
Electrochemotherapy Using Doxorubicin and Nanosecond Electric Field Pulses: A Pilot in Vivo Study

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
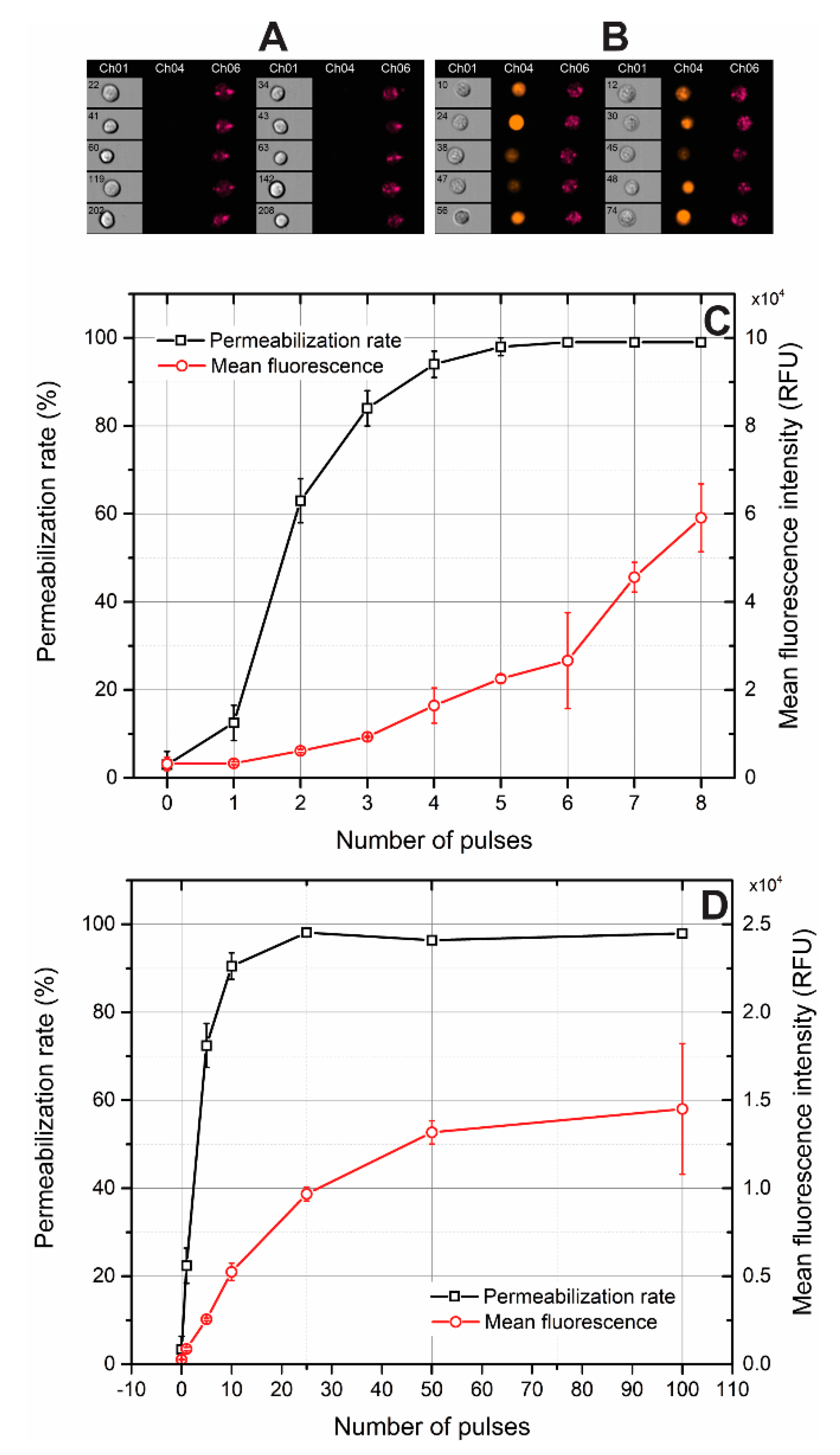
2.1. Electroporation of Sp2/0 Cells In Vitro
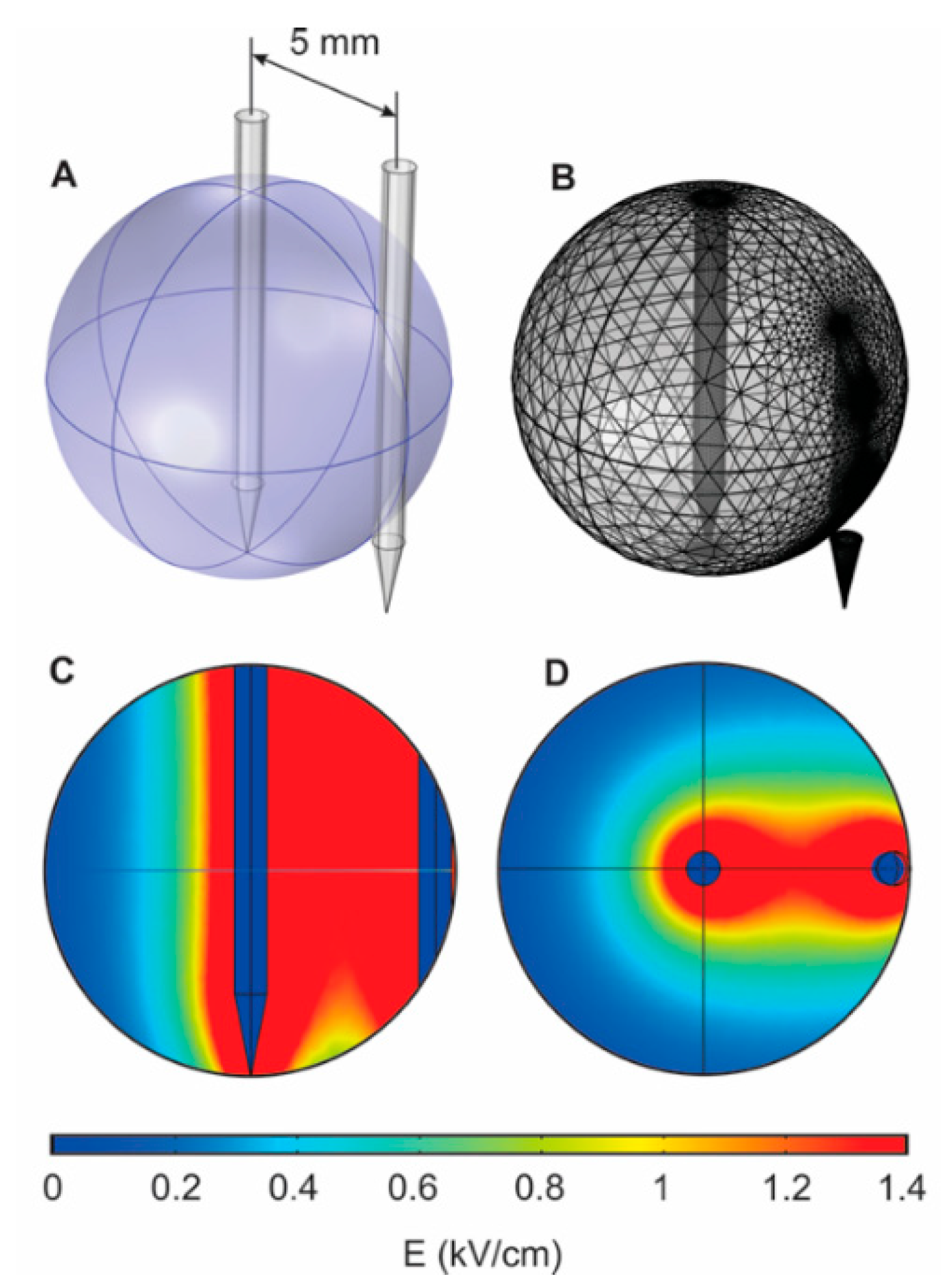
2.2. Electric Field Distribution and Invasive Electrode Positioning Strategy
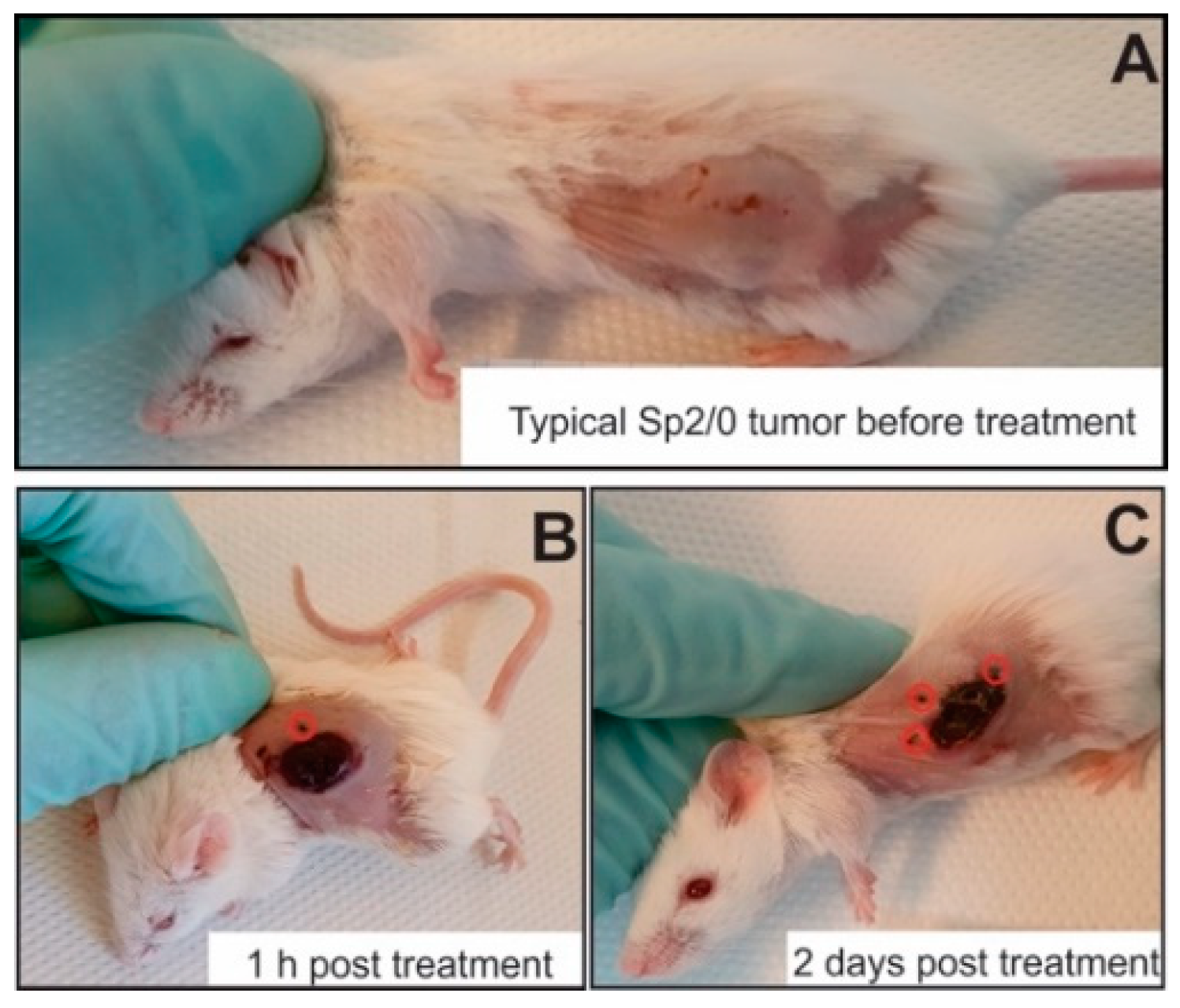
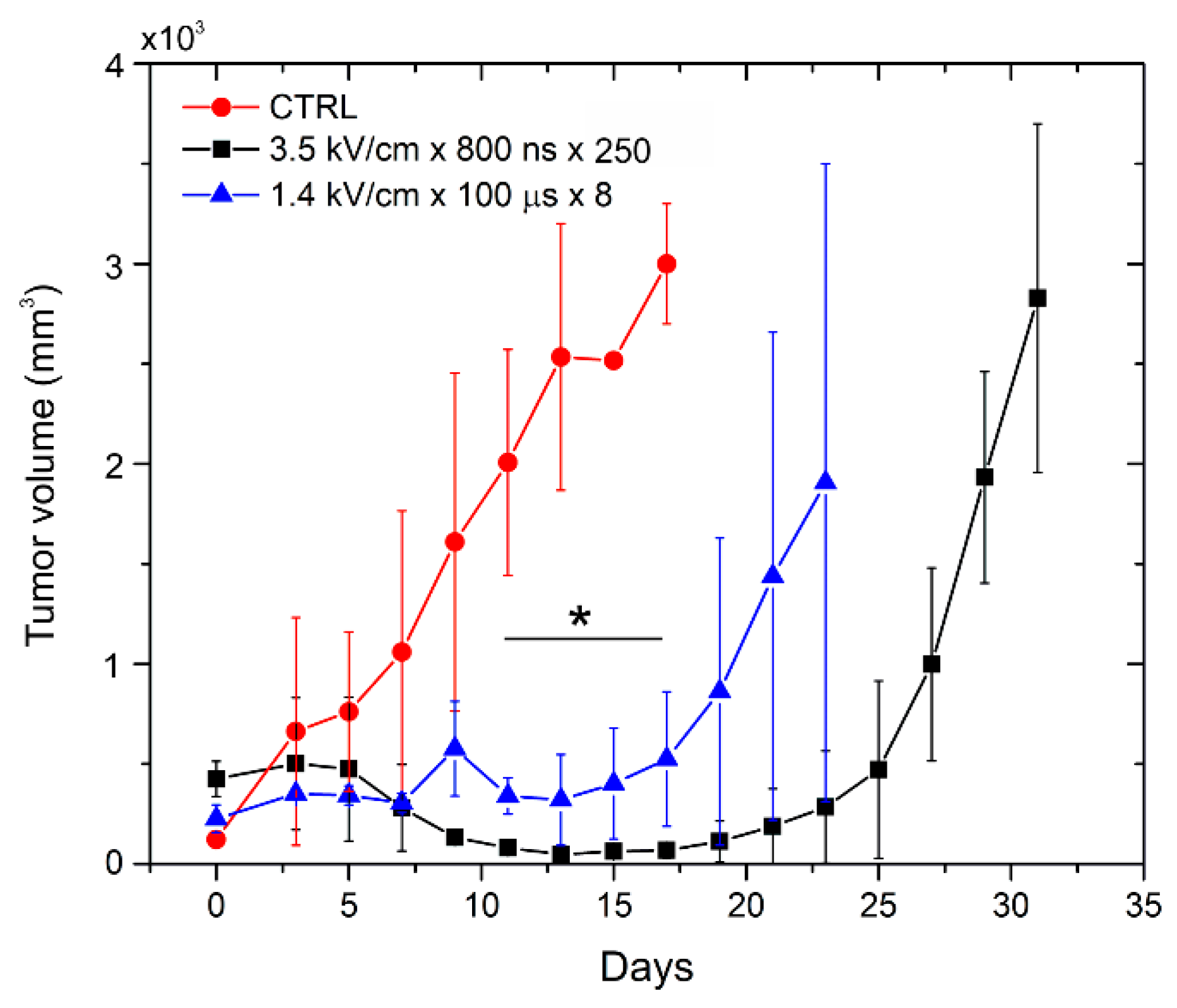
2.3. Efficacy of Microsecond and Nanosecond Range Electrochemotherapy
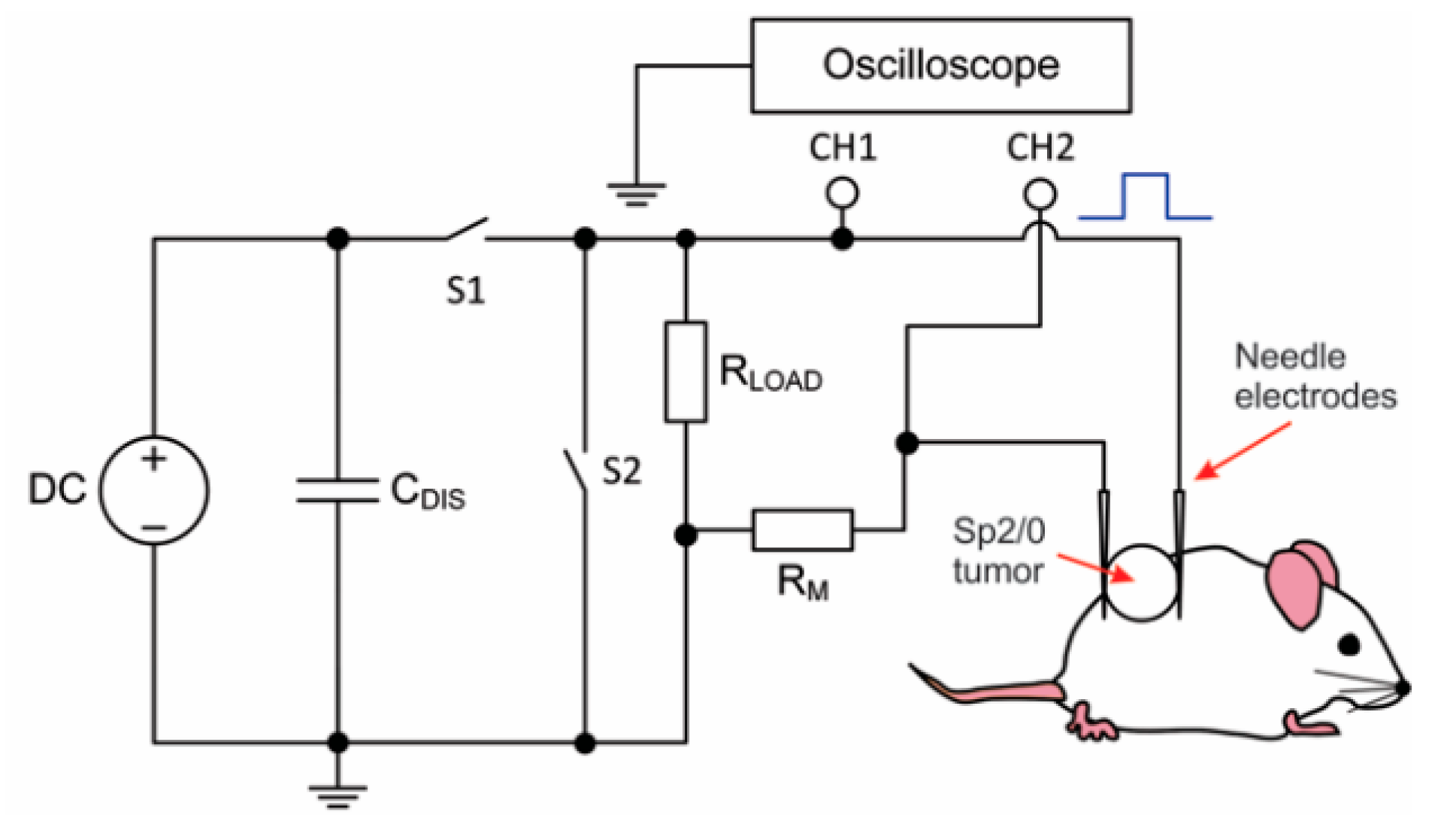
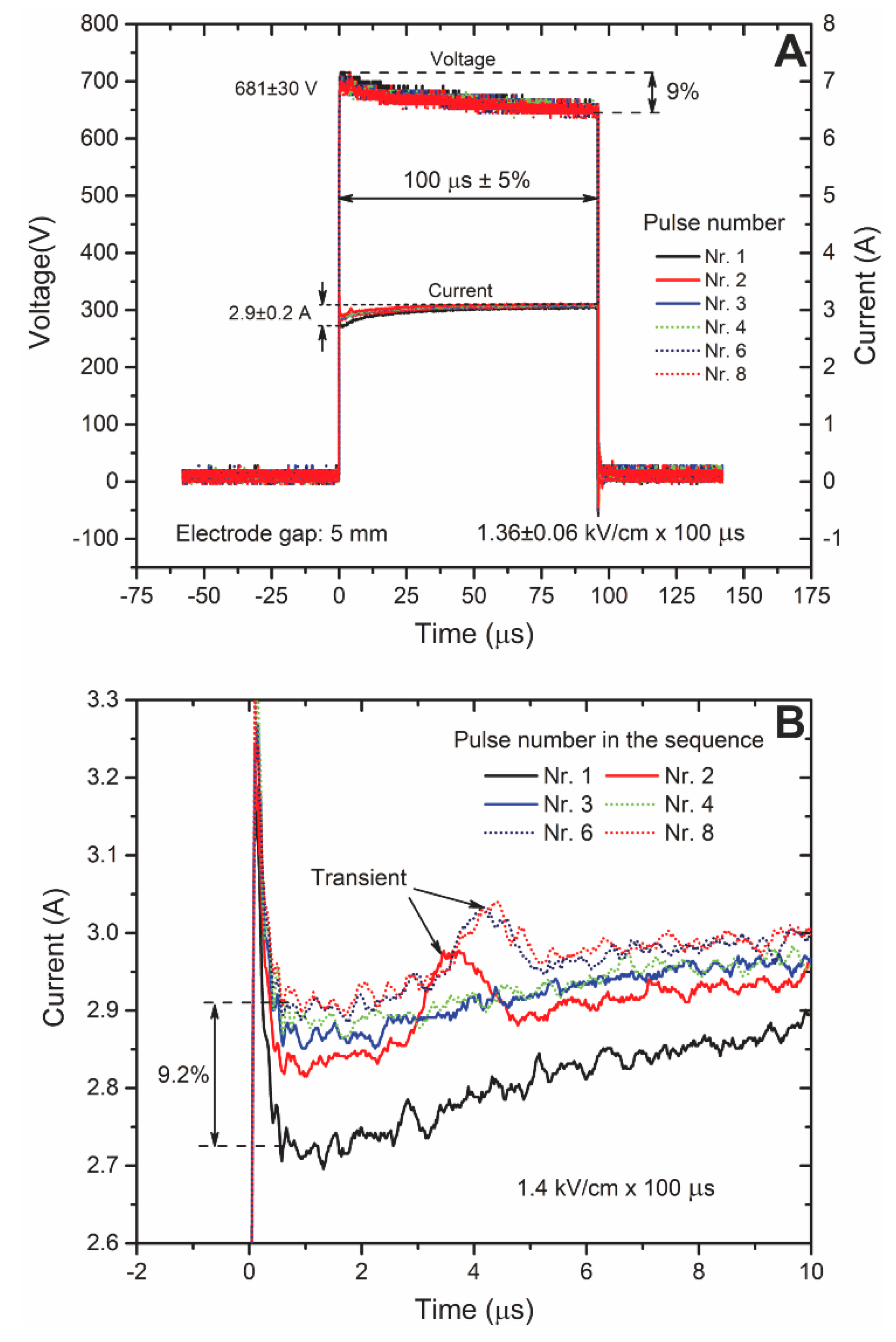
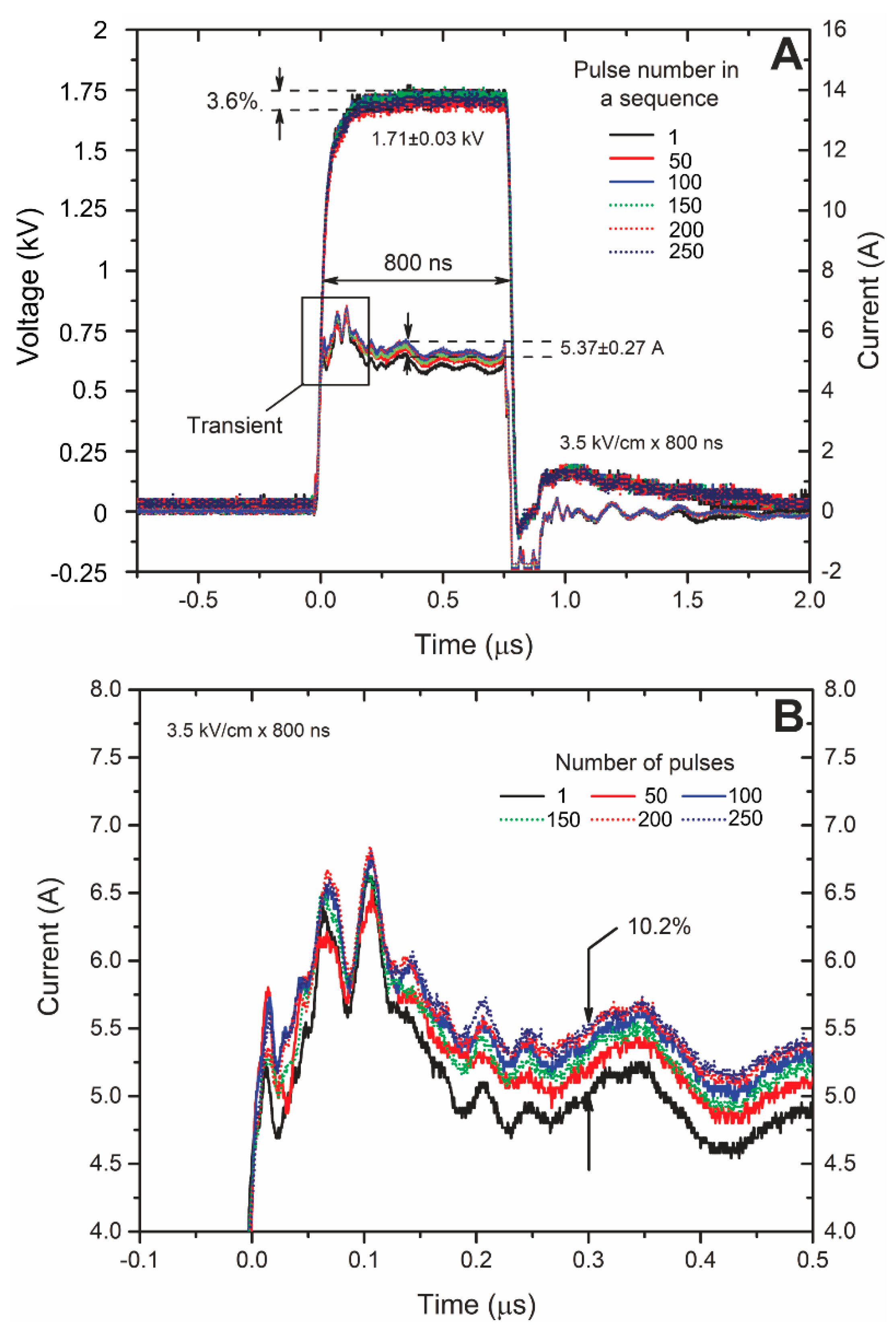
2.4. Current and Voltage Waveforms
3. Discussion
4. Materials and Methods
4.1. The Pulsed Power Setup
4.2. Finite Element Method Simulation
4.3. Mice and Tumor Induction
4.4. Cell Permeabilization Assay
4.5. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
References
- Teissie, J.; Golzio, M.; Rols, M.P. Mechanisms of cell membrane electropermeabilization: A minireview of our present (lack of?) knowledge. Biochim. Biophys. Acta Gen. Subj. 2005, 1724, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Rems, L.; Miklavčič, D. Tutorial: Electroporation of cells in complex materials and tissue. J. Appl. Phys. 2016, 119, 201101. [Google Scholar] [CrossRef]
- Wagstaff, P.G.K.; Buijs, M.; de Bruin, D.M.; Zondervan, P.J.; Jmch, J.; Rosette, D.; Pes, M.P.L. Irreversible electroporation: State of the art. Dovepress 2016, 9, 2437–2446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castellví, Q.; Ginestà, M.M.; Capellà, G.; Ivorra, A. Tumor growth delay by adjuvant alternating electric fields which appears non-thermally mediated. Bioelectrochemistry 2015, 105, 16–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venslauskas, M.S.; Šatkauskas, S. Mechanisms of transfer of bioactive molecules through the cell membrane by electroporation. Eur. Biophys. J. 2015, 44, 277–289. [Google Scholar] [CrossRef]
