Structural and Biomedical Properties of Common Additively Manufactured Biomaterials: A Concise Review


Department of Industrial and Mechanical Engineering, Norwegian University of Science and Technology, Richard Birkelands vei 2b, 7034 Trondheim, Norway
*
Author to whom correspondence should be addressed.
Metals 2020, 10(12), 1677; https://doi.org/10.3390/met10121677
Submission received: 31 October 2020
/
Revised: 30 November 2020
/
Accepted: 10 December 2020
/
Published: 15 December 2020
(This article belongs to the Special Issue Environmental Effects on the Fatigue Behavior of Conventionally and Additively Manufactured Metallic Materials)
Abstract
:Biomaterials are in high demand due to the increasing geriatric population and a high prevalence of cardiovascular and orthopedic disorders. The combination of additive manufacturing (AM) and biomaterials is promising, especially towards patient-specific applications. With AM, unique and complex structures can be manufactured. Furthermore, the direct link to computer-aided design and digital scans allows for a direct replicable product. However, the appropriate selection of biomaterials and corresponding AM methods can be challenging but is a key factor for success. This article provides a concise material selection guide for the AM biomedical field. After providing a general description of biomaterial classes—biotolerant, bioinert, bioactive, and biodegradable—we give an overview of common ceramic, polymeric, and metallic biomaterials that can be produced by AM and review their biomedical and mechanical properties. As the field of load-bearing metallic implants experiences rapid growth, we dedicate a large portion of this review to this field and portray interesting future research directions. This article provides a general overview of the field, but it also provides possibilities for deepening the knowledge in specific aspects as it comprises comprehensive tables including materials, applications, AM techniques, and references.
1. Introduction
Biomaterials play an integral role in medicine and can enhance the quality and longevity of human life. Biomaterials have been in use for at least 4000 years, and the first historical use dates back to antiquity when ancient Egyptians made sutures from animal sinew [1]. Today, millions of patients worldwide are being treated with biomaterial-based implantable products in the form of bone implants, joint replacement devices, stents, controlled drug delivery devices, pacemakers, surgical meshes, dental and cosmetic implants, dermal fillers, etc. The biomaterials market is in rapid growth due to the increasing geriatric population and a high prevalence of cardiovascular and orthopedic disorders. In 2019, the biomaterials market was worth $109 billion, and by 2026 it is estimated to reach $287 billion [2,3].
The combination of biomaterials with additive manufacturing (AM) is a new and promising avenue. AM has particular benefits at low production quantities and effective material usage [4]. By implementing AM, customized parts can be manufactured and conventional manufacturing constraints can be omitted, allowing the production of unique complex structures that cannot be manufactured otherwise. AM is also a useful technology for customized surgery tools, surgery education, and training. The direct link to computer-aided design proves to be important in the biomedical sector, where medical scan data can be utilized for direct production of tools and devices. This is already widely implemented in the dental industry, where AM is used to fabricate a series of custom-made clear aligners using digital impressions, which further allows the orthodontists to forecast treatment outcomes [5]. However, unlike conventional manufacturing methods, AM is not ideal for high-volume production since the unit cost of manufacturing is independent of the production volume. Taking this into account, AM of biomaterials should be aimed towards patient-specific applications.
The combination of AM and biomaterials is promising and will undoubtedly shape the field of biomedical engineering to come [6], especially regarding patient-specific clinical applications. This prospect has been taken up by a number of authors, indicated by the large number of AM biomaterial review articles published in the literature. For example, comprehensive overviews of AM for biomedical applications have been published by González-Henríquez et al. [7] with focus on polymers, Galante et al. give an overview of AM ceramics [8], and Trevisan et al. on titanium alloys [9]. Multiple authors have also compiled comprehensive details on the different AM techniques [10,11]. In contrast to these comprehensive review articles, this review article has a broader scope and puts biomaterial selection in the foreground before detailing respective AM processes and applications. A biomedical materials science researcher, or a clinical practitioner that is aware of the material and has specific needs, may embark in AM-related opportunities and get an overview of related research by reading this article. The purpose of this review article is, hence, to provide an overview of current biomaterials in view of their processability with AM and then give an overview of the fields that are currently heavily explored via this combination. We put a particular focus on biocompatible AM metals for load-bearing biomedical applications, for which we dedicate a large portion of this review. In what follows, we will classify the different types of biomaterials, give a short overview of relevant AM methods for the aforementioned materials, and sketch clinical applications that are of relevance and leverage from this combination.
2. Biomaterials and Their Classifications
Biomaterials are materials that interact with biological systems. They are either natural or synthetic, alive or lifeless, and are often used in medical applications to augment or replace a natural function. Biomaterials can be classified based on their level of biocompatibility as being bioactive, biodegradable, bioinert, and/or biotolerant.
A bioactive material in the bone tissue environment can create an environment compatible with osteogenesis by making chemical bonds with the bone tissue [12]. Bioactive materials can be divided into two classes: osteoconductive and osteoinductive materials [13]. Osteoconductive materials allow bone growth along the surface of the bioactive material. The ceramics hydroxyapatite and tricalcium phosphate are examples of such osteoconductive materials [14]. Osteoinductive materials can stimulate the growth of new bone. Some osteoinductive materials are also referred to as osteoproductive materials in that bone growth can be stimulated away from the implant site [15]. Bioactive glasses are examples of such osteoproductive materials [16]. When a bioactive material is implanted into the human body, it stimulates a biological response from the body, which leads to a series of biophysical and biochemical reactions between the implant and tissue that eventually lead to a mechanically strong chemical bonding [12].
Biotolerant materials are accepted by the host, but separated from the host tissue by the formation of a fibrous tissue (scar tissue). This fibrous tissue layer is induced by the release of ions, corrosion products, and chemical compounds from the implant [17]. Almost all synthetic polymers and most metals fall into this category.
Bioinert materials are stable in the human body and do not react with body fluids or tissues. Generally, bioinert materials are encapsulated by fibrous tissues to isolate them from the surrounding bone, similar to biotolerant materials. However, under certain conditions, bioinert materials can have direct structural and functional connection with the adjacent bone tissue without being separated from the host tissue [18]. Titanium and its alloys are examples of such bioinert materials.
Biodegradable materials are materials that dissolve in contact with body fluids. The dissolution products are usually secreted via the kidneys, without causing serious effects to the environment. Biodegradable materials are used for medical goods such as surgical sutures, tissues in growth materials, and controlled drug release [19,20]. The most common biodegradable materials are polymers such as polyglycolic and polylactic acids, and their co-polymers [21]. Examples of biodegradable ceramics are calcium phosphates [22], and magnesium is an example of a biodegradable metal [23]. In 2005, researchers Zartner et al. implanted a biodegradable 3 mm magnesium stent in a 6 week old preterm baby, born at week 26 of gestation [24].
Figure 1 illustrates the different biomaterial classifications. An example of a biotolerant material is illustrated in Figure 1a, where a fibrous layer is surrounding the screw. Figure 1b shows a bioinert material, where there is a direct contact between the bone tissue and the implant screw. A bioactive material is shown in Figure 1c, where the material has caused a chemical reaction between the implant screw and the bone tissue. Figure 1d illustrates a biodegradable material, where the material has degraded and the degradation products were released into the bone tissue.
3. Additive Manufacturing Techniques
Numerous AM techniques are available for medical and tissue engineering purposes. Some techniques involve the printing of live cells along with other materials, also known as bioprinting [25]. However, as this review focuses on biomaterials with a particular focus on metals for load-bearing applications, we will focus on the non-cellular fabrication techniques. These include the following:
- Powder bed fusion—The powder bed fusion (PBF) methods use either electron beam or laser to selectively consolidate material powder. These techniques are known as electron beam melting (EBM), selective laser melting (SLM), and selective laser sintering (SLS). SLM and EBM both fully melt and fuse the powder material, while SLS heats it to the point that the powder can fuse together on a molecular level. All PBF techniques involve spreading material powder over the previous layers.
- Binder jetting—The binder jetting technique is similar to the PBF technique in that it utilizes material powder that is spread over previous layers. However, unlike PBF, which melts and fuses the powder, this technique uses a binder as an adhesive for its consolidation in layers of defined cross-sections.
- Material extrusion—The material extrusion technique, also known as fused deposition modeling, pushes raw material in the form of polymer wires through a heated nozzle. The material is deposited as polymer roads that are arranged to define a cross-section of the part. These lines are then stacked in a layer-by-layer fashion.
- Material jetting—The material jetting technique uses a liquid photopolymer resin that is cured with ultraviolet (UV) or near-UV light. Similar to the material extrusion technique, the material is deposited from a nozzle which moves horizontally across the build platform. The material is then cured, defining a cross-section of the part. Individual cross-sections are consolidated in a layer-by-layer fashion as the building platform moves in the vertical direction.
- Vat polymerization—The vat polymerization technique is similar to the material jetting technique inasmuch as it employs photopolymer resins that are cured with UV light in a layer-by-layer fashion. In contrast to material jetting, the resin remains in a material vat, where the build platform is submerged. The build platform moves downwards (or upwards depending on the position of the light source) to create additional layers on top of the previous.
A more elaborate description of these techniques can be found in other reviews such as [10] or [26]. These techniques all have their pros and cons and can process different types of materials. With regards to biomaterials, we will further discriminate between ceramics, polymers, and metals. The following sections will discuss each material category, their biomedical applications, and AM fabrication methods.
4. Biocompatible Ceramics
Ceramics are nonmetallic and inorganic elements formed by ionic bonding and produced under a high-temperature process called firing. Ceramics that are used as biomaterials are called bioceramics, which have excellent biocompatibility, and are often used as implants within bones, joints, and teeth. Bioceramics can be categorized as either bioinert or bioactive, and bioactive ceramics may be degradable or non-degradable [27].
Bioinert ceramics have high chemical stability and high mechanical strength in vivo. In addition to being chemically inert, bioinert ceramics have a significantly lower coefficient of friction and wear rate than metals [28]. Hence, bioinert ceramics are often used for femoral heads of hip implants [29]. Examples of bioinert ceramics are aluminum oxide and zirconium oxide [30,31]. Aluminum oxide (Al2O3), also known as alumina, has high hardness, low friction, and excellent wear and corrosion resistance [32]. Due to these properties, alumina has been developed as an alternative to surgical metal alloys for orthopedic and dental applications [33]. Zirconium dioxide (ZrO2), also known as zirconia, is a white amorphous powder derived from zirconium. Because of its strength and high resistance to wear, it is often used for fixed partial dentures and other prosthetic devices [34]. Zirconia has also been used as a coating on titanium in dental implants [35]. Furthermore, zirconia implants have shown to accumulate less bacteria than commercially pure Ti implants in vivo [36].
Bioactive ceramics are integrated with bone tissues via chemical reactions that lead to the formation of hydroxycarbonate apatite without causing inflammation. The bond is usually stronger than the bone itself [28]. Bioactive ceramics include glasses, glass-ceramics, and other ceramics. Among them are bioglass and calcium phosphates (CPs) [27]. Some CPs are based on hydroxyapatite (HA) and tricalcium phosphate (TCP), which have been extensively studied as bone replacement materials [37]. HA(Ca10(PO4)6(OH)2) is a bioactive and non-degradable bioceramic with chemical and structural similarity to bone minerals [38].
The degradable bioactive ceramics are designed to gradually degrade in a predetermined time frame to assist as scaffolds or replace the host tissue. However, there are complications in maintaining the strength and stability throughout their lifetime due to the degradation of the material. In this manner, TCP (Ca3(PO4)2) has a chemical composition similar to bone tissue mineral and has a good resorbability and bioactivity with higher rates of biodegradation than HA under in vivo conditions [14].
Since ceramics are generally hard and brittle and have poor fatigue properties, they are less suitable for load-bearing applications. However, bioactive materials, such as HA and bioglass, are common materials to use as bioactive coatings on metallic implants for load-bearing applications [39,40]. Ceramic coatings on metal implants have three major benefits: they (1) enhance the formation of bone, (2) allow direct bonding with bone, and (3) reduce metal corrosion as well as related corrosion product release. Sometimes the corrosion rate is too high for the body to handle, and a ceramic coating can help reduce this rate to a tolerable level [41]. Common fabrication methods for bioceramics include electrophoretic deposition [42], plasma spraying [43], and dip coating [35]. Bioceramics with metallic core structures are also used as coatings for prosthesis [44].
AM can be a useful tool to produce customized dental restorations. The combination of digital scans and AM allow for a nearly identical replication of the patient model. Not only does the layer-by-layer approach reduce material consumption, but it also allows the construction of complex structures. Recently, lithium disilicate glass ceramic dental restorations have been manufactured using a stereolithography-based AM method, with outstanding mechanical properties of over 400 MPa flexural strength, excellent translucency and accuracy [45]. Researchers Mitteramskogler et al. utilized vat polymerization and modified a special digital light processing system to improve the geometrical accuracy of 45 vol% zirconia green parts [46]. Zirconia-toughened alumina ceramics have also been fabricated with excellent properties using vat polymerization [47].
As many ceramics express unique bioactive properties, AM of biocompatible ceramics is also a promising candidate for customized bone tissue engineering. Researchers Liu et al. manufactured HA porous scaffolds using vat polymerization [48]. The scaffolds demonstrated favorable in vitro biocompatibility for orthopedic applications. Researchers Schmidleithner et al. also used vat polymerization to manufacture TCP scaffolds for bone regeneration [49]. The scaffolds were manufactured with <2 vol% error in porosity and <6% relative deviation of average pore sizes. In addition, the cells cultured on the scaffolds had an increase in collagen deposition and alkaline phosphatase activity when compared to 2D tissue culture plastic. These results suggest that AM, particularly vat polymerization, is a promising manufacturing method to manufacture customized scaffold structures for bone tissue engineering.
