
Biomaterials for Periodontal and Peri-Implant Regeneration
by
 , , , and
, , , and
Leonardo Mancini
1,* ,
,
Mario Romandini
2 ,
,
Adriano Fratini
1,
Lorenzo Maria Americo
1, 
Saurav Panda
3,4 and
Enrico Marchetti
1 1
Department of Life, Health and Environmental Sciences, University of L’Aquila, 67100 L’Aquila, Italy
2
ETEP Research Group (Etiology and Therapy of Periodontal and Peri-implant Diseases), University Complutense, 28040 Madrid, Spain
3
Department of Periodontics and Oral Implantology, Institute of Dental Sciences, Siksha O Anusandhan (Deemed to Be) University, Bhubaneswar 759146, Odisha, India
4
Department of Biomedical, Surgical and Dental Sciences, University of Milan, 20122 Milan, Italy
*
Author to whom correspondence should be addressed.
Materials 2021, 14(12), 3319; https://doi.org/10.3390/ma14123319
Submission received: 20 May 2021
/
Revised: 3 June 2021
/
Accepted: 9 June 2021
/
Published: 15 June 2021
(This article belongs to the Special Issue Biomaterials in Periodontology and Implantology)
Abstract
:Periodontal and peri-implant regeneration is the technique that aims to restore the damaged tissue around teeth and implants. They are surrounded by a different apparatus, and according to it, the regenerative procedure can differ for both sites. During the last century, several biomaterials and biological mediators were proposed to achieve a complete restoration of the damaged tissues with less invasiveness and a tailored approach. Based on relevant systematic reviews and articles searched on PubMed, Scopus, and Cochrane databases, data regarding different biomaterials were extracted and summarized. Bone grafts of different origin, membranes for guided tissue regeneration, growth factors, and stem cells are currently the foundation of the routinary clinical practice. Moreover, a tailored approach, according to the patient and specific to the involved tooth or implant, is mandatory to achieve a better result and a reduction in patient morbidity and discomfort. The aim of this review is to summarize clinical findings and future developments regarding grafts, membranes, molecules, and emerging therapies. In conclusion, tissue engineering is constantly evolving; moreover, a tailor-made approach for each patient is essential to obtain a reliable result and the combination of several biomaterials is the elective choice in several conditions.
1. Introduction
The improved quality and expectancy of life of the current population leads to an increase in injuries and bone disease in older people who have a diminished capacity to restore and regenerate the damaged tissues [1]. Oral and craniofacial tissue injuries are still a very challenging situation for dentists and oral surgeons. To facilitate dentists in their clinical practice, tissue engineering is in constant evolution, and each year several biomaterials are proposed to achieve better results in periodontal and peri-implant regeneration [2]. The principal target of periodontal and peri-implant tissue engineering is to regenerate the supporting tissue of the teeth or implants. Tooth loss, bone, and soft tissue remodeling are consequences of an inflammatory process or age-related decay [3,4]. Periodontitis has been estimated in about 27% of the global population, and to restore missing tooth implants, therapy is a primary alternative to mobile prosthesis [5,6,7]. This condition leads the clinician to evaluate the predisposition of bone and supporting tissue around the missing tooth site. In several conditions, this required a regenerative approach before or during the implant insertion [8,9]. Peri-implantitis has been estimated in 20% of the population and is defined as an inflammatory process that occurs around implants with soft tissue inflammation and supporting bone loss [10].
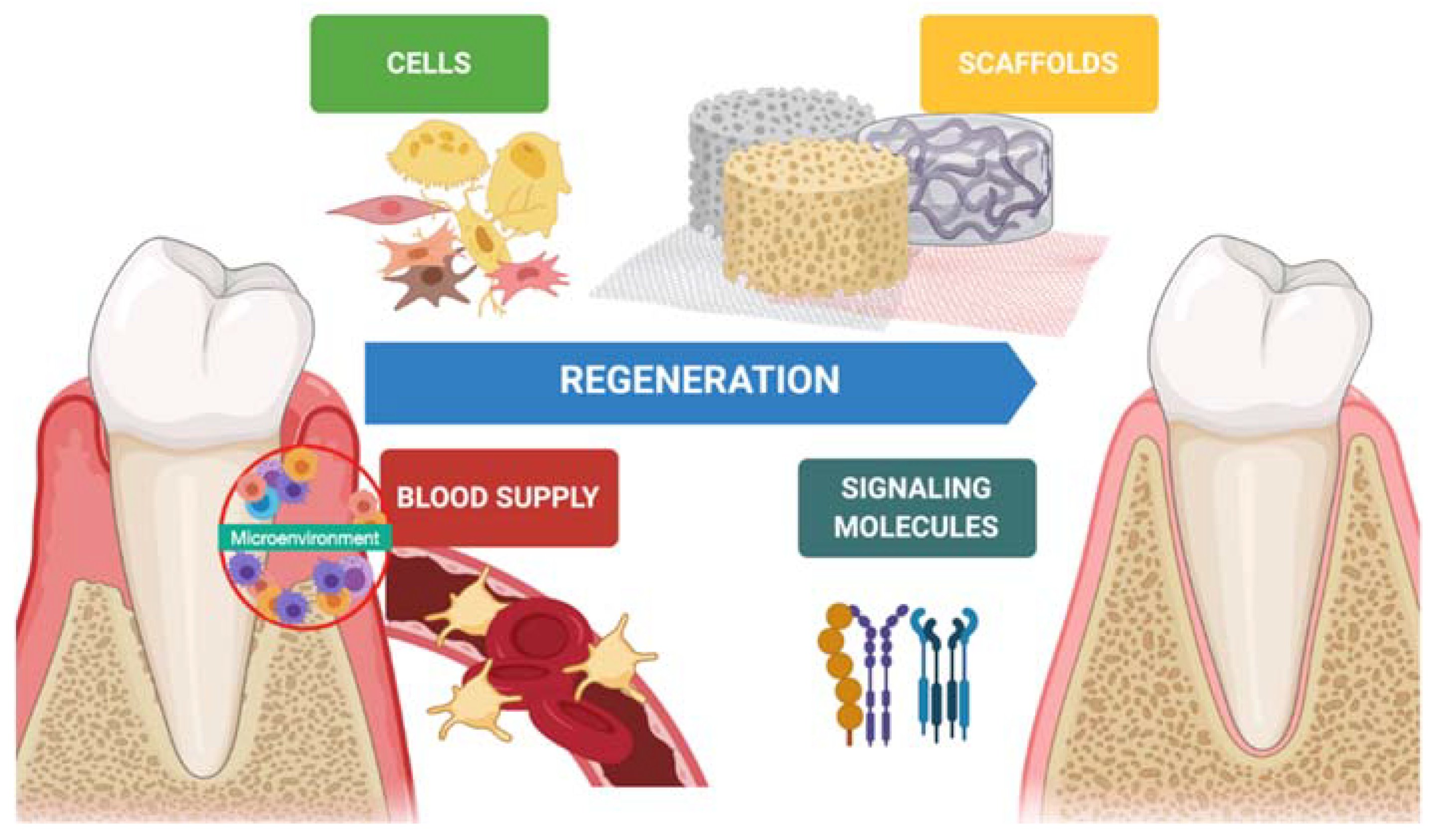
In the last decades, hard tissue regeneration has reached good outcomes regarding newly formed bone, mineralization, and osteoinduction [11]. On the other hand, soft tissue regeneration has also gained interest in preventing advanced forms of periodontitis, peri-implantitis, and mucogingival disorders [12]. Indeed, keratinized tissue, tissue thickness, and supracrestal tissue height around teeth and implants is desirable to achieve better esthetic outcomes and guarantee long-term stability [13,14]. Periodontal regeneration is one of several disciplines that has benefitted from tissue engineering. Biomaterials (scaffolds), molecules (growth factors), and stem cells are keys in the regenerative process, and a synergy between them improves the quality and predictability of the technique (Figure 1).
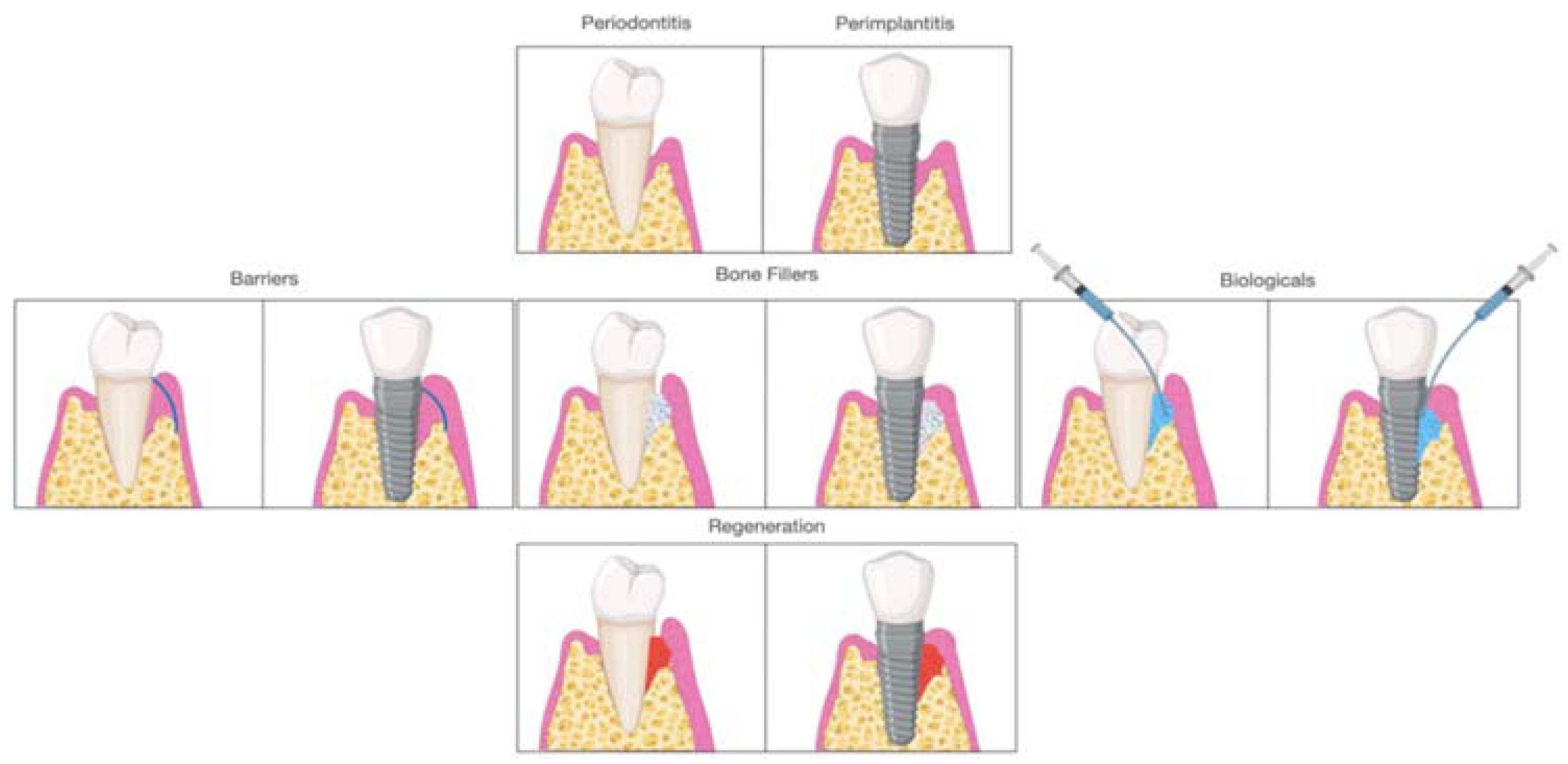
Early on, periodontal regeneration used the concept of guided tissue regeneration (GTR), selecting cell populations to colonize the periodontal wound following surgical exposure [15]. The use of bone substitutes in conjunction with barriers aims to prevent epithelial migration. This allows the periodontal ligament cells (PDL) to populate the protected site, providing positive effects in particular cases [16,17]. Decades of research have expanded from this concept, and different biomaterials are available to clinicians and researchers for alveolar bone regeneration. According to the mechanism of action, biomaterials are classified as barriers, bone fillers, and biologicals. In several situations, such as GTR, treatment components are not used alone but always in combination. Barriers are materials that cover the periodontal defect, protecting them from epithelial downgrowth. Bone fillers are scaffolds or bone grafts that replace the missing portion of the alveolar bone [18]. Biologics are growth factors, cell therapy, or substances that can be directly administrated in the defect (Figure 2).
