Diagnostics, Risk Factors, Treatment and Outcomes of Acute Kidney Injury in a New Paradigm

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Definition of AKI, Persistent AKI, and Renal Recovery after AKI
2.1. Definition of AKI
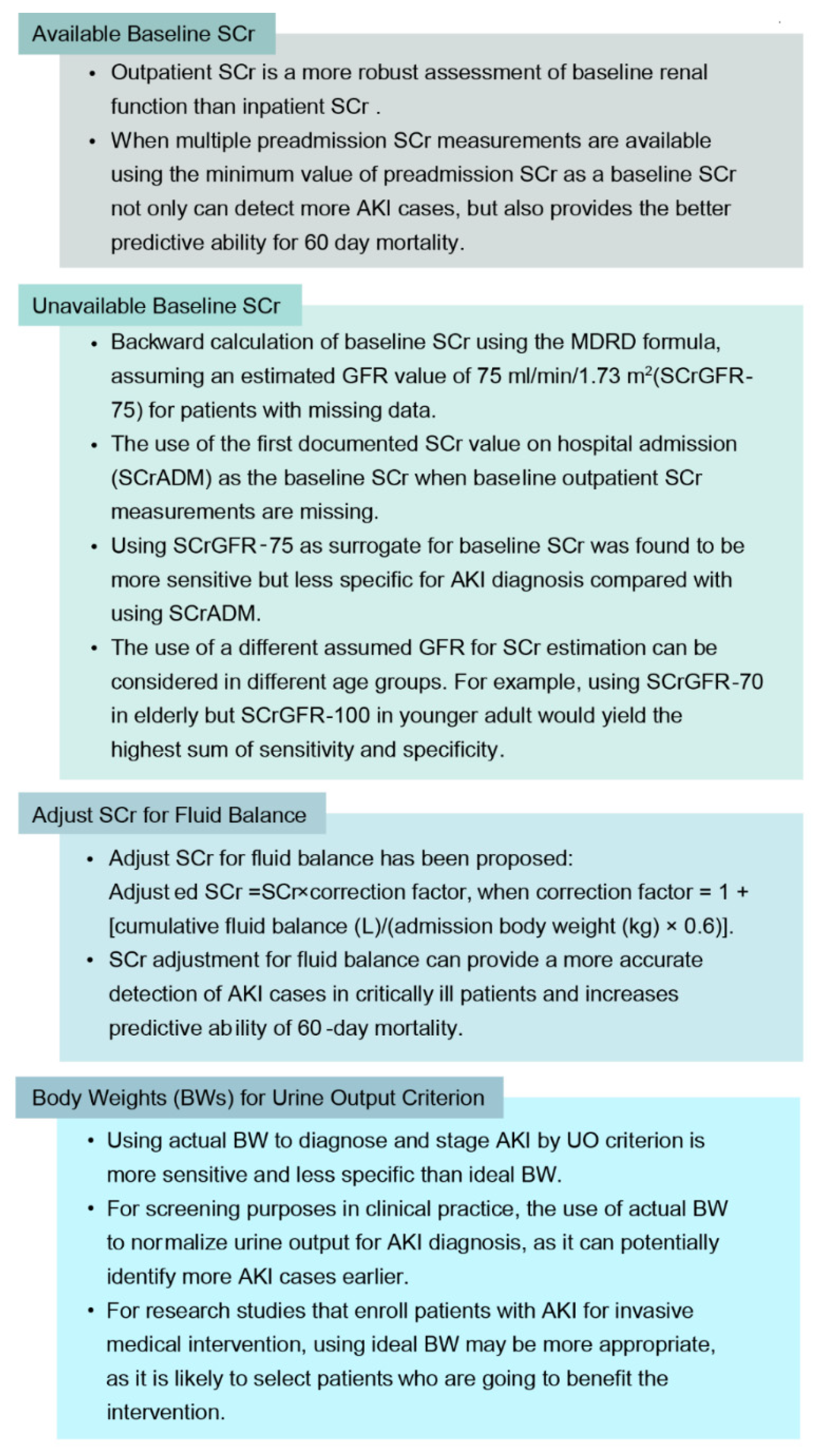
2.2. Baseline SCr, Adjust SCr for Fluid Balance, and Body Weights for Urine Output Criterion
2.3. Persistent AKI and Renal Recovery after AKI
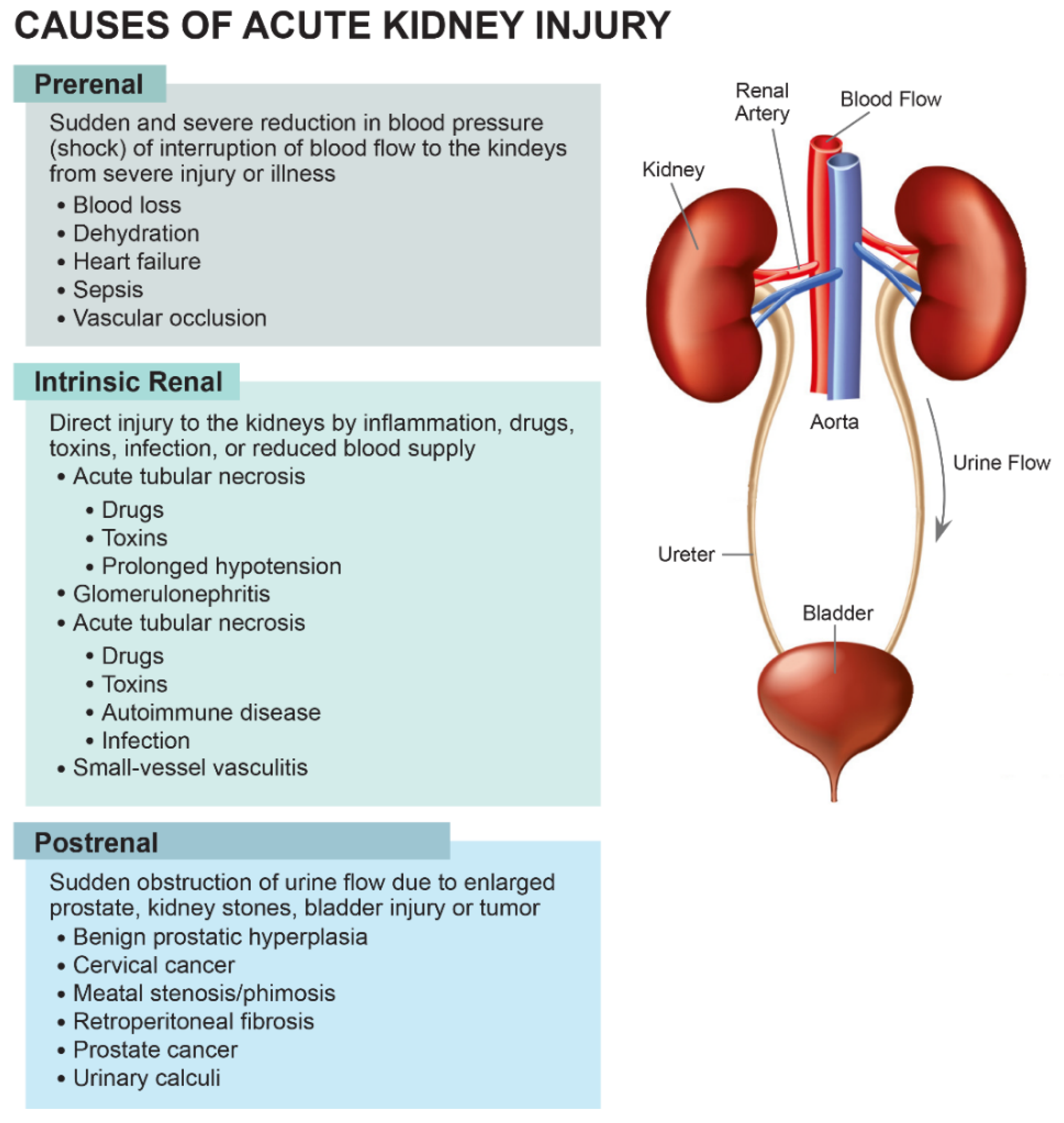
3. Causes and Diagnosis of AKI
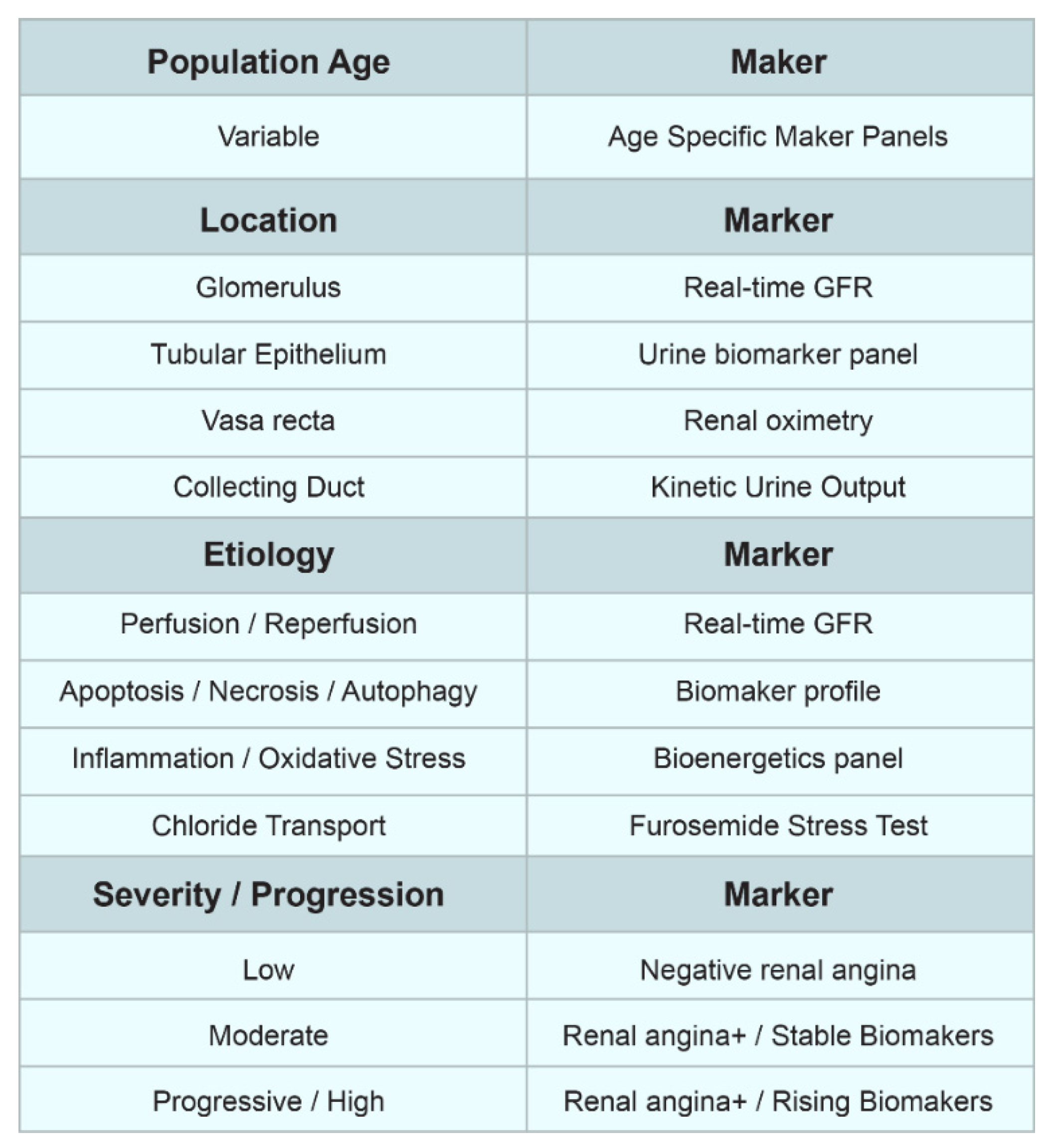
4. Biomarkers of Acute Kidney Injury (AKI)
5. Risk Factors
6. Outcomes and Mortality Risk among Patients with AKI
7. AKI Prevention and Management of AKI
7.1. AKI Prevention
7.2. Management of AKI
8. Potential Directions and Future Scope
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Levey, A.S.; James, M.T. Acute Kidney Injury. Ann. Intern. Med. 2017, 167, ITC66–ITC80. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Bellomo, R.; Kellum, J.A. Acute kidney injury. Lancet 2019, 394, 1949–1964. [Google Scholar] [CrossRef]
- Gameiro, J.; Agapito Fonseca, J.; Jorge, S.; Lopes, J.A. Acute Kidney Injury Definition and Diagnosis: A Narrative Review. J. Clin. Med. 2018, 7, 307. [Google Scholar] [CrossRef] [PubMed]
- Jadlowiec, C.; Smith, M.; Neville, M.; Mao, S.; Abdelwahab, D.; Reddy, K.; Moss, A.; Aqel, B.; Taner, T. Acute Kidney Injury Patterns following Transplantation of Steatotic Liver Allografts. J. Clin. Med. 2020, 9, 954. [Google Scholar] [CrossRef] [Green Version]
- Manohar, S.; Kompotiatis, P.; Thongprayoon, C.; Cheungpasitporn, W.; Herrmann, J.; Herrmann, S.M. Programmed cell death protein 1 inhibitor treatment is associated with acute kidney injury and hypocalcemia: Meta-analysis. Nephrol. Dial. Transplant. 2019, 34, 108–117. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Sakhuja, A.; Erickson, S.B. Admission hyperphosphatemia increases the risk of acute kidney injury in hospitalized patients. J. Nephrol. 2018, 31, 241–247. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Sakhuja, A.; Kashani, K. U-shape association of serum albumin level and acute kidney injury risk in hospitalized patients. PLoS ONE 2018, 13, e0199153. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Harrison, A.M.; Erickson, S.B. Elevated admission serum calcium phosphate product as an independent risk factor for acute kidney injury in hospitalized patients. Hosp. Pract. 2019, 47, 73–79. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Sakhuja, A.; Erickson, S.B. Admission calcium levels and risk of acute kidney injury in hospitalised patients. Int. J. Clin. Pract. 2018, 72, e13057. [Google Scholar] [CrossRef]
- Cheungpasitporn, W.; Thongprayoon, C.; Harrison, A.M.; Erickson, S.B. Admission hyperuricemia increases the risk of acute kidney injury in hospitalized patients. Clin. Kidney J. 2016, 9, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Cheungpasitporn, W.; Thongprayoon, C.; Erickson, S.B. Admission hypomagnesemia and hypermagnesemia increase the risk of acute kidney injury. Ren. Fail. 2015, 37, 1175–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, P.K.; Burdmann, E.A.; Mehta, R.L. Acute kidney injury: Global health alert. Kidney Int. 2013, 83, 372–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerdá, J.; Liu, K.D.; Cruz, D.N.; Jaber, B.L.; Koyner, J.L.; Heung, M.; Okusa, M.D.; Faubel, S. Promoting Kidney Function Recovery in Patients with AKI Requiring RRT. Clin. J. Am. Soc. Nephrol. 2015, 10, 1859–1867. [Google Scholar] [CrossRef] [PubMed]
- Silver, S.A.; Long, J.; Zheng, Y.; Chertow, G.M. Cost of Acute Kidney Injury in Hospitalized Patients. J. Hosp. Med. 2017, 12, 70–76. [Google Scholar] [CrossRef] [Green Version]
- Hansrivijit, P.; Lertjitbanjong, P.; Thongprayoon, C.; Cheungpasitporn, W.; Aeddula, N.R.; Salim, S.A.; Chewcharat, A.; Watthanasuntorn, K.; Srivali, N.; Mao, M.A.; et al. Acute Kidney Injury in Pediatric Patients on Extracorporeal Membrane Oxygenation: A Systematic Review and Meta-analysis. Medicines 2019, 6, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Shah, I.K.; Kashyap, R.; Park, S.J.; Kashani, K. Long-term Outcomes and Prognostic Factors for Patients Requiring Renal Replacement Therapy ater Cardiac Surgery. Mayo Clin. Proc. 2015, 90, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Silver, S.A.; Chertow, G.M. The Economic Consequences of Acute Kidney Injury. Nephron 2017, 137, 297–301. [Google Scholar] [CrossRef]
- Selby, N.M.; Kolhe, N.V.; McIntyre, C.W.; Monaghan, J.; Lawson, N.; Elliott, D.; Packington, R.; Fluck, R.J. Defining the cause of death in hospitalised patients with acute kidney injury. PLoS ONE 2012, 7, e48580. [Google Scholar] [CrossRef]
- Mehta, R.L.; Cerdá, J.; Burdmann, E.A.; Tonelli, M.; García-García, G.; Jha, V.; Susantitaphong, P.; Rocco, M.; Vanholder, R.; Sever, M.S.; et al. International Society of Nephrology’s 0by25 initiative for acute kidney injury (zero preventable deaths by 2025): A human rights case for nephrology. Lancet 2015, 385, 2616–2643. [Google Scholar] [CrossRef]
- Charlton, J.R.; Portilla, D.; Okusa, M.D. A basic science view of acute kidney injury biomarkers. Nephrol. Dial. Transplant. 2014, 29, 1301–1311. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, S.M.; Chawla, L.S.; Kane-Gill, S.L.; Hsu, R.K.; Kramer, A.A.; Goldstein, S.L.; Kellum, J.A.; Ronco, C.; Bagshaw, S.M. Utilizing electronic health records to predict acute kidney injury risk and outcomes: Workgroup statements from the 15(th) ADQI Consensus Conference. Can. J. Kidney Health Dis. 2016, 3, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheungpasitporn, W.; Kashani, K. Electronic Data Systems and Acute Kidney Injury. Contrib. Nephrol. 2016, 187, 73–83. [Google Scholar] [PubMed]
- Kellum, J.A. KDIGO clinical practice guideline for acute kidney injury, Section 2: AKI Definition. Kidney Int. Suppl. 2012, 2, 19–36. [Google Scholar]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute Dialysis Quality Initiative w. Acute renal failure—Definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [Green Version]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Kittanamongkolchai, W.; Srivali, N.; Ungprasert, P.; Kashani, K. Optimum methodology for estimating baseline serum creatinine for the acute kidney injury classification. Nephrology 2015, 20, 881–886. [Google Scholar] [CrossRef]
- Acosta-Ochoa, I.; Bustamante-Munguira, J.; Mendiluce-Herrero, A.; Bustamante-Bustamante, J.; Coca-Rojo, A. Impact on Outcomes across KDIGO-2012 AKI Criteria according to Baseline Renal Function. J. Clin. Med. 2019, 8, 1323. [Google Scholar] [CrossRef] [Green Version]
- Siew, E.D.; Ikizler, T.A.; Matheny, M.E.; Shi, Y.; Schildcrout, J.S.; Danciu, I.; Dwyer, J.P.; Srichai, M.; Hung, A.M.; Smith, J.P.; et al. Estimating baseline kidney function in hospitalized patients with impaired kidney function. Clin. J. Am. Soc. Nephrol. 2012, 7, 712–719. [Google Scholar] [CrossRef]
