
Time-Limited Eating and Continuous Glucose Monitoring in Adolescents with Obesity: A Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
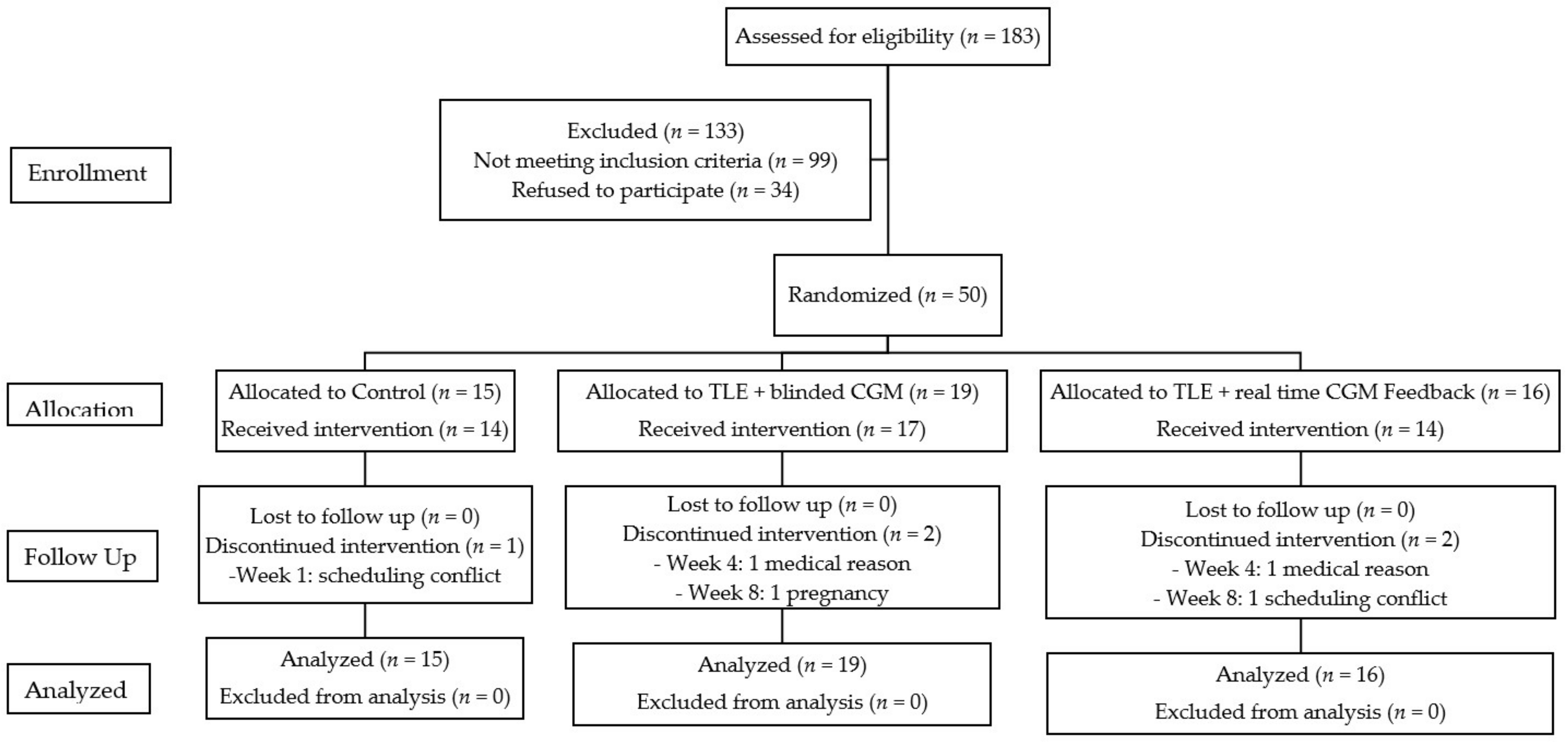
2.1. Study Design
2.2. Participants
2.3. Intervention Components
2.4. Measurements
2.4.1. Primary Outcome—Feasibility
2.4.2. Secondary Outcome
2.4.3. Continuous Glucose Monitoring
2.5. Statistical Analysis
3. Results
3.1. Primary Outcome—Feasibility
3.1.1. Characteristics of Participants Recruited
3.1.2. Adherence
3.2. Secondary Outcomes
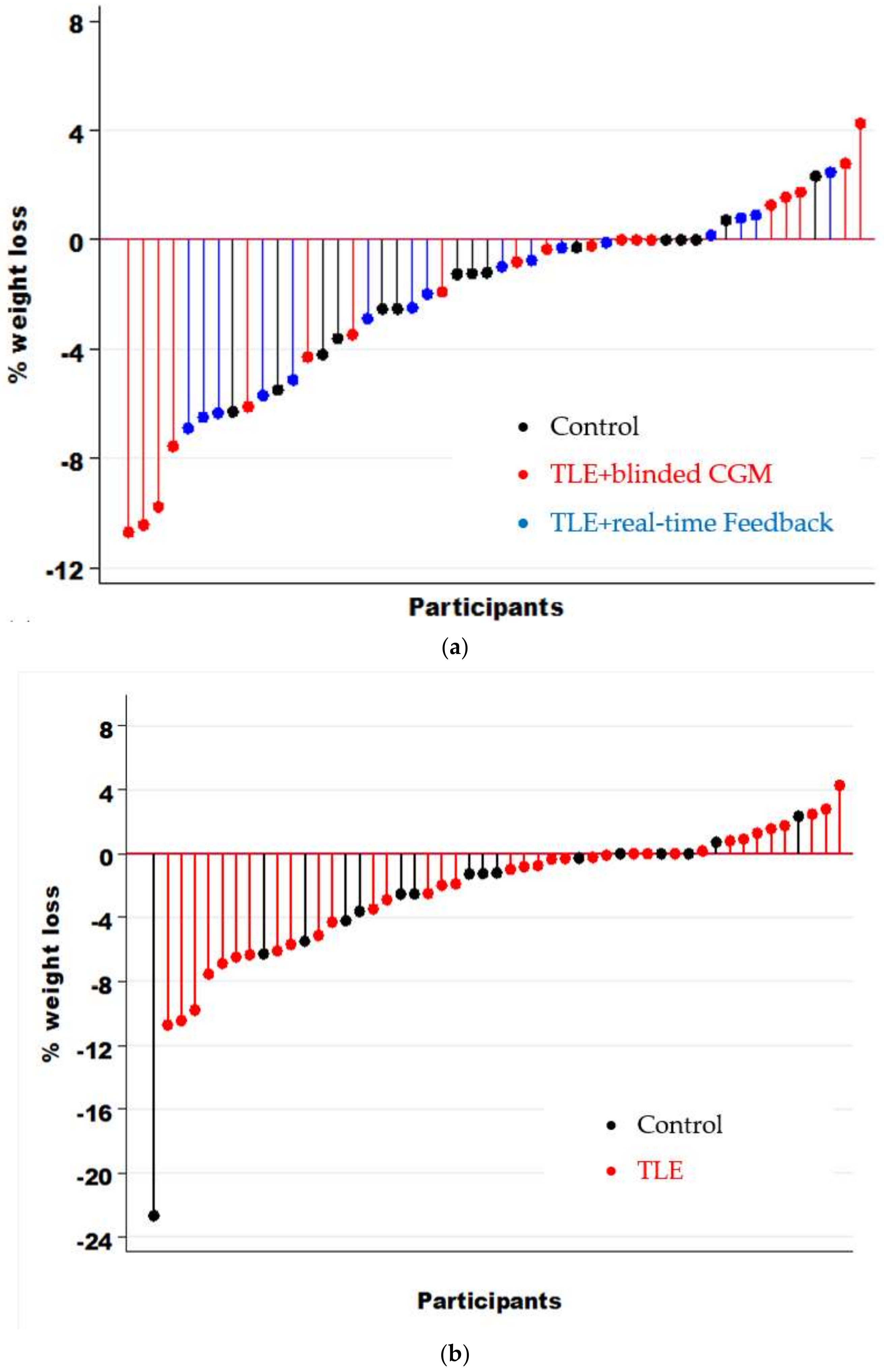
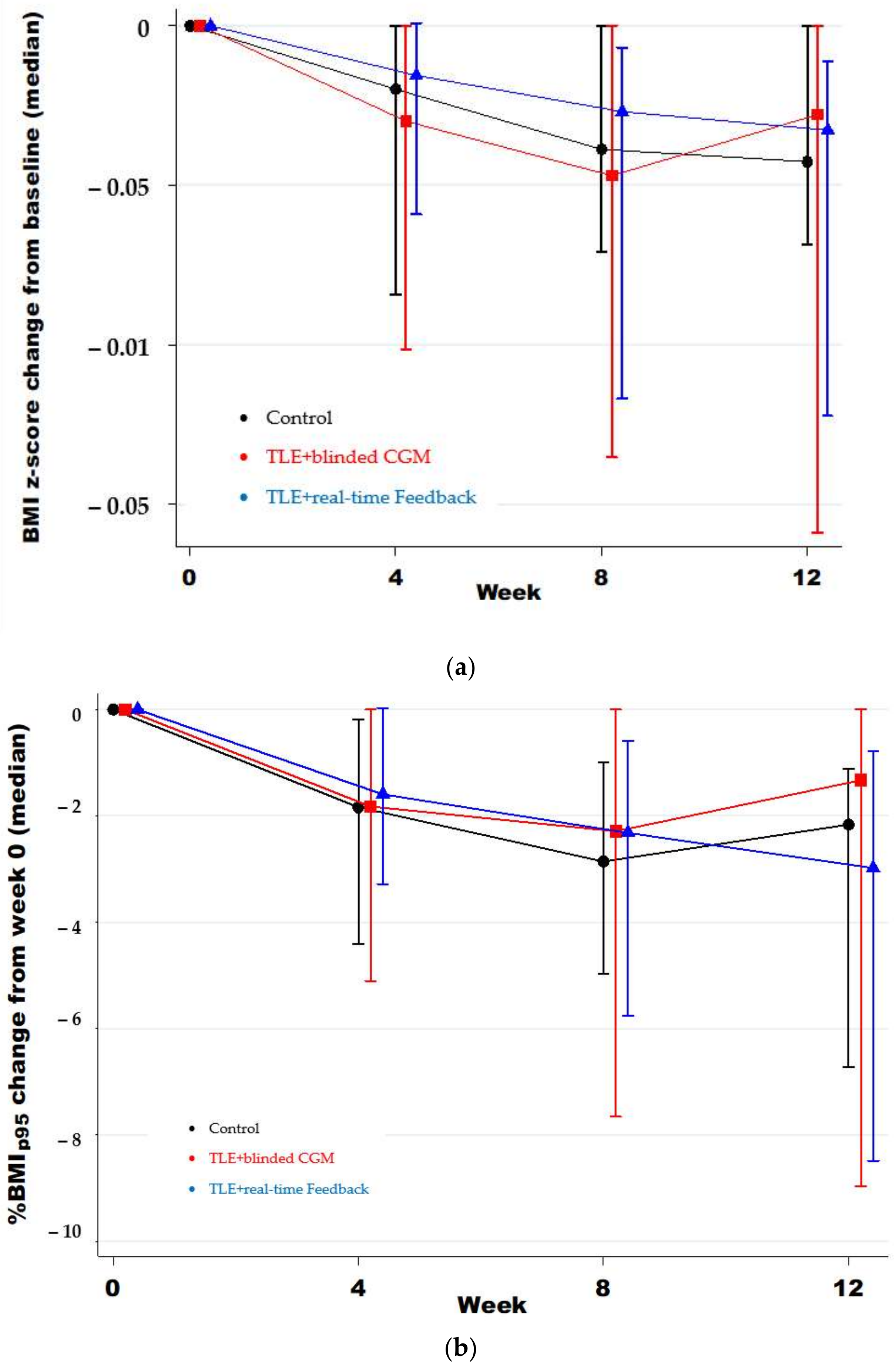
3.2.1. Weight Loss
3.2.2. Dietary Intake and Quality
3.2.3. Physical Activity
3.2.4. Eating Behaviors and Attitudes
3.2.5. Quality of Life
3.3. Continuous Glucose Monitoring
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Copeland, K.C.; Zeitler, P.; Geffner, M.; Guandalini, C.; Higgins, J.; Hirst, K.; Kaufman, F.R.; Linder, B.; Marcovina, S.; McGuigan, P.; et al. Characteristics of adolescents and youth with recent-onset type 2 diabetes: The TODAY cohort at baseline. J. Clin. Endocrinol. Metab. 2011, 96, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Marcus, M.D.; Wilfley, D.E.; El Ghormli, L.; Zeitler, P.; Linder, B.; Hirst, K.; Ievers-Landis, C.E.; van Buren, D.J.; Walders-Abramson, N.; TODAY Study Group. Weight change in the management of youth-onset type 2 diabetes: The TODAY clinical trial experience. Pediatr. Obes. 2017, 12, 337–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- August, G.P.; Caprio, S.; Fennoy, I.; Freemark, M.; Kaufman, F.R.; Lustig, R.H.; Silverstein, J.H.; Speiser, P.W.; Styne, D.M.; Montori, V.M. Prevention and treatment of pediatric obesity: An Endocrine Society clinical practice guideline based on expert opinion. J. Clin. Endocrinol. Metab. 2008, 93, 4576–4599. [Google Scholar] [CrossRef] [Green Version]
- Cardel, M.I.; Atkinson, M.A.; Taveras, E.M.; Holm, J.C.; Kelly, A.S. Obesity Treatment among Adolescents: A Review of Current Evidence and Future Directions. JAMA Pediatr. 2020, 174, 609–617. [Google Scholar] [CrossRef]
- Ogden, C.L.; Fryar, C.D.; Martin, C.B.; Freedman, D.S.; Carroll, M.D.; Gu, Q.; Hales, C.M. Trends in obesity prevalence by race and hispanic origin—1999–2000 to 2017–2018. JAMA J. Am. Med. Assoc. 2020, 324, 1208–1210. [Google Scholar] [CrossRef]
- Hales, C.M.; Fryar, C.D.; Carroll, M.D.; Freedman, D.S.; Ogden, C.L. Trendsinobesity and severe obesity prevalence in usyouth and adultsby sex and age, 2007–2008 to 2015–2016. JAMA J. Am. Med. Assoc. 2018, 319, 1723–1725. [Google Scholar] [CrossRef] [Green Version]
- Songer, T.J.; Haymond, M.W.; Glazner, J.E.; Klingensmith, G.J.; Laffel, L.M.; Zhang, P.; Hirst, K.; TODAY Study Group. Healthcare and associated costs related to type 2 diabetes in youth and adolescence: The TODAY clinical trial experience. Pediatr. Diabetes 2019, 20, 702–711. [Google Scholar] [CrossRef]
- Suglia, S.F.; Koenen, K.C.; Boynton-Jarrett, R.; Chan, P.S.; Clark, C.J.; Danese, A.; Faith, M.S.; Goldstein, B.I.; Hayman, L.L.; Isasi, C.R.; et al. Childhood and Adolescent Adversity and Cardiometabolic Outcomes: A Scientific Statement From the American Heart Association. Circulation 2018, 137, e15–e28. [Google Scholar] [CrossRef]
- Grossman, D.C.; Bibbins-Domingo, K.; Curry, S.J.; Barry, M.J.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W., Jr.; Kemper, A.R.; Krist, A.H.; Kurth, A.E.; et al. Screening for Obesity in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA 2017, 317, 2417–2426. [Google Scholar]
