Self-Efficacy and Emotional Intelligence as Predictors of Perceived Stress in Nursing Professionals

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Emotional Intelligence, Self-Efficacy and Perceived Stress
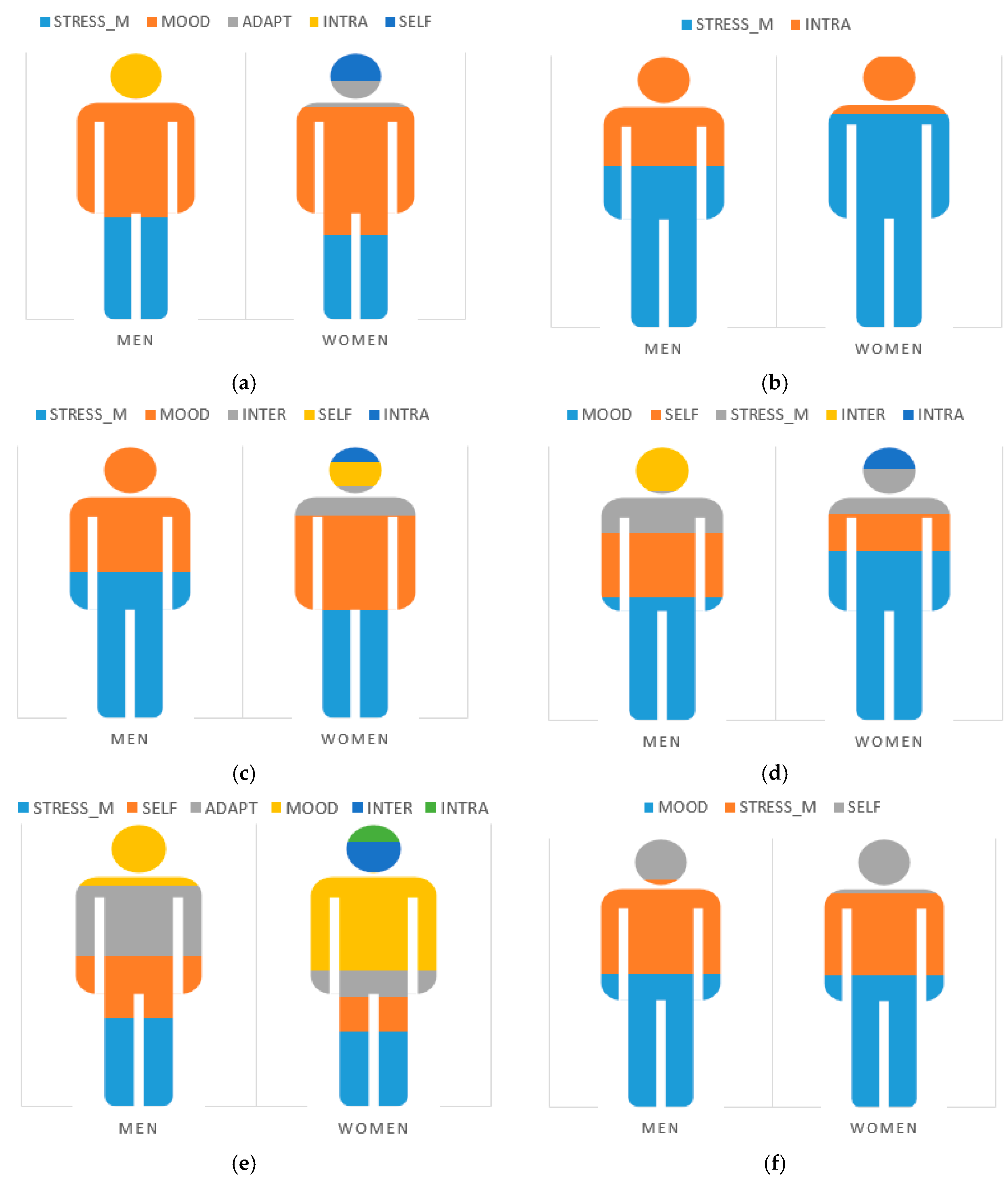
3.2. Predictors of the Harassment–Social Acceptance Dimension of Perceived Stress
3.3. Predictors of the Overload Dimension of Perceived Stress
3.4. Predictors of the Irritability–Tension–Fatigue Dimension of Perceived Stress
3.5. Predictors of the Energy–Joy Dimension of Perceived Stress
3.6. Predictors of the Fear–Anxiety Dimension of Perceived Stress
3.7. Predictors of the Self-Realization–Satisfaction Dimension of Perceived Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lazarus, R.S. Emotion and Adaptation; Oxford University Press: New York, NY, USA, 1991. [Google Scholar]
- Lazarus, R.S.; Folkman, S. Estrés y Procesos Cognitivos [Stress and Cognitive Processes]; Martínez Roca: Barcelona, Spain, 1986. [Google Scholar]
- García-Rodríguez, A.; Gutiérrez-Bedmar, M.; Bellón-Saameño, J.Á.; Muñoz-Bravo, C.; Fernández-Crehuet, J.N. Psychosocial stress environment and health workers in public health: Differences between primary and hospital care. Aten. Primaria 2015, 47, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Batool, I.; Nishat, N.; Yaqoob, A. A work-related stress among nurses of public hospitals of AJ&K"-Cross-Sectional Descriptive Study. HealthMed. 2012, 6, 1651–1660. [Google Scholar]
- Munnangi, S.; Dupiton, L.; Boutin, A.; Angus, L.D. Burnout, perceived stress, and job satisfaction among trauma nurses at a level I safetynet trauma center. J. Trauma Nurs. 2018, 25, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Levenstein, S.; Prantera, C.; Varvo, V.; Scribano, M.L.; Berto, E.; Luzi, C.; Andreoli, A. Development of the Perceived Stress Questionnaire: a new tool for psychosomatic research. J. Psychosom. Res. 1993, 37, 19–32. [Google Scholar] [CrossRef]
- Birks, Y.; McKendree, J.; Watt, I. Emotional intelligence and perceived stress in healthcare students: a multi-institutional, multi-professional survey. BMC Med. Educ. 2009, 9, 61. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.; Fethney, J.; Kozlowski, D.; Fois, R.; Reza, F.; McCloughen, A. Emotional intelligence and perceived stress of Australian pre-registration healthcare students: A multi-disciplinary cross-sectional study. Nurse Educ. Today 2018, 66, 51–56. [Google Scholar] [CrossRef]
- Ko, C.M. Mediating effect of stress on relationship between emotional intelligence and burnout among nursing college students. J. Korean Soc. Sch. Health 2015, 28, 239–247. [Google Scholar] [CrossRef]
- Montes-Berges, B.; Augusto, J.M. Exploring the relationship between perceived emotional intelligence, coping, social support and mental health in nursing students. J. Psychiatr. Ment. Health Nurs. 2007, 14, 163–171. [Google Scholar] [CrossRef]
