
Effect of Biologically Oriented Preparation Technique on the Stress Concentration of Endodontically Treated Upper Central Incisor Restored with Zirconia Crown: 3D-FEA

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
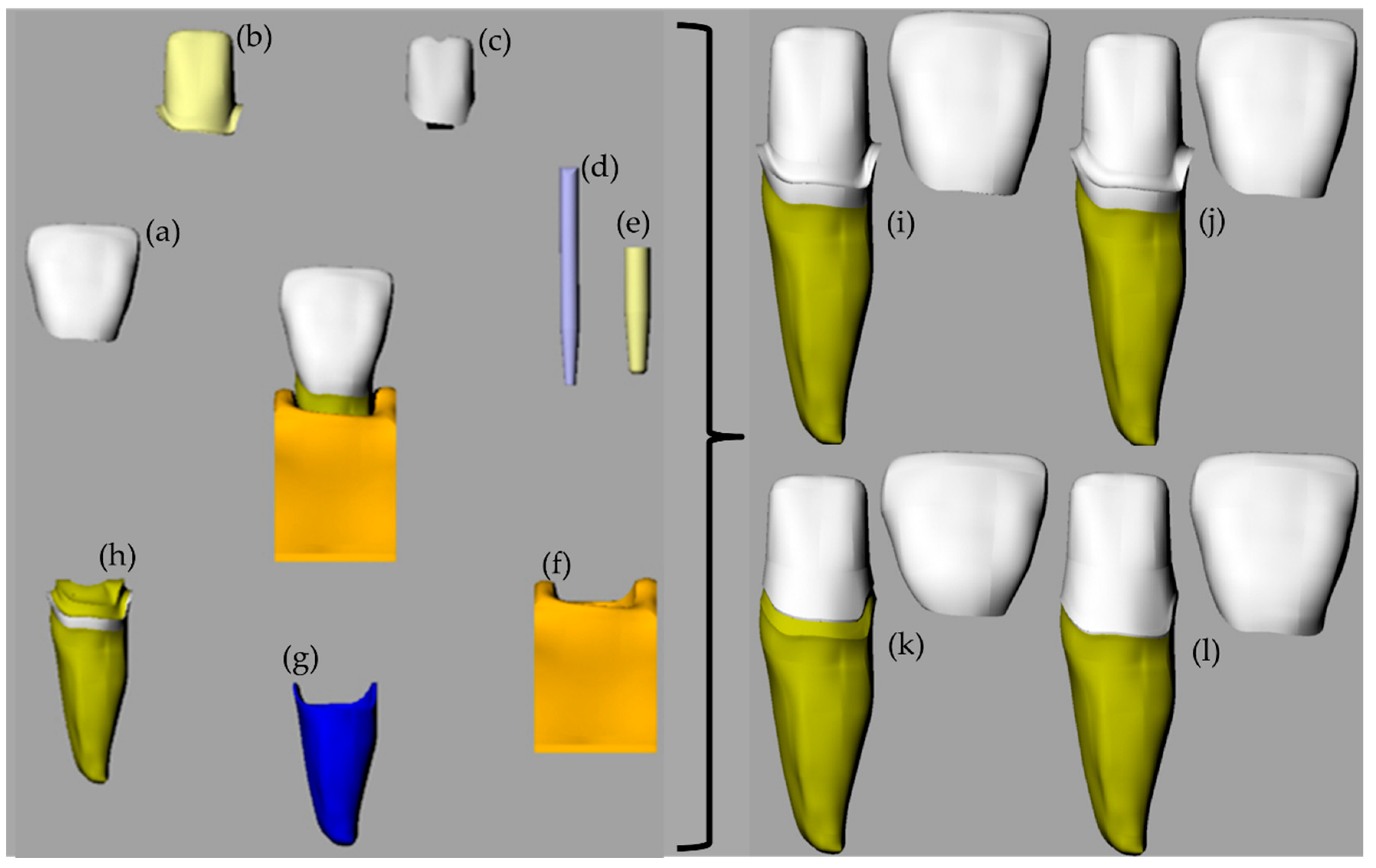
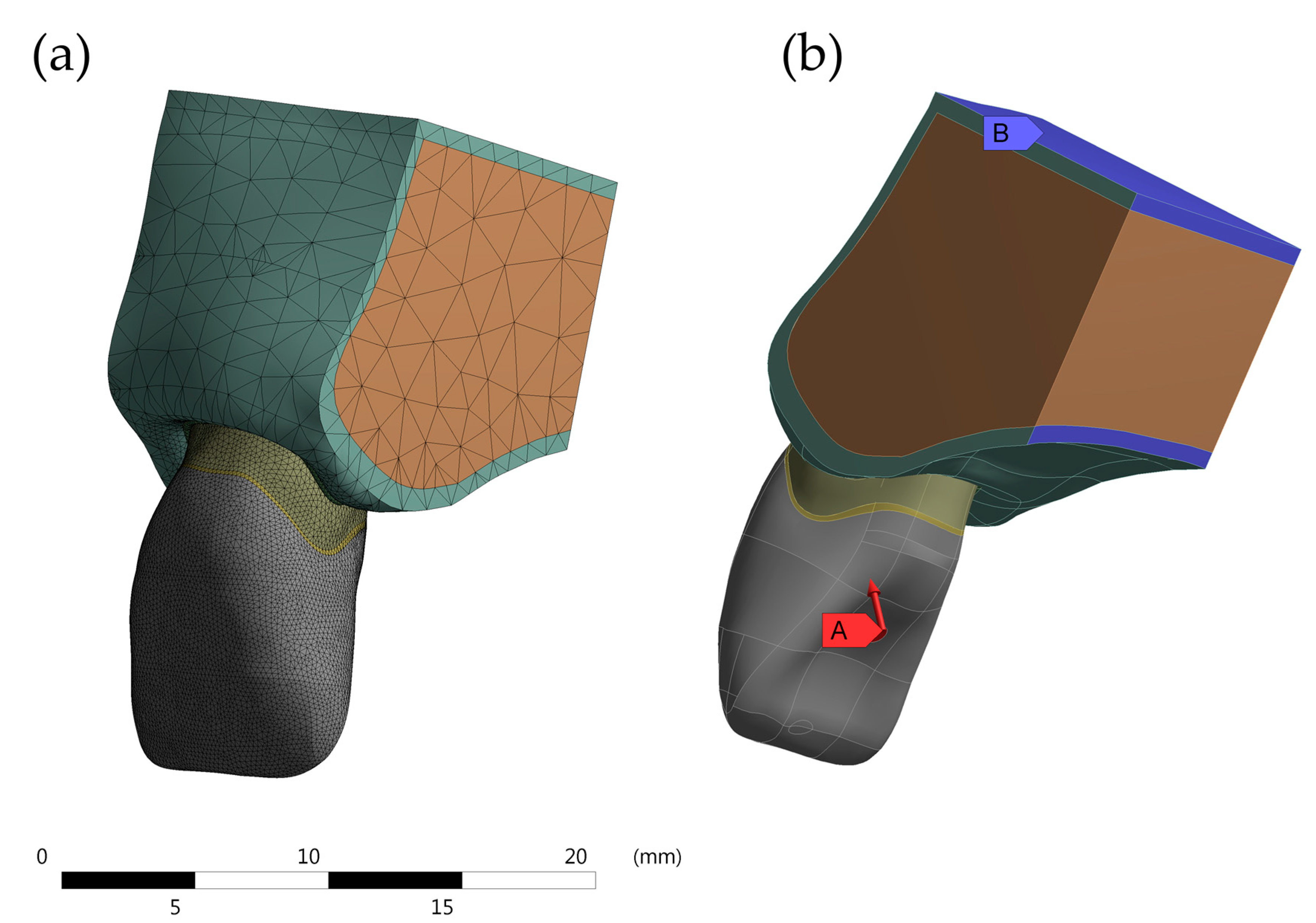
2. Methods
- SM model—preparation in 90° shoulder in CEJ with marginal thickness of 0.5 mm and incisal reduction of 2 mm; zirconia crown with 1 mm thickness and cement layer in 0.1 mm; fiberglass post number 02 Exact (Angelus© Londrina, Brazil) with cement layer in 0.3 mm and remaining coronary (ferrule) with 1 mm height, 360° around the element.
- CM model—preparation with chamfer in CEJ with marginal thickness of 0.5 mm and incisal reduction of 2 mm; zirconia crown with 1 mm thickness and cement layer in 0.1 mm; fiberglass post number 02 Exact (Angelus© Londrina, Brazil) with cement layer in 0.3 mm and remaining coronary (ferrule) with 1 mm height, 360° around the element.
- BOPT model—preparation BOPT in CEJ with marginal thickness of 0.5 mm and incisal reduction of 2 mm; zirconia crown with 1 mm thickness and cement layer in 0.1 mm; fiberglass post number 02 Exact (Angelus© Londrina, Brazil) with cement layer in 0.3 mm and remaining coronary (ferrule) with 1 mm height, 360° around the element.
- BOPTB model—preparation similar to BOPT, positioned 1 mm below the CEJ with marginal thickness of 0.5 mm and incisal reduction of 2 mm; zirconia crown with 1 mm thickness and cement layer in 0.1 mm; fiberglass post number 02 Exact (Angelus© Londrina, Brazil) with cement layer in 0.3 mm and remaining coronary (ferrule) with 1 mm height, 360° around the element.BOPTB model—preparation similar to BOPT, positioned 1 mm below the CEJ with marginal thickness of 0.5 mm and incisal reduction of 2 mm; zirconia crown with 1 mm thickness and cement layer in 0.1 mm; fiberglass post number 02 Exact (Angelus© Londrina, Brazil) with cement layer in 0.3 mm and remaining coronary (ferrule) with 1 mm height, 360° around the element.
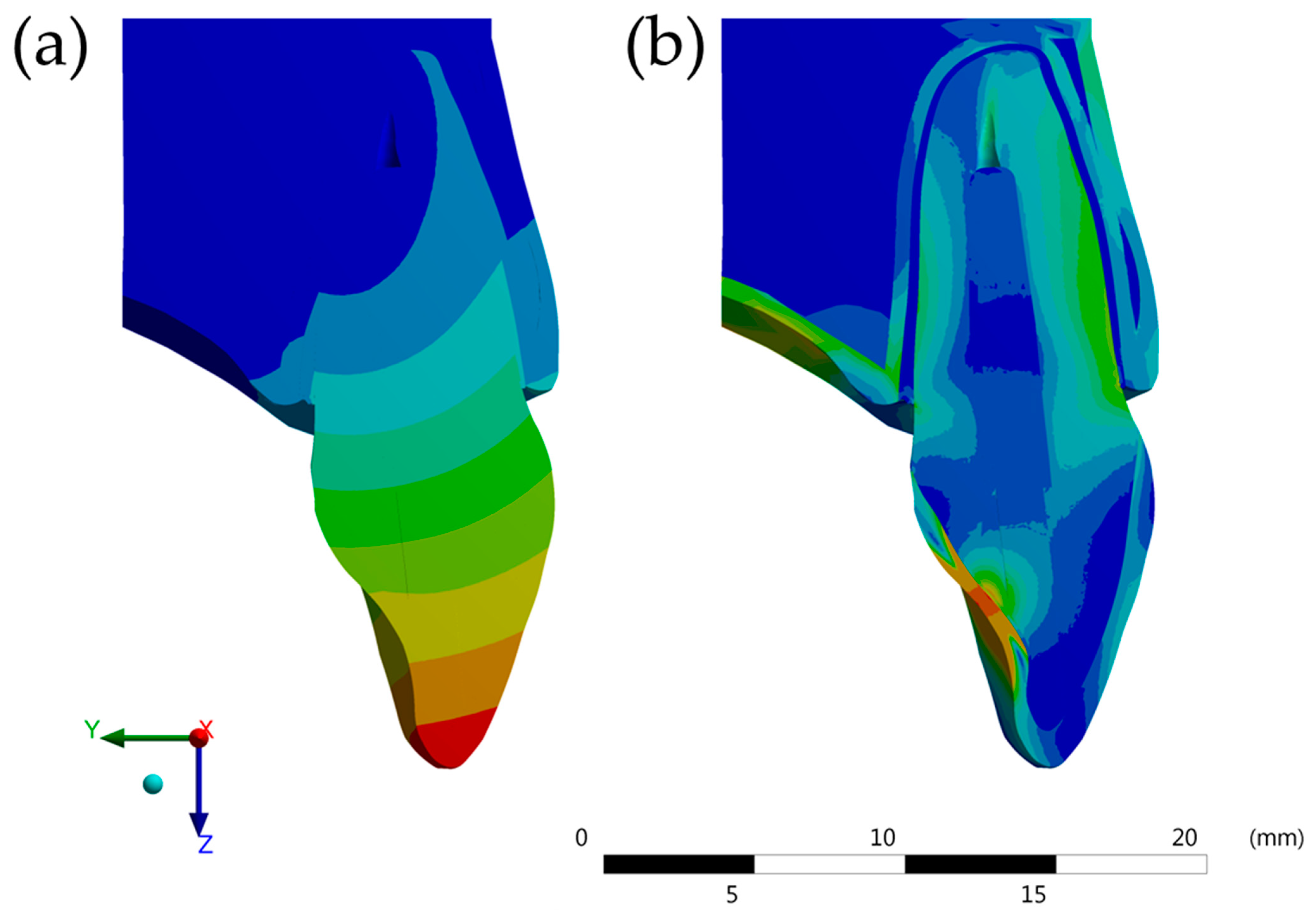