- Siew, E.D.; Matheny, M.E.; Ikizler, T.A.; Lewis, J.B.; Miller, R.A.; Waitman, L.R.; Go, A.S.; Parikh, C.R.; Peterson, J.F. Commonly used surrogates for baseline renal function affect the classification and prognosis of acute kidney injury. Kidney Int. 2010, 77, 536–542. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Harrison, A.; Kittanamongkolchai, W.; Ungprasert, P.; Srivali, N.; Akhoundi, A.; Kashani, K.B. The comparison of the commonly used surrogates for baseline renal function in acute kidney injury diagnosis and staging. BMC Nephrol. 2016, 17, 6. [Google Scholar] [CrossRef] [Green Version]
- Ad-hoc working group of ERBP; Fliser, D.; Laville, M.; Covic, A.; Fouque, D.; Vanholder, R.; Juillard, L.; Van Biesen, W. A European Renal Best Practice (ERBP) position statement on the Kidney Disease Improving Global Outcomes (KDIGO) clinical practice guidelines on acute kidney injury: Part 1: Definitions, conservative management and contrast-induced nephropathy. Nephrol. Dial. Transplant. 2012, 27, 4263–4272. [Google Scholar]
- Pickering, J.W.; Endre, Z.H. Back-calculating baseline creatinine with MDRD misclassifies acute kidney injury in the intensive care unit. Clin. J. Am. Soc. Nephrol. 2010, 5, 1165–1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, C.Y.; Ordoñez, J.D.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Go, A.S. The risk of acute renal failure in patients with chronic kidney disease. Kidney Int. 2008, 74, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spoorenberg, S.M.; Meijvis, S.C.; Navis, G.; Bos, W.J. Age- and gender-adjusted eGFR to estimate baseline creatinine for RIFLE criteria. NDT Plus. 2011, 4, 365–366. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Srivali, N.; Ungprasert, P.; Kittanamongkolchai, W.; Kashani, K. The impact of fluid balance on diagnosis, staging and prediction of mortality in critically ill patients with acute kidney injury. J. Nephrol. 2016, 29, 221–227. [Google Scholar] [CrossRef]
- Liu, K.D.; Thompson, B.T.; Ancukiewicz, M.; Steingrub, J.S.; Douglas, I.S.; Matthay, M.A.; Wright, P.; Peterson, M.W.; Rock, P.; Hyzy, R.C.; et al. Acute kidney injury in patients with acute lung injury: Impact of fluid accumulation on classification of acute kidney injury and associated outcomes. Crit. Care Med. 2011, 39, 2665–2671. [Google Scholar] [CrossRef] [Green Version]
- Macedo, E.; Bouchard, J.; Soroko, S.H.; Chertow, G.M.; Himmelfarb, J.; Ikizler, T.A.; Paganini, E.P.; Mehta, R.L. Fluid accumulation, recognition and staging of acute kidney injury in critically-ill patients. Crit. Care 2010, 14, R82. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Akhoundi, A.; Ahmed, A.H.; Kashani, K.B. Actual versus ideal body weight for acute kidney injury diagnosis and classification in critically ill patients. BMC Nephrol. 2014, 15, 176. [Google Scholar] [CrossRef] [Green Version]
- Kellum, J.A. Persistent Acute Kidney Injury. Crit. Care Med. 2015, 43, 1785–1786. [Google Scholar] [CrossRef] [Green Version]
- Perinel, S.; Vincent, F.; Lautrette, A.; Dellamonica, J.; Mariat, C.; Zeni, F.; Cohen, Y.; Tardy, B.; Souweine, B.; Darmon, M. Transient and Persistent Acute Kidney Injury and the Risk of Hospital Mortality in Critically Ill Patients: Results of a Multicenter Cohort Study. Crit. Care Med. 2015, 43, e269–e275. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Srivali, N.; Kittanamongkolchai, W.; Harrison, A.; Greason, K.L.; Kashani, K.B. Persistent acute kidney injury following transcatheter aortic valve replacement. J. Card. Surg. 2017, 32, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, A.; Kogan, E.; Hammerman, H.; Markiewicz, W.; Aronson, D. The impact of transient and persistent acute kidney injury on long-term outcomes after acute myocardial infarction. Kidney Int. 2009, 76, 900–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.S.; A Kim, Y.; Kim, M.J.; Kang, Y.U.; Kim, C.S.; Bae, E.H.; Ma, S.K.; Ahn, Y.; Jeong, M.H.; Kim, S.W. Relation between transient or persistent acute kidney injury and long-term mortality in patients with myocardial infarction. Am. J. Cardiol. 2013, 112, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Wi, J.; Ko, Y.G.; Kim, J.S.; Kim, B.K.; Choi, D.; Ha, J.W.; Hong, M.K. Impact of contrast-induced acute kidney injury with transient or persistent renal dysfunction on long-term outcomes of patients with acute myocardial infarction undergoing percutaneous coronary intervention. Heart 2011, 97, 1753–1757. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.S.; Bae, E.H.; Ma, S.K.; Kweon, S.S.; Kim, S.W. Impact of Transient and Persistent Acute Kidney Injury on Chronic Kidney Disease Progression and Mortality after Gastric Surgery for Gastric Cancer. PLoS ONE 2016, 11, e0168119. [Google Scholar] [CrossRef]
- Chawla, L.S.; Bellomo, R.; Bihorac, A.; Goldstein, S.L.; Siew, E.D.; Bagshaw, S.M.; Bittleman, D.; Cruz, D.; Endre, Z.H.; Fitzgerald, R.L.; et al. Acute kidney disease and renal recovery: Consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat. Rev. Nephrol. 2017, 13, 241–257. [Google Scholar] [CrossRef] [Green Version]
- Kellum, J.A.; Sileanu, F.E.; Bihorac, A.; Hoste, E.A.; Chawla, L.S. Recovery after Acute Kidney Injury. Am. J. Respir. Crit. Care Med. 2017, 195, 784–791. [Google Scholar] [CrossRef] [Green Version]
- Bagshaw, S.M. Epidemiology of renal recovery after acute renal failure. Curr. Opin. Crit. Care 2006, 12, 544–550. [Google Scholar] [CrossRef]
- Pannu, N.; James, M.; Hemmelgarn, B.; Klarenbach, S. Association between AKI, recovery of renal function, and long-term outcomes after hospital discharge. Clin. J. Am. Soc. Nephrol. 2013, 8, 194–202. [Google Scholar] [CrossRef]
- Swaminathan, M.; Hudson, C.C.; Phillips-Bute, B.G.; Patel, U.D.; Mathew, J.P.; Newman, M.F.; Milano, C.A.; Shaw, A.; Stafford-Smith, M. Impact of early renal recovery on survival after cardiac surgery-associated acute kidney injury. Ann. Thorac. Surg. 2010, 89, 1098–1104. [Google Scholar] [CrossRef]
- Wajda, J.; Dumnicka, P.; Sporek, M.; Maziarz, B.; Kolber, W.; Ząbek-Adamska, A.; Ceranowicz, P.; Kuźniewski, M.; Kuśnierz-Cabala, B. Does Beta-Trace Protein (BTP) Outperform Cystatin C as a Diagnostic Marker of Acute Kidney Injury Complicating the Early Phase of Acute Pancreatitis? J. Clin. Med. 2020, 9, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antal, O.; Ștefănescu, E.; Mleșnițe, M.; Bălan, A.M.; Caziuc, A.; Hagău, N. Hemodynamic Predictors for Sepsis-Induced Acute Kidney Injury: A Preliminary Study. J. Clin. Med. 2020, 9, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.H.; Sol, I.S.; Park, J.T.; Kim, J.H.; Shin, J.W.; Park, M.; Lee, J.; Kim, Y.H.; Kim, K.W.; Shin, J.I.; et al. Continuous Renal Replacement Therapy (CRRT) in Children and the Specialized CRRT Team: A 14-Year Single-Center Study. J. Clin. Med. 2019, 9, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.-C.; Chang, C.-H.; Cheng, Y.-L.; Kuo, G.; Chen, S.-W.; Li, Y.-J.; Chen, Y.; Tian, Y.-C. Diagnostic Performance of Cyclophilin A in Cardiac Surgery-Associated Acute Kidney Injury. J. Clin. Med. 2019, 9, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, S.; Orieux, A.; Clouzeau, B.; Rigothier, C.; Combe, C.; Gruson, D.; Boyer, A. The Incidence of Chronic Kidney Disease Three Years after Non-Severe Acute Kidney Injury in Critically Ill Patients: A Single-Center Cohort Study. J. Clin. Med. 2019, 8, 2215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.-K.; Wu, C.-L.; Su, T.-C.; Kou, Y.R.; Kor, C.-T.; Lee, T.-S.; Tarng, D.-C. Renal Tubular TRPA1 as a Risk Factor for Recovery of Renal Function from Acute Tubular Necrosis. J. Clin. Med. 2019, 8, 2187. [Google Scholar] [CrossRef] [Green Version]