- Saczko, J.; Pilat, J.; Choromanska, A.; Rembialkowska, N.; Bar, J.; Kaminska, I.; Zalewski, J.; Kulbacka, J. The effectiveness of chemotherapy and electrochemotherapy on ovarian cell lines in vitro. Neoplasma 2016, 63, 450–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivey, J.W.; Latouche, E.L.; Richards, M.L.; Lesser, G.J.; Debinski, W.; Davalos, R.V.; Verbridge, S.S. Enhancing Irreversible Electroporation by Manipulating Cellular Biophysics with a Molecular Adjuvant. Biophys. J. 2017, 113, 472–480. [Google Scholar] [CrossRef] [Green Version]
- Probst, U.; Fuhrmann, I.; Beyer, L.; Wiggermann, P. Electrochemotherapy as a new modality in interventional oncology: A review. Technol. Cancer Res. Treat. 2018, 17, 1533033818785329. [Google Scholar] [CrossRef] [Green Version]
- Tremble, L.F.; O’Brien, M.A.; Soden, D.M.; Forde, P.F. Electrochemotherapy with cisplatin increases survival and induces immunogenic responses in murine models of lung cancer and colorectal cancer. Cancer Lett. 2019, 442, 475–482. [Google Scholar] [CrossRef]
- Marty, M.; Sersa, G.; Garbay, J.R.; Gehl, J.; Collins, C.G.; Snoj, M.; Billard, V.; Geertsen, P.F.; Larkin, J.O.; Miklavcic, D.; et al. Electrochemotherapy—An easy, highly effective and safe treatment of cutaneous and subcutaneous metastases: Results of ESOPE (European Standard Operating Procedures of Electrochemotherapy) study. Eur. J. CancerSuppl. 2006, 4, 3–13. [Google Scholar] [CrossRef]
- Campana, L.G.; Mocellin, S.; Basso, M.; Puccetti, O.; De Salvo, G.L.; Chiarion-Sileni, V.; Vecchiato, A.; Corti, L.; Rossi, C.R.; Nitti, D. Bleomycin-based electrochemotherapy: Clinical outcome from a single institution’s experience with 52 patients. Ann. Surg. Oncol. 2009, 16, 191–199. [Google Scholar] [CrossRef] [PubMed]
