
Breast Cancer Screening during COVID-19 Emergency: Patients and Department Management in a Local Experience


 , , and
, , and
Abstract
:1. Introduction
2. Methods
- Breast screening patients:
- (a)
- Asymptomatic patients who undergo mammography exam following the specific screening program, according to national regulations.
- (b)
- Patients with suspected breast lesion revealed through the mammographic exam, thus needing to complete the work-up with ultrasound and needle biopsy.
- Breast ambulatory patients:
- (a)
- Patients who have to complete the mammography work-up with ultrasound, following the surgeon recommendation.
- (b)
- Symptomatic breast cancer patients (new onset palpable nodule; skin or nipple retraction; orange peel skin; unilateral secretion from the nipple).
- ●
- Non-COVID-19 patient;
- ●
- Confirmed COVID-19 in asymptomatic screening patient;
- ●
- Suspected COVID-19 in symptomatic or confirmed breast cancer patient;
- ●
- Confirmed COVID-19 in symptomatic or confirmed breast cancer patient.
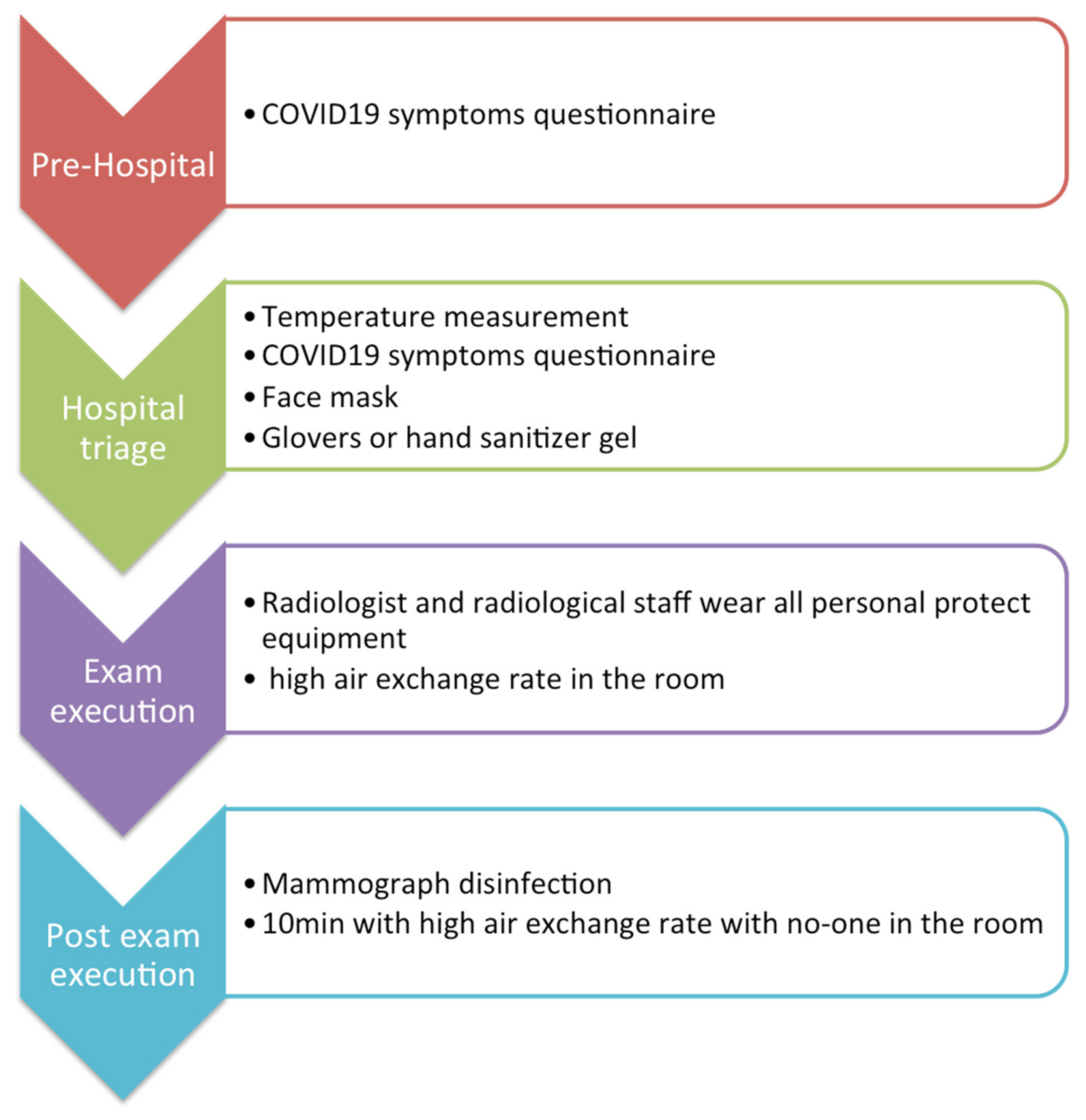
2.1. Practice Organization in the Radiology Breast Screening Department
2.2. Infection Prevention in a Radiology Breast Screening Department
- ●
- Non-COVID-19 patient: Patients without COVID-19 infection, as laboratory-confirmed by a reverse transcriptase-polymerase chain reaction (RT-PCR) test, were defined as non-COVID-19 patients [13]. However, since the laboratory tests had not yet been used as a screening tool to identify COVID-19 patients and many people may be asymptomatic or pauci-symptomatic, it would be appropriate for health professionals to consider all patients as if they were infected [14]. Therefore, all patients must wear a surgical mask and maintain the minimum distance of 1 m from others while waiting for a radiological procedure. No one, including any accompanying person, is allowed to stay in the waiting room. The healthcare staff should a wear surgical mask, avoid direct contact with patient’s oral and respiratory secretions, wear goggles or face shields and gloves and also wash hands before wearing and after removing gloves. A surgical cap and shoe covers are welcome. The ultrasound probe should be protected by a dedicated cover and disinfected after every single procedure [14,15,16]. After each radiological exam, the room and the radiological equipment must be cleaned and disinfected with chloro-derivate solutions and the room should be appropriately ventilated (>25 cycles/h) [14,17,18].
- ●
- Confirmed COVID-19 in asymptomatic screening patient: Considering the highly contagious nature of SARS-CoV-2, and taking count that this category of patients has no urgency to perform the mammographic exam, their appointments were rescheduled, as soon as was possible, after two negative nasopharyngeal swabs for SARS-CoV-2 RT-PCR test.
