
Beneficial Effects of Green Tea EGCG on Skin Wound Healing: A Comprehensive Review
by
Fa-Wei Xu
1,†, 
Ying-Li Lv
2,†,
Yu-Fan Zhong
1,
Ya-Nan Xue
1,
Yong Wang
1,
Li-Yun Zhang
1,
Xian Hu
1 and
Wei-Qiang Tan
1,* 1
Department of Plastic Surgery, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, 3 East Qingchun Road, Hangzhou 310016, China
2
Tea Research Institute, College of Agriculture and Biotechnology, Zhejiang University, Hangzhou 310013, China
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Molecules 2021, 26(20), 6123; https://doi.org/10.3390/molecules26206123
Submission received: 8 September 2021
/
Revised: 2 October 2021
/
Accepted: 4 October 2021
/
Published: 11 October 2021
(This article belongs to the Special Issue Flavor Compounds in Tea: Formation, Transformation and Health Beneficial Effects)
Abstract
:Epigallocatechin gallate (EGCG) is associated with various health benefits. In this review, we searched current work about the effects of EGCG and its wound dressings on skin for wound healing. Hydrogels, nanoparticles, micro/nanofiber networks and microneedles are the major types of EGCG-containing wound dressings. The beneficial effects of EGCG and its wound dressings at different stages of skin wound healing (hemostasis, inflammation, proliferation and tissue remodeling) were summarized based on the underlying mechanisms of antioxidant, anti-inflammatory, antimicrobial, angiogenesis and antifibrotic properties. This review expatiates on the rationale of using EGCG to promote skin wound healing and prevent scar formation, which provides a future clinical application direction of EGCG.
1. Introduction
The skin is the first line of defense against external aggressors. The skin’s integrity can be damaged by trauma, tears, cuts or contusions, resulting in skin wounds. Full-thickness wounds that extend beyond the two layers of skin (dermis and epidermis) heal through a granulation process and scar formation [1]. Scars are apparently distinguished from the surrounding skin (e.g., darker colour, stretched, depressed or raised), and may also have various symptoms such as inflammation, erythema, pruritus and pain. In some cases, pathological scars (e.g., hypertrophic and keloid scars) inevitably form, adversely impacting sufferers’ life quality. In addition, some diseases such as diabetes impede wound healing process through causing long-term inflammation [2]. Wound healing requires suitable environment to promote healing process, e.g., optimal moisture and redox environment [3,4]. Plant polyphenols as natural antioxidant agents are cost-effective alternatives to current pharmacologic therapeutics, which have been formulated or fabricated in wound dressings to improve the conditions for wound healing [5,6].
Green tea is characterized by the high content of polyphenols, which is produced from the tea plant Camellia sinensis. (−)-Epigallocatechin gallate (EGCG) is regarded as the most abundant compound in tea leaves with excellent bioactivities, such as antioxidant/free radical scavenging [7], anti-inflammatory and antimicrobial properties [8,9]. However, the clinical application of EGCG is restricted by its low bioavailability, since EGCG is unstable under the alkalescent condition of the intestinal track and circulatory system [10]. It was reported that a single injection of EGCG hardly accelerated the healing process of the wound on the back of rats [11]. Thus, topical application might be an ideal route to fully achieve the functionalities of EGCG, considering the avoidance of gastrointestinal digestion and less adverse effects on other organs. The potential application of EGCG to skin wound treatment has been investigated, and some positive results in vitro and in vivo have been achieved [12,13,14,15]. The effects of EGCG on wound healing are associated with the application form and the dosage of EGCG, study models and treatment methods.
This review appraises the developments of EGCG-containing wound dressings for skin wounds. The actions of EGCG in different healing processes are elaborated, and the underlying mechanisms are summarized, including anti-inflammatory, antioxidant, antimicrobial, angiogenesis and antifibrotic effects. This review provides a reference for developing EGCG as a wound-healing agent for clinical use.
2. The Application Forms of EGCG to Wound Healing
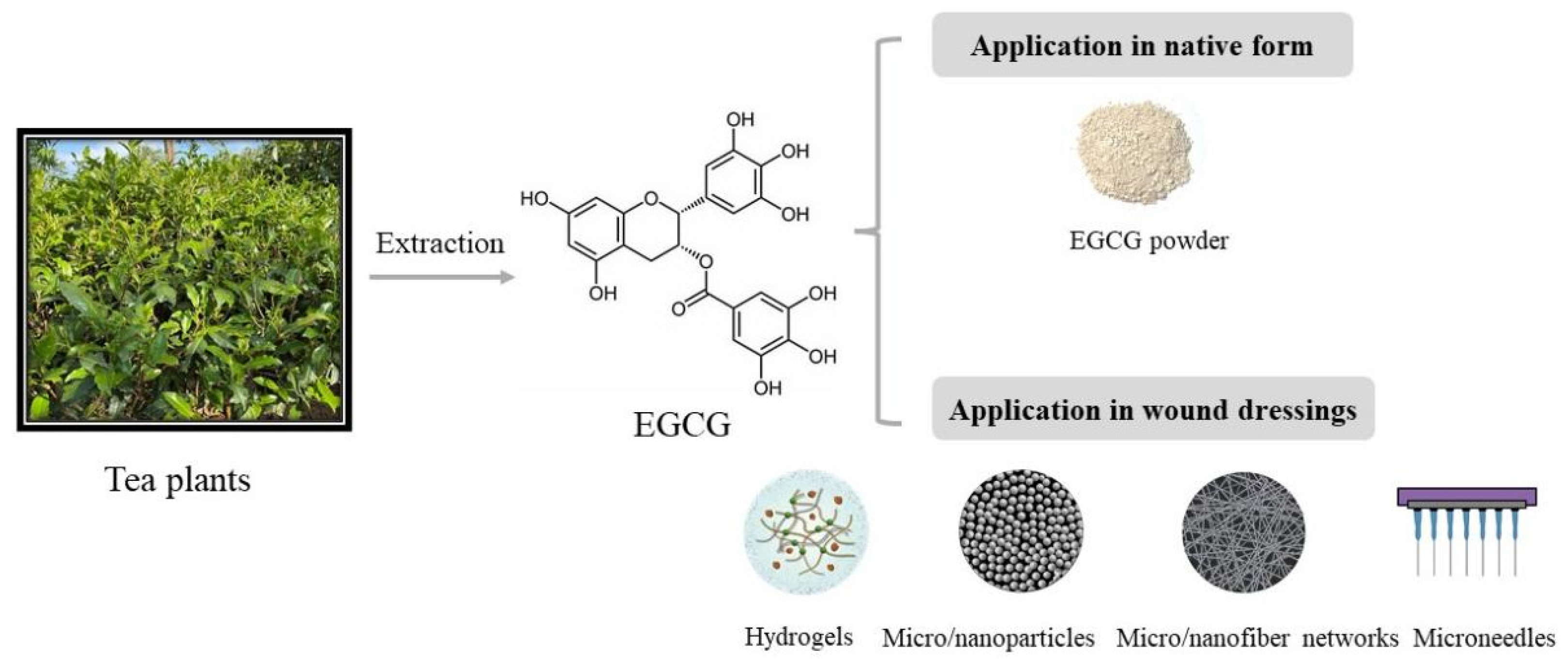
Since many phytonutrients, such as EGCG, are water soluble, neither aqueous solutions nor powders are feasible for clinical applications due to their low adhesion abilities and the limited permeabilities of the skin. Hence, various types of wound dressings have been developed for topical treatments [16,17]. Except for the native form of EGCG used in many studies [13,18], EGCG can also be incorporated into different types of wound dressings, such as hydrogels [19,20], nanoparticles [21,22] and electrospun fibers [23], in order to retain its biofunctionalities and integrate it with the surrounding host tissues [24]. Figure 1 shows the basic application forms of EGCG to skin wound healing. Biomaterials used for cutaneous delivery systems have to meet several requirements, such as biocompatibility, biodegradation, good permeability to moisture and oxygen, good adhesive and infiltrative properties, as well as a reduction in infections and mechanical irritations [25].
Hydrogels are insoluble hydrophilic materials with high water content (70–90%) and a soft elastic property [26] which can be produced from synthetic polymers or natural macromolecule polymers. High-molecular polymers, e.g., poly (methacrylates) and polyvinyl pyrrolidine, are artificial polymers that are widely used, while polysaccharides (e.g., chitosan, hyaluronic acid, alginate and cellulose) and proteins (e.g., collagen, alginate and gelatin) are common natural hydrogels [12]. Hydrogels have been used for translational medicine and sealants with the advantages of better tissue adhesive character [19,27], rapid gelation and injectable properties [28,29] as well as good biocompatibility [30]. EGCG was conjugated with hyaluronic acids, and the conjugates further reacted with tyramine-conjugated hyaluronic acids through tyrosinase to form a crosslinked adhesive hydrogel [20]. A simplified one-pot synthesis method of EGCG–chitosan hydrogels were developed through enzyme-mediated cross-linking [12]. EGCG was copolymerized with 3-acrylamido phenyl boronic acid and acrylamide to form a hydrogel with adequate mechanical properties and tissue adhesiveness [31]. In addition to direct complexation with bioactives, hydrogels can also be used as a carrier of fabricated structures to improve their physical properties, such as nanoparticles.
Microencapsulation is a protective technology of encapsulating bioactives into micro/nanoparticles, with the range of 10 to 100 nm for nanoparticles and a larger range up to 800 μm for microparticles [10,32]. Microencapsulation technology has been widely used in the fields of medicine, functional foods and cosmetics [10,33,34]. Metal nanoparticles, particularly gold, silver and copper nanoparticles or bimetallic nanostructures, showed the excellent potential for wound treatment due to their unique surface and electronic properties. However, the toxicity of metal nanoparticles is still a concern to the public. Nanoparticles are usually carried by other matrices in the forms of ointment, gel or a patch to achieve tissue adhesive, good compatibility and anti-inflammatory properties while reducing cytotoxicity [22,35]. Natural biomacromolecules, such as chitosan and gelatin, are also commonly used materials for constructing microparticles [10]. EGCG–gelatin–chitosan microparticles were constructed and incorporated into a poly(γ-glutamic acid)/gelatin hydrogel to fabricate a sandwiched dressing for enhancing wound regeneration [36]. Nano- and microscale particles fabricated by synthetic polymers such as poly(lactide-co-glycolic acid) (PLGA) were also used for incorporating EGCG to promote wound healing, with the advantages of biocompatibility and a sustainable anti-inflammatory effect [37]. In addition, some growth factors are good candidates for coating in order to endow the recombinant nanoparticles with targeted therapeutic effect in the wound area, for instance, epidermal growth factor (EGF) [38,39].