- García-Sánchez, T.; Leray, I.; Ronchetti, M.; Cadossi, R.; Mir, L.M. Impact of the number of electric pulses on cell electrochemotherapy in vitro: Limits of linearity and saturation. Bioelectrochemistry 2019, 129, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Drąg-Zalesińska, M.; Saczko, J.; Choromańska, A.; Szewczyk, A.; Rembiałkowska, N.; Kulbacka, J.; Rzechonek, A. Cisplatin and vinorelbine-mediated electrochemotherapeutic approach against multidrug resistant small cell lung cancer (H69Ar) in vitro. Anticancer Res. 2019, 39, 3711–3718. [Google Scholar] [CrossRef] [PubMed]
- Tunikowska, J.; Antończyk, A.; Rembiałkowska, N.; Jóźwiak, Ł.; Novickij, V.; Kulbacka, J. The first application of nanoelectrochemotherapy in feline oral malignant melanoma treatment— case study. Animals 2020, 10, 556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittal, L.; Raman, V.; Camarillo, I.G.; Garner, A.L.; Fairbanks, A.J.; Dunn, G.A.; Sundararajan, R. Synergy of micro and nanosecond electrical pulses with chemotherapeutics on human cancer cell viability. In Proceedings of the Annual Report-Conference on Electrical Insulation and Dielectric Phenomena, CEIDP, Fort Worth, TX, USA, 22–25 October 2017. [Google Scholar]
- Zhang, Y.; Mao, Z.; Wang, B.; Zhang, J.; Lu, N.; Hong, R.; Dong, S.; Yao, C.; Liu, Q.H. Enhanced Antitumor Efficacy Achieved through Combination of nsPEFs and Low-Dosage Paclitaxel. IEEE Trans. Biomed. Eng. 2019, 66, 3129–3135. [Google Scholar] [CrossRef] [PubMed]
- Nuccitelli, R.; Chen, X.; Pakhomov, A.G.; Baldwin, W.H.; Sheikh, S.; Pomicter, J.L.; Ren, W.; Osgood, C.; Swanson, R.J.; Kolb, J.F.; et al. A new pulsed electric field therapy for melanoma disrupts the tumor’s blood supply and causes complete remission without recurrence. Int. J. Cancer 2009, 125, 438–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuccitelli, R. Application of Pulsed Electric Fields to Cancer Therapy. Bioelectricity 2019, 1, 30–34. [Google Scholar] [CrossRef]
- Mi, Y.; Xu, J.; Tang, X.; Yao, C.; Li, C. Electroporation simulation of a multicellular system exposed to high-frequency 500 ns pulsed electric fields. IEEE Trans. Dielectr. Electr. Insul. 2017, 24, 3985–3994. [Google Scholar] [CrossRef]