- ●
- Suspected COVID-19 in symptomatic or confirmed breast cancer patient: As in the first scenario, the patient must wear a surgical mask and follow the rules of social distancing in the waiting room. Radiological staff should wear an FFP2 mask (filtering face piece), goggles or face shield, gloves and cap. Ultrasound and mammographic machines must be covered by a plastic sheet and disinfected after the procedure with chloro-derivate solutions and the room should be appropriately ventilated (>25 cycles/h) [14,18].
- ●
- Confirmed COVID-19 in symptomatic or confirmed breast cancer patient: Considering the highly contagious nature of SARS-CoV-2, the patient wears a surgical mask and stays isolated from other people. Radiological staff must wear an FFP3 mask, eye protection, impermeable full-length long-sleeved gown, gloves and cap. Staff will pay maximum attention to the dressing and undressing procedures, as suggested by the Spallanzani Hospital [19]. Ultrasound and mammographic machines have to be covered by a plastic sheet and disinfected after the procedure with chloro-derivate solutions and the room should be appropriately ventilated (>25 cycles/h) [14,15,18].
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| WHO | World Health Organization |
| COVID-19 | coronavirus disease ‘19 |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| US | ultrasound |
| SIRM | Italian Society of Radiology and Interventional Radiology |
| MRI | magnetic resonance imaging |
| RT-PCR | reverse transcriptase-polymerase chain reaction |
| FFP | filtering face piece |
| BIRADS | breast imaging reporting and data system |
References
- Lake, M.A. What we know so far: COVID-19 current clinical knowledge and research. Clin. Med. 2020, 20, 124–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 26 November 2020).
- Salute M della. Ministero della Salute. Available online: http://www.salute.gov.it/portale/home.html (accessed on 26 November 2020).
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [Green Version]
- Kimball, A.; Hatfield, K.M.; Arons, M.; James, A.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; Tanwar, S.; Chisty, Z.; et al. Asymptomatic and Presymptomatic SARS-CoV-2 Infections in Residents of a Long-Term Care Skilled Nursing Facility—King County, Washington, March 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, M. The Front Line: Visualizing the Occupations with the Highest COVID-19 Risk. Visual Capitalist 2020. Available online: https://www.visualcapitalist.com/the-front-line-visualizing-the-occupations-with-the-highest-covid-19-risk/ (accessed on 15 April 2020).