Networks composed of nano-/micrometer electrospun fibers have been developed for temporary wound dressing, which have the features of porosity, tunable wettability, degradation and biocompatibility [23,40]. Electrospinning technology is used to entrap phenolic compounds within polymer matrices [41], for example, PLGA [23,42], polycaprolactone (PCL)/gelatin nanofibers mats [43] and polysaccharide-based nanofibrous materials [44]. The EGCG-loaded polymer matrices are associated with a sustainable release of EGCG [42], prolonged oxidation [43] and an effect of promoting wound healing [23].
Microneedles have been used for delivering bioactives via the transdermal route [45,46,47]. Microneedle devices can help the bioactives pass through the epidermis, led by these micro-needles [48]. Biomaterials, such as chitosan [49], hyaluronic acid [45] and maltose [46], are used to fabricate microneedles through in situ polymerization using a mold-based technique. Microneedles loaded with green tea extract were prepared and showed the potential therapeutic effect on wound healing based on the antibacterial property [45]. The peptides delivered by poly(ethylene glycol) diacrylate microneedles inhibited the expression of collagen I to suppress the formation of keloid scars [50]. Although there is still no report about the direct application of EGCG-loaded microneedles to skin wound treatment, the microneedle-mediated intradermal delivery system has been used to lead EGCG to deeper skin layers for dermal applications [46], e.g., atopic dermatitis treatment [51]. This implies the great potential of using EGCG-loaded microneedle devices to promote skin wound healing. No matter what topical application forms of EGCG are used, the promoting effects of EGCG on wound healing are based on its basic pharmacological functions.
3. Beneficial Effects of EGCG at Different Healing Stages
The skin wound healing process has four sequential and overlapping stages, including hemostasis, inflammation, proliferation and tissue remodeling [52], which involves various types of cells (e.g., leukocytes, fibroblasts and keratinocytes) and several factors, such as cytokines, chemokines, growth factors and enzymes. These cells and factors are differentially featured at each wound healing stage [53].
Hemostasis happens very quickly after injury, which is accompanied by clotting. As injury occurs, platelets stick together to seal the break in vessel, followed by coagulation and the formation of a platelet plug. In addition, platelet activation also leads to the activation of the immune system and the transition to the inflammatory phase through the release of cytokines and growth factors, such as transforming growth factor β (TGF-β), EGF, platelet-derived growth factor (PDGF) and fibroblast growth factor (FGF) [52,54]. Hemostatic hydrogel is developed for halting bleeding quickly, and good adhesiveness, self-recovery capacity and antibacterial properties are desired [55]. A hemostatic hydrogel was prepared by adding self-assembled keratin–EGCG nanoparticles into cellulose hydrogel, which not only improved the physical properties of pure keratin materials but also exhibited good adhesiveness and hemadsorption [56]. As bleeding is controlled, the inflammatory phase starts, which is characterized by the recruitment of neutrophils, macrophages and lymphocytes.
The inflammatory phase is critical to clear out pathogenic organisms and create a suitable environment for the subsequent tissue repair and regeneration phase [52]. The inflammation phase occurs shortly after injury (first 48 h), which is characterized by the transduction of signaling cascades, the recruitment of neutrophils, monocytes and macrophages at the wound area as well as the release of various growth factors, cytokines and chemokines [53,54]. In the wound environment, neutrophils upregulate the gene expressions of chemokines, such as tumor necrosis factor α (TNFα), interleukin (IL)-1β, IL-6, IL-8, vascular endothelial growth factor (VEGF) and monocyte chemoattractant protein-1 (MCP-1); recruit macrophages, T cells and additional neutrophils; and promote angiogenesis and proliferation of fibroblasts and keratinocytes [52,57]. Monocytes arrive at the wound and differentiate into macrophages or dendritic cells. Macrophages are responsible for phagocytosing apoptotic neutrophils, removing bacteria and dead cells in the wound area and cooperating with neutrophils during the inflammatory phase [58]. Macrophages also secrete cytokines such as PDGF, TGF-β, β-FGF, TNFα, IL-1 and IL-6 [53]. In addition, macrophages phenotypically transit to a reparative state that resolves from inflammation and stimulates keratinocytes and fibroblasts for the subsequential tissue regeneration [54], promoting the transition to the proliferative phase. During the inflammatory phase, neutrophils are the main cells that produce proteases and reactive oxygen species (ROS) that cause cell damage if not properly controlled [54]. EGCG was reported to have the inhibitory effects on the infiltration of neutrophils [59] as well as the migration and adhesion of monocytes [60]. In light of the claimed anti-inflammatory property of EGCG, many studies have been carried out to investigate the inhibitory effect of EGCG alone or combined with other phytonutrients on the generation of pro-inflammatory cytokines (e.g., TNFα, IL-1β, IL-8 and IL-6) in relevant skin cells and the wound tissues of tested animals, and positive results were achieved [11,13,61].
The proliferative phase involves the re-establishment of vessels, the generation of granulation tissue and the re-epithelialization of the wound surface. At this stage, fibroblasts are the major cells involved in the formation of granulation tissue, macrophages are the dominant inflammatory cells during the proliferative phase of skin wound repair [53] and keratinocytes are the predominant cells in the epidermis for epithelialization [62]. The interactions between keratinocytes and fibroblasts are critical for skin repair [63]. The new tissue in the wound area is generated based on collagen and an extracellular matrix (ECM), both of which are mainly synthesized by fibroblasts. Several molecules derived from macrophages, such as TNFα, IL-1 and IL-6, can induce the generation of pro-re-epithelialization molecules in fibroblasts [64]. At the early stage of tissue repair, fibroblasts start to differentiate into α-smooth muscle actin (SMA)-expressing myofibroblasts that actively produce ECM proteins for wound contraction, and myofibroblasts reach a peak number in the proliferation phase [65]. Myofibroblast-induced fibrosis can be overactivated by TGF-β, IL-4 and IL-13 [66]. The long-term overactivation of fibroblasts and myofibroblasts is associated with excessive collagen production and aberrant scar formation [67], and the TGF-β/Smad signaling pathway is regarded as a canonical pathway of regulating the collagen formation in fibroblasts and myofibroblasts [67]. EGCG upregulated the gene expression of klotho in normal human epidermal keratinocytes through protein kinase A (PKA)-cAMP responsive element-binding protein (CREB) signaling, leading to the differentiation of keratinocytes [68]. EGCG mediated the TGF-β1-induced collagen contraction in fibroblasts through suppressing myofibroblast differentiation and reducing the gene expressions of connective tissue growth factor and collagen type I gene [69]. In a human keloid organ culture, EGCG reduced the generation of collagen-I and -III at the transcriptional and protein levels, depleted the mast cells and decreased the cellularity and blood vessel count after 4 weeks of treatment [70]. The animal studies showed that the applications of EGCG and their wound dressings promoted the wound healing process [36,59,71]. An EGCG/PLGA membrane treatment greatly improved the infiltration of surrounding cells and increased the immunoreactivity of Ki-67 (re-epithelialization marker) and CD 31 (blood vessel formation marker) at the wound site of nude mice, implying that EGCG/PLGA membrane treatment is beneficial to wound healing by promoting cell infiltration, re-epithelialization and angiogenesis [23]. The gelatin and chitosan nanoparticles of EGCG and ascorbic acid have promoting effects on collagen accumulation and angiogenesis but an inhibitory effect on the infiltration of inflammatory cells at the wound area of diabetic mice [72]. The in vivo study showed an EGCG-containing sandwiched dressing facilitated wound tissue regeneration and accelerated the healing process [36]. An accelerated skin regeneration was also observed in the treatment with EGCG–chitosan hydrogels [12]. EGCG exerted a blocking effect on the TGF-β1/Smad signal transduction in anaplastic thyroid carcinoma cells [73], suggesting its prospect of suppressing the formation of aberrant scars.
Remodeling refers to the transition process from granulation tissue to scar, which can last up to a year. This progress involves the clean-up of inflammatory cells, the deceleration of angiogenesis and the replacement of type III collagen in granulation tissues with type I collagen. Paralleled fibrils are formed, leading to a low cellularity scar. Myofibroblasts are responsible for carefully coordinating the breakdown of the granulation tissue and its replacement with the stronger type I collagen [52,74], which progressively vanish in the later remodeling phase. The impact of EGCG on scar maturation is still not clear. Table 1 lists the roles of EGCG and its wound dressings in the biophysiological events during the wound healing process. EGCG has various positive effects on wound healing at the stages of inflammation and proliferation.
4. Mechanisms Underlying the Beneficial Effects of EGCG on Skin Wound Healing
4.1. Antioxidant Effect
Reactive oxygen species (ROS) exert adverse effects on cells and tissues. Generally, low ROS levels are conducive to the activation of cell signaling pathways and angiogenesis, whereas high ROS levels induce oxidative stress and compromise tissue repair, leading to chronic nonhealing wounds accompanied by inflammation [76]. Abundant phytonutrients, also known as natural antioxidants/free radical scavengers, are able to protect tissues from oxidative damage. The antioxidant effect of EGCG as a bioactive component during skin wound healing has been testified in both cell and animal studies.
H2O2, UV radiation and chemical reagents, such as Rosup agent, can be used to induce the oxidative stress of skin cells [31,43,77]. In a H2O2-induced human dermal fibroblast injury, EGCG exerted antioxidant ability by enhancing the activities of superoxide dismutase (SOD) and plasma glutathione peroxidase (GSH-Px) while decreasing the malonaldehyde (MDA) level [77]. The EGCG released from polycaprolactone/gelatin nanofibers scavenged the toxic ROS species produced by the human fetal foreskin fibroblasts as exposed to either H2O2 or UV radiation and also reduced the oxidative damage to the growth of cells [43]. Zhao et al. (2021) reported that the EGCG-3-acrylamido phenyl boronic acid-acrylamide (EACPA) hydrogel treatment largely reduced the intracellular ROS in the L929 fibroblasts stimulated by Rosup [31].
In the wound tissues of animal models, the enzymes responsible for cytoprotection against oxidative stress are important parameters to evaluate the antioxidant effect of EGCG and its wound dressings in addition to ROS scavenging activity. The application of EGCG, α-lipoic acid and gold nanoparticles mixture (AuEA) to the wound area of BALB/c mice significantly elevated the protein level of SOD in the wound tissue, compared with the vehicle control group [78]. Heme oxygenase 1 (HO-1) is a cytoprotective enzyme responding to cellular stress [79], the induction of which is associated with the efficient wound closure and neovascularization [80]. EGCG significantly elevated the HO-1 protein level compared with the placebo, which showed the great potential for scar therapy applications [15].