- Zhang, B.; Kuang, D.; Tang, X.; Mi, Y.; Luo, Q.; Song, G. Effect of low-field high-frequency nsPEFs on the biological behaviors of human A375 melanoma cells. IEEE Trans. Biomed. Eng. 2018, 65, 2093–2100. [Google Scholar] [CrossRef]
- Mi, Y.; Xu, J.; Tang, X.; Bian, C.; Liu, H.; Yang, Q.; Tang, J. Scaling Relationship of In Vivo Muscle Contraction Strength of Rabbits Exposed to High-Frequency Nanosecond Pulse Bursts. Technol. Cancer Res. Treat. 2018, 17, 1533033818788078. [Google Scholar] [CrossRef] [Green Version]
- Yadav, D.K.; Kumar, S.; Choi, E.H.; Kim, M.H. Electric-field-induced electroporation and permeation of reactive oxygen species across a skin membrane. J. Biomol. Struct. Dyn. 2020, 2, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Yusupov, M.; Van der Paal, J.; Neyts, E.C.; Bogaerts, A. Synergistic effect of electric field and lipid oxidation on the permeability of cell membranes. Biochim. Biophys. Acta Gen. Subj. 2017, 1861, 839–847. [Google Scholar] [CrossRef] [PubMed]
- Pakhomova, O.N.; Khorokhorina, V.A.; Bowman, A.M.; Rodaite-Riševičiene, R.; Saulis, G.; Xiao, S.; Pakhomov, A.G. Oxidative effects of nanosecond pulsed electric field exposure in cells and cell-free media. Arch. Biochem. Biophys. 2012, 527, 55–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beebe, S.J.; Sain, N.M.; Ren, W. Induction of Cell Death Mechanisms and Apoptosis by Nanosecond Pulsed Electric Fields (nsPEFs). Cells 2013, 2, 136–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruzgys, P.; Novickij, V.; Novickij, J.; Šatkauskas, S. Influence of the electrode material on ROS generation and electroporation efficiency in low and high frequency nanosecond pulse range. Bioelectrochemistry 2019, 127, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Fiorentzis, M.; Kalirai, H.; Katopodis, P.; Seitz, B.; Viestenz, A.; Coupland, S.E. Electrochemotherapy