- Granata, V.; Fusco, R.; Izzo, F.; Setola, S.V.; Coppola, M.; Grassi, R.; Reginelli, A.; Cappabianca, S.; Petrillo, A. Covid-19 infection in cancer patients: The management in a diagnostic unit. Radiol. Oncol. 2021, 1, 1–9. [Google Scholar] [CrossRef]
- National Library of Medicine. PubMed.gov. Available online: https://pubmed.ncbi.nlm.nih.gov/ (accessed on 26 June 2020).
- Torbica, A.; Fattore, G. The “Essential Levels of Care” in Italy: When being explicit serves the devolution of powers. Eur. J. Heal. Econ. 2005, 6, 46–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salute M della. Screening per il Tumore della Mammella. Available online: http://www.salute.gov.it/portale/salute/p1_5.jsp?lingua=italiano&id=23&area=Screening (accessed on 21 April 2020).
- Pediconi, F.; Galati, F.; Bernardi, D.; Belli, P.; Brancato, B.; Calabrese, M.; Camera, L.; Carbonaro, L.A.; Caumo, F.; Clauser, P.; et al. Breast imaging and cancer diagnosis during the COVID-19 pandemic: Recommendations from the Italian College of Breast Radiologists by SIRM. Radiol. Med. 2020, 125, 926–930. [Google Scholar] [CrossRef] [PubMed]
- Salute M della. Nuovo Coronavirus. Available online: http://www.salute.gov.it/nuovocoronavirus?gclid=EAIaIQobChMIz_rmnZPP6gIVgrTtCh0M6wYPEAAYASAAEgKY0fD_BwE (accessed on 21 April 2020).
- Cozzi, D.; Albanesi, M.; Cavigli, E.; Moroni, C.; Bindi, A.; Luvarà, S.; Lucarini, S.; Busoni, S.; Mazzoni, L.N.; Miele, V. Chest X-ray in new Coronavirus Disease 2019 (COVID-19) infection: Findings and correlation with clinical outcome. Radiol. Med. 2020, 125, 730–737. [Google Scholar] [CrossRef]
- Too, C.W.; Wen, D.W.; Patel, A.; Syafiq, A.R.A.; Liu, J.; Leong, S.; Gogna, A.; Lo, R.H.G.; Tashi, S.; Lee, K.A.; et al. Interventional Radiology Procedures for COVID-19 Patients: How we Do it. Cardiovasc. Interv. Radiol. 2020, 43, 827–836. [Google Scholar] [CrossRef]
- Checklist for Preparing Your IR Service for COVID-19. Available online: https://www.cirse.org/wp-content/uploads/2020/04/cirse_APSCVIR_Checklist_COVID19_prod.pdf (accessed on 27 March 2020).
- Modalità di Comportamento per L’effettuazione di un Esame Ecografico in Questo Momento Pandemico Su. Available online: https://www.sirm.org/wp-content/uploads/2020/03/Modalita%CC%80-di-comportamento-per-l%E2%80%99effettuazione-di-un-esame-ecografico-.pdf.pdf (accessed on 22 March 2020).
- Jin, Y.-H.; Cai, L.; Cheng, Z.-S.; Cheng, H.; Deng, T.; Fan, Y.-P.; Fang, C.; Huang, D.; Huang, L.-Q.; Huang, Q.; et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med. Res. 2020, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Coccolini, F.; Perrone, G.; Chiarugi, M.; Di Marzo, F.; Ansaloni, L.; Scandroglio, I.; Marini, P.; Zago, M.; De Paolis, P.; Forfori, F.; et al. Surgery in COVID-19 patients: Operational directives. World J. Emerg. Surg. 2020, 15, 1–7. [Google Scholar] [CrossRef]
- Pianura, E.; Stefano, F.D.; Cristofaro, M.; Petrone, A.; Albarello, F.; Fusco, N.; Schininà, V. COVID-19: A review of the literature and the experience of INMI Lazzaro Spallanzani two months after the epidemic outbreak. J. Radiol. Rev. 2020, 7, 196–207. [Google Scholar] [CrossRef]
- Yeh, E.D.; Jacene, H.A.; Bellon, J.R.; Nakhlis, F.; Birdwell, R.L.; Georgian-Smith, D.; Giess, C.S.; Hirshfield-Bartek, J.; Overmoyer, B.; van den Abbeele, A.D.; et al. What Radiologists Need to Know about Diagnosis and Treatment of Inflammatory. Breast Cancer: A Multidisciplinary Approach. RadioGraphics 2013, 33, 2003–2017. [Google Scholar] [CrossRef] [PubMed]
- I 5 Tumori Più Frequenti in Italia Nel 2019. Available online: http://www.salute.gov.it/imgs/C_17_notizie_3897_4_file.pdf (accessed on 21 January 2020).