- Briggs, M.; Fleischhacker, S.; Mueller, C.G. Position of the American Dietetic Association, School Nutrition Association, and Society for Nutrition Education: Comprehensive School Nutrition Services. J. Nutr. Educ. Behav. 2010, 42, 360–371. [Google Scholar] [CrossRef]
- Hoelscher, D.M.; Kirk, S.; Ritchie, L.; Cunningham-Sabo, L. Position of the Academy of Nutrition and Dietetics: Interventions for the Prevention and Treatment of Pediatric Overweight and Obesity. J. Acad. Nutr. Diet. 2013, 113, 1375–1394. [Google Scholar] [CrossRef]
- Martin, A.; Saunders, D.H.; Shenkin, S.D.; Sproule, J. Lifestyle intervention for improving school achievement in overweight or obese children and adolescents. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef] [Green Version]
- Briggs, M.; Safaii, S.; Beall, D.L. Position of the American Dietetic Association, Society for Nutrition Education, and American School Food Service Association-Nutrition services: An essential component of comprehensive school health programs. J. Am. Diet. Assoc. 2003, 103, 505–514. [Google Scholar]
- Gabel, K.; Kroeger, C.M.; Trepanowski, J.F.; Hoddy, K.K.; Cienfuegos, S.; Kalam, F.; Varady, K.A. Differential Effects of Alternate-Day Fasting Versus Daily Calorie Restriction on Insulin Resistance. Obesity 2019, 27, 1443–1450. [Google Scholar] [CrossRef] [PubMed]
- Varady, K.A.; Gabel, K. Safety and efficacy of alternate day fasting. Nat. Rev. Endocrinol. 2019, 15, 686–687. [Google Scholar] [CrossRef] [PubMed]
- Trepanowski, J.F.; Kroeger, C.M.; Barnosky, A.; Klempel, M.C.; Bhutani, S.; Hoddy, K.K.; Gabel, K.; Freels, S.; Rigdon, J.; Rood, J.; et al. Effect of alternate-day fasting on weight loss, weight maintenance, and cardioprotection among metabolically healthy obese adults: A randomized clinical trial. JAMA Intern. Med. 2017, 177, 930–938. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.W.; Villani, V.; Buono, R.; Wei, M.; Kumar, S.; Yilmaz, O.H.; Cohen, P.; Sneddon, J.B.; Perin, L.; Longo, V.D. Fasting-Mimicking Diet Promotes Ngn3-Driven β-Cell Regeneration to Reverse Diabetes. Cell 2017, 168, 775–788.e12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Groot, S.; Lugtenberg, R.T.; Cohen, D.; Welters, M.J.P.; Ehsan, I.; Vreeswijk, M.P.G.; Smit, V.T.H.B.M.; de Graaf, H.; Heijns, J.B.; Portielje, J.E.A.; et al. Fasting mimicking diet as an adjunct to neoadjuvant chemotherapy for breast cancer in the multicentre randomized phase 2 DIRECT trial. Nat. Commun. 2020, 11, 1–9. [Google Scholar] [CrossRef]
- Melkani, G.C.; Panda, S. Time-restricted feeding for prevention and treatment of cardiometabolic disorders. J. Physiol. 2017, 595. Epub ahead of print. [Google Scholar] [CrossRef] [Green Version]
- Currenti, W.; Buscemi, S.; Cincione, R.I.; Cernigliaro, A.; Godos, J.; Grosso, G.; Galvano, F. Time-restricted feeding and metabolic outcomes in a cohort of Italian adults. Nutrients 2021, 13, 1651. [Google Scholar] [CrossRef] [PubMed]
- Tinsley, G.M.; Forsse, J.S.; Butler, N.K.; Paoli, A.; Bane, A.A.; La Bounty, P.M.; Morgan, G.B.; Grandjean, P.W. Time-restricted feeding in young men performing resistance training: A randomized controlled trial. Eur. J. Sport Sci. 2017, 17. [Google Scholar] [CrossRef]
- Balasubramanian, P.; DelFavero, J.; Ungvari, A.; Papp, M.; Tarantini, A.; Price, N.; de Cabo, R.; Tarantini, S. Time-restricted feeding (TRF) for prevention of age-related vascular cognitive impairment and dementia. Ageing Res. Rev. 2020, 64, 101189. [Google Scholar] [CrossRef] [PubMed]
- Rothschild, J.; Hoddy, K.K.; Jambazian, P.; Varady, K.A. Time-restricted feeding and risk of metabolic disease: A review of human and animal studies. Nutr. Rev. 2014, 72, 308–318. [Google Scholar] [CrossRef]