Table 1 shows examples of bioceramics and AM methods, in addition to the characterization and examples of biomedical applications.
5. Biocompatible Polymers and Co-Polymers
Polymers have been widely studied for medical applications such as drug delivery and bone tissue engineering [67,68]. From a biomedical perspective, polymers and co-polymers can be divided into two classes: biodegradable and biotolerant. The role of polymeric implants for permanent load-bearing applications is rare [68]. However, since polymers are ideally tunable in their interaction with the biological environment, the degradable class is often studied for temporal devices [68]. Hence, the main focus in this section will be on biodegradable polymers and their fabrication with AM.
AM biodegradable polymers, both synthetic and natural, are used for fabricating controlled release drug delivery vehicles, temporary three-dimensional porous structures as scaffolds for tissue engineering, and temporary prostheses [69]. As the degradation is the main property to tune in these application, one has to be aware of the different degradation mechanisms at play. The degradation of polymers can be classified into hydrolytical and enzymatical degradation. Most natural polymers, such as chitosan, alginate, collagen, gelatin, cellulose, and fibrinogen, undergo enzymatic degradation, meaning that the polymeric material is degraded by the enzymes that are secreted by tissues, immune system, or microorganisms that are present in the biological environment [70]. The rate of enzymatic degradation varies significantly with the implantation site, depending on the availability and concentration of respective enzymes. Since natural polymers are mostly used as ’bioinks’ in bioprinting, and are hence generally connected to fabrication methods including the deposition of cells in the process, this report will focus mainly on hydrolytically degradable polymers.
Hydrolytically degradable polymers involves cleavage of hydrolytically sensitive bonds in the polymer, which finally leads to polymer erosion [71]. Erosion can be categorized as bulk or surface erosion, or a combination thereof. In surface erosion, the polymer degrades from the exterior surface, while the inside of the material does not degrade until all the surrounding material has been degraded. Bulk erosion is characterized by an equal degradation throughout the whole material. These erosion mechanisms are extremely important in determining which material is best for a desired application. Surface erosion is preferred for sustained drug delivery, and it can offer several benefits for bone tissue engineering, retention of mechanical integrity, enhanced bone ingrowth, and ensure that the scaffold implant is gradually replaced by bone tissue [72]. Examples of hydrolytically degradable polymers are poly(α-esters), such as poly(glycolic acid) (PGA), poly(lactic acid) (PLA), poly(lactide-co-glycolide acid) (PLGA), and polycaprolactone (PCL) [73]. PGA has a melting point greater than 200 °C, a glass transition temperature of 35–40 °C, and a high tensile modulus ( 12.8 GPa) [74]. Due to the rapid degradation and insolubility, PGA is usually used for short-term tissue engineering scaffolds and as sutures [75]. PLA comes in different optical isomers, the most used forms for biomedical research are poly(l-lactic acid) (PLLA) and poly (d,l-lactic acid) (PDLLA). The more crystalline PLLA has a melting point of 175 °C, glass transition temperature of 60–65 °C, and mechanical strength of 4.8 GPa [76]. PLLA has a very slow degradation and has been used as bone fixators [77]. To tune the degradation kinetics of PLLA, it is often combined with other forms of PLA, such as PDLLA that has a sterically different structure and, hence, different mechanical and degradation properties [78].
Mixed with glycolic acid, PLA forms the copolymer PLGA, which is already approved by the U.S. Food and Drug Administration (FDA), and is one of the most investigated degradable polymer for biomedical applications [79,80]. It has a rapid degradation compared to other polyesters and is, therefore, utilized extensively in drug delivery applications such as chemotherapeutics [81], vaccines [82], antibiotics [83], etc. In addition, PLGA demonstrates great cell adhesion and proliferation properties, making it an excellent choice for tissue engineering applications.
AM of polymeric and co-polymeric implants gives the flexibility to produce patient-specific customized implants and on-demand products. A large amount of research has gone into examining the possibilities of implementing AM to produce customized implants, as, for example, cardiovascular stents. These stents intend to keep arteries open and enable blood flow to the heart. Researchers Guerra et al. used material extrusion to manufacture stents using PCL/PLA composites [84]. They discovered that this printing process was highly suitable for producing composite stents with approximately 85–95% accuracy, medium levels of degradation rates, and good biocompatibility. Furthermore, researchers Jia et al. designed and fabricated self-expandable biodegradable vascular stents from PLA using material extrusion [85]. Another promising application is implantable biodegradable bone fixators. These have several advantages due to their ability to degrade once their function is fulfilled, omitting the need for a procedure to remove the fixator after recovery. This reduces costs and triggers enhanced bone healing compared to traditional plates and screws [86]. However, there are limitations with biodegradable polymers compared to conventional metallic bone fixators. There is a need to pre-drill holes for the biodegradable screws. Working around this issue is the subject of various research articles. For example, Yeon et al. [87] manufactured a PLA/HA/Silk composite bone clip using material extrusion, which they implanted in rat femur bone. The bone clip demonstrated excellent alignment of the bony segments making it a promising candidate for the internal bone fixation system. Furthermore, as this type of bone fixator is designed to be clipped around the bone, it can be installed without a drilled hole.
Another prospective clinical area lies in the field of tissue engineering with AM plastics and is related to mimicking the meniscus. Nearly half of knee arthroscopic procedures were performed for meniscal tears in the United States [88]. Researchers Zhang and Jiang et al. [89] utilized material extrusion to manufacture PCL scaffolds with three distinct mean pore sizes (pore sizes: 215, 320, and 515 μm). They did a total meniscectomy on several rabbits and replaced the meniscus with the PCL scaffolds. They discovered that the preferred mean pore size was 215 μm, showing increased fibrocartilaginous tissue formation and enhanced mechanical properties compared to the other pore sizes. There were no significant differences in degradation ratio between the different pore sizes.
Although the possibilities in biomedical research employing AM polymers seem endless, the clinical use of respective fabrics is predominantly confined to models for surgical planning, education, and training [90,91]. The largest adoption of AM polymers in the biomedical sector is connected to the manufacturing of custom in-ear hearing aids and dental aligners. AM polymers have found wide acceptance and spread in this field, where companies such as Sonova [92] and Align technology [5] lead the market in their respective segments. They use liquid photopolymers and vat polymerization to produce hundreds of thousands of parts with high precision since several years already [93]. Here, each part is uniquely customized from person-specific geometric data, and the printed part is either designed to use directly as is or to use as a mold for vacuum-forming FDA-approved polymers.
Table 2 shows a list of biopolymers, their characterization, AM methods, and the biomedical applications.
6. Biocompatible Metals
Metals are known for their high stiffness, wear resistance, ductility and thermal and electrical conductivity. Metallic materials are commonly used for orthopedic and orthodontic implants, bone fixators, artificial joints and external fixators, in addition to medical devices and related accessories. Due to their mechanical properties, metallic implants are difficult to replace by the more biocompatible ceramics and polymer substitutes. Most biocompatible metals are classified as biotolerant, the exception is titanium and its alloys, which are classified as bioinert. The most used biocompatible metals are titanium and its alloys, stainless steel, and cobalt chromium alloys [117,118]. So far, only powder bed fusion technologies are able to process these materials in medical grade.
Ti6Al4V is a common material for orthopedic implants due to its high strength-to-weight ratio and corrosion resistance, in addition to its unique biocompatibility [119]. In 1952, Per-Ingvar Brånemark accidentally discovered the osseointegration capability of using commercially pure Ti, where the living bone formed a direct structural and functional connection with the implant surface [120]. Ti6Al4V is classified as inert, meaning that the material can, in certain conditions, have direct contact with the adjacent bone tissue without introducing any chemical reactions between the implant and the host tissue. Once the material is implanted into the body, it passivates itself by the formation of an adhesive oxide layer. This oxide layer prevents an extensive flow of electrons and ions in the body fluid or surrounding tissue [121]. The vanadium in the alloy acts as beta-phase stabilizer, whereas the aluminum acts an alpha-phase condition stabilizer, which contributes to an increase in strength and decrease in weight.
Along with Ti6Al4V, stainless steel (SS) is a common material for biomedical implants and is a low-cost and readily available material. Out of the numerous grades of stainless steels, the 300 series is utilized in medical applications, usually the medical grades 304 and 316 L. SS does not offer the same biocompatibility as Ti6Al4V, and it is considered a biotolerant material. With surface treatments and coatings, it is possible to increase its biocompatibility and corrosion behavior. Because of its high strength and corrosion resistance, SS is often used in bone plates, screws, spinal fixation, hip and knee components, and medical devices [122].
Another class of biotolerant materials are cobalt chromium alloys. These alloys are most used under conditions of wear due to their high wear resistance [123]. Chromium forms an oxide layer on the surface of the alloy making it corrosion resistant in a biological surrounding. Cobalt ensures a continuous phase, which results in homogeneous properties and, hence, is suitable for bone implants [124].
Even though the metals do not express bioactive properties, the biocompatibility of the metals can be further enhanced by creating bio-inspired surfaces, as covered in a review article by Chaoming Xie [125].
AM metal implants for biomedical applications have been in use for several years. The most utilized area is for dental applications. Previously, ExOne’s dental systems used binder jetting to make gold copings to serve as substructures for crowns and bridges. In 2007 it was pulled from the market, most likely due to the increased price of gold [126]. While AM is a good choice for manufacturing such gold copings, the most researched area in the AM metallic dental field is related to dental implants with titanium alloys. Researchers Tunchel et al. did a 3 year follow-up clinical study to examine the survival rate of titanium dental implants [127]. Eighty-two patients and a total of 110 titanium dental implants were installed. The implants showed a survival rate of 94.5% and proved to be a potential option for the rehabilitation of single-tooth gaps.
Although AM metals have been clinically tested and widely used in the dental industry, AM can also open up new possibilities for long-lasting orthopedic implants for load-bearing applications. Section 7 addresses the possibilities and challenges with AM metallic load-bearing implants. Table 3 shows a list of examples of biocompatible metals, their characterization and applications, in addition to suitable AM methods for each material.
7. Load-Bearing Applications
Metals are generally used for load-bearing applications (LBAs) due to their superior mechanical properties, such as ductility, fatigue life, and strength. AM metal implants are, therefore, also the preferred choice for LBAs in the biomedical field.
While conventional, solid, metallic implants have been used in bone and dental applications for centuries, AM implants are relatively new on the market. Researchers Jardini et al. [147] successfully manufactured and implanted a customized titanium implant for a 22 year old male for the surgical reconstruction of a large cranial defect using AM technology. An upper cervical spine of a 12 year old was also successfully manufactured and implanted using AM with a titanium alloy powder by researchers Xu et al. [148]. Images taken 1 year later revealed evidence of successful osseointegration. Although both examples are not highly LBAs, there is still a lot of research done in the field related to AM for LBAs.
Today’s solid metallic implants face serious problems related to bone loss around the implantation site in LBAs. Even though successful osseointegration might have been achieved after implantation, aseptic loosening is still the main cause of all revisions for total hip replacements. A study from the period 1995–2011 in Scandinavia and Finland revealed that aseptic loosening is the cause of 47 of all revisions for total hip replacements [149]. This mode of failure is often caused by stress shielding, which is a condition where the adjacent bone is shielded from stress due to new loading conditions after implantation. Bone remodeling is triggered by mechanical loading [150]. Considering the differences in stiffness between human bone and most metallic implant materials, the implant is usually the main carrier of the load, eventually leading to bone loss of the stress shielded bone. Figure 2a shows a schematic representation of the loading conditions and bone loosening in a hip implant.
Ti6Al4V is the most favorable biocompatible metal for load-bearing applications due to its mechanical properties. Both Co-Cr-based alloys and SS express significantly higher density and stiffness than Ti-6Al-4V, making them less ideal for larger bone implants in load-bearing applications (Co-Cr-based alloys: 8.3–9.2 g −3, 204–240 GPa; 316L SS: 7.9 g −3, 210 GPa; Ti-6Al-4V: 4.4–4.5 g cm−3, 110 GPa) [151,152,153].
Although Ti6Al4V is one of the most favorable metals, this alloy has a disadvantage due to the addition of aluminum as an alloying element. Even though aluminum is important for the strength and fracture toughness of the alloy [154], it is known as a toxic element to the human body. Research suggests that aluminum can interfere with bone mineralization [155]. Despite this, Ti6Al4V has been shown to have a cytotoxicity comparable to pure titanium metal, which can be explained by the low amount of aluminum alloy element [156]. Nonetheless, a lot of research has gone into modifying titanium materials. Researchers Konvalov et al. used an electropulse treatment of commercially pure titanium alloy VT1-0, and they discovered that this enhances the fatigue life by 1.3 times [157]. Alternative alloys are also highly explored. The β-type titanium alloys have a lower Young’s modulus, which can prevent stress shielding. The biocompatible Ti-29Nb-13Ta-4.6Zr (TNTZ) alloy has been reported with a Young’s modulus value as low as 60 GPa, compared to that of Ti6Al4V of 110 GPa [158]. However, the TNTZ alloy is also reported to have poorer strength and fatigue properties compared to Ti-6Al-4V [159]. In order to improve the mechanical properties, TNTZ has been alloyed with additions of Fe, Si, and/or O [159]. Recently, a modified TNTZ-Si alloy has also been manufactured using EBM [160]. However, since Ti-6Al-4V is already a widely implemented alloy for AM and medical applications [126], this review will focus on this alloy. Moreover, by implementing AM it is possible to manufacture porous scaffold implants designed to tune the stiffness to match the ones of human bone.
