COVID-19 and Congenital Heart Disease: Results from a Nationwide Survey

 ,
,  , , , and
, , , and
Abstract
:1. Background
2. Methods
2.1. Data Collection and Data Quality
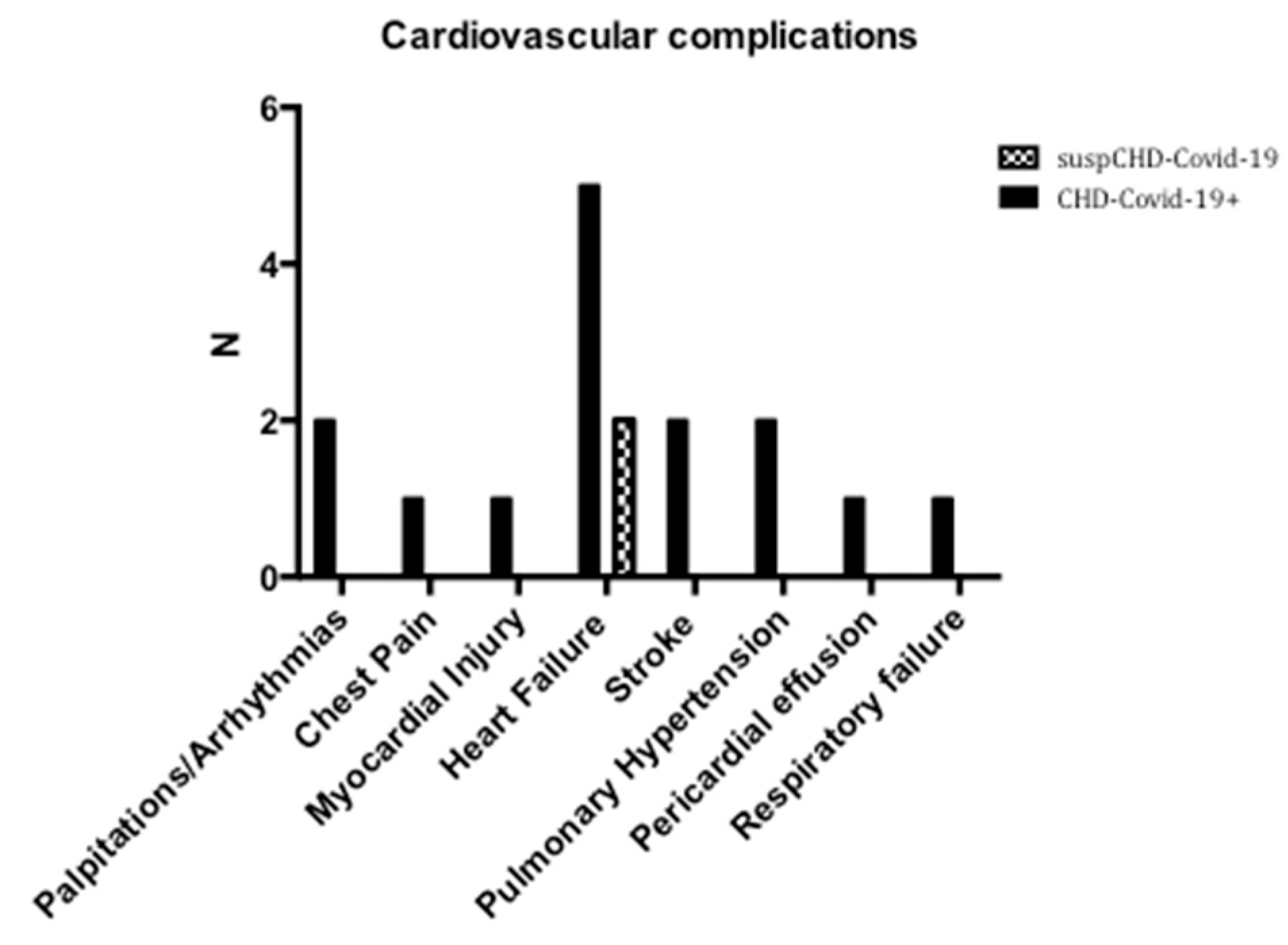
2.2. Cardiovascular Complications
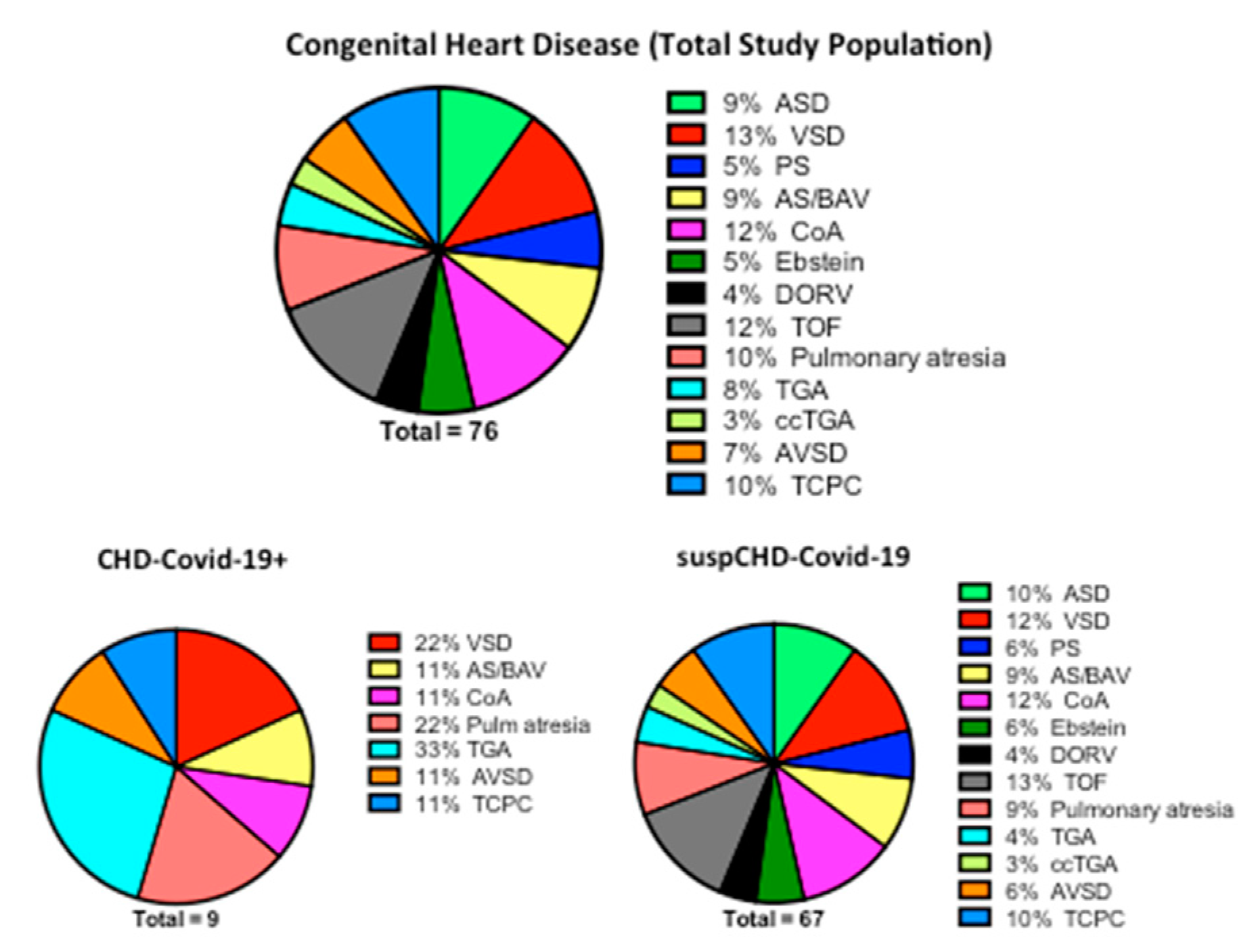
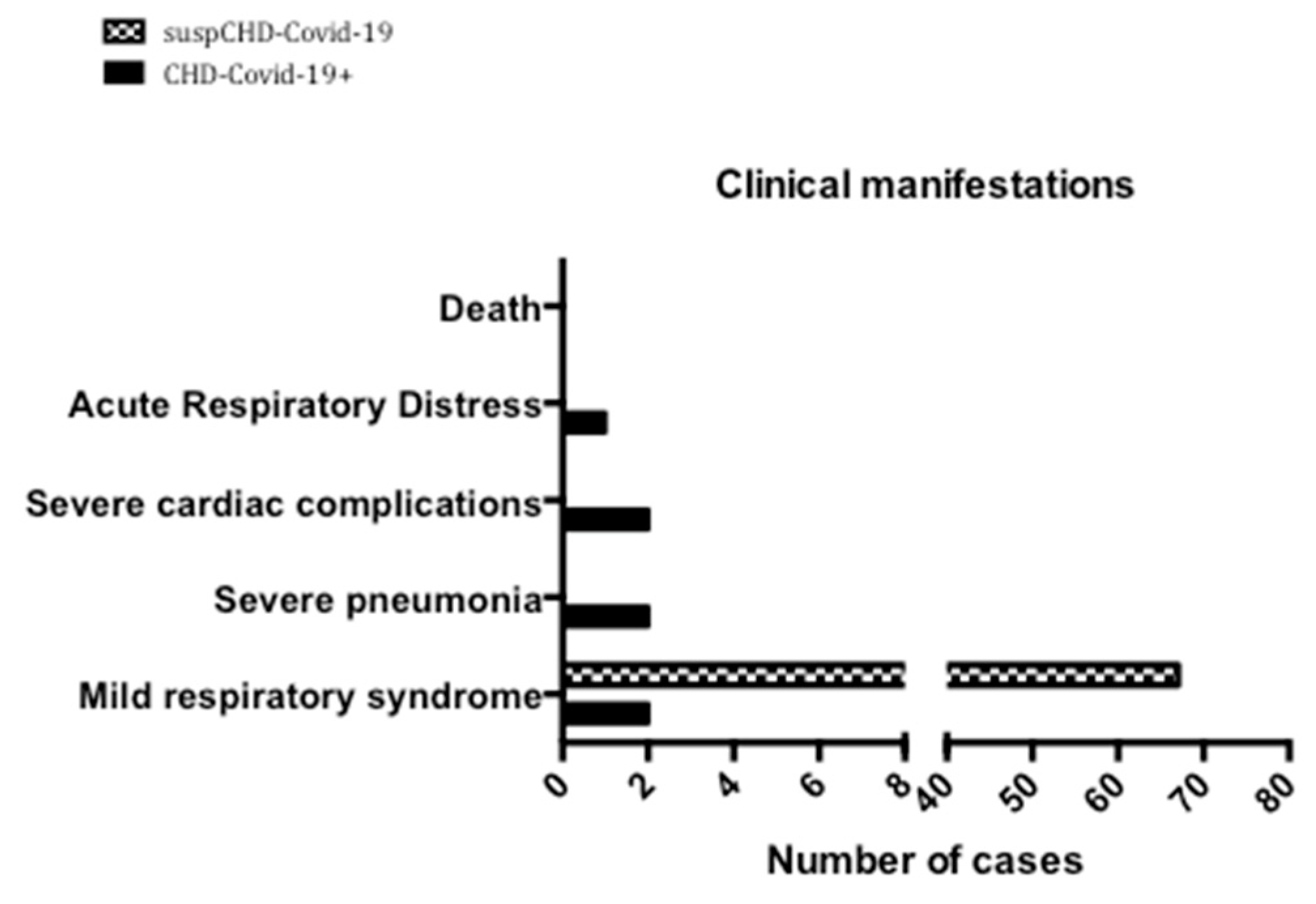
3. Results
3.1. Cardiovascular Complications
3.2. Clinical Management and Treatment
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, B.; Yang, J.; Zhao, F.; Zhi, L.; Wang, X.; Liu, L.; Bi, Z.; Zhao, Y. Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin. Res. Cardiol. 2020, 109, 531–538. [Google Scholar] [CrossRef]
- Tan, W.; Aboulhosn, J. The cardiovascular burden of coronavirus disease 2019 (COVID-19) with a focus on congenital heart disease. Int. J. Cardiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Morray, B.H.; Gordon, B.M.; Crystal, M.A.; Goldstein, B.H.; Qureshi, A.M.; Torres, A.J.; Epstein, S.M.; Crittendon, I.; Ing, F.F.; Sathanandam, S.K. Resource Allocation and Decision Making for Pediatric and Congenital Cardiac Catheterization During the Novel Coronavirus SARS-CoV-2 (COVID-19) Pandemic: A U.S. Multi-Institutional Perspective. J. Invasive Cardiol. 2020, 32, E103–E109. [Google Scholar]
- Brida, M.; Chessa, M.; Gu, M.; GAtzoulis, M.A. The globe on the spotlight: Coronavirus disease 2019 (Covid-19). Int. J. Cardiol. 2020. [Google Scholar] [CrossRef]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Zhang, W.; Wang, Y.; Bao, S.; Li, Y.; et al. SARS-CoV-2 infection in children. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics 2020, e20200702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (nCoV) Infection Is Suspected. Available online: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-whennovel-coronavirus-(ncov)-infection-is-suspected (accessed on 12 April 2020).