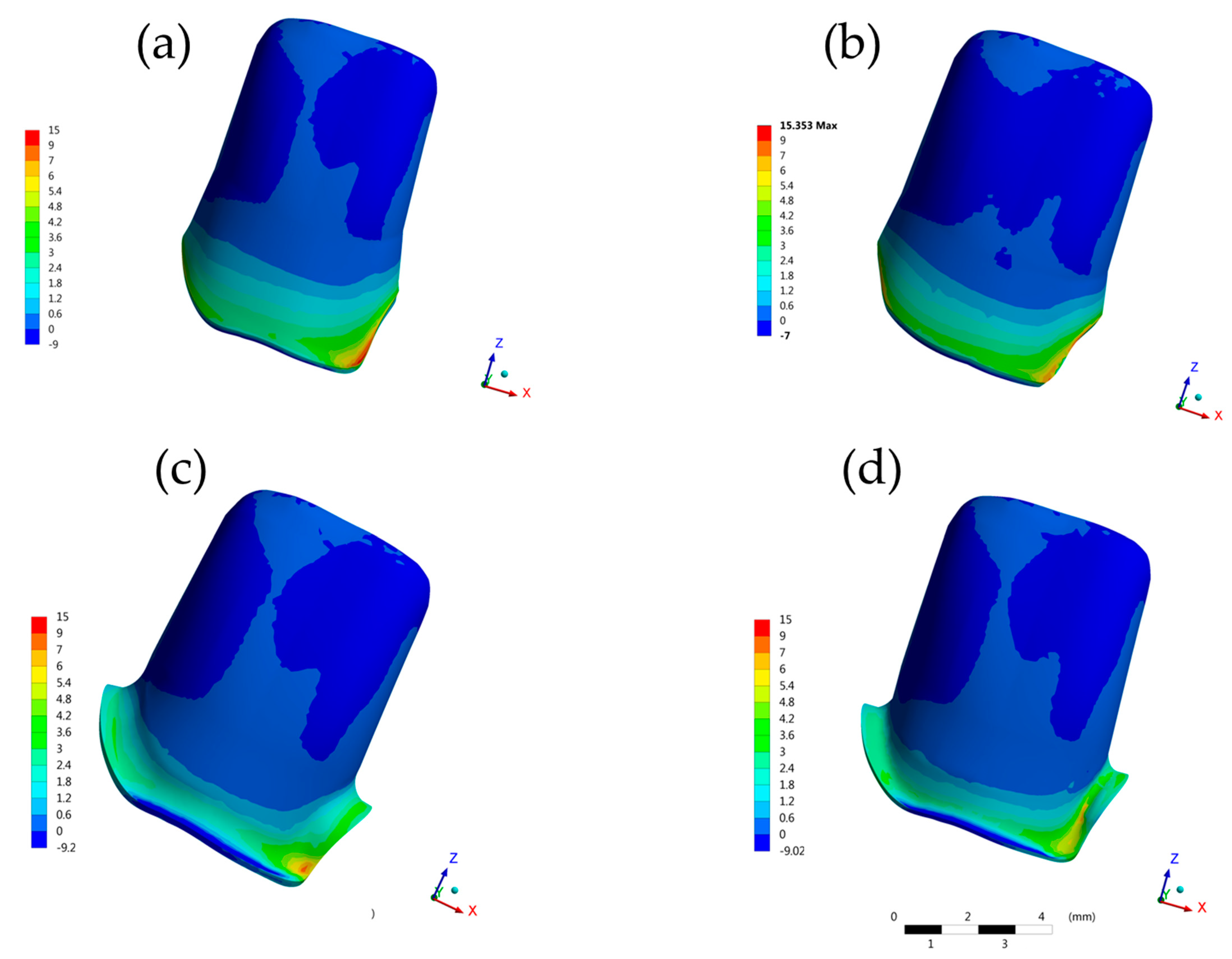
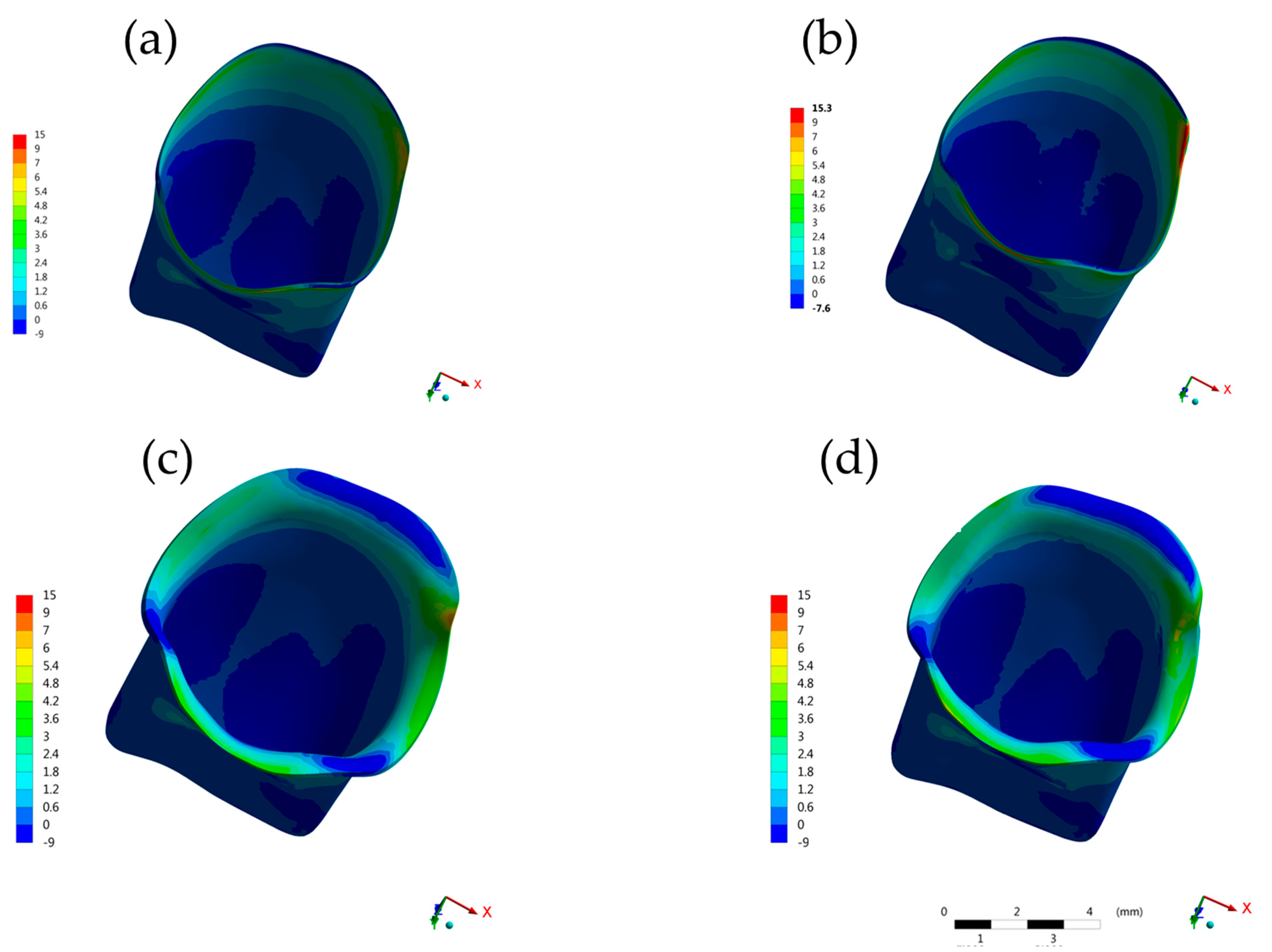
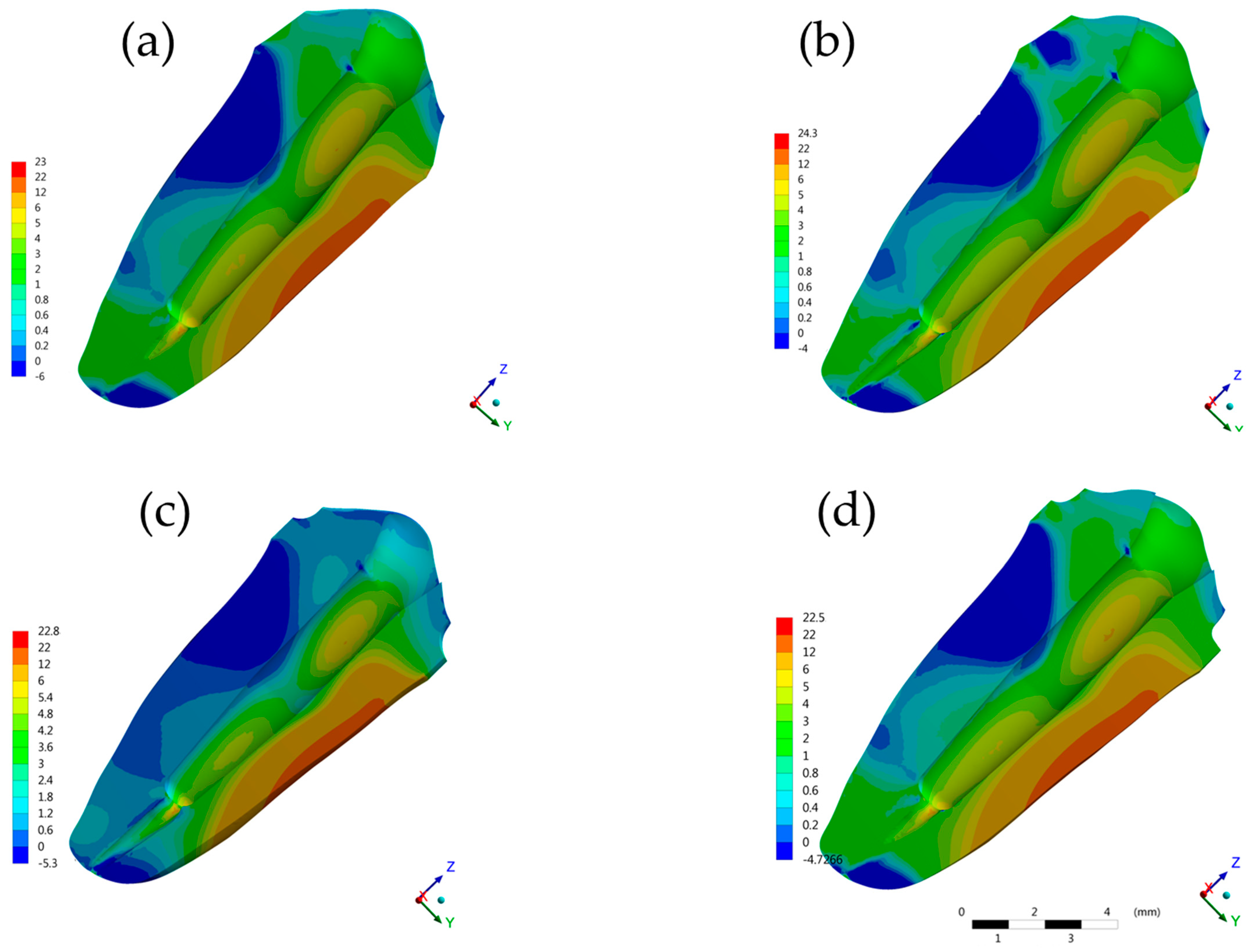
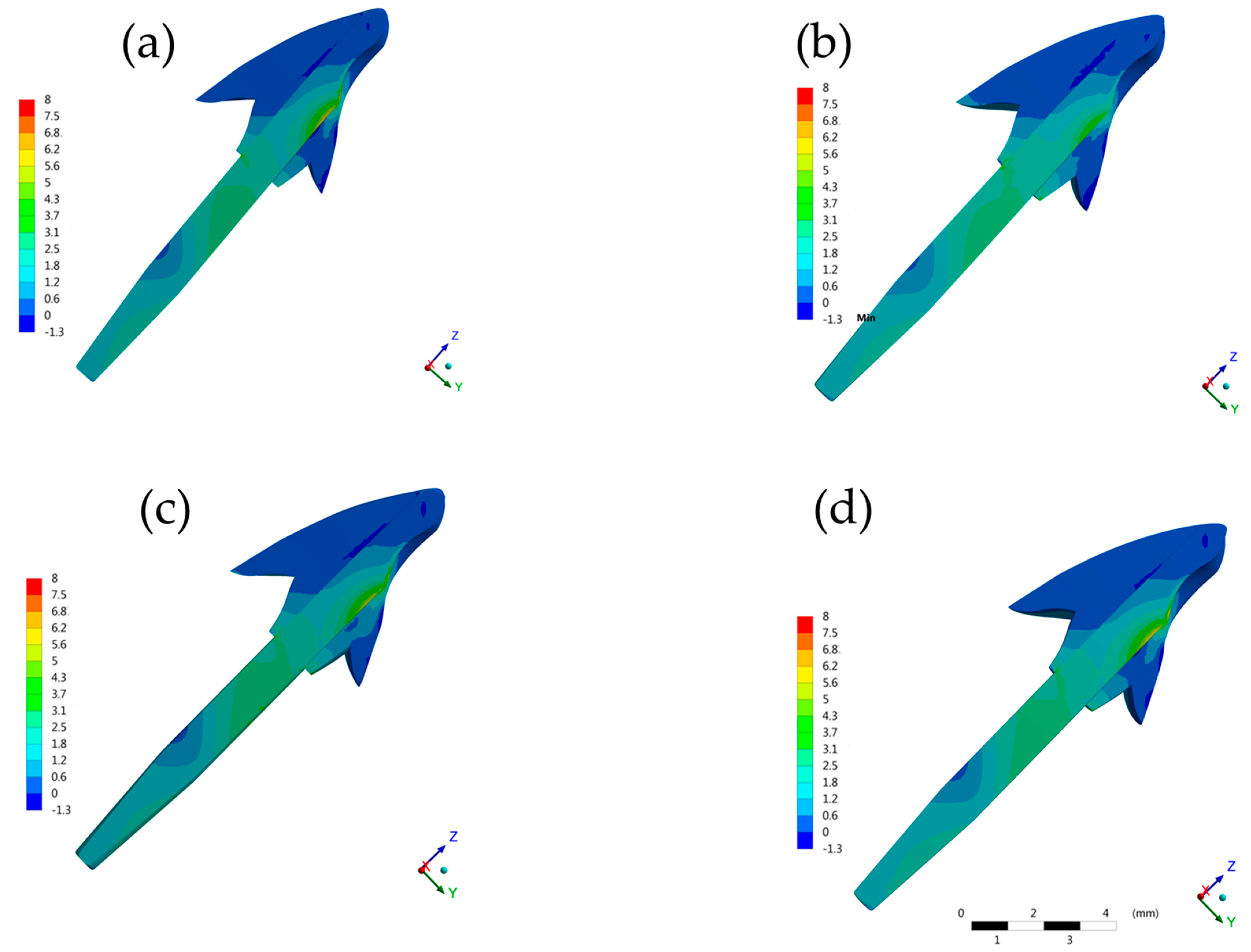
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Sample Availability
References
- Trushkowsky, R.D. Restoration of endodontically treated teeth: Criteria and technique considerations. Quintessence Int. 2014, 45, 557–567. [Google Scholar] [CrossRef]
- Lempel, E.; Lovász, B.V.; Bihari, E.; Krajczár, K.; Jeges, S.; Tóth, Á.; Szalma, J. Long-term clinical evaluation of direct resin composite restorations in vital vs. endodontically treated posterior teeth—Retrospective study up to 13 years. Dent. Mater. 2019, 35, 1308–1318. [Google Scholar] [CrossRef]
- Rocca, G.; Daher, R.; Saratti, C.; Sedláček, R.; Suchy, T.; Feilzer, A.; Krejci, I. Restoration of severely damaged endodontically treated premolars: The influence of the endo-core length on marginal integrity and fatigue resistance of lithium disilicate CAD-CAM ceramic endocrowns. J. Dent. 2018, 68, 41–50. [Google Scholar] [CrossRef]
- Da Silva Alves Santos, T.; Abu Hasna, A.; Abreu, R.T.; Tribst, J.P.M.; de Andrade, G.S.; Borges, A.L.S.; Torres, C.R.G.; Carvalho, C.A.T. Fracture resistance and stress distribution of weakened teeth reinforced with a bundled glass fiber–reinforced resin post. Clin. Oral Investig. 2021, 1–11. [Google Scholar] [CrossRef]
- Penteado, M.M.; de Andrade, G.S.; Araujo, R.M.; Borges, A.L.S.; Valandro, L.F.; Pereira, G.K.R.; da Silva, J.M.F. Fatigue survival of endodontically treated teeth restored with different fiber-reinforced composite resin post strategies versus universal 2-piece fiber post system: An in vitro study. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef]
- Skupien, J.A.; Cenci, M.S.; Opdam, N.J.; Kreulen, C.; Huysmans, M.-C.; Pereira-Cenci, T. Crown vs. composite for post-retained restorations: A randomized clinical trial. J. Dent. 2016, 48, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Yee, K.; Bhagavatula, P.; Stover, S.; Eichmiller, F.; Hashimoto, L.; MacDonald, S.; Barkley, G. Survival Rates of Teeth with Primary Endodontic Treatment after Core/Post and Crown Placement. J. Endod. 