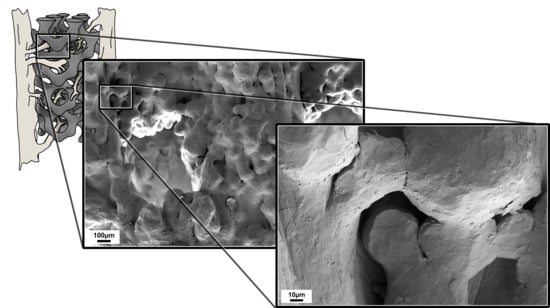
AM porous scaffold bone implants can be designed to mimic the stiffness of human bone [161]. This can pave the way towards a long-lasting bone implant. Moreover, the porous scaffold structure will likely yield better bone in-growth, resulting in a better osseointegration, as shown in Figure 2b. The products marketed for medical use have to be strictly tested to ensure that they are in accordance with the standards established by the specific rules for respective implants. The process of approving AM implants for use in LBA is complicated due to the changes of mechanical and biological properties connected to AM processing.
AM metallic parts have generally rough surfaces, as seen in Figure 3. This also results in a decreased fatigue life. The human femur bone is the largest, most voluminous, and strongest bone in the human body. It is responsible for bearing the largest percentage of the body weight, and it can support up to 30 times the weight of an adult [162]. In other words, a hip implant should express the same mechanical properties as the femur bone. Researchers Masuo et al. looked at surface roughness of electron beam melted (EBM) and selective laser melted (SLM) specimens, and they discovered that surface roughness had a strong detrimental influence on fatigue strength. Polished EBM and SLM samples express better fatigue properties compared to as-built samples, and post-processing with hot isostatic pressing further drastically improved fatigue strength [163]. Little difference in fatigue life was seen between as-built EBM and SLM specimens. Researchers Zhang et al. discovered that the low-cycle fatigue properties of SLM Ti-6Al-4V are comparable to wrought Ti-6Al-4V samples [164]. It has also been shown that the fatigue fracture always originates from the surface or subsurface defects [164]. More research is necessary to determine if AM porous scaffold implants can be used for a longer time in LBAs.
Another factor of importance related to the rough surface is the bone growth. As the surfaces of AM parts are rough, it is important to evaluate how these surfaces will impact the adhesion and bone growth of bone cells. Research performed by the authors suggests that the bone growth on rough additive manufactured surfaces is better compared to that grown on polished surfaces [166]. Figure 4 shows the bone matrix development after 21 days of culturing with bone marrow-derived human mesenchymal stem cells (Product no. PT-2501, Lot 0000318006, Lonza Inc, Walkersville, MD, USA) on EBM as-built samples compared to EBM polished samples. The bone matrix was sputtered with 4 nm platinum/palladium and can be seen as a dark grey color. The light grey color is the Ti-6Al-4V material. Here we see what appears as a thicker bone matrix for the as-built sample, with only a few partially melted particles appearing through the matrix, while there is only a thin matrix layer for the polished sample. With more adhesion sites on the rough as-built surface, it might suggest that the bone growth will be better for AM surfaces compared to polished surfaces.
Although the porous scaffold structures appear to be good for bone growth and stiffness reduction, there are still limitations related to the pore size of the scaffolds. Too small pore sizes might result in trapped metallic powder, which must be avoided. Figure 5 shows how the metallic powder is trapped inside a porous Ti-6Al-4V scaffold manufactured by EBM. This can be removed using post-processing, for example chemical etching [167,168].
8. Summary and Outlook
Additive manufacturing is a promising manufacturing method of biomaterials of various kinds when it comes to patient-specific applications. In recent years, research on the implantation of AM biomaterials into the human body has been actively pursued. Here the advantages of AM in low batch size production and customizable design are of tremendous benefit. In this article, we provided a concise state-of-the-art overview of implantable biomaterials and suitable AM technologies that is accessible to a broad readership. We have classified biomaterials defining the terms biocompatibility, bioactivity, biotolerance, bioinertness, and biodegradability. We give a short overview of AM fabrication methods relevant in the field and give a short overview of ceramics, polymers, and metals relevant to the field of biomedical applications. Here, biocompatible ceramics express great biocompatibility and are mostly used for applications related to bone tissue engineering. AM biocompatible polymers and copolymers are interesting, particularly due to their controllable degradation. The polymers and co-polymers can be found in either biotolerant, bioactive, or biodegradable classes, and they can be used in multiple applications, such as vascular, intravascular, controlled drug release, and bone tissue engineering applications. Finally, we review application methods for AM biocompatible metals, their fabrication methods, and their biocompatibility. Most metals fall under the biotolerant category. Titanium and its alloys can, however, in certain conditions be bioinert. Due to their strength and fatigue properties, most biocompatible metals are used in orthopedic applications, but they can also be used in vascular and dental applications. We particularly provide details on how metals, specifically titanium alloys, can be beneficial for load-bearing applications for long-term use, and how these can provide better bone in-growth. In this regard we also review interesting research directions worth exploring such as how surface modification can change both fatigue properties and cell proliferation.
Based on the rapid increase in research papers and clinical applications of porous metallic AM scaffolds, the authors expect this field to experience rapid growth and increasing popularity over the next years. By overcoming regulatory hurdles [126], the entire range of technologies (SLM in addition to EBM) and post-processing opportunities (e.g., surface modification of the porous scaffolds to enhance the fatigue life) may be applicable to clinical uses. However, critical issues such as the problem of trapped powder in complex porous architectures must be addressed to enable widespread acceptance. In addition, a proper method of predicting elastic moduli and fatigue properties by fabricated scaffold design will have high potential for further customization and utilization of the AM benefits. A scenario can be envisioned where more active patients with higher bone density may receive an implant with a higher stiffness as opposed to patients with lower bone density. Here the design can be adapted to the X-ray image of the bone around the site of implantation. With such possibilities, the full potential of AM can be unfolded lying in the direct conversion of computer generated architectures into physical devices. As seen for other fields with fully digital workflows enabled by AM (such as hearing aid shells), we could expect to see a transition to more clinical research with load-bearing applications.
By motivation of a digital workflow for customized implants, there are also many other possibilities related to implementing non-metallic AM devices in clinics, as, for example, the fabrication of personalized vascular stents. However, here the regulatory hurdles to overcome are even larger as the FDA currently limits the use of AM stents in clinics. The largest issue here is one that can be generalized for many AM biomaterials, namely the process and the material properties are interlinked. With this manufacturing process, the material properties evolve at the same time as the geometry, making these two aspects interlinked. From a regulatory perspective, this means that, although the material might still be FDA-approved, the combination of the AM process and the material might not, which creates many open challenges to be met before the approval of AM implantable medical devices that, once overcome, will potentially change the field of biomedical implants profoundly. Due to similar reasons, the clinical use of AM alternatives to bone fixators is limited, and the field of AM customized tissue engineering is even further away from clinical implementation; therefore, we expect an increase in efforts with regards to medical clearance for these respective materials and processes.
Author Contributions
All authors have contributed to this work. K.S.Ø.; writing, literature research, graphic design and microscopy imaging, J.T.; writing, review and editing, C.W.E.; review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
K.S.Ø. was funded by a scholarship of the Department of Mechanical and Industrial Engineering at NTNU.
Acknowledgments
The Research Council of Norway is acknowledged for the support to the Norwegian Micro- and Nano-Fabrication Facility, NorFab, project number 245963/F50. Glenn Buene is acknowledged for assisting with x-ray microtomography.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chellamani, K.P.; Veerasubramanian, D.; Balaji, R.V. Surgical sutures: An overview. J. Acad. Ind. Res. 2013, 1, 778–782. [Google Scholar]
- Markets, M.A. Biomaterials Market by Type of Materials (Metallic, Ceramic, Polymers, Natural) & By Application (Cardiovascular, Orthopedic, Dental, Plastic Surgery, Wound Healing, Neurological disorders, Tissue Engineering, Ophthalmology). In Global Forecast to 2024; Research and Markets: Dublin, Ireland, 2019. [Google Scholar]
- Consulting, A.R.A. Biomaterials Market Size, Share, Growth. In Scope|Forecast 2026; Acumen Research and Consulting: Maharashtra, India, 2019. [Google Scholar]
- Thomas, D.; Gilbert, S. Costs and Cost Effectiveness of Additive Manufacturing: A Literature Review and Discussion; NIST Special Publication: Gaithersburg, MD, USA, 2014; p. 96. [Google Scholar] [CrossRef]
- Kravitz, N.D.; Kusnoto, B.; BeGole, E.; Obrez, A.; Agran, B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Zadpoor, A.A.; Malda, J. Additive manufacturing of biomaterials, tissues, and organs. Ann. Biomed. Eng. 2017, 45, 1–11. [Google Scholar] [CrossRef] [PubMed]
- González-Henríquez, C.M.; Sarabia-Vallejos, M.A.; Rodriguez-Hernandez, J. Polymers for additive manufacturing and 4D-printing: Materials, methodologies, and biomedical applications. Prog. Polym. Sci. 2019, 94, 57–116. [Google Scholar] [CrossRef]
- Galante, R.; Figueiredo-Pina, C.G.; Serro, A.P. Additive manufacturing of ceramics for dental applications: A review. Dent. Mater. 2019, 35, 825–846. [Google Scholar] [CrossRef]
- Trevisan, F.; Calignano, F.; Aversa, A.; Marchese, G.; Lombardi, M.; Biamino, S.; Ugues, D.; Manfredi, D. Additive manufacturing of titanium alloys in the biomedical field: Processes, properties and applications. J. Appl. Biomater. Funct. Mater. 2018, 16, 57–67. [Google Scholar] [CrossRef]
- Ngo, T.D.; Kashani, A.; Imbalzano, G.; Nguyen, K.T.Q.; Hui, D. Additive manufacturing (3D printing): A review of materials, methods, applications and challenges. Compos. Part B Eng. 2018, 143, 172–196. [Google Scholar] [CrossRef]
- Abdulhameed, O.; Al-Ahmari, A.; Ameen, W.; Mian, S.H. Additive manufacturing: Challenges, trends, and applications. Adv. Mech. Eng. 2019, 11, 1687814018822880. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.; Courtney, J.M.; Qian, H. Bioactive Materials in Medicine: Design and Applications, 1st ed.; Woodhead Publishing: Cambridge, UK, 2011. [Google Scholar]
- Jones, J.R. Review of bioactive glass: From Hench to hybrids. Acta Biomater. 2013, 9, 4457–4486. [Google Scholar] [CrossRef]