4.2. Anti-Inflammatory Effect
Inflammation plays an important role in fighting pathogens and skin wound healing. Table 2 shows the anti-inflammatory effects of EGCG and its wound dressings. Different cell lines are used to establish inflammatory models, including keratinocytes [14], macrophages [20,31], endothelial cells and muscle cells, which are stimulated by lipopolysaccharides (LPS) or TNFα [13,14]. Clearly, EGCG in the native form or in wound dressings exerted inhibition on the generation of certain pro-inflammatory cytokines released to the supernatants of cells, such as TNFα, IL-1β and IL-8 [13,14,20], or downregulated the corresponding gene expressions in cells [31,37]. The anti-inflammatory effect of EGCG was also verified in the animal studies, with reduced levels of IL-1β, TNFα and IL-6 in the wound tissues [13,31]. In addition, the combinational effects of EGCG and other phytonutrients on the anti-inflammatory activity during skin wound healing were also reported [61]. The presence of EGCG in the mixture of ginkgo biloba leaves exerted cumulative downregulating effect on the secretion of IL-8 in the culture supernatants of normal human keratinocytes stimulated with TNFα [61].
The nuclear factor kappa B (NF-κB) pathway plays a crucial role in inflammation [8]. NF-κB can be activated under oxidative stress and translocated to the nucleus, inducing the transcription of the downstream genes such as TNFA, CXCL8 and iNOS. The upregulated gene expressions of TNFA, CXCL8 and iNOS lead to increased levels of TNFα, IL-8 and NO, respectively [8]. The pro-inflammatory effects of certain cytokines (e.g., TNFα and IL-1β) are associated with their abilities to stimulate NF-κB activation. EGCG reduced inflammation in acne by suppressing the NF-κB pathway [81]. The Notch signaling pathway regulates the cell-fate determination during development [82]. EGCG inhibited the LPS-induced inflammation response in mouse macrophages through targeting the Notch signaling pathway [13]. In addition to the verified NF-κB and Notch signal pathways in the skin cells or the wound tissues of animal studies, the roles of inflammation-related signal pathways in skin wound healing, such as mitogen-activated protein kinase (MAPK) and nuclear factor erythroid 2-related factor 2 (Nrf2) [8], are also worthy of investigations.
Different from pro-inflammatory cytokines, IL-4 and IL-10 are the anti-inflammatory cytokines known to suppress pro-inflammatory cytokine production [83]. Zhao et al. used an EGCG-loaded EACPA hydrogel to treat the wound area of diabetic C57BL/6 mice and found that the EGCG-loaded EACPA hydrogel treated wound tissue had higher levels of IL-4 and IL-10 than those of the undressed and Tegaderm film treated groups [31].
There are two phenotypes of macrophages: M1 macrophages (classically activated) and M2 macrophages (alternatively activated). M1 macrophages contribute to inflammation, while M2 macrophages promote collagen synthesis. In the Raw 264.7 macrophage cells simulated with LPS, Arginase-1 (ARG-1), CD163 and CD206, as a functional marker of the M2 phenotype [84,85], were transcriptionally upregulated upon EACPA hydrogel treatment [31]. CD68, as an M1 phenotype marker [86], was downregulated at the protein level in the wound tissue of diabetes mellitus mice treated with AuEA compared to the vehicle control group [59]. Moreover, EGCG or EGCG-containing wound dressing suppressed the responses of immune cells such as monocytes and macrophages in an in vivo mouse skin full defect model [12].
4.3. Antimicrobial Effect
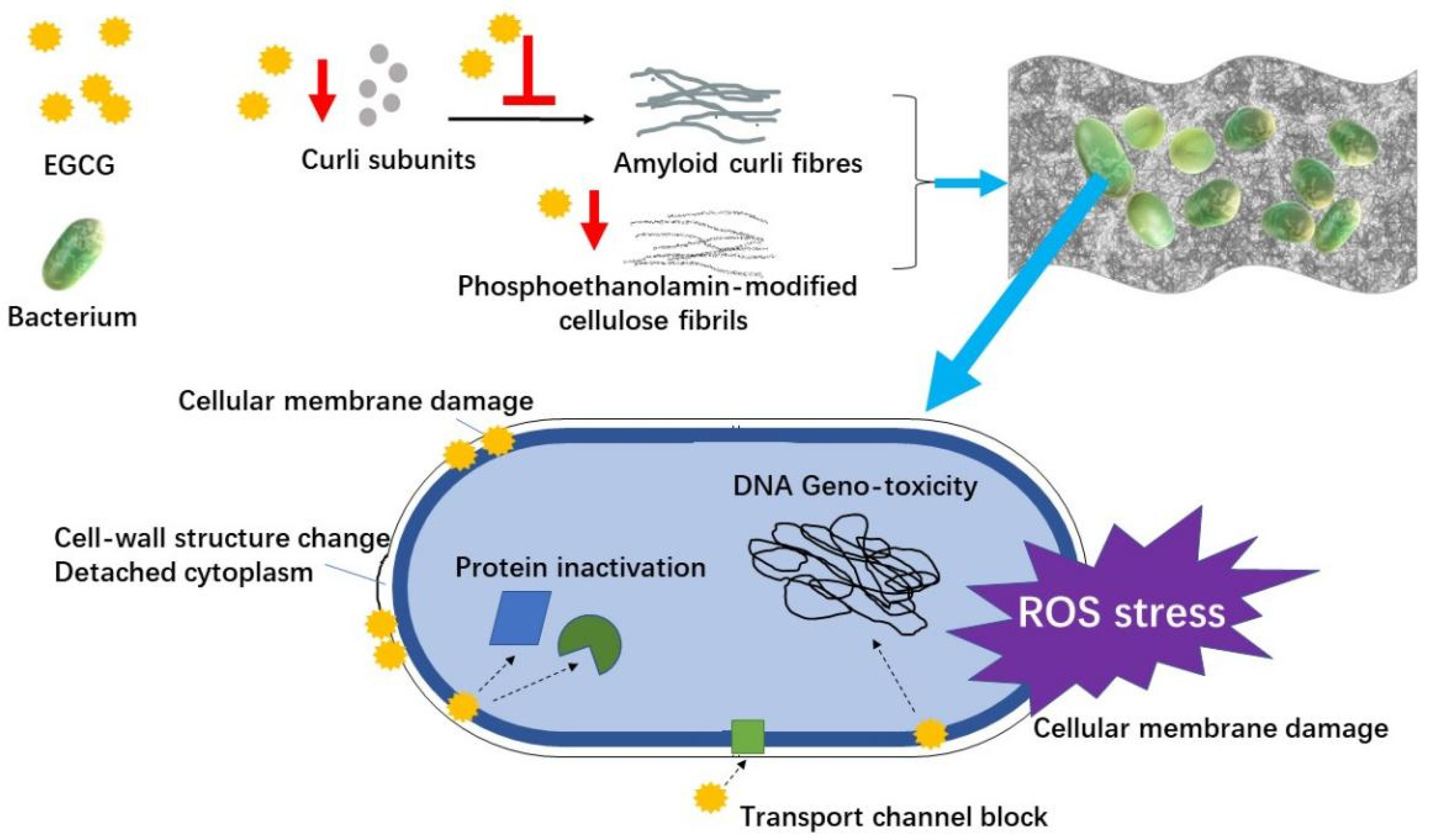
An infection can retard the wound healing process. Diminishing bacterial infection is an effective route to accelerate healing. Pseudomonas aeruginosa, Staphylococcus aureus and Escherichia coli are the common bacteria present in the wound area [22,35], which cause skin infections more frequently in the patients who have hypoimmunity [18]. Most chronic wounds in humans are involved with the formation of bacterial biofilms [87]. Staphylococcus aureus and Pseudomonas aeruginosa are able to form the biofilms that limit the penetration of antimicrobial therapeutics [35,88,89]. Figure 2 shows the antimicrobial mechanism of EGCG in the skin wound healing process, including the antimicrobial effect on bacteria and the inhibitory effect on the formation of biofilms.
Tea extract containing abundant EGCG inhibits the growth of bacteria via various ways, including disrupting cell membranes through interacting with surface proteins, decomposing essential metabolites, inhibiting relevant enzyme, inducing ROS stress, changing cell-wall structure, detaching cytoplasm, and so on [90,91,92,93]. It was reported that EGCG inhibited the glucose uptake of Escherichia coli through the interaction with an outer membrane porin protein, which resulted in the growth inhibition of Escherichia coli [94]. Thioredoxin and thioredoxin reductase are crucial to bacterial DNA synthesis and defense against oxidative stress [95]. EGCG showed an inhibitory efficacy towards thioredoxin and thioredoxin reductase in Staphylococcus aureus and Escherichia coli, leading to the suppressed growth of these pathogens [96]. The antibacterial activity of EGCG-containing gold nanoparticles (AuNPs) against Staphylococcus aureus, Pseudomonas aeruginosa and Escherichia coli was reported, which was attributed to the morphological deformations of bacteria due to the surface interaction with AuNPs [21]. A sandwiched dressing containing gelatin/chitosan/EGCG nanoparticles showed the antimicrobial property against Escherichia coli, Pseudomonas aeruginosa and Staphylococcus aureus [36]. The antibacterial activity was also verified in EGCG-containing hydrogel [12] and EGCG-containing wound patches [22].
Bacterial biofilms, mainly consisting of bacteria, polysaccharides, proteins, and lipids, fabricate a compact structure of hydrated extracellular polymeric substances [35]. EGCG interfered with the assembly of amyloid fibers from curli subunits and the generation of phosphoethanolamin-modified cellulose fibrils, which impeded the formation of biofilms [97,98]. Curli are extracellular protein fiber and functional amyloid aggregates produced by certain bacteria such as Escherichia coli. EGCG reduced the expression of CsgD in Escherichia coli, which is a key activator of curli and cellulose biosynthesis [97]. Highly fibrillation-prone protein FapC is the major component of the functional amyloid produced by many Pseudomonas strains. EGCG exerted an inhibitory effect on the formation of amyloids through aggregating FapC monomers into oligomers [99]. EGCG inhibited the development of biofilm formed by Pseudomonas aeruginosa and reduced the elastase activity, swimming and swarming motility [100]. The biofilm formed by Staphylococcus aureus V329 was disassembled by EGCG [101]. Due to its anti-amyloidogenic property, EGCG is regarded as an effective antimicrobial agent for preventing the formation of biofilms in chronic wound infection [98].
4.4. Angiogenesis Effect
Angiogenesis is the process of new branching network formation, which is mediated by various pro- and antiangiogenic factors. VEGF, as an important proangiogenic factor, can be produced by inflammatory cells [102]. The inflammatory reaction stimulated by TNFα regulates the expression of VEGF [102]. Conversely, VEGF is also involved in the regulation of inflammation, reinforcing the interrelation between inflammation and angiogenesis. The angiogenic effects of EGCG and its wound dressings are shown in Table 2. The topical treatments with EGCG-containing cream impacted the expression of VEGF, which is conducive to the prevention of telangiectasias [103]. The receptor of advanced glycation end products (RAGE) was related to oxidative stress and abnormal angiogenesis in wound healing [104,105]. The topical treatment with AuEA accelerated skin repair in diabetic mice through decreasing the transcription of RAGE and Angiopoietin-2 while increasing the gene expression of VEGF [59]. In the wound tissue of a human study, VEGFA and CD31 were reduced at both the transcriptional and protein levels under zonal priming and direct topical treatment with EGCG in first 1–2 weeks of recovery compared to the placebo control group [15]. The antiangiogenic effects of EGCG was involved in the inhibition of PI3K/AKT and MEK/ERK pathways [106].