with bleomycin and cisplatin enhances cytotoxicity in primary and metastatic uveal melanoma cell lines in vitro. Neoplasma 2018, 65, 210–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campana, L.G.; Galuppo, S.; Marconato, R.; Matthiessen, L.W. Electrochemotherapy for Breast Cancer. In Handbook of Electroporation; Springer: Berlin/Heidelberg, Germany, 2017; ISBN 9783319328867. [Google Scholar]
- Sauer, H.; Pütz, V.; Fischer, K.; Hescheler, J.; Wartenberg, M. Increased doxorubicin uptake and toxicity in multicellular tumour spheroids treated with DC electrical fields. Br. J. Cancer 1999, 80, 1204–1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rembiałkowska, N.; Dubińska-Magiera, M.; Sikora, A.; Szlasa, W.; Szewczyk, A.; Czapor-Irzabek, H.; Daczewska, M.; Saczko, J.; Kulbacka, J. Doxorubicin assisted by microsecond electroporation promotes irreparable morphological alternations in sensitive and resistant human breast adenocarcinoma cells. Appl. Sci. 2020, 10, 2765. [Google Scholar] [CrossRef] [Green Version]
- Gianulis, E.C.; Labib, C.; Saulis, G.; Novickij, V.; Pakhomova, O.N.; Pakhomov, A.G. Selective susceptibility to nanosecond pulsed electric field (nsPEF) across different human cell types. Cell. Mol. Life Sci. 2016, 4, 1741–1754. [Google Scholar] [CrossRef]
- Dermol-Černe, J.; Miklavčič, D.; Reberšek, M.; Mekuč, P.; Bardet, S.M.; Burke, R.; Arnaud-Cormos, D.; Leveque, P.; O’Connor, R. Plasma membrane depolarization and permeabilization due to electric pulses in cell lines of different excitability. Bioelectrochemistry 2018, 122, 103–114. [Google Scholar] [CrossRef]
- Batista Napotnik, T.; Miklavčič, D. In vitro electroporation detection methods—An overview. Bioelectrochemistry 2018, 120, 166–182. [Google Scholar] [CrossRef] [PubMed]