2018, 44, 220–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuntiprawon, M.; Wilson, P.R. The effect of cement thickness on the fracture strength of all-ceramic crowns. Aust. Dent. J. 1995, 40, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Gavelis, J.; Morency, J.; Riley, E.; Sozio, R. The effect of various finish line preparations on the marginal seal and occlusal seat of full crown preparations. J. Prosthet. Dent. 2004, 92, 1–7. [Google Scholar] [CrossRef]
- Yu, H.; Chen, Y.-H.; Cheng, H.; Sawase, T. Finish-line designs for ceramic crowns: A systematic review and meta-analysis. J. Prosthet. Dent. 2019, 122, 22–30.e5. [Google Scholar] [CrossRef]
- Jalalian, E.; Aletaha, N.S. The effect of two marginal designs (chamfer and shoulder) on the fracture resistance of all ceramic restorations, Inceram: An in vitro study. J. Prosthodont. Res. 2010, 55, 121–125. [Google Scholar] [CrossRef] [Green Version]
- Carlini-Júnior, B.; Cecchin, D.; Farina, A.P.; Pereira, G.D.S.; Prieto, L.T.; Paulillo, L.A.M.S. Influence of remaining coronal structure and of the marginal design on the fracture strength of roots restored with cast post and core. Acta Odontol. Scand. 2012, 71, 278–282. [Google Scholar] [CrossRef]
- Abduljabbar, T.; Sherfudhin, H.; Alsaleh, S.; Al-Helal, A.A.; Al-Orini, S.S.; Al-Aql, N.A. Fracture resistance of three post and core systems in endodontically treated teeth restored with all-ceramic crowns. King Saud Univ. J. Dent. Sci. 2012, 3, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Serra-Pastor, B.; Loi, I.; Fons-Font, A.; Solá-Ruíz, M.F.; Agustín-Panadero, R. Periodontal and prosthetic outcomes on teeth prepared with biologically oriented preparation technique: A 4-year follow-up prospective clinical study. J. Prosthodont. Res. 2019, 63, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Agustín-Panadero, R.; Solà, F. Vertical preparation for fixed prosthesis rehabilitation in the anterior sector. J. Prosthet. Dent. 2015, 114, 474–478. [Google Scholar] [CrossRef]
