
Eating Habits during the COVID-19 Lockdown in Italy: The Nutritional and Lifestyle Side Effects of the Pandemic


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Survey Methodology
2.2. The Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Variables
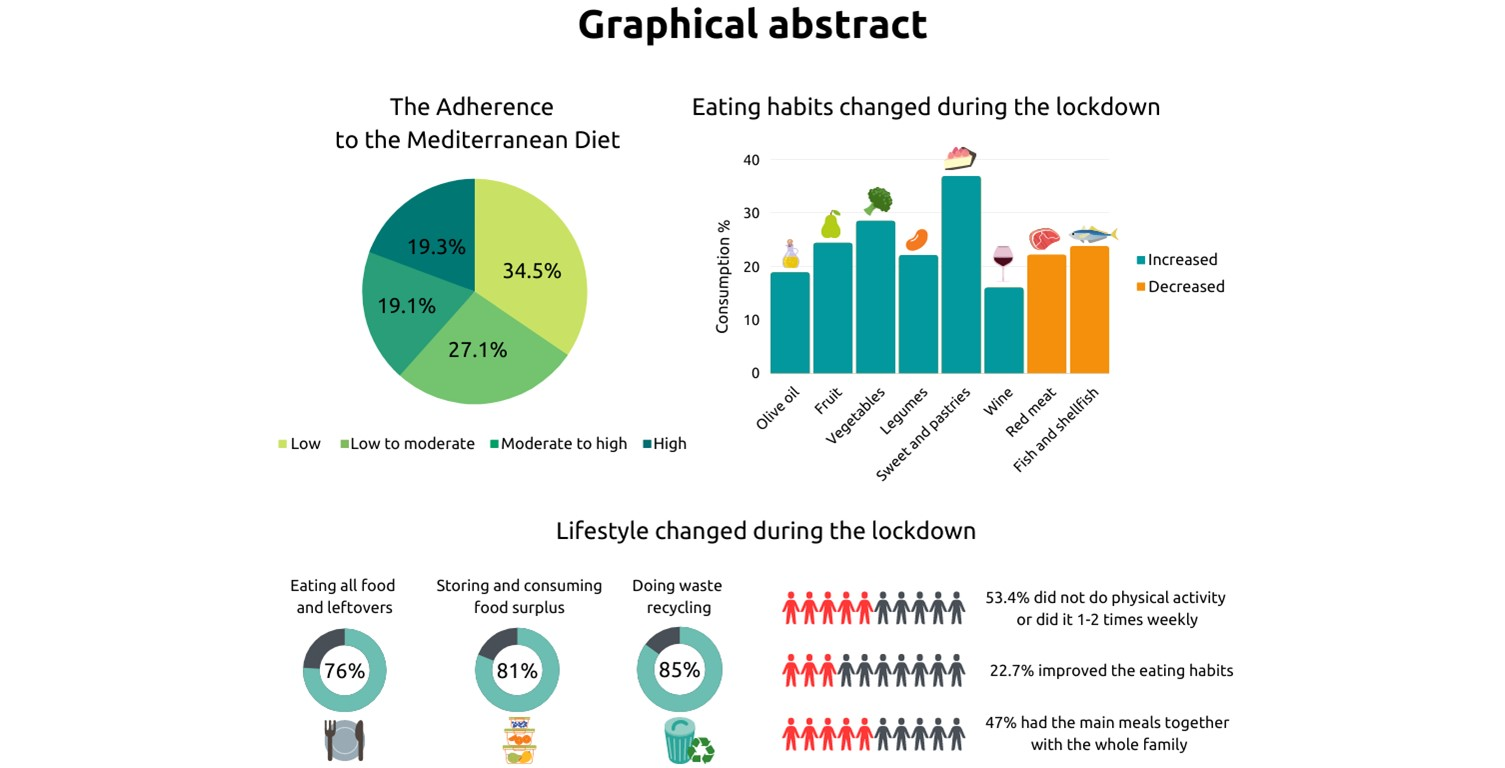
3.2. Adherence to the Mediterranean Diet (AMD) before the Lockdown
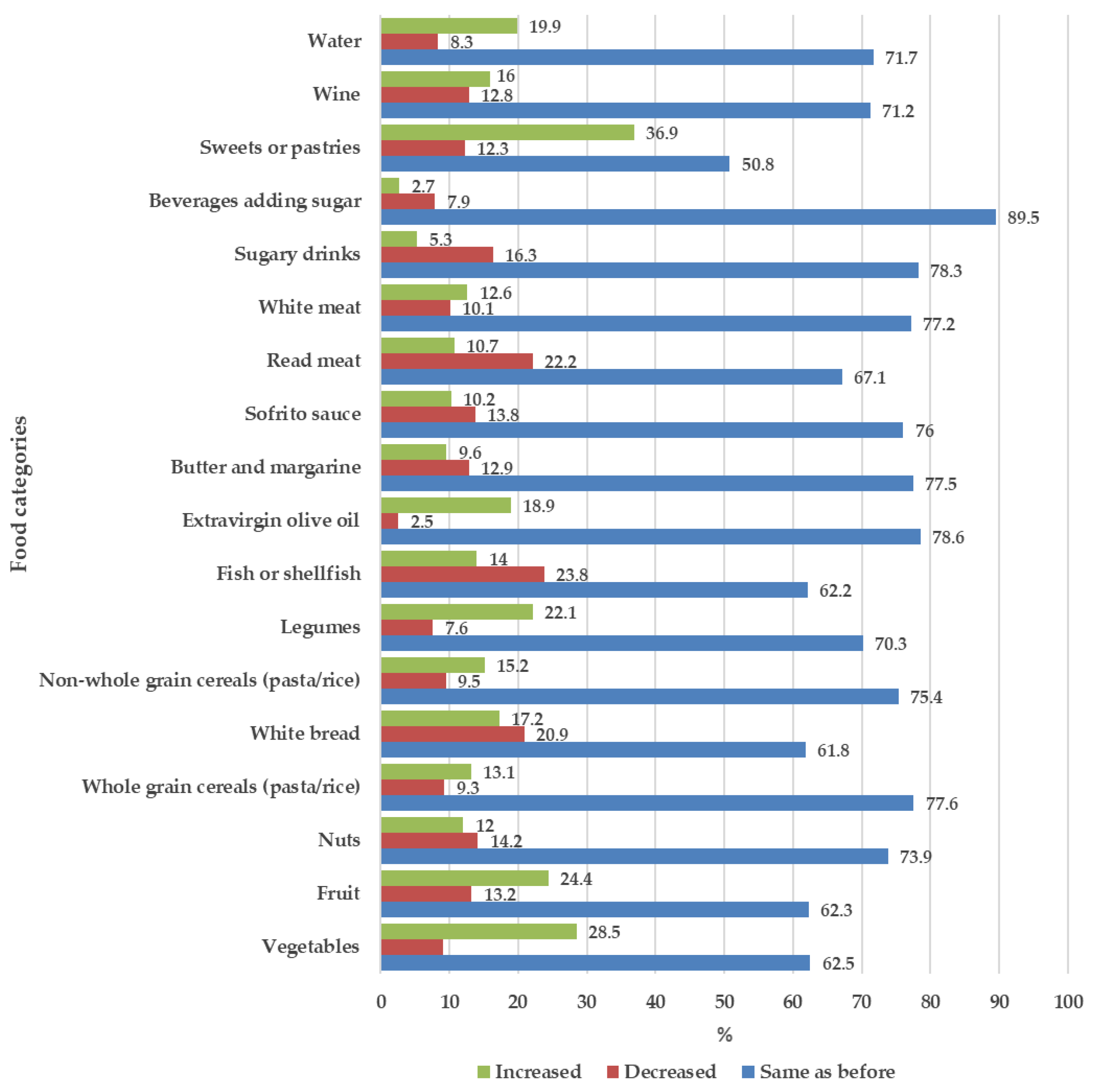
3.3. Changes in Eating Habits and Lifestyle during the Lockdown
3.4. Effects of Lockdown on the Relationship between Adherence to the Mediterranean Diet (AMD) and Eating Habits and Lifestyle Changes
3.5. Ponderal Status (BMI) and Changes in Eating Habits
3.6. Dietary Change Patterns Clusters during the Lockdown
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Di Renzo, L.; Gualtieri, P.; Cinelli, G.; Bigioni, G.; Soldati, L.; Attinà, A.; Bianco, F.F.; Caparello, G.; Camodeca, V.; Carrano, E.; et al. Psychological Aspects and Eating Habits during COVID-19 Home Confinement: Results of EHLC-COVID-19 Italian Online Survey. Nutrients 2020, 12, 2152. [Google Scholar] [CrossRef]
- Moccia, L.; Janiri, D.; Pepe, M.; Dattoli, L.; Molinaro, M.; De Martin, V.; Chieffo, D.; Janiri, L.; Fiorillo, A.; Sani, G.; et al. Affective Temperament, Attachment Style, and the Psychological Impact of the COVID-19 Outbreak: An Early Report on the Italian General Population. Brain. Behav. Immun. 