- Rynders, C.A.; Thomas, E.A.; Zaman, A.; Pan, Z.; Catenacci, V.A.; Melanson, E.L. Effectiveness of intermittent fasting and time-restricted feeding compared to continuous energy restriction for weight loss. Nutrients 2019, 11, 2442. [Google Scholar] [CrossRef] [Green Version]
- Gabel, K.; Hoddy, K.K.; Burgess, H.J.; Varady, K.A. Effect of 8-h time-restricted feeding on sleep quality and duration in adults with obesity. Appl. Physiol. Nutr. Metab. 2019, 44, 903–906. [Google Scholar] [CrossRef]
- Pellegrini, M.; Cioffi, I.; Evangelista, A.; Ponzo, V.; Goitre, I.; Ciccone, G.; Ghigo, E.; Bo, S. Effects of time-restricted feeding on body weight and metabolism. A systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2020, 21, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Sutton, E.F.; Beyl, R.; Early, K.S.; Cefalu, W.T.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes. Cell Metab. 2018, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabel, K.; Hoddy, K.K.; Varady, K.A. Safety of 8-h time restricted feeding in adults with obesity. Appl. Physiol. Nutr. Metab. 2019, 44, 107–109. [Google Scholar] [CrossRef] [Green Version]
- Cienfuegos, S.; Gabel, K.; Kalam, F.; Ezpeleta, M.; Pavlou, V.; Lin, S.; Wiseman, E.; Varady, K.A. The effect of 4-h versus 6-h time restricted feeding on sleep quality, duration, insomnia severity and obstructive sleep apnea in adults with obesity. Nutr. Health 2021. [Google Scholar] [CrossRef]
- Gabel, K.; Hoddy, K.K.; Haggerty, N.; Song, J.; Kroeger, C.M.; Trepanowski, J.F.; Panda, S.; Varady, K.A. Effects of 8-hour time restricted feeding on body weight and metabolic disease risk factors in obese adults: A pilot study. Nutr. Healthy Aging 2018, 4, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Conceição, E.M.; Crosby, R.; Mitchell, J.E.; Engel, S.G.; Wonderlich, S.A.; Simonich, H.K.; Peterson, C.B.; Crow, S.J.; Le Grange, D. Picking or nibbling: Frequency and associated clinical features in bulimia nervosa, anorexia nervosa, and binge eating disorder. Int. J. Eat. Disord. 2013, 46, 815–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elran-Barak, R.; Sztainer, M.; Goldschmidt, A.B.; Crow, S.J.; Peterson, C.B.; Hill, L.L.; Crosby, R.D.; Powers, P.; Mitchell, J.E.; Le Grange, D. Dietary Restriction Behaviors and Binge Eating in Anorexia Nervosa, Bulimia Nervosa and Binge Eating Disorder: Trans-diagnostic Examination of the Restraint Model. Eat. Behav. 2015, 18, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Wilson, G.T. Relation of dieting and voluntary weight loss to psychological functioning and binge eating. Ann. Intern. Med. 1993, 119, 727–730. [Google Scholar] [CrossRef]
- O’Connor, S.G.; Boyd, P.; Bailey, C.P.; Shams-White, M.M.; Agurs-Collins, T.; Hall, K.; Reedy, J.; Sauter, E.R.; Czajkowski, S.M. Perspective: Time-Restricted Eating Compared with Caloric Restriction: Potential Facilitators and Barriers of Long-Term Weight Loss Maintenance. Adv. Nutr. 2021, 12, 325–333. [Google Scholar] [CrossRef]
- Vidmar, A.P.; Goran, M.I.; Naguib, M.; Fink, C.; Wee, C.P.; Hegedus, E.; Lopez, K.; Gonzalez, J.; Raymond, J.K. Time limited eating in adolescents with obesity (time LEAd): Study protocol. Contemp. Clin. Trials 2020, 95, 106082. [Google Scholar] [CrossRef]
- Fenger, K.N.; Andersen, I.G.; Holm, L.A.; Holm, J.C.; Homøe, P. Quality of life in children and adolescents with overweight or obesity: Impact of obstructive sleep apnea. Int. J. Pediatr. Otorhinolaryngol. 2020, 138, 110320. [Google Scholar] [CrossRef]
- Eiser, C.; Varni, J.W. Health-related quality of life and symptom reporting: Similarities and differences between children and their parents. Eur. J. Pediatr. 2013, 172, 1299–1304. [Google Scholar] [CrossRef]
