
How the COVID-19 Pandemic Impacted Medical Education during the Last Year of Medical School: A Class Survey

 and
and
Abstract
:1. Introduction
2. Methods
3. Results
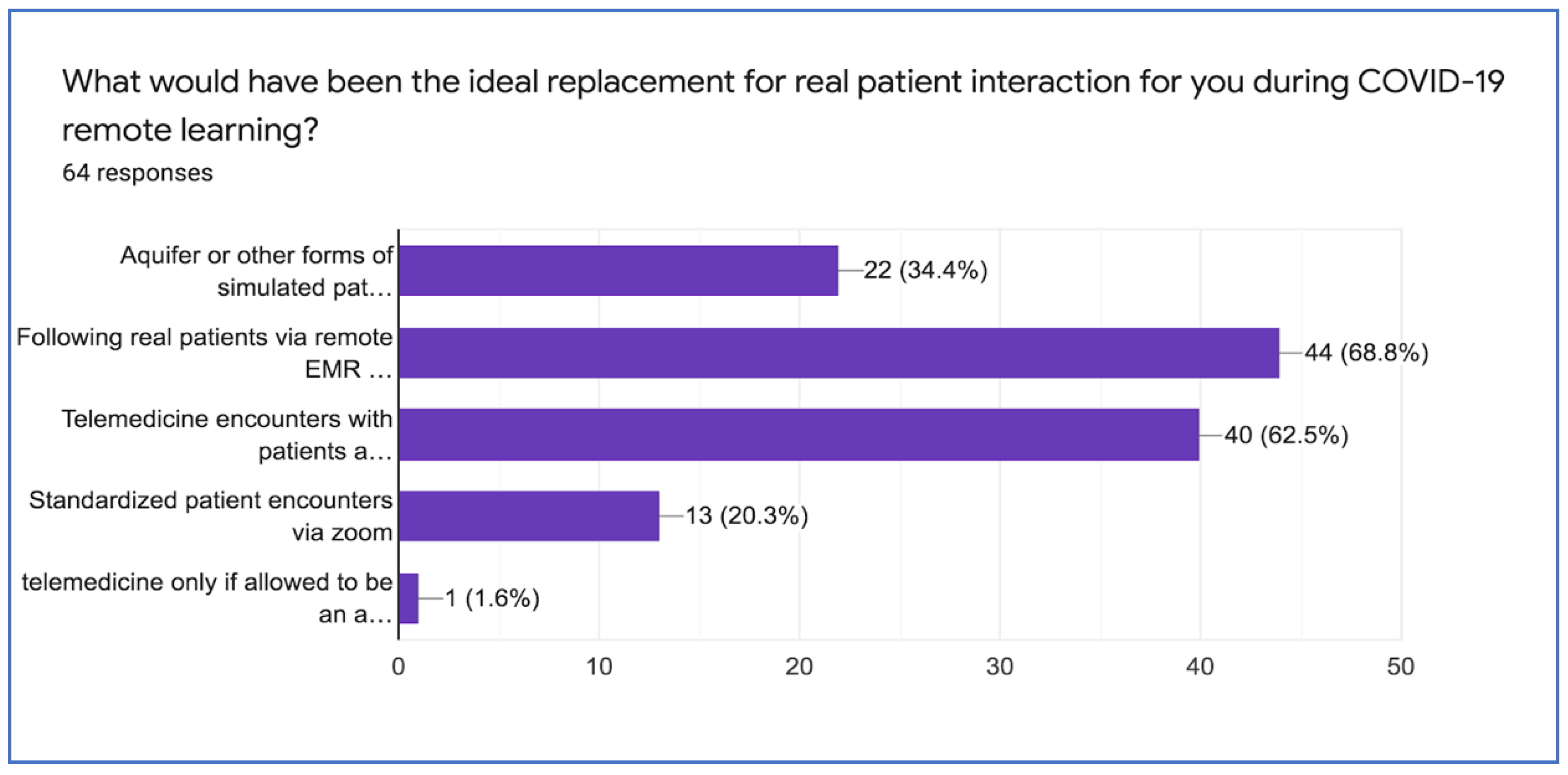
3.1. Quantitative Analysis
3.2. Qualitative Responses (Excerpts)
“Jacobs School of Medicine and Biomedical Sciences (JSMBS) did a good job considering the circumstances.”