Efforts have been made over recent years to stimulate bone and soft tissue regeneration around teeth as well as edentulous areas and around implants affected by peri-implantitis [19,20,21]. This review aimed to highlight new frontiers regarding periodontal and peri-implant regeneration with a perspective on the application of biomaterials and emerging therapies.
2. Materials
Grafting materials are commonly used in periodontal tissue engineering to restore the alveolar bone proper, providing adequate regeneration and tooth stability over the years, or the soft and hard tissues around teeth and implants for clinical and esthetic reasons [22]. They include biological and synthetic materials in various shapes and forms, such as granules, particles, gel, 3D scaffolds, injectable substances, polymers, and matrices. According to the type of regeneration and technique, these materials are used alone or in combinations to improve and accentuate the regenerative process. The followed biomaterials were classified and selected according to the scientific evidence extracted from systematic reviews and articles searched on PubMed, Scopus, and Cochrane databases with the following keywords: “Periodontal regeneration” AND/OR “Biomaterials” OR “Peri-implant regeneration” AND “Bone grafts” AND/OR “Biologics” OR “Stem cells”.
2.1. Bone Fillers
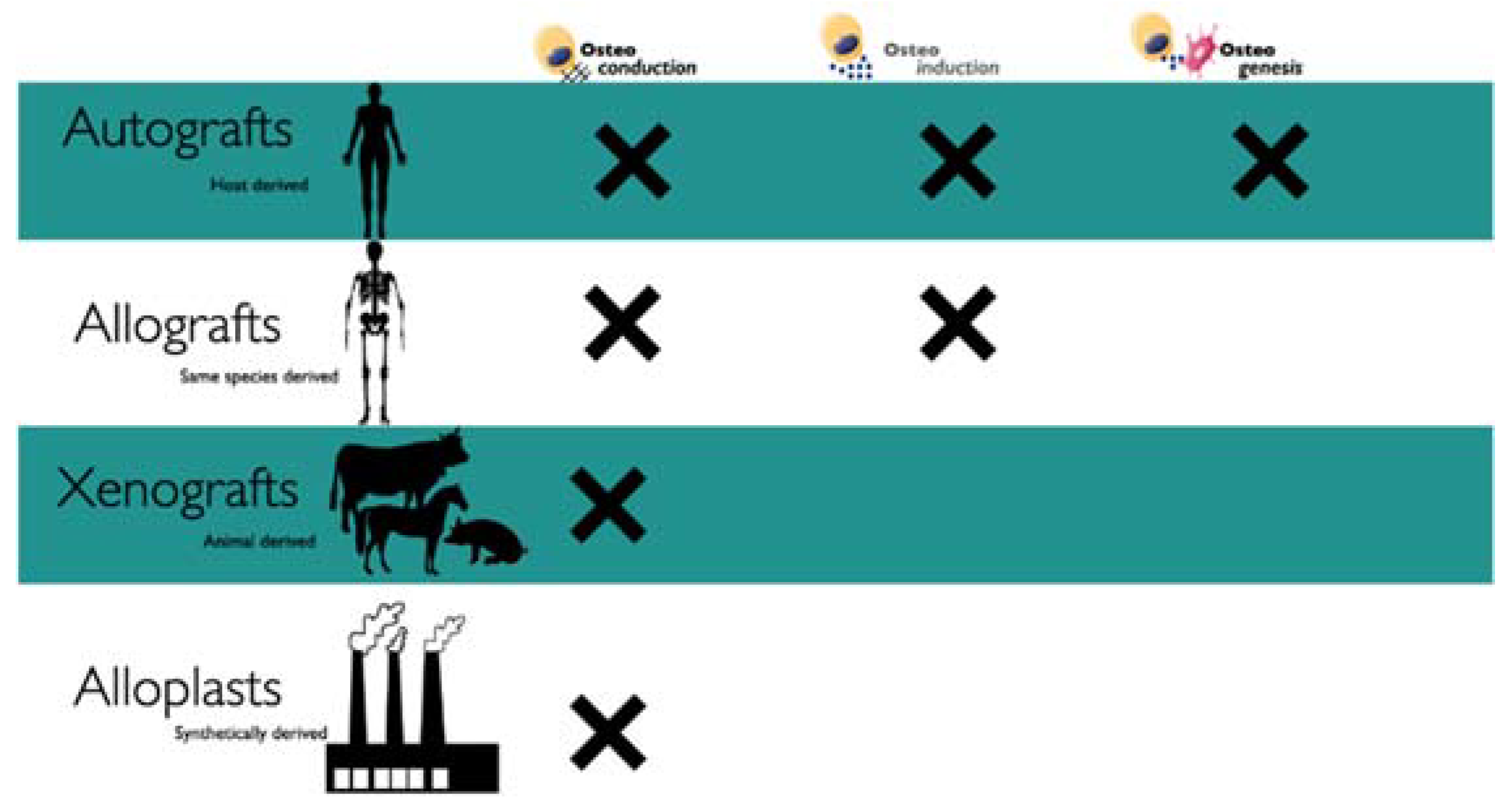
Bone fillers are used in ridge preservation or augmentation and to restore the missing volume of periodontal defects; the presence of teeth or implants next to the defect is important for the regenerative potential. These types of graft are classified according to their origin (Figure 3).
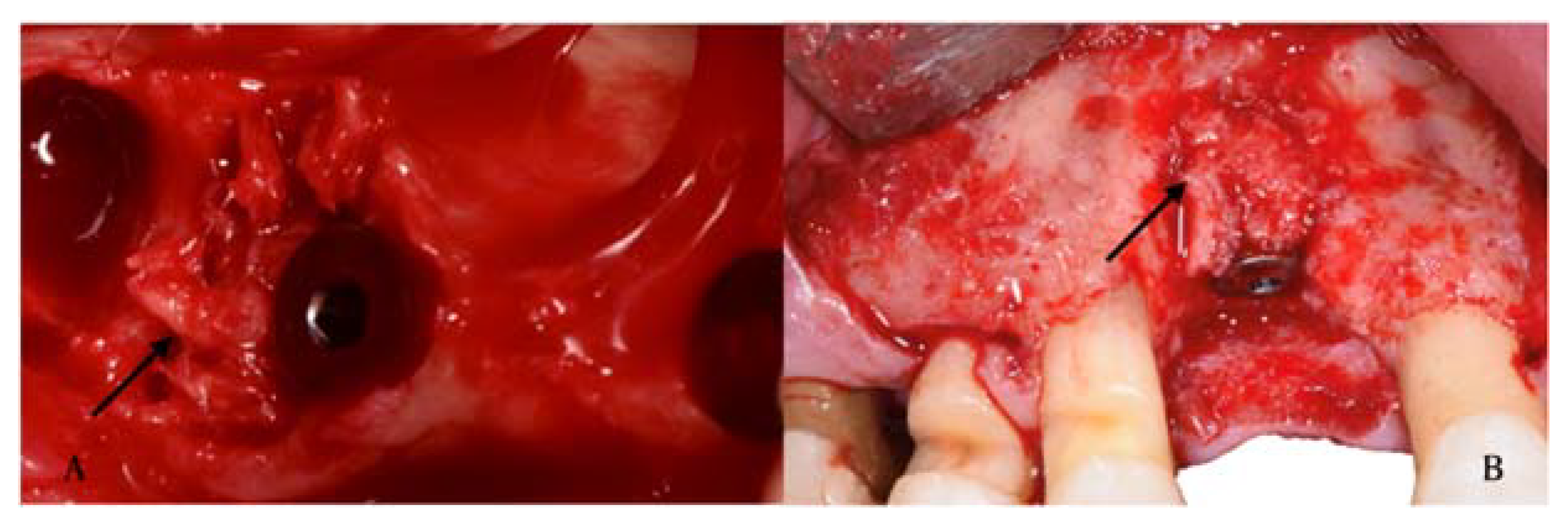
- Autografts are the gold standard due to the osteogenic, osteoconductive, and osteoinductive potential and the absence of foreign body reactions (FBR) [23]. Depending on the size of the defect, the autograft is usually harvested intraorally from the extraction socket, edentulous ridge, symphysis, tuberosity, or buccal plate (Figure 4).
In the presence of large defects, the harvesting process is obtained from extraoral sites, such as the tibia, skull, or iliac crest [24]. These types of interventions require a second site surgery, which increases stress and discomfort for the patient. In using autografts, there are advantages, such as osteogenic potential and reduced risk of disease transmission, but at the same time, the second site surgery includes risk of possible complications, postoperative pain, and limited availability make this approach less attractive for large sites. In the history of periodontal regeneration, the use of autografts was suggested firstly by Nabers and O’Leary in 1965; they proposed the use of cortical bone chips removed manually from within the surgical site [25]. Cushing, in 1969, suggested the use of grafts from the iliac crest for the induction of new bone in the periodontium [26,27]. According to this study, a complete regeneration and furcation coverage was achieved, but nowadays, due to the minimally invasive approach, the presence of several biomaterials is not widespread [28]. In the implant field, autogenous bone is a gold standard. Indeed, the implant survival rate for implants surrendered by autografts, reported in the literature, is between 70–100% [29,30]. The worst records were for the iliac crest with high resorption and implant failure [31]. Data are controversial for some studies that reported similar results between intra and extraoral grafts [32,33].
- Allografts are biological materials harvested from the same species. The advantage of allografts is the elimination of a second surgical site and tissue availability. Tissue banks are involved in the extraction process from which tissue is extracted, and depending on the treatment, it is possible to obtain freeze-dried bone (FDBAs) or decalcified freeze-dried bone (DFDBAs). The disadvantage in using these types of biomaterials is the possible FBR and disease transmission; although, in the last years, severe and rigid procedures have been developed to reduce the risk [34,35]. Nevertheless, researchers and clinicians identified allografts as reliable sources for the regenerative procedure since they can serve as osteoconductive or osteoinductive biomaterials preserved of proteins in their matrix [36]. The allograft’s decalcification leads to an exposure of bone morphogenic proteins (BMPs) that are effective molecules in bone regeneration [36]. In the case of allograft, the exposure of BMPs showed an increase in bone resorption during the follow-up period. Nevertheless, a disadvantage in using allografts is the high cost compared to xenografts and autografts [37]. Moreover, it is not available in several counties for ethical and legal reasons.