- Averdunk, L.; Fitzner, C.; Levkovich, T.; Leaf, D.E.; Sobotta, M.; Vieten, J.; Ochi, A.; Moeckel, G.; Marx, G.; Stoppe, C.; et al. Secretory Leukocyte Protease Inhibitor (SLPI)-A Novel Predictive Biomarker of Acute Kidney Injury after Cardiac Surgery: A Prospective Observational Study. J. Clin. Med. 2019, 8, 1931. [Google Scholar] [CrossRef] [Green Version]
- Wu, V.C.; Chueh, S.J.; Chang, J.T.; Hsu, B.G.; Ostermann, M.; Chu, T.S. Acute Kidney Injury and Septic Shock-Defined by Updated Sepsis-3 Criteria in Critically Ill Patients. J. Clin. Med. 2019, 8, 1731. [Google Scholar] [CrossRef] [Green Version]
- Lertjitbanjong, P.; Thongprayoon, C.; Cheungpasitporn, W.; O’Corragain, O.A.; Srivali, N.; Bathini, T.; Watthanasuntorn, K.; Aeddula, N.R.; Salim, S.A.; Ungprasert, P.; et al. Acute Kidney Injury after Lung Transplantation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 1731. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-J.; Bae, J.; Kwon, Y.; Jang, H.S.; Yoo, S.; Jeong, C.W.; Kim, J.-T.; Kim, W.H. General Anesthetic Agents and Renal Function after Nephrectomy. J. Clin. Med. 2019, 8, 1530. [Google Scholar] [CrossRef] [Green Version]
- Yoon, H.-K.; Lee, H.-J.; Yoo, S.; Park, S.-K.; Kwon, Y.; Jun, K.; Jeong, C.W.; Kim, W.H. Acute Kidney Injury Adjusted for Parenchymal Mass Reduction and Long-Term Renal Function after Partial Nephrectomy. J. Clin. Med. 2019, 8, 1482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabbian, F.; Savriè, C.; De Giorgi, A.; Cappadona, R.; Simone, D.; Boari, B.; Storari, A.; Gallerani, M.; Manfredini, R.; De Giorgi, A.; et al. Acute Kidney Injury and In-Hospital Mortality: A Retrospective Analysis of a Nationwide Administrative Database of Elderly Subjects in Italy. J. Clin. Med. 2019, 8, 1371. [Google Scholar] [CrossRef] [Green Version]
- Doyle, J.; Sarnowski, A.; Saadat, F.; Samuels, T.L.; Huddart, S.; Quiney, N.; Dickinson, M.C.; McCormick, B.; Debrunner, R.; Preece, J.; et al. Does the Implementation of a Quality Improvement Care Bundle Reduce the Incidence of Acute Kidney Injury in Patients Undergoing Emergency Laparotomy? J. Clin. Med. 2019, 8, 1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, M.J.; Tsai, S.F.; Lee, C.T.; Wu, C.Y. The Predictive Value of Hyperuricemia on Renal Outcome after Contrast-Enhanced Computerized Tomography. J. Clin. Med. 2019, 8, 1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Lertjitbanjong, P.; Aeddula, N.R.; Bathini, T.; Watthanasuntorn, K.; Srivali, N.; Mao, M.A.; Kashani, K. Incidence and Impact of Acute Kidney Injury in Patients Receiving Extracorporeal Membrane Oxygenation: A Meta-Analysis. J. Clin. Med. 2019, 8, 981. [Google Scholar] [CrossRef] [Green Version]
- Ortiz-Soriano, V.; Donaldson, K.; Du, G.; Li, Y.; Lambert, J.; Cleland, D.; Thornton, A.; Fanucchi, L.C.; Huaman, M.A.; Neyra, J.A. Incidence and Cost of Acute Kidney Injury in Hospitalized Patients with Infective Endocarditis. J. Clin. Med. 2019, 8, 927. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-J.; Park, H.-S.; Go, Y.-J.; Koh, W.U.; Kim, H.; Song, J.-G.; Ro, Y.-J. Effect of Anesthetic Technique on the Occurrence of Acute Kidney Injury after Total Knee Arthroplasty. J. Clin. Med. 2019, 8, 778. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.Y.; Hong, J.H.; Koh, D.H.; Lee, J.; Nam, H.J.; Kim, S.Y. Effect of Diabetes Mellitus on Acute Kidney Injury after Minimally Invasive Partial Nephrectomy: A Case-Matched Retrospective Analysis. J. Clin. Med. 2019, 8, 468. [Google Scholar] [CrossRef] [Green Version]
- Oh, T.K.; Song, I.A.; Jeon, Y.T.; Jo, Y.H. Fluctuations in Serum Chloride and Acute Kidney Injury among Critically Ill Patients: A Retrospective Association Study. J. Clin. Med. 2019, 8, 447. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Kaewput, W.; Thamcharoen, N.; Bathini, T.; Watthanasuntorn, K.; Lertjitbanjong, P.; Sharma, K.; Salim, S.A.; Ungprasert, P.; Wijarnpreecha, K.; et al. Incidence and Impact of Acute Kidney Injury after Liver Transplantation: A Meta-Analysis. J. Clin. Med. 2019, 8, 372. [Google Scholar] [CrossRef] [Green Version]
- Vilander, L.M.; Vaara, S.T.; Kaunisto, M.A.; Pettilä, V. Common Inflammation-Related Candidate Gene Variants and Acute Kidney Injury in 2647 Critically Ill Finnish Patients. J. Clin. Med. 2019, 8, 342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaewput, W.; Thongprayoon, C.; Rangsin, R.; Mao, M.A.; Satirapoj, B.; Cheungpasitporn, W. The association between renal function and neurological diseases in type 2 diabetes: A multicenter nationwide cross-sectional study. Hosp. Pract. 2019, 47, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.H.; Lee, H.C.; Lim, L.; Ryu, H.G.; Jung, C.W. Intraoperative Oliguria with Decreased SvO2 Predicts Acute Kidney Injury after Living Donor Liver Transplantation. J. Clin. Med. 2018, 8, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, T.K.; Song, I.A.; Cho, Y.J.; Lim, C.; Jeon, Y.T.; Bae, H.J.; Jo, Y.H. Preadmission Statin Therapy Is Associated with a Lower Incidence of Acute Kidney Injury in Critically Ill Patients: A Retrospective Observational Study. J. Clin. Med. 2018, 8, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.-S.; Kim, Y.J.; Ryoo, S.M.; Sohn, C.H.; Seo, D.W.; Ahn, S.; Lim, K.S.; Kim, W. One--Year Progression and Risk Factors for the Development of Chronic Kidney Disease in Septic Shock Patients with Acute Kidney Injury: A Single-Centre Retrospective Cohort Study. J. Clin. Med. 2018, 7, 554. [Google Scholar] [CrossRef] [Green Version]
- Zelt, J.G.E.; Mielniczuk, L.M.; Liu, P.P.; Dupuis, J.-Y.; Chih, S.; Akbari, A.; Sun, L. Utility of Novel Cardiorenal Biomarkers in the Prediction and Early Detection of Congestive Kidney Injury Following Cardiac Surgery. J. Clin. Med. 2018, 7, 540. [Google Scholar] [CrossRef] [Green Version]
- Marouli, D.; Stylianou, K.; Papadakis, E.; Kroustalakis, N.; Kolyvaki, S.; Papadopoulos, G.; Ioannou, C.; Papaioannou, A.; Daphnis, E.; Georgopoulos, D.; et al. Preoperative Albuminuria and Intraoperative Chloride Load: Predictors of Acute Kidney Injury following Major Abdominal Surgery. J. Clin. Med. 2018, 7, 431. [Google Scholar] [CrossRef] [Green Version]
- Kee, Y.K.; Kim, D.; Kim, S.-J.; Kang, D.-H.; Choi, K.B.; Oh, H.J.; Ryu, D.-R. Factors Associated with Early Mortality in Critically Ill Patients following the Initiation of Continuous Renal Replacement Therapy. J. Clin. Med. 2018, 7, 334. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-C.; Yoon, H.-K.; Nam, K.; Cho, Y.J.; Kim, T.K.; Kim, W.H.; Bahk, J.-H. Derivation and Validation of Machine Learning Approaches to Predict Acute Kidney Injury after Cardiac Surgery. J. Clin. Med. 2018, 7, 322. [Google Scholar] [CrossRef] [Green Version]