- Salovey, P.; Mayer, J.D. Emotional Intelligence. Imagin. Cogn. Pers. 1990, 9, 185–211. [Google Scholar] [CrossRef]
- Goleman, D. Emotional Intelligence; Bantam Books: New York, NY, USA, 1995. [Google Scholar]
- Bar-On, R. The Emotional Quotient Inventory (EQ-i): Technical Manual; Multi-Health Systems: Toronto, ON, Canada, 1997. [Google Scholar]
- Molero, M.M.; Pérez-Fuentes, M.C.; Gázquez, J.J.; Simón, M.M.; Martos, A. Burnout Risk and Protection Factors in Certified Nursing Aides. Int. J. Environ. Res. Public Health 2018, 15, 1116. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J.; Oropesa, N.F. The role of Emotional Intelligence in Engagement in Nurses. Int. J. Environ. Res. Public Health 2018, 15, 1915. [Google Scholar] [CrossRef]
- Tagoe, T.; Quarshie, E.N.B. The relationship between emotional intelligence and job satisfaction among nurses in Accra. Nurs. Open 2017, 4, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, V.S.; Guerrero, E.; Chambel, M.J. Emotional intelligence and health students’ well-being: A two-wave study with students of medicine, physiotherapy and nursing. Nurse Educ. Today 2018, 63, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Nel, J.A.; Jonker, C.S.; Rabie, T. Emotional intelligence and wellness among employees working in the nursing environment. J. Psychol. Afr. 2013, 23, 195–203. [Google Scholar] [CrossRef]
- Por, J.; Barriball, L.; Fitzpatrick, J.; Roberts, J. Emotional intelligence: Its relationship to stress, coping, well-being and professional performance in nursing students. Nurse Educ. Today 2011, 31, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Sommaruga, M.; Casu, G.; Giaquinto, F.; Gremigni, P. Self-perceived provision of patient centered care by healthcare professionals: The role of emotional intelligence and general self-efficacy. Patient Educ. Couns. 2017, 100, 974–980. [Google Scholar] [CrossRef] [PubMed]
- Snowden, A.; Stenhouse, R.; Duers, L.; Marshall, S.; Carver, F.; Brown, N.; Young, J. The relationship between emotional intelligence, previous caring experience and successful completion of a pre-registration nursing/midwifery degree. J. Adv. Nurs. 2018, 74, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Kozlowski, D.; Hutchinson, M.; Hurley, J.; Rowley, J.; Sutherland, J. The role of emotion in clinical decision making: an integrative literature review. BMC Med. Educ. 2017, 17, 255. [Google Scholar] [CrossRef] [PubMed]
- Gerits, L.; Derksen, J.J.; Verbruggen, A.B.; Katzko, M. Emotional intelligence profiles of nurses caring for people with severe behaviour problems. Pers. Individ. Dif. 2005, 38, 33–43. [Google Scholar] [CrossRef]
- Azimi, S.; AsgharNejad, A.A.; Kharazi, M.J.; Khoei, N. Emotional intelligence of dental students and patient satisfaction. Eur. J. Dent. Educ. 2010, 14, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Peña-Sarrionandia, A.; Mikolajczak, M.; Gross, J.J. Integrating emotion regulation and emotional intelligence traditions: a meta-analysis. Front. Psychol. 2015, 6, 160. [Google Scholar] [CrossRef] [PubMed]
