sudo, K.; Takeda, M.; Sano, M.; Kibira, S.; et al. Validity of Ultrasound Lung Comets for Assessment of the Severity of Interstitial Pneumonia. J. Ultrasound Med. 2018, 37, 1523–1531. [Google Scholar] [CrossRef]
- Falcetta, A.; Leccardi, S.; Testa, E.; Papaleo, F.; Fenoglio, L.; Melchio, R. The role of lung ultrasound in the diagnosis of interstitial lung disease. Shanghai Chest 2018, 2, 41. [Google Scholar] [CrossRef]
- Mojoli, F.; Bouhemad, B.; Mongodi, S.; Lichtenstein, D. Lung Ultrasound for Critically Ill Patients. Am. J. Respir. Crit. Care Med. 2019, 199, 701–714. [Google Scholar] [CrossRef]
- Edis, E.C.; Hatipoğlu, O.N.; Pamuk, Ö.N.; Eraslan, R.M.; Aktöz, M.; Tuncel, S.A. Effectiveness of Thoracic Ultrasonography in the Evaluation of the Severity of Pulmonary Involvement in Patients with Systemic Sclerosis. Arch. Rheumatol. 2016, 31, 364–370. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Mathis, G.; Blaivas, M.; Volpicelli, G.; Seibel, A.; Wastl, D.; Yi, D. Lung B-line artifacts and their use. J. Thorac. Dis. 2016, 8, 1356–1365. [Google Scholar] [CrossRef]
- Goldin, J.G.; Lynch, D.A.; Strollo, D.C.; Suh, R.D.; Schraufnagel, D.E.; Clements, P.J.; Elashoff, R.M.; Furst, D.E.; Vasunilashorn, S.; McNitt-Gray, M.F.; et al. High-resolution CT scan findings in patients with symptomatic scleroderma-related interstitial lung disease. Chest 2008, 134, 358–367. [Google Scholar] [CrossRef]
- Kim, H.; Tashkin, D.; Clements, P.J.; Li, G.; Brown, M.; Elashoff, R.; Gjertson, D.; Abtin, F.; Lynch, D.; Strollo, D.; et al. A computer-aided diagnosis system for quantitative scoring of extent of lung fibrosis in scleroderma patients. Clin. Exp. Rheumatol. 2010, 28, S26–S35. [Google Scholar]
- Andersen, C.A.; Holden, S.; Vela, J.; Rathleff, M.S.; Jensen, M.B. Point-of-Care Ultrasound in General Practice: A Systematic Review. Ann. Fam. Med. 2019, 17, 61–69. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Total (n = 58) | UIP (n = 35) | NSIP (n = 11) | Micronodules or Other Radiological Interstitial Abnormality (n = 12) | p |
|---|---|---|---|---|---|
| Male gender no. (%) | 34 (58.6) | 23 (65.7) | 5 (45.5) | 6 (50.0) | 0.391 |
| Age (years) | 58.97 ± 15.59 | 66.03 ± 11.37 a,b | 53.55 ± 11.37 | 43.33 ± 16.95 | <0.001 |
| Diagnosis of CTDs (connective tissue diseases) no. (%) | 10 (17.2) | 5 (14.3) | 3 (27.3) | 2 (16.7) | 0.609 |
| Oxygen saturation (SaO2) % | 95 (93–96) | 94 (91–96)b | 94 (93.5–95.5) c | 97 (95.5–97) | 0.010 |
| PaO2 (at rest) mmHg | 65.74 ± 13.21 | 64.6 ± 13.52 | 68.18 ± 10.44 | 69.53 ± 17.03 | 0.707 |
| DLCO (diffusing capacity of the lung for carbone monoxide) (%Predicted value) | 44.8 (31.45–53.05) | 40.2 (30.65–48.6) b | 42.8 (33.35–53.05) c | 67.7 (49.65–80.35) | 0.003 |
| Alveolar volume (VA) (%) | 62.59 ± 18.60 | 60.00 ± 16.72 b | 54.23 ± 18.64 | 78.46 ± 20.21 | 0.035 |
| HRCT(chest high-resolution computed tomography) score | 21.66 ± 7.79 | 23.94 ± 6.62 b | 22.64 ± 9.05 c | 14.08 ± 4.91 | <0.001 |
| Total number of B-lines score (total sum of B-lines) | 78.72 ± 44.31 | 101.77 ± 32.94 a,b | 63.91 ± 36.46 c | 25.08 ± 23.75 | <0.001 |
| Total number of positive chest areas score (with ≥ 3 B-lines) | 7.5 (4–10) | 9 (8–10) a,b | 7 (4–7) c | 0.5 (0–4) | <0.001 |
| Borg fatigue scale | 2 (0.5–3) | 2 (1–3) | 1 (0–2) | 1 (0–2.5) | 0.066 |
| Borg dyspnea scale | 0 (0–2) | 0.5 (0–2) | 0 (0–1) | 0 (0–1) | 0.488 |
| Pulmonary hypertension on echocardiographic exam mmHg | 34.98 ± 18.56 | 37.75 ± 19.19 | 32.75 ± 19.62 | 23.00 ± 6.71 | 0.249 |
| FVC (forced vital capacity) (L) | 2.63 ± 0.93 | 2.48 ± 0.69 b | 2.45 ± 1.01 | 3.31 ± 1.27 | 0.024 |
| FVC (%) | 76.91 ± 23.47 | 77.35 ± 22.07 | 65.20 ± 24.10 | 87.22 ± 24.06 | 0.086 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Man, M.A.; Dantes, E.; Domokos Hancu, B.; Bondor, C.I.; Ruscovan, A.; Parau, A.; Motoc, N.S.; Marc, M. Correlation between Transthoracic Lung Ultrasound Score and HRCT Features in Patients with Interstitial Lung Diseases. J. Clin. Med. 2019, 8, 1199. https://doi.org/10.3390/jcm8081199
Man MA, Dantes E, Domokos Hancu B, Bondor CI, Ruscovan A, Parau A, Motoc NS, Marc M. Correlation between Transthoracic Lung Ultrasound Score and HRCT Features in Patients with Interstitial Lung Diseases. Journal of Clinical Medicine. 2019; 8(8):1199. https://doi.org/10.3390/jcm8081199
Chicago/Turabian StyleMan, Milena Adina, Elena Dantes, Bianca Domokos Hancu, Cosmina Ioana Bondor, Alina Ruscovan, Adriana Parau, Nicoleta Stefania Motoc, and Monica Marc. 2019. "Correlation between Transthoracic Lung Ultrasound Score and HRCT Features in Patients with Interstitial Lung Diseases" Journal of Clinical Medicine 8, no. 8: 1199. https://doi.org/10.3390/jcm8081199