- Douvris, A.; Zeid, K.; Hiremath, S.; Brown, P.A.; Sood, M.M.; Arkoub, R.A.; Malhi, G.; Clark, E. Safety Lapses Prior to Initiation of Hemodialysis for Acute Kidney Injury in Hospitalized Patients: A Patient Safety Initiative. J. Clin. Med. 2018, 7, 317. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-Y.; Wu, V.-C.; Huang, W.-C.; Yeh, Y.-C.; Wu, M.-S.; Huang, C.-C.; Wu, M.-S.; Fang, J.-T.; Wu, C.-J.; Nsarf, T.; et al. Norepinephrine Administration Is Associated with Higher Mortality in Dialysis Requiring Acute Kidney Injury Patients with Septic Shock. J. Clin. Med. 2018, 7, 274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiao, C.-C.; Kan, W.-C.; Wang, J.-J.; Lin, Y.-F.; Chen, L.; Chueh, E.; Huang, Y.-T.; Chiang, W.-P.; Tseng, L.-J.; Wang, C.-H.; et al. Risk of Incident Non-Valvular Atrial Fibrillation after Dialysis-Requiring Acute Kidney Injury. J. Clin. Med. 2018, 7, 248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.-H.; Chang, H.-M.; Wang, C.-Y.; Chen, L.; Chen, L.W.; Lai, C.-H.; Kuo, S.-W.; Wang, H.-C.; Wu, V.-C. Long-Term Outcomes in Patients with Incident Chronic Obstructive Pulmonary Disease after Acute Kidney Injury: A Competing-Risk Analysis of a Nationwide Cohort. J. Clin. Med. 2018, 7, 237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awdishu, L.; Connor, A.I.; Bouchard, J.; Macedo, E.; Chertow, G.M.; Mehta, R.L. Use of Estimating Equations for Dosing Antimicrobials in Patients with Acute Kidney Injury Not Receiving Renal Replacement Therapy. J. Clin. Med. 2018, 7, 211. [Google Scholar] [CrossRef] [Green Version]
- Wu, V.-C.; Shiao, C.-C.; Chi, N.-H.; Wang, C.-H.; Chueh, J.S.; Liou, H.-H.; Spapen, H.; Honore, P.M.; Chu, T.-S. Outcome Prediction of Acute Kidney Injury Biomarkers at Initiation of Dialysis in Critical Units. J. Clin. Med. 2018, 7, 202. [Google Scholar] [CrossRef] [Green Version]
- Selby, A.R.; Hall, R.G. Utilizing the Patient Care Process to Minimize the Risk of Vancomycin-Associated Nephrotoxicity. J. Clin. Med. 2019, 8, 781. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.J.; Fan, P.C.; Kou, G.; Chang, S.W.; Chen, Y.T.; Lee, C.C.; Chang, C.H. Meta-Analysis: Urinary Calprotectin for Discrimination of Intrinsic and Prerenal Acute Kidney Injury. J. Clin. Med. 2019, 8, 74. [Google Scholar] [CrossRef] [Green Version]
- Abassi, Z.; Rosen, S.; Lamothe, S.; Heyman, S.N. Why Have Detection, Understanding and Management of Kidney Hypoxic Injury Lagged Behind those for the Heart? J. Clin. Med. 2019, 8, 267. [Google Scholar] [CrossRef] [Green Version]
- Case, J.; Khan, S.; Khalid, R.; Khan, A. Epidemiology of acute kidney injury in the intensive care unit. Crit. Care Res. Pract. 2013, 2013, 479730. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Lertjitbanjong, P.; Hansrivijit, P.; Crisafio, A.; Mao, M.A.; Watthanasuntorn, K.; Aeddula, N.R.; Bathini, T.; Kaewput, W.; Cheungpasitporn, W. Acute Kidney Injury in Patients Undergoing Cardiac Transplantation: A Meta-Analysis. Medicines 2019, 6, 108. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Srivali, N.; Kittanamongkolchai, W.; Greason, K.L.; Kashani, K.B. Incidence and risk factors of acute kidney injury following transcatheter aortic valve replacement. Nephrology 2016, 21, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- Kanduri, S.R.; Cheungpasitporn, W.; Thongprayoon, C.; Bathini, T.; Kovvuru, K.; Garla, V.; Medaura, J.; Vaitla, P.; Kashani, K.B. Incidence and Mortality of Acute Kidney Injury in Patients Undergoing Hematopoietic Stem Cell Transplantation: A Systematic Review and Meta-analysis. QJM Int. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lagny, M.-G.; Jouret, F.; Koch, J.-N.; Blaffart, F.; Donneau, A.-F.; Albert, A.; Roediger, L.; Krzesinski, J.-M.; Defraigne, J.-O. Incidence and outcomes of acute kidney injury after cardiac surgery using either criteria of the RIFLE classification. BMC Nephrol. 2015, 16, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vives, M.; Hernandez, A.; Parramon, F.; Estanyol, N.; Pardina, B.; Muñoz, A.; Alvarez, P.; Hernandez, C. Acute kidney injury after cardiac surgery: Prevalence, impact and management challenges. Int. J. Nephrol. Renovasc. Dis. 2019, 12, 153–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mårtensson, J.; Bellomo, R. Sepsis-Induced Acute Kidney Injury. Crit. Care Clin. 2015, 31, 649–660. [Google Scholar] [CrossRef] [PubMed]
- Panitchote, A.; Mehkri, O.; Hastings, A.; Hanane, T.; Demirjian, S.; Torbic, H.; Mireles-Cabodevila, E.; Krishnan, S.; Duggal, A. Factors associated with acute kidney injury in acute respiratory distress syndrome. Ann. Intensive Care 2019, 9, 74. [Google Scholar] [CrossRef]
- Darmon, M.; Clec’H, C.; Adrie, C.; Argaud, L.; Allaouchiche, B.; Azoulay, E.; Bouadma, L.; Garrouste-Orgeas, M.; Haouache, H.; Schwebel, C.; et al. Acute respiratory distress syndrome and risk of AKI among critically ill patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 1347–1353. [Google Scholar] [CrossRef] [Green Version]
- Wijarnpreecha, K.; Thongprayoon, C.; Edmonds, P.J.; Cheungpasitporn, W. Associations of sugar- and artificially sweetened soda with nonalcoholic fatty liver disease: A systematic review and meta-analysis. QJM 2016, 109, 461–466. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Srivali, N.; Ungprasert, P.; Kittanamongkolchai, W.; Greason, K.L.; Kashani, K.B. Acute kidney injury after transcatheter aortic valve replacement: A systematic review and meta-analysis. Am. J. Nephrol. 2015, 41, 372–382. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Lin, J.; Mao, M.A.; Qian, Q. Acute kidney injury in octogenarians after heart valve replacement surgery: A study of two periods over the last decade. Clin. Kidney J. 2017, 10, 648–654. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Thamcharoen, N.; Ungprasert, P.; Kittanamongkolchai, W.; Mao, M.A.; Sakhuja, A.; Greason, K.L.; Kashani, K.B. Association of frailty status with acute kidney injury and mortality after transcatheter aortic valve replacement: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0177157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Srivali, N.; Kittanamongkolchai, W.; Sakhuja, A.; Greason, K.L.; Kashani, K.B. The association between renal recovery after acute kidney injury and long-term mortality after transcatheter aortic valve replacement. PLoS ONE 2017, 12, e0183350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakhuja, A.; Kashani, K.; Schold, J.; Cheungpasitporn, W.; Soltesz, E.; Demirjian, S. Hospital procedure volume does not predict acute kidney injury after coronary artery bypass grafting-a nationwide study. Clin. Kidney J. 2017, 10, 769–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Srivali, N.; Harrison, A.M.; Gunderson, T.M.; Kittanamongkolchai, W.; Greason, K.L.; Kashani, K.B. AKI after Transcatheter or Surgical Aortic Valve Replacement. J. Am. Soc. Nephrol. 2016, 27, 1854–1860. [Google Scholar] [CrossRef]