- Buonomo, O.C.; Materazzo, M.; Pellicciaro, M.; Caspi, J.; Piccione, E.; Vanni, G. Tor Vergata University-Hospital in the Beginning of COVID-19-Era: Experience and Recommendation for Breast Cancer Patients. In Vivo 2020, 34, 1661–1665. [Google Scholar] [CrossRef] [PubMed]
- Bleicher, R.J. Timing and Delays in Breast Cancer Evaluation and Treatment. Ann. Surg. Oncol. 2018, 25, 2829–2838. [Google Scholar] [CrossRef]
- Gathani, T.; Clayton, G.; MacInnes, E.; Horgan, K. The COVID-19 pandemic and impact on breast cancer diagnoses: What happened in England in the first half of 2020. Br. J. Cancer 2021, 124, 710–712. [Google Scholar] [CrossRef]
- Vanni, G.; Pellicciaro, M.; Materazzo, M.; Bruno, V.; Oldani, C.; Pistolese, C.A.; Buonomo, C.; Caspi, J.; Gualtieri, P.; Chiaravalloti, A.; et al. Lockdown of Breast Cancer Screening for COVID-19: Possible Scenario. In Vivo 2020, 34, 3047–3053. [Google Scholar] [CrossRef]
- Cancino, R.S.; Sun, P.; Mesa, R.E.; Tomlinson, G.; Wang, J. The Impact of COVID-19 on Cancer Screening: Challenges and Opportunities. JMIR Cancer 2020, 6, e21697. [Google Scholar] [CrossRef]
- Román, M.; Sala, M.; Domingo, L.; Posso, M.; Louro, J.; Castells, X. Personalized breast cancer screening strategies: A systematic review and quality assessment. PLoS ONE 2019, 14, e0226352. [Google Scholar] [CrossRef] [Green Version]
- Salem, C.; Hajj, M.-A.; Kourié, H.; Haddad, A.; Khaddage, A.; Ayoub, E.N.; Jabbour, K.; Moubarak, M.; Atallah, D. Radiology management of a ‘breast unit’ during COVID-19 pandemic: A single institution experience. Future Oncol. 2020, 16, 2917–2922. [Google Scholar] [CrossRef]
- Rocco, N.; Montagna, G.; Di Micco, R.; Benson, J.; Criscitiello, C.; Chen, L.; Di Pace, B.; Colmenarejo, A.J.E.; Harder, Y.; Karakatsanis, A.; et al. The Impact of the COVID-19 Pandemic on Surgical Management of Breast Cancer: Global Trends and Future Perspectives. Oncologist 2021, 26, 66–67. [Google Scholar] [CrossRef]
- Mantellini, P.; Battisti, F.; Armaroli, P.; Giubilato, P.; Ventura, L.; Zorzi, M.; Battagello, J.; de Bianchi, P.S.; Senore, C.; Zappa, M. Ritardi maturati dai programmi di screening oncologici ai tempi del COVID-19 in Italia, velocità della ripartenza e sti-ma dei possibili ritardi diagnostici [Oncological organized screening programmes in the COVID-19 era: An Italian survey on accrued delays, reboot velocity, and diagnostic delay estimates]. Epidemiol. Prev. 2020, 44, 344–352. [Google Scholar]
- Carotti, M.; Salaffi, F.; Sarzi-Puttini, P.; Agostini, A.; Borgheresi, A.; Minorati, D.; Galli, M.; Marotto, D.; Giovagnoni, A. Chest CT features of coronavirus disease 2019 (COVID-19) pneumonia: Key points for radiologists. Radiol. Med. 2020, 125, 636–646. [Google Scholar] [CrossRef]
- Shaw, B.; Daskareh, M.; Gholamrezanezhad, A. The lingering manifestations of COVID-19 during and after convalescence: Update on long-term pulmonary consequences of coronavirus disease 2019 (COVID-19). Radiol. Med. 2021, 126, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Belfiore, M.P.; Urraro, F.; Grassi, R.; Giacobbe, G.; Patelli, G.; Cappabianca, S.; Reginelli, A. Artificial intelligence to codify lung CT in Covid-19 patients. Radiol. Med. 2020, 125, 500–504. [Google Scholar] [CrossRef] [PubMed]