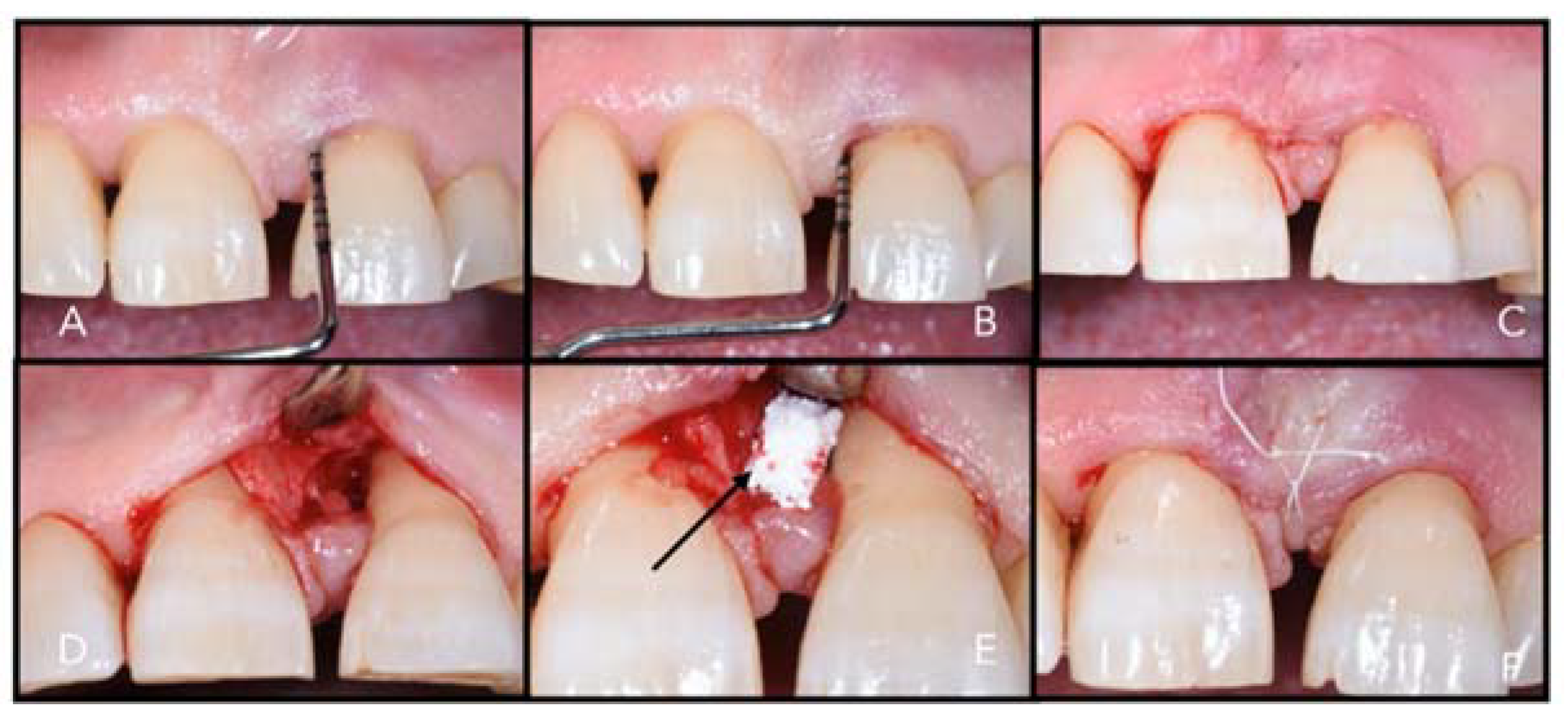
- Xenografts are bone substitutes obtained from other species, such as bovine or porcine grafts, and transplanted into humans. The main disadvantage of xenografts is the antigenicity; indeed, these tissues need to be carefully treated to remove the organic components [18]. Several commercial products have been proposed based on this protocol (Table 1), such as Geistlich Bio-Oss® particles (Geistlich Pharma, Wolhusen, Switzerland), which are harvested bovine and is considered a global reference product in oral regeneration (Figure 5). Despite positive results from several studies, the disadvantage is in the unpredictable grade of regeneration and resorption. The advantages are a single surgical procedure, availability, and reduced patient morbidity. According to Stavropoulos et al. (2005, 2010), the use of deproteinized bovine bone (DBB) in adjunct to GTR renders the defect more stable on a long-term follow-up [38,39,40].
2.2. Barriers
After the exposure and debridement of a periodontal defect, several types of cells can recolonize the lesion, such as epithelial cells, which have a fast turnover, fibroblasts cells, or bone and PDL cells [51]. Barriers are used to limit and select cells allowing the regeneration of a specific tissue, such as bone or PDL, reducing the downgrowth of epithelial cells in the defect and not allowing the formation of a long junctional epithelium [52]. Moreover, barriers are used to maintain the space of the defect, facilitating cell replication and tissue regeneration [52]. Traditionally, barriers are divided into resorbable and non-resorbable (needing a second phase for removal). Otherwise, it is possible to classify these matrixes according to their origin, including autogenous, xenogeneic, allogenic, and alloplastic. The efficacy of several membranes was discussed in two articles from Kao et al. (2015) and Sculean et al. (2015) in which positive and negative effects were analyzed [53,54]. The most used in periodontal regeneration are xenogeneic membranes (bovine or porcine origin) enriched with collagen and characterized by a cross or no cross-linked process that can reduce or improve the resorption time. According to Garcia et al. (2017), no differences were achieved regarding guided bone regeneration (GBR) in using cross or no cross-linked matrices; however, regarding tissue integration and postoperative complications, the cross-linked membranes seem to be less predictable [55]. The first type of membrane used in 1980 was based on cellulose acetate, and since then, different types of materials have been developed and studied [52].
2.2.1. Resorbable Barriers
The demand for resorbable barriers during the last decade increased due to a reduction in the numbers of surgeries and biomaterial resorption. The main positive factors that need to be considered are a reduction in patient discomfort, bioactive properties, and the ease of handling [56]. Unfavorable factors are the unpredictable resorption pattern related to the degradation process (hydrolytic or enzymatic) and the possible presence of inflammation related to the degradation process [57]. The raw material may be natural or synthetic, and natural is more biocompatible but with an unpredictable resorption pattern. On the other hand, synthetics have a predictable degradability and a mechanical resistance that is customized according to the production process [58]. The most used and widespread is the collagen harvested, as said before, from animals. Type I collagen is responsible for the attraction and activation of PDL cells and fibroblasts. Thus, it is one of the most used for membrane production (Table 2) [59].
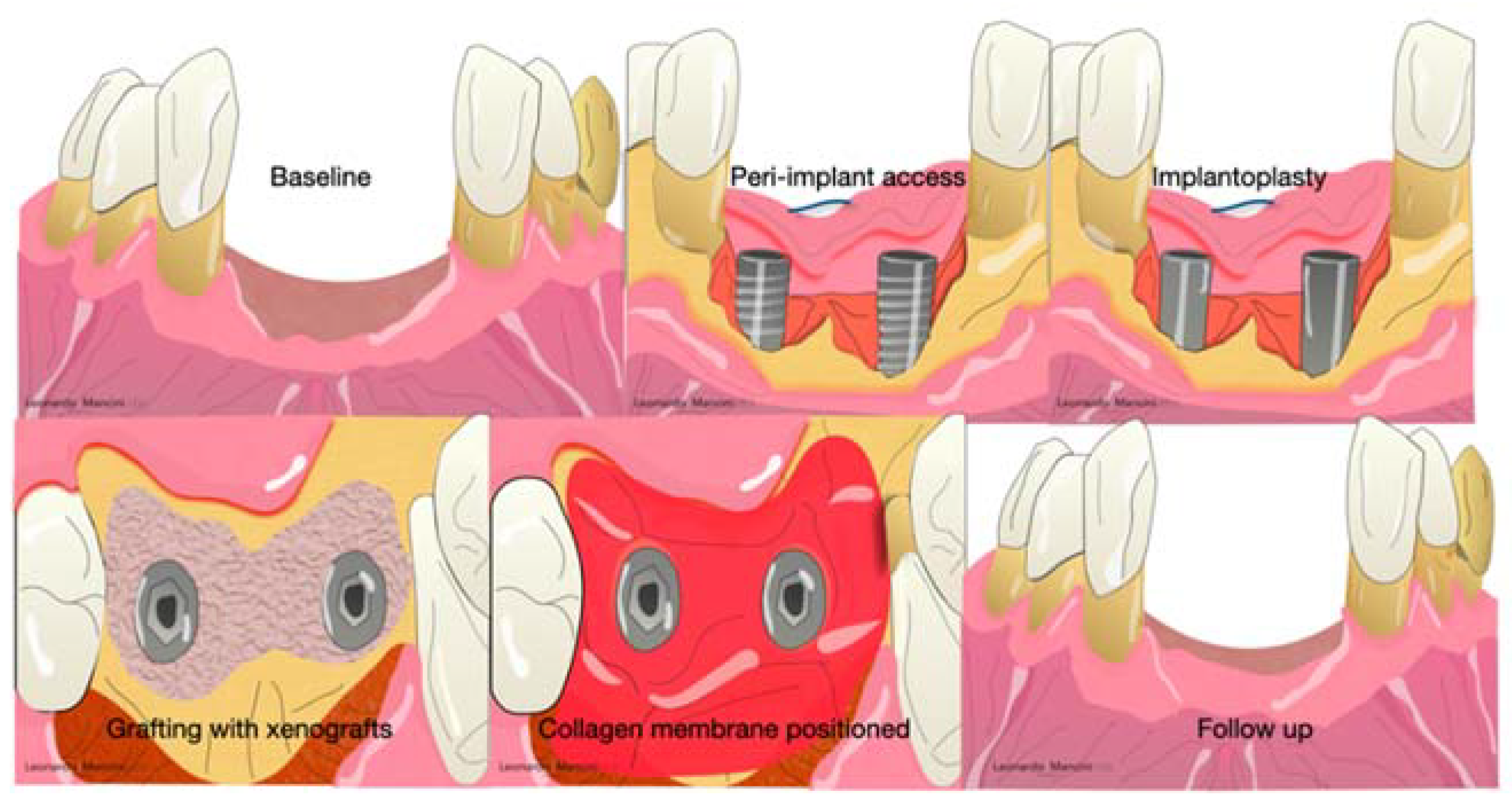
Collagen membranes are used not only in periodontal regeneration but also in peri-implant regeneration and, in several cases, regenerative procedures associated with an implantoplasty or heavy decontamination of the implant surfaces (Figure 6).
2.2.2. Non-Resorbable Barriers
The main advantages of non-resorbable membranes are the high mechanical stability and the cell’s migration inhibition [56]. However, there are some criticisms, such as the second surgical intervention possible exposure, and accentuated inflammation in case of infection [56]. The most widespread and used during the last decade were polytetrafluoroethylene (ePTFE) and titanium-reinforced membranes [60]. PTFE was developed by Gore-Tex (W. L. Gore & Associates, Inc., Newark, Denmark) in 1990. The particularities were the presence of a double layer with different functions; the first layer is porous, and the aim is to promote cell ingrowth. The other side acts as a space provider to inhibit epithelial cell downgrowth. Several randomized clinical trials showed interesting results after three months of healing in periodontal regeneration [61,62,63,64,65,66]. Others reported several complications (exposure, suppuration, pain) probably related to the flap handling and suture collapsing [65]. Nowadays, these barriers are not used due to the introduction of minimally invasive approaches (minimally invasive surgical technique, single flap approach, or modified minimally invasive approach) that can achieve periodontal regeneration without the selection of cells but with the use of growth factors inside the defect associated with a minimal flaps design that maintains the space in favor of blood clot stability [66,67,68,69,70]. Moreover, with these techniques, the handling of a membrane is not easy to obtain.
2.3. Biologics
Biological mediators are considered the last innovation in oral regeneration. It is possible to classify these mediators in stem cells, growth factors, and gene therapy. The most used and widespread are platelet-rich growth factors (PDGF), bone morphogenetic proteins (BMP), and enamel matrix derivatives (EMD).
- PDGF is primarily involved in wound healing; several studies showed its function and ability to enhance the proliferation and migration of PDL cells [71,72]. Moreover, the chemotactic effect leads to a promotion of collagen synthesis and can stimulate gingival fibroblasts to the hyaluronate synthesis [73,74,75,76]. This growth factor might be effective alone or in combination with other growth factors, such as the insulin-like growth factor-1 (IGF-1). Indeed, several in vivo studies showed the efficacy of PDGF in periodontal regeneration alone or combined, and it always demonstrated the new formation of cementum and the production of collagen [77,78,79]. Thanks to molecular cloning, it is now possible to reproduce a recombinant human PDGF [77]. Nevertheless, this type of recombinant product is not sold in several nations, such as Italy, for ethical problems. The most used and analyzed product is GEM 21S®, (Osteohealth, Shirley, NY, USA) with in vivo and in vitro studies [80].