- Muriithi, A.K.; Nasr, S.H.; Leung, N. Utility of urine eosinophils in the diagnosis of acute interstitial nephritis. Clin. J. Am. Soc. Nephrol. 2013, 8, 1857–1862. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, M.T.; Maynard, S.E.; Kimmel, P.L. Misapplications of commonly used kidney equations: Renal physiology in practice. Clin. J. Am. Soc. Nephrol. 2009, 4, 528–534. [Google Scholar] [CrossRef] [Green Version]
- Chawla, L.S.; Davison, D.; Brasha-Mitchell, E.; Koyner, J.L.; Arthur, J.; Shaw, A.; Tumlin, J.; A Trevino, S.; Kimmel, P.L.; Seneff, M.G. Development and standardization of a furosemide stress test to predict the severity of acute kidney injury. Crit. Care 2013, 17, R207. [Google Scholar] [CrossRef] [Green Version]
- Koyner, J.L.; Davison, D.L.; Brasha-Mitchell, E.; Chalikonda, D.M.; Arthur, J.; Shaw, A.; Tumlin, J.A.; Trevino, S.A.; Bennett, M.R.; Kimmel, P.L.; et al. Furosemide stress test and biomarkers for the prediction of AKI severity. J. Am. Soc. Nephrol. 2015, 26, 2023–2031. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Kashani, K. Serum creatinine level, a surrogate of muscle mass, predicts mortality in critically ill patients. J. Thorac. Dis. 2016, 8, E305–E311. [Google Scholar] [CrossRef] [Green Version]
- Kashani, K.; Cheungpasitporn, W.; Ronco, C. Biomarkers of acute kidney injury: The pathway from discovery to clinical adoption. Clin. Chem. Lab Med. 2017, 55, 1074–1089. [Google Scholar] [CrossRef]
- Capasso, A.; Benigni, A.; Capitanio, U.; Danesh, F.R.; Di Marzo, V.; Gesualdo, L.; Grandaliano, G.; Jaimes, E.A.; Malyszko, J.; Perazella, M.A.; et al. Summary of the International Conference on Onco-Nephrology: An emerging field in medicine. Kidney Int. 2019, 96, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Parikh, C.R.; Coca, S.G.; Thiessen-Philbrook, H.; Shlipak, M.G.; Koyner, J.L.; Wang, Z.; Edelstein, C.L.; Devarajan, P.; Patel, U.D.; Zappitelli, M.; et al. Postoperative biomarkers predict acute kidney injury and poor outcomes after adult cardiac surgery. J. Am. Soc. Nephrol. 2011, 22, 1748–1757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siew, E.D.; Ware, L.B.; Bian, A.; Shintani, A.; Eden, S.K.; Wickersham, N.; Cripps, B.; Ikizler, T.A. Distinct injury markers for the early detection and prognosis of incident acute kidney injury in critically ill adults with preserved kidney function. Kidney Int. 2013, 84, 786–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srisawat, N.; Wen, X.; Lee, M.; Kong, L.; Elder, M.; Carter, M.; Unruh, M.; Finkel, K.; Vijayan, A.; Ramkumar, M.; et al. Urinary biomarkers and renal recovery in critically ill patients with renal support. Clin. J. Am. Soc. Nephrol. 2011, 6, 1815–1823. [Google Scholar] [CrossRef]
- Damman, K.; Masson, S.; Hillege, H.L.; Maggioni, A.P.; Voors, A.A.; Opasich, C.; Van Veldhuisen, D.J.; Montagna, L.; Cosmi, F.; Tognoni, G.; et al. Clinical outcome of renal tubular damage in chronic heart failure. Eur. Heart J. 2011, 32, 2705–2712. [Google Scholar] [CrossRef] [Green Version]
- Hall, I.E.; Yarlagadda, S.G.; Coca, S.G.; Wang, Z.; Doshi, M.; Devarajan, P.; Han, W.K.; Marcus, R.J.; Parikh, C.R. IL-18 and urinary NGAL predict dialysis and graft recovery after kidney transplantation. J. Am. Soc. Nephrol. 2010, 21, 189–197. [Google Scholar] [CrossRef]
- Nauta, F.L.; Bakker, S.J.L.; Van Oeveren, W.; Navis, G.; Van Der Heide, J.J.H.; Van Goor, H.; De Jong, P.E.; Gansevoort, R.T. Albuminuria, proteinuria, and novel urine biomarkers as predictors of long-term allograft outcomes in kidney transplant recipients. Am. J. Kidney Dis. 2011, 57, 733–743. [Google Scholar] [CrossRef]
- Zhang, W.R.; Garg, A.X.; Coca, S.G.; Devereaux, P.J.; Eikelboom, J.; Kavsak, P.; McArthur, E.; Thiessen-Philbrook, H.; Shortt, C.; Shlipak, M.; et al. Plasma IL-6 and IL-10 Concentrations Predict AKI and Long-Term Mortality in Adults after Cardiac Surgery. J. Am. Soc. Nephrol. 2015, 26, 3123–3132. [Google Scholar] [CrossRef] [Green Version]
- Arthur, J.; Hill, E.G.; Alge, J.; Lewis, E.C.; Neely, B.A.; Janech, M.G.; Tumlin, J.A.; Chawla, L.S.; Shaw, A. Evaluation of 32 urine biomarkers to predict the progression of acute kidney injury after cardiac surgery. Kidney Int. 2014, 85, 431–438. [Google Scholar] [CrossRef] [Green Version]
- Parikh, C.R.; Abraham, E.; Ancukiewicz, M.; Edelstein, C.L. Urine IL-18 is an early diagnostic marker for acute kidney injury and predicts mortality in the intensive care unit. J. Am. Soc. Nephrol. 2005, 16, 3046–3052. [Google Scholar] [CrossRef] [Green Version]
- Nejat, M.; Pickering, J.W.; Walker, R.J.; Westhuyzen, J.; Shaw, G.M.; Frampton, C.M.; Endre, Z.H. Urinary cystatin C is diagnostic of acute kidney injury and sepsis, and predicts mortality in the intensive care unit. Crit. Care 2010, 14, R85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doi, K.; Negishi, K.; Ishizu, T.; Katagiri, D.; Fujita, T.; Matsubara, T.; Yahagi, N.; Sugaya, T.; Noiri, E. Evaluation of new acute kidney injury biomarkers in a mixed intensive care unit. Crit. Care Med. 2011, 39, 2464–2469. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.; Larsson, A.; Venge, P.; Bellomo, R.; Martensson, J. Assessment of cell-cycle arrest biomarkers to predict early and delayed acute kidney injury. Dis. Markers 2015, 2015, 158658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meersch, M.; Schmidt, C.; Van Aken, H.; Martens, S.; Rossaint, J.; Singbartl, K.; Goerlich, D.; Kellum, J.A.; Zarbock, A. Urinary TIMP-2 and IGFBP7 as early biomarkers of acute kidney injury and renal recovery following cardiac surgery. PLoS ONE 2014, 9, e93460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heller, F.; Frischmann, S.; Grunbaum, M.; Zidek, W.; Westhoff, T.H. Urinary calprotectin and the distinction between prerenal and intrinsic acute kidney injury. Clin. J. Am. Soc. Nephrol. 2011, 6, 2347–2355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Chen, C.; Tian, J.; Zha, Y.; Xiong, Y.; Sun, Z.; Chen, P.; Li, J.; Yang, T.; Ma, C.; et al. Urinary Angiotensinogen Level Predicts AKI in Acute Decompensated Heart Failure: A Prospective, Two-Stage Study. J. Am. Soc. Nephrol. 2015, 26, 2032–2041. [Google Scholar] [CrossRef]
- Du, J.; Cao, X.; Zou, L.; Chen, Y.; Guo, J.; Chen, Z.; Hu, S.-S.; Zheng, Z. MicroRNA-21 and risk of severe acute kidney injury and poor outcomes after adult cardiac surgery. PLoS ONE 2013, 8, e63390. [Google Scholar] [CrossRef]
- Leblanc, M.; Kellum, J.A.; Gibney, R.T.; Lieberthal, W.; Tumlin, J.; Mehta, R. Risk factors for acute renal failure: Inherent and modifiable risks. Curr. Opin. Crit. Care 2005, 11, 533–536. [Google Scholar] [CrossRef]
- Cheungpasitporn, W.; Thongprayoon, C.; Kashani, K. Transcatheter Aortic Valve Replacement: A Kidney’s Perspective. J. Ren. Inj. Prev. 2016, 5, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Cartin-Ceba, R.; Kashiouris, M.; Plataki, M.; Kor, D.J.; Gajic, O.; Casey, E.T. Risk factors for development of acute kidney injury in critically ill patients: A systematic review and meta-analysis of observational studies. Crit. Care Res. Pract. 2012, 2012, 691013. [Google Scholar] [CrossRef]