- Szczygiel, D.D.; Mikolajczak, M. Emotional Intelligence Buffers the Effects of Negative Emotions on Job Burnout in Nursing. Front. Psychol. 2018, 9, 2649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, D.L.; Newman, D.A. Emotional Intelligence: An Integrative Meta-Analysis and Cascading Model. J. Appl. Psychol. 2010, 95, 54–78. [Google Scholar] [CrossRef] [PubMed]
- Shoji, K.; Cieslak, R.; Smoktunowicz, E.; Rogala, A.; Benight, C.C.; Luszczynska, A. Associations between job burnout and self-efficacy: A meta-analysis. Anxiety Stress Coping 2016, 29, 367–386. [Google Scholar] [CrossRef] [PubMed]
- Bodys-Cupak, I.; Majda, A.; Zalewska-Puchała, J.; Kamińska, A. The impact of a sense of self-efficacy on the level of stress and the ways of coping with difficult situations in Polish nursing students. Nurse Educ. Today 2016, 45, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.C.; Yu, P.; Chang, S.Y. Longitudinal relationships between two self-efficacy types and stress in active older adults in Taichung City, Taiwan. Int. J. Ment. Health Promot. 2016, 18, 95–105. [Google Scholar] [CrossRef]
- Osuna, J.A. Estrés en médicos residentes en una Unidad de Atención Médica de tercer nivel [Stress in doctors residing in a third level Medical Care Unit]. Cir. Gen. 2006, 28, 103–109. [Google Scholar]
- Cherniss, C. Long-term consequences of burnout: An exploratory study. J. Organ. Behav. 1992, 13, 1–11. [Google Scholar] [CrossRef]
- Schaufeli, W.; Enzmann, D. The Burnout Companion to Study and Practice: A Critical Analysis; CRC Press: Boca Ranton, FL, USA, 1998. [Google Scholar]
- Luszczynska, A.; Gutiérrez-Doña, B.; Schwarzer, R. General self-efficacy in various domains of human functioning: Evidence from five countries. Int. J. Psychol. Res. 2005, 40, 80–89. [Google Scholar] [CrossRef]
- Ebstrup, J.F.; Eplov, L.F.; Pisinger, C.; Jørgensen, T. Association between the Five Factor personality traits and perceived stress: is the effect mediated by general self-efficacy? Anxiety Stress Coping 2011, 24, 407–419. [Google Scholar] [CrossRef] [PubMed]
- Şahin, F.; Çetin, F. The mediating role of general self-efficacy in the relationship between the big five personality traits and perceived stress: a weekly assessment study. Psychol. Stud. 2017, 62, 35–46. [Google Scholar] [CrossRef]
- Sanz-Carrillo, C.; García-Campayo, J.; Rubio, A.; Santed, M.A.; Montoro, M. Validation of the Spanish version of the Perceived Stress Questionnaire. J. Psychosomat. Res. 2002, 52, 167–172. [Google Scholar] [CrossRef]
- Baessler, J.; Schawarzer, R. Evaluación de la autoeficacia: Adaptación Española de la Escala de Autoeficacia General. Ansiedad Estrés 1996, 2, 1–7. [Google Scholar]