- BMPs are factors that belong to the superfamily of transforming growth factor-beta (TGF-ß), are abundant in bone tissue, and are produced by several cells including osteoclasts and osteoblasts. Two types (BMP-4 and BMP-7) are commonly enclosed in allografts, demonstrating osteoinductivity and influencing cells’ behavior in bone regeneration [81,82,83]. Moreover, BMPs act as a chemoattractant for osteoblast precursors and undifferentiated stem cells (MSCs) through the activation of genes related to bone formation, such as osteocalcin [84,85]. A disadvantage in the extraction of BMPs is the synthetic production, which is very expensive, and there is a limitation for the encapsulation in synthetic biomaterials [85].
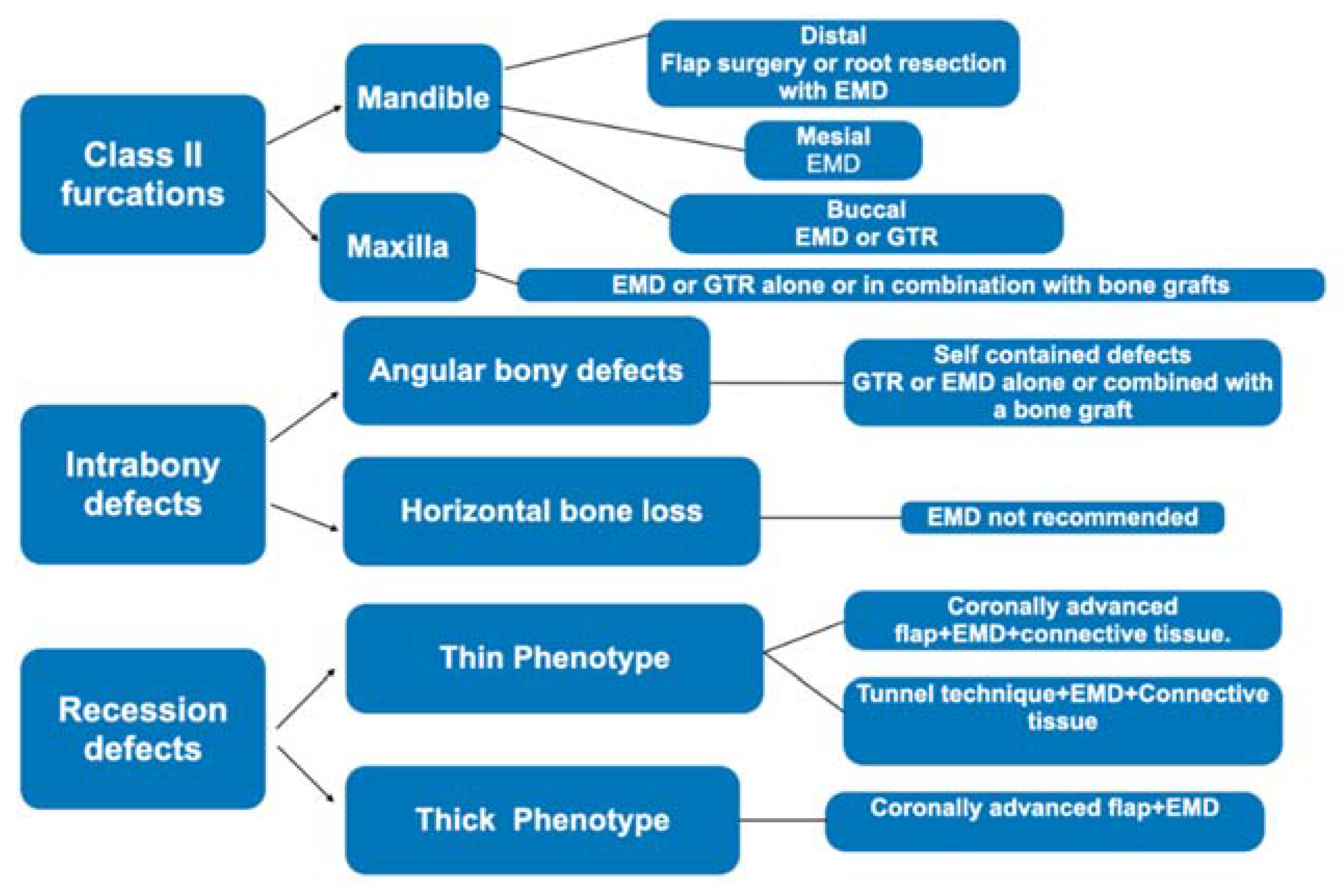
- EMD is released by Hertwig’s cells during the formation of teeth and periodontal tissue, and these proteins are situated on the root surface, influencing the initial steps of cementum, alveolar bone, and periodontal ligament formation [86,87]. In origin (1996), a Swedish factory (Biora, Malmö, Sweden) released the actual and unique EMD derivatives extracted from porcine enamel in the form of purified acid. Later, Straumann AS acquired the title and Emdogain® (Straumann AG, Basel, Switzerland) is the name of the unique enamel derivates on the market. It is composed mainly of amelogenins, which are specific proteins fundamental in the enamel mineralization process. In physiological conditions, the amelogenins are nano formed, and during the enzymatic degradation by metalloproteinases (MMP), they release bioactive peptides for weeks [88]. In this process, there are advantages, such as the stimulation of new bone and wound healing conditioning. On the other hand, this process might create root resorption due to the presence of MMP and an inflammatory pattern during the regenerative phase [89]. The advantage of using EMD is the mimic action, which can recruit cementoblasts to form new root cementum and consequently facilitate the formation of a new periodontal ligament [89]. This product has been on the market since 1997, and several articles underlined the ease of handling, an interesting result in periodontal regeneration [90,91,92,93,94]. Miron et al. in (2016) collected all the data regarding EMD in periodontal regeneration, and in this study, the use of EMD was relevant in adjunct to non-surgical therapy and regenerative procedures, according to the defect size and shape (Figure 7) [95]. According to the literature, EMD, after 25 years from its introduction, seems to be unique in demonstrating a histological periodontal regeneration with new cementum and periodontal ligament and the presence of Sharpey’s fibers in the periodontal structure [95]. Regarding the use of EMD around implants, data collected from a randomized clinical trial, according to Isehed et al. (2016), revealed that EMD delivered promising but insufficient regeneration associated with an alteration of the Gram-negative flora [96].
- Hyaluronic acid (HA) is a natural glycosaminoglycan contained in several tissues, such as connective tissue. It is an excellent scaffold for periodontal regeneration. Moreover, it seems to have an antimicrobial and anti-inflammatory effect [97,98]. The principal factor that makes this a promising biomaterial is the viscoelastic property and the capacity for absorbing a considerable amount of water. This renders hyaluronic acid a periodontal filler, and, in several situations, it has a protective function as a barrier for bacteria and viruses. Pilloni et al. (2019) suggested the use of HA with a collagen membrane in periodontal defects [99,100]. A systematic review from Eliezer et al. suggested that the addition of HA to non-surgical and surgical periodontal therapy may have additional clinical effects on the clinical attachment level (CAL, 0.73 mm; 95% CI, 0.28 to 1.17 mm; p < 0.0001), periodontal depth (PD, 0.36 mm; 95% CI, −0.54 to −0.19 mm; p < 0.0001), and bleeding on probing (BoP, 5%; 95% CI, −22 to −8%; p < 0.001) [101]. Regarding the use of HA in peri-implant defects, several studies suggest the benefit in microflora diversity, and at the same time, HA acts as a protective shield against bacteria colonization [102,103]. Interesting data from an animal study suggested the inhibition of the downgrowth of connective tissue inside the peri-implant defect, facilitating bone regeneration and implant stability [104].
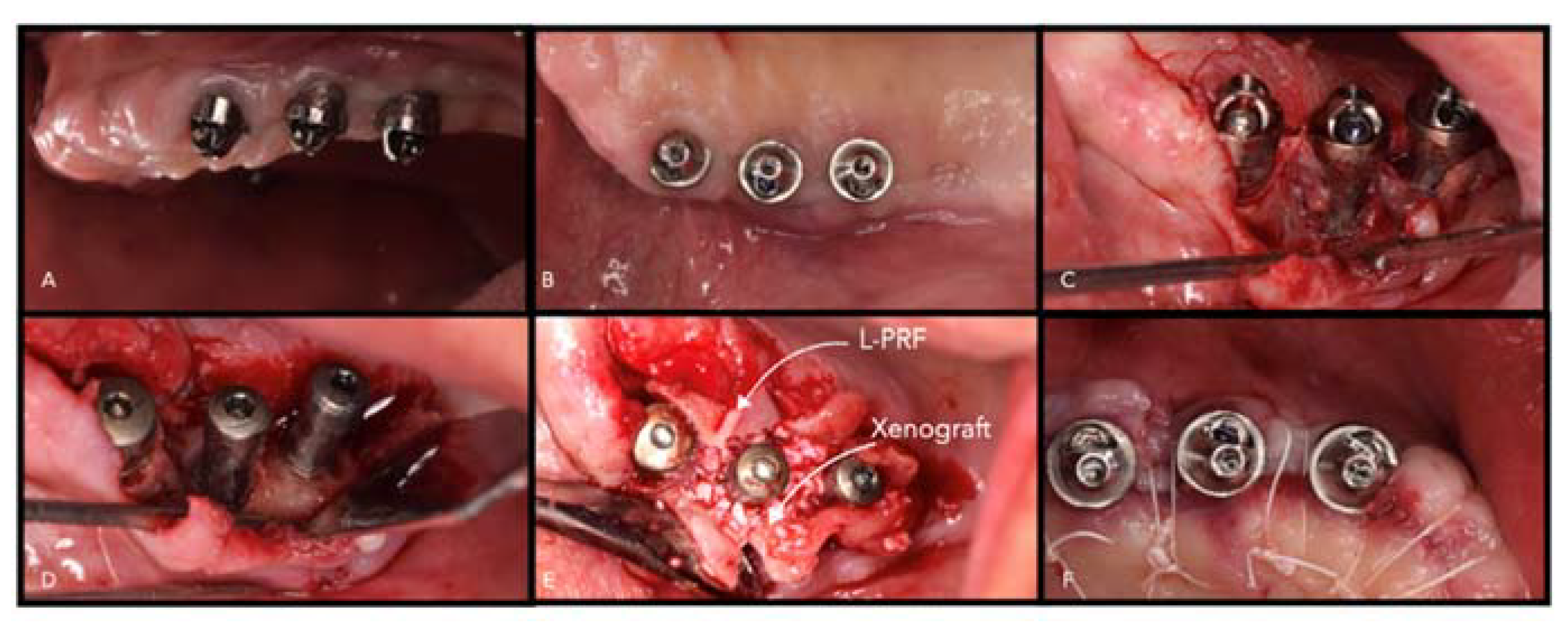
- Autologous platelet concentrates (APG) are promising biomaterials in periodontal and peri-implant regeneration. There are several protocols published (platelet-rich fibrin, PRF/A-PRF/L-PRF; platelet-rich plasma (PRP) platelet-rich growth factors, (PRGF) in the literature, and the main composition is based on platelet fibrin and growth factors, such as PDGF, vascular endothelial growth factors (VEGF), and transforming growth factors beta (TGF- b) [75,76,105]. They are defined as natural living cell scaffolds and according to several systematic reviews are valid biomaterials in periodontal and peri-implant regeneration [106,107,108] (Figure 8). The advantages are autologous origin and the fast and chip protocol. On the other hand, the handling and the production process differs among the types (PRF, A-PRF, PRP, PRGF). Another disadvantage is the fast resorption pattern that was estimated to be among 14 and 20 days [105]. Nevertheless, due to the fibrin scaffold and the presence of growth factors, they are promising biomaterial. Future studies are investigating PRF as a drug delivery system in periodontal defects [109].