- Loi, I.; Di Felice, A. Biologically oriented preparation technique (BOPT): A new approach for prosthetic restoration of periodontically healthy teeth. Eur. J. Esthet. Dent. 2013, 8, 10–23. [Google Scholar] [PubMed]
- Perestrelo, P.; Bártolo, P.; Paranhos, M.; Noritomi, P.; Silva, J. Cranial Biomechanical Simulation. Procedia CIRP 2013, 5, 305–309. [Google Scholar] [CrossRef]
- Ausiello, P.; Ciaramella, S.; Di Rienzo, A.; Lanzotti, A.; Ventre, M.; Watts, D.C. Adhesive class I restorations in sound molar teeth incorporating combined resin-composite and glass ionomer materials: CAD-FE modeling and analysis. Dent. Mater. 2019, 35, 1514–1522. [Google Scholar] [CrossRef] [PubMed]
- Martorelli, M.; Ausiello, P. A novel approach for a complete 3D tooth reconstruction using only 3D crown data. Int. J. Interact. Des. Manuf. (IJIDeM) 2013, 7, 125–133. [Google Scholar] [CrossRef]
- Ausiello, P.; Piva, A.D.; Borges, A.; Lanzotti, A.; Zamparini, F.; Epifania, E.; Tribst, J.M. Effect of Shrinking and No Shrinking Dentine and Enamel Replacing Materials in Posterior Restoration: A 3D-FEA Study. Appl. Sci. 2021, 11, 2215. [Google Scholar] [CrossRef]
- Sherfudhin, H.; Hobeich, J.; Carvalho, C.A.; Aboushelib, M.N.; Sadig, W.; Salameh, Z. Effect of different ferrule designs on the fracture resistance and failure pattern of endodontically treated teeth restored with fiber posts and all-ceramic crowns. J. Appl. Oral Sci. 2011, 19, 28–33. [Google Scholar] [CrossRef]
- De Oliverira Dal Piva, A.M.; Tribst, J.P.M.; de Assunção e Souza, R.O.; Souto Borges, A.L. Influence of Alveolar Bone Loss and Cement Layer Thickness on the Biomechanical Behavior of Endodontically Treated Maxillary Incisors: A 3-dimensional Finite Element Analysis. J. Endod. 2017, 43, 791–795. [Google Scholar] [CrossRef] [Green Version]
- Lang, N.P. Periodontal considerations in prosthetic dentistry. Periodontol. 2000 1995, 9, 118–131. [Google Scholar] [CrossRef] [PubMed]