- Chan, J.F.W.; Yuan, S.; Kok, K.H.; To, K.K.W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.Y.; Poon, R.W.S. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.; Culebras, A.; Elkind, M.S.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An updated definition of stroke for the 21st century: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef] [Green Version]
- Fan, E.; Brodie, D.; Slutsky, A.S. Acute Respiratory Distress Syndrome: Advances in Diagnosis and Treatment. JAMA 2018, 319, 698–710. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J. Infect. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prete, M.; Favoino, E.; Catacchio, G.; Racanelli, V.; Perosa, F. SARS-CoV-2 Inflammatory Syndrome. Clinical Features and Rationale for Immunological Treatment. Int. J. Mol. Sci. 2020, 21, 3377. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità [Higher Institute of Health]. Integrated surveillance of COVID-19 in Italy. Available online: https://www.iss.it/en/covid-19-integrated-surveillance (accessed on 29 April 2020).
- Sabatino, J. Prey in Heroes’ Capes. JACC Case Rep. 2020. [Google Scholar] [CrossRef]
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; Petersen, S.E.; Mossialos, E.A.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2019. Eur. Heart J. 2020, 41, 12–85. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 76) | suspCHD-Covid-19 (n = 67) | |
|---|---|---|
| Age (years) | 34.7 | 30 |
| Sex (female, n) | 36 (47%) | 32 (48%) |
| Hypertension | 5 (7%) | 5 (7.5%) |
| Diabetes | 1 (1%) | 0 |
| Obesity | 7 (9%) | 5 (7.5%) |
| Smokers | 1 (1%) | 1 (1.4%) |
| Pulmonary hypertension | 2 (3%) | 1 (1.4%) |
| AF/atrial tachicardia | 7 (9%) | 6 (9%) |
| Previous cardio-embolic stroke | 2 (3%) | 2 (3%) |
| Patients | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristics | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
| Age (years) | 35 | 30 | 30 | 0.3 | 48 | 52 | 47 | 2 | 1 |
| Sex | Female | Male | Male | Male | Male | Female | Male | Female | Female |
| CHD | Univentricular heart s/p TCPC | TGA | VSD | Multiple | TGA (Mustard) | pAVSD | Ao stenosis; COA | PAx/VSD | TGA; PAx/VSD |
| Atrial switch | |||||||||
| LV-PA conduit | VSD (PAB) | ||||||||
| CV risk factors | None | None | Obesity | None | DM, Obesity | None | None | None | None |
| CV comorbidity | None | None | None | None | AF | PH, PLE, AV block | HF | None | None |
| CV complications | None | None | Chest pain | MyoInj; PEE; HF | HF | Stroke, Arrhythmias | Stroke, arrhythmias, worsening HF; ECMO implantation | HF; PH | HF; PH |
| Death (yes/no) | No | No | No | No | No | No | No | No | No |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sabatino, J.; Ferrero, P.; Chessa, M.; Bianco, F.; Ciliberti, P.; Secinaro, A.; Oreto, L.; Avesani, M.; Bucciarelli, V.; Calcaterra, G.; et al. COVID-19 and Congenital Heart Disease: Results from a Nationwide Survey. J. Clin. Med. 2020, 9, 1774. https://doi.org/10.3390/jcm9061774
Sabatino J, Ferrero P, Chessa M, Bianco F, Ciliberti P, Secinaro A, Oreto L, Avesani M, Bucciarelli V, Calcaterra G, et al. COVID-19 and Congenital Heart Disease: Results from a Nationwide Survey. Journal of Clinical Medicine. 2020; 9(6):1774. https://doi.org/10.3390/jcm9061774
Chicago/Turabian StyleSabatino, Jolanda, Paolo Ferrero, Massimo Chessa, Francesco Bianco, Paolo Ciliberti, Aurelio Secinaro, Lilia Oreto, Martina Avesani, Valentina Bucciarelli, Giuseppe Calcaterra, and et al. 2020. "COVID-19 and Congenital Heart Disease: Results from a Nationwide Survey" Journal of Clinical Medicine 9, no. 6: 1774. https://doi.org/10.3390/jcm9061774