- Cheungpasitporn, W.; Thongprayoon, C.; Kashani, K. Updates on the risk factors of acute kidney injury after transcatheter aortic valve replacement. J. Ren. Inj. Prev. 2017, 6, 16–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Gillaspie, E.A.; Greason, K.L.; Kashani, K.B. Association of blood transfusion with acute kidney injury after transcatheter aortic valve replacement: A meta-analysis. World J. Nephrol. 2016, 5, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Odutayo, A.; Wong, C.X.; Farkouh, M.; Altman, U.G.; Hopewell, S.; Emdin, C.A.; Hunn, B.H. AKI and Long-Term Risk for Cardiovascular Events and Mortality. J. Am. Soc. Nephrol. 2017, 28, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Pickering, J.W.; Blunt, I.R.H.; Than, M.P. Acute Kidney Injury and mortality prognosis in Acute Coronary Syndrome patients: A meta-analysis. Nephrology 2018, 23, 237–246. [Google Scholar] [CrossRef]
- Shi, Q.; Hong, L.; Mu, X.; Zhang, C.; Chen, X. Meta-analysis for outcomes of acute kidney injury after cardiac surgery. Medicine 2016, 95, e5558. [Google Scholar] [CrossRef]
- Giordana, F.; D’Ascenzo, F.; Nijhoff, F.; Moretti, C.; D’Amico, M.; Biondi-Zoccai, G.; Sinning, J.M.; Nickenig, G.; Van Mieghem, N.M.; Chieffo, A.; et al. Meta-analysis of predictors of all-cause mortality after transcatheter aortic valve implantation. Am. J. Cardiol. 2014, 114, 1447–1455. [Google Scholar] [CrossRef]
- Abdul Salim, S.; Tran, H.; Thongprayoon, C.; Fülöp, T.; Cheungpasitporn, W. Comparison of drug-coated balloon angioplasty versus conventional angioplasty for arteriovenous fistula stenosis: Systematic review and meta-analysis. J. Vasc. Access 2019. [Google Scholar] [CrossRef]
- De Carvalho, J.R.; Villela-Nogueira, C.A.; Luiz, R.R.; Guzzo, P.L.; Rosa, J.M.D.S.; Rocha, E.; Coelho, H.S.M.; Perez, R.D.M. Acute kidney injury network criteria as a predictor of hospital mortality in cirrhotic patients with ascites. J. Clin. Gastroenterol. 2012, 46, e21–e26. [Google Scholar] [CrossRef]
- Mandelbaum, T.; Scott, D.J.; Lee, J.; Mark, R.G.; Malhotra, A.; Waikar, S.S.; Howell, M.D.; Talmor, D. Outcome of critically ill patients with acute kidney injury using the Acute Kidney Injury Network criteria. Crit. Care Med. 2011, 39, 2659–2664. [Google Scholar] [CrossRef] [Green Version]
- Wongrakpanich, S.; Kallis, C.; Prasad, P.; Rangaswami, J.; Rosenzweig, A. The Study of Rhabdomyolysis in the Elderly: An Epidemiological Study and Single Center Experience. Aging Dis. 2018, 9, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Vandenberghe, W.; Gevaert, S.; Kellum, J.A.; Bagshaw, S.M.; Peperstraete, H.; Herck, I.; Decruyenaere, J.; Hoste, E. Acute Kidney Injury in Cardiorenal Syndrome Type 1 Patients: A Systematic Review and Meta-Analysis. Cardiorenal. Med. 2016, 6, 116–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folkestad, T.; Brurberg, K.G.; Nordhuus, K.M.; Tveiten, C.K.; Guttormsen, A.B.; Os, I.; Beitland, S. Acute kidney injury in burn patients admitted to the intensive care unit: A systematic review and meta-analysis. Crit. Care 2020, 24, 2–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, J.; Ng, K.P.; Sims, D.; Gill, P.; Cockwell, P.; Ferro, C. Incidence and impact on outcomes of acute kidney injury after a stroke: A systematic review and meta-analysis. BMC Nephrol. 2018, 19, 283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juwon, L.; Jang, G.; Kim, S.; Kim, D.; Lee, J.; Park, H.; Lee, J.; Kim, S.; Kim, Y.; Kim, S.Y.; et al. Outcomes of acute kidney injury patients with and without cancer. Ren. Fail. 2015, 37, 332–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barakat, M.F.; McDonald, H.I.; Collier, T.J.; Smeeth, L.; Nitsch, D.; Quint, J.K. Acute kidney injury in stable COPD and at exacerbation. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 2067–2077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiaccadori, E.; Lombardi, M.; Leonardi, S.; Rotelli, C.F.; Tortorella, G.; Borghetti, A. Prevalence and clinical outcome associated with preexisting malnutrition in acute renal failure: A prospective cohort study. J. Am. Soc. Nephrol. 1999, 10, 581–593. [Google Scholar] [PubMed]
- Bai, Z.; Primignani, M.; Guo, X.; Zheng, K.; Li, H.; Qi, X. Incidence and mortality of renal dysfunction in cirrhotic patients with acute gastrointestinal bleeding: A systematic review and meta-analysis. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 1181–1188. [Google Scholar] [CrossRef]
- Fiaccadori, E.; Maggiore, U.; Clima, B.; Melfa, L.; Rotelli, C.; Borghetti, A. Incidence, risk factors, and prognosis of gastrointestinal hemorrhage complicating acute renal failure. Kidney Int. 2001, 59, 1510–1519. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Srivali, N.; Harrison, A.; Kittanamongkolchai, W.; Greason, K.L.; Kashani, K.B. Transapical versus transfemoral approach and risk of acute kidney injury following transcatheter aortic valve replacement: A propensity-adjusted analysis. Ren. Fail. 2017, 39, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Gillaspie, E.A.; Greason, K.L.; Kashani, K.B. The risk of acute kidney injury following transapical versus transfemoral transcatheter aortic valve replacement: A systematic review and meta-analysis. Clin. Kidney J. 2016, 9, 560–566. [Google Scholar] [CrossRef] [Green Version]
- Perner, A.; Haase, N.; Guttormsen, A.B.; Tenhunen, J.; Klemenzson, G.; Åneman, A. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N. Engl. J. Med. 2012, 367, 124–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, A.; Pieper, K.; Myburgh, J.A.; Perkovic, V.; Finfer, S.; Yang, Q.; Li, Q.; Billot, L. Reanalysis of the Crystalloid versus Hydroxyethyl Starch Trial (CHEST). N. Engl. J. Med. 2017, 377, 298–300. [Google Scholar] [CrossRef] [PubMed]
- Semler, M.W.; Self, W.H.; Wanderer, J.P.; Ehrenfeld, J.M.; Wang, L.; Byrne, D.W.; Stollings, J.L.; Kumar, A.B.; Hughes, C.G.; Hernandez, A.; et al. Balanced Crystalloids versus Saline in Critically Ill Adults. N. Engl. J. Med. 2018, 378, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Semler, M.W.; Wanderer, J.P.; Wang, L.; Byrne, D.W.; Collins, S.P.; Slovis, C.M.; Lindsell, C.J.; Ehrenfeld, J.M.; Siew, E.D.; et al. Balanced Crystalloids versus Saline in Noncritically Ill Adults. N. Engl. J. Med. 2018, 378, 819–828. [Google Scholar] [CrossRef]
- Cheungpasitporn, W.; Thongprayoon, C.; Brabec, B.A.; Edmonds, P.J.; O’Corragain, O.A.; Erickson, S.B. Oral hydration for prevention of contrast-induced acute kidney injury in elective radiological procedures: A systematic review and meta-analysis of randomized controlled trials. N. Am. J. Med. Sci. 2014, 6, 618–624. [Google Scholar] [CrossRef] [Green Version]
