Acceptance and Commitment Therapy (ACT) Improves Sleep Quality, Experiential Avoidance, and Emotion Regulation in Individuals with Insomnia—Results from a Randomized Interventional Study

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Methods
2.1. Study Procedure
2.2. Participants
2.3. Sample Size Calculation
2.4. Randomization
2.5. Measures
2.5.1. Experiential Avoidance
2.5.2. Subjective Sleep: Pittsburgh Sleep Quality Index (PSQI)
2.5.3. Sleep Log
2.5.4. Dysfunctional Beliefs and Attitudes about Sleep (DBAS)
2.5.5. Sleep Problem Acceptance Questionnaire (SPAQ)
2.5.6. Difficulties in Emotion Regulation Scale (DERS)
2.6. Intervention: Acceptance and Commitment Therapy (ACT)
2.7. Active Control Condition
2.8. Statistical Analysis
3. Results
3.1. Sociodemographic and Sleep-Related Information at Baseline
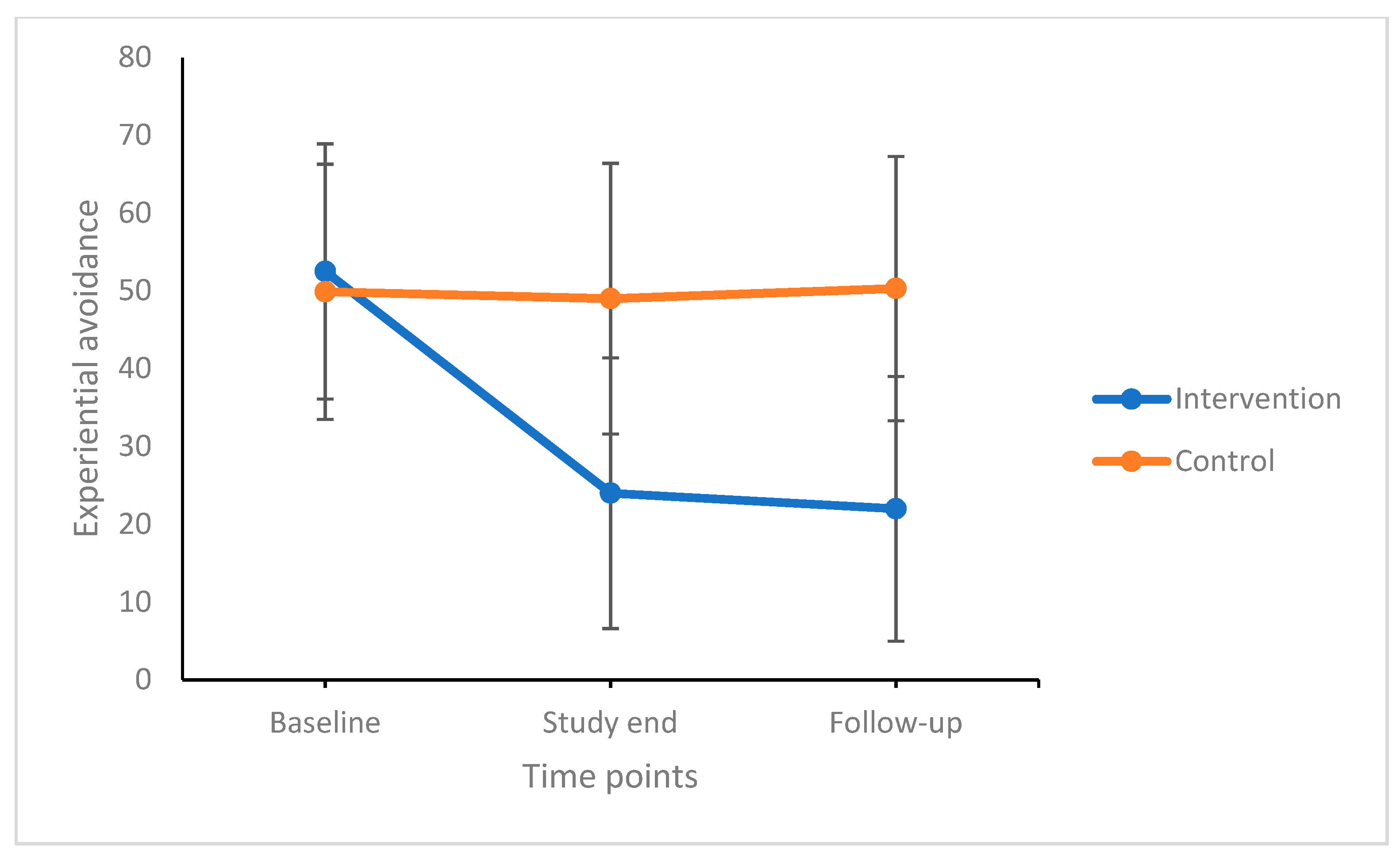
3.2. Changes in Subjective Sleep Quality, Dysfunctional Beliefs and Attitudes about Sleep, Sleep Problems Acceptance, Difficulties in Emotion Regulation, and Experiential Avoidance over Time between and within the Intervention and Control Conditions
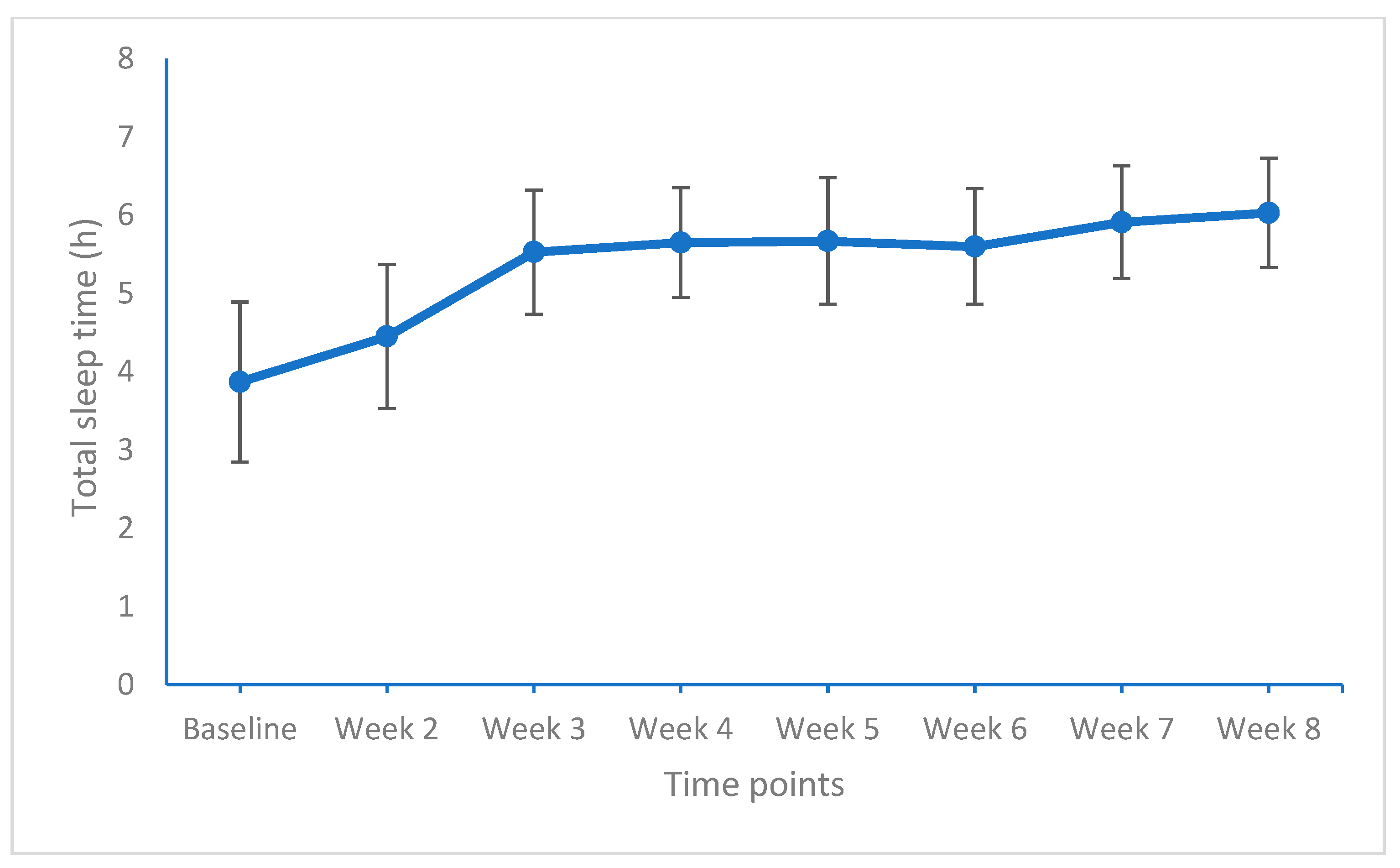
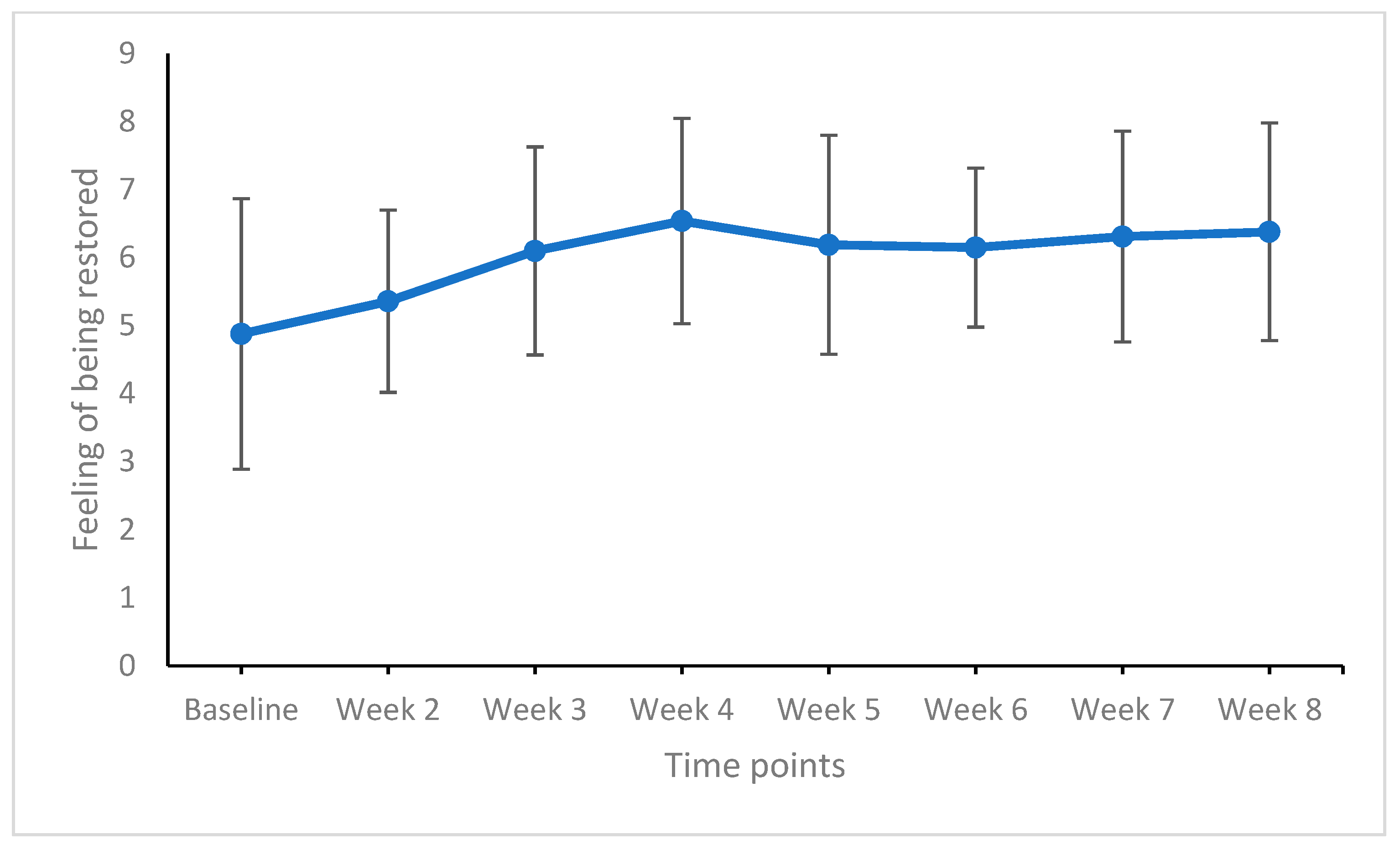
3.3. Micro-Analysis; Weekly Changes in Total Sleep Time, Sleep Quality, and the Feeling of Being Restored in the Intervention Group
3.4. Changes in Experiential Avoidance and Associations with Sleep Quality, Dysfunctional Beliefs and Attitudes about Sleep, Sleep Problems Acceptance, and Difficulties in Emotion Regulation at the End of the Study in the Intervention Condition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kyle, S.D.; Morgan, K.; Espie, C.A. Insomnia and health-related quality of life. Sleep Med. Rev. 2010, 14, 69–82. [Google Scholar] [CrossRef]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef]
- Moree, W.J.; Li, B.-F.; Jovic, F.; Coon, T.; Yu, J.; Gross, R.S.; Tucci, F.; Marinkovic, D.; Zamani-Kord, S.; Malany, S. Characterization of novel selective H1-antihistamines for clinical evaluation in the treatment of insomnia. J. Med. Chem. 2009, 52, 5307–5310. [Google Scholar] [CrossRef]
- Morin, C.M.; LeBlanc, M.; Daley, M.; Gregoire, J.; Merette, C. Epidemiology of insomnia: Prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Med. 2006, 7, 123–130. [Google Scholar] [CrossRef]
- Saddichha, S. Diagnosis and treatment of chronic insomnia. Ann. Indian Acad. Neurol. 2010, 13, 94. [Google Scholar] [CrossRef]
- Bioulac, S.; Franchi, J.M.; Arnaud, M.; Sagaspe, P.; Moore, N.; Salvo, F.; Philip, P. Risk of Motor Vehicle Accidents Related to Sleepiness at the Wheel: A Systematic Review and Meta-Analysis. Sleep 2017, 40. [Google Scholar] [CrossRef] [Green Version]
- Garbarino, S.; Magnavita, N.; Guglielmi, O.; Maestri, M.; Dini, G.; Bersi, F.M.; Toletone, A.; Chiorri, C.; Durando, P. Insomnia is associated with road accidents. Further evidence from a study on truck drivers. PLoS ONE 2017, 12, e0187256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goncalves, M.; Amici, R.; Lucas, R.; Akerstedt, T.; Cirignotta, F.; Horne, J.; Leger, D.; McNicholas, W.T.; Partinen, M.; Teran-Santos, J.; et al. Sleepiness at the wheel across Europe: A survey of 19 countries. J. Sleep Res. 2015, 24, 242–253. [Google Scholar] [CrossRef]
- Gupta, R.; Pandi-Perumal, S.R.; Almeneessier, A.S.; BaHammam, A.S. Hypersomnolence and Traffic Safety. Sleep Med. Clin. 2017, 12, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Leger, D.; Bayon, V.; Ohayon, M.M.; Philip, P.; Ement, P.; Metlaine, A.; Chennaoui, M.; Faraut, B. Insomnia and accidents: Cross-sectional study (EQUINOX) on sleep-related home, work and car accidents in 5293 subjects with insomnia from 10 countries. J. Sleep Res. 2014, 23, 143–152. [Google Scholar] [CrossRef] [Green Version]