- Rojbani, H.; Nyan, M.; Ohya, K.; Kasugai, S. Evaluation of the osteoconductivity of a-tricalcium phosphate, B-tricalcium phosphate, and hydroxyapatite combined with or without simvastatin in rat calvarial defect. J. Biomed. Mater. Res. Part A 2011, 98A, 488–498. [Google Scholar] [CrossRef]
- Tran, P.A.; Sarin, L.; Hurt, R.H.; Webster, T.J. Opportunities for nanotechnology-enabled bioactive bone implants. J. Mater. Chem. 2009, 19, 2653–2659. [Google Scholar] [CrossRef]
- Popa, A.C.; Stan, G.E.; Enculescu, M.; Tanase, C.; Tulyaganov, D.U.; Ferreira, J.M.F. Superior biofunctionality of dental implant fixtures uniformly coated with durable bioglass films by magnetron sputtering. J. Mech. Behav. Biomed. Mater. 2015, 51, 313–327. [Google Scholar] [CrossRef] [PubMed]
- Plenk, H., Jr. The Role of Materials Biocompatibility for Functional Electrical Stimulation Applications. Artif. Organs 2011, 35, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, C.P.; Stumpf, A. Biomaterials. In Dental Ceramics: Microstructure, Properties and Degradation; Topics in Mining, Metallurgy and Materials Engineering; Springer: Berlin/Heidelberg, Germany, 2013; pp. 9–13. [Google Scholar] [CrossRef]
- Tian, H.; Tang, Z.; Zhuang, X.; Chen, X.; Jing, X. Biodegradable synthetic polymers: Preparation, functionalization and biomedical application. Prog. Polym. Sci. 2012, 37, 237–280. [Google Scholar] [CrossRef]
- Prajapati, S.K.; Jain, A.; Jain, A.; Jain, S. Biodegradable polymers and constructs: A novel approach in drug delivery. Eur. Polym. J. 2019, 120, 109191. [Google Scholar] [CrossRef]
- Godavitarne, C.; Robertson, A.; Peters, J.; Rogers, B. Biodegradable materials. Orthop. Trauma 2017, 31, 316–320. [Google Scholar] [CrossRef]
- Xie, Y.; Chen, Y.; Sun, M.; Ping, Q. A mini review of biodegradable calcium phosphate nanoparticles for gene delivery. Curr. Pharm. Biotechnol. 2013, 14, 918–925. [Google Scholar] [CrossRef]
- Peron, M.; Berto, F.; Torgersen, J. Magnesium and Its Alloys as Implant Materials: Corrosion, Mechanical and Biological Performances; CRC Press: Boca Raton, FL, USA, 2020. [Google Scholar]
- Zartner, P.; Cesnjevar, R.; Singer, H.; Weyand, M. First successful implantation of a biodegradable metal stent into the left pulmonary artery of a preterm baby. Catheter. Cardiovasc. Interv. 2005, 66, 590–594. [Google Scholar] [CrossRef]
- Murphy, S.V.; Atala, A. 3D bioprinting of tissues and organs. Nat. Biotechnol. 2014, 32, 773–785. [Google Scholar] [CrossRef]
- Jasiuk, I.; Abueidda, D.W.; Kozuch, C.; Pang, S.; Su, F.Y.; McKittrick, J. An Overview on Additive Manufacturing of Polymers. JOM 2018, 70, 275–283. [Google Scholar] [CrossRef]
- Rahaman, M.N. Bioactive ceramics and glasses for tissue engineering. In Tissue Engineering Using Ceramics and Polymers (Second Edition); Boccaccini, A.R., Ma, P.X., Eds.; Woodhead Publishing: Cambridge, UK, 2014; pp. 67–114. [Google Scholar] [CrossRef]
- Farid, S.B. Bioceramics: For Materials Science and Engineering; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar] [CrossRef]
- Chevalier, J.; Gremillard, L. Ceramics for medical applications: A picture for the next 20 years. J. Eur. Ceram. Soc. 2009, 29, 1245–1255. [Google Scholar] [CrossRef]
- Wittenbrink, I.; Hausmann, A.; Schickle, K.; Lauria, I.; Davtalab, R.; Foss, M.; Keller, A.; Fischer, H. Low-aspect ratio nanopatterns on bioinert alumina influence the response and morphology of osteoblast-like cells. Biomaterials 2015, 62, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Bashir, M.; Riaz, S.; Kayani, Z.N.; Naseem, S. Effects of the organic additives on dental zirconia ceramics: Structural and mechanical properties. J. Sol. Gel. Sci. Technol. 2015, 74, 290–298. [Google Scholar] [CrossRef]
- Gonzalez, J.; Mireles, J.; Lin, Y.; Wicker, R. Characterization of ceramic components fabricated using binder jetting additive manufacturing technology. Ceram. Int. 2016, 42, 10559–10564. [Google Scholar] [CrossRef] [Green Version]
- Ferrage, L.; Bertrand, G.; Lenormand, P.; Grossin, D.; Ben-Nissan, B. A review of the additive manufacturing (3DP) of bioceramics: Alumina, zirconia (PSZ) and hydroxyapatite. J. Aust. Ceram. Soc. 2017, 53, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Gautam, C.; Joyner, J.; Gautam, A.; Rao, J.; Vajtai, R. Zirconia based dental ceramics: Structure, mechanical properties, biocompatibility and applications. Dalton Trans. 2016, 45, 19194–19215. [Google Scholar] [CrossRef]
- Sollazzo, V.; Pezzetti, F.; Scarano, A.; Piattelli, A.; Bignozzi, C.A.; Massari, L.; Brunelli, G.; Carinci, F. Zirconium oxide coating improves implant osseointegration in vivo. Dent. Mater. 2008, 24, 357–361. [Google Scholar] [CrossRef]
- Rimondini, L.; Cerroni, L.; Carrassi, A.; Torricelli, P. Bacterial colonization of zirconia ceramic surfaces: An in vitro and in vivo study. Int. J. Oral Maxillofac. Implant. 2002, 17, 793–798. [Google Scholar]
- Dutta, S.R.; Passi, D.; Singh, P.; Bhuibhar, A. Ceramic and non-ceramic hydroxyapatite as a bone graft material: A brief review. Ir. J. Med. Sci. 2015, 184, 101–106. [Google Scholar] [CrossRef]
- Fathi, M.H.; Hanifi, A.; Mortazavi, V. Preparation and bioactivity evaluation of bone-like hydroxyapatite nanopowder. J. Mater. Process. Technol. 2008, 202, 536–542. [Google Scholar] [CrossRef]
- Sola, A.; Bellucci, D.; Cannillo, V.; Cattini, A. Bioactive glass coatings: A review. Surf. Eng. 2011, 27, 560–572. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, S.; Zeng, X.; Ma, L.L.; Weng, W.; Yan, W.; Qian, M. Osteoblastic cell response on fluoridated hydroxyapatite coatings. Acta Biomater. 2007, 3, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Peron, M.; Bin Afif, A.; Dadlani, A.L.; Berto, F.; Torgersen, J. Improving stress corrosion cracking behavior of AZ31 alloy with conformal thin titania and zirconia coatings for biomedical applications. J. Mech. Behav. Biomed. Mater. 2020, 111, 104005. [Google Scholar] [CrossRef] [PubMed]
- Alzubaydi, T.L.; AlAmeer, S.S.; Ismaeel, T.; AlHijazi, A.Y.; Geetha, M. In vivo studies of the ceramic coated titanium alloy for enhanced osseointegration in dental applications. J. Mater. Sci. Mater. Med. 2008, 20, 35. [Google Scholar] [CrossRef]
- Pillai, R.S.; Frasnelli, M.; Sglavo, V.M. HA/B-TCP plasma sprayed coatings on Ti substrate for biomedical applications. Ceram. Int. 2018, 44, 1328–1333. [Google Scholar] [CrossRef]
- Epinette, J.A.; Manley, M.T. Fifteen Years of Clinical Experience with Hydroxyapatite Coatings in Joint Arthroplasty; Springer: Berlin/Heidelberg, Germany, 2013; Google-Books-ID: gdwFCAAAQBAJ. [Google Scholar]
- Baumgartner, S.; Gmeiner, R.; Schönherr, J.A.; Stampfl, J. Stereolithography-based additive manufacturing of lithium disilicate glass ceramic for dental applications. Mater. Sci. Eng. 2020, 116, 111180. [Google Scholar] [CrossRef]
- Mitteramskogler, G.; Gmeiner, R.; Felzmann, R.; Gruber, S.; Hofstetter, C.; Stampfl, J.; Ebert, J.; Wachter, W.; Laubersheimer, J. Light curing strategies for lithography-based additive manufacturing of customized ceramics. Addit. Manuf. 2014, 1, 110–118. [Google Scholar] [CrossRef]
- Wu, H.; Liu, W.; He, R.; Wu, Z.; Jiang, Q.; Song, X.; Chen, Y.; Cheng, L.; Wu, S. Fabrication of dense zirconia-toughened alumina ceramics through a stereolithography-based additive manufacturing. Ceram. Int. 2017, 43, 968–972. [Google Scholar] [CrossRef]
- Liu, Z.; Liang, H.; Shi, T.; Xie, D.; Chen, R.; Han, X.; Shen, L.; Wang, C.; Tian, Z. Additive manufacturing of hydroxyapatite bone scaffolds via digital light processing and in vitro compatibility. Ceram. Int. 2019, 45, 11079–11086. [Google Scholar] [CrossRef]
- Schmidleithner, C.; Malferarri, S.; Palgrave, R.; Bomze, D.; Schwentenwein, M.; Kalaskar, D.M. Application of high resolution DLP stereolithography for fabrication of tricalcium phosphate scaffolds for bone regeneration. Biomed. Mater. 2019, 14, 045018. [Google Scholar] [CrossRef]
- Gupta, A.; Tripathi, G.; Lahiri, D.; Balani, K. Compression Molded Ultra High Molecular Weight Polyethylene–Hydroxyapatite–Aluminum Oxide–Carbon Nanotube Hybrid Composites for Hard Tissue Replacement. J. Mater. Sci. Technol. 2013, 29, 514–522. [Google Scholar] [CrossRef]
- Zhou, M.; Liu, W.; Wu, H.; Song, X.; Chen, Y.; Cheng, L.; He, F.; Chen, S.; Wu, S. Preparation of a defect-free alumina cutting tool via additive manufacturing based on stereolithography – Optimization of the drying and debinding processes. Ceram. Int. 2016, 42, 11598–11602. [Google Scholar] [CrossRef]
- Chartier, T.; Chaput, C.; Doreau, F.; Loiseau, M. Stereolithography of structural complex ceramic parts. J. Mater. Sci. 2002, 37, 3141–3147. [Google Scholar] [CrossRef]
- Manicone, P.F.; Rossi Iommetti, P.; Raffaelli, L. An overview of zirconia ceramics: Basic properties and clinical applications. J. Dent. 2007, 35, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Shahzad, K.; Deckers, J.; Zhang, Z.; Kruth, J.P.; Vleugels, J. Additive manufacturing of zirconia parts by indirect selective laser sintering. J. Eur. Ceram. Soc. 2014, 34, 81–89. [Google Scholar] [CrossRef]
- Zhang, B.; Pei, X.; Song, P.; Sun, H.; Li, H.; Fan, Y.; Jiang, Q.; Zhou, C.; Zhang, X. Porous bioceramics produced by inkjet 3D printing: Effect of printing ink formulation on the ceramic macro and micro porous architectures control. Compos. Part B Eng. 2018, 155, 112–121. [Google Scholar] [CrossRef]
- Shuai, C.; Gao, C.; Nie, Y.; Hu, H.; Zhou, Y.; Peng, S. Structure and properties of nano-hydroxypatite scaffolds for bone tissue engineering with a selective laser sintering system. Nanotechnology 2011, 22, 285703. [Google Scholar] [CrossRef]
- Miranda, P.; Pajares, A.; Saiz, E.; Tomsia, A.P.; Guiberteau, F. Fracture modes under uniaxial compression in hydroxyapatite scaffolds fabricated by robocasting. J. Biomed. Mater. Res. Part A 2007, 83, 646–655. [Google Scholar] [CrossRef]
- Gao, Y.; Cao, W.L.; Wang, X.Y.; Gong, Y.D.; Tian, J.M.; Zhao, N.M.; Zhang, X.F. Characterization and osteoblast-like cell compatibility of porous scaffolds: Bovine hydroxyapatite and novel hydroxyapatite artificial bone. J. Mater. Sci. Mater. Med. 2006, 17, 815–823. [Google Scholar] [CrossRef]
- Warnke, P.H.; Seitz, H.; Warnke, F.; Becker, S.T.; Sivananthan, S.; Sherry, E.; Liu, Q.; Wiltfang, J.; Douglas, T. Ceramic scaffolds produced by computer-assisted 3D printing and sintering: Characterization and biocompatibility investigations. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 93, 212–217. [Google Scholar] [CrossRef]
- Gmeiner, R.; Deisinger, U.; Schonherr, J.; Lechner, B.; Detsch, R.; Boccaccini, A.; Stampfl, J. Additive manufacturing of bioactive glasses and silicate bioceramics. J. Ceram. Sci. Technol. 2015, 6, 75–86. [Google Scholar] [CrossRef]
- Shuai, C.; Mao, Z.; Han, Z.; Peng, S.; Li, Z. Fabrication and characterization of calcium silicate scaffolds for tissue engineering. J. Mech. Med. Biol. 2014, 14, 1450049. [Google Scholar] [CrossRef]
- Vorndran, E.; Klarner, M.; Klammert, U.; Grover, L.M.; Patel, S.; Barralet, J.E.; Gbureck, U. 3D Powder Printing of Beta-Tricalcium Phosphate Ceramics Using Different Strategies. Adv. Eng. Mater. 2008, 10, B67–B71. [Google Scholar] [CrossRef]
- Felzmann, R.; Gruber, S.; Mitteramskogler, G.; Tesavibul, P.; Boccaccini, A.R.; Liska, R.; Stampfl, J. Lithography-Based Additive Manufacturing of Cellular Ceramic Structures. Adv. Eng. Mater. 2012, 14, 1052–1058. [Google Scholar] [CrossRef]
- Bian, W.; Li, D.; Lian, Q.; Zhang, W.; Zhu, L.; Li, X.; Jin, Z. Design and fabrication of a novel porous implant with pre-set channels based on ceramic stereolithography for vascular implantation. Biofabrication 2011, 3, 034103. [Google Scholar] [CrossRef]
- Bose, S.; Darsell, J.; Kintner, M.; Hosick, H.; Bandyopadhyay, A. Pore size and pore volume effects on alumina and TCP ceramic scaffolds. Mater. Sci. Eng. 2003, 23, 479–486. [Google Scholar] [CrossRef]