2020, 87, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating Habits and Lifestyle Changes during COVID-19 Lockdown: An Italian Survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; De Michieli, F.; Ghigo, E.; et al. Changes in Weight and Nutritional Habits in Adults with Obesity during the “Lockdown” Period Caused by the COVID-19 Virus Emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef] [PubMed]
- Scarmozzino, F.; Visioli, F. Covid-19 and the Subsequent Lockdown Modified Dietary Habits of Almost Half the Population in an Italian Sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef] [PubMed]
- Romeo-Arroyo, E.; Mora, M.; Vázquez-Araújo, L. Consumer Behavior in Confinement Times: Food Choice and Cooking Attitudes in Spain. Int. J. Gastron. Food Sci. 2020, 21, 100226. [Google Scholar] [CrossRef]
- Epicentro ISS. #Let’s Stay Active, Also at Home! Available online: https://www.Epicentro.Iss.It/En/Coronavirus/Sars-Cov-2-Healthy-Lifestyles-Physical-Activity (accessed on 20 February 2021).
- Epicentro ISS. Nutrition during the COVID-19 Emergency. Available online: https://www.Epicentro.Iss.It/En/Coronavirus/Sars-Cov-2-Healthy-Lifestyles-Nutrition (accessed on 19 February 2021).
- World Health Organization. Nutrition Advice for Adults during the COVID-19 Outbreak. Available online: http://www.Emro.Who.Int/Nutrition/Nutrition-Infocus/Nutrition-Advice-for-Adults-during-the-Covid-19-Outbreak.Html#:~:Text=Eat%20fresh%20and%20unprocessed%20foods%20every%20day&text=Daily%2C%20eat%3A%202%20cups%20of,%E2%88%923%20times%20per%20week) (accessed on 19 February 2021).