- Langus, J.; Kranjc, M.; Kos, B.; Šuštar, T.; Miklavčič, D. Dynamic finite-element model for efficient modelling of electric currents in electroporated tissue. Sci. Rep. 2016, 6, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Golberg, A.; Rubinsky, B. Towards Electroporation Based Treatment Planning considering Electric Field Induced Muscle Contractions. Technol. Cancer Res. Treat. 2013, 11, 189–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kranjc, M.; Kranjc, S.; Bajd, F.; Serša, G.; Serša, I.; Miklavčič, D. Predicting irreversible electroporation-induced tissue damage by means of magnetic resonance electrical impedance tomography. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Bhonsle, S.; Dong, S.; Lv, Y.; Liu, H.; Safaai-Jazi, A.; Davalos, R.V.; Yao, C. Characterization of Conductivity Changes during High-Frequency Irreversible Electroporation for Treatment Planning. IEEE Trans. Biomed. Eng. 2017, 65, 1810–1819. [Google Scholar] [CrossRef] [PubMed]
- Ruarus, A.H.; Vroomen, L.G.P.H.; Puijk, R.S.; Scheffer, H.J.; Faes, T.J.C.; Meijerink, M.R. Conductivity Rise During Irreversible Electroporation: True Permeabilization or Heat? Cardiovasc. Interv. Radiol. 2018, 41, 1257–1266. [Google Scholar] [CrossRef] [Green Version]
- Haemmerich, D.; Schutt, D.J.; Wright, A.W.; Webster, J.G.; Mahvi, D.M. Electrical conductivity measurement of excised human metastatic liver tumours before and after thermal ablation. Physiol. Meas. 2009, 30, 459. [Google Scholar] [CrossRef] [Green Version]
- Corovic, S.; Bester, J.; Miklavcic, D. An e-learning application on electrochemotherapy. Biomed. Eng. Online 2009, 8, 26. [Google Scholar] [CrossRef] [Green Version]
- Garcia, P.A.; Davalos, R.V.; Miklavcic, D. A numerical investigation of the electric and thermal cell kill distributions in electroporation-based therapies in tissue. PLoS ONE 2014, 9, e103083. [Google Scholar] [CrossRef]
- Haemmerich, D.; Staelin, S.T.; Tsai, J.Z.; Tungjitkusolmun, S.; Mahvi, D.M.; Webster, J.G. In vivo electrical conductivity of hepatic tumours. Proc. Physiol. Meas. 2003, 24, 251. [Google Scholar] [CrossRef] [Green Version]