- Godet-Cayré, V.; Pelletier-Fleury, N.; Le Vaillant, M.; Dinet, J.; Massuel, M.A.; Léger, D. Insomnia and absenteeism at work. Who pays the cost? Sleep 2006, 29, 179–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leger, D. Working with poor sleep. Sleep 2014, 37, 1401–1403. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, L.R.; Fischer, F.M.; Lowden, A. Sleep deprivation of working adolescents--A hidden work hazard. Scand. J. Work Environ. Health 2006, 32, 328–330. [Google Scholar] [CrossRef] [Green Version]
- Kawakami, N.; Takatsuka, N.; Shimizu, H. Sleep disturbance and onset of type 2 diabetes. Diabetes Care 2004, 27, 282–283. [Google Scholar] [CrossRef] [Green Version]
- Mallon, L.; Broman, J.E.; Hetta, J. Sleep complaints predict coronary artery disease mortality in males: A 12-year follow-up study of a middle-aged Swedish population. J. Intern. Med. 2002, 251, 207–216. [Google Scholar] [CrossRef]
- Hertenstein, E.; Feige, B.; Gmeiner, T.; Kienzler, C.; Spiegelhalder, K.; Johann, A.; Jansson-Fröjmark, M.; Palagini, L.; Rücker, G.; Riemann, D. Insomnia as a predictor of mental disorders: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 43, 96–105. [Google Scholar] [CrossRef]
- American Academy of Sleep Medicine. The International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Dolenc Groselj, L.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Gonçalves, M.; et al. European guideline for the diagnosis and treatment of insomnia. J. Sleep Res. 2017, 26, 675–700. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Lee, C.T.; Yeung, W.F.; Chan, M.S.; Chung, E.W.; Lin, W.L. Sleep hygiene education as a treatment of insomnia: A systematic review and meta-analysis. Fam. Pr. 2018, 35, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.R.; Dickson, C.; Han, H. Cognitive behavioural treatment for insomnia in primary care: A systematic review of sleep outcomes. Br. J. Gen. Pract. J. R. Coll. Gen. Pract. 2019, 69, e657–e664. [Google Scholar] [CrossRef]
- Seyffert, M.; Lagisetty, P.; Landgraf, J.; Chopra, V.; Pfeiffer, P.N.; Conte, M.L.; Rogers, M.A. Internet-Delivered Cognitive Behavioral Therapy to Treat Insomnia: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0149139. [Google Scholar] [CrossRef]
- Zachariae, R.; Lyby, M.S.; Ritterband, L.M.; O’Toole, M.S. Efficacy of internet-delivered cognitive-behavioral therapy for insomnia-A systematic review and meta-analysis of randomized controlled trials. Sleep Med. Rev. 2015, 30, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Trauer, J.M.; Qian, M.Y.; Doyle, J.S.; Rajaratnam, S.M.; Cunnington, D. Cognitive Behavioral Therapy for Chronic Insomnia: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2015, 163, 191–204. [Google Scholar] [CrossRef]
- Banno, M.; Harada, Y.; Taniguchi, M.; Tobita, R.; Tsujimoto, H.; Tsujimoto, Y.; Kataoka, Y.; Noda, A. Exercise can improve sleep quality: A systematic review and meta-analysis. PeerJ 2018, 6, e5172. [Google Scholar] [CrossRef] [Green Version]
- Cristini, J.; Weiss, M.; De Las Heras, B.; Medina-Rincón, A.; Dagher, A.; Postuma, R.B.; Huber, R.; Doyon, J.; Rosa-Neto, P.; Carrier, J.; et al. The effects of exercise on sleep quality in persons with Parkinson’s disease: A systematic review with meta-analysis. Sleep Med. Rev. 2020, 55, 101384. [Google Scholar] [CrossRef] [PubMed]
- Mercier, J.; Savard, J.; Bernard, P. Exercise interventions to improve sleep in cancer patients: A systematic review and meta-analysis. Sleep Med. Rev. 2017, 36, 43–56. [Google Scholar] [CrossRef]