- Harnack, L.; Stevens, M.; Van Heel, N.; Schakel, S.; Dwyer, J.T.; Himes, J. A computer-based approach for assessing dietary supplement use in conjunction with dietary recalls. Journal of food composition and analysis: An official publication of the United Nations University, International Network of Food Data Systems. J. Food Compos. Anal. 2008, 21, S78–S82. [Google Scholar] [CrossRef] [Green Version]
- Thissen, D.; Liu, Y.; Magnus, B.; Quinn, H.; Gipson, D.S.; Dampier, C.; Huang, I.C.; Hinds, P.S.; Selewski, D.T.; Reeve, B.B.; et al. Estimating minimally important difference (MID) in PROMIS pediatric measures using the scale-judgment method. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2016, 25, 13–23. [Google Scholar] [CrossRef] [Green Version]
- Wiedemann, A.A.; Ivezaj, V.; Gueorguieva, R.; Potenza, M.N.; Grilo, C.M. Examining self-weighing behaviors and associated features and treatment outcomes in patients with binge-eating disorder and obesity with and without food addiction. Nutrients 2021, 13, 29. [Google Scholar] [CrossRef]
- Sievert, Y.A.; Schakel, S.F.; Buzzard, I.M. Maintenance of a nutrient database for clinical trials. Control. Clin. Trials 1989, 10, 416–425. [Google Scholar] [CrossRef]
- Johnson, R.K.; Driscoll, P.; Goran, M.I. Comparison of multiple-pass 24-hour recall estimates of energy intake with total energy expenditure determined by the doubly labeled water method in young children. J. Am. Diet. Assoc. 1996, 96, 1140–1144. [Google Scholar] [CrossRef]
- Hullmann, S.E.; Ryan, J.L.; Ramsey, R.R.; Chaney, J.M.; Mullins, L.L. Measures of general pediatric quality of life: Child Health Questionnaire (CHQ), DISABKIDS Chronic Generic Measure (DCGM), KINDL-R, Pediatric Quality of Life Inventory (PedsQL) 4.0 Generic Core Scales, and Quality of My Life Questionnaire (QoML). Arthritis Care Res. 2011, 63, S420–S430. [Google Scholar] [CrossRef] [PubMed]
- Feskanich, D.; Sielaff, B.H.; Chong, K.; Buzzard, I.M. Computerized collection and analysis of dietary intake information. Comput. Methods Programs Biomed. 1989, 30, 47–57. [Google Scholar] [CrossRef]
- Varni, J.W.; Burwinkle, T.M.; Jacobs, J.R.; Gottschalk, M.; Kaufman, F.; Jones, K.L. The PedsQLTM in type 1 and type 2 diabetes: Reliability and validity of the Pediatric Quality of Life InventoryTM Generic Core Scales and Type 1 Diabetes Module. Diabetes Care 2003, 26, 631–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Eynde, E.; Camfferman, R.; Putten, L.R.; Renders, C.M.; Seidell, J.C.; Halberstadt, J. Changes in the Health-Related Quality of Life and Weight Status of Children with Overweight or Obesity Aged 7 to 13 Years after Participating in a 10-Week Lifestyle Intervention. Child. Obes. 2020, 16, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Gunawardana, S.; Gunasinghe, C.B.; Harshani, M.S.; Seneviratne, S.N. Physical and psychosocial quality of life in children with overweight and obesity from Sri Lanka. BMC Public Health 2021, 21, 86. [Google Scholar] [CrossRef] [PubMed]
- Chamay-Weber, C.; Combescure, C.; Lanza, L.; Carrard, I.; Haller, D.M. Screening Obese Adolescents for Binge Eating Disorder in Primary Care: The Adolescent Binge Eating Scale. J. Pediatr. 2017, 185, 68–72.e1. [Google Scholar] [CrossRef] [PubMed]
- Manasse, S.M.; Michael, M.L.; Lin, M.; Gillikin, L.; Zhang, F.; Forman, E.M.; Juarascio, A. Can a Short Screening Tool Discriminate Between Overeating and Binge Eating in Treatment-Seeking Individuals with Obesity? Obesity 2021, 29, 706–712. [Google Scholar] [CrossRef]
- Lee, V.; Thurston, T.; Thurston, C. A Comparison of Discovered Regularities in Blood Glucose Readings across Two Data Collection Approaches Used with a Type 1 Diabetic Youth. Methods Inf. Med. 2017, 56, e84–e91. [Google Scholar] [CrossRef] [Green Version]