- Angelidi, A.M.; Kokkinos, A.; Katechaki, E.; Ros, E.; Mantzoros, C.S. Mediterranean Diet as a Nutritional Approach for COVID-19. Metabolism 2021, 114, 154407. [Google Scholar] [CrossRef]
- Lopez-Garcia, E.; Rodriguez-Artalejo, F.; Li, T.Y.; Fung, T.T.; Li, S.; Willett, W.C.; Rimm, E.B.; Hu, F.B. The Mediterranean-Style Dietary Pattern and Mortality among Men and Women with Cardiovascular Disease. Am. J. Clin. Nutr. 2014, 99, 172–180. [Google Scholar] [CrossRef] [Green Version]
- Martínez-González, M.Á.; de la Fuente-Arrillaga, C.; Nunez-Cordoba, J.M.; Basterra-Gortari, F.J.; Beunza, J.J.; Vazquez, Z.; Benito, S.; Tortosa, A.; Bes-Rastrollo, M. Adherence to Mediterranean Diet and Risk of Developing Diabetes: Prospective Cohort Study. BMJ 2008, 336, 1348–1351. [Google Scholar] [CrossRef] [Green Version]
- Schröder, H.; Marrugat, J.; Vila, J.; Covas, M.I.; Elosua, R. Adherence to the Traditional Mediterranean Diet Is Inversely Associated with Body Mass Index and Obesity in a Spanish Population. J. Nutr. 2004, 134, 3355–3361. [Google Scholar] [CrossRef]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health Benefits of the Mediterranean Diet: Metabolic and Molecular Mechanisms. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 318–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trichopoulou, A.; Lagiou, P.; Kuper, H.; Trichopoulos, D. Cancer and Mediterranean Dietary Traditions. Cancer Epidemiol. Biomark. 2000, 9, 869–873. [Google Scholar]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean Diet and Health Status: An Updated Meta-Analysis and a Proposal for a Literature-Based Adherence Score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widmer, R.J.; Flammer, A.J.; Lerman, L.O.; Lerman, A. The Mediterranean Diet, Its Components, and Cardiovascular Disease. Am. J. Med. 2015, 128, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warburton, D.E.R. Health Benefits of Physical Activity: The Evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beisel, W.R. Nutrition and Immune Function: Overview. J. Nutr. 1996, 126, 2611S–2615S. [Google Scholar] [CrossRef] [Green Version]
- Calder, P.C.; Jackson, A.A. Undernutrition, Infection and Immune Function. Nutr. Res. Rev. 2000, 13, 3–29. [Google Scholar] [CrossRef] [PubMed]
- Samartín, S.; Chandra, R.K. Obesity, Overnutrition and the Immune System. Nutr. Res. 2001, 21, 243–262. [Google Scholar] [CrossRef]
- ISMEA. Emergenza COVID–19 Rapporto Sulla Domanda e l’offerta Dei Prodotti Alimentari Nelle Prime Settimane Di Diffusione Del Virus. Available online: http://www.Ismea.It/Flex/Cm/Pages/ServeBLOB.Php/L/IT/IDPagina/10990 (accessed on 26 February 2021).
- ISMEA. Emergenza COVID–19 2° Rapporto Sulla Domanda e l’offerta Dei Prodotti Alimentari Nell’emergenza Covid-19. Available online: http://www.Ismea.It/Flex/Cm/Pages/ServeBLOB.Php/L/IT/IDPagina/11016 (accessed on 26 February 2021).
- Available online: https://www.Crea.Gov.It/En/Web/Alimenti-e-Nutrizione/-/Osservatorio-Sugli-Sprechi-Alimentari (accessed on 19 May 2021).
- Linee Guida per Una Sana Alimentazione Revisione 2018. ISBN 9788833850375. Available online: https://www.Crea.Gov.It/En/Web/Alimenti-e-Nutrizione/-/Linee-Guida-per-Una-Sana-Alimentazione-2018 (accessed on 21 May 2021).
- Pappalardo, G.; Cerroni, S.; Nayga, R.M.; Yang, W. Impact of Covid-19 on Household Food Waste: The Case of Italy. Front. Nutr. 2020, 7, 585090. [Google Scholar] [CrossRef]
- United Nations. Department of Economic and Social Affairs Sustainable Development. The 17 Goals. Available online: https://Sdgs.Un.Org/Goals (accessed on 15 May 2021).
- World Medical Association. Wma Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. 2018. Available online: https://www.Wma.Net/Policies-Post/Wma-Declaration-of-Helsinki-Ethical-Principles-for-Medical-Research-Involving-Human-Subjects/ (accessed on 19 February 2021).
- Lehdonvirta, V.; Oksanen, A.; Räsänen, P.; Blank, G. Social Media, Web, and Panel Surveys: Using Non-Probability Samples in Social and Policy Research. Policy Internet 2021, 13, 134–155. [Google Scholar] [CrossRef]
- Álvarez-Álvarez, I.; Martínez-González, M.Á.; Sánchez-Tainta, A.; Corella, D.; Díaz-López, A.; Fitó, M.; Vioque, J.; Romaguera, D.; Martínez, J.A.; Wärnberg, J.; et al. Adherence to an Energy-Restricted Mediterranean Diet Score and Prevalence of Cardiovascular Risk Factors in the PREDIMED-Plus: A Cross-Sectional Study. Rev. Esp. Cardiol. Engl. Ed. 2019, 72, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Ros, E.; Covas, M.I.; Fiol, M.; Warnberg, J.; Aros, F.; Ruiz-Gutierrez, V.; Lamuela-Raventos, R.M.; et al. Cohort Profile: Design and Methods of the PREDIMED Study. Int. J. Epidemiol. 2012, 41, 377–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galilea-Zabalza, I.; Buil-Cosiales, P.; Salas-Salvadó, J.; Toledo, E.; Ortega-Azorín, C.; Díez-Espino, J.; Vázquez-Ruiz, Z.; Zomeño, M.D.; Vioque, J.; Martínez, J.A.; et al. Mediterranean Diet and Quality of Life: Baseline Cross-Sectional Analysis of the PREDIMED-PLUS Trial. PLoS ONE 2018, 13, e0198974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FAO. Food-Based Dietary Guidelines. Available online: http://www.Fao.Org/Nutrition/Education/Food-Dietary-Guidelines/En/#:~:Text=Food%2Dbased%20dietary%20guidelines%20(Also,Healthy%20eating%20habits%20and%20lifestyles (accessed on 20 June 2021).