3.3. In Person Learning Is Best
“I think that neuro rotation also gave me better exposure to learning how patient care works during a pandemic. Same with my surgery sub-i. It was there that I saw the frustration of forgetting to order the COVID test, faced the struggle of wearing N95 for 8 h during an emergency case, and even saw some vascular complications of COVID, and also was able to see teams work covid into their ddx’s where it wouldn’t have been previously. I saw none of this while I was reading aquifer cases.”
“The in-hospital learning was the only thing that was affected that mattered. Book learning which mainly occurs through Uworld and anki wasn’t. A feasible solution would be to allow medical students to still do rotations even though there will be less volume, it is better than anything else. If students find it too risky and wish to sacrifice their education, that is on them.”
3.4. Shortcomings of Remote Learning
“I think my outpatient gyn procedure skills suffered as a result of remote learning because I couldn’t see actual patients and perform procedures. I only did a model once with the clerkship director but I didn’t feel like that was enough for me.”
3.5. Fears
“Biggest fear is using medical students as free labor to deal with staffing concerns. If we are kept in the clinical environment it must be because it is truly safe and not because the hospitals need more bodies. School leadership needs to advocate for our wellbeing and work on building parallel curricula in the event that we are pulled out of in person learning. “Telemedicine is reasonable and has potential to be valuable part of education.”
“I think learning how telehealth works and even how to do as close as you can to a physical exam over telehealth would be INCREDIBLY valuable. I wish I could have tuned in to some pediatric telehealth visits and just seen how they did the exams! Valuable to have the “clinical experience” but also telehealth will likely become more and more important in our clinical arsenal, as I don’t think this will be the last pandemic we face in our careers.”
“The only reasonable response to a second wave of COVID-19 would be to implement a telemedicine care model via iPads to facilitate patient interaction whilst maintaining appropriate distance.”
4. Discussion
4.1. Strengths
4.2. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Themes/Subthemes | Student Quotes |
|---|---|
In person learning is best
| “I think students, especially those who will be graduating in less than 6 months should be kept in person as much as possible as they will soon be doctors, pandemic or not and must learn how to see patients so as not to compromise care as interns.” “I think that neuro rotation also gave me better exposure to learning how patient care works during a pandemic. Same with my surgery sub-i…It was there that I saw the frustration of forgetting to order the COVID test, faced the struggle of wearing N95 for 8 h during an emergency case, and even saw some vascular complications of COVID, and also was able to see teams work covid into their ddx’s where it wouldn’t have been previously. I saw none of this while I was reading aquifer cases.” |
| Desire for better communication, more unified approach | “We really need better communication with the deans. We never know what’s happening during this.” “There should be a unified approach throughout all clerkships. Try to get students to participate in rounds virtually and do aquifer cases as well. I think those 2 options are the best.” |
Areas missed out on: practical/procedural skills
| “I do feel like I missed out on some practical skills because of COVID. I think more in person simulations, if possible if the school does not close, would be helpful if we can’t be in hospitals.” “Students are most impacted by the lack of resident/attending teaching because they miss bedside rounds, as well as increased time strain from COVID patients in general. I think my outpatient gyn procedure skills suffered as a result of remote learning because I couldn’t see actual patients and perform procedures. I only did a model once with the clerkship director but I didn’t feel like that was enough for me.” “I really felt most engaged during the family medicine morning rounds with Dr. Corliss. She would ask us questions about the disease process at random, and as much as it was stressful, you couldn’t disengage.” |