- Gabriel, S.; Lau, R.W.; Gabriel, C. The dielectric properties of biological tissues: III. Parametric models for the dielectric spectrum of tissues. Phys. Med. Biol. 1996, 41, 2271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neal, R.E.; Garcia, P.A.; Robertson, J.L.; Davalos, R.V. Experimental characterization and numerical modeling of tissue electrical conductivity during pulsed electric fields for irreversible electroporation treatment planning. IEEE Trans. Biomed. Eng. 2012, 59, 1076–1085. [Google Scholar] [CrossRef] [PubMed]
- Schoenbach, K.; Joshi, R.; Beebe, S.; Baum, C. A scaling law for membrane permeabilization with nanopulses. IEEE Trans. Dielectr. Electr. Insul. 2009, 16, 1224–1235. [Google Scholar] [CrossRef]
- Rubinsky, L.; Guenther, E.; Mikus, P.; Stehling, M.; Rubinsky, B. Electrolytic Effects During Tissue Ablation by Electroporation. Technol. Cancer Res. Treat. 2016, 15, 95–103. [Google Scholar] [CrossRef] [Green Version]
- Garcia, P.A.; Rossmeisl, J.H.; Neal, R.E.; Ellis, T.L.; Davalos, R.V. A parametric study delineating irreversible electroporation from thermal damage based on a minimally invasive intracranial procedure. Biomed. Eng. Online 2011, 10, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kjeken, R.; Tjelle, T.E.; Kvale, D.; Mathiesen, I. 157. Clinical Evaluation of Pain and Muscle Damage Induced by Electroporation of Skeletal Muscle in Humans. Mol. Ther. 2004, 9, S60. [Google Scholar]
- Frey, W.; White, J.A.; Price, R.O.; Blackmore, P.F.; Joshi, R.P.; Nuccitelli, R.; Beebe, S.J.; Schoenbach, K.H.; Kolb, J.F. Plasma membrane voltage changes during nanosecond pulsed electric field exposure. Biophys. J. 2006, 90, 3608–3615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golberg, A.; Bruinsma, B.G.; Uygun, B.E.; Yarmush, M.L. Tissue heterogeneity in structure and conductivity contribute to cell survival during irreversible electroporation ablation by “electric field sinks”. Sci. Rep. 2014, 5, 8485. [Google Scholar] [CrossRef] [Green Version]