4.5. Antifibrotic Effect
Fibrosis is related to abnormal repair in response to chronic tissue damage [107]. It is characterized by an increase in fibrous connective tissues in the dermis or subcutis due to the excessive proliferation of fibroblasts and the formation of collagen fibers. Fibroblasts are mesenchymal cells that play important roles in the fibrosis process. Fibroblasts are related to ECM accumulation and inflammation, contributing to fibrosis pathogenesis [108]. A keloid is a common fibroproliferative disorder related with an abnormal wound healing process [70]. Abnormal collagen synthesis leads to an imbalance in the metabolism of ECM [109]. EGCG greatly inhibited the production of type I collagen in the fibroblasts co-cultured with mast cells [109]. The antifibrotic effect of EGCG was also investigated using the model of human-derived keloid fibroblasts transplanted onto nude mice, and the productions of collagen and keloids were reduced under EGCG treatment. EGCG suppresses the pathological characteristics of keloids through inhibiting the STAT3 signaling pathway [110]. Syed et al. (2013) developed a keloid organ culture model for evaluating the antifibrotic bioactives in scarring and found that EGCG treatment decreased the size of the keloid, suppressed intrakeloid proliferation, reduced collagen production and downregulated the transcription of major fibrosis-related pathways, including VEGF, matrix metalloproteinases (MMP-2 and -9) and TGF-β2 [70]. The PI3K/AKT signaling pathway and the TGF-β signaling pathway play important roles in fibrosis [111,112], however, no relevant regulatory effect of EGCG has been reported yet.
5. Beneficial Effects of EGCG Derivatives on Skin Wound Healing
In addition to microencapsulation, the derivatization of EGCG is an important way to alter the physicochemical properties of EGCG, for example, methylation, alkylation and glycosylation. Epigallocatechin-3-(3″-O-methyl), the methylated derivatives of EGCG, scavenged the free radicals and elevated the expression of HO-1 in the keratinocytes as exposed to H2O2 [113]. Together with antibiotics, the lipid-soluble EGCG-stearate synergistically prevented the formation of biofilms produced by Escherichia coli, Pseudomonas aeruginosa, Staphylococcus aureus, Staphylococcus epidermidis and Mycobacterium smegmatis [114]. The alkylation of EGCG with long alkyl chains elevated its antimicrobial effect, particularly against Staphylococcus aureus [115]. The lipophilic derivatives of EGCG were prepared through the reaction with stearic acid, eicosapentaenoic acid and docosahexaenoic acid, which had a greater 1,1-diphenyl-2-picrylhydrazyl (DPPH) radical scavenging ability compared to EGCG [116]. Two EGCG glycosides were prepared to improve the water stability [117]. Considering the improved stability and enhanced bioactivities after derivatization reactions, the derivatives of EGCG could be used as lipophilic antioxidant or antibacterial agents for clinical usage. This provides a supplementary way of applying EGCG to skin wound repair.
6. Conclusions and Perspective
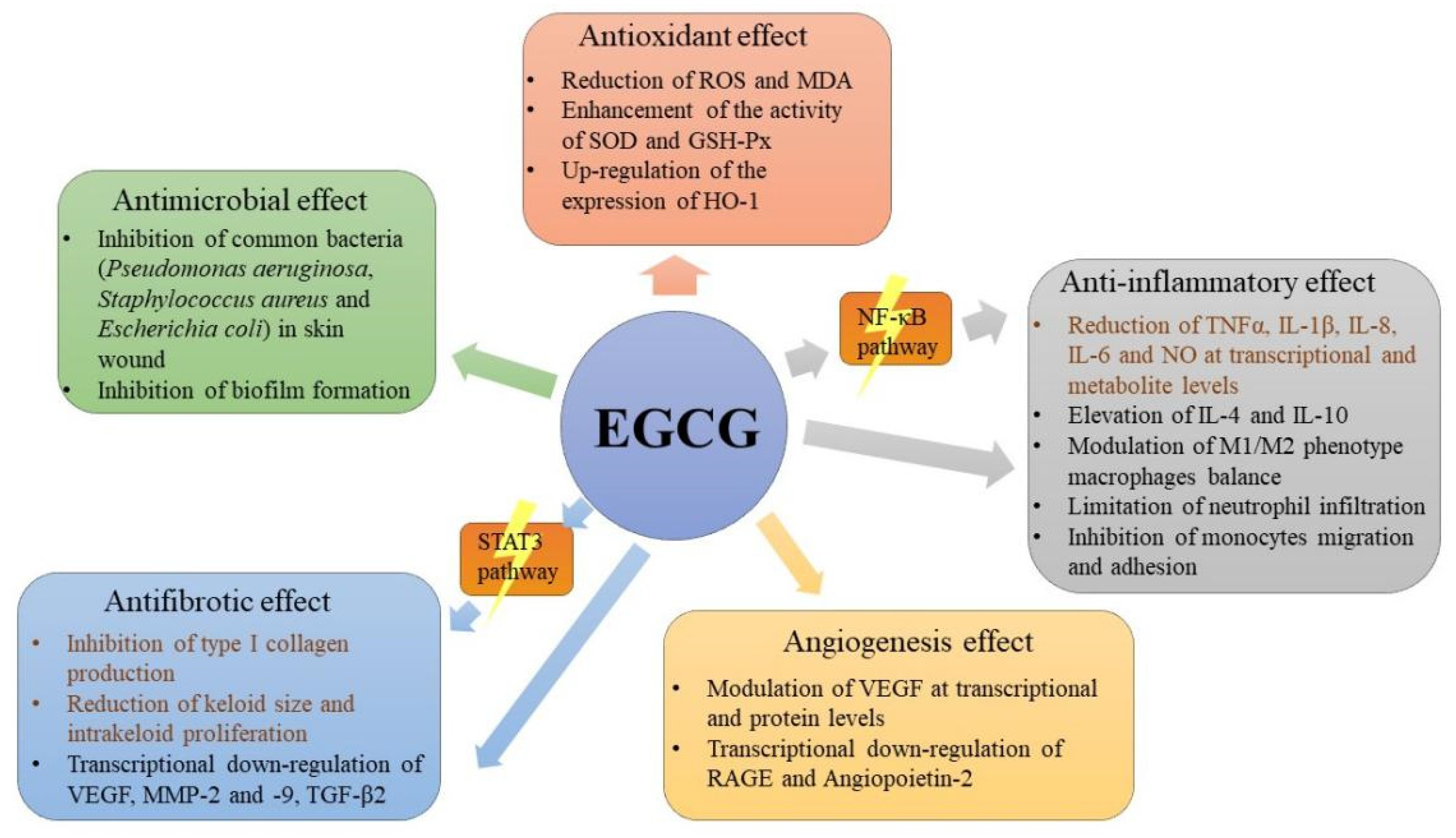
Tea has been known for its various health benefits, such as antioxidant, anti-inflammatory and antimicrobial effects due to the high amounts of catechin compounds, especially EGCG. However, the oral administration application is extremely restricted by the low bioavailability of EGCG. This intrigues the research interest in the potential application of EGCG as a topical treatment. This review summarizes the beneficial effects of EGCG at different skin wound healing stages. In addition to the application of EGCG in its native form, EGCG is also carried by different types of wound dressings to achieve better adhesive and infiltrative properties. EGCG can be carried/fabricated into hydrogels, nanoparticles, micro/nanofiber networks and microneedles. Abundant cell line studies and a few animal studies indicate that EGCG promotes skin wound healing based on its antioxidant, anti-inflammatory, antimicrobial, angiogenesis and antifibrotic effects and its targeting of the inflammation-related NF-κB signal pathway and fibrosis-related STAT3-signaling pathway. The possible mechanisms underlying the beneficial effects of EGCG on skin wound healing are depicted in Figure 3.
Cell line experiments are an important route to investigate the anti-inflammatory effects of bioactives, which can be roughly divided into two groups: one is the cells pretreated with bioactive products and then stimulated with an inflammatory inductor, the other is the cells firstly stimulated with an inflammatory inductor and then treated with bioactive products. Based on the simulation/treatment order, the meaning of the result could be different, which deserves careful addresses in the articles. Various models of cell studies and animal studies are used for investigating the effects of EGCG and its wound dressings on wound healing, which makes it difficult to compare the performance of EGCG-containing formulas. A standard testing method on skin wound healing is in need for evaluations of efficacy and effectiveness. Moreover, the anti-scarring results of EGCG need more evidence from clinical trials to substantiate their benefits on skin wound healing. Considering the anti-inflammatory effect of EGCG, it is postulated that the effect could be optimized if the topical product was applied shortly at an appropriate time after wounding rather than the period of re-epithelialization and a visible scar formation of wounds, which also brings up a future research direction.