- Giudice, R.L.; Lizio, A.; Cervino, G.; Fabiana, N.; Francesco, P.; Ausiello, P.; Cicciù, M. The Horizontal Root Fractures. Diagnosis, Clinical Management and Three-Year Follow-Up. Open Dent. J. 2018, 12, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Comlekoglu, M.; Dundar, M.; Özcan, M.; Gungor, M.; Gokce, B.; Artunç, C. Influence of Cervical Finish Line Type on the Marginal Adaptation of Zirconia Ceramic Crowns. Oper. Dent. 2009, 34, 586–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizonaki, M.; Jacquet, W.; Bottenberg, P.; Depla, L.; Boone, M.; De Coster, P.J. Evaluation of marginal and internal fit of lithium disilicate CAD-CAM crowns with different finish lines by using a micro-CT technique. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef]
- Hunter, A.; Hunter, A. Gingival crown margin configurations: A review and discussion. Part I: Terminology and widths. J. Prosthet. Dent. 1990, 64, 548–552. [Google Scholar] [CrossRef]
- Hunter, A. Gingival margins for crowns: A review and discussion. Part II: Discrepancies and configurations. J. Prosthet. Dent. 1990, 64, 636–642. [Google Scholar] [CrossRef]
- Euán, R.; Figueras-Álvarez, O.; Cabratosa-Termes, J.; Barberà, M.B.-D.; Gomes-Azevedo, S. Comparison of the Marginal Adaptation of Zirconium Dioxide Crowns in Preparations with Two Different Finish Lines. J. Prosthodont. 2012, 21, 291–295. [Google Scholar] [CrossRef]
- Quintas, A.F.; Oliveira, F.; Bottino, M.A. Vertical marginal discrepancy of ceramic copings with different ceramic materials, finish lines, and luting agents: An in vitro evaluation. J. Prosthet. Dent. 2004, 92, 250–257. [Google Scholar] [CrossRef]
- Subasi, G.; Ozturk, N.; Inan, O.; Bozogullari, N. Evaluation of marginal fit of two all-ceramic copings with two finish lines. Eur. J. Dent. 2012, 6, 163–168. [Google Scholar]
- Molin, M.K.; Karlsson, S.L.; Kristiansen, M.S. Influence of film thickness on joint bend strength of a ceramic/resin composite joint. Dent. Mater. 1996, 12, 245–249. [Google Scholar] [CrossRef]