- Yang, P.Y.; Ho, K.H.; Chen, H.C.; Chien, M.Y. Exercise training improves sleep quality in middle-aged and older adults with sleep problems: A systematic review. J. Physiother. 2012, 58, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Rusch, H.L.; Rosario, M.; Levison, L.M.; Olivera, A.; Livingston, W.S.; Wu, T.; Gill, J.M. The effect of mindfulness meditation on sleep quality: A systematic review and meta-analysis of randomized controlled trials. Ann. N. Y. Acad. Sci. 2019, 1445, 5–16. [Google Scholar] [CrossRef]
- Brand, S.; Holsboer-Trachsler, E.; Naranjo, J.R.; Schmidt, S. Influence of mindfulness practice on cortisol and sleep in long-term and short-term meditators. Neuropsychobiology 2012, 65, 109–118. [Google Scholar] [CrossRef]
- Yeung, V.; Sharpe, L.; Glozier, N.; Hackett, M.L.; Colagiuri, B. A systematic review and meta-analysis of placebo versus no treatment for insomnia symptoms. Sleep Med. Rev. 2018, 38, 17–27. [Google Scholar] [CrossRef]
- Harvey, A.G.; Tang, N.K. Cognitive behaviour therapy for primary insomnia: Can we rest yet? Sleep Med. Rev. 2003, 7, 237–262. [Google Scholar] [CrossRef]
- Dalrymple, K.L.; Fiorentino, L.; Politi, M.C.; Posner, D. Incorporating principles from acceptance and commitment therapy into cognitive-behavioral therapy for insomnia: A case example. J. Contemp. Psychother. 2010, 40, 209–217. [Google Scholar] [CrossRef]
- Biglan, A.; Hayes, S.C.; Pistorello, J. Acceptance and commitment: Implications for prevention science. Prev. Sci. 2008, 9, 139–152. [Google Scholar] [CrossRef] [Green Version]
- Eustis, E.H.; Hayes-Skelton, S.A.; Roemer, L.; Orsillo, S.M. Reductions in experiential avoidance as a mediator of change in symptom outcome and quality of life in acceptance-based behavior therapy and applied relaxation for generalized anxiety disorder. Behav. Res. 2016, 87, 188–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, R. Embracing your demons: An overview of acceptance and commitment therapy. Psychother. Aust. 2006, 12, 2–8. [Google Scholar]
- Hayes, S.C. Acceptance and commitment therapy: Towards a unified model of behavior change. World Psychiatry Off. J. World Psychiatr. Assoc. (Wpa) 2019, 18, 226–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, S.C. Acceptance and Commitment Therapy, Relational Frame Theory, and the Third Wave of Behavioral and Cognitive Therapies - Republished Article. Behav. Ther. 2016, 47, 869–885. [Google Scholar] [CrossRef]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and commitment therapy: Model, processes and outcomes. Behav Res 2006, 44, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Stockton, D.; Kellett, S.; Berrios, R.; Sirois, F.; Wilkinson, N.; Miles, G. Identifying the Underlying Mechanisms of Change During Acceptance and Commitment Therapy (ACT): A Systematic Review of Contemporary Mediation Studies. Behav. Cogn. Psychother. 2019, 47, 332–362. [Google Scholar] [CrossRef]
- Wicksell, R.K.; Olsson, G.L.; Hayes, S.C. Psychological flexibility as a mediator of improvement in Acceptance and Commitment Therapy for patients with chronic pain following whiplash. Eur. J. Pain 2010, 14, 1059.e1051–1059.e1011. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.Q.; Leeming, E.; Smith, P.; Chung, P.K.; Hagger, M.S.; Hayes, S.C. Acceptance and Commitment Therapy for Health Behavior Change: A Contextually-Driven Approach. Front Psychol. 2017, 8, 2350. [Google Scholar] [CrossRef]
- Harris, R. ACT Made Simple: An Easy-to-Read Primer on Acceptance and Commitment Therapy; New Harbinger Press: Oakland, CA, USA, 2019. [Google Scholar]