Funding
This work was supported by the grants from National Natural Science Foundation of China (No.82172206, 81671918) and Zhejiang Provincial Medical and Healthy Science Foundation of China(2019ZD028).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Delmore, B.; Cohen, J.M.; O’Neill, D.; Chu, A.; Pham, V.; Chiu, E. Reducing postsurgical wound complications: A critical review. Adv. Skin Wound Care 2017, 30, 272–285. [Google Scholar] [CrossRef]
- Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound repair and regeneration. Nature 2008, 453, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Tinti, F.; Soory, M. Mechanisms for redox actions of nicotine and glutathione in cell culture, relevant to periodontitis. Sci. Rep. 2012, 2, 566. [Google Scholar] [CrossRef] [PubMed]
- Messaoud, M.; Marsiquet, C.; Revol-Cavalier, F.; Rat, V.; Marchand, G. Flexible sensors for real-time monitoring of moisture levels in wound dressings. J. Wound Care 2018, 27, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.; Son, K.H.; Chang, H.W.; Kang, S.S.; Kim, H.P. Inhibition of chronic skin inflammation by topical anti-inflammatory flavonoid preparation, Ato Formula (R). Arch. Pharm. Res. 2006, 29, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.Z.; Xu, Z.J.; Liu, G.T.; Wu, J. Polyphenols as a versatile component in tissue engineering. Acta Biomater. 2021, 119, 57–74. [Google Scholar] [CrossRef]
- Fu, N.; Zhou, Z.H.; Jones, T.B.; Tan, T.T.Y.; Wu, W.D.; Lin, S.X.; Chen, X.D.; Chan, P.P.Y. Production of monodisperse epigallocatechin gallate (EGCG) microparticles by spray drying for high antioxidant activity retention. Int. J. Pharm. 2011, 413, 155–166. [Google Scholar] [CrossRef]
- Shi, M.; Wang, Z.S.; Huang, L.Y.; Dong, J.J.; Zheng, X.Q.; Lu, J.L.; Liang, Y.R.; Ye, J.H. Utilization of albumin fraction from defatted rice bran to stabilize and deliver (−)-epigallocatechin gallate. Food Chem. 2020, 311, 125894. [Google Scholar] [CrossRef]
- Gordon, N.C.; Wareham, D.W. Antimicrobial activity of the green tea polyphenol (−)-epigallocatechin-3-gallate (EGCG) against clinical isolates of Stenotrophomonas maltophilia. Int. J. Antimicrob. Agents 2010, 36, 129–131. [Google Scholar] [CrossRef]
- Ye, J.H.; Augustin, M.A. Nano- and micro-particles for delivery of catechins: Physical and biological performance. Crit. Rev. Food Sci. 2019, 59, 1563–1579. [Google Scholar] [CrossRef]
- Li, M.; Xu, J.X.; Shi, T.X.; Yu, H.Y.; Bi, J.P.; Chen, G.Z. Epigallocatechin-3-gallate augments therapeutic effects of mesenchymal stem cells in skin wound healing. Clin. Exp. Pharmacol. Physiol. 2016, 43, 1115–1124. [Google Scholar] [CrossRef]
- Kim, B.S.; Kim, S.H.; Kim, K.; An, Y.H.; So, K.H.; Kim, B.G.; Hwang, N.S. Enzyme-mediated one-pot synthesis of hydrogel with the polyphenol cross-linker for skin regeneration. Mater. Today Bio 2020, 8, 100079. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.W.; Zhu, Q.Q.; Yang, X.Y.; Xu, H.H.; Sun, B.; Wang, X.J.; Sheng, J. Wound healing can be improved by (−)-epigallocatechin gallate through targeting Notch in streptozotocin-induced diabetic mice. FASEB J. 2019, 33, 953–964. [Google Scholar] [CrossRef] [PubMed]
- Trompezinski, S.; Denis, A.; Schmitt, D.; Viac, J. Comparative effects of polyphenols from green tea (EGCG) and soybean (genistein) on VEGF and IL-8 release from normal human keratinocytes stimulated with the proinflammatory cytokine TNF alpha. Arch. Dermatol. Res. 2003, 295, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Ud-Din, S.; Foden, P.; Mazhari, M.; Al-Habba, S.; Baguneid, M.; Bulfone-Paus, S.; McGeorge, D.; Bayat, A. A double-blind, randomized trial shows the role of zonal priming and direct topical application of epigallocatechin-3-gallate in the modulation of cutaneous scarring in human skin. J. Investig. Dermatol. 2019, 139, 1680–1690. [Google Scholar] [CrossRef] [Green Version]
- Hurd, T.; Woodmansey, E.J.; Watkins, H.M.A. A retrospective review of the use of a nanocrystalline silver dressing in the management of open chronic wounds in the community. Int. Wound J. 2021. [Google Scholar] [CrossRef]
- Vivcharenko, V.; Wojcik, M.; Palka, K.; Przekora, A. Highly porous and superabsorbent biomaterial made of marine-derived polysaccharides and ascorbic acid as an optimal dressing for exuding wound management. Materials 2021, 14, 1211. [Google Scholar] [CrossRef]
- Jeon, J.; Kim, J.H.; Lee, C.K.; Oh, C.H.; Song, H.J. The antimicrobial activity of (−)-epigallocatehin-3-gallate and green tea extracts against Pseudomonas aeruginosa and Escherichia coli isolated from skin wounds. Ann. Dermatol. 2014, 26, 564–569. [Google Scholar] [CrossRef] [Green Version]
- Feng, Q.; Wei, K.C.; Lin, S.E.; Xu, Z.; Sun, Y.X.; Shi, P.; Li, G.; Bian, L.M. Mechanically resilient, injectable, and bioadhesive supramolecular gelatin hydrogels crosslinked by weak host-guest interactions assist cell infiltration and in situ tissue regeneration (vol 101, pg 217, 2016). Biomaterials 2017, 112, 346–347. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Kim, K.; Kim, B.S.; An, Y.H.; Lee, U.J.; Lee, S.H.; Kim, S.L.; Kim, B.G.; Hwang, N.S. Fabrication of polyphenol-incorporated anti-inflammatory hydrogel via high-affinity enzymatic crosslinking for wet tissue adhesion. Biomaterials 2020, 242, 119905. [Google Scholar] [CrossRef]
- Avila, S.R.R.; Schuenck, G.P.D.; Silva, L.P.C.E.; Keijok, W.J.; Xavier, L.M.; Endringer, D.C.; Oliveira, J.P.; Schuenck, R.P.; Guimaraes, M.C.C. High antibacterial in vitro performance of gold nanoparticles synthesized by epigallocatechin 3-gallate. J. Mater. Res. 2021, 36, 518–532. [Google Scholar] [CrossRef]
- Kar, A.K.; Singh, A.; Dhiman, N.; Purohit, M.P.; Jagdale, P.; Kamthan, M.; Singh, D.; Kumar, M.; Ghosh, D.; Patnaik, S. Polymer-assisted in situ synthesis of silver nanoparticles with epigallocatechin gallate (EGCG) impregnated wound patch potentiate controlled inflammatory responses for brisk wound healing. Int. J. Nanomed. 2019, 14, 9837–9854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.L.; Lee, J.H.; Kwon, B.J.; Lee, M.H.; Han, D.W.; Hyon, S.H.; Park, J.C. Promotion of full-thickness wound healing using epigallocatechin-3-O-gallate/poly (lactic-co-glycolic acid) membrane as temporary wound dressing. Artif. Organs 2014, 38, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Sridharan, R.; Cameron, A.R.; Kelly, D.J.; Kearney, C.J.; O’Brien, F.J. Biomaterial based modulation of macrophage polarization: A review and suggested design principles. Mater. Today 2015, 18, 313–325. [Google Scholar] [CrossRef]
- Mir, M.; Ali, M.N.; Barakullah, A.; Gulzar, A.; Arshad, M.; Fatima, S.; Asad, M. Synthetic polymeric biomaterials for wound healing: A review. Prog. Biomater. 2018, 7, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhivya, S.; Padma, V.V.; Santhini, E. Wound dressings—A review. Biomedicine 2015, 5, 22. [Google Scholar] [CrossRef]
- Lee, B.P.; Konst, S. Novel hydrogel actuator inspired by reversible mussel adhesive protein chemistry. Adv. Mater. 2014, 26, 3415–3419. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Yan, B.; Yang, J.Q.; Chen, L.Y.; Zeng, H.B. Novel mussel-inspired injectable self-healing hydrogel with anti-biofouling property. Adv. Mater. 2015, 27, 1294–1299. [Google Scholar] [CrossRef]
- Gao, Y.; Li, Z.; Huang, J.; Zhao, M.; Wu, J. In situ formation of injectable hydrogels for chronic wound healing. J. Mater. Chem. B 2020, 8, 8768–8780. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Peppas, N.A. Hydrogels and Scaffolds for Immunomodulation. Adv. Mater. 2014, 26, 6530–6541. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.D.; Pei, D.N.; Yang, Y.X.; Xu, K.; Yu, J.; Zhang, Y.C.; Zhang, Q.; He, G.; Zhang, Y.F.; Li, A.; et al. Green tea derivative driven smart hydrogels with desired functions for chronic diabetic wound treatment. Adv. Funct. Mater. 2021, 31, 2009442. [Google Scholar] [CrossRef]
- Rudramurthy, G.R.; Swamy, M.K. Potential applications of engineered nanoparticles in medicine and biology: An update. J. Biol. Inorg. Chem. 2018, 23, 1185–1204. [Google Scholar] [CrossRef] [PubMed]
- Simovic, S.; Heard, P.; Hui, H.; Song, Y.M.; Peddie, F.; Davey, A.K.; Lewis, A.; Rades, T.; Prestidge, C.A. Dry hybrid lipid-silica microcapsules engineered from submicron lipid droplets and nanoparticles as a novel delivery system for poorly soluble drugs. Mol. Pharm. 2009, 6, 861–872. [Google Scholar] [CrossRef] [PubMed]
- Martins, I.M.; Barreiro, M.F.; Coelho, M.; Rodrigues, A.E. Microencapsulation of essential oils with biodegradable polymeric carriers for cosmetic applications. Chem. Eng. J. 2014, 245, 191–200. [Google Scholar] [CrossRef] [Green Version]
- Permana, A.D.; Anjani, Q.K.; Sartini; Utomo, E.; Volpe-Zanutto, F.; Paredes, A.J.; Evary, Y.M.; Mardikasari, S.A.; Pratama, M.R.; Tuany, I.N.; et al. Selective delivery of silver nanoparticles for improved treatment of biofilm skin infection using bacteria-responsive microparticles loaded into dissolving microneedles. Mat. Sci. Eng. C 2021, 120, 111786. [Google Scholar]
- Lin, Y.H.; Lin, J.H.; Li, T.S.; Wang, S.H.; Yao, C.H.; Chung, W.Y.; Ko, T.H. Dressing with epigallocatechin gallate nanoparticles for wound regeneration. Wound Repair Regen. 2016, 24, 287–301. [Google Scholar] [CrossRef]
- Wu, Y.R.; Choi, H.J.; Kang, Y.G.; Kim, J.K.; Shin, J.W. In vitro study on anti-inflammatory effects of epigallocatechin-3-gallate-loaded nano- and microscale particles. Int. J. Nanomed. 2017, 12, 7007–7013. [Google Scholar] [CrossRef] [Green Version]
- Chu, Y.J.; Yu, D.M.; Wang, P.H.; Xu, J.; Li, D.Q.; Ding, M. Nanotechnology promotes the full-thickness diabetic wound healing effect of recombinant human epidermal growth factor in diabetic rats. Wound Repair Regen. 2010, 18, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Hong, Y.L.; Wu, T.L. Novel silver and nanoparticle-encapsulated growth factor co-loaded chitosan composite hydrogel with sustained antimicrobility and promoted biological properties for diabetic wound healing. Mat. Sci. Eng. C 2021, 118, 111385. [Google Scholar] [CrossRef]