- Harpe, S.E. How to Analyze Likert and Other Rating Scale Data. Curr. Pharm. Teach. Learn. 2015, 7, 836–850. [Google Scholar] [CrossRef]
- ISTAT, Italian Population Statistics. Available online: http://Dati.Istat.It/.Accessed (accessed on 19 May 2021).
- Molina-Montes, E.; Uzhova, I.; Verardo, V.; Artacho, R.; García-Villanova, B.; Jesús Guerra-Hernández, E.; Kapsokefalou, M.; Malisova, O.; Vlassopoulos, A.; Katidi, A.; et al. Impact of COVID-19 Confinement on Eating Behaviours across 16 European Countries: The COVIDiet Cross-National Study. Food Qual. Prefer. 2021, 93, 104231. [Google Scholar] [CrossRef]
- Linting, M.; Meulman, J.J.; Groenen, P.J.F.; van der Koojj, A.J. Nonlinear Principal Components Analysis: Introduction and Application. Psychol. Methods 2007, 12, 336–358. [Google Scholar] [CrossRef] [Green Version]
- Linting, M.; van der Kooij, A. Nonlinear Principal Components Analysis with CATPCA: A Tutorial. J. Pers. Assess. 2012, 94, 12–25. [Google Scholar] [CrossRef] [PubMed]
- Mazzocchi, M. Statistics for Marketing and Consumer Research, 1st ed.; Sage: London, UK, 2008. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis: A Global Perspective, 7th ed.; Pearson: London, UK, 2010. [Google Scholar]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Ruggiero, E.; Mignogna, C.; Costanzo, S.; Persichillo, M.; Di Castelnuovo, A.; Esposito, S.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; et al. Changes in the Consumption of Foods Characterising the Mediterranean Dietary Pattern and Major Correlates during the COVID-19 Confinement in Italy: Results from Two Cohort Studies. Int. J. Food Sci. Nutr. 2021, 1–13. [Google Scholar] [CrossRef]
- Rodríguez-Pérez, C.; Molina-Montes, E.; Verardo, V.; Artacho, R.; García-Villanova, B.; Guerra-Hernández, E.J.; Ruíz-López, M.D. Changes in Dietary Behaviours during the COVID-19 Outbreak Confinement in the Spanish COVIDiet Study. Nutrients 2020, 12, 1730. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef] [PubMed]
- Bennett, G.; Young, E.; Butler, I.; Coe, S. The Impact of Lockdown During the COVID-19 Outbreak on Dietary Habits in Various Population Groups: A Scoping Review. Front. Nutr. 2021, 8, 626432. [Google Scholar] [CrossRef]
- Skotnicka, M.; Karwowska, K.; Kłobukowski, F.; Wasilewska, E.; Małgorzewicz, S. Dietary Habits before and during the COVID-19 Epidemic in Selected European Countries. Nutrients 2021, 13, 1690. [Google Scholar] [CrossRef]
- Bonaccio, M.; Bonanni, A.E.; Di Castelnuovo, A.; De Lucia, F.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; on behalf of the Moli-sani Project. Investigators Low Income Is Associated with Poor Adherence to a Mediterranean Diet and a Higher Prevalence of Obesity: Cross-Sectional Results from the Moli-Sani Study. BMJ Open 2012, 2, e001685. [Google Scholar] [CrossRef] [Green Version]
- Cecchetto, C.; Aiello, M.; Gentili, C.; Ionta, S.; Osimo, S.A. Increased Emotional Eating during COVID-19 Associated with Lockdown, Psychological and Social Distress. Appetite 2021, 160, 105122. [Google Scholar] [CrossRef]
- Ingram, J.; Maciejewski, G.; Hand, C.J. Changes in Diet, Sleep, and Physical Activity Are Associated With Differences in Negative Mood During COVID-19 Lockdown. Front. Psychol. 2020, 11, 588604. [Google Scholar] [CrossRef]
- Aucejo, E.M.; French, J.; Ugalde Araya, M.P.; Zafar, B. The Impact of COVID-19 on Student Experiences and Expectations: Evidence from a Survey. J. Public Econ. 2020, 191, 104271. [Google Scholar] [CrossRef]
- Kartseva, M.A.; Kuznetsova, P.O. The Economic Consequences of the Coronavirus Pandemic: Which Groups Will Suffer More in Terms of Loss of Employment and Income? Popul. Econ. 2020, 4, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Armitage, R.; Nellums, L.B. COVID-19 and the Consequences of Isolating the Elderly. Lancet Public Health 2020, 5, e256. [Google Scholar] [CrossRef] [Green Version]
- Brooke, J.; Jackson, D. Older People and COVID-19: Isolation, Risk and Ageism. J. Clin. Nurs. 2020, 29, 2044–2046. [Google Scholar] [CrossRef] [PubMed]
- Epicentro. Alimentazione Dei Bambini e Ragazzi Durante L’emergenza COVID-19. Available online: https://www.Epicentro.Iss.It/Coronavirus/Sars-Cov-2-Stili-Vita-Alimentazione-Bambini-e-Ragazzi (accessed on 17 May 2021).