3. Emerging Technologies
3.1. Stem Cell Therapies
Stem cells are cells of the human body capable of differentiating into any cell of an organism and are self-renewing. They are defined as unspecialized, and, in their evolution, there are various steps of specialization [110]. Research on cell-based approaches is concentrated on the use of mesenchymal stem cells (MSCs), multipotent stem cells with excellent biological proprieties obtainable from nearly all organs and tissues [111].
Periodontal ligament stem cells (PDL-SCs) are used in periodontal ligaments or cementum regeneration. They can be found in alveolar bone and root surfaces, though the PDL-SCs on the alveolar bone show better differentiation abilities. PDL-SCs can differentiate into mesenchymal cell lineages to generate adipocytes, collagen-forming cells, osteoblast-like cells, cementum tissue, and Sharpey’s fibers in vitro [110].
The discovery of periodontal ligament mesenchymal stem cells (PDL-MSCs) into the PDL proposes the important implication of them in the regeneration of the periodontium and its homeostasis. Although the use of PDL-MSCs on bone formation has provided contrasting results, the effect in increasing cementum and PDL formation seems to give good results. This capacity could be supported by the fact that PDL-MSCs express higher levels of various PDL-specific proteins than other MSCs [112]. From a clinical point of view, the use of stem cells is a promising adjuvant in the regenerative procedure. In any case, the limited availability and the requirement of a specialized laboratory render the use limited. In the last three years, a new concept was developed to facilitate the extraction through a mechanical process using simple handling directly in the dental office. Indeed, according to a previous review, this type of extraction seems to be promising in oral regeneration thanks to the combination with scaffolds as collagen membranes or grafts [111]. Studies on stem cells and innovative scaffolds show a potential improvement in term of periodontal regeneration [113,114]. Regarding the use in peri-implant regeneration, preclinical data showed promising results; nevertheless, further clinical studies are needed to validate their effect in peri-implant defects [115].
3.2. Three-Dimensional Printing
The introduction of 3D printing in the regenerative field enabled new bioresorbable polymers to be printed and customized for individual cases. The processes are several.
- Inkjet model: consists of using inkjet printing with powder and liquid solutions to select and dispose of cells, create an extracellular matrix, and allows the use of a customized scaffold [116]. Park et al. (2012, 2014) published the use of a 3D fiber scaffold for guiding PDL cells and facilitating the mineralization of tissue [117,118]. Goh et al. (2015) analyzed the use of a 3D scaffold in socket preservation with normal bone healing and better-preserved volume [109].
- Fusion model: allows building personalized scaffolds but without the inclusion of cells, growth factors, and proteins [116]. The polymer used is lactic-co-glycolic acid with good characteristics of resorption and mechanical strength.
- 3D plotting allows the production of a soft scaffold composed of hydrogel with easy incorporation of cells. A limitation is the possible inhibition of cell-to-cell communication, influencing the signaling and proliferation process [119,120]. On the other hand, the use of living cells in the scaffold has great results for tissue formation.
4. Summary and Future Directions
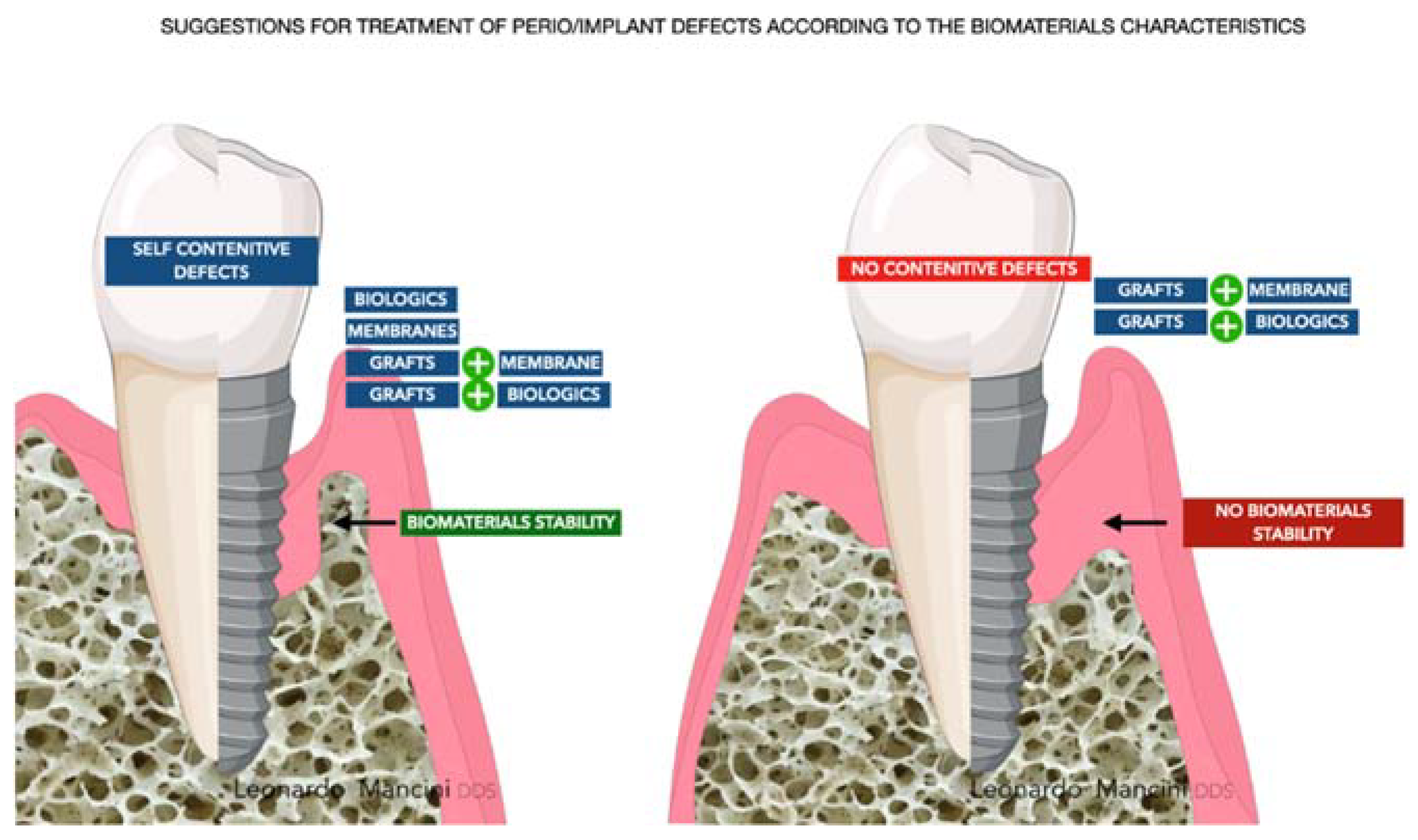
The challenge for each periodontist is to restore all the components of the periodontal compartment (cementum, periodontal ligament, and bone). The regeneration around implants, from the tissue aspect, seems to be easier due to the regeneration of bone only. Nevertheless, it is still a crucial site due to the absence of the anatomical apparatus enriched with vessels, proteins, and growth factors located around teeth. The main elements that need to be considered to have a reliable regeneration are the managing of the occlusal load, mechanical stability of the biomaterial used (grafts better than biologics alone), the reduced FBR due to chemical and thermic treatments that allow the processing of particles, microbiological flora around the defects, dysbiosis control, and, lastly, wound stability. FBR should be discussed carefully due to possible failure related to exposure and infection of the grafts. Exposure is a crucial aspect in daily practice and in many, from an expected regeneration follow-up, has revealed the presence of fibrous encapsulation or graft rejection. The principles, mentioned before, are to be applied for every type of biomaterial and are at the basis of the regenerative process. Moreover, with the introduction of 3D biomaterials and the use of growth factors, signaling is another aspect that needs to be considered to recruit cells and guarantee a proper regenerative response around teeth or implants. However, the main targets are and will be the cost-effective and tailored approaches providing function and esthetics. According to this review for the question “Which is the best biomaterial?”, there is not a specific answer, but the synergetic potential of several biomaterials and the tailored approach lead to a reliable result and predictable regeneration (Figure 9).
Author Contributions
Conceptualization, L.M. and M.R.; methodology, A.F.; software, L.M.; validation, S.P., E.M., and L.M.A.; formal analysis, L.M.; investigation, L.M.; resources, M.R.; data curation, A.F.; writing—original draft preparation, L.M.; writing—review and editing, L.M.A.; visualization, E.M.; supervision, S.P.; project administration, E.M.; funding acquisition, E.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable. No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Yun, M.H. Changes in regenerative capacity through lifespan. Int. J. Mol. Sci. 2015, 16, 25392–25432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallum, E.A.; Ribeiro, F.V.; Ruiz, K.S.; Sallum, A.W. Experimental and clinical studies on regenerative periodontal therapy. Periodontology 2000 2019, 79, 22–55. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction: An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Chappuis, V.; Araújo, M.G.; Buser, D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000 2017, 73, 73–83. [Google Scholar] [CrossRef]
- Frencken, J.E.; Sharma, P.; Stenhouse, L.; Green, D.; Laverty, D.; Dietrich, T. Global epidemiology of dental caries and severe periodontitis—A comprehensive review. J. Clin. Periodontol. 2017, 44, S94–S105. [Google Scholar] [CrossRef]
- Romandini, M.; Gioco, G.; Perfetti, G.; Deli, G.; Staderini, E.; Lafori, A. The association between periodontitis and sleep duration. J. Clin. Periodontol. 2017, 44, 490–501. [Google Scholar] [CrossRef] [PubMed]
- Romandini, M.; Shin, H.S.; Romandini, P.; Laforí, A.; Cordaro, M. Hormone-related events and periodontitis in women. J. Clin. Periodontol. 2020, 47, 429–441. [Google Scholar] [CrossRef]
- Schwarz, F.; Giannobile, W.V.; Jung, R.E.; Groups of the 2nd Osteology Foundation Consensus Meeting. Evidence-based knowledge on the aesthetics and maintenance of peri-implant soft tissues: Osteology Foundation Consensus Report Part 2—Effects of hard tissue augmentation procedures on the maintenance of peri-implant tissues. Clin. Oral Implant. Res. 2018, 29 (Suppl. S15), 11–13. [Google Scholar] [CrossRef] [Green Version]
- Sanz-Sánchez, I.; Carrillo de Albornoz, A.; Figuero, E.; Schwarz, F.; Jung, R.; Sanz, M.; Thoma, D. Effects of lateral bone augmentation procedures on peri-implant health or disease: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. S15), 18–31. [Google Scholar] [CrossRef]
- Derks, J.; Tomasi, C. Peri-implant health and disease. A systematic review of current epidemiology. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S158–S171. [Google Scholar] [CrossRef]
- García-Gareta, E.; Coathup, M.J.; Blunn, G.W. Osteoinduction of bone grafting materials for bone repair and regeneration. Bone 2015, 81, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Tavelli, L.; McGuire, M.K.; Zucchelli, G.; Rasperini, G.; Feinberg, S.E.; Wang, H.-L.; Giannobile, W.V. Biologics-based regenerative technologies for periodontal soft tissue engineering. J. Periodontal. 2020, 91, 147–154. [Google Scholar] [CrossRef]
- Romandini, M.; Pedrinaci, I.; Lima, C.; Soldini, M.C.; Araoz, A.; Sanz, M. Prevalence and risk/protective indicators of buccal soft tissue dehiscence around dental implants. J. Clin. Periodontol. 2021, 48, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Tavelli, L.; McGuire, M.K.; Rasperini, G.; Feinberg, S.E.; Wang, H.-L.; Giannobile, W.V. Autogenous soft tissue grafting for periodontal and peri-implant plastic surgical reconstruction. J. Periodontal. 2020, 91, 9–16. [Google Scholar] [CrossRef]
- Melcher, A.H. On the repair potential of periodontal tissues. J. Periodontol. 1976, 47, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Gottlow, J.; Nyman, S.; Lindhe, J.; Karring, T.; Wennström, J. New attachment formation in the human periodontium by guided tissue regeneration: Case reports. J. Clin. Periodontol. 1986, 13, 604–616. [Google Scholar] [CrossRef] [PubMed]
- Susin, C.; Fiorini, T.; Lee, J.; De Stefano, J.A.; Dickinson, D.P.; Wikesjo, U.M.E. Wound healing following surgical and regenerative periodontal therapy. Periodontology 2000 2015, 68, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Bosshardt, D.D.; Sculean, A. Does periodontal tissue regeneration really work? Periodontology 2000 2009, 51, 208–219. [Google Scholar] [CrossRef]