- Butscher, A.; Bohner, M.; Roth, C.; Ernstberger, A.; Heuberger, R.; Doebelin, N.; von Rohr, P.R.; Müller, R. Printability of calcium phosphate powders for three-dimensional printing of tissue engineering scaffolds. Acta Biomater. 2012, 8, 373–385. [Google Scholar] [CrossRef]
- Liechty, W.B.; Kryscio, D.R.; Slaughter, B.V.; Peppas, N.A. Polymers for Drug Delivery Systems. Annu. Rev. Chem. Biomol. Eng. 2010, 1, 149–173. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Ma, P.X. Polymeric Scaffolds for Bone Tissue Engineering. Ann. Biomed. Eng. 2004, 32, 477–486. [Google Scholar] [CrossRef]
- Nair, L.S.; Laurencin, C.T. Biodegradable polymers as biomaterials. Prog. Polym. Sci. 2007, 32, 762–798. [Google Scholar] [CrossRef]
- Banerjee, A.; Chatterjee, K.; Madras, G. Enzymatic degradation of polymers: A brief review. Mater. Sci. Technol. 2014, 30, 567–573. [Google Scholar] [CrossRef]
- Rey-Vinolas, S.; Engel, E.; Mateos-Timoneda, M. Polymers for bone repair. In Bone Repair Biomaterials (Second Edition); Pawelec, K.M., Planell, J.A., Eds.; Woodhead Publishing Series in Biomaterials; Woodhead Publishing: Cambridge, UK, 2019; pp. 179–197. [Google Scholar] [CrossRef]
- Rezwan, K.; Chen, Q.Z.; Blaker, J.J.; Boccaccini, A.R. Biodegradable and bioactive porous polymer/inorganic composite scaffolds for bone tissue engineering. Biomaterials 2006, 27, 3413–3431. [Google Scholar] [CrossRef] [PubMed]
- Ulery, B.D.; Nair, L.S.; Laurencin, C.T. Biomedical Applications of Biodegradable Polymers. J. Polym. Sci. Part B Polym. Phys. 2011, 49, 832–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maurus, P.B.; Kaeding, C.C. Bioabsorbable implant material review. Oper. Tech. Sport. Med. 2004, 12, 158–160. [Google Scholar] [CrossRef]
- Budak, K.; Sogut, O.; Aydemir Sezer, U. A review on synthesis and biomedical applications of polyglycolic acid. J. Polym. Res. 2020, 27, 208. [Google Scholar] [CrossRef]
- Middleton, J.C.; Tipton, A.J. Synthetic biodegradable polymers as orthopedic devices. Biomaterials 2000, 21, 2335–2346. [Google Scholar] [CrossRef]
- Ueda, H.; Tabata, Y. Polyhydroxyalkanonate derivatives in current clinical applications and trials. Adv. Drug Deliv. Rev. 2003, 55, 501–518. [Google Scholar] [CrossRef]
- Yu, B.; Cao, Y.; Sun, H.; Han, J. The Structure and Properties of Biodegradable PLLA/PDLA for Melt-Blown Nonwovens. J. Polym. Environ. 2017, 25, 510–517. [Google Scholar] [CrossRef]
- Gentile, P.; Chiono, V.; Carmagnola, I.; Hatton, P.V. An Overview of Poly(lactic-co-glycolic) Acid (PLGA)-Based Biomaterials for Bone Tissue Engineering. Int. J. Mol. Sci. 2014, 15, 3640–3659. [Google Scholar] [CrossRef]
- Elmowafy, E.M.; Tiboni, M.; Soliman, M.E. Biocompatibility, biodegradation and biomedical applications of poly(lactic acid)/poly(lactic-co-glycolic acid) micro and nanoparticles. J. Pharm. Investig. 2019, 49, 347–380. [Google Scholar] [CrossRef]
- Betancourt, T.; Brown, B.; Brannon-Peppas, L. Doxorubicin-loaded PLGA nanoparticles by nanoprecipitation: Preparation, characterization and in vitro evaluation. Nanomedicine 2007, 2, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.; Gupta, V.; Ahsan, F. Particle size influences the immune response produced by hepatitis B vaccine formulated in inhalable particles. Pharm. Res. 2010, 27, 905–919. [Google Scholar] [CrossRef] [PubMed]
- Jhunjhunwala, S.; Raimondi, G.; Thomson, A.W.; Little, S.R. Delivery of rapamycin to dendritic cells using degradable microparticles. J. Control. Release Off. J. Control. Release Soc. 2009, 133, 191–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, A.J.; Cano, P.; Rabionet, M.; Puig, T.; Ciurana, J. 3D-Printed PCL/PLA Composite Stents: Towards a New Solution to Cardiovascular Problems. Materials 2018, 11, 1679. [Google Scholar] [CrossRef] [Green Version]
- Jia, H.; Gu, S.Y.; Chang, K. 3D printed self-expandable vascular stents from biodegradable shape memory polymer. Adv. Polym. Technol. 2018, 37, 3222–3228. [Google Scholar] [CrossRef]
- Brennan Fournet, M.E.; Azaman, F.A.; Gunbay, S.; Chen, Y.Y.; Devine, D.M. Orthopaedic 3D Printing in Orthopaedic Medicine. In Polymer-Based Additive Manufacturing: Biomedical Applications; Devine, D.M., Ed.; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 121–142. [Google Scholar] [CrossRef]
- Yeon, Y.K.; Park, H.S.; Lee, J.M.; Lee, J.S.; Lee, Y.J.; Sultan, M.T.; Seo, Y.B.; Lee, O.J.; Kim, S.H.; Park, C.H. New concept of 3D printed bone clip (polylactic acid/hydroxyapatite/silk composite) for internal fixation of bone fractures. J. Biomater. Sci. Polym. Ed. 2018, 29, 894–906. [Google Scholar] [CrossRef]
- Kim, S.; Bosque, J.; Meehan, J.P.; Jamali, A.; Marder, R. Increase in Outpatient Knee Arthroscopy in the United States: A Comparison of National Surveys of Ambulatory Surgery, 1996 and 2006. JBJS 2011, 93, 994–1000. [Google Scholar] [CrossRef]
- Zhang, Z.Z.; Jiang, D.; Ding, J.X.; Wang, S.J.; Zhang, L.; Zhang, J.Y.; Qi, Y.S.; Chen, X.S.; Yu, J.K. Role of scaffold mean pore size in meniscus regeneration. Acta Biomater. 2016, 43, 314–326. [Google Scholar] [CrossRef]
- Haleem, A.; Javaid, M.; Saxena, A. Additive manufacturing applications in cardiology: A review. Egypt. Heart J. 2018, 70, 433–441. [Google Scholar] [CrossRef]
- Tejo-Otero, A.; Buj-Corral, I.; Fenollosa-Artés, F. 3D Printing in Medicine for Preoperative Surgical Planning: A Review. Ann. Biomed. Eng. 2020, 48, 536–555. [Google Scholar] [CrossRef]
- Snova. 3D Printing Technology for Improved Hearing; Sonova International: Stäfa, Switzerland; Available online: https://www.sonova.com/en/story/innovation/3d-printing-technology-improved-hearing (accessed on 31 October 2020).
- Gibson, I.; Rosen, D.; Stucker, B. Design for Additive Manufacturing. In Additive Manufacturing Technologies: 3D Printing, Rapid Prototyping, and Direct Digital Manufacturing; Gibson, I., Rosen, D., Stucker, B., Eds.; Springer: New York, NY, USA, 2015; pp. 399–435. [Google Scholar] [CrossRef]
- Vert, M. Polymeric biomaterials: Strategies of the past vs. strategies of the future. Prog. Polym. Sci. 2007, 32, 755–761. [Google Scholar] [CrossRef]
- Bai, J.; Zhang, B.; Song, J.; Bi, G.; Wang, P.; Wei, J. The effect of processing conditions on the mechanical properties of polyethylene produced by selective laser sintering. Polym. Test. 2016, 52, 89–93. [Google Scholar] [CrossRef]
- Salmoria, G.V.; Ahrens, C.H.; Klauss, P.; Paggi, R.A.; Oliveira, R.G.; Lago, A. Rapid manufacturing of polyethylene parts with controlled pore size gradients using selective laser sintering. Mater. Res. 2007, 10, 211–214. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Ramakrishna, S.; Bouten, C.V.C.; Narayan, R. Biomedical applications of additive manufacturing: Present and future. Curr. Opin. Biomed. Eng. 2017, 2, 105–115. [Google Scholar] [CrossRef]
- Kim, J.; Creasy, T.S. Selective laser sintering characteristics of nylon 6/clay-reinforced nanocomposite. Polym. Test. 2004, 23, 629–636. [Google Scholar] [CrossRef]
- Pruitt, L.; Furmanski, J. Polymeric biomaterials for load-bearing medical devices. JOM 2009, 61, 14–20. [Google Scholar] [CrossRef]
- Gibson, I.; Rosen, D.; Stucker, B. Vat Photopolymerization Processes. In Additive Manufacturing Technologies: 3D Printing, Rapid Prototyping, and Direct Digital Manufacturing; Springer: New York, NY, USA, 2015; pp. 63–106. [Google Scholar] [CrossRef]
- Velu, R.; Singamneni, S. Evaluation of the influences of process parameters while selective laser sintering PMMA powders. Proc. Inst. Mech. Eng. Part C J. Mech. Eng. Sci. 2015, 229, 603–613. [Google Scholar] [CrossRef]
- Choi, J.; Wicker, R.B.; Quintana, R. Fabrication and characterization of embedded horizontal micro-channels using line-scan stereolithography. Rapid Prototyp. J. 2011, 17, 351–361. [Google Scholar] [CrossRef] [Green Version]
- Ramakrishna, S.; Mayer, J.; Wintermantel, E.; Leong, K.W. Biomedical applications of polymer-composite materials: A review. Compos. Sci. Technol. 2001, 61, 1189–1224. [Google Scholar] [CrossRef]
- Kurtz, S.M. An Overview of PEEK Biomaterials. In PEEK Biomaterials Handbook; Kurtz, S.M., Ed.; Plastics Design Library, William Andrew Publishing: Oxford, UK, 2012; pp. 1–7. [Google Scholar] [CrossRef]
- Schmidt, M.; Pohle, D.; Rechtenwald, T. Selective Laser Sintering of PEEK. CIRP Ann. 2007, 56, 205–208. [Google Scholar] [CrossRef]
- Chen, Q.; Liang, S.; Thouas, G.A. Elastomeric biomaterials for tissue engineering. Prog. Polym. Sci. 2013, 38, 584–671. [Google Scholar] [CrossRef]
- Guelcher, S.A. Biodegradable Polyurethanes: Synthesis and Applications in Regenerative Medicine. Tissue Eng. Part Rev. 2008, 14, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Partee, B.; Hollister, S.J.; Das, S. Selective Laser Sintering Process Optimization for Layered Manufacturing of CAPA® 6501 Polycaprolactone Bone Tissue Engineering Scaffolds. J. Manuf. Sci. Eng. 2005, 128, 531–540. [Google Scholar] [CrossRef]
- Chen, C.H.; Lee, M.Y.; Shyu, V.B.H.; Chen, Y.C.; Chen, C.T.; Chen, J.P. Surface modification of polycaprolactone scaffolds fabricated via selective laser sintering for cartilage tissue engineering. Mater. Sci. Eng. 2014, 40, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Shor, L.; Güçeri, S.; Chang, R.; Gordon, J.; Kang, Q.; Hartsock, L.; An, Y.; Sun, W. Precision extruding deposition (PED) fabrication of polycaprolactone (PCL) scaffolds for bone tissue engineering. Biofabrication 2009, 1, 015003. [Google Scholar] [CrossRef] [Green Version]
- Sobral, J.M.; Caridade, S.G.; Sousa, R.A.; Mano, J.F.; Reis, R.L. Three-dimensional plotted scaffolds with controlled pore size gradients: Effect of scaffold geometry on mechanical performance and cell seeding efficiency. Acta Biomater. 2011, 7, 1009–1018. [Google Scholar] [CrossRef] [Green Version]
- Korpela, J.; Kokkari, A.; Korhonen, H.; Malin, M.; Närhi, T.; Seppälä, J. Biodegradable and bioactive porous scaffold structures prepared using fused deposition modeling. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101B, 610–619. [Google Scholar] [CrossRef]
- Ge, Z.; Wang, L.; Heng, B.C.; Tian, X.F.; Lu, K.; Tai Weng Fan, V.; Yeo, J.F.; Cao, T.; Tan, E. Proliferation and Differentiation of Human Osteoblasts within 3D printed Poly-Lactic-co-Glycolic Acid Scaffolds. J. Biomater. Appl. 2009, 23, 533–547. [Google Scholar] [CrossRef]
- Lee, M.; Wu, B.M.; Dunn, J.C.Y. Effect of scaffold architecture and pore size on smooth muscle cell growth. J. Biomed. Mater. Res. Part A 2008, 87, 1010–1016. [Google Scholar] [CrossRef]
- Lee, M.; Dunn, J.C.Y.; Wu, B.M. Scaffold fabrication by indirect three-dimensional printing. Biomaterials 2005, 26, 4281–4289. [Google Scholar] [CrossRef]
- Guo, T.; Holzberg, T.R.; Lim, C.G.; Gao, F.; Gargava, A.; Trachtenberg, J.E.; Mikos, A.G.; Fisher, J.P. 3D printing PLGA: A quantitative examination of the effects of polymer composition and printing parameters on print resolution. Biofabrication 2017, 9, 024101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manam, N.S.; Harun, W.S.W.; Shri, D.N.A.; Ghani, S.A.C.; Kurniawan, T.; Ismail, M.H.; Ibrahim, M.H.I. Study of corrosion in biocompatible metals for implants: A review. J. Alloys Compd. 2017, 701, 698–715. [Google Scholar] [CrossRef] [Green Version]
- DebRoy, T.; Wei, H.L.; Zuback, J.S.; Mukherjee, T.; Elmer, J.W.; Milewski, J.O.; Beese, A.M.; Wilson-Heid, A.; De, A.; Zhang, W. Additive manufacturing of metallic components—Process, structure and properties. Prog. Mater. Sci. 2018, 92, 112–224. [Google Scholar] [CrossRef]
- Venkatesh, B.D.; Chen, D.L.; Bhole, S.D. Effect of heat treatment on mechanical properties of Ti–6Al–4V ELI alloy. Mater. Sci. Eng. 2009, 506, 117–124. [Google Scholar] [CrossRef]