- De Carvalho, A.G.; de Andrade, G.; Tribst, J.M.; Grassi, E.; Ausiello, P.; Saavedra, G.; Bressane, A.; de Melo, R.M.; Borges, A. Mechanical Behavior of Different Restorative Materials and Onlay Preparation Designs in Endodontically Treated Molars. Materials 2021, 14, 1923. [Google Scholar] [CrossRef] [PubMed]
- Tribst, J.P.M.; Dal Piva, A.M.O.; de Jager, N.; Bottino, M.A.; de Kok, P.; Kleverlaan, C.J. Full-Crown Versus Endocrown Approach: A 3D-Analysis of Both Restorations and the Effect of Ferrule and Restoration Material. J. Prosthodont. 2020, 28, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Ausiello, P.P.; Ciaramella, S.; Lanzotti, A.; Ventre, M.; Borges, A.; Tribst, J.P.; Piva, A.D.; Garcia-Godoy, F. Mechanical behavior of Class I cavities restored by different material combinations under loading and polymerization shrinkage stress. A 3D-FEA study. Am. J. Dent. 2019, 32, 55–60. [Google Scholar] [PubMed]
- Kasem, A.T.; Sakrana, A.A.; Ellayeh, M.; Özcan, M. Evaluation of zirconia and zirconia-reinforced glass ceramic systems fabricated for minimal invasive preparations using a novel standardization method. J. Esthet. Restor. Dent. 2020, 32, 560–568. [Google Scholar] [CrossRef]
- Reich, S.; Petschelt, A.; Lohbauer, U. The effect of finish line preparation and layer thickness on the failure load and fractography of ZrO2 copings. J. Prosthet. Dent. 2008, 99, 369–376. [Google Scholar] [CrossRef]
- Beuer, F.; Aggstaller, H.; Edelhoff, D.; Gernet, W. Effect of Preparation Design on the Fracture Resistance of Zirconia Crown Copings. Dent. Mater. J. 2008, 27, 362–367. [Google Scholar] [CrossRef] [Green Version]
- De Andrade, G.S.; Tribst, J.P.M.; Orozco, E.I.; Augusto, M.G.; Bottino, M.A.; Borges, A.L.; Anami, L.C.; Saavedra, G.D. Influence of different post-endodontic restoration on the fatigue survival and biomechanical behavior of central incisors. Am. J. Dent. 2020, 33, 227–234. [Google Scholar]
- Raedel, M.; Fiedler, C.; Jacoby, S.; Boening, K.W. Survival of teeth treated with cast post and cores: A retrospective analysis over an observation period of up to 19.5 years. J. Prosthet. Dent. 2015, 114, 40–45. [Google Scholar] [CrossRef]