- Okkio Alla Salute. Available online: https://www.Salute.Gov.It/Portale/Temi/P2_6.Jsp?Lingua=italiano&id=2952&area=stiliVita&menu=sorveglianza (accessed on 17 May 2021).
- Browne, N.T.; Snethen, J.A.; Greenberg, C.S.; Frenn, M.; Kilanowski, J.F.; Gance-Cleveland, B.; Burke, P.J.; Lewandowski, L. When Pandemics Collide: The Impact of COVID-19 on Childhood Obesity. J. Pediatr. Nurs. 2021, 56, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Principato, L.; Secondi, L.; Cicatiello, C.; Mattia, G. Caring More about Food: The Unexpected Positive Effect of the Covid-19 Lockdown on Household Food Management and Waste. Socioecon. Plann. Sci. 2020, 100953. [Google Scholar] [CrossRef]
- Spreco Zero. Available online: https://www.Sprecozero.It/Wp-Content/Uploads/2021/01/MAGGIO-IORESTOACASA-E-RIDUCO-LO-SPRECO-SURVEY-WASTE-WATCHER-Copia.Pdf (accessed on 26 February 2021).
- Scalvedi, M.L.; Rossi, L. Comprehensive Measurement of Italian Domestic Food Waste in a European Framework. Sustainability 2021, 13, 1492. [Google Scholar] [CrossRef]
- Bisoffi, S.; Ahrné, L.; Aschemann-Witzel, J.; Báldi, A.; Cuhls, K.; DeClerck, F.; Duncan, J.; Hansen, H.O.; Hudson, R.L.; Kohl, J.; et al. COVID-19 and Sustainable Food Systems: What Should We Learn Before the Next Emergency. Front. Sustain. Food Syst. 2021, 5, 650987. [Google Scholar] [CrossRef]
- Mishra, V.; Seyedzenouzi, G.; Almohtadi, A.; Chowdhury, T.; Khashkhusha, A.; Axiaq, A.; Wong, W.Y.E.; Harky, A. Health Inequalities During COVID-19 and Their Effects on Morbidity and Mortality. J. Healthc. Leadersh. 2021, 13, 19–26. [Google Scholar] [CrossRef]
- Sachs, J.D.; Abdool Karim, S.; Aknin, L.; Allen, J.; Brosbøl, K.; Cuevas Barron, G.; Daszak, P.; Espinosa, M.F.; Gaspar, V.; Gaviria, A.; et al. Lancet COVID-19 Commission Statement on the Occasion of the 75th Session of the UN General Assembly. Lancet 2020, 396, 1102–1124. [Google Scholar] [CrossRef]
- Pinstrup-Andersen, P. Food Security: Definition and Measurement. Food Secur. 2009, 1, 5–7. [Google Scholar] [CrossRef]
- Pereira, M.; Oliveira, A.M. Poverty and Food Insecurity May Increase as the Threat of COVID-19 Spreads. Public Health Nutr. 2020, 23, 3236–3240. [Google Scholar] [CrossRef]
- Marí-Dell’Olmo, M.; Gotsens, M.; Pasarín, M.I.; Rodríguez-Sanz, M.; Artazcoz, L.; Garcia de Olalla, P.; Rius, C.; Borrell, C. Socioeconomic Inequalities in COVID-19 in a European Urban Area: Two Waves, Two Patterns. Int. J. Environ. Res. Public. Health 2021, 18, 1256. [Google Scholar] [CrossRef] [PubMed]
- Power, M.; Doherty, B.; Pybus, K.; Pickett, K. How Covid-19 Has Exposed Inequalities in the UK Food System: The Case of UK Food and Poverty. Emerald Open Res. 2020, 2, 11. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Eating Habits and Lifestyle Changes | Strongly Disagree (%) | Disagree (%) | Neither Agree Nor Disagree (%) | Agree (%) | Strongly Agree (%) |
|---|---|---|---|---|---|
| Q1. I need to pay attention to my spending, and I should limit my purchases of expensive foods | 25.4 | 15.4 | 30.4 | 19.4 | 9.4 |
| Q2. My cooking habits did not change, I continued to cook as before | 11.7 | 15 | 25.3 | 22.9 | 25.2 |
| Q3. I feel I am better at cooking | 17.4 | 9.6 | 37.4 | 22.1 | 13.4 |
| Q4. I have purchased and tried new foods that I never tasted before | 24.9 | 15.2 | 26.7 | 23.5 | 9.7 |
| Q5. I cannot always find the foods I would like to eat | 33.6 | 20.6 | 17.6 | 21 | 7.3 |
| Q6 I ate all food I had cooked, including leftovers | 7.1 | 5.1 | 11.4 | 26.1 | 50.3 |
| Q7. I do not know how to store and consume all foods that I bought | 62 | 19 | 11.6 | 5.5 | 1.9 |
| Q8. Separate collection of waste is very difficult, I cannot do it | 70 | 15 | 8.1 | 3.5 | 3.6 |
| Q9. I eat more comfort food than before (i.e., prosecco, snacks, sweets, etc) | 48.8 | 17.3 | 11.3 | 14.5 | 8.1 |
| Q10. I eat a lot of snacks during the day | 42.1 | 22.1 | 16.6 | 13.3 | 5.9 |
| Q11. I have improved my eating habits | 26.6 | 18.9 | 31.8 | 14.6 | 8.1 |
| Q12. I need to go on a diet to lose weight | 27.2 | 18.1 | 19.3 | 18 | 17.3 |
| Q14. I have the perception that the elderly have difficulties with shopping and suffer from social isolation | 8.3 | 8.4 | 17.2 | 27.3 | 38.7 |
| Q15. I eat the main meals together with the rest of my family more frequently than before | 18.7 | 7 | 27.3 | 16.4 | 30.6 |
| Changes of Food Habits during Lockdown (Classes–Quartiles) | Total | AMD Classes before Lockdown | |||
|---|---|---|---|---|---|
| Low | Low to Moderate | Moderate to High | High | ||
| No Changes | 26.4 | 32.7 a | 22.9 | 24.8 | 21.6 |
| Small Changes (1–2) | 30.6 | 27.2 | 33.8 | 28.3 | 34.2 b |
| Medium Changes (3–4) | 20.7 | 23.2 c | 19.3 | 25 d | 14.1 |
| Large Changes > 4 | 22.4 | 17 | 24 e | 21.9 f | 30.1 g |
| Total | 100 | 100 | 100 | 100 | 100 |
 or
or  describes favourable food consumption changes, = describes unchanged food consumption,
describes favourable food consumption changes, = describes unchanged food consumption,  and
and  describes unfavourable food consumption changes; * p < 0.05.