- Brånemark, P.I.; Zarb, G.A.G.A.; Albrektsson, T. Tissue-Integrated Prostheses: Osseointegration in Clinical Dentistry; Quintessence Publishing: Chicago, IL, USA, 1985. [Google Scholar]
- Biehl, V.; Breme, J. Metallic Biomaterials. Mater. Und Werkst. 2001, 32, 137–141. [Google Scholar] [CrossRef]
- Desai, S.; Bidanda, B.; Bártolo, P. Metallic and Ceramic Biomaterials: Current and Future Developments. In Bio-Materials and Prototyping Applications in Medicine; Bártolo, P., Bidanda, B., Eds.; Springer: Boston, MA, USA, 2008; pp. 1–14. [Google Scholar] [CrossRef]
- Hanawa, T. Evaluation techniques of metallic biomaterials in vitro. Sci. Technol. Adv. Mater. 2002, 3, 289–295. [Google Scholar] [CrossRef]
- Saini, M.; Singh, Y.; Arora, P.; Arora, V.; Jain, K. Implant biomaterials: A comprehensive review. World J. Clin. Cases WJCC 2015, 3, 52–57. [Google Scholar] [CrossRef]
- Xie, C. Bio-inspired nanofunctionalisation of biomaterial surfaces: A review. Biosurface Biotribology 2019, 5, 83–92. [Google Scholar] [CrossRef]
- Wohlers, T.; Campbell, I.; Diegel, O.; Kowen, J.; Huff, R. Wohlers Report 2019—3D Printing and Additive Manufacturing State of the Industry Annual Worldwide Progress Report; Wohlers Associates, Inc.: Fort Collins, CO, USA, 2019. [Google Scholar]
- Tunchel, S.; Blay, A.; Kolerman, R.; Mijiritsky, E.; Shibli, J.A. 3D Printing/Additive Manufacturing Single Titanium Dental Implants: A Prospective Multicenter Study with 3 Years of Follow-Up. Int. J. Dent. 2016, 2016, 9. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.; Dickens, P. Selective laser melting (SLM) of pure gold for manufacturing dental crowns. Rapid Prototyp. J. 2014, 20, 471–479. [Google Scholar] [CrossRef]
- Murr, L.E.; Gaytan, S.M.; Martinez, E.; Medina, F.; Wicker, R.B. Next Generation Orthopaedic Implants by Additive Manufacturing Using Electron Beam Melting. Int. J. Biomater. 2012. [Google Scholar] [CrossRef] [PubMed]
- Niinomi, M. Recent metallic materials for biomedical applications. Metall. Mater. Trans. 2002, 33, 477. [Google Scholar] [CrossRef]
- Koutsoukis, T.; Zinelis, S.; Eliades, G.; Al-Wazzan, K.; Rifaiy, M.A.; Jabbari, Y.S.A. Selective Laser Melting Technique of Co-Cr Dental Alloys: A Review of Structure and Properties and Comparative Analysis with Other Available Techniques. J. Prosthodont. 2015, 24, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Hermawan, H.; Ramdan, D.; Djuansjah, J.R.P. Metals for Biomedical Applications. Biomed. Eng. Theory Appl. 2011. [Google Scholar] [CrossRef] [Green Version]
- Dewidar, M.M.; Khalil, K.A.; Lim, J.K. Processing and mechanical properties of porous 316L stainless steel for biomedical applications. Trans. Nonferrous Met. Soc. China 2007, 17, 468–473. [Google Scholar] [CrossRef]
- Gong, H.; Snelling, D.; Kardel, K.; Carrano, A. Comparison of Stainless Steel 316L Parts Made by FDM- and SLM-Based Additive Manufacturing Processes. JOM 2019, 71, 880–885. [Google Scholar] [CrossRef]
- Wang, C.; Tan, X.; Liu, E.; Tor, S.B. Process parameter optimization and mechanical properties for additively manufactured stainless steel 316L parts by selective electron beam melting. Mater. Des. 2018, 147, 157–166. [Google Scholar] [CrossRef]
- Lodhi, M.J.K.; Deen, K.M.; Greenlee-Wacker, M.C.; Haider, W. Additively manufactured 316L stainless steel with improved corrosion resistance and biological response for biomedical applications. Addit. Manuf. 2019, 27, 8–19. [Google Scholar] [CrossRef]
- Tang, H.P.; Yang, G.Y.; Jia, W.P.; He, W.W.; Lu, S.L.; Qian, M. Additive manufacturing of a high niobium-containing titanium aluminide alloy by selective electron beam melting. Mater. Sci. Eng. 2015, 636, 103–107. [Google Scholar] [CrossRef]
- Terrazas, C.A.; Mireles, J.; Gaytan, S.M.; Morton, P.A.; Hinojos, A.; Frigola, P.; Wicker, R.B. Fabrication and characterization of high-purity niobium using electron beam melting additive manufacturing technology. Int. J. Adv. Manuf. Technol. 2016, 84, 1115–1126. [Google Scholar] [CrossRef]
- Ramírez, G.; Rodil, S.E.; Arzate, H.; Muhl, S.; Olaya, J.J. Niobium based coatings for dental implants. Appl. Surf. Sci. 2011, 257, 2555–2559. [Google Scholar] [CrossRef]
- Wauthle, R.; van der Stok, J.; Amin Yavari, S.; Van Humbeeck, J.; Kruth, J.P.; Zadpoor, A.A.; Weinans, H.; Mulier, M.; Schrooten, J. Additively manufactured porous tantalum implants. Acta Biomater. 2015, 14, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.P.; Yang, K.; Jia, L.; He, W.W.; Yang, L.; Zhang, X.Z. Tantalum Bone Implants Printed by Selective Electron Beam Manufacturing (SEBM) and Their Clinical Applications. JOM 2020, 72, 1016–1021. [Google Scholar] [CrossRef]
- Wauthle, R.; Ahmadi, S.M.; Amin Yavari, S.; Mulier, M.; Zadpoor, A.A.; Weinans, H.; Van Humbeeck, J.; Kruth, J.P.; Schrooten, J. Revival of pure titanium for dynamically loaded porous implants using additive manufacturing. Mater. Sci. Eng. 2015, 54, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Rack, H.J.; Qazi, J.I. Titanium alloys for biomedical applications. Mater. Sci. Eng. 2006, 26, 1269–1277. [Google Scholar] [CrossRef]
- Yamanaka, K.; Saito, W.; Mori, M.; Matsumoto, H.; Sato, S.; Chiba, A. Abnormal grain growth in commercially pure titanium during additive manufacturing with electron beam melting. Materialia 2019, 6, 100281. [Google Scholar] [CrossRef]
- Ataee, A.; Li, Y.; Fraser, D.; Song, G.; Wen, C. Anisotropic Ti-6Al-4V gyroid scaffolds manufactured by electron beam melting (EBM) for bone implant applications. Mater. Des. 2018, 137, 345–354. [Google Scholar] [CrossRef]
- Liang, H.; Yang, Y.; Xie, D.; Li, L.; Mao, N.; Wang, C.; Tian, Z.; Jiang, Q.; Shen, L. Trabecular-like Ti-6Al-4V scaffolds for orthopedic: Fabrication by selective laser melting and in vitro biocompatibility. J. Mater. Sci. Technol. 2019, 35, 1284–1297. [Google Scholar] [CrossRef]
- Jardini, A.L.; Larosa, M.A.; Filho, R.M.; Zavaglia, C.A.D.C.; Bernardes, L.F.; Lambert, C.S.; Calderoni, D.R.; Kharmandayan, P. Cranial reconstruction: 3D biomodel and custom-built implant created using additive manufacturing. J. Cranio. Maxillofac. Surg. 2014, 42, 1877–1884. [Google Scholar] [CrossRef]
- Xu, N.; Wei, F.; Liu, X.; Jiang, L.; Cai, H.; Li, Z.; Yu, M.; Wu, F.; Liu, Z. Reconstruction of the Upper Cervical Spine Using a Personalized 3D-Printed Vertebral Body in an Adolescent With Ewing Sarcoma. Spine 2016, 41, E50. [Google Scholar] [CrossRef]
- Mäkelä, K.T.; Matilainen, M.; Pulkkinen, P.; Fenstad, A.M.; Havelin, L.I.; Engesaeter, L.; Furnes, O.; Overgaard, S.; Pedersen, A.B.; Kärrholm, J.; et al. Countrywise results of total hip replacement. Acta Orthop. 2014, 85, 107–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokota, H.; Leong, D.J.; Sun, H.B. Mechanical Loading: Bone Remodeling and Cartilage Maintenance. Curr. Osteoporos. Rep. 2011, 9, 237. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.C.; Chen, L.Y. A Review on Biomedical Titanium Alloys: Recent Progress and Prospect. Adv. Eng. Mater. 2019, 21, 1801215. [Google Scholar] [CrossRef] [Green Version]
- Xie, F.; He, X.; Cao, S.; Qu, X. Structural and mechanical characteristics of porous 316L stainless steel fabricated by indirect selective laser sintering. J. Mater. Process. Technol. 2013, 213, 838–843. [Google Scholar] [CrossRef]
- Ehtemam-Haghighi, S.; Cao, G.; Zhang, L.C. Nanoindentation study of mechanical properties of Ti based alloys with Fe and Ta additions. J. Alloys Compd. 2017, 692, 892–897. [Google Scholar] [CrossRef]
- Niinomi, M. Mechanical properties of biomedical titanium alloys. Mater. Sci. Eng. 1998, 243, 231–236. [Google Scholar] [CrossRef]
- Klein, G.L. Aluminum toxicity to bone: A multisystem effect? Osteoporos. Sarcopenia 2019, 5, 2–5. [Google Scholar] [CrossRef]
- Koike, M.; Lockwood, P.E.; Wataha, J.C.; Okabe, T. Initial cytotoxicity of novel titanium alloys. J. Biomed. Mater. Res. Part B Appl. Biomater. 2007, 83, 327–331. [Google Scholar] [CrossRef]
- Konovalov, S.; Komissarova, I.; Ivanov, Y.; Gromov, V.; Kosinov, D. Structural and phase changes under electropulse treatment of fatigue-loaded titanium alloy VT1-0. J. Mater. Res. Technol. 2019, 8, 1300–1307. [Google Scholar] [CrossRef]
- Niinomi, M.; Boehlert, C.J. Titanium Alloys for Biomedical Applications. In Advances in Metallic Biomaterials: Tissues, Materials and Biological Reactions; Niinomi, M., Narushima, T., Nakai, M., Eds.; Springer Series in Biomaterials Science and Engineering; Springer: Berlin/Heidelberg, Germany, 2015; pp. 179–213. [Google Scholar] [CrossRef]
- Raducanu, D.; Cojocaru, V.D.; Nocivin, A.; Cinca, I.; Serban, N.; Cojocaru, E.M. Contributions to Mechanical Characteristics Improvement of Some Biomedical TNTZ Alloys by Adding Fe, Si, and O: A Comparative Study. JOM 2019, 71, 264–271. [Google Scholar] [CrossRef]
- Yang, K.; Wang, J.; Tang, H.; Li, Y. Additive manufacturing of in-situ reinforced Ti–35Nb–5Ta–7Zr (TNTZ) alloy by selective electron beam melting (SEBM). J. Alloys Compd. 2020, 826, 154178. [Google Scholar] [CrossRef]
- Zhang, X.Z.; Leary, M.; Tang, H.P.; Song, T.; Qian, M. Selective electron beam manufactured Ti-6Al-4V lattice structures for orthopedic implant applications: Current status and outstanding challenges. Curr. Opin. Solid State Mater. Sci. 2018, 22, 75–99. [Google Scholar] [CrossRef]
- Arun, K.V.; Jadhav, K.K. Behaviour of Human Femur Bone Under Bending and Impact Loads. Eur. J. Clin. Biomed. Sci. 2016, 2, 6. [Google Scholar] [CrossRef]
- Masuo, H.; Tanaka, Y.; Morokoshi, S.; Yagura, H.; Uchida, T.; Yamamoto, Y.; Murakami, Y. Influence of defects, surface roughness and HIP on the fatigue strength of Ti-6Al-4V manufactured by additive manufacturing. Int. J. Fatigue 2018, 117, 163–179. [Google Scholar] [CrossRef]
- Zhang, P.; He, A.N.; Liu, F.; Zhang, K.; Jiang, J.; Zhang, D.Z. Evaluation of Low Cycle Fatigue Performance of Selective Laser Melted Titanium Alloy Ti–6Al–4V. Metals 2019, 9, 1041. [Google Scholar] [CrossRef] [Green Version]
- Ødegaard, K.S.; Ouyang, L.; Torgersen, J.; Standal, T.; Westhrin, M.; Ma, Q.; Wan, D.; Elverum, C.W. Revealing the influence of electron beam melted Ti-6Al-4V scaffold and donor age in the osteogenesis of human mesenchymal stem cells. Manuscript in Preparation.
- Ødegaard, K.S.; Torgersen, J.; Standal, T.; Westhrin, M.; Ma, Q.; Wan, D.; Afif, A.B.; Dadlani, A.; Elverum, C.W. Investigating the effects of surface treatments on electron beam melted Ti-6Al-4V disks on the osteogenesis of human mesenchymal stem cells. Manuscript in preparation.
- Łyczkowska, E.; Szymczyk, P.; Dybała, B.; Chlebus, E. Chemical polishing of scaffolds made of Ti–6Al–7Nb alloy by additive manufacturing. Arch. Civ. Mech. Eng. 2014, 14, 586–594. [Google Scholar] [CrossRef]
- Wysocki, B.; Idaszek, J.; Szlązak, K.; Strzelczyk, K.; Brynk, T.; Kurzydłowski, K.J.; Święszkowski, W. Post Processing and Biological Evaluation of the Titanium Scaffolds for Bone Tissue Engineering. Materials 2016, 9, 197. [Google Scholar] [CrossRef]
Figure 1.
Schematic representation of biomaterial classifications explained using the case of a bone screw.
Figure 1.
Schematic representation of biomaterial classifications explained using the case of a bone screw.

Figure 2.
Schematic representation of (a) new loading conditions in solid hip implants, and (b) bone in-growth of porous scaffolds
Figure 2.
Schematic representation of (a) new loading conditions in solid hip implants, and (b) bone in-growth of porous scaffolds

Figure 3.
Scanning electron microscope images showing the morphologies of electron beam melted Ti-6Al-4V three-dimensional porous scaffold structure with 800 μm pore and lattice size [165]
Figure 3.
Scanning electron microscope images showing the morphologies of electron beam melted Ti-6Al-4V three-dimensional porous scaffold structure with 800 μm pore and lattice size [165]

Figure 4.