- Baba, N.Z.; Goodacre, C.J.; Daher, T. Restoration of endodontically treated teeth: The seven keys to success. Gen. Dent. 2009, 57, 596–603. [Google Scholar]
- Pantaleón, D.S.; Morrow, B.R.; Cagna, D.R.; Pameijer, C.H.; Garcia-Godoy, F. Influence of remaining coronal tooth structure on fracture resistance and failure mode of restored endodontically treated maxillary incisors. J. Prosthet. Dent. 2018, 119, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, J.A.; Engelman, M.J. Ferrule design and fracture resistance of endodontically treated teeth. J. Prosthet. Dent. 1990, 63, 529–536. [Google Scholar] [CrossRef]
- Borges, A.L.S.; Grangeiro, M.T.V.; de Andrade, G.S.; de Melo, R.M.; Baroudi, K.; Silva-Concilio, L.R.; Tribst, J.P.M. Stress Concentration of Endodontically Treated Molars Restored with Transfixed Glass Fiber Post: 3D-Finite Element Analysis. Materials 2021, 14, 4249. [Google Scholar] [CrossRef] [PubMed]
- Avetisyan, A.; Markaryan, M.; Rokaya, D.; Tovani-Palone, M.; Zafar, M.; Khurshid, Z.; Vardanyan, A.; Heboyan, A. Characteristics of Periodontal Tissues in Prosthetic Treatment with Fixed Dental Prostheses. Molecules 2021, 26, 1331. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, Z.; Tariq, R.; Asiri, F.Y.; Abid, K.; Zafar, M.S. Literature search strategies in dental education and research. J. Taibah Univ. Med Sci. 2021. [Google Scholar] [CrossRef]
- Heboyan, A.; Manrikyan, M.; Zafar, M.; Rokaya, D.; Nushikyan, R.; Vardanyan, I.; Vardanyan, A.; Khurshid, Z. Bacteriological Evaluation of Gingival Crevicular Fluid in Teeth Restored Using Fixed Dental Prostheses: An In Vivo Study. Int. J. Mol. Sci. 2021, 22, 5463. [Google Scholar] [CrossRef] [PubMed]
- Erdemir, A.; Guess, T.M.; Halloran, J.; Tadepalli, S.C.; Morrison, T.M. Considerations for reporting finite element analysis studies in biomechanics. J. Biomech. 2012, 45, 625–633. [Google Scholar] [CrossRef] [Green Version]
- Syed, A.U.Y.; Rokaya, D.; Shahrbaf, S.; Martin, N. Three-Dimensional Finite Element Analysis of Stress Distribution in a Tooth Restored with Full Coverage Machined Polymer Crown. Appl. Sci. 2021, 11, 1220. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Elastic Modulus (GPa) | Poisson’s Ratio | |