or describes favourable food consumption changes, = describes unchanged food consumption, and describes unfavourable food consumption changes; * p < 0.05.
describes unfavourable food consumption changes; * p < 0.05.
or describes favourable food consumption changes, = describes unchanged food consumption, and describes unfavourable food consumption changes; * p < 0.05.| Food Categories | Food Consumption | Total | AMD | |||
|---|---|---|---|---|---|---|
| Low | Low to Moderate | Moderate to High | High | |||
| Nuts | Increased | 12 | 7.8 | * 13.6 | * 14.5 | ( ) * 14.6 |
| Decreased | 14.2 | 15.1 | 15.5 | 17.1 | 7.7 | |
| Same as before | 72.8 | 77.1 | 70.9 | 68.4 | 77.7 | |
| Legumes | Increased | 22.1 | 17.1 | * 22.5 | * 26.3 | ( ) * 26.6 |
| Decreased | 7.6 | 7.8 | 8.3 | 7.3 | 6.5 | |
| Same as before | 70.3 | (=) * 75.1 | 69.2 | 66.4 | 66.9 | |
| Whole cereals | Increased | 13.1 | 9.2 | 11.4 | * 15.6 | ( ) * 20.1 |
| Decreased | 9.3 | 7.6 | 10.6 | 10.3 | 9.5 | |
| Same as before | 77.6 | (=) * 83.2 | 78 | 74.2 | 70.4 | |
| Vegetables | Increased | 28.5 | 28.1 | 28.9 | 27.2 | 29.7 |
| Decreased | 9 | ( ) * 7.9 | * 14.3 | * 9.5 | 3 | |
| Same as before | 62.5 | 64 | 56.8 | 63.3 | 67.3 | |
| Fish and shellfish | Increased | 14 | 12.9 | 11 | * 15.5 | ( ) * 18.7 |
| Decreased | 23.8 | 22.4 | 28.9 | 26.5 | 16.7 | |
| Same as before | 62.2 | 64.7 | 60.1 | 58 | 64.6 | |
| White bread | Increased | 17.2 | ( ) * 20.3 | * 21.4 | * 15.2 | 8 |
| Decreased | 20.9 | 16.2 | 19.7 | 18.4 | 33.6 | |
| Same as before | 61.9 | 63.5 | 59 | 66.4 | 58.4 | |
| Non-whole pasta and rice | Increased | 15.2 | ( ) * 17.3 | * 16 | * 17 | 8.4 |
| Decreased | 8.5 | 5.8 | 9.1 | 10.6 | * 15.3 | |
| Same as before | 76.3 | 76.9 | 74.8 | 72.4 | 76.3 | |
| Red meat | Increased | 10.7 | ( ) 13.7 | 9.2 | * 12.3 | 5.9 |
| Decreased | 22.2 | 19 | 19.3 | 19.8 | ( ) * 34.1 | |
| Same as before | 67.1 | * 67.3 | * 71.6 | * 67.9 | 59.9 | |
| Butter and margarine | Increased | 5.3 | ( ) * 12.7 | 9.8 | 8.4 | 4.8 |
| Decreased | 16.3 | 12.2 | 13.7 | 11.1 | 14.5 | |
| Same as before | 78.4 | 75.1 | 76.4 | 80.5 | 80.7 | |
| Sweet and pastries | Increased | 36.9 | ( ) * 43.5 | 34.6 | * 42 | 23.3 |
| Decreased | 12.3 | 6.6 | * 15.5 | * 12.9 | ( ) * 17.3 | |
| Same as before | 50.8 | 49.9 | 49.9 | 45.1 | * 59.4 | |
| Drinking beverages adding sugar | Increased | 2.7 | 3.3 | 3.1 | 2.5 | 1.1 |
| Decreased | 7.9 | * 5.3 | * 11.3 | 5.3 | ( ) * 10.1 | |
| Same as before | 89.4 | * 91.4 | 85.5 | * 92.3 | 88.8 | |
| Sugary drinks | Increased | 5.3 | ( ) * 8.8 | 4.4 | 3.8 | 2 |
| Decreased | 16.3 | 14.7 | * 21.9 | 13.9 | 14 | |
| Same as before | 78.4 | 76.5 | 73.8 | * 82.3 | (=) * 83.9 | |
| Wine | Increased | 16 | 16.5 | 15 | 19.8 | 12.6 |
| Decreased | 12.8 | ( ) * 8 | * 16 | * 14.5 | ( ) * 15.2 | |
| Same as before | 71.2 | 75.5 | 69 | 65.6 | 72.2 | |
| Water | Increased | 19.9 | 17 | 20.2 | 19.5 | ( ) * 25.3 |
| Decreased | 8.3 | 8.2 | 7.6 | 10.1 | 7.8 | |
| Same as before | 71.7 | * 74.8 | 72.2 | 70.5 | 66.9 | |
| Total | 100 | 100 | 100 | 100 | 100 | |
describes favourable food consumption changes, and describe unfavourable food consumption changes; * p < 0.05.