- Eifert, G.H. Acceptance and Commitment Therapy (ACT); Hogrefe: Göttingen, Germany, 2011. [Google Scholar]
- Folke, F.; Parling, T.; Melin, L. Acceptance and commitment therapy for depression: A preliminary randomized clinical trial for unemployed on long-term sick leave. Cogn. Behav. Pract. 2012, 19, 583–594. [Google Scholar] [CrossRef]
- Swain, J.; Hancock, K.; Hainsworth, C.; Bowman, J. Acceptance and commitment therapy in the treatment of anxiety: A systematic review. Clin. Psychol. Rev. 2013, 33, 965–978. [Google Scholar] [CrossRef] [PubMed]
- Twohig, M.P. Acceptance and commitment therapy for treatment-resistant posttraumatic stress disorder: A case study. Cogn. Behav. Pract. 2009, 16, 243–252. [Google Scholar] [CrossRef]
- Salari, N.; Khazaie, H.; Hosseinian-Far, A.; Khaledi-Paveh, B.; Ghasemi, H.; Mohammadi, M.; Shohaimi, S. The effect of acceptance and commitment therapy on insomnia and sleep quality: A systematic review. BMC Neurol 2020, 20, 300. [Google Scholar] [CrossRef]
- Khazaie, H.; Zakiei, A.; Rezaei, M.; Hoseini, S.M.; Alikhani, M. Emotional dysregulation leads to reduced sleep quality when the level of repetitive negative thoughts is high: Findings of a structural equation model. Iran. J. Psychiatry Behav. Sci. 2019, 13. [Google Scholar] [CrossRef]
- Khazaie, H.; Zakiei, A.; Komasi, S. A simultaneous cluster analysis of cognitive, emotional, and personality factors and insomnia and sleep quality among earthquake victims. Disaster Med. Public Health Prep. 2019, 13, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Lappalainen, P.; Langrial, S.; Oinas-Kukkonen, H.; Muotka, J.; Lappalainen, R. ACT for sleep-internet-delivered self-help ACT for sub-clinical and clinical insomnia: A randomized controlled trial. J. Contextual Behav. Sci. 2019, 12, 119–127. [Google Scholar] [CrossRef]
- Hertenstein, E.; Thiel, N.; Lüking, M.; Külz, A.K.; Schramm, E.; Baglioni, C.; Spiegelhalder, K.; Riemann, D.; Nissen, C. Quality of Life Improvements after Acceptance and Commitment Therapy in Nonresponders to Cognitive Behavioral Therapy for Primary Insomnia. Psychother. Psychosom. 2014, 83, 371–373. [Google Scholar] [CrossRef]
- Daly-Eichenhardt, A.; Scott, W.; Howard-Jones, M.; Nicolaou, T.; McCracken, L.M. Changes in Sleep Problems and Psychological Flexibility following Interdisciplinary Acceptance and Commitment Therapy for Chronic Pain: An Observational Cohort Study. Front Psychol 2016, 7, 1326. [Google Scholar] [CrossRef] [Green Version]
- Garland, S.N.; Zhou, E.S.; Gonzalez, B.D.; Rodriguez, N. The quest for mindful sleep: A critical synthesis of the impact of mindfulness-based interventions for insomnia. Curr. Sleep Med. Rep. 2016, 2, 142–151. [Google Scholar] [CrossRef] [Green Version]
- McCracken, L.M.; Williams, J.L.; Tang, N.K. Psychological flexibility may reduce insomnia in persons with chronic pain: A preliminary retrospective study. Pain Med. 2011, 12, 904–912. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Strosahl, K.; Wilson, K.G.; Bissett, R.T.; Pistorello, J.; Toarmino, D.; Polusny, M.A.; Dykstra, T.A.; Batten, S.V.; Bergan, J. Measuring experiential avoidance: A preliminary test of a working model. Psychol. Rec. 2004, 54, 553–578. [Google Scholar] [CrossRef] [Green Version]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy; The Guilford Press: New York NY, USA, 2012. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Khazaie, H.; Zakiei, A. Efficacy of Acceptance and Commitment Therapyon Emotional Dysregulation and Sleep Quality in Patientswith Chronic Insomnia. J. Maz. Univ. Med Sci. 2019, 29, 52–63. [Google Scholar]