- Locilento, D.A.; Mercante, L.A.; Andre, R.S.; Mattoso, L.H.C.; Luna, G.L.F.; Brassolatti, P.; Anibal, F.D.; Correa, D.S. Biocompatible and biodegradable electrospun nanofibrous membranes loaded with grape seed extract for wound dressing application. J. Nanomater. 2019, 2019, 2472964. [Google Scholar] [CrossRef] [Green Version]
- Khoshnoudi-Nia, S.; Sharif, N.; Jafari, S.M. Loading of phenolic compounds into electrospun nanofibers and electrosprayed nanoparticles. Trends Food Sci. Tech. 2020, 95, 59–74. [Google Scholar] [CrossRef]
- Shin, Y.C.; Shin, D.M.; Lee, E.J.; Lee, J.H.; Kim, J.E.; Song, S.H.; Hwang, D.Y.; Lee, J.J.; Kim, B.; Lim, D.; et al. Hyaluronic acid/PLGA core/shell fiber matrices loaded with EGCG beneficial to diabetic wound healing. Adv. Healthc. Mater. 2016, 5, 3035–3045. [Google Scholar] [CrossRef]
- Pires, F.; Santos, J.F.; Bitoque, D.; Silva, G.A.; Marletta, A.; Nunes, V.A.; Ribeiro, P.A.; Silva, J.C.; Raposo, M. Polycaprolactone/gelatin nanofiber membranes containing EGCG-loaded liposomes and their potential use for skin regeneration. ACS Appl. Bio Mater. 2019, 2, 4790–4800. [Google Scholar] [CrossRef]
- Zemljic, L.F.; Maver, U.; Glaser, T.K.; Bren, U.; Hrncic, M.K.; Petek, G.; Persin, Z. Electrospun composite nanofibrous materials based on (poly)-phenol-polysaccharide formulations for potential wound treatment. Materials 2020, 13, 2631. [Google Scholar] [CrossRef]
- Park, S.Y.; Lee, H.U.; Lee, Y.C.; Kim, G.H.; Park, E.C.; Han, S.H.; Lee, J.G.; Choi, S.; Heo, N.S.; Kim, D.L.; et al. Wound healing potential of antibacterial microneedles loaded with green tea extracts. Mat. Sci. Eng. C 2014, 42, 757–762. [Google Scholar] [CrossRef]
- Puri, A.; Nguyen, H.X.; Banga, A.K. Microneedle-mediated intradermal delivery of epigallocatechin-3-gallate. Int. J. Cosmet. Sci. 2016, 38, 512–523. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Yadav, S. Microneedling: Advances and widening horizons. Indian Dermatol. Online J. 2016, 7, 244–254. [Google Scholar] [PubMed]
- Waghule, T.; Singhvi, G.; Dubey, S.K.; Pandey, M.M.; Gupta, G.; Singh, M.; Dua, K. Microneedles: A smart approach and increasing potential for transdermal drug delivery system. Biomed. Pharmacother. 2019, 109, 1249–1258. [Google Scholar] [CrossRef] [PubMed]
- Chi, J.J.; Zhang, X.X.; Chen, C.W.; Shao, C.M.; Zhao, Y.J.; Wang, Y.G. Antibacterial and angiogenic chitosan microneedle array patch for promoting wound healing. Bioact. Mater. 2020, 5, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.Y.; Yeo, D.C.; Wiraja, C.; Tey, H.L.; Mrksich, M.; Xu, C.J. Peptide delivery with poly(ethylene glycol) diacrylate microneedles through swelling effect. Bioeng. Transl. Med. 2017, 2, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Chiu, Y.H.; Wu, Y.W.; Hung, J.I.; Chen, M.C. Epigallocatechin gallate/L-ascorbic acid-loaded poly-gamma-glutamate microneedles with antioxidant, anti-inflammatory, and immunomodulatory effects for the treatment of atopic dermatitis. Acta Biomater. 2021, 130, 223–233. [Google Scholar] [CrossRef]
- Ellis, S.; Lin, E.J.; Tartar, D. Immunology of wound healing. Curr. Dermatol. Rep. 2018, 7, 350–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canedo-Dorantes, L.; Canedo-Ayala, M. Skin acute wound healing: A comprehensive review. Int. J. Inflamm. 2019, 2019, 3706315. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; DiPietro, L.A. Factors affecting woundhealing. J. Dent. Res. 2010, 89, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Dai, L.; Si, C.L.; Zeng, Z.G. Antibacterial and hemostatic hydrogel via nanocomposite from cellulose nanofibers. Carbohydr. Polym. 2018, 195, 63–70. [Google Scholar] [CrossRef]
- Sun, Z.; Chen, X.; Ma, X.; Cui, X.; Yi, Z.; Li, X. Cellulose/keratin–catechin nanocomposite hydrogel for wound hemostasis. J. Mater. Chem. B 2018, 6, 6133–6141. [Google Scholar] [CrossRef]
- Theilgaard-Monch, K.; Knudsen, S.; Follin, P.; Borregaard, N. The transcriptional activation program of human neutrophils in skin lesions supports their important role in wound healing. J. Immunol. 2004, 172, 7684–7693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosique, R.G.; Rosique, M.J.; Farina, J.A. Curbing inflammation in skin wound healing: A review. Int. J. Inflamm. 2015, 2015, 316235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.A.; Chen, H.M.; Yao, Y.D.; Hung, C.F.; Tu, C.S.; Liang, Y.J. Topical treatment with anti-oxidants and Au nanoparticles promote healing of diabetic wound through receptor for advance glycation end-products. Eur. J. Pharm. Sci. 2012, 47, 875–883. [Google Scholar] [CrossRef]
- Melgarejo, E.; Medina, M.A.; Sanchez-Jimenez, F.; Urdiales, J.L. Epigallocatechin gallate reduces human monocyte mobility and adhesion in vitro. Br. J. Pharmacol. 2009, 158, 1705–1712. [Google Scholar] [CrossRef] [Green Version]
- Trompezinski, S.; Bonneville, M.; Pernet, I.; Denis, A.; Schmitt, D.; Viac, J. Gingko biloba extract reduces VEGF and CXCL-8/IL-8 levels in keratinocytes with cumulative effect with epigallocatechin-3-gallate. Arch. Dermatol. Res. 2010, 302, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Shin, Y.K.; Kim, K.Y. Promotion of keratinocyte proliferation by tracheloside through ERK1/2 Stimulation. Evid.-Based Complementary Altern. Med. 2018, 2018, 4580627. [Google Scholar] [CrossRef] [PubMed]
- Seo, G.Y.; Lim, Y.; Koh, D.; Huh, J.S.; Hyun, C.; Kim, Y.M.; Cho, M. TMF and glycitin act synergistically on keratinocytes and fibroblasts to promote wound healing and anti-scarring activity. Exp. Mol. Med. 2017, 49, e302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takehara, K. Growth regulation of skin fibroblasts. J. Dermatol. Sci. 2000, 24, S70–S77. [Google Scholar] [CrossRef]
- Darby, I.A.; Laverdet, B.; Bonte, F.; Desmouliere, A. Fibroblasts and myofibroblasts in wound healing. Clin. Cosmet. Investig. Dermatol. 2014, 7, 301–311. [Google Scholar] [PubMed] [Green Version]
- Hinz, B. The role of myofibroblasts in wound healing. Curr. Res. Transl. Med. 2016, 64, 171–177. [Google Scholar] [CrossRef]
- Zhang, T.; Wang, X.F.; Wang, Z.C.; Lou, D.; Fang, Q.Q.; Hu, Y.Y.; Zhao, W.Y.; Zhang, L.Y.; Wu, L.H.; Tan, W.Q. Current potential therapeutic strategies targeting the TGF-beta/Smad signaling pathway to attenuate keloid and hypertrophic scar formation. Biomed. Pharmacother. 2020, 129, 110287. [Google Scholar] [CrossRef]
- Kim, H.J.; Chang, H.; Han, S.H.; Lee, M.S.; Jung, J.Y.; An, S.; Baek, S.Y.; Lee, J.H.; Lee, J.H.; Lee, T.R.; et al. Epigallocatechin-3-O-(3-O-methyl)-gallate-induced differentiation of human keratinocytes involves Klotho-mediated regulation of protein kinase-cAMP responsive element-binding protein signaling. Int. J. Mol. Sci. 2014, 15, 5749–5761. [Google Scholar] [CrossRef] [Green Version]
- Klass, B.R.; Branford, O.A.; Grobbelaar, A.O.; Rolfe, K.J. The effect of epigallocatechin-3-gallate, a constituent of green tea, on transforming growth factor-beta 1-stimulated wound contraction. Wound Repair Regen. 2010, 18, 80–88. [Google Scholar] [CrossRef]
- Syed, F.; Bagabir, R.A.; Paus, R.; Bayat, A. Ex vivo evaluation of antifibrotic compounds in skin scarring: EGCG and silencing of PAI-1 independently inhibit growth and induce keloid shrinkage. Lab. Investig. 2013, 93, 946–960. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.H.; Chen, C.Y.; Chen, P.J.; Tan, S.W.; Chen, C.N.; Chen, H.M.; Tu, C.S.; Liang, Y.J. Gas-injection of gold nanoparticles and anti-oxidants promotes diabetic wound healing. RSC Adv. 2014, 4, 4656–4662. [Google Scholar] [CrossRef]
- Sun, M.H.; Xie, Q.J.; Cai, X.Q.; Liu, Z.H.; Wang, Y.; Dong, X.; Xu, Y. Preparation and characterization of epigallocatechin gallate, ascorbic acid, gelatin, chitosan nanoparticles and their beneficial effect on wound healing of diabetic mice. Int. J. Biol. Macromol. 2020, 148, 777–784. [Google Scholar] [CrossRef]
- Li, T.; Zhao, N.; Lu, J.; Zhu, Q.; Liu, X.; Hao, F.; Jiao, X. Epigallocatechin gallate (EGCG) suppresses epithelial-Mesenchymal transition (EMT) and invasion in anaplastic thyroid carcinoma cells through blocking of TGF-beta1/Smad signaling pathways. Bioengineered 2019, 10, 282–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yannas, I.V.; Tzeranis, D.S.; So, P.T.C. Regeneration of injured skin and peripheral nerves requires control of wound contraction, not scar formation. Wound Repair Regen. 2017, 25, 177–191. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Guo, X.W.; Li, L.; Wang, H.W.; Kim, W. The antioxidant property of chitosan green tea polyphenols complex induces transglutaminase activation in wound healing. J. Med. Food 2013, 16, 487–498. [Google Scholar] [CrossRef]
- Dunnill, C.; Patton, T.; Brennan, J.; Barrett, J.; Dryden, M.; Cooke, J.; Leaper, D.; Georgopoulos, N.T. Reactive oxygen species (ROS) and wound healing: The functional role of ROS and emerging ROS-modulating technologies for augmentation of the healing process. Int. Wound J. 2017, 14, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Feng, B.; Fang, Y.; Wei, S.M. Effect and mechanism of epigallocatechin-3-gallate (EGCG). against the hydrogen peroxide-induced oxidative damage in human dermal fibroblasts. J. Cosmet. Sci. 2013, 64, 35–44. [Google Scholar] [PubMed]
- Leu, J.G.; Chen, S.A.; Chen, H.M.; Wu, W.M.; Hung, C.F.; Yao, Y.D.; Tu, C.S.; Liang, Y.J. The effects of gold nanoparticles in wound healing with antioxidant epigallocatechin gallate and alpha-lipoic acid. Nanomed. Nanotechnol. Biol. Med. 2012, 8, 767–775. [Google Scholar] [CrossRef]
- Adedoyin, O.; Boddu, R.; Traylor, A.; Lever, J.M.; Bolisetty, S.; George, J.F.; Agarwal, A. Heme oxygenase-1 mitigates ferroptosis in renal proximal tubule cells. Am. J. Physiol.-Renal Phisiol. 2018, 314, F702–F714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grochot-Przeczek, A.; Lach, R.; Mis, J.; Skrzypek, K.; Gozdecka, M.; Sroczynska, P.; Dubiel, M.; Rutkowski, A.; Kozakowska, M.; Zagorska, A.; et al. Heme oxygenase-1 accelerates cutaneous wound healing in mice. PLoS ONE 2009, 4, e5803. [Google Scholar] [CrossRef] [Green Version]