- Sanjuán, P.; Pérez, A.M.; Bermúdez, J. Escala de autoeficacia general: datos psicométricos de la adaptación para población Española. Psicothema 2000, 12, 509–513. [Google Scholar]
- Pérez-Fuentes, M.C.; Gázquez, J.J.; Mercader, I.; Molero, M.M. Brief Emotional Intelligence Inventory for Senior Citizens (EQ-i-M20). Psicothema 2014, 26, 524–530. [Google Scholar] [CrossRef]
- Bar-On, R.; Parker, J.D.A. Emotional Quotient Inventory: Youth Version (EQi:YV): TECHNICAL manual; Multi-Health Systems: Toronto, ON, Canada, 2000. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; The Guilford Press: New York, NY, USA, 2013. [Google Scholar]



{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. SELF | - | ||||||||||
| 2. H–SA | −0.31 *** | - | |||||||||
| 3. OVER | −0.02 | 0.49 *** | - | ||||||||
| 4. I–T–F | −0.30 *** | 0.76 *** | 0.62 *** | - | |||||||
| 5. E–J | 0.39 *** | −0.61 *** | −0.32 *** | −0.64 *** | - | ||||||
| 6. F–A | −0.29 *** | 0.61 *** | 0.47 *** | 0.71 *** | −0.45 *** | - | |||||
| 7. SR–S | −0.38 *** | 0.69 *** | 0.37 *** | 0.68 *** | −0.58 *** | 0.60 *** | - | ||||
| 8. INTRA | 0.30 *** | −0.24 *** | −0.10 *** | −0.22 *** | 0.31 *** | −0.20 *** | −0.23 *** | - | |||
| 9. INTER | 0.42 *** | −0.23 *** | 0.03 | −0.18 *** | 0.34 *** | −0.14 *** | −0.27 *** | 0.39 *** | - | ||
| 10. STRESS_M | 0.20 *** | −0.45 *** | −0.24 *** | −0.50 *** | 0.32 *** | −0.39 *** | −0.40 *** | 0.10 *** | 0.18 *** | - | |
| 11. ADAPT | 0.57 *** | −0.28 *** | −0.02 | −0.27 *** | 0.42 *** | −0.26 *** | −0.35 *** | 0.45 *** | 0.59 *** | 0.20 *** | - |
| 12. MOOD | 0.49 *** | −0.53 *** | −0.14 *** | −0.48 *** | 0.59 *** | −0.43 *** | −0.53 *** | 0.41 *** | 0.46 *** | 0.36 *** | 0.60 *** |
| Harassment–Social Acceptance | Model | R | R2 | Corrected R2 | Change statistics | Durbin–Watson | |||||||
| Standard error of estimation | Change in R2 | Change in F | Sig. of change in F | ||||||||||
| 1 | 0.53 | 0.28 | 0.28 | 0.43 | 0.28 | 699.41 | 0.000 | 1.93 | |||||
| 2 | 0.59 | 0.35 | 0.35 | 0.41 | 0.07 | 208.67 | 0.000 | ||||||
| 3 | 0.60 | 0.36 | 0.36 | 0.41 | 0.00 | 9.01 | 0.003 | ||||||
| 4 | 0.60 | 0.36 | 0.36 | 0.41 | 0.00 | 15.58 | 0.000 | ||||||
| 5 | 0.60 | 0.37 | 0.36 | 0.41 | 0.00 | 8.40 | 0.004 | ||||||
| Model 5 | Non-standardized coefficients | Standardized coefficients | t | Sig. | Collinearity | ||||||||
| B | Standard Error | Beta | Tol. | VIF | |||||||||
| (Constant) | 3.76 | 0.08 | 45.36 | 0.000 | |||||||||
| Mood | −0.35 | 0.02 | −0.42 | −16.23 | 0.000 | 0.52 | 1.89 | ||||||
| Stress management | −0.26 | 0.01 | −0.29 | −14.51 | 0.000 | 0.86 | 1.16 | ||||||
| Self-efficacy | −0.01 | 0.00 | −0.10 | −4.28 | 0.000 | 0.63 | 1.57 | ||||||
| Adaptability | 0.11 | 0.02 | 0.12 | 4.56 | 0.000 | 0.49 | 2.00 | ||||||
| Intrapersonal | −0.04 | 0.01 | −0.06 | −2.89 | 0.004 | 0.76 | 1.31 | ||||||