- Zakiei, A.; Khazaie, H. The Effectiveness of Acceptance and Commitment Therapy on Insomnia Patients (A Single-arm Trial Plan). J. Turk. Sleep Med. 2019, 6, 65–73. [Google Scholar] [CrossRef]
- First, M. Structured Clinical Interview for the DSM (SCID). In The Encyclopedia of Clinical Psychology; Wiley: Marblehead, MA, USA, 2015; pp. 1–6. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Alikhani, M.; Ebrahimi, A.; Farnia, V.; Khazaie, H.; Radmehr, F.; Mohamadi, E.; Davarinejad, O.; Dürsteler, K.; Sadeghi Bahmani, D.; Brand, S. Effects of treatment of sleep disorders on sleep, psychological and cognitive functioning and biomarkers in individuals with HIV/AIDS and under methadone maintenance therapy. J. Psychiatr. Res. 2020, 130, 260–272. [Google Scholar] [CrossRef]
- Farnia, V.; Alikhani, M.; Ebrahimi, A.; Golshani, S.; Sadeghi Bahmani, D.; Brand, S. Ginseng treatment improves the sexual side effects of methadone maintenance treatment. Psychiatry Res. 2019, 276, 142–150. [Google Scholar] [CrossRef]
- Jahangard, L.; Sadeghi, A.; Ahmadpanah, M.; Holsboer-Trachsler, E.; Sadeghi Bahmani, D.; Haghighi, M.; Brand, S. Influence of adjuvant omega-3-polyunsaturated fatty acids on depression, sleep, and emotion regulation among outpatients with major depressive disorders - Results from a double-blind, randomized and placebo-controlled clinical trial. J. Psychiatr. Res. 2018, 107, 48–56. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Farrahi Moghaddam, J.; Nakhaee, N.; Sheibani, V.; Garrusi, B.; Amirkafi, A. Reliability and validity of the Persian version of the Pittsburgh Sleep Quality Index (PSQI-P). Sleep Breath. Schlaf Atm. 2012, 16, 79–82. [Google Scholar] [CrossRef]
- Chehri, A.; Nourozi, M.; Eskandari, S.; Khazaie, H.; Hemati, N.; Jalali, A. Validation of the Persian version of the Pittsburgh Sleep Quality Index in elderly population. Sleep Sci. (Sao PauloBraz.) 2020, 13, 119–124. [Google Scholar] [CrossRef]
- Chehri, A.; Brand, S.; Goldaste, N.; Eskandari, S.; Brühl, A.; Sadeghi Bahmani, D.; Khazaie, H. Psychometric Properties of the Persian Pittsburgh Sleep Quality Index for Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 7095. [Google Scholar] [CrossRef]
- Backhaus, J.; Riemann, D. Schlafstörungen bewältigen [Treating Insomnia]; Beltz: Weinheim, Germany; Basel, Switzerland, 1996. [Google Scholar]
- Morin, C.M.; Vallières, A.; Ivers, H. Dysfunctional beliefs and attitudes about sleep (DBAS): Validation of a brief version (DBAS-16). Sleep 2007, 30, 1547–1554. [Google Scholar] [CrossRef] [Green Version]
- Bothelius, K.; Jernelöv, S.; Fredrikson, M.; McCracken, L.M.; Kaldo, V. Measuring acceptance of sleep difficulties: The development of the sleep problem acceptance questionnaire. Sleep 2015, 38, 1815–1822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gratz, K.L.; Roemer, L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- McKay, M.; Forsyth, J.P.; Eifert, G.H. Your Life on Purpose. How to Find What Matters and Create the Life You Want; New Harbinger Publications: Oakland, CA, USA, 2010. [Google Scholar]
- Wengenroth, M. Acceptance and Commitment Therapy (ACT); Therapy Tools; Beltz: Weinheim, Germany; Basel, Switzerland, 2017. [Google Scholar]
- Sadeghi Bahmani, D.; Motl, R.W.; Razazian, N.; Khazaie, H.; Brand, S. Aquatic exercising may improve sexual function in females with multiple sclerosis—An exploratory study. Mult. Scler. Relat. Disord. 2020, 43, 102106. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi Bahmani, D.; Razazian, N.; Farnia, V.; Alikhani, M.; Tatari, F.; Brand, S. Compared to an active control condition, in persons with multiple sclerosis two different types of exercise training improved sleep and depression, but not fatigue, paresthesia, and intolerance of uncertainty. Mult. Scler. Relat. Disord. 2019. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi Bahmani, D.; Razazian, N.; Motl, R.W.; Farnia, V.; Alikhani, M.; Pühse, U.; Gerber, M.; Brand, S. Physical activity interventions can improve emotion regulation and dimensions of empathy in persons with multiple sclerosis: An exploratory study. Mult. Scler. Relat. Disord. 2020, 37, 101380. [Google Scholar] [CrossRef] [PubMed]