| JSMBS did a good job with what they had; there is no good replacement | “Surgery clerkship leader (Dr. M) did a good job in response to generate a curriculum. WISE-MD was very helpful. She also got feedback from us to try to reduce the amount of Aquifer and cut out a few of the low-yield faculty lectures.” “Overall, I feel the school did pretty well with the remote learning (aquifer and other guided cases, videos for content review, small group sessions) and with brief clinical exposure when it was safe to do so.” “I feel that UB did a great job implementing a virtual curriculum within a very timely fashion, within the context of a unique global pandemic. Although nothing replaces real in-person interactions, I believe that the Aquifer cases and assigned videos/readings were adequate to learn the necessary material and then the shortened clinical immersion experiences gave the opportunity to apply that learned material.” |
| Desire for better replacement than Aquifer learning modules | “I would really like to see the university not rely as much on aquifer for our education should there be a second wave. The cases were too easy to click through and disengage from, and third year is normally so clinical and so engaging it felt like I wasn’t even in medical school.” “Virtual stimulated cases like aquifer are poor replacements and become just another chore for students to perform.” “I think clerkship administration did the best they could in response to COVID. But since they could prepare more for a second wave, methods of learning other than Aquifer would be useful, such as telemedicine visits, following patients virtually through EMR, etc.” |
Fears:
| “I have been asked a few times on interviews how my education was affected by covid, and I made the mistake of telling the first place I only have 8 days of actual in person peds clinical experience and 8 days of family med in person clinical experience and I think I just scared the crap out of them hiring me.” “When my N95 was crushed and pretty much ruined, it was really key that one of the attendings was assertive in securing a new one for me from the NICU, because I had had issues when I went down by myself to get a new one. Understandably so—I know PPE is in high demand. But it can be tough to advocate for yourself when you’re a med student on the wards and some folks don’t think you need one.” “Biggest fear is using medical students as free labor to deal with staffing concerns. If we are kept in the clinical environment it must be because it is truly safe and not because the hospitals need more bodies. School leadership needs to advocate for our wellbeing and work on building parallel curricula in the event that we are pulled out of in person learning.” |
Telemedicine is reasonable and valuable part of our education
| “I think telemedicine would be an amazing to introduce into our education. Especially since post-COVID most are predicting this will become standard practice...I also think we could have done more educating students on COVID and what healthcare looks like in the midst of a pandemic.” “I think learning how telehealth works and even how to do as close as you can to a physical exam over telehealth would be INCREDIBLY valuable. I wish I could have tuned in to some pediatric telehealth visits and just seen how they did the exams! Valuable to have the “clinical experience” but also telehealth will likely become more and more important in our clinical arsenal, as I don’t think this will be the last pandemic we face in our careers. I think telemedicine is a reasonable option but both faculty and students need to be taught how to make this happen. Students should not just be silent observers on telemedicine calls.” |
| Following patients virtually is a feasible option | “I felt following patients via EMR was most effective. This was essentially my daily exercise prior to COVID except it leaves out the physical exam, which can’t be replaced regardless. It’s as close as you can get to the real thing.” Negative feedback: “On pediatrics, when we would chart check patients and then present them in the afternoon to attendings, I feel like the idea was right, with having us read about real patients, but the actual presenting wasn’t helpful because we could essentially just read off yesterday’s progress note written by a resident, so we weren’t doing any thinking.” “I thought that following patients virtually was a great experience because we were given time to research the patients and their conditions making us better prepared for the team conversations about them and giving us the opportunity to learn more.” |
References
- Wyles, S.P.; Meyer, F.B.; Hayden, R.; Scarisbrick, I.; Terzic, A. Digital regenerative medicine and surgery pedagogy for virtual learning in the time of COVID-19. Regen. Med. 2020, 15, 1937–1941. [Google Scholar] [CrossRef]
- Wang, X.; Gui, J. Cell-mediated immunity to SARS-CoV-2. Pediatr. Investig. 2020, 4, 281–291. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Director-General’s Opening Remarks at The Media Briefing on COVID-19. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 19 December 2020).