- Yoon, J.Y.; Kwon, H.H.; Min, S.U.; Thiboutot, D.M.; Suh, D.H. Epigallocatechin-3-gallate improves acne in humans by modulating intracellular molecular targets and inhibiting P. acnes. J. Investig. Dermatol. 2013, 133, 429–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, S.J. Notch signalling: A simple pathway becomes complex. Nat. Rev. Mol. Cell Biol. 2006, 7, 678–689. [Google Scholar] [CrossRef] [PubMed]
- Hocke, A.C.; Ermert, M.; Althoff, A.; Brell, B.; N’Guessan, P.D.; Suttorp, N.; Ermert, L. Regulation of interleukin IL-4, IL-13, IL-10, and their downstream components in lipopolysaccharide-exposed rat lungs. Comparison of the constitutive expression between rats and humans. Cytokine 2006, 33, 199–211. [Google Scholar] [CrossRef] [PubMed]
- Lisi, L.; Ciotti, G.M.P.; Braun, D.; Kalinin, S.; Curro, D.; Dello Russo, C.; Coli, A.; Mangiola, A.; Anile, C.; Feinstein, D.L.; et al. Expression of iNOS, CD163 and ARG-1 taken as M1 and M2 markers of microglial polarization in human glioblastoma and the surrounding normal parenchyma. Neurosci. Lett. 2017, 645, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Tariq, M.; Zhang, J.Q.; Liang, G.K.; He, Q.J.; Ding, L.; Yang, B. Gefitinib inhibits M2-like polarization of tumor-associated macrophages in Lewis lung cancer by targeting the STAT6 signaling pathway. Acta Pharmacol. Sin. 2017, 38, 1501–1511. [Google Scholar] [CrossRef] [Green Version]
- Minami, K.; Hiwatashi, K.; Ueno, S.; Sakoda, M.; Iino, S.; Okumura, H.; Hashiguchi, M.; Kawasaki, Y.; Kurahara, H.; Mataki, Y.; et al. Prognostic significance of CD68, CD163 and Folate receptor beta positive macrophages in hepatocellular carcinoma. Exp. Ther. Med. 2018, 15, 4465–4476. [Google Scholar]
- Duckworth, P.F.; Rowlands, R.S.; Barbour, M.E.; Maddocks, S.E. A novel flow-system to establish experimental biofilms for modelling chronic wound infection and testing the efficacy of wound dressings. Microbiol. Res. 2018, 215, 141–147. [Google Scholar] [CrossRef]
- Bowler, P.G.; Duerden, B.I.; Armstrong, D.G. Wound microbiology and associated approaches to wound management. Clin. Microbiol. Rev. 2001, 14, 244–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doern, G.V.; Jones, R.N.; Pfaller, M.A.; Kugler, K.C.; Beach, M.L.; Grp, S.S. Bacterial pathogens isolated from patients with skin and soft tissue infections: Frequency of occurrence and antimicrobial susceptibility patterns from the SENTRY Antimicrobial Surveillance Program (United States and Canada, 1997). Diagn. Microbiol. Infect. Dis. 1999, 34, 65–72. [Google Scholar] [CrossRef]
- Bansal, S.; Choudhary, S.; Sharma, M.; Kumar, S.S.; Lohan, S.; Bhardwaj, V.; Syan, N.; Jyoti, S. Tea: A native source of antimicrobial agents. Food Res. Int. 2013, 53, 568–584. [Google Scholar] [CrossRef]
- Sun, T.Y.; Qin, B.J.; Gao, M.C.; Yin, Y.L.; Wang, C.Y.; Zang, S.Z.; Li, X.L.; Zhang, C.L.; Xin, Y.; Jiang, T. Effects of epigallocatechin gallate on the cell-wall structure of Mycobacterial smegmatis mc(2) 155. Nat. Prod. Res. 2015, 29, 2122–2124. [Google Scholar] [CrossRef] [PubMed]
- Reygaert, W.C. The antimicrobial possibilities of green tea. Front. Microbiol. 2014, 5, 434. [Google Scholar] [CrossRef] [PubMed]
- Nikoo, M.; Regenstein, J.M.; Gavlighi, H.A. Antioxidant and antimicrobial activities of (−)-Epigallocatechin-3-gallate (EGCG) and its potential to preserve the quality and safety of foods. Compr. Rev. Food Sci. Food Saf. 2018, 17, 732–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakayama, M.; Shimatani, K.; Ozawa, T.; Shigemune, N.; Tsugukuni, T.; Tomiyama, D.; Kurahachi, M.; Nonaka, A.; Miyamoto, T. A study of the antibacterial mechanism of catechins: Isolation and identification of Escherichia coli cell surface proteins that interact with epigallocatechin gallate. Food Control 2013, 33, 433–439. [Google Scholar] [CrossRef]
- Lu, J.; Vlamis-Gardikas, A.; Kandasamy, K.; Zhao, R.; Gustafsson, T.N.; Engstrand, L.; Hoffner, S.; Engman, L.; Holmgren, A. Inhibition of bacterial thioredoxin reductase: An antibiotic mechanism targeting bacteria lacking glutathione. FASEB J. 2013, 27, 1394–1403. [Google Scholar] [CrossRef] [Green Version]
- Liang, W.; Fernandes, A.P.; Holmgren, A.; Li, X.M.; Zhong, L.W. Bacterial thioredoxin and thioredoxin reductase as mediators for epigallocatechin 3-gallate-induced antimicrobial action. FEBS J. 2016, 283, 446–458. [Google Scholar] [CrossRef] [PubMed]
- Serra, D.O.; Mika, F.; Richter, A.M.; Hengge, R. The green tea polyphenol EGCG inhibits E-coli biofilm formation by impairing amyloid curli fibre assembly and downregulating the biofilm regulator CsgD via the sigma(E)-dependent sRNA RybB. Mol. Microbiol. 2016, 101, 136–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hengge, R. Targeting bacterial biofilms by the green tea polyphenol EGCG. Molecules 2019, 24, 2403. [Google Scholar] [CrossRef] [Green Version]
- Najarzadeh, Z.; Mohammad-Beigi, H.; Pedersen, J.N.; Christiansen, G.; Sonderby, T.V.; Shojaosadati, S.A.; Morshedi, D.; Stromgaard, K.; Meisl, G.; Sutherland, D.; et al. Plant polyphenols inhibit functional amyloid and biofilm formation in Pseudomonas strains by directing monomers to off-pathway oligomers. Biomolecules 2019, 9, 659. [Google Scholar] [CrossRef] [Green Version]
- Hao, S.Q.; Yang, D.; Zhao, L.; Shi, F.; Ye, G.; Fu, H.L.; Lin, J.C.; Guo, H.R.; He, R.; Li, J.L.; et al. EGCG-mediated potential inhibition of biofilm development and quorum sensing in Pseudomonas aeruginosa. Int. J. Mol. Sci. 2021, 22, 4946. [Google Scholar] [CrossRef] [PubMed]
- Taglialegna, A.; Navarro, S.; Ventura, S.; Garnett, J.A.; Matthews, S.; Penades, J.R.; Lasa, I.; Valle, J. Staphylococcal Bap proteins build amyloid scaffold biofilm matrices in response to environmental signals. PLoS Pathog. 2016, 12, e1005711. [Google Scholar] [CrossRef] [Green Version]
- Angelo, L.S.; Kurzrock, R. Vascular endothelial growth factor and its relationship to inflammatory mediators. Clin. Cancer Res. 2007, 13, 2825–2830. [Google Scholar] [CrossRef] [Green Version]
- Domingo, D.S.; Camouse, M.M.; Hsia, A.H.; Matsui, M.; Maes, D.; Ward, N.L.; Cooper, K.D.; Baron, E.D. Anti-angiogenic effects of epigallocatechin-3-gallate in human skin. Int. J. Clin. Exp. Pathol. 2010, 3, 706–709. [Google Scholar]
- Huijberts, M.S.P.; Schaper, N.C.; Schalkwijk, C.G. Advanced glycation end products and diabetic foot disease. Diabetes-Metab. Res. 2008, 24, S19–S24. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Lee, K.W. Protective effect of (−)-epigallocatechin gallate against advanced glycation endproducts-induced injury in neuronal cells. Biol. Pharm. Bull. 2007, 30, 1369–1373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankar, S.; Chen, Q.; Srivastava, R.K. Inhibition of PI3K/AKT and MEK/ERK pathways act synergistically to enhance antiangiogenic effects of EGCG through activation of FOXO transcription factor. J. Mol. Signal. 2008, 3, 7. [Google Scholar] [CrossRef] [Green Version]
- Meyer, M.; Muller, A.K.; Yang, J.X.; Sulcova, J.; Werner, S. The role of chronic inflammation in cutaneous fibrosis: Fibroblast growth factor receptor deficiency in Keratinocytes as an example. J. Investig. Dermatol. Symp. Proc. 2011, 15, 48–52. [Google Scholar] [CrossRef] [Green Version]
- Deng, C.C.; Hu, Y.F.; Zhu, D.H.; Cheng, Q.; Gu, J.J.; Feng, Q.L.; Zhang, L.X.; Xu, Y.P.; Wang, D.; Rong, Z.L.; et al. Single-cell RNA-seq reveals fibroblast heterogeneity and increased mesenchymal fibroblasts in human fibrotic skin diseases. Nat. Commun. 2021, 12, 3709. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.Z.; Kelly, A.P.; Wang, L.N.; French, S.W.; Tang, X.D.; Duong, H.S.; Messadi, D.V.; Le, A.D. Green tea extract and (−)-epigallocatechin-3-gallate inhibit mast cell-stimulated type I collagen expression in keloid fibroblasts via blocking PI-3K/Akt signaling pathways. J. Investig. Dermatol. 2006, 126, 2607–2613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, G.; Yoon, B.S.; Moon, J.H.; Kim, B.; Jun, E.K.; Oh, S.; Kim, H.; Song, H.J.; Noh, J.Y.; Oh, C.; et al. Green tea polyphenol epigallocatechin-3-gallate suppresses collagen production and proliferation in keloid fibroblasts via inhibition of the STAT3-signaling pathway. J. Investig. Dermatol. 2008, 128, 2429–2441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jimenez-Uribe, A.P.; Gomez-Sierra, T.; Aparicio-Trejo, O.E.; Orozco-Ibarra, M.; Pedraza-Chaverri, J. Backstage players of fibrosis: NOX4, mTOR, HDAC, and S1P; companions of TGF-beta. Cell Signal. 2021, 87, 110123. [Google Scholar] [CrossRef]
- Shi, J.; Li, J.; Guan, H.; Cai, W.; Bai, X.; Fang, X.; Hu, X.; Wang, Y.; Wang, H.; Zheng, Z.; et al. Anti-fibrotic actions of interleukin-10 against hypertrophic scarring by activation of PI3K/AKT and STAT3 signaling pathways in scar-forming fibroblasts. PLoS ONE 2014, 9, e98228. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.; Han, S.Y.; Hwang, K.; Kim, D.; Kim, E.M.; Hossain, M.A.; Kim, J.H.; Cho, J.Y. Antioxidant and cytoprotective effects of (−)-epigallocatechin-3-(3″-O-methyl) gallate. Int. J. Mol. Sci. 2019, 20, 3993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shinde, S.; Lee, L.H.; Chu, T.C. Inhibition of biofilm formation by the synergistic action of EGCG-S and antibiotics. Antibiotics 2021, 10, 102. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Kaihatsu, K.; Nishino, K.; Ogawa, M.; Kato, N.; Yamaguchi, A. Antibacterial and antifungal activities of new acylated derivatives of epigallocatechin gallate. Front. Microbiol. 2012, 3, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, Y.; Shahidi, F. Lipophilized epigallocatechin gallate (EGCG) derivatives as novel antioxidants. J. Agric. Food Chem. 2011, 59, 6526–6533. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, J.; Hu, J.M.; Huang, Y.W.; Wu, X.Y.; Zi, C.T.; Wang, X.J.; Sheng, J. Synthesis and biological testing of novel glucosylated epigallocatechin gallate (EGCG) derivatives. Molecules 2016, 21, 620. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
The native and wound dressing forms of EGCG.