- Jasbi, M.; Sadeghi Bahmani, D.; Karami, G.; Omidbeygi, M.; Peyravi, M.; Panahi, A.; Mirzaee, J.; Holsboer-Trachsler, E.; Brand, S. Influence of adjuvant mindfulness-based cognitive therapy (MBCT) on symptoms of post-traumatic stress disorder (PTSD) in veterans-results from a randomized control study. Cogn. Behav. 2018. [Google Scholar] [CrossRef]
- Norouzi, E.; Gerber, M.; Masrur, F.; Vaezmousavi, M.; Pühse, U.; Brand, S. Implementation of a Mindfulness-Based Stress Reduction (MBSR) program to reduce stress, anxiety and depression and to improve psychological well-being among retired Iranian football players. Psychol. Sport Exerc. 2019, 36. [Google Scholar] [CrossRef]
- Cordier, D.; Gerber, M.; Brand, S. Effects of two types of exercise training on psychological well-being, sleep, quality of life and physical fitness in patients with high-grade glioma (WHO III and IV): Study protocol for a randomized controlled trial. Cancer Commun. (Lond. Engl.) 2019, 39, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcus, D.K.; O’Connell, D.; Norris, A.L.; Sawaqdeh, A. Is the Dodo bird endangered in the 21st century? A meta-analysis of treatment comparison studies. Clin. Psychol. Rev. 2014, 34, 519–530. [Google Scholar] [CrossRef]
- Becker, B.J. Synthesizing standardized mean-change measures. Br. J. Math. Stat. Psychol. 1988, 41, 257–278. [Google Scholar] [CrossRef]
- Harvey, A.G. A transdiagnostic approach to treating sleep disturbance in psychiatric disorders. Cogn. Behav. 2009, 38 (Suppl. 1), 35–42. [Google Scholar] [CrossRef]
- Leventhal, A.M.; Zvolensky, M.J. Anxiety, depression, and cigarette smoking: A transdiagnostic vulnerability framework to understanding emotion-smoking comorbidity. Psychol. Bull. 2015, 141, 176–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norton, P.J.; Barrera, T.L.; Mathew, A.R.; Chamberlain, L.D.; Szafranski, D.D.; Reddy, R.; Smith, A.H. Effect of transdiagnostic cbt for anxiety disorders on comorbid diagnoses. Depress Anxiety 2013, 30, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Norton, P.J.; Paulus, D.J. Toward a Unified Treatment for Emotional Disorders: Update on the Science and Practice. Behav. Ther. 2016, 47, 854–868. [Google Scholar] [CrossRef]
- Norton, P.J.; Roberge, P. Transdiagnostic Therapy. Psychiatr. Clin. North Am. 2017, 40, 675–687. [Google Scholar] [CrossRef]
- Pearl, S.B.; Norton, P.J. Transdiagnostic versus diagnosis specific cognitive behavioural therapies for anxiety: A meta-analysis. J. Anxiety Disord. 2017, 46, 11–24. [Google Scholar] [CrossRef]
- Holtzman, N.S.; Strube, M.J. Above and beyond short-term mating, long-term mating is uniquely tied to human personality. Evol. Psychol. Int. J. Evol. Approaches Psychol. Behav. 2013, 11, 1101–1129. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Session | Specification |
|---|---|
| Session One |
|
| Session Two |
|
| Sessions Threeand Four |
|
| Sessions Fiveand Six |
|
| Sessions Sevenand Eight |
|
| Groups | Statistics | ||
|---|---|---|---|
| Intervention | Control | ||
| N | 17 | 18 | |
| Sex (female/male) | 10/7 | 12/6 | X2(N = 35, df = 1) = 0.23 |
| Civil status (single/married) | 5/12 | 6/12 | X2(N = 35, df = 1) = 0.06 |