- Welsh, J.B.; Derdzinski, M.; Parker, A.S.; Puhr, S.; Jimenez, A.; Walker, T. Real-Time Sharing and Following of Continuous Glucose Monitoring Data in Youth. Diabetes Ther. 2019, 10, 751–755. [Google Scholar] [CrossRef] [Green Version]
- van der Linden, J.; Welsh, J.B.; Walker, T.C. Sustainable Use of a Real-Time Continuous Glucose Monitoring System from 2018 to 2020. Diabetes Technol. Ther. 2021, 23, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Franklin, E.V.; Simpson, V.; Berthet-Miron, M.; Gupta, O.T.; Barlow, S.E. A Pilot Study Evaluating a Binge-Eating Screener in Children: Development of the Children’s Brief Binge-Eating Questionnaire in a Pediatric Obesity Clinic. Clin. Pediatr. 2019, 58, 1063–1071. [Google Scholar] [CrossRef]
- Gill, S.; Panda, S. A Smartphone App Reveals Erratic Diurnal Eating Patterns in Humans that Can Be Modulated for Health Benefits. Cell Metab. 2015, 22, 789–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Štveráková, T.; Jačisko, J.; Busch, A.; Šafářová, M.; Kolář, P.; Kobesová, A. The impact of COVID-19 on Physical Activity of Czech children. PLoS ONE 2021, 16, e0254244. [Google Scholar] [CrossRef]
- Shanmugam, H.; Di Ciaula, A.; Di Palo, D.M.; Molina-Molina, E.; Garruti, G.; Faienza, M.F.; vanErpecum, K.; Portincasa, P. Multiplying effects of COVID-19 lockdown on metabolic risk and fatty liver. Eur. J. Clin. Investig. 2021, 51, e13597. [Google Scholar] [CrossRef]
- Al-Musharaf, S.; Aljuraiban, G.; Bogis, R.; Alnafisah, R.; Aldhwayan, M.; Tahrani, A. Lifestyle changes associated with COVID-19 quarantine among young Saudi women: A prospective study. PLoS ONE 2021, 16, e0250625. [Google Scholar] [CrossRef] [PubMed]
- Brazendale, K.; Beets, M.W.; Weaver, R.G.; Pate, R.R.; Turner-McGrievy, G.M.; Kaczynski, A.T.; Chandler, J.L.; Bohnert, A.; von Hippel, P.T. Understanding differences between summer vs. school obesogenic behaviors of children: The structured days hypothesis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–14. [Google Scholar] [CrossRef]
- Brazendale, K.; Beets, M.W.; Turner-McGrievy, G.M.; Kaczynski, A.T.; Pate, R.R.; Weaver, R.G. Children’s Obesogenic Behaviors During Summer Versus School: A Within-Person Comparison. J. Sch. Health 2018, 88, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Brazendale, K.; Beets, M.W.; Armstrong, B.; Weaver, R.G.; Hunt, E.T.; Pate, R.R.; Brusseau, T.A.; Bohnert, A.M.; Olds, T.; Tassitano, R.M.; et al. The impact of summer vacation on children’s obesogenic behaviors and body mass index: A natural experiment. Int. J. Behav. Nutr. Phys. Act. 2020, 17. [Google Scholar] [CrossRef]
- Paterson, D.C.; Ramage, K.; Moore, S.A.; Riazi, N.; Tremblay, M.S.; Faulkner, G. Exploring the impact of COVID-19 on the movement behaviors of children and youth: A scoping review of evidence after the first year. J. Sport Health Sci. 2021. [Google Scholar] [CrossRef]
- Regmi, P.; Chaudhary, R.; Page, A.J.; Hutchison, A.T.; Vincent, A.D.; Liu, B.; Heilbronn, L. Early or delayed time-restricted feeding prevents metabolic impact of obesity in mice. J. Endocrinol. 2021, 248, 75–86. [Google Scholar] [CrossRef]
- Jones, R.; Pabla, P.; Mallinson, J.; Nixon, A.; Taylor, T.; Bennett, A.; Tsintzas, K. Two weeks of early time-restricted feeding (eTRF) improves skeletal muscle insulin and anabolic sensitivity in healthy men. Am. J. Clin. Nutr. 2020, 112, 1015–1028. [Google Scholar] [CrossRef] [PubMed]
- Charlot, A.; Hutt, F.; Sabatier, E.; Zoll, J. Beneficial Effects of Early Time-Restricted Feeding on Metabolic Diseases: Importance of Aligning Food Habits with the Circadian Clock. Nutrients 2021, 13, 1405. [Google Scholar] [CrossRef] [PubMed]