- Jepsen, S.; Schwarz, F.; Cordaro, L.; Derks, J.; Hämmerle, C.; Heitz-Mayfield, L.J.; Hernández-Alfaro, F.; Meijer, H.J.A.; Naenni, N.; Ortiz-Vigon, A.; et al. Regeneration of alveolar ridge defects—Consensus report of Group 4 of the 15th European Workshop on Periodontology on Bone Regeneration. J. Clin. Periodontol. 2019, 46 (Suppl. 21), 277–286. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Dahlin, C.; Apatzidou, D.; Artzi, Z.; Bozic, D. Biomaterials and regenerative technologies used in bone regeneration in the craniomaxillofacial region: Consensus report of Group 2 of the 15th European Workshop on Periodontology on Bone Regeneration. J. Clin. Periodontol. 2019, 46 (Suppl. 21), 82–91. [Google Scholar] [CrossRef]
- Cosyn, J.; Thoma, D.S.; Hämmerle, C.H.; De Bruyn, H. Esthetic assessments in implant dentistry: Objective and subjective criteria for clinicians and patients. Periodontology 2000 2017, 73, 193–202. [Google Scholar] [CrossRef] [Green Version]
- Haugen, H.J.; Lyngstadaas, S.P.; Rossi, F.; Perale, G. Bone grafts: Which is the ideal biomaterial? J. Clin. Periodontol. 2019, 46 (Suppl. 21), 92–102. [Google Scholar] [CrossRef]
- Bernardi, S.; Macchiarelli, G.; Bianchi, S. Autologous Materials in Regenerative Dentistry: Harvested Bone, Platelet Concentrates and Dentin Derivates. Molecules 2020, 25, 5330. [Google Scholar] [CrossRef] [PubMed]
- Torroni, A.; Marianetti, T.M.; Romandini, M.; Gasparini, G.; Cervelli, D. Mandibular reconstruction with different techniques. J. Craniofac. Surg. 2015, 26, 885–890. [Google Scholar] [CrossRef]
- Nabers, C.L.; O’Leary, T.J. Autogenous bone trasplant in the treatment of osseus defects. J. Periodontol. 1965, 36, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Cushing, M. Autogenous red marrow grafts: Potential induction of osteogenesis. J. Periodontol. 1969, 40, 492–497. [Google Scholar] [CrossRef]
- Sottosanti, J.S.; Bierly, J.A. The storage of marrow and its relation to periodontal grafting procedures. J. Periodontol. 1975, 46, 162–170. [Google Scholar] [CrossRef]
- Rocchietta, I.; Fontana, F.; Simion, M. Clinical outcomes of vertical bone augmentation to enable dental implant placement: A systematic review. J. Clin. Periodontol. 2008, 35, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, P.; Duvina, M.; Barbato, L.; Biondi, E.; Nuti, N. Bone regeneration in dentistry. Clin. Cases Miner. Bone Metab. 2011, 8, 24. [Google Scholar]
- Chiapasco, M.; Casentini, P.; Zaniboni, M. Bone augmentation procedures in implant dentistry. Int. J. Oral Maxillofac. Implant. 2009, 24, 237–259. [Google Scholar]
- Arrington, E.D.; Smith, W.J.; Chambers, H.G.; Bucknell, A.L.; Davino, N.A. Complications of iliac crest bone graft harvesting. Clin. Orthop. Relat. Res. 1996, 329, 300–309. [Google Scholar] [CrossRef]
- Proussaefs, P.; Lozada, J. The use of intraorally harvested autogenous block grafts for vertical alveolar ridge augmentation: A human study. Int. J. Periodontics Restor. Dent. 2005, 25, 351–363. [Google Scholar]
- Schallhorn, R.G. The use of autogenous hip marrow biopsy implants for bony crater defects. J. Periodontol. 1968, 39, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Boyce, T.; Edwards, J.; Scarborough, N. Allograft bone: The influence of processing on safety and performance. Orthop. Clin. 1999, 30, 571–581. [Google Scholar] [CrossRef]
- Tomford, W.W. Transmission of disease through transplantation of musculoskeletal allografts. J. Bone Jt. Surg. Am. 1995, 77, 1742–1754. [Google Scholar] [CrossRef]
- Urist, M.R. Bone: Formation by autoinduction. Science 1965, 150, 893–899. [Google Scholar] [CrossRef]
- Al Ghamdi, A.; Shibly, O.; Ciancio, S. Osseous grafting part II: Xenografts and alloplasts for periodontal regeneration—A literature review. J. Int. Acad. Periodontol. 2010, 12, 39–44. [Google Scholar]
- Stavropoulos, A.; Karring, T. Five-year results of guided tissue regeneration in combination with deproteinized bovine bone (Bio-Oss) in the treatment of intrabony periodontal defects: A case series report. Clin. Oral Investig. 2005, 9, 271–277. [Google Scholar] [CrossRef]
- Falacho, R.I.; Palma, P.J.; Marques, J.A.; Figueiredo, M.H.; Caramelo, F.; Dias, I.; Viegas, C.; Guerra, F. Collagenated Porcine Heterologous Bone Grafts: Histomorphometric Evaluation of Bone Formation Using Different Physical Forms in a Rabbit Cancellous Bone Model. Molecules 2021, 26, 1339. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A. Maxillary Sinus Augmentation with Decellularized Bovine Compact Particles: A Radiological, Clinical, and Histologic Report of 4 Cases. BioMed Res. Int. 2017, 2594670. [Google Scholar] [CrossRef]
- Kozakiewicz, M.; Wach, T. New Oral Surgery Materials for Bone Reconstruction—A Comparison of Five Bone Substitute Materials for Dentoalveolar Augmentation. Materials 2020, 13, 2935. [Google Scholar] [CrossRef]
- Kollati, P.; Koneru, S.; Dwarakanath, C.D.; Gottumukkala, S. Effectiveness of naturally derived bovine hydroxyapatite (Cerabone™) combined with platelet-rich fibrin matrix in socket preservation: A randomized controlled clinical trial. J. Indian Soc. Periodontol. 2019, 23, 145–151. [Google Scholar] [PubMed]
- Kyyak, S.; Blatt, S.; Schiegnitz, E.; Heimes, D.; Staedt, H.; Thiem, D.; Sagheb, K.; Al-Nawas, B.; Kämmerer, P.W. Activation of Human Osteoblasts via Different Bovine Bone Substitute Materials with and without Injectable Platelet Rich Fibrin In Vitro. Front. Bioeng. Biotechnol. 2021, 9, 599224. [Google Scholar] [CrossRef] [PubMed]
- Matos, S.; Guerra, F.; Krauser, J.T.; Figueiredo, H.; Marcelino, J.P.; Sanz, M. Evaluation of an anorganic bovine-derived mineral with P-15 hydrogel bone graft: Preliminary study in a rabbit cranial bone model. Clin. Oral Implant. Res. 2012, 23, 698–705. [Google Scholar] [CrossRef]
- Ortiz-Puigpelat, O.; Simões, A.; Caballé-Serrano, J.; Hernández-Alfaro, F. Blood absorption capacity of different xenograft bone substitutes: An in vitro study. J. Clin. Exp. Dent. 2019, 11, e1018–e1024. [Google Scholar] [CrossRef]
- Rombouts, C.; Jeanneau, C.; Camilleri, J.; Laurent, P.; About, I. Characterization and angiogenic potential of xenogeneic bone grafting materials: Role of periodontal ligament cells. Dent. Mater. J. 2016, 35, 900–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, V.J.; Michalek, J.E.; Liu, Q.; Mealey, B.L. Ridge preservation following tooth extraction using bovine xenograft compared with porcine xenograft: A randomized controlled clinical trial. J. Periodontol. 2020, 91, 361–368. [Google Scholar] [CrossRef]
- Lee, J.H.; Yi, G.S.; Lee, J.W.; Kim, D.J. Physicochemical characterization of porcine bone-derived grafting material and comparison with bovine xenografts for dental applications. J. Periodontal Implant Sci. 2017, 47, 388–401. [Google Scholar] [CrossRef] [Green Version]
- Stievano, D.; di Stefano, A.; Ludovichetti, M.; Pagnutti, S.; Gazzola, F.; Boato, C.; Stellini, E. Maxillary sinus lift through heterologous bone grafts and simultaneous acid-etched implants placement: Five-year follow-up. Minerva Chirurgica 2008, 63, 79–91. [Google Scholar] [PubMed]
- Stavropoulos, A.; Karring, T. Guided tissue regeneration combined with a deproteinized bovine bone mineral (Bio-Oss) in the treatment of intrabony periodontal defects—6-year results from a randomized-controlled clinical trial. J. Clin. Periodontol. 2010, 37, 200–210. [Google Scholar] [CrossRef]
- Caton, J.; de Furia, E.; Polson, A.; Nyman, S. Periodontal regeneration via selective cell repopulation. J. Periodontol. 1987, 58, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Nyman, S.; Gottlow, J.; Lindhe, J.; Karring, T.; Wennstrom, J. New attachment formation by guided tissue regeneration. J. Periodontal Res. 1987, 22, 252–254. [Google Scholar] [CrossRef] [PubMed]
- Kao, R.T.; Nares, S.; Reynolds, M.A. Periodontal regeneration—Intrabony defects: A systematic review from the AAP Regeneration Workshop. J. Periodontol. 2015, 86 (Suppl. S2), S77–S104. [Google Scholar] [CrossRef]
- Sculean, A.; Nikolidakis, D.; Nikou, G.; Ivanovic, A.; Chapple, I.L.C.; Stavropoulos, A. Biomaterials for promoting periodontal regeneration in human intrabony defects: A systematic review. Periodontology 2000 2015, 68, 182–216. [Google Scholar] [CrossRef]
- Jiménez Garcia, J.; Berghezan, S.; Caramês, J.; Dard, M.M.; Marques, D. Effect of cross-linked vs non-cross-linked collagen membranes on bone: A systematic review. J. Periodontal Res. 2017, 52, 955–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aurer, A.; Jorgic-Srdjak, K. Membranes for periodontal regeneration. Acta Stomatol. Croat. 2005, 39, 107–112. [Google Scholar]
- Singh, A.K. GTR membranes: The barriers for periodontal regeneration. DHR Int. J. Med. Sci. 2013, 4, 31–38. [Google Scholar]
- Minabe, M. A critical review of the biologic rationale for guided tissue regeneration. J. Periodontol. 1991, 62, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Bunyaratavej, P.; Wang, H.L. Collagen membranes: A review. J. Periodontol. 2001, 72, 215–229. [Google Scholar] [CrossRef] [Green Version]
- Bartee, B.K.; Carr, J. Evaluation of a high-density polytetrafluoroethylene (n-PTFE) membrane as a barrier material to facilitate guided bone regeneration in the rat mandible. J. Oral Implantol. 1995, 21, 88–95. [Google Scholar]
- Marouf, H.A.; El-Guindi, H.M. Efficacy of high-density versus semipermeable PTFE membranes in an elderly experimental model. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2000, 89, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Babo, P.S.; Pires, R.L.; Reis, R.L.; Gomes, M.E. Membranes for periodontal tissues regeneration. Ciência Tecnol. Mater. 2014, 26, 108–117. [Google Scholar]
- Monteiro, A.; Macedo, L.; Macedo, N.-L.; Balducci, I. Polyurethane and PTFE membranes for guided bone regeneration: Histopathological and ultrastructural evaluation. Med. Oral Patol. Oral Cir. Bucal 2010, 15, e401–e406. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Pini Prato, G.; Tonetti, M.S. Periodontal regeneration of human intrabony defects with titanium reinforced membranes: A controlled clinical trial. J. Periodontol. 1995, 66, 797–803. [Google Scholar] [CrossRef] [PubMed]