| Overload | Model | R | R2 | Corrected R2 | Change statistics | Durbin– Watson | |||||||
| Standard error of estimation | Change in R2 | Change in F | Sig. of change in F | ||||||||||
| 1 | 0.24 | 0.05 | 0.05 | 0.55 | 0.05 | 111.03 | 0.000 | 1.98 | |||||
| 2 | 0.25 | 0.06 | 0.06 | 0.55 | 0.00 | 11.83 | 0.001 | ||||||
| Model 2 | Non-standardized coefficients | Standardized coefficients | t | Sig. | Collinearity | ||||||||
| B | Standard Error | Beta | Tol. | VIF | |||||||||
| (Constant) | 3.37 | 0.08 | 39.22 | 0.000 | |||||||||
| Stress management | −0.23 | 0.02 | −0.23 | −10.16 | 0.000 | 0.99 | 1.01 | ||||||
| Intrapersonal | −0.06 | 0.01 | −0.07 | −3.44 | 0.001 | 0.99 | 1.01 | ||||||
| Irritability–Tension–Fatigue | Model | R | R2 | Corrected R2 | Change statistics | Durbin–Watson | |||||||
| Standard error of estimation | Change in R2 | Change in F | Sig. of change in F | ||||||||||
| 1 | 0.50 | 0.25 | 0.25 | 0.47 | 0.25 | 617.98 | 0.000 | 1.99 | |||||
| 2 | 0.60 | 0.36 | 0.36 | 0.43 | 0.10 | 293.32 | 0.000 | ||||||
| 3 | 0.60 | 0.36 | 0.36 | 0.43 | 0.00 | 11.31 | 0.001 | ||||||
| 4 | 0.61 | 0.37 | 0.37 | 0.43 | 0.00 | 14.73 | 0.000 | ||||||
| 5 | 0.61 | 0.37 | 0.37 | 0.43 | 0.00 | 8.64 | 0.003 | ||||||
| Model 5 | Non-standardized coefficients | Standardized coefficients | t | Sig. | Collinearity | ||||||||
| B | Standard Error | Beta | Tol. | VIF | |||||||||
| (Constant) | 4.17 | 0.09 | 45.46 | 0.000 | |||||||||
| Stress management | −0.36 | 0.01 | −0.38 | −18.97 | 0.000 | 0.86 | 1.16 | ||||||
| Mood | −0.29 | 0.02 | −0.32 | −13.07 | 0.000 | 0.57 | 1.72 | ||||||
| Self-Efficacy | −0.01 | 0.00 | −0.09 | −4.04 | 0.000 | 0.70 | 1.42 | ||||||
| Interpersonal | 0.10 | 0.02 | 0.09 | 4.41 | 0.000 | 0.69 | 1.43 | ||||||
| Intrapersonal | −0.05 | 0.01 | −0.06 | −2.94 | 0.003 | 0.77 | 1.29 | ||||||
| Energy–Joy | Model | R | R2 | Corrected R2 | Change statistics | Durbin–Watson | |||||||
| Standard error of estimation | Change in R2 | Change in F | Sig. of change in F | ||||||||||
| 1 | 0.59 | 0.35 | 0.35 | 0.48 | 0.35 | 972.00 | 0.000 | 1.94 | |||||
| 2 | 0.60 | 0.36 | 0.36 | 0.47 | 0.01 | 38.94 | 0.000 | ||||||
| 3 | 0.61 | 0.38 | 0.37 | 0.47 | 0.01 | 36.42 | 0.000 | ||||||
| 4 | 0.62 | 0.38 | 0.38 | 0.47 | 0.00 | 11.47 | 0.001 | ||||||
| 5 | 0.62 | 0.38 | 0.38 | 0.47 | 0.00 | 3.98 | 0.046 | ||||||
| Model 5 | Non-standardized coefficients | Standardized coefficients | t | Sig. | Collinearity | ||||||||
| B | Standard Error | Beta | Tol. | VIF | |||||||||
| (Constant) | 0.29 | 0.09 | 2.97 | 0.003 | |||||||||
| Mood | 0.44 | 0.02 | 0.44 | 18.31 | 0.000 | 0.57 | 1.72 | ||||||
| Stress management | 0.13 | 0.02 | 0.12 | 6.33 | 0.000 | 0.86 | 1.16 | ||||||
| Self-efficacy | 0.01 | 0.00 | 0.11 | 4.95 | 0.000 | 0.70 | 1.42 | ||||||
| Intrapersonal | 0.05 | 0.01 | 0.06 | 2.84 | 0.004 | 0.77 | 1.29 | ||||||
| Interpersonal | 0.05 | 0.02 | 0.04 | 1.99 | 0.046 | 0.69 | 1.43 | ||||||