- Borghesi, A.; Maroldi, R. COVID-19 outbreak in Italy: Experimental chest X-ray scoring system for quantifying and monitoring disease progression. Radiol. Med. 2020, 125, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Di Serafino, M.; Notaro, M.; Rea, G.; Iacobellis, F.; Paoli, V.D.; Acampora, C.; Ianniello, S.; Brunese, L.; Romano, L.; Vallone, G. The lung ultrasound: Facts or artifacts? In the era of COVID-19 outbreak. Radiol. Med. 2020, 125, 738–753. [Google Scholar] [CrossRef]
- Giovagnoni, A. Facing the COVID-19 emergency: We can and we do. Radiol. Med. 2020, 125, 337–338. [Google Scholar] [CrossRef] [Green Version]
- Brogna, B.; Bignardi, E.; Brogna, C.; Volpe, M.; Lombardi, G.; Rosa, A.; Gagliardi, G.; Capasso, P.; Gravino, E.; Maio, F.; et al. A Pictorial Review of the Role of Imaging in the Detection, Management, Histopathological Correlations, and Complications of COVID-19 Pneumonia. Diagnostics 2021, 11, 437. [Google Scholar] [CrossRef]
- Neri, E.; Miele, V.; Coppola, F.; Grassi, R. Use of CT and artificial intelligence in suspected or COVID-19 positive patients: Statement of the Italian Society of Medical and Interventional Radiology. Radiol. Med. 2020, 125, 505–508. [Google Scholar] [CrossRef]
- Borghesi, A.; Zigliani, A.; Masciullo, R.; Golemi, S.; Maculotti, P.; Farina, D.; Maroldi, R. Radiographic severity index in COVID-19 pneumonia: Relationship to age and sex in 783 Italian patients. Radiol. Med. 2020, 125, 461–464. [Google Scholar] [CrossRef]
- Gatti, M.; Calandri, M.; Barba, M.; Biondo, A.; Geninatti, C.; Gentile, S.; Greco, M.; Morrone, V.; Piatti, C.; Santonocito, A.; et al. Baseline chest X-ray in coronavirus disease 19 (COVID-19) patients: Association with clinical and laboratory data. Radiol. Med. 2020, 125, 1271–1279. [Google Scholar] [CrossRef]
- Agostini, A.; Floridi, C.; Borgheresi, A.; Badaloni, M.; Pirani, P.E.; Terilli, F.; Ottaviani, L.; Giovagnoni, A. Proposal of a low-dose, long-pitch, dual-source chest CT protocol on third-generation dual-source CT using a tin filter for spectral shaping at 100 kVp for CoronaVirus Disease 2019 (COVID-19) patients: A feasibility study. Radiol. Med. 2020, 125, 365–373. [Google Scholar] [CrossRef] [Green Version]
- Caruso, D.; Polici, M.; Zerunian, M.; Pucciarelli, F.; Polidori, T.; Guido, G.; Rucci, C.; Bracci, B.; Muscogiuri, E.; De Dominicis, C.; et al. Quantitative Chest CT analysis in discriminating COVID-19 from non-COVID-19 patients. Radiol. Med. 2021, 126, 243–249. [Google Scholar] [CrossRef]
- Palmisano, A.; Scotti, G.M.; Ippolito, D.; Morelli, M.J.; Vignale, D.; Gandola, D.; Sironi, S.; De Cobelli, F.; Ferrante, L.; Spessot, M.; et al. Chest CT in the emergency department for suspected COVID-19 pneumonia. Radiol. Med. 2021, 126, 498–502. [Google Scholar] [CrossRef]
- Grassi, R.; Belfiore, M.P.; Montanelli, A.; Patelli, G.; Urraro, F.; Giacobbe, G.; Fusco, R.; Granata, V.; Petrillo, A.; Sacco, P.; et al. COVID-19 pneumonia: Computer-aided quantification of healthy lung parenchyma, emphysema, ground glass and consolidation on chest computed tomography (CT). Radiol. Med. 2020. [Google Scholar] [CrossRef]
- Cappabianca, S.; Fusco, R.; De Lisio, A.; Paura, C.; Clemente, A.; Gagliardi, G.; Lombardi, G.; Giacobbe, G.; Russo, G.M.; Belfiore, M.P.; et al. Correction to: Clinical and laboratory data, radiological structured report findings and quantitative evaluation of lung involvement on baseline chest CT in COVID-19 patients to predict prognosis. Radiol. Med. 2021, 126, 29–39. [Google Scholar] [CrossRef]