- Murphy, K.G. Postoperative healing complications associated with Gore-Tex periodontal material, part I: Incidence and characterization. Int. J. Periodontics Restor. Dent. 1995, 15, 363–375. [Google Scholar]
- Cortellini, P.; Prato, G.P.; Tonetti, M.S. The modified papilla preservation technique: A new surgical approach for interproximal regenerative procedures. J. Periodontol. 1995, 66, 261–266. [Google Scholar] [CrossRef]
- Cortellini, P.; Prato, G.P.; Tonetti, M.S. The simplified papilla preservation flap: A novel surgical approach for the management of soft tissues in regenerative procedures. Int. J. Periodontics Restor. Dent. 1999, 19, 589–599. [Google Scholar]
- Cortellini, P.; Tonetti, M.S. A minimally invasive surgical technique with an enamel matrix derivative in the regenerative treatment of intra-bony defects: A novel approach to limit morbidity. J. Clin. Periodontol. 2007, 34, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Trombelli, L.; Farina, R.; Franceschetti, G. Use of the single flap approach in periodontal reconstructive surgery. Dent. Cadmos 2007, 8, 15–25. [Google Scholar]
- Aimetti, M.; Fratini, A.; Manavella, V.; Giraudi, M.; Citterio, F.; Ferrarotti, F.; Mariani, G.M.; Cairo, F.; Baima, G.; Romano, F. Pocket resolution in regenerative treatment of intrabony defects with papilla preservation techniques: A systematic review and meta-analysis of randomized clinical trials. J. Clin. Periodontol. 2021, 48, 843–858. [Google Scholar] [CrossRef]
- Dennison, D.K.; Vallone, D.R.; Pinero, G.J.; Rittman, B.; Caffesse, R.G. Differential effect of TGF-β1 and PDGF on proliferation of periodontal ligament cells and gingival fibroblasts. J. Periodontol. 1994, 65, 641–648. [Google Scholar] [CrossRef]
- Oates, T.W.; Rouse, C.A.; Cochran, D.L. Mitogenic effects of growth factors on human periodontal ligament cells in vitro. J. Periodontol. 1993, 64, 142–148. [Google Scholar] [CrossRef]
- Giannobile, W.; Whitson, S.; Lynch, S. Non-coordinate control of bone formation displayed by growth factor combinations with IGF-I. J. Dent. Res. 1997, 76, 1569–1578. [Google Scholar] [CrossRef] [PubMed]
- Strauss, F.J.; Stähli, A.; Gruber, R. The use of platelet-rich fibrin to enhance the outcomes of implant therapy: A systematic review. Clin. Oral Implant. Res. 2018, 29 (Suppl. S18), 6–19. [Google Scholar] [CrossRef]
- Mancini, L.; Tarallo, F.; Quinzi, V.; Fratini, A.; Mummolo, S. Platelet-Rich Fibrin in Single and Multiple Coronally Advanced Flap for Type 1 Recession: An Updated Systematic Review and Meta-Analysis. Medicina 2021, 57, 144. [Google Scholar] [CrossRef]
- Tarallo, F.; Mancini, L.; Pitzurra, L.; Bizzarro, S.; Tepedino, M.; Marchetti, E. Use of Platelet-Rich Fibrin in the Treatment of Grade 2 Furcation Defects: Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2104. [Google Scholar] [CrossRef] [PubMed]
- Nevins, M.; Camelo, M.; Nevins, M.L.; Schenk, R.K.; Lynch, S.E. Periodontal regeneration in humans using recombinant human platelet-derived growth factor-BB (rhPDGF-BB) and allogenic bone. J. Periodontol. 2003, 74, 1282–1292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannobile, W.V.; Hernandez, R.A.; Finkelman, R.D.; Ryarr, S.; Kiritsy, C.P. Comparative effects of plateletderived growth factor-BB and insulin-like growth factor-I, individually and in combination, on periodontal regeneration in Macaca fascicularis. J. Periodontal Res. 1996, 31, 301–312. [Google Scholar] [CrossRef]
- Lynch, S.E.; Buser, D.; Hernandez, R.A.; Weber, H.; Stich, H.; Fox, C.H.; Williams, R.C. Effects of the platelet-derived growth factor/insulin-like growth factor-I combination on bone regeneration around titanium dental implants: Results of a pilot study in beagle dogs. J. Periodontol. 1991, 62, 710–716. [Google Scholar] [CrossRef]
- Izumi, Y.; Aoki, A.; Yamada, Y.; Kobayashi, H.; Iwata, T.; Akizuki, T.; Suda, T.; Nakamura, S.; Wara-Aswapati, N.; Ueda, M.; et al. Current and future periodontal tissue engineering. Periodontology 2000 2011, 56, 166–187. [Google Scholar] [CrossRef]
- Thoma, D.S.; Payer, M.; Jakse, N.; Bienz, S.P.; Husler, J.; Schmidlin, P.R.; Jung, U.-W.; Hammerle, C.H.F.; Jung, R.E. Randomized, controlled clinical two-centre study using xenogeneic block grafts loaded with recombinant human bone morphogenetic protein-2 or autogenous bone blocks for lateral ridge augmentation. J. Clin. Periodontol. 2018, 45, 265–276. [Google Scholar] [CrossRef] [Green Version]
- Giannobile, W. Periodontal tissue engineering by growth factors. Bone 1996, 19, S23–S37. [Google Scholar] [CrossRef]
- Chiu, H.C.; Chiang, C.Y.; Tu, H.P.; Wikesjo, U.M.; Susin, C. Effects of bone morphogenetic protein-6 on periodontal wound healing/regeneration in supraalveolar periodontal defects in dogs. J. Clin. Periodontol. 2013, 40, 624–630. [Google Scholar] [CrossRef]
- Sigurdsson, T.J.; Lee, M.B.; Kubota, K.; Turek, T.J.; Wozney, J.M. Periodontal repair in dogs: Recombinant human bone morphogenetic protein-2 significantly enhances periodontal regeneration. J. Periodontol. 1995, 66, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Wikesjo, U.M.; Guglielmoni, P.; Promsudthi, A.; Cho, K.S.; Trombelli, L.; Selvig, K.A.; Jin, L.; Wozney, J.M. Periodontal repair in dogs: Effect of rhBMP-2 concentration on regeneration of alveolar bone and periodontal attachment. J. Clin. Periodontol. 1999, 26, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Luan, X.; Ito, Y.; Diekwisch, T.G. Evolution and development of Hertwig’s epithelial root sheath. Dev. Dyn. 2006, 235, 1167–1180. [Google Scholar] [CrossRef] [Green Version]
- Zeichner-David, M.; Oishi, K.; Su, Z.; Zakartchenko, V.; Chen, L.S.; Arzate, H.; Bringas, P., Jr. Role of Hertwig’s epithelial root sheath cells in tooth root development. Dev. Dyn. 2003, 228, 651–663. [Google Scholar] [CrossRef]
- Giannobile, W.V.; Somerman, M.J. Growth and amelogenin-like factors in periodontal wound healing—A systematic review. Ann. Periodontol. 2003, 8, 193–204. [Google Scholar] [CrossRef]
- Hammarström, L. Enamel matrix, cementum development and regeneration. J. Clin. Periodontol. 1997, 24, 658–668. [Google Scholar] [CrossRef] [PubMed]
- Jentsch, H.; Purschwitz, R. A clinical study evaluating the treatment of supra-alveolar-type defects with access flap surgery with and without an enamel matrix protein derivative: A pilot study. J. Clin. Periodontol. 2008, 35, 713–718. [Google Scholar] [CrossRef]
- Jepsen, S.; Heinz, B.; Jepsen, K.; Arjomand, M.; Hoffmann, T.; Richter, S.; Reich, E.; Sculean, A.; Gonzales, J.R.; Bodeker, R.H.; et al. A randomized clinical trial comparing enamel matrix derivative and membrane treatment of buccal Class II furcation involvement in mandibular molars, Part I: Study design and results for primary outcomes. J. Periodontal. 2004, 75, 1150–1160. [Google Scholar] [CrossRef] [Green Version]
- McGuire, M.K.; Nunn, M. Evaluation of human recession defects treated with coronally advanced flaps and either enamel matrix derivative or connective tissue, Part 1: Comparison of clinical parameters. J. Periodontal. 2003, 74, 1110–1125. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Tonetti, M.S.; Zabalegui, I.; Sicilia, A.; Blanco, J.; Rebelo, H.; Rasperini, G.; Merli, M.; Cortellini, P.; Suvan, J.E. Treatment of intrabony defects with enamel matrix proteins or barrier membranes: Results from a multicenter practice-based clinical trial. J. Periodontol. 2004, 75, 726–733. [Google Scholar] [CrossRef] [PubMed]
- Romandini, M.; Calatrava, J.; Nobili, A.; Calzavara, D.; Sanz, M. Treatment of severe intra-bony lesions with emd application and different soft-tissue management techniques: A case report. Dent. Cadmos 2021, 89, 314–318. [Google Scholar] [CrossRef]
- Miron, R.J.; Sculean, A.; Cochran, D.L.; Froum, S.; Zucchelli, G. Twenty years of enamel matrix derivative: The past, the present and the future. J. Clin. Periodontol. 2016, 43, 668–683. [Google Scholar] [CrossRef] [PubMed]
- Isehed, C.; Holmlund, A.; Renvert, S.; Svenson, B.; Johansson, I.; Lundberg, P. Effectiveness of enamel matrix derivative on the clinical and microbiological outcomes following surgical regenerative treatment of peri-implantitis: A randomized controlled trial. J. Clin. Periodontol. 2016, 43, 863–873. [Google Scholar] [CrossRef]
- Palma, P.J.; Ramos, J.C.; Martins, J.B.; Diogenes, A.; Figueiredo, M.H.; Ferreira, P.; Viegas, C.; Santos, J.M. Histologic Evaluation of Regenerative Endodontic Procedures with the Use of Chitosan Scaffolds in Immature Dog Teeth with Apical Periodontitis. J. Endod. 2017, 43, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Fujioka-Kobayashi, M.; Müller, H.D.; Mueller, A.; Lussi, A.; Sculean, A.; Schmidlin, P.R.; Miron, R.J. In vitro effects of hyaluronic acid on human periodontal ligament cells. BMC Oral Health 2017, 17, 44. [Google Scholar] [CrossRef] [Green Version]
- Pilloni, A.; Nardo, F.; Rojas, M.A. Surgical treatment of a cemental tear-associated bony defect using hyaluronic acid and a resorbable collagen membrane: A 2-year follow-up. Clin. Adv. Periodontics 2019, 9, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Pilloni, A.; Rojas, M.A.; Marini, L.; Russo, P.; Shirakata, Y.; Sculean, A.; Iacono, R. Healing of intrabony defects following regenerative surgery by means of single-flap approach in conjunction with either hyaluronic acid or an enamel matrix derivative: A 24-month randomized controlled clinical trial. Clin. Oral Investig. 2021. [Google Scholar] [CrossRef]
- Eliezer, M.; Imber, J.C.; Sculean, A.; Pandis, N.; Teich, S. Hyaluronic acid as adjunctive to non-surgical and surgical periodontal therapy: A systematic review and meta-analysis. Clin. Oral Investig. 2019, 23, 3423–3435. [Google Scholar] [CrossRef] [PubMed]
- Soriano-Lerma, A.; Magan-Fernandez, A.; Gijon, J.; Sanchez-Fernandez, E.; Soriano, M.; Garcia-Salcedo, J.A.; Mesa, F. Short-term effects of hyaluronic acid on the subgingival microbiome in peri-implantitis: A randomized controlled clinical trial. J. Periodontol. 2020, 91, 734–745. [Google Scholar] [CrossRef] [PubMed]