Figure 2.
The antimicrobial mechanism of EGCG in skin wound healing process.

Figure 3.
The possible mechanisms underlying the beneficial effects of EGCG on skin wound healing.


{kind=link}
{kind=link}
{kind=link}
Table 1.
The roles of EGCG and its wound dressings in the biophysiological events at different wound healing stages.
Table 1.
The roles of EGCG and its wound dressings in the biophysiological events at different wound healing stages.
| Wound Healing Stage | Role of EGCG and Its Wound Dressings | Ref. |
|---|---|---|
| Hemostasis | Increasing hemadsorption | [56] |
| Inflammation | Limiting the infiltration of neutrophils | [59] |
| Inhibiting the migration and adhesion of monocytes | [60] | |
| Proliferation | Advancing re-epithelialization | [68,75] |
| Accelerating angiogenesis | [23] | |
| Altering collagen synthesis | [69,70,72] | |
| Reducing ECM formation | [70] | |
| Remodeling | No reference about the effect of EGCG on collagen remodeling, vascular maturation and regression |
Table 2.
The anti-inflammatory and angiogenic effects of EGCG and its wound dressings.
| Compounds | Model | Treatments | Results 1 | Ref. |
|---|---|---|---|---|
| EGCG | RAW 264.7 | Inductor: 200 EU/mL LPS Treatment time: pretreatment with EGCG for 30 min and then stimulation with LPS for a further 24 h Culture medium: fresh medium without fetal bovine serum | Effective concentration: 20 µg/mL EGCG In culture supernatants: IL-1β↓ In cells: protein abundance of Notch signaling pathway Notch-1↓, Notch-2↓, Cleave-Notch-1↓, and Hes-1↓ | [13] |
| DM mouse | Wound creation: two circular, full-thickness wounds (8 mm) on the back Treatment time: daily, 14 d Groups: (1) normal group: 6 normal mice received 1% carboxymethylcellulose vehicle; (2) diabetes group: 6 DM mice were applied with 1% carboxymethylcellulose vehicle; (3) EGCG group: 6 DM mice treated with 10 mg/mL EGCG | Effective concentration: 10 µg/mL EGCG In wound tissue: compared with the diabetes group, IL-1β↓, TNFα↓, IL-6↓, the protein abundance of Notch signaling pathway Notch-1↓and Notch-2↓, macrophage accumulation↓ | ||
| EGCG | NHKs | Inductor: 250 U/mL TNFα Treatment time: coexistence treatment with EGCG and TNFα for 48 h Culture medium: fresh medium without EGF or bovine pituitary extract | Effective concentration: 1~10 µM EGCG In culture supernatants: IL-8↓ | [14] |
| EGCG | Human body | Wound creation: a full thickness skin biopsy (5 mm diameter) on both upper inner arms Treatment time: twice daily, 1–2 weeks Groups: (1) normal group: placebo treatment; (2) EGCG group: zonal priming and direct topical treatment with EGCG | In wound tissue: the protein and mRNA abundances of VEGFA↓and CD31↓ | [15] |
| GBE-EGCG mixture | NHKs | Inductor: 250 U/mL TNFα Treatment time: coexistence treatment with GBE (0.1 or 0.5%) and/or EGCG for 48 h Culture medium: fresh medium without EGF or bovine pituitary extract | Effective concentration for cumulative downregulating effect: 1 µM EGCG added to 0.1% and 0.5% GBE In culture supernatants: IL-8↓ | [61] |
| EGCG-containing gold nanoparticles (AuEA) | Male BALB/c mice | Wound creation: two circular, 1 cm, full-thickness wounds on the bilateral upper back Treatment time: daily, 7 d Groups: (1) normal group: the left wound treated with vehicle; (2) AuEA group: treatment with AuEA ointment | Effective concentration: 1 mg/g EGCG + 30 mg/g α-lipoic acid (EA) + 0.07 mg/g AuNP ointment In wound tissue: CD68 protein↓, VEGF protein↑ | [59] |
| EGCG-loaded PLGA particles | Fibroblasts | Inductor: 100 ng/mL LPS Treatment time: coexistence treatment with EGCG microparticles and LPS for 24 h Culture medium: DMEM supplemented with 10% (v/v) FBS, and 1% (v/v) penicillin/streptomycin | Effective concentration: equivalent to 400 μg/mL EGCG in microparticles In cells: expressions of TNFA↓, IL-1β↓, IL-6↓ | [37] |
| EGCG-containing hydrogel (HA_TE) | RAW 264.7 | Inductor: 100 ng/mL LPS Treatment time: the hydrogel placed on Transwell, and then stimulated with LPS for a further 24 h Culture medium: not specifically mentioned | Effective concentration: 0.1–1.0% HA_TE (w/v) In culture supernatants: TNFα↓ | [20] |
| EGCG-chitosan hydrogel | RAW 264.7 | Inductor: 100 ng/mL LPS Treatment time: stimulated with LPS for 6 h, and then treated with the collected EGCG-contained medium for 24 h Culture medium: DMEM supplemented with 10% (v/v) FBS, 1% (w/v) L-glutamine, and 1% (v/v) penicillin/streptomycin | Effective concentration: 3 mM~11 mM EGCG of the hydrogel In culture supernatants: TNFα↓ | [12] |
| EGCG-containing EACPA hydrogel | Raw 264.7 | Inductor: 1 µg/mL LPS Treatment time: stimulated with LPS for 24 h, and then treated with EACPA hydrogel extract for 24 h Culture medium: DMEM culture medium | Effective concentration: EACPA hydrogel extract with 10 mg mL−1 In cells: the expressions of both iNOS and IL-1β↓, the expressions of CD163, CD206 and ARG-1↑ | [31] |
| Diabetic C57BL/6 mice | Wound creation: full-thickness longitudinal incisions (8 mm) on the back. Treatment time: daily, 3 d Groups: (1) normal group: the wound undressed; (2) Tegaderm film group: treatment with Tegaderm film; (3) EACPA hydrogel group | Effective concentration: EACPA hydrogel with 9 mm EA complex In wound tissue: the concentrations of both IL-1β and IL-6↓, the concentrations of both IL-4 and IL-10↑ | ||
| EGCG/PLGA membrane | BALB/c nude mice | Wound creation: a full thickness skin wound (12 mm) on the upper back Treatment: implanting for 2 weeks Groups: (1) normal group: PLGA membrane implanting; (2) EGCG group: EGCG/PLGA membrane implanting | Effective concentration: EGCG/PLGA membrane containing 1 wt% EGCG In wound tissue: the immunoreactivities of Ki-67↑ and CD 31↑ | [23] |
1 Compared with control. EU: endotoxin unit; NHKs: normal human keratinocytes; DM: diabetes mellitus; RAW 264.7: a murine leukemia macrophage cell line; HUVECs: human umbilical vein endothelial cells; HASMCs: human aortic smooth muscle cells; GBE: Ginkgo biloba leaves; AuEA: gold nanoparticles + EGCG + α-lipoic acid mixture; HA_TE: EGCG-hyaluronic acids-tyramine hydrogel; EACPA hydrogel: EGCG-3-acrylamido phenyl boronic acid-acrylamide hydrogel; EGCG: epigallocatechin gallate; TP: green tea polyphenol; TPN @ H: green tea polyphenol nanospheres in PVA/alginate hydrogel; PLGA: poly (lactide-co-glycolic acid); TNFα: tumor necrosis factor α; LPS: lipopolysaccharides; EGF: epidermal growth factor; IL: interleukin; VEGF: vascular endothelial growth factor.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Xu, F.-W.; Lv, Y.-L.; Zhong, Y.-F.; Xue, Y.-N.; Wang, Y.; Zhang, L.-Y.; Hu, X.; Tan, W.-Q. Beneficial Effects of Green Tea EGCG on Skin Wound Healing: A Comprehensive Review. Molecules 2021, 26, 6123. https://doi.org/10.3390/molecules26206123
AMA Style
Xu F-W, Lv Y-L, Zhong Y-F, Xue Y-N, Wang Y, Zhang L-Y, Hu X, Tan W-Q. Beneficial Effects of Green Tea EGCG on Skin Wound Healing: A Comprehensive Review. Molecules. 2021; 26(20):6123. https://doi.org/10.3390/molecules26206123
Chicago/Turabian StyleXu, Fa-Wei, Ying-Li Lv, Yu-Fan Zhong, Ya-Nan Xue, Yong Wang, Li-Yun Zhang, Xian Hu, and Wei-Qiang Tan. 2021. "Beneficial Effects of Green Tea EGCG on Skin Wound Healing: A Comprehensive Review" Molecules 26, no. 20: 6123. https://doi.org/10.3390/molecules26206123