- Cheungpasitporn, W.; Thongprayoon, C.; A Mao, M.; A Mao, S.; D’Costa, M.R.; Kittanamongkolchai, W.; Kashani, K.B. Contrast-induced acute kidney injury in kidney transplant recipients: A systematic review and meta-analysis. World J. Transplant. 2017, 7, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Cheungpasitporn, W.; Srivali, N.; Erickson, S.B. Admission serum magnesium levels and the risk of acute respiratory failure. Int. J. Clin. Pract. 2015, 69, 1303–1308. [Google Scholar] [CrossRef]
- Thamcharoen, N.; Thongprayoon, C.; Edmonds, P.J.; Cheungpasitporn, W. Periprocedural Nebivolol for the Prevention of Contrast-Induced Acute Kidney Injury: A Systematic Review and Meta-analysis. N. Am. J. Med. Sci. 2015, 7, 446–451. [Google Scholar] [CrossRef] [Green Version]
- Cheungpasitporn, W.; Thongprayoon, C.; Srivali, N.; O’Corragain, O.A.; Edmonds, P.; Ungprasert, P.; Kittanamongkolchai, W.; Erickson, S.B. Preoperative renin-angiotensin system inhibitors use linked to reduced acute kidney injury: A systematic review and meta-analysis. Nephrol. Dial. Transplant. 2015, 30, 978–988. [Google Scholar] [CrossRef] [Green Version]
- Tomson, C.; Tomlinson, L.A. Stopping RAS Inhibitors to Minimize AKI: More Harm than Good? Clin. J. Am. Soc. Nephrol. 2019, 14, 617–619. [Google Scholar] [CrossRef] [Green Version]
- Ungprasert, P.; Cheungpasitporn, W.; Crowson, C.S.; Matteson, E.L. Individual non-steroidal anti-inflammatory drugs and risk of acute kidney injury: A systematic review and meta-analysis of observational studies. Eur. J. Intern. Med. 2015, 26, 285–291. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, P.; Tolwani, A. Renal replacement therapy III: IHD, CRRT, SLED. Crit. Care Clin. 2005, 21, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Tolwani, A. Continuous renal-replacement therapy for acute kidney injury. N. Engl. J. Med. 2012, 367, 2505–2514. [Google Scholar] [CrossRef] [Green Version]
- Cerdá, J.; Ronco, C. Modalities of continuous renal replacement therapy: Technical and clinical considerations. Semin. Dial. 2009, 22, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Mehta, R.L.; Angus, D.C.; Palevsky, P.; Ronco, C. The first international consensus conference on continuous renal replacement therapy. Kidney Int. 2002, 62, 1855–1863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerda, J.; Sheinfeld, G.; Ronco, C. Fluid overload in critically ill patients with acute kidney injury. Blood Purif. 2010, 29, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Tandukar, S.; Palevsky, P.M. Continuous Renal Replacement Therapy: Who, When, Why, and How. Chest 2019, 155, 626–638. [Google Scholar] [CrossRef] [Green Version]
- Ronco, C.; Bellomo, R.; Ricci, Z. Continuous renal replacement therapy in critically ill patients. Nephrol. Dial. Transplant. 2001, 16, 67–72. [Google Scholar] [CrossRef] [Green Version]
- Schwenger, V.; Weigand, M.A.; Hoffmann, O.; Dikow, R.; Kihm, L.P.; Seckinger, J.; Miftari, N.; Schaier, M.; Hofer, S.; Haar, C.; et al. Sustained low efficiency dialysis using a single-pass batch system in acute kidney injury—A randomized interventional trial: The REnal Replacement Therapy Study in Intensive Care Unit PatiEnts. Crit. Care 2012, 16, R140. [Google Scholar] [CrossRef] [Green Version]
- Villa, G.; Neri, M.; Bellomo, R.; Cerda, J.; De Gaudio, A.R.; De Rosa, S.; Garzotto, F.; Honore, P.M.; Kellum, J.A.; Lorenzin, A.; et al. Nomenclature for renal replacement therapy and blood purification techniques in critically ill patients: Practical applications. Crit. Care 2016, 20, 283. [Google Scholar] [CrossRef] [Green Version]
- Lins, R.L.; Elseviers, M.M.; Van Der Niepen, P.; Hoste, E.; Malbrain, M.L.; Damas, P.; Devriendt, J. Intermittent versus continuous renal replacement therapy for acute kidney injury patients admitted to the intensive care unit: Results of a randomized clinical trial. Nephrol. Dial. Transplant. 2009, 24, 512–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinsonneau, C.; Camus, C.; Combes, A.; De Beauregard, M.A.C.; Klouche, K.; Boulain, T.; Pallot, J.-L.; Chiche, J.-D.; Taupin, P.; Landais, P.; et al. Continuous venovenous haemodiafiltration versus intermittent haemodialysis for acute renal failure in patients with multiple-organ dysfunction syndrome: A multicentre randomised trial. Lancet 2006, 368, 379–385. [Google Scholar] [CrossRef]
- Nash, D.M.; Przech, S.; Wald, R.; O’Reilly, D. Systematic review and meta-analysis of renal replacement therapy modalities for acute kidney injury in the intensive care unit. J. Crit. Care 2017, 41, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, J.O.; Wald, R.; Bagshaw, S.M.; Burns, K.E.; Adhikari, N.K. Hemofiltration compared to hemodialysis for acute kidney injury: Systematic review and meta-analysis. Crit. Care 2012, 16, R146. [Google Scholar] [CrossRef] [Green Version]
- Ronco, C.; Bellomo, R.; Homel, P.; Brendolan, A.; Dan, M.; Piccinni, P.; La Greca, G. Effects of different doses in continuous veno-venous haemofiltration on outcomes of acute renal failure: A prospective randomised trial. Lancet 2000, 356, 26–30. [Google Scholar] [CrossRef]
- Intensity of Renal Support in Critically Ill Patients with Acute Kidney Injury. N. Engl. J. Med. 2008, 359, 7–20. [CrossRef]
- Bellomo, R.; Cass, A.; Cole, L.; Finfer, S.; Gallagher, M.P.; Billot, L.; McArthur, C.; McGuinness, S.; Myburgh, J.; Norton, R.; et al. Intensity of continuous renal-replacement therapy in critically ill patients. N. Engl. J. Med. 2009, 361, 1627–1638. [Google Scholar]
- Clark, E.; Molnar, A.O.; Joannes-Boyau, O.; Honoré, P.M.; Sikora, L.; Bagshaw, S.M. High-volume hemofiltration for septic acute kidney injury: A systematic review and meta-analysis. Crit. Care 2014, 18, R7. [Google Scholar] [CrossRef] [Green Version]
- Combes, A.; Cozic, N.; Guidon, C.; Thiranos, J.-C.; Rigal, J.-C.; Benhaoua, H.; Abry, B.; Chastre, J.; Bréchot, N.; Amour, J.; et al. Early High-Volume Hemofiltration versus Standard Care for Post-Cardiac Surgery Shock. The HEROICS Study. Am. J. Respir. Crit. Care Med. 2015, 192, 1179–1190. [Google Scholar] [CrossRef]
- Gaudry, S.; Hajage, D.; Schortgen, F.; Martin-Lefevre, L.; Pons, B.; Boulet, E.; Boyer, A.; Chevrel, G.; Lerolle, N.; Carpentier, D.; et al. Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit. N. Engl. J. Med. 2016, 375, 122–133. [Google Scholar] [CrossRef]
- Barbar, S.D.; Clere-Jehl, R.; Bourredjem, A.; Hernu, R.; Montini, F.; Bruyère, R.; Lebert, C.; Bohé, J.; Badie, J.; Eraldi, J.-P.; et al. Timing of Renal-Replacement Therapy in Patients with Acute Kidney Injury and Sepsis. N. Engl. J. Med. 2018, 379, 1431–1442. [Google Scholar] [CrossRef] [PubMed]
- Zarbock, A.; Kellum, J.A.; Schmidt, C.; Van Aken, H.; Wempe, C.; Pavenstädt, H.; Boanta, A.; Gerß, J.; Meersch, M. Effect of Early vs Delayed Initiation of Renal Replacement Therapy on Mortality in Critically Ill Patients With Acute Kidney Injury: The ELAIN Randomized Clinical Trial. JAMA 2016, 315, 2190–2199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z. No “optimal timing” of renal-replacement therapy in critically ill patients with acute kidney injury. Ann. Transl. Med. 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Gaudry, S.; Hajage, D.; Martin-Lefevre, L.; Louis, G.; Moschietto, S.; Beauport, D.T.; La Combe, B.; Pons, B.; De Prost, N.; Besset, S.; et al. The Artificial Kidney Initiation in Kidney Injury 2 (AKIKI2): Study protocol for a randomized controlled trial. Trials 2019, 20, 726. [Google Scholar] [CrossRef]