Scanning electron microscope images showing the development of bone matrix after 21 days of culturing with bone marrow-derived human mesenchymal stem cells. (a,c) Cell-free as-built and polished controls, respectively. (b,d) As-built and polished samples cultured with mesenchymal stem cells for 21 days, respectively [166]
Figure 4.
Scanning electron microscope images showing the development of bone matrix after 21 days of culturing with bone marrow-derived human mesenchymal stem cells. (a,c) Cell-free as-built and polished controls, respectively. (b,d) As-built and polished samples cultured with mesenchymal stem cells for 21 days, respectively [166]

Figure 5.
Micro CT image of a porous Ti-6Al-4V scaffold manufactured by electron beam melting. (a) Shows the μCT progression. The green line indicates the cross-section imaging plane for (b). The red circle represents the area where the metallic powder is trapped [165]
Figure 5.
Micro CT image of a porous Ti-6Al-4V scaffold manufactured by electron beam melting. (a) Shows the μCT progression. The green line indicates the cross-section imaging plane for (b). The red circle represents the area where the metallic powder is trapped [165]


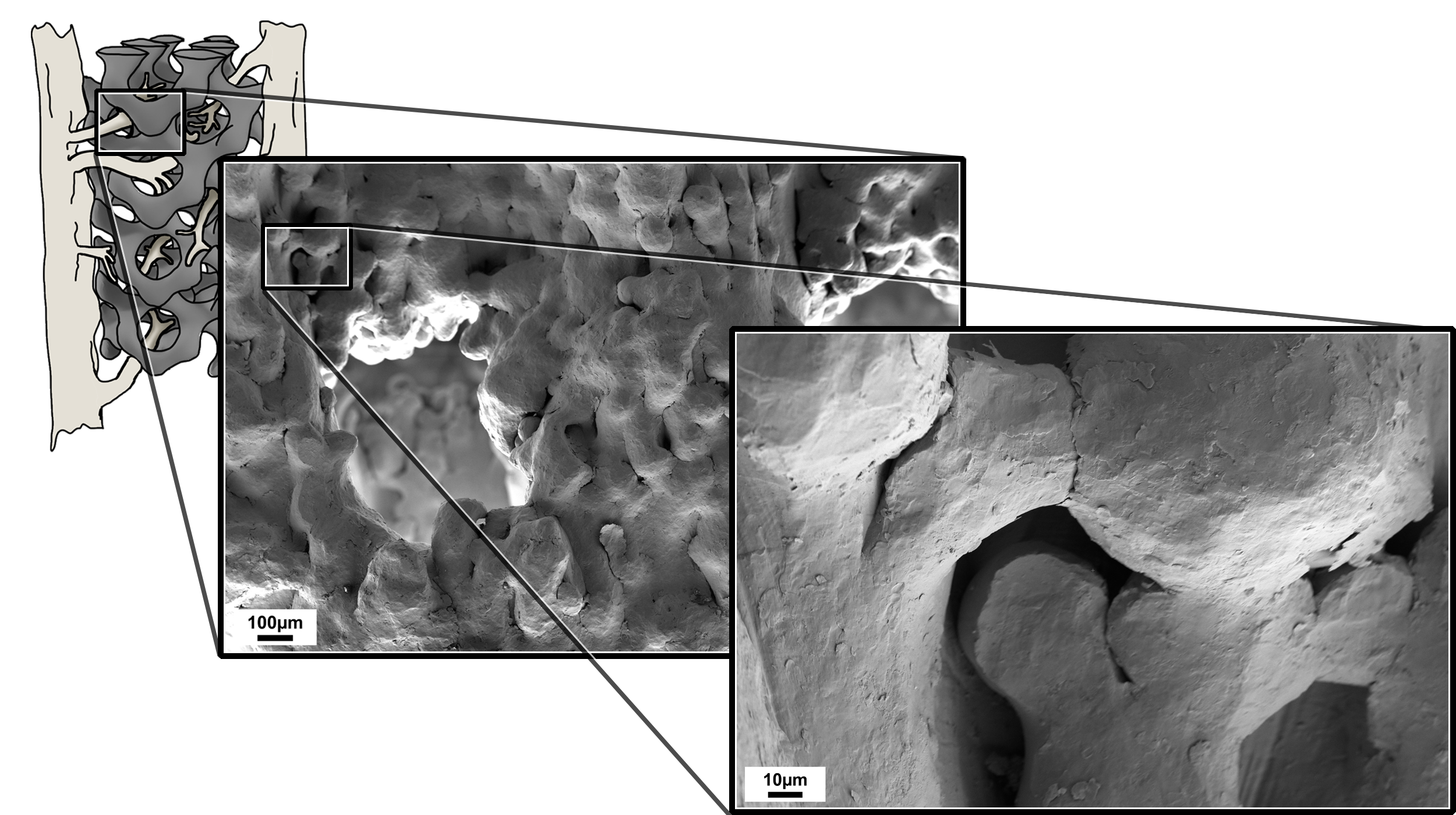{kind=link}
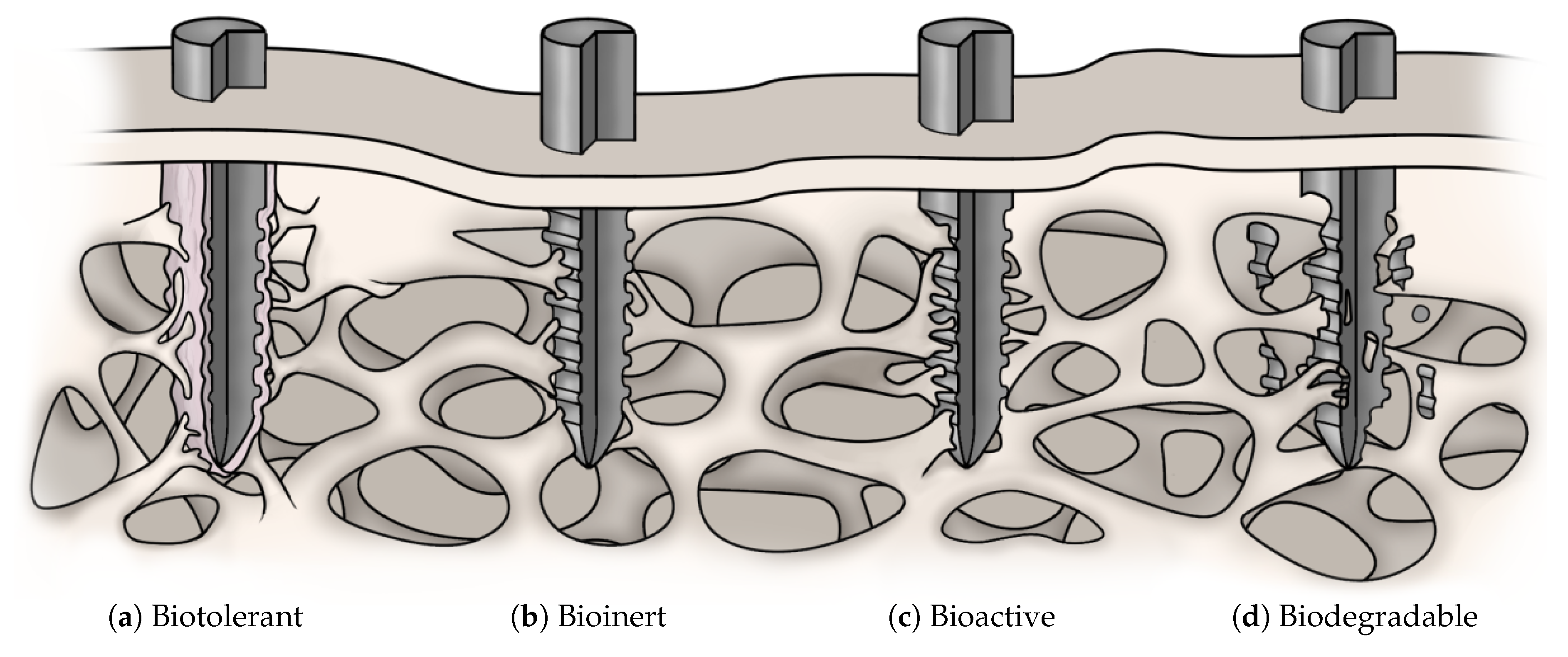{kind=link}
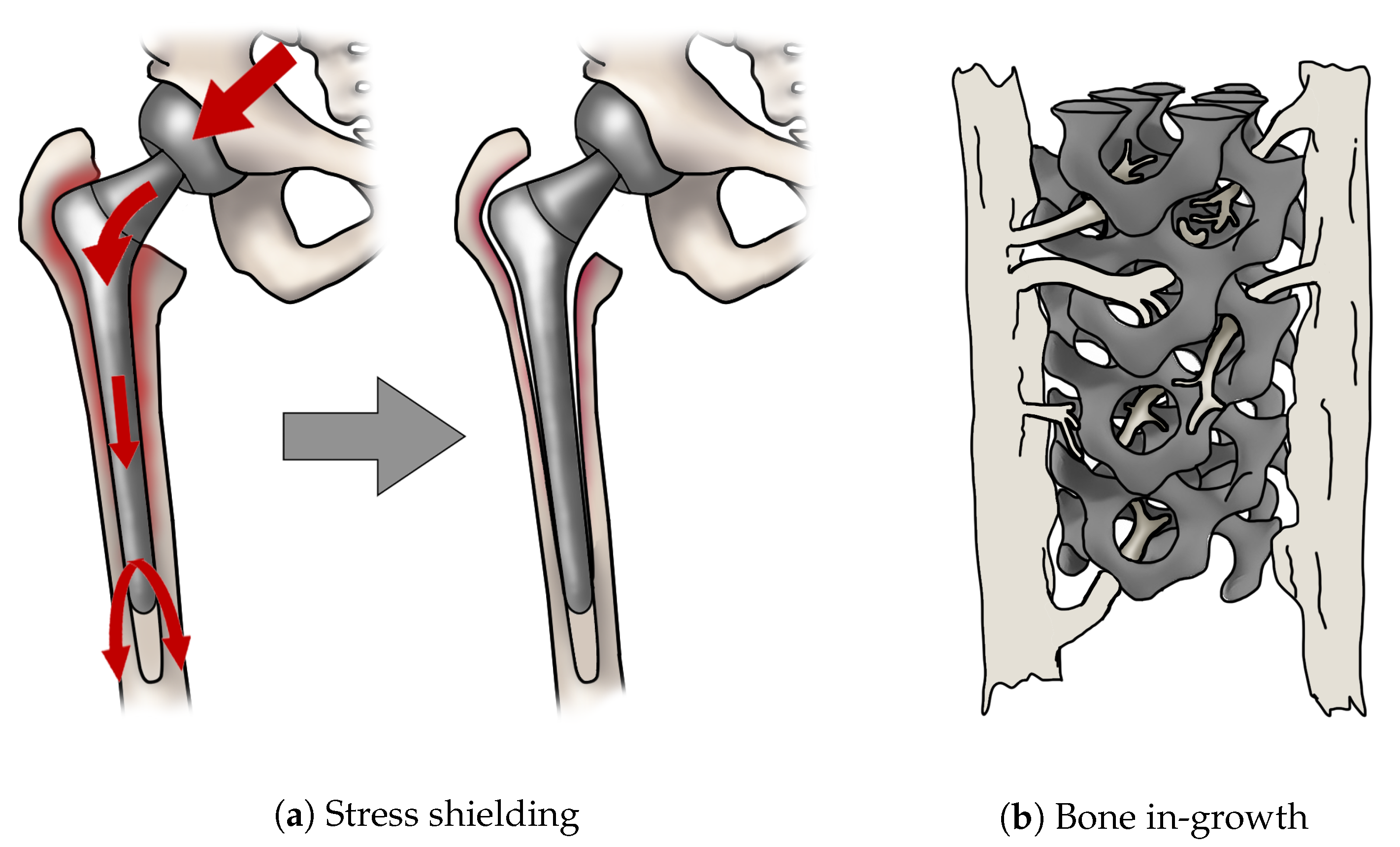{kind=link}
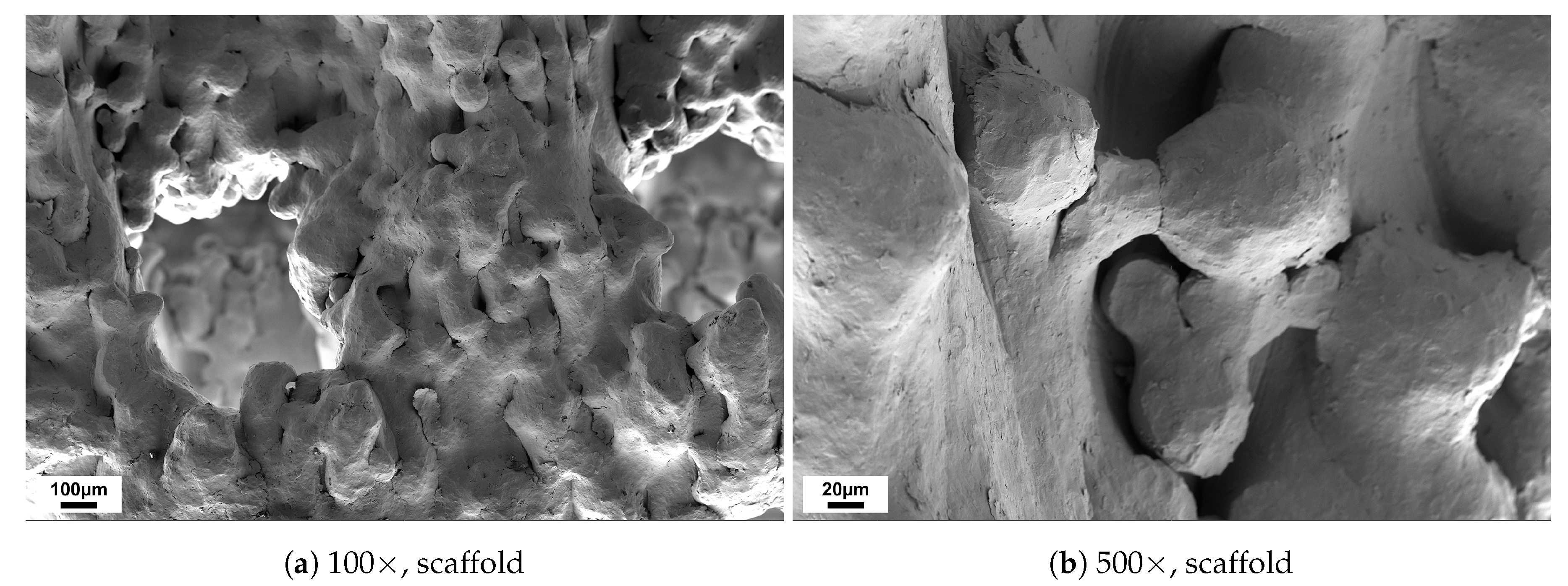{kind=link}
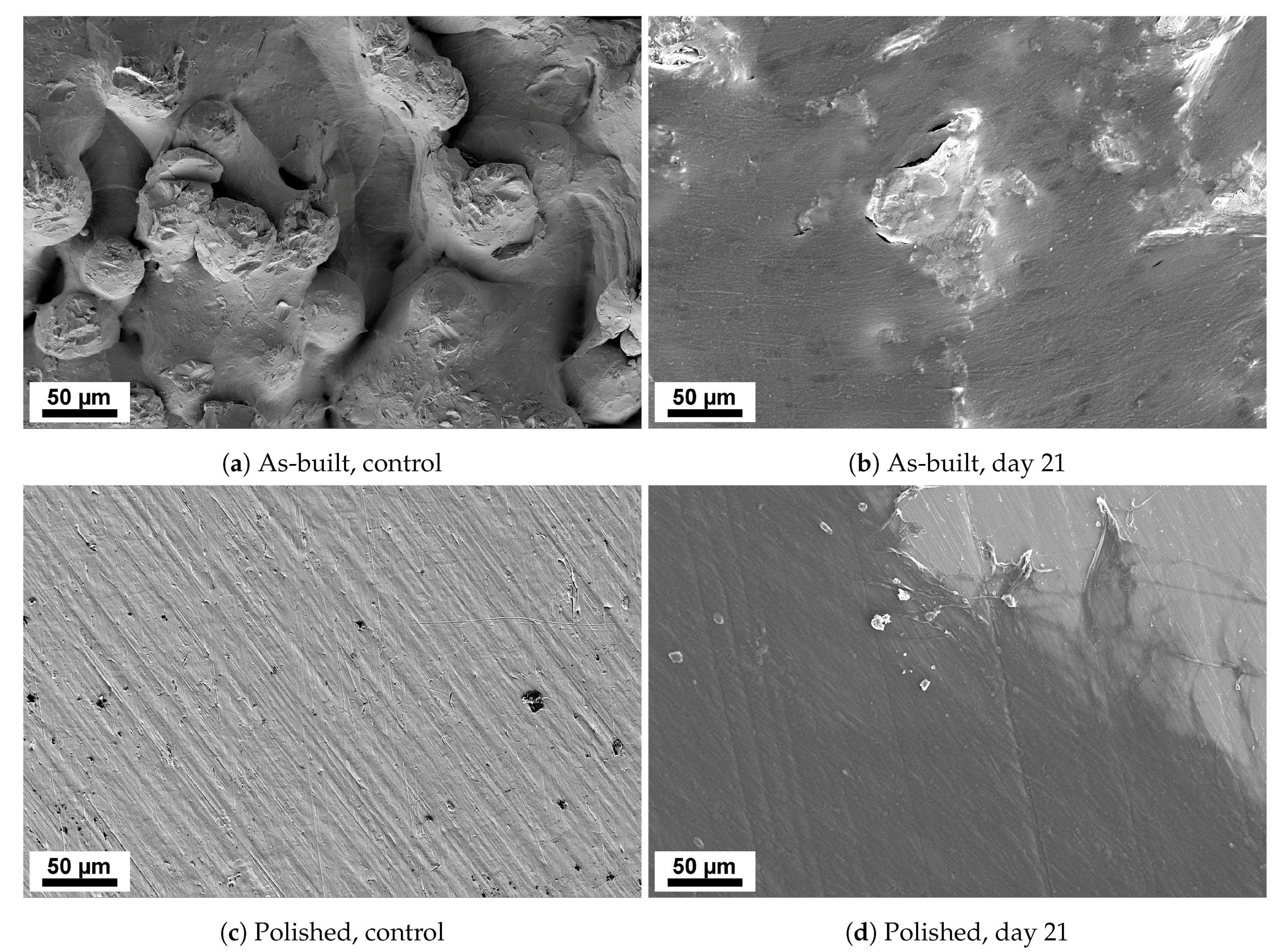{kind=link}
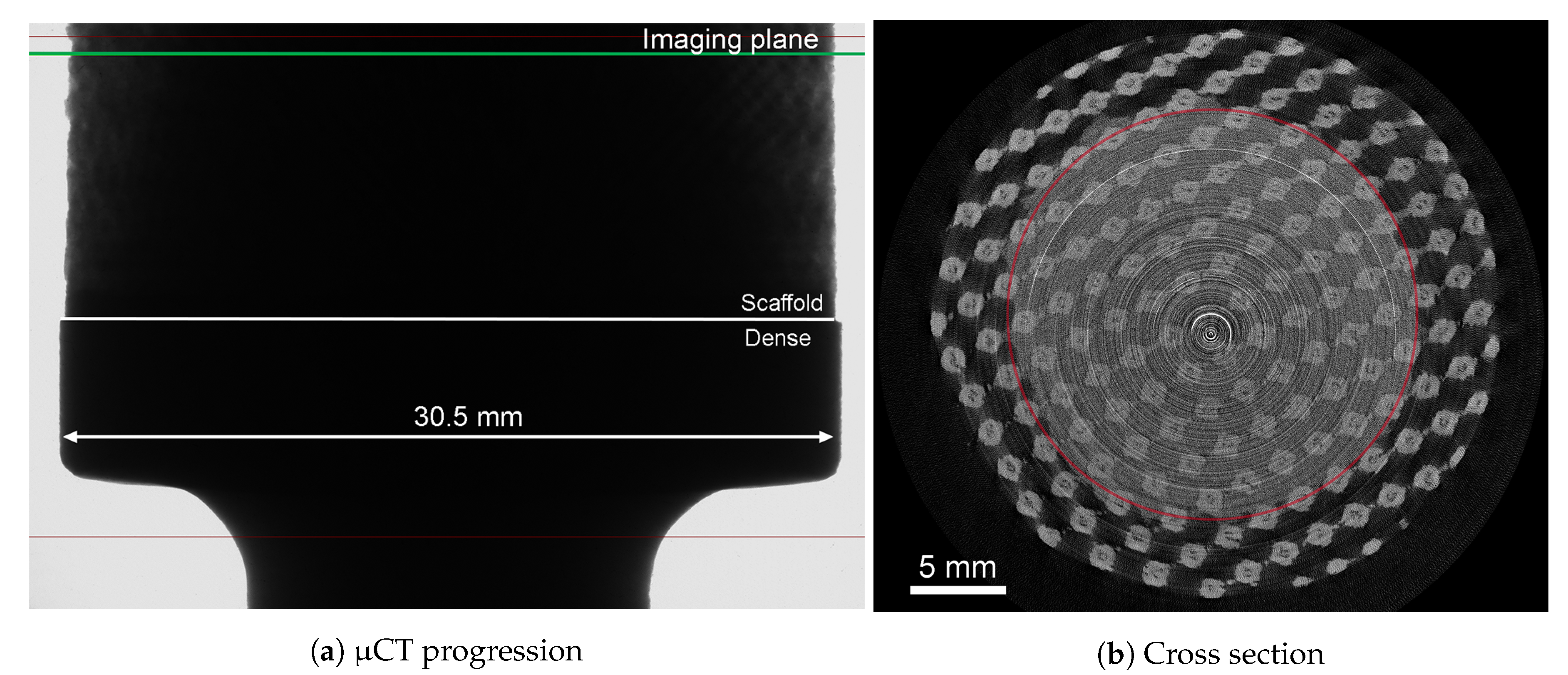{kind=link}
Table 1.
Biocompatible ceramics. The table gives an example of biocompatible ceramics, their characterization, applications, and additive manufacturing methods.
Table 1.
Biocompatible ceramics. The table gives an example of biocompatible ceramics, their characterization, applications, and additive manufacturing methods.
| Ceramics | ||||
|---|---|---|---|---|
| Biomaterial | Characterization | Fabrication Method(s) | Application | Ref |
| Al oxide | Bioinert | Binder Jetting, vat polymerization | Osteosynthetic devices, bearing surfaces | [32,50,51,52] |
| Zirconium oxide | Powder bed fusion (SLS) | Fixed partial dentures | [53,54] | |
| grayHydroxyapatite | Bioactive | Vat polymerization, powder bed fusion (SLS), material extrusion and binder jetting | Bone tissue engineering | [55,56,57,58,59] |
| Bioglass | Vat photopolymerization | Bone tissue engineering | [60] | |
| Calcium silicate | Powder bed fusion (SLS) | Tissue engineering | [61] | |
| grayTricalcium phosphate | Bioactive/ Biodegradable | Binder jetting, vat polymerization, material extrusion | Bone tissue engineering | [62,63,64,65,66] |
Table 2.
Biocompatible polymers and co-polymers. The table gives an overview of biocompatible polymers and co-polymers, their characterization, applications, and additive manufacturing methods.
Table 2.
Biocompatible polymers and co-polymers. The table gives an overview of biocompatible polymers and co-polymers, their characterization, applications, and additive manufacturing methods.
| Polymers and Co-Polymers | |||||
|---|---|---|---|---|---|
| Biomaterial | Abbr. | Characterization | Fabrication Method(s) | Application | Ref |