- Böhm, B.; Karwiese, S.D.; Böhm, H.; Oberhoffer, R. Effects of Mobile Health Including Wearable Activity Trackers to Increase Physical Activity Outcomes Among Healthy Children and Adolescents: Systematic Review. JMIR mHealth uHealth 2019, 7, e8298. [Google Scholar] [CrossRef] [PubMed]
- Akturk, H.K.; Dowd, R.; Shankar, K.; Derdzinski, M. Real-World Evidence and Glycemic Improvement Using Dexcom G6 Features. Diabetes Technol. Ther. 2021, 23, S21–S26. [Google Scholar] [CrossRef]
- Brazendale, K.; Beets, M.W.; Armstrong, B.; Weaver, R.G.; Hunt, E.T.; Pate, R.R.; Brusseau, T.A.; Bohnert, A.M.; Olds, T.; Tassitano, R.M.; et al. Children’s moderate-to-vigorous physical activity on weekdays versus weekend days: A multi-country analysis. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 1–13. [Google Scholar] [CrossRef]
- Stavridou, A.; Kapsali, E.; Panagouli, E.; Thirios, A.; Polychronis, K.; Bacopoulou, F.; Psaltopoulou, T.; Tsolia, M.; Sergentanis, T.N.; Tsitsika, A. Obesity in Children and Adolescents during COVID-19 Pandemic. Children 2021, 8, 135. [Google Scholar] [CrossRef]
- Nakajima, R.; Kamada, H.; Kasai, T.; Tomaru, Y.; Waku, M.; Yamaki, A.; Ban, A.; Miyakawa, S.; Yamazaki, M.; Shiraki, H. Effect of temporary school closure due to COVID-19 on musculoskeletal function in elementary school children. J. Rural Med. JRM 2021, 16, 154–159. [Google Scholar] [CrossRef]
- Conceição, E.; Orcutt, M.; Mitchell, J.; Engel, S.; Lahaise, K.; Jorgensen, M.; Woodbury, K.; Hass, N.; Garcia, L.; Wonderlich, S. Eating disorders after bariatric surgery: A case series. Int. J. Eat. Disord. 2013, 46, 274–279. [Google Scholar] [CrossRef] [Green Version]
- Fawcett, E.; Van Velthoven, M.H.; Meinert, E. Long-Term Weight Management Using Wearable Technology in Overweight and Obese Adults: Systematic Review. JMIR mHealth uHealth 2020, 8, e13461. [Google Scholar] [CrossRef]
- Adafer, R.; Messaadi, W.; Meddahi, M.; Patey, A.; Haderbache, A.; Bayen, S.; Messaadi, N. Food Timing, Circadian Rhythm and Chrononutrition: A Systematic Review of Time-Restricted Eating’s Effects on Human Health. Nutrients 2020, 12, 3770. [Google Scholar] [CrossRef]
- Crose, A.; Alvear, A.; Singroy, S.; Wang, Q.; Manoogian, E.; Panda, S.; Mashek, D.G.; Chow, L.S. Time-restricted eating improves quality of life measures in overweight humans. Nutrients 2021, 13, 1430. [Google Scholar] [CrossRef] [PubMed]
- Kroes, M.; Osei-Assibey, G.; Baker-Searle, R.; Huang, J. Impact of weight change on quality of life in adults with overweight/obesity in the United States: A systematic review. Curr. Med. Res. Opin. 2016, 32, 485–508. [Google Scholar] [CrossRef] [PubMed]
- Kolotkin, R.L.; Andersen, J.R. A systematic review of reviews: Exploring the relationship between obesity, weight loss and health-related quality of life. Clin. Obes. 2017, 7, 273–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Androutsos, O.; Perperidi, M.; Georgiou, C.; Chouliaras, G. Lifestyle Changes and Determinants of Children’s and Adolescents’ Body Weight Increase during the First COVID-19 Lockdown in Greece: The COV-EAT Study. Nutrients 2021, 13, 930. [Google Scholar] [CrossRef] [PubMed]
- Cipolla, C.; Curatola, A.; Ferretti, S.; Giugno, G.; Condemi, C.; Delogu, A.B.; Birritella, L.; Lazzareschi, I. Eating habits and lifestyle in children with obesity during the COVID19 lockdown: A survey in an Italian center. Acta Bio-Med. Atenei Parm. 2021, 92, e2021196. [Google Scholar] [CrossRef]
- Cheng, H.P.; Wong, J.S.L.; Selveindran, N.M.; Hong, J.Y.H. Impact of COVID-19 lockdown on glycaemic control and lifestyle changes in children and adolescents with type 1 and type 2 diabetes mellitus. Endocrine 2021. [Google Scholar] [CrossRef] [PubMed]