- Alhowail, A.H.; Bloemer, J.; Majrashi, M.; Pinky, P.D.; Bhattacharya, S.; Yongli, Z.; Bhattacharya, D.; Eggert, M.; Woodie, L.; Buabeid, M.A.; et al. Doxorubicin-induced neurotoxicity is associated with acute alterations in synaptic plasticity, apoptosis, and lipid peroxidation. Toxicol. Mech. Methods 2019, 29, 457–466. [Google Scholar] [CrossRef]
- Novickij, V.; Grainys, A.; Butkus, P.; Tolvaišienė, S.; Švedienė, J.; Paškevičius, A.; Novickij, J. High-frequency submicrosecond electroporator. Biotechnol. Biotechnol. Equip. 2016, 30, 607–613. [Google Scholar] [CrossRef] [Green Version]
- Novickij, V.; Girkontaite, I.; Grainys, A.; Zinkevičiene, A.; Lastauskiene, E.; Švediene, J.; Paškevičius, A.; Markovskaja, S.; Novickij, J. Measurement of Transient Permeability of Sp2/0 Myeloma Cells: Flow Cytometric Study. Meas. Sci. Rev. 2016, 16, 300–304. [Google Scholar] [CrossRef] [Green Version]
Sample Availability: Samples of the compounds are not available. |







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Novickij, V.; Malyško, V.; Želvys, A.; Balevičiūtė, A.; Zinkevičienė, A.; Novickij, J.; Girkontaitė, I. Electrochemotherapy Using Doxorubicin and Nanosecond Electric Field Pulses: A Pilot in Vivo Study. Molecules 2020, 25, 4601. https://doi.org/10.3390/molecules25204601
Novickij V, Malyško V, Želvys A, Balevičiūtė A, Zinkevičienė A, Novickij J, Girkontaitė I. Electrochemotherapy Using Doxorubicin and Nanosecond Electric Field Pulses: A Pilot in Vivo Study. Molecules. 2020; 25(20):4601. https://doi.org/10.3390/molecules25204601
Chicago/Turabian StyleNovickij, Vitalij, Veronika Malyško, Augustinas Želvys, Austėja Balevičiūtė, Auksė Zinkevičienė, Jurij Novickij, and Irutė Girkontaitė. 2020. "Electrochemotherapy Using Doxorubicin and Nanosecond Electric Field Pulses: A Pilot in Vivo Study" Molecules 25, no. 20: 4601. https://doi.org/10.3390/molecules25204601