- Doarn, C.R. Development of telemedicine and NASA’s contribution. Aerosp. Med. Hum. Perform. 2015, 86, 504–505. [Google Scholar] [CrossRef]
- Doarn, C.r.; Nicogossian, A.E.; Merrell, R.C. Applications of telemedicine in the United States space program. Telemed. J. 1998, 4, 19–30. [Google Scholar] [CrossRef]
- Teoli, D.; Aeddula, N.R. Telemedicine. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020; Available online: https://pubmed-ncbi-nlm-nih-gov.gate.lib.buffalo.edu/30570964/ (accessed on 19 December 2020).
- American Telemedicine Association (ATA). Telehealth Defining 21st Century Care. 2020. Available online: https://www.americantelemed.org/resource/why-telemedicine/ (accessed on 3 January 2021).
- World Health Organization (WHO). Telehealth. Analysis of Third Global Survey on eHealth Based on the Reported Data by Countries. 2016. Available online: https://www.who.int/gho/goe/telehealth/en/ (accessed on 3 January 2021).
- ATA. What Is Telemedicine, Exactly? TELEMEDICINE Defined. Available online: https://www.americantelemed.org/ata-news/what-is-telemedicine-exactly/ (accessed on 3 January 2021).
- Bashshur, R.L. On the definition and evaluation of telemedicine. Telemed. J. 1995, 1, 19–30. [Google Scholar] [CrossRef]
- United States Department of Health and Human Services (HHS). What Is Telehealth? 18 November 2020. Available online: https://telehealth.hhs.gov/patients/understanding-telehealth/#what-is-telehealth (accessed on 3 January 2021).
- Richmond, T.; Peterson, C.; Cason, J.; Billings, M.; Terrell, E.A.; Lee, A.D.W.; Towey, M.; Parmanto, B.; Saptono, A.; Cohn, E.R.; et al. American telemedicine association’s principles for delivering telerehabilitation services. Int. J. Telerehabilitation 2017, 20, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Jumreornvong, O.; Yang, E.; Race, J.; Appel, J. Telemedicine and medical education in the age of COVID-19. Acad. Med. 2020, 95, 1838–1843. [Google Scholar] [CrossRef] [PubMed]
- Aron, J.A.; Bulteel, A.J.B.; Clayman, K.A.; Cornett, J.A.; Filtz, K.; Heneghan, L.; Hubbell, K.T.; Huff, R.; Richter, A.J.; Yu, K.; et al. A role for telemedicine in medical education during the COVID-19 pandemic. Acad. Med. 2020, 95, e4–e5. [Google Scholar] [CrossRef] [PubMed]
- Menon, A.; Klein, E.J.; Kollars, K.; Kleinhenz, A.L.K. Medical students are not essential workers: Examining institutional responsibility furing the COVID-19 pandemic. Acad. Med. 2020, 95, 1149–1151. [Google Scholar] [CrossRef] [PubMed]
- Iancu, A.M.; Kemp, M.T.; Alam, H.B. Unmuting medical students’ education: Utilizing telemedicine during the COVID-19 pandemic and beyond. J. Med. Internet Res. 2020, 22, e19667. [Google Scholar] [CrossRef]
- Rolak, S.; Keefe, A.M.; Davidson, E.L.; Aryal, P.; Parajuli, S. Impacts and challenges of United States medical students during the COVID-19 pandemic. World J. Clin. Cases 2020, 8, 3136–3141. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Bhasker, S. Addressing the Covid-19 burden on medical education and training: The role of telemedicine and tele-education during and beyond the pandemic. Front. Public Health 2020, 8, 589669. [Google Scholar] [CrossRef] [PubMed]
- Said, J.T.; Schwartz, A.W. Remote medical educaiton: Adapting Kern’s curriculum design to tele-teaching. Med. Sci. Educ. 2021, 1–8. [Google Scholar] [CrossRef]