describes favourable food consumption changes, and describe unfavourable food consumption changes; * p < 0.05.| Eating Habits and Lifestyle | Total | AMD | ||||
|---|---|---|---|---|---|---|
| Low | Low to Moderate | Moderate to High | High | |||
| I have improved my eating habits | Low | 45.5 | ( ) * 54.2 | * 40.6 | * 44.1 | 38.5 |
| Medium | 31.8 | 27.7 | 36.7 | 31.1 | 33.1 | |
| High | 21.7 | 18.1 | 22.8 | * 24.7 | ( ) * 28.4 | |
| I eat more comfort food than before | Low | 66.1 | 53 | 71.7 | 69.1 | * 78.5 |
| Medium | 11.3 | * 17.1 | 9.6 | 7.9 | 6.9 | |
| High | 22.6 | ( ) * 29.9 | 18.7 | 23 | 14.6 | |
| I need to go on a diet to lose weight | Low | 45.3 | 79.6 | 77.6 | * 85.6 | * 83.5 |
| Medium | 19.3 | 18.9 | 20 | 17.3 | 21 | |
| High | 35.4 | ( ) * 38.1 | * 36.7 | * 36.8 | 27.1 | |
| Total | 100 | 100 | 100 | 100 | 100 | |
or describe favourable food consumption changes, = describes food consumption unchanged; * p < 0.05.
or describe favourable food consumption changes, = describes food consumption unchanged; * p < 0.05.| Food Categories | Food Consumption | Total | BMI Class | |||
|---|---|---|---|---|---|---|
| Underweight 3.5 | Normal Weight 57.1 | Overweight 29.1 | Obese 10.3 | |||
| Extra virgin olive oil | Increased | 19 | 10.6 | 16.1 | ( ) * 23.5 | ( ) * 25 |
| Decreased | 2.5 | 0.6 | 2.6 | 2.9 | 1.2 | |
| Same as before | 78.5 | * 88.8 | 81.3 | 73.6 | 73.8 | |
| Fruit | Increased | 24.5 | 19.7 | 23.4 | 27.3 | 24.5 |
| Decreased | 13.3 | 4.6 | 9.6 | * 17.6 | * 24.7 | |
| Same as before | 62.2 | (=) * 75.7 | (=) * 67.1 | 55.1 | 50.7 | |
| Vegetables | Increased | 28.6 | 20.9 | 27.9 | 28.1 | ( ) * 36.3 |
| Decreased | 9 | 4 | 7.5 | 11.9 | 11 | |
| Same as before | 62.4 | (=) * 75 | (=) * 64.6 | 60 | 52.7 | |
| Legumes | Increased | 22.2 | 16.6 | 22.3 | 19.5 | ( ) * 31 |
| Decreased | 7.6 | 3.8 | 8 | 6.3 | 10.4 | |
| Same as before | 58.6 | * 79.5 | * 69.7 | * 74.2 | 58.6 | |
| Fish and shellfish | Increased | 14.1 | 5.8 | 14.4 | 11.2 | ( ) * 23.1 |
| Decreased | 23.9 | 12.1 | 23.7 | 27.4 | 19.5 | |
| Same as before | 62 | * 82.2 | 61.9 | 61.5 | 57.3 | |
| Nuts | Increased | 12 | 5.4 | 12.2 | 11.8 | 13.3 |
| Decreased | 14.2 | 8.8 | 15.5 | 12.7 | 12.9 | |
| Same as before | 73.8 | * 85.8 | 72.3 | 75.4 | 73.8 | |
| Butter and margarine | Increased | 9.6 | 3.7 | 10.3 | 8.2 | 11.8 |
| Decreased | 12.9 | 4.3 | 11.6 | * 15.8 | * 14.9 | |
| Same as before | 77.5 | * 92 | 78 | 76 | 73.3 | |
| Red meat | Increased | 10.7 | 4.8 | 10 | 12.8 | 10.6 |
| Decreased | 22.2 | 12.3 | 23.4 | 20.1 | 25 | |
| Same as before | 67.1 | * 82.9 | 66.6 | 67.1 | 64.4 | |
| Sofrito | Increased | 10.2 | 5.9 | 9.8 | 10.6 | 13.4 |
| Decreased | 13.9 | 5.7 | 10.1 | * 16.6 | * 29.9 | |
| Same as before | 75.9 | * 88.4 | * 80.1 | 72.8 | 56.7 | |
| Sugary drinks | Increased | 5.4 | 1 | 5.3 | 4.9 | 8.1 |
| Decreased | 6.4 | 6.73 | 12.8 | 19.3 | ( ) * 31.4 | |
| Same as before | 78.2 | * 92.3 | * 81.9 | 75.7 | 60.55 | |
| Sweets and pastries | Increased | 37 | * 54.3 | 37.7 | 35.6 | 31.28 |
| Decreased | 12.3 | 7.7 | 10.6 | 13.4 | ( ) * 20.02 | |
| Same as before | 50.7 | 38 | 51.7 | 51 | 48.7 | |
| Drinking beverages adding sugar | Increased | 2.7 | 4.5 | 2.2 | 2.1 | 6.2 |
| Decreased | 7.9 | 6.8 | 6.7 | 4.9 | ( ) * 22.9 | |
| Same as before | 89.4 | 88.8 | 91.1 | 92.9 | 70.8 | |
| Water | Increased | 19.9 | 10.7 | 20.2 | 15.8 | 32.8 |
| Decreased | 8.4 | 3.9 | 9.2 | 8.1 | 6.2 | |
| Same as before | 71.8 | * 85.4 | 70.6 | * 76.1 | 61.1 | |