| Polyethylene | PE | Biotolerant | Powder bed fusion (SLS) | Vascular prostheses, cardiac valves and hip joints | [94,95,96,97] |
| Poly(hexano-6-lactam) | PA6 | Powder bed fusion (SLS) | Intravascular balloon catheters | [98,99] | |
| Poly(methyl methacrylate) | PMMA | Powder bed fusion (SLS) and vat polymerization | Anchoring of hip prostheses, vertebroplasties and eyeglass lenses | [94,97,100,101] | |
| Poly(tetrafluorethylene) | PTFE | Vat photopolymerization | Orthopedy and vascular clips | [94,102,103] | |
| gray Poly(aryletherketone) | PAEK | Bioactive | Powder bed fusion (SLS) | Orthopedic and spinal implants | [97,104,105] |
| Polyurethane | PUR | Biostable and biodegradable | Vat photopolymerization | Cardiovascular devices | [100,106,107] |
| gray Polycaprolactone | PCL | Biodegradable | Powder bed fusion (SLS) and material extrusion | Tissue engineering and controlled drug release | [108,109,110,111] |
| Poly(lactic acid) | PLA | Material extrusion | Bioabsorbable fixation, bone regeneration and fixation and drug delivery | [112] | |
| Poly(lactic acid-co-glycolic acid) | PLGA | Material jetting and material extrusion | Therapeutic devices, drug delivery and tissue engineering | [113,114,115,116] | |
Table 3.
Biocompatible metals. The table gives an example of biocompatible metals, their characterization, applications, and additive manufacturing methods.
Table 3.
Biocompatible metals. The table gives an example of biocompatible metals, their characterization, applications, and additive manufacturing methods.
| Metals | ||||
|---|---|---|---|---|
| Biomaterial | Characterization | Fabrication Method(s) | Application | Ref |
| Gold | Biotolerant | Powder bed fusion (SLM) and binder jetting | Dental restorations | [126,128] |
| Co-Cr-Mo alloys | Powder bed fusion (EBM and SLM) | Orthopedic and dental implants | [129,130,131] | |
| Stainless steel | Powder bed fusion (EBM and SLM) and material extrusion | Cardiovascular stents and orthopedic implants | [130,132,133,134,135,136] | |
| Niobium | Powder bed fusion (EBM) | Vascular stents and coating for orthopedic implants | [137,138,139] | |
| Tantalum | Powder bed fusion (EBM and SLM) | Orthopedic implants | [140,141] | |
| grayCommercially pure titanium | Bioinert | Powder bed fusion (EBM and SLM) | Orthopedic and dental implants | [142,143,144] |
| Titanium alloy (Ti-6Al-4V) | Powder bed fusion (EBM and SLM) | Orthopedic and dental implants | [143,145,146] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ødegaard, K.S.; Torgersen, J.; Elverum, C.W. Structural and Biomedical Properties of Common Additively Manufactured Biomaterials: A Concise Review. Metals 2020, 10, 1677. https://doi.org/10.3390/met10121677
AMA Style
Ødegaard KS, Torgersen J, Elverum CW. Structural and Biomedical Properties of Common Additively Manufactured Biomaterials: A Concise Review. Metals. 2020; 10(12):1677. https://doi.org/10.3390/met10121677
Chicago/Turabian StyleØdegaard, Kristin S., Jan Torgersen, and Christer W. Elverum. 2020. "Structural and Biomedical Properties of Common Additively Manufactured Biomaterials: A Concise Review" Metals 10, no. 12: 1677. https://doi.org/10.3390/met10121677
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.