- Przulj, D.; Ladmore, D.; Smith, K.M.; Phillips-Waller, A.; Hajek, P. Time restricted eating as a weight loss intervention in adults with obesity. PLoS ONE 2021, 16, e0246186. [Google Scholar] [CrossRef]
- Phillips, N.E.; Mareschal, J.; Schwab, N.; Manoogian, E.N.C.; Borloz, S.; Ostinelli, G.; Gauthier-Jaques, A.; Umwali, S.; Gonzalez Rodriguez, E.; Aeberli, D.; et al. The Effects of Time-Restricted Eating versus Standard Dietary Advice on Weight, Metabolic Health and the Consumption of Processed Food: A Pragmatic Randomised Controlled Trial in Community-Based Adults. Nutrients 2021, 13, 1042. [Google Scholar] [CrossRef]
- Anton, S.D.; Lee, S.A.; Donahoo, W.T.; McLaren, C.; Manini, T.; Leeuwenburgh, C.; Pahor, M. The Effects of Time Restricted Feeding on Overweight, Older Adults: A Pilot Study. Nutrients 2019, 11, 1500. [Google Scholar] [CrossRef] [Green Version]
- Jebeile, H.; Lister, N.B.; Baur, L.A.; Garnett, S.P.; Paxton, S.J. Eating disorder risk in adolescents with obesity. Obes. Rev. 2021, 22, e13173. [Google Scholar] [CrossRef]
- Raynor, H.A.; Mazzeo, S.E.; LaRose, J.G.; Adams, E.L.; Thornton, L.M.; Caccavale, L.J.; Bean, M.K. Effect of a high-intensity dietary intervention on changes in dietary intake and eating pathology during a multicomponent adolescent obesity intervention. Nutrients 2021, 13, 1850. [Google Scholar] [CrossRef]
- Jebeile, H.; Gow, M.L.; Baur, L.A.; Garnett, S.P.; Paxton, S.J.; Lister, N.B. Association of Pediatric Obesity Treatment, Including a Dietary Component, with Change in Depression and Anxiety: A Systematic Review and Meta-analysis. JAMA Pediatr. 2019, 173, e192841. [Google Scholar] [CrossRef]
- Gabel, K.; Marcell, J.; Cares, K.; Kalam, F.; Cienfuegos, S.; Ezpeleta, M.; Varady, K.A. Effect of time restricted feeding on the gut microbiome in adults with obesity: A pilot study. Nutr. Health 2020, 26, 79–85. [Google Scholar] [CrossRef]
- Cienfuegos, S.; Gabel, K.; Kalam, F.; Ezpeleta, M.; Wiseman, E.; Pavlou, V.; Lin, S.; Oliveira, M.L.; Varady, K.A. Effects of 4- and 6-h Time-Restricted Feeding on Weight and Cardiometabolic Health: A Randomized Controlled Trial in Adults with Obesity. Cell Metab. 2020, 32, 366–378. [Google Scholar] [CrossRef] [PubMed]
- Garaulet, M.; Gómez-Abellán, P.; Alburquerque-Béjar, J.J.; Lee, Y.C.; Ordovás, J.M.; Scheer, F.A. Timing of food intake predicts weight loss effectiveness. Int. J. Obes. 2013, 37, 604–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchison, A.T.; Regmi, P.; Manoogian, E.N.C.; Fleischer, J.G.; Wittert, G.A.; Panda, S.; Heilbronn, L.K. Time-Restricted Feeding Improves Glucose Tolerance in Men at Risk for Type 2 Diabetes: A Randomized Crossover Trial. Obesity 2019, 27, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Brandhorst, S.; Shelehchi, M.; Mirzaei, H.; Cheng, C.W.; Budniak, J.; Groshen, S.; Mack, W.J.; Guen, E.; Di Biase, S.; et al. Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and cardiovascular disease. Sci. Transl. Med. 2017, 9. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 50) | Control (n = 15) | TLE + Blinded CGM (n = 19) | TLE + Real-Time CGM Feedback (n = 16) | p | |
|---|---|---|---|---|---|
| Age (in year) 1 | 16.43 ± 1.17 | 16.38 ± 1.25 | 16.16 ± 1.16 | 16.80 ± 1.09 | 0.3 a |
| Sex 2 | 0.8 b | ||||
| Male | 14 (28.0) | 3 (20.0) | 6 (31.5) | 5 (31.2) | |
| Female | 36 (72.0) | 12 (80.0) | 13 (68.4) | 11 (68.7) | |
| Race 2 | 0.05 b | ||||
| White | 5 (10.0) | 3 (20.0) | 1 (5.2) | 1 (6.0) | |
| Black | 3 (6.0) | 1 (6.6) | 2 (10.5) | 0 (0) | |
| Asian | 4 (8.0) | 3 (20.0) | 1 (5.2) | 0 (0) | |