- Regmi, K.; Jones, L. A systematic rview of the factors – enablers and barriers – affecting e-learning in health sciences education. BMC Med. Educ. 2020, 20, 91. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.-J.; Kang, Y.; Kim, G. The gap between medical faculty’s perception and use of e-learning resources. Med. Educ Online 2017, 22, 1338504. [Google Scholar] [CrossRef]
- Childs, S.; Blenkinsopp, E.; Hall, A.; Walton, G. Effective e-learning for health professionals and students-barriers and their solutions. A systematic review of the literature-findings from the HEXL project. Health Inf. Libr. J. 2005, 22, 20–32. [Google Scholar] [CrossRef]
- Venkatesh, S.; Rao, Y.K.; Nagaraja, H.; Woolley, T.; Alele, F.O.; Malau-Aduli, B.S. Factors influencing medical students’ experiences and satisfaction with blended integrated E-learning. Med. Princ. Pr. 2020, 29, 396–402. [Google Scholar] [CrossRef]
- Guze, P.A. Using technology to meet the challenges of medical education. Trans. Am. Clin. Climatol. Assoc. 2015, 126, 260–270. [Google Scholar]
- Connolly, S.L.; Stolzmann, K.L.; Heyworth, L.; Weaver, K.R.; Bauer, M.S.; Miller, S.J. Rapid increase in telemental health within the Department of Beterans Affairs during the COVID-19 pandemic. Telemed. e-Health 2020. [Google Scholar] [CrossRef]
- Choi, B.; Jegatheeswaran, L.; Minocha, A.; Alhilani, M.; Nakhoul, M.; Mutengesa, E. The impact of the COVID-19 pandemic on final year medical students in the United Kingdom: A national survey. BMC Med. Educ. 2020, 20, 206. [Google Scholar] [CrossRef]
- Aquifer (n.d.). About Advancing Clinical Teaching & Learning. Available online: https://aquifer.org/about-aquifer/ (accessed on 28 February 2021).
- Babchuk, W.A. Fundamentals of qualitative analysis in family medicine. Fam. Med. Community Health 2019, 7, e000040. [Google Scholar] [CrossRef] [Green Version]
- Harrison, A.G.; Lin, T.; Wang, P. Mechanisms of SARS-CoV-2 transmission and pathogenesis. Trends Immunol. 2020, 41, 1100–1115. [Google Scholar] [CrossRef] [PubMed]
- Rose, S. Medical student education in the time of COVID-19. JAMA. 2020, 323, 2131–2132. [Google Scholar] [CrossRef]
- Masic, I. E-learning as a new method of medical education. Acta Inform. Medica 2008, 16, 102–117. [Google Scholar] [CrossRef] [Green Version]
- Martin, C. On 4-th-Year Medical Student Education during the COVID-19 Pandemic; Interviewed by Gillian Franklin: Buffalo, NY, USA, 2021. [Google Scholar]
- Ashrafzadeh, S.; Imadojemu, S.E.; Vieugels, R.A.; Buzney, E.A. Strategies for effective medical student education in dermatology during the COVID-19 pandemic. J. Am. Acad. Dermatol. 2021, 84, e33–e34. [Google Scholar] [CrossRef] [PubMed]
- Shahrvini, B.; Baxter, S.L.; Coffey, C.S.; MacDonald, B.V.; Lander, L. Pre-clinical remote undergraduate medical education during the COVID-19 pandemic: A survey study. BMC Med. Educ. 2021, 21, 13. [Google Scholar] [CrossRef]
- Drexler, R.; Hambrecht, J.M.; Oldhafer, K.J. Involvement of medical students during the coronavirus disease 2019 pandemic: A cross-sectional survey study. Cureus 2020, 12, e10147. [Google Scholar] [CrossRef] [PubMed]