| Fear–Anxiety | Model | R | R2 | Corrected R2 | Change statistics | Durbin–Watson | |||||||
| Standard error of estimation | Change in R2 | Change in F | Sig. of change in F | ||||||||||
| 1 | 0.43 | 0.19 | 0.19 | 0.63 | 0.19 | 418.20 | 0.000 | 1.97 | |||||
| 2 | 0.50 | 0.25 | 0.25 | 0.60 | 0.06 | 148.95 | 0.000 | ||||||
| 3 | 0.51 | 0.26 | 0.26 | 0.60 | 0.00 | 17.74 | 0.000 | ||||||
| 4 | 0.51 | 0.26 | 0.26 | 0.60 | 0.00 | 19.89 | 0.000 | ||||||
| 5 | 0.52 | 0.27 | 0.27 | 0.60 | 0.00 | 6.35 | 0.012 | ||||||
| Model 5 | Non-standardized coefficients | Standardized coefficients | t | Sig. | Collinearity | ||||||||
| B | Standard Error | Beta | Tol. | VIF | |||||||||
| (Constant) | 4.39 | 0.12 | 34.64 | 0.000 | |||||||||
| Mood | −0.35 | 0.03 | −0.30 | −11.55 | 0.000 | 0.57 | 1.72 | ||||||
| Stress management | −0.33 | 0.02 | −0.27 | −12.43 | 0.000 | 0.86 | 1.16 | ||||||
| Self-efficacy | −0.01 | 0.00 | −0.12 | −5.05 | 0.000 | 0.70 | 1.42 | ||||||
| Interpersonal | 0.16 | 0.03 | 0.12 | 4.92 | 0.000 | 0.69 | 1.43 | ||||||
| Intrapersonal | −0.05 | 0.02 | −0.05 | −2.52 | 0.012 | 0.77 | 1.29 | ||||||
| Self-Realization–Satisfaction | Model | R | R2 | Corrected R2 | Change statistics | Durbin–Watson | |||||||
| Standard error of estimation | Change in R2 | Change in F | Sig. of change in F | ||||||||||
| 1 | 0.53 | 0.28 | 0.28 | 0.47 | 0.28 | 719.94 | 0.000 | 1.91 | |||||
| 2 | 0.58 | 0.33 | 0.33 | 0.46 | 0.05 | 133.08 | 0.000 | ||||||
| 3 | 0.59 | 0.35 | 0.35 | 0.45 | 0.01 | 47.09 | 0.000 | ||||||
| Model 3 | Non-standardized coefficients | Standardized coefficients | t | Sig. | Collinearity | ||||||||
| B | Standard Error | Beta | Tol. | VIF | |||||||||
| (Constant) | 4.22 | 0.09 | 46.70 | 0.000 | |||||||||
| Mood | −0.35 | 0.02 | −0.37 | −16.26 | 0.000 | 0.68 | 1.47 | ||||||
| Stress management | −0.23 | 0.02 | −0.23 | −11.52 | 0.000 | 0.86 | 1.15 | ||||||
| Self-efficacy | −0.01 | 0.00 | −0.15 | −6.86 | 0.000 | 0.75 | 1.32 | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molero Jurado, M.d.M.; Pérez-Fuentes, M.d.C.; Oropesa Ruiz, N.F.; Simón Márquez, M.d.M.; Gázquez Linares, J.J. Self-Efficacy and Emotional Intelligence as Predictors of Perceived Stress in Nursing Professionals. Medicina 2019, 55, 237. https://doi.org/10.3390/medicina55060237
Molero Jurado MdM, Pérez-Fuentes MdC, Oropesa Ruiz NF, Simón Márquez MdM, Gázquez Linares JJ. Self-Efficacy and Emotional Intelligence as Predictors of Perceived Stress in Nursing Professionals. Medicina. 2019; 55(6):237. https://doi.org/10.3390/medicina55060237
Chicago/Turabian StyleMolero Jurado, María del Mar, María del Carmen Pérez-Fuentes, Nieves Fátima Oropesa Ruiz, María del Mar Simón Márquez, and José Jesús Gázquez Linares. 2019. "Self-Efficacy and Emotional Intelligence as Predictors of Perceived Stress in Nursing Professionals" Medicina 55, no. 6: 237. https://doi.org/10.3390/medicina55060237