| Hispanic | 27 (54.0) | 7 (46.7) | 13 (68.4) | 7 (43.8) | |
| Am. Indian | 2 (4.0) | 0 (0) | 1 (5.2) | 1 (6.2) | |
| Mixed race | 6 (12.0) | 1 (6.6) | 0 (0) | 5 (31.2) | |
| Ethnicity 2 | 0.1 b | ||||
| Non-Hispanic | 15 (30.0) | 8 (53.3) | 4 (21.1) | 3 (18.7) | |
| Hispanic | 32 (64.0) | 7 (46.6) | 14 (73.6) | 11 (68.7) | |
| Weight (kg) 3 | 101.4 (87.9, 123.8) | 104.3 (74.8, 123.1) | 99.5 (84.6, 123.2) | 110.5 (92.2, 128.3) | 0.9 c |
| %BMIp95 3 | 125.9 (111, 158) | 141.1 (114.4, 167.0) | 122.6 (110.0, 158.5) | 123.9 (109.8, 159.1) | 0.9 c |
| BMI z-score 1 | 2.30 ± 0.5 | 2.34 ± 0.5 | 2.28 ± 0.4 | 2.30 ± 0.5 | 0.9 a |
| Week | Control (n = 15) | TLE + Blinded CGM (n = 19) | TLE + Real-Time CMG Feedback (n = 16) |
|---|---|---|---|
| 1 | 5.1 (1.9) | 4.03 (1.9) | 4.5 (1.9) |
| 2 | 5.6 (1.3) | 5.3 (1.3) | 5.3 (1.2) |
| 3 | 5.6 (1.3) | 5.4 (1.3) | 6.7 (1.3) |
| 4 | 6.1 (1.6) | 5.1 (1.6) | 5.3 (1.4) |
| 5 | 5.9 (1.6) | 5.1 (1.6) | 5.4 (1.7) |
| 6 | 4.9 (1.3) | 5.4 (1.3) | 5.9 (1.1) |
| 7 | 6.7 (1.3) | 5.3 (1.3) | 6.0 (1.0) |
| 8 | 5.4 (1.1) | 5.4 (1.1) | 4.9 (1.1) |
| 9 | 5.9 (1.0) | 5.1 (1.0) | 4.8 (1.5) |
| 10 | 6.1 (1.2) | 5.3 (1.2) | 5.3 (1.4) |
| 11 | 5.5 (1.5) | 5.3 (1.5) | 5.1 (1.0) |
| 12 | 4.9 (1.0) | 5.3 (1.0) | 4.9 (1.1) |
| Weight Change | Control (n = 15) | TLE + Blinded CGM (n = 19) | TLE + Real-Time CGM Feedback (n = 16) | p | Effect Size |
|---|---|---|---|---|---|
| BMI z-score change | −0.05 ± 0.09 | −0.09 ± 0.14 | −0.11 ± 0.19 | 0.6 | 0.04 |
| %BMIp95 change | −3.27 ± 3.34 | −3.76 ± 5.76 | −4.85 ± 5.08 | 0.7 | 0.04 |
| %BMIp95 | % Change | 95% CI | p |
|---|---|---|---|
| Week | |||
| 0 | Ref | -- | -- |
| 4 | −2.0 | (−2.7, −1.3) | <0.0001 |
| 8 | −2.9 | (−3.8, −1.9) | <0.0001 |
| 12 | −3.3 | (−4.4, −2.1) | <0.0001 |
| Intervention group | |||
| Control | Ref | -- | -- |
| TLE + blinded CGM | −3.4 | (−17.6, 13.3) | 0.7 |
| TLE + real-time CGM feedback | −4.3 | (−17.9, 11.7) | 0.6 |
| BMI z-score | β | 95% CI | p |
| Week | |||
| 0 | Ref | -- | -- |
| 4 | −0.05 | (−0.1, −0.03) | <0.0001 |
| 8 | −0.08 | (−0.1, −0.04) | <0.0001 |
| 12 | −0.09 | (−0.1, −0.05) | <0.0001 |
| Intervention group | |||
| Control | Ref | -- | -- |
| TLE + blinded CGM | −0.08 | (−0.4, 0.2) | 0.6 |
| TLE + real-time CGM feedback | −0.06 | (−0.4, 0.3) | 0.7 |
| Glycemic Profile | β | 95% CI | p |
|---|---|---|---|
| Average blood glucose | |||
| Visit Week | |||
| 0 | Ref | ||
| 4 | 2.7 | (−4.3, 9.7) | 0.4 |
| 8 | 3.3 | (−3.6, 10.3) | 0.3 |
| 12 | 3.3 | (−7.9, 14.6) | 0.6 |
| Intervention group | |||
| Control | Ref | ||
| TLE + blinded CGM | −4.2 | (−14.7, 6.1) | 0.4 |
| TLE + real-time feedback | −7.1 | (−20.2, 6.0) | 0.2 |
| Estimated HbA1c | |||
| Week | |||
| 0 | Ref | ||
| 4 | 0.1 | (−0.1, 0.3) | 0.3 |
| 8 | 0.1 | (−0.1, 0.3) | 0.3 |
| 12 | 0.1 | (−0.2, 0.4) | 0.5 |
| Intervention group | |||
| Control | Ref | ||
| TLE + blinded CGM | −0.2 | (−0.5, 0.1) | 0.2 |
| TLE + real-time feedback | −0.3 | (−0.7, 0.1) | 0.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vidmar, A.P.; Naguib, M.; Raymond, J.K.; Salvy, S.J.; Hegedus, E.; Wee, C.P.; Goran, M.I. Time-Limited Eating and Continuous Glucose Monitoring in Adolescents with Obesity: A Pilot Study. Nutrients 2021, 13, 3697. https://doi.org/10.3390/nu13113697
Vidmar AP, Naguib M, Raymond JK, Salvy SJ, Hegedus E, Wee CP, Goran MI. Time-Limited Eating and Continuous Glucose Monitoring in Adolescents with Obesity: A Pilot Study. Nutrients. 2021; 13(11):3697. https://doi.org/10.3390/nu13113697
Chicago/Turabian StyleVidmar, Alaina P., Monica Naguib, Jennifer K. Raymond, Sarah Jeanne Salvy, Elizabeth Hegedus, Choo Phei Wee, and Michael I. Goran. 2021. "Time-Limited Eating