| Highest education (middle school/diploma/higher education) | 2/10/5 | 8/4/6 | X2(N = 35, df = 1) = 6.24 * |
| Current job position (unemployed/employed) | 12/5 | 8/10 | X2(N = 35, df = 1) = 2.58 |
| M (SD) | M (SD) | ||
| Age (years) | 41.45 (8.66) | 41.47 (7.48) | t(33) = 0.01 |
| Weight | 69.89 (11.37) | 74.35 (11.32) | t(33) = 1.16 |
| Pittsburgh Sleep Quality Index (PSQI) | 15.76 (2.13) | 18.00 (3.14) | t(33) = 2.44 * d = 0.83 (L) |
| Dysfunctional Beliefs and Attitudes about Sleep (DBAS) | 90.82 (10.44) | 84.78 (12.62) | t(33) = 1.54 d = 0.52 (M) |
| Sleep Problem Acceptance (SPAQ) | 17.76 (6.75) | 11.22 (6.52) | t(33) = 2.92 ** d = 0.98 (L) |
| Experiential Avoidance (EA) | 52.70 (8.97) | 49.89 (16.43) | t(33) = 0.62 d = 0.21 (S) |
| Difficulties in emotion regulation scale (DERS) | 108.88 (28.67) | 126.44 (27.87) | t(33) = 1.84 d = 0.62 (M) |
| Baseline | Study End | Follow-Up | ||||
|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | Intervention | Control | |
| N | 17 | 18 | 17 | 18 | 17 | 18 |
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | |
| Pittsburgh Sleep Quality Index (PSQI) | 15.76 (2.13) | 18.00 (3.14) | 4.77 (2.54) | 12.89 (5.26) | 4.06 (1.75) | 12.50 (4.58) |
| Dysfunctional Beliefs and Attitudes about Sleep (DBAS) | 90.82 (10.44) | 84.78 (12.62) | 31.76 (16.002) | 81.88 (13.32) | 31.29 (14.69) | 81.05 (13.59) |
| Sleep Problem Acceptance (SPAQ) | 17.76 (6.75) | 11.22 (6.52) | 35.71 (7.39) | 13 (7.93) | 37.89 (8.56) | 14.06 (7.53) |
| Experiential Avoidance (EA) | 52.53 (8.71) | 49.89 (16.43) | 24.06 (8.81) | 49.78 (17.36) | 22.29 (7.72) | 50.28 (17.03) |
| Difficulties in emotion regulation scale (DERS) | 108.88 (28.67) | 126.44 (27.87) | 60.47 (13.26) | 126.22 (27.11) | 62.29 (14.68) | 128.94 (25.42) |
| Inferential Statistics | |||||||
|---|---|---|---|---|---|---|---|
| Time | Group | Time × Group Interaction | Greenhouse-Geisser ε | ||||
| F | (ES) | F | (ES) | F | (ES) | ||
| Sleep quality (PSQI) | F(2,64) = 0.843 | 0.026 (S) | F(1,32) = 29.94 *** | 0.484 (L) | F(2,64) = 27.01 *** | 0.458 (L) | 0.596 |
| Dysfunctional Beliefs and Attitudes about Sleep (DBAS) | F(2,64) = 5.36 * | 0.143 (L) | F(1,32) = 39.40 *** | 0.552 (L) | F(2,64) = 207.82 *** | 0.867 (L) | 0.529 |
| Sleep Problem Acceptance (SPAQ) | F(2,64) = 0.092 | 0.003 (T) | F(1,32) = 40.69 *** | 0.560 (L) | F(2,64) = 112.32 *** | 0.778 (L) | 0.742 |
| Experiential Avoidance (EA) | F(2,64) = 2.31 | 0.832 (L) | F(1,32) = 8.36 ** | 0.207 (L) | F(2,64) = 141.89 *** | 0.816 (L) | 0.666 |
| Difficulties in emotion regulation scale (DERS) | F(2,64) = 1.52 | 0.045 (S) | F(1,32) = 34.06 *** | 0.516 (L) | F(2,64) = 34.92 *** | 0.522 (L) | 0.552 |
| Statistics | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| F ε | Week-by-Week Comparisons (Cohen’s d) | ||||||||
| Total sleep duration (h) | M (SD) | F(7,112) 39.04 *** 0.709 | BL-W2 | BL-W3 | BL-W4 | BL-W5 | BL-W6 | BL-W7 | BL-W8 |
| Baseline | 3.87 (1.02) | 0.59 (M) | 1.02 (L) | 1.95 (L) | 1.87 (L) | 1.95 (L) | 2.31 (L) | 2.46 (L) | |
| Week 2 | 4.45 (0.92) | - | W2-W3 | W2-W4 | W2-W5 | W2-W6 | W2-W7 | W2-W8 | |
| - | 1.25 (L) | 1.45 (L) | 1.38 (L) | 1.37 (L) | 1.76 (L) | 1.92 (L) | |||
| Week 3 | 5.53 (0.79) | - | - | W3-W4 | W3-W5 | W3-W6 | W3-W7 | W3-W8 | |
| - | - | 0.12 (T) | 0.16 (T) | 0.09 (T) | 0.50 (M) | 0.88 (L) | |||
| Week 4 | 5.65 (0.70) | - | - | - | W4-W5 | W4-W6 | W4-W7 | W4-W8 | |
| - | - | - | 0.01 (T) | 0.07 (T) | 0.36 (S) | 0.52 (M) | |||
| Week 5 | 5.67 (0.81) | - | - | - | - | W5-W6 | W5-W7 | W5-W8 | |
| - | - | - | - | 0.07 (T) | 0.34 (S) | 0.49 (S) | |||
| Week 6 | 5.60 (0.74) | - | - | - | - | - | W6-W7 | W6-W8 | |