| Wine | Increased | 16 | 6.4 | 16.9 | 17.4 | 10.6 |
| Decreased | 12.8 | 5.7 | 11.4 | 12.4 | ( ) * 24.2 | |
| Same as before | 71.2 | 87.9 | 71.7 | 70.2 | 65.2 | |
| Total | 100 | 100 | 100 | 100 | 100 | |
| Groups | % | Food Consumption Pattern |
|---|---|---|
| Group 1- ”healthy eaters” | 26.8 | increased consumption of legumes, whole grain cereals and non-whole pasta and rice, nuts, sweets and pastries |
| Group 2- “less eaters” | 7.5 | decreased consumption of olive oil, fish and shellfish, nuts, legumes, white meat, whole grain cereals and non-whole pasta and rice, vegetables, red meat, butter and margarine, sugary drinks, sweets and pastries and sofrito sauce |
| Group 3- “usual eaters” | 51.4 | unchanged consumption |
| Group 4- ”more eaters” | 41.4 | increased consumption of almost all categories (coexist an increased and a decreased consumption of olive oil, whole grain cereals and adding sugar to beverages) |
| Sociodemographic Variables | Total | Group 1 | Group 2 | Group 3 | Group 4 | |
|---|---|---|---|---|---|---|
| Healthy Eaters | Less Eaters | Usual Eaters | More Eaters | |||
| Gender | Man | 48.2 | 49.6 | * 66.3 | 45.1 | 46.9 |
| Woman | 51.8 | * 50.4 | 33.7 | * 54.9 | * 53.1 | |
| Age | 18–29 | 14.6 | 13 | * 21.5 | 12.8 | * 20.3 |
| 30–49 | 32.2 | 28.7 | 28.8 | 31.2 | * 44.2 | |
| 50–69 | 32.9 | 33.3 | * 47.7 | 29.9 | 35.5 | |
| ≥70 | 20.3 | * 25 | 2 | * 26.2 | 0 | |
| AMD | Total | Group 1 | Group 2 | Group 3 | Group 4 | |
| Low | 34.5 | 30.2 | 25 | * 38.6 | 33 | |
| Low to moderate | 27.1 | 22.3 | *41.9 | 27.2 | 27.5 | |
| Moderate to high | 19.1 | 17.5 | 18.6 | 19.1 | 22.1 | |
| High | 19.3 | * 29.9 | 14.5 | 15.1 | 17.3 | |
| BMI class | Total | Group 1 | Group 2 | Group 3 | Group 4 | |
| Underweight | 3.5 | 1.8 | 1.7 | * 4.8 | 2.7 | |
| Normal weight | 57.2 | 57.1 | 53.4 | 56.9 | 60.4 | |
| Overweight | 29.1 | 30 | 25.5 | 29.5 | 27.5 | |
| Obese | 10.3 | 11.2 | * 19.4 | 8.7 | 9.4 | |
| Body weight changes | Total | Group 1 | Group 2 | Group 3 | Group 4 | |
| I do not know | 11.2 | 10.1 | * 18.7 | 10.6 | 11.6 | |
| My weight did not increase | 52.3 | 51.3 | 46.7 | * 55.8 | 44.3 | |
| 1–2 kg | 25.3 | 25.8 | 23.5 | 24.1 | 29.5 | |
| 3–5 kg | 10.1 | * 12.1 | 9.7 | 8.5 | 12.3 | |
| More than 5 kg | 1.1 | 0.8 | 1.5 | 0.9 | 2.3 | |
| Physical activity | Total | Group 1 | Group 2 | Group 3 | Group 4 | |
| I did not do physical activity | 37.2 | * 41.1 | 26.1 | 39.1 | 29 | |
| Less frequently | 11.1 | 10.9 | * 16.6 | 9.5 | * 14.8 | |
| 1–2 times per week | 16.2 | 17.2 | 20.8 | 14.1 | 19.4 | |
| 3–4 times per week | 18.3 | 17.5 | 18.2 | 17.9 | 21.6 | |
| 5 and more times per week | 17.2 | 13.4 | 18.3 | * 19.5 | 15.3 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grant, F.; Scalvedi, M.L.; Scognamiglio, U.; Turrini, A.; Rossi, L. Eating Habits during the COVID-19 Lockdown in Italy: The Nutritional and Lifestyle Side Effects of the Pandemic. Nutrients 2021, 13, 2279. https://doi.org/10.3390/nu13072279
Grant F, Scalvedi ML, Scognamiglio U, Turrini A, Rossi L. Eating Habits during the COVID-19 Lockdown in Italy: The Nutritional and Lifestyle Side Effects of the Pandemic. Nutrients. 2021; 13(7):2279. https://doi.org/10.3390/nu13072279
Chicago/Turabian StyleGrant, Federica, Maria Luisa Scalvedi, Umberto Scognamiglio, Aida Turrini, and Laura Rossi. 2021. "Eating Habits during the COVID-19 Lockdown in Italy: The Nutritional and Lifestyle Side Effects of the Pandemic" Nutrients 13, no. 7: 2279. https://doi.org/10.3390/nu13072279