- De Araújo Nobre, M.; Cintra, N.; Maló, P. Peri-implant maintenance of immediate function implants: A pilot study comparing hyaluronic acid and chlorhexidine. Int. J. Dent. Hyg. 2007, 5, 87–94. [Google Scholar] [CrossRef]
- Ghanaati, S.; Barbeck, M.; Hilbig, U.; Hoffmann, C.; Unger, R.E.; Sader, R.A.; Peters, F.; Kirkpatrick, C.J. An injectable bone substitute composed of beta-tricalcium phosphate granules, methylcellulose and hyaluronic acid inhibits connective tissue influx into its implantation bed in vivo. Acta Biomater. 2011, 7, 4018–4028. [Google Scholar] [CrossRef]
- Marchetti, E.; Mancini, L.; Bernardi, S.; Bianchi, S.; Cristiano, L.; Torge, D.; Marzo, G.; Macchiarelli, G. Evaluation of Different Autologous Platelet Concentrate Biomaterials: Morphological and Biological Comparisons and Considerations. Materials 2020, 13, 2282. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Karanxha, L.; Panda, S.; Bucchi, C.; Nadathur Doraiswamy, J.; Sankari, M.; Ramamoorthi, S.; Varghese, S.; Taschieri, S. Autologous platelet concentrates for treating periodontal infrabony defects. Cochrane Database Syst. Rev. 2018, 11, CD011423. [Google Scholar] [CrossRef] [PubMed]
- Panda, S.; Karanxha, L.; Goker, F.; Satpathy, A.; Taschieri, S.; Francetti, L.; Chandra Das, A.; Kumar, M.; Panda, S.; del Fabbro, M. Autologous Platelet Concentrates in Treatment of Furcation Defects—A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2019, 20, 1347. [Google Scholar] [CrossRef] [Green Version]
- Panda, S.; Purkayastha, A.; Mohanty, R.; Nayak, R.; Satpathy, A.; Chandra Das, A.; Kumar, M.; Mohanty, G.; Panda, S.; Fabbro, M.D. Plasma rich in growth factors (PRGF) in non-surgical periodontal therapy: A randomized clinical trial. Braz. Oral Res. 2020, 34, e034. [Google Scholar] [CrossRef] [PubMed]
- Polak, D.; Clemer-Shamai, N.; Shapira, L. Incorporating antibiotics into platelet-rich fibrin: A novel antibiotics slow-release biological device. J. Clin. Periodontol. 2019, 46, 241–247. [Google Scholar] [CrossRef]
- Zakrzewski, W.; Dobrzyński, M.; Szymonowicz, M.; Rybak, Z. Stem cells: Past, present, and future. Stem Cell Res. Ther. 2019, 10, 68. [Google Scholar] [CrossRef]
- Trovato, L.; Naro, F.; D’Aiuto, F.; Moreno, F. Promoting tissue repair by micrograft stem cells delivery. Stem Cells Int. 2020, 2195318. [Google Scholar] [CrossRef] [PubMed]
- Tassi, S.A.; Sergio, N.Z.; Misawa, M.Y.O.; Villar, C.C. Efficacy of stem cells on periodontal regeneration: Systematic review of preclinical studies. J. Periodontal Res. 2017, 52, 793–812. [Google Scholar] [CrossRef]
- Liu, J.; Ruan, J.; Weir, M.D.; Ren, K.; Schneider, A.; Wang, P.; Oates, T.W.; Chang, X.; Xu, H.H.K. Periodontal bone-ligament-cementum regeneration via scaffolds and stem cells. Cells 2019, 8, 537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mummolo, S.; Mancini, L.; Quinzi, V.; D’Aquino, R.; Marzo, G.; Marchetti, E. Rigenera® autologous micrografts in oral regeneration: Clinical, histological, and radiographical evaluations. Appl. Sci. 2020, 10, 5084. [Google Scholar] [CrossRef]
- Zheng, R.C.; Park, Y.K.; Cho, J.J.; Kim, S.K.; Heo, S.J.; Koak, J.Y.; Lee, J.H. Bone regeneration at dental implant sites with suspended stem cells. J. Dent. Res. 2014, 93, 1005–1013. [Google Scholar] [CrossRef] [Green Version]
- Chia, H.N.; Wu, B.M. Recent advances in 3D printing of biomaterials. J. Biol. Eng. 2015, 9, 4. [Google Scholar] [CrossRef] [Green Version]
- Park, C.H.; Rios, H.F.; Jin, Q.; Sugai, J.V.; Padial-Molina, M.; Taut, A.D.; Flanagan, C.L.; Hollister, S.J.; Giannobile, W.V. Tissue engineering bone-ligament complexes using fiber-guiding scaffolds. Biomaterials 2012, 33, 137–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.H.; Rios, H.F.; Taut, A.D.; Padial-Molina, M.; Flanagan, C.L.; Pilipchuk, S.P.; Hollister, S.J.; Giannobile, W.V. Image-based, fiber guiding scaffolds: A platform for regenerating tissue interfaces. Tissue Eng. Part C Methods 2014, 20, 533–542. [Google Scholar] [CrossRef] [Green Version]
- Goh, B.T.; Teh, L.Y.; Tan, D.B.; Zhang, Z.; Teoh, S.H. Novel 3D polycaprolactone scaffold for ridge preservation—A pilot randomised controlled clinical trial. Clin. Oral Implant. Res. 2015, 26, 271–277. [Google Scholar] [CrossRef]
- Obregon, F.; Vaquette, C.; Ivanovski, S.; Hutmacher, D.W.; Bertassoni, L.E. Three-dimensional bioprinting for regenerative dentistry and craniofacial tissue engineering. J. Dent. Res. 2015, 94 (Suppl. S9), S143–S152. [Google Scholar] [CrossRef]
Figure 1.
Iconographic representation of the factors involved in periodontal regeneration.

Figure 2.
Approaches for regenerating periodontal and peri-implant sites after treating the disease.
Figure 2.
Approaches for regenerating periodontal and peri-implant sites after treating the disease.

Figure 3.
Characteristic of bone grafts according to the origin.

Figure 4.
Examples of autografts in the peri-implant site. (A) Autologous bone grafts in residual defect after post extractive implant, (B) autologous bone grafts on implant after peri-implantitis.
Figure 4.
Examples of autografts in the peri-implant site. (A) Autologous bone grafts in residual defect after post extractive implant, (B) autologous bone grafts on implant after peri-implantitis.

Figure 5.
Example of xenografts in a periodontal defect. (A) Probing depth, (B) bone sounding, (C) flap design, (D) periodontal defect, (E) collagenated bovine bone graft, (F) primary wound closure.
Figure 5.
Example of xenografts in a periodontal defect. (A) Probing depth, (B) bone sounding, (C) flap design, (D) periodontal defect, (E) collagenated bovine bone graft, (F) primary wound closure.

Figure 6.
Example of peri-implant regeneration after peri-implantitis with xenografts and collagen membranes. After the peri-implant access, a heavy implant debridement was achieved and an implantoplasty was mandatory to remove the infected surface. The peri-implant defect was filled with xenogeneic grafts and covered with a resorbable membrane.
Figure 6.
Example of peri-implant regeneration after peri-implantitis with xenografts and collagen membranes. After the peri-implant access, a heavy implant debridement was achieved and an implantoplasty was mandatory to remove the infected surface. The peri-implant defect was filled with xenogeneic grafts and covered with a resorbable membrane.

Figure 7.
Clinical indications for EMD in periodontal regeneration with respect to the defect’s type modified from Miron et al. [95].
Figure 7.
Clinical indications for EMD in periodontal regeneration with respect to the defect’s type modified from Miron et al. [95].

Figure 8.
Peri-implant defects treated with L-PRF and xenografts. (A) Baseline, (B) baseline occlusal view, (C) access flap, (D) implantoplasty, (E) L-PRF membranes and xenografts in the defect, (F) primary wound healing.
Figure 8.
Peri-implant defects treated with L-PRF and xenografts. (A) Baseline, (B) baseline occlusal view, (C) access flap, (D) implantoplasty, (E) L-PRF membranes and xenografts in the defect, (F) primary wound healing.

Figure 9.
Biomaterials and their possible implications in periodontal/peri-implant regeneration.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Commercialized bone substitutes and heating temperature according to their production process and the manufacturing protocol.
Table 1.
Commercialized bone substitutes and heating temperature according to their production process and the manufacturing protocol.
| Commercial Name | Sources | Heating Temperature |
|---|---|---|
| Bio-Oss® | Bovine | 300 °C [38] |
| Re-bone® | Bovine | −80 °C to 121 °C [41] |
| Endobon® | Bovine | 900 °C [42] |
| cerabone® | Bovine | 1250 °C [43] |
| creosTM | Bovine | 600 °C [44] |
| PepGen P-15® | Bovine | 1100 °C [45] |
| SmartBone® | Bovine + Porcine | 50 °C < [46] |
| Gen-Os® | Porcine | 130 °C [47] |
| Zcore® | Porcine | 500 °C to 620 °C [48] |
| THE GraftTM | Porcine | 400 °C [49] |
| Equimatrix® | Equine | N/A |
| Bio-Gen® | Equine | 130 °C [50] |
Table 2.
Collagen membranes classified according to the sources, main components, and cross-linking agent, as reported on the manufacturing instructions.
Table 2.
Collagen membranes classified according to the sources, main components, and cross-linking agent, as reported on the manufacturing instructions.
| Commercial Name | Sources | Main Components | Cross-Linking Agent | Resorption Rate |
|---|---|---|---|---|
| Bio-Gide | Porcine | Type I and III collagen | None | 24 weeks |
| Biostite | Calfskin | 88% HA 9.5% type I collagen and 2.5% chondroitin sulfate | Diphenylphosphoryl azide | 4–8 weeks |
| BioMend | Bovine | 100% type I collagen | Formaldehyde | 6–8 weeks |
| BioBar | Bovine | 100% type I collagen | N/A | 6–8 months |
| BioMend-Extend | Bovine | 100% type I collagen | Formaldehyde | 18 weeks |
| Periogen | Bovine | Type I and III collagen | Glutaraldehyde | 4–8 weeks |
| Paroguide | Calfskin | 96% type I collagen and 4% chondroitin sulfate | Diphenylphosphoryl azide | 4–8 weeks |
| OsteoBiol | Equine | 100% equine collagen | None | 8 weeks |
| Tissue Guide | Bovine dermis + tendon | Atelocollagen + tendon collagen | Hexamethylene diisocyanate | 4–8 weeks |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Mancini, L.; Romandini, M.; Fratini, A.; Americo, L.M.; Panda, S.; Marchetti, E. Biomaterials for Periodontal and Peri-Implant Regeneration. Materials 2021, 14, 3319. https://doi.org/10.3390/ma14123319
AMA Style
Mancini L, Romandini M, Fratini A, Americo LM, Panda S, Marchetti E. Biomaterials for Periodontal and Peri-Implant Regeneration. Materials. 2021; 14(12):3319. https://doi.org/10.3390/ma14123319
Chicago/Turabian StyleMancini, Leonardo, Mario Romandini, Adriano Fratini, Lorenzo Maria Americo, Saurav Panda, and Enrico Marchetti. 2021. "Biomaterials for Periodontal and Peri-Implant Regeneration" Materials 14, no. 12: 3319. https://doi.org/10.3390/ma14123319
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.