|---|---|---|---|
| Dentin | 24.35 | 0.30 | |
| Enamel | 84.82 | 0.30 | |
| Cortical bone | 13.7 | 0.30 | |
| Medullary bone | 1.37 | 0.30 | |
| Periodontal ligament | 0.05 | 0.45 | |
| Resin core build-up | 12.3 | 0.24 | |
| Resin cement | 7 | 0.28 | |
| Zirconia | 210 | 0.30 | |
| Glass fiber post | E | G | |
| X = 37 | XY = 3.1 | XY = 0.27 | |
| Y = 9.5 | XZ = 3.5 | XZ = 0.34 | |
| Z = 9.5 | YZ = 3.1 | YZ = 0.27 | |
| Model | Region | Stress Peak |
|---|---|---|
| BOPT | Crown margin | 51.71 |
| Cervical dentin | 4.38 | |
| BOPTB | Crown margin | 59.04 |
| Cervical dentin | 12.21 | |
| CM | Crown margin | 43.42 |
| Cervical dentin | 7.65 | |
| SM | Crown margin | 40.18 |
| Cervical dentin | 6.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sichi, L.G.B.; Pierre, F.Z.; Arcila, L.V.C.; de Andrade, G.S.; Tribst, J.P.M.; Ausiello, P.; di Lauro, A.E.; Borges, A.L.S. Effect of Biologically Oriented Preparation Technique on the Stress Concentration of Endodontically Treated Upper Central Incisor Restored with Zirconia Crown: 3D-FEA. Molecules 2021, 26, 6113. https://doi.org/10.3390/molecules26206113
Sichi LGB, Pierre FZ, Arcila LVC, de Andrade GS, Tribst JPM, Ausiello P, di Lauro AE, Borges ALS. Effect of Biologically Oriented Preparation Technique on the Stress Concentration of Endodontically Treated Upper Central Incisor Restored with Zirconia Crown: 3D-FEA. Molecules. 2021; 26(20):6113. https://doi.org/10.3390/molecules26206113
Chicago/Turabian StyleSichi, Luigi Giovanni Bernardo, Fernanda Zapater Pierre, Laura Viviana Calvache Arcila, Guilherme Schmitt de Andrade, João Paulo Mendes Tribst, Pietro Ausiello, Alessandro Espedito di Lauro, and Alexandre Luiz Souto Borges. 2021. "Effect of Biologically Oriented Preparation Technique on the Stress Concentration of Endodontically Treated Upper Central Incisor Restored with Zirconia Crown: 3D-FEA" Molecules 26, no. 20: 6113. https://doi.org/10.3390/molecules26206113