- Smith, O.M.; Wald, R.; Adhikari, N.K.; Pope, K.; Weir, M.A.; Bagshaw, S.M. Standard versus Accelerated initiation of Renal Replacement Therapy in Acute Kidney Injury: Study Protocol for a Multi-National, Multi-Center, Randomized Controlled Trial. Can. J. Kidney Health Dis. 2019, 6, 320. [Google Scholar]
- Sutherland, S.M. Electronic Health Record-Enabled Big-Data Approaches to Nephrotoxin-Associated Acute Kidney Injury Risk Prediction. Pharmacotherapy 2018, 38, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.K. Dynamic Biomarker Assessment: A Diagnostic Paradigm to Match the AKI Syndrome. Front. Pediatr. 2019, 7, 535. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Stage | Serum Creatinine | Urine Output |
|---|---|---|
| 1 | 1.5–1.9 times baseline OR 0.3 mg/dL increase | <0.5 mL/kg/h for 6–12 h |
| 2 | 2.0–2.9 times baseline | <0.5 mL/kg/h for ≥12 h |
| 3 | 3.0 times baseline OR Increase in serum creatinine to ≥4.0 mg/dL OR initiation of replacement therapy | <0.3 mL/kg/h for ≥24 h OR anuria for ≥12 h |
| Patient Populations/Settings | Incidence of AKI |
|---|---|
| - General hospitalized patients - ICU - Cardiac surgery - Transcatheter Aortic Valve Replacement - Sepsis - Acute respiratory distress syndrome - Extracorporeal Membrane Oxygenation ○ AKI ○ Severe AKI requiring RRT - Liver transplantation ○ AKI ○ Severe AKI requiring RRT | 10%–20% 20%–50% 30%–50% 28% 16%–25% 44%–50% 63% 45% 41% 8% |
| - Lung transplantation ○ AKI ○ Severe AKI requiring RRT - Cardiac Transplantation ○ AKI ○ Severe AKI requiring RRT - Hematopoietic Stem Cell Transplantation ○ AKI ○ Severe AKI requiring RRT - Total Hip Arthroplasty ○ AKI - Severe AKI requiring RRT | 53% 9% 47% 12% 55% 8% 6% 0.5% |
| Diagnostic Test | Findings | Pathologic Condition (s) |
|---|---|---|
| Urinalysis with microscopy | Hyaline cast | Prerenal azotemia |
| Muddy brown cast | ATN | |
| Dysmorphic RBC & RBC casts | GN | |
| WBC casts | AIN | |
| Crystals | Crystal induced nephropathy, drugs, nephrolithiasis | |
| Monomorphic RBCs, WBCs | UTI, Nephrolithiasis, Genitourinary tumors etc | |
| Protein | GN, Monoclonal gammopathy | |
| CBC with peripheral smear | Anemia, Schistocytes, low platelets | TMA |
| Serum osmolality | Osmolar gap & severe metabolic acidosis | Toxin |
| Creatinine kinase | >5000 IU/L | Rhabdomyolysis |
| Serologic tests | HIV antibody | HIV associated nephropathy, HIV induced immunocomplex kidney disease |
| Hepatitis serology | Membranous GN, MPGN | |
| ANA, dsDNA | Lupus nephritis | |
| C- ANCA, P- ANCA | ANCA vasculitis | |
| Rheumatoid factor, Cryoglobulins | Cryoglobulinemia, MPGN | |
| Anti—GBM antibody | Good pasture syndrome | |
| ASO | Infection related GN | |
| Low Complement levels | Lupus, Infection related GN, atheroemboli, MPGN, shunt nephritis | |
| Fractional excretion of sodium (FeNa) * | <1% | Prerenal azotemia |
| Fractional Excretion of urea (Fe Urea) | <35% | Prerenal azotemia |
| POCUS (Volume Assessment) | IVC diameter ↓ (>50% w/inspiration) | Hypovolemia |
| Renal USG | Hydronephrosis, Hydroureter | Nephrolithiasis, Retroperitoneal fibrosis, BPH, Phimosis, Ureteral obstruction |
| Renal vein thrombosis | Hypercoagulable state | |
| Renal biopsy | Variable | GN, ATN, AIN, crystal induced nephropathy |
| Newer biomarkers | ↑ NGAL, KIM 1, (TIMP-2)∙(IGFBP7) ** | "Damage biomarkers" increased much before rise in creatinine |
| Novel Biomarkers | Specimen | Type | Representation | Study Population |
|---|---|---|---|---|
| NGAL | Serum, urine | Upregulated protein | Distal tubules | Cardiac surgery, Critically ill, CRS, KT |
| KIM-1 | Urine | Upregulated protein | Proximal tubules | Cardiac surgery, KT |
| L-FABP | Urine | Upregulated protein | Proximal tubules | Cardiac surgery, Critically ill |
| IL-10 | Urine | Cytokine | Inflammatory cascades | Cardiac surgery |
| IL-18 | Urine | Cytokine | Inflammatory cascades | Cardiac surgery, Critically ill, KT |
| Urine Cystatin C | Serum, urine | Functional | Proximal tubules (urine), glomerular (serum) | Critically ill |
| NAG | Urine | Enzyme | Proximal tubules | Critically ill, KT |
| IGFBP7 | Urine | Upregulated protein | Proximal tubules | Critically ill, cardiac surgery |
| TIMP-2 | Urine | Upregulated protein | Proximal tubules | Critically ill, cardiac surgery |
| Calprotectin | Urine | Upregulated protein | Renal inflammation | Hospitalized patients |
| AGT | Urine | Enzyme | Renin-angiotensin activation | Heart failure |
| microRNA | Urine | RNA fragment | Proximal and distal tubules | Cardiac surgery |
| Modifiable | Non-Modifiable |
|---|---|
|
|
| Patient Populations | Odds Ratio (95% CI) for Mortality |
|---|---|
| Acute coronary syndrome | 4.1 (3.3–5.0) |
| Cardiac surgery | 6.27 (3.6–11.0) |
| TAVR | 18.0 (6.3–52.0) |
| ECMO | 3.7 (2.9–4.9) |
| Liver transplantation | 3.0 (2.3–3.8) |
| Cirrhosis | 2.6 (1.5–4.7) |
| Lung transplantation | 1.5 (1.1–1.9) |
| Stem cell transplantation | 3.0 (2.1–4.5) |
| Heart transplantation | 2.7 (1.6–3.3) |
| Critically ill patients | 1.4 to 2.5 |
| Rhabdomyolysis | 3.3 (1.1–9.7) |
| Cardiorenal syndrome | 4.9 (3.7–6.5) |
| Burn patients | 11.3 (7.3–17.4) |
| Ischemic stroke | 2.5 (1.5–4.1) |
| Cancer | 3.0 (2.3–3.9) |
| COPD | 1.8 (1.6–2.0) |
| Malnutrition | 2.0 (1.5–2.7) |
| Gastrointestinal bleeding | 2.6 to 4.9 |
| General Measures | |
| Identify patients at risk |
|
| Use of Clinical decision support systems (CDSS) |
|
| Maintain euvolemia |
|
| Avoid nephrotoxic medications. |
|
| Judicious use of contrasted studies |
|
| Avoid hypotension |
|
| Renal function monitoring |
|
| Specific Clinical Scenarios | |
| Patients undergoing a procedure needing IV contrast use |
|
| Traumatic and non-traumatic rhabdomyolysis |
|
| Patients undergoing cardiac surgery | Preoperative:
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongprayoon, C.; Hansrivijit, P.; Kovvuru, K.; Kanduri, S.R.; Torres-Ortiz, A.; Acharya, P.; Gonzalez-Suarez, M.L.; Kaewput, W.; Bathini, T.; Cheungpasitporn, W. Diagnostics, Risk Factors, Treatment and Outcomes of Acute Kidney Injury in a New Paradigm. J. Clin. Med. 2020, 9, 1104. https://doi.org/10.3390/jcm9041104
Thongprayoon C, Hansrivijit P, Kovvuru K, Kanduri SR, Torres-Ortiz A, Acharya P, Gonzalez-Suarez ML, Kaewput W, Bathini T, Cheungpasitporn W. Diagnostics, Risk Factors, Treatment and Outcomes of Acute Kidney Injury in a New Paradigm. Journal of Clinical Medicine. 2020; 9(4):1104. https://doi.org/10.3390/jcm9041104
Chicago/Turabian StyleThongprayoon, Charat, Panupong Hansrivijit, Karthik Kovvuru, Swetha R. Kanduri, Aldo Torres-Ortiz, Prakrati Acharya, Maria L. Gonzalez-Suarez, Wisit Kaewput, Tarun Bathini, and Wisit Cheungpasitporn. 2020. "Diagnostics, Risk Factors, Treatment and Outcomes of Acute Kidney Injury in a New Paradigm" Journal of Clinical Medicine 9, no. 4: 1104. https://doi.org/10.3390/jcm9041104