- Fincham, J.E. Response rates and responsiveness for surveys, standards and the journal. Am. J. Pharm. Educ. 2008, 72, 43. [Google Scholar] [CrossRef] [Green Version]
- Baruch, Y.; Holtom, B.C. Survey response rate levels and trends in organizational research. Human Relations. Hum. Relat. 2008, 61, 1139–1160. [Google Scholar] [CrossRef] [Green Version]
- Saleh, A.; Bista, K. Examining factors impacting online survey response rates in educational research: Perceptions of graduate students. Online Submiss. 2017, 13, 63–74. [Google Scholar]
- Royal, K.D.; Flammer, K. Survey incentives in medical education: What do students say will entice them to participate in surveys? Med. Sci. Edu. 2017, 27, 339–344. [Google Scholar] [CrossRef]
- Kassam-Adams, N.; Marsac, M.L.; Kohser, K.L.; Kenardy, J.A.; March, S.; Winston, F.K. A new method for assessing content validity in model-based creation and iteration of eHealth interventions. J. Med. Internet Res. 2015, 17, e95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussein, R.; Everett, B.; Ramjan, L.M.; Hu, W.; Salamonson, Y. New graduate nurses’ experiences in a clinical specialty: A follow up study of newcomer perceptions of transitional support. BMC Nurs. 2017, 16, 42. [Google Scholar] [CrossRef] [Green Version]

| Specialty | Response n (%) N = 63 |
|---|---|
| Surgery | 6 (9.5) |
| Internal Medicine | 13 (20.6) |
| Pediatrics | 4 (6.3) |
| Obstetrics and Gynecology | 1 (1.2) |
| Psychiatry | 2 (3.2) |
| Family Medicine | 2 (3.2) |
| Other (EM, Anesthesia, etc.) | 8 (12.7) |
| Sub-internship | 21 (33) |
| Telemedicine Patient Care Involvement | Used Aquifer Simulated Cases as Primary Clinical Experience | |
|---|---|---|
| Specialty | Response n/Total (%) | Response n/Total (%) |
| Surgery | 1/25 (4.0%) | 22/23 (95.7%) |
| Internal Medicine | 10/34 (29.4%) | 32/35 (91.4%) |
| Pediatrics | 8/51 (15.7%) | 24/27 (88.9%) |
| Obstetrics and Gynecology | 1/26 (3.9%) | 21/24 (87.5%) |
| Psychiatry | 1/21(4.8%) | 16/21 (76.2%) |
| Family Medicine | 8/25 (32.0%) | 18/24 (75.0%) |
| Sub-internship | 5/25 (20.0%) | 1/15 (6.67%) |
| Questionnaire Item: Education Received during COVID Impacted Clerkships Adequately Prepared You for the Following? N = 63 | Response n (%) | |
|---|---|---|
| Yes | No | |
| Self examinations | 48 (76.2%) | 15 (23.8%) |
| USMLE Step 2 CK examination | 48 (76.2%) | 15 (23.8%) |
| Internship year | 23 (36.5%) | 40 (63.5%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franklin, G.; Martin, C.; Ruszaj, M.; Matin, M.; Kataria, A.; Hu, J.; Brickman, A.; Elkin, P.L. How the COVID-19 Pandemic Impacted Medical Education during the Last Year of Medical School: A Class Survey. Life 2021, 11, 294. https://doi.org/10.3390/life11040294
Franklin G, Martin C, Ruszaj M, Matin M, Kataria A, Hu J, Brickman A, Elkin PL. How the COVID-19 Pandemic Impacted Medical Education during the Last Year of Medical School: A Class Survey. Life. 2021; 11(4):294. https://doi.org/10.3390/life11040294
Chicago/Turabian StyleFranklin, Gillian, Clare Martin, Marc Ruszaj, Maliyat Matin, Akaash Kataria, Jinwei Hu, Arlen Brickman, and Peter L. Elkin. 2021. "How the COVID-19 Pandemic Impacted Medical Education during the Last Year of Medical School: A Class Survey" Life 11, no. 4: 294. https://doi.org/10.3390/life11040294