| - | - | - | - | - | 0.42 (M) | 0.58 (M) | |||
| Week 7 | 5.91 (0.72) | - | - | - | - | - | - | W7-W8 | |
| - | - | - | - | - | - | 0.15 (T) | |||
| Week 8 | 6.03 (0.70) | - | - | - | - | - | - | - | |
| F ε | Week-by-Week Comparisons (Cohen’s d) | ||||||||
| Subjective sleep quality | M (SD) | F(7, 112) 10.82 *** 0.403 0.241 | BL-W2 | BL-W3 | BL-W4 | BL-W5 | BL-W6 | BL-W7 | BL-W8 |
| Baseline | 4.69 (1.45) | 0.49 (S) | 0.82 (L) | 0.82 (L) | 0.81 (L) | 0.91 (L) | 0.99 (L) | 1.04 (L) | |
| Week 2 | 5.34 (1.10) | - | W2-W3 | W2-W4 | W2-W5 | W2-W6 | W2-W7 | W2-W8 | |
| - | 0.43 (S) | 0.41 (S) | 0.42 (S) | 0.50 (M) | 0.62 (M) | 0.69 (M) | |||
| Week 3 | 5.89 (1.44) | - | - | W3-W4 | W3-W5 | W3-W6 | W3-W7 | W3-W8 | |
| - | - | 0.03 (T) | 0.01 (T) | 0.02 (T) | 0.51 (M) | 0.24 (M) | |||
| Week 4 | 5.85 (1.39) | - | - | - | W4-W5 | W4-W6 | W4-W7 | W4-W8 | |
| - | - | - | 0.01 (T) | 0.05 (T) | 0.20 (S) | 0.28 (S) | |||
| Week 5 | 5.87 (1.45) | - | - | - | - | W5-W6 | W5-W7 | W5-W8 | |
| - | - | - | - | 0.03 (T) | 0.19 (T) | 0.25 (S) | |||
| Week 6 | 5.92 (1.24) | - | - | - | - | - | W6-W7 | W6-W8 | |
| - | - | - | - | - | 0.17 (T) | 0.23 (S) | |||
| Week 7 | 6.15 (1.46) | - | - | - | - | - | - | W7-W8 | |
| - | - | - | - | - | - | 0.05 (T) | |||
| Week 8 | 6.23 (1.45) | - | - | - | - | - | - | - | |
| F ε | Week-by-Week Comparisons (Cohen’s d) | ||||||||
| Feeling of being restored | F(7, 112) 10.05 *** 0.386 0.234 | BL-W2 | BL-W3 | BL-W4 | BL-W5 | BL-W6 | BL-W7 | BL-W8 | |
| Baseline | 4.88 (1.99) | 0.29 (M) | 0.69 (M) | 0.95 (L) | 0.73 (M) | 0.78 (M) | 0.81 (L) | 0.84 (L) | |
| Week 2 | 5.36 (1.34) | - | W2-W3 | W2-W4 | W2-W5 | W2-W6 | W2-W7 | W2-W8 | |
| - | 0.51 (M) | 0.82 (L) | 0.56 (M) | 0.63 (M) | 0.66 (M) | 0.70 (M) | |||
| Week 3 | 6.10 (1.53) | - | - | W3-W4 | W3-W5 | W3-W6 | W3-W7 | W3-W8 | |
| - | - | 0.29 (S) | 0.06 (T) | 0.04 (T) | 0.14 (T) | 0.18 (T) | |||
| Week 4 | 6.54 (1.51) | - | - | - | W4-W5 | W4-W6 | W4-W7 | W4-W8 | |
| - | - | - | 0.22 (S) | 0.29 (S) | 0.15 (T) | 0.10 (T) | |||
| Week 5 | 6.19 (1.61) | - | - | - | - | W5-W6 | W5-W7 | W5-W8 | |
| - | - | - | - | 0.02 (T) | 0.08 (T) | 0.13 (T) | |||
| Week 6 | 6.15 (1.17) | - | - | - | - | - | W6-W7 | W6-W8 | |
| - | - | - | - | - | 0.12 (T) | 0.17 (T) | |||
| Week 7 | 6.31 (1.55) | - | - | - | - | - | - | W7-W8 | |
| - | - | - | - | - | - | 0.04 (T) | |||
| Week 8 | 6.38 (1.60) | - | - | - | - | - | - | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zakiei, A.; Khazaie, H.; Rostampour, M.; Lemola, S.; Esmaeili, M.; Dürsteler, K.; Brühl, A.B.; Sadeghi-Bahmani, D.; Brand, S. Acceptance and Commitment Therapy (ACT) Improves Sleep Quality, Experiential Avoidance, and Emotion Regulation in Individuals with Insomnia—Results from a Randomized Interventional Study. Life 2021, 11, 133. https://doi.org/10.3390/life11020133
Zakiei A, Khazaie H, Rostampour M, Lemola S, Esmaeili M, Dürsteler K, Brühl AB, Sadeghi-Bahmani D, Brand S. Acceptance and Commitment Therapy (ACT) Improves Sleep Quality, Experiential Avoidance, and Emotion Regulation in Individuals with Insomnia—Results from a Randomized Interventional Study. Life. 2021; 11(2):133. https://doi.org/10.3390/life11020133
Chicago/Turabian StyleZakiei, Ali, Habibolah Khazaie, Masoumeh Rostampour, Sakari Lemola, Maryam Esmaeili, Kenneth Dürsteler, Annette Beatrix Brühl, Dena Sadeghi-Bahmani, and Serge Brand. 2021. "Acceptance and Commitment Therapy (ACT) Improves Sleep Quality, Experiential Avoidance, and Emotion Regulation in Individuals with Insomnia—Results from a Randomized Interventional Study" Life 11, no. 2: 133. https://doi.org/10.3390/life11020133