- Giannitto, C.; Sposta, F.M.; Repici, A.; Vatteroni, G.; Casiraghi, E.; Casari, E.; Ferraroli, G.M.; Fugazza, A.; Sandri, M.T.; Chiti, A.; et al. Chest CT in patients with a moderate or high pretest probability of COVID-19 and negative swab. Radiol. Med. 2020, 125, 1260–1270. [Google Scholar] [CrossRef]
- Lombardi, A.F.; Afsahi, A.M.; Gupta, A.; Gholamrezanezhad, A. Severe acute respiratory syndrome (SARS), Middle East respiratory syndrome (MERS), influenza, and COVID-19, beyond the lungs: A review article. Radiol. Med. 2021, 126, 561–569. [Google Scholar] [CrossRef]
- Ierardi, A.M.; Wood, B.J.; Arrichiello, A.; Bottino, N.; Bracchi, L.; Forzenigo, L.; Andrisani, M.C.; Vespro, V.; Bonelli, C.; Amalou, A.; et al. Preparation of a radiology department in an Italian hospital dedicated to COVID-19 patients. Radiol. Med. 2020, 125, 894–901. [Google Scholar] [CrossRef]
- Fichera, G.; Stramare, R.; De Conti, G.; Motta, R.; Giraudo, C. It’s not over until it’s over: The chameleonic behavior of COVID-19 over a six-day period. Radiol. Med. 2020, 125, 514–516. [Google Scholar] [CrossRef]
- Reginelli, A.; Grassi, R.; Feragalli, B.; Belfiore, M.; Montanelli, A.; Patelli, G.; La Porta, M.; Urraro, F.; Fusco, R.; Granata, V.; et al. Coronavirus Disease 2019 (COVID-19) in Italy: Double Reading of Chest CT Examination. Biology 2021, 10, 89. [Google Scholar] [CrossRef]
- Grassi, R.; Fusco, R.; Belfiore, M.P.; Montanelli, A.; Patelli, G.; Urraro, F.; Petrillo, A.; Granata, V.; Sacco, P.; Mazzei, M.A.; et al. Coronavirus disease 2019 (COVID-19) in Italy: Features on chest computed tomography using a structured report system. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Questions | Yes | No |
|---|---|---|
| Do you have fever at the moment? | ||
| Do you have cough? | ||
| Did you have dyspnea or any respiratory disease, recently? | ||
| Did you have anosmia or dysgeusia symptoms, recently? | ||
| Did you have diarrhea, recently? | ||
| Did you have unusual fatigue, recently? | ||
| Did you have rash or ophthalmological disorders, recently? | ||
| Have you done COVID-19 serology test? | If yes, ask for the test’s result | |
| Have you performed nasopharyngeal swab for COVID-19? | If yes, ask for the test’s result |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maio, F.; Tari, D.U.; Granata, V.; Fusco, R.; Grassi, R.; Petrillo, A.; Pinto, F. Breast Cancer Screening during COVID-19 Emergency: Patients and Department Management in a Local Experience. J. Pers. Med. 2021, 11, 380. https://doi.org/10.3390/jpm11050380
Maio F, Tari DU, Granata V, Fusco R, Grassi R, Petrillo A, Pinto F. Breast Cancer Screening during COVID-19 Emergency: Patients and Department Management in a Local Experience. Journal of Personalized Medicine. 2021; 11(5):380. https://doi.org/10.3390/jpm11050380
Chicago/Turabian StyleMaio, Francesca, Daniele Ugo Tari, Vincenza Granata, Roberta Fusco, Roberta Grassi, Antonella Petrillo, and Fabio Pinto. 2021. "Breast Cancer Screening during COVID-19 Emergency: Patients and Department Management in a Local Experience" Journal of Personalized Medicine 11, no. 5: 380. https://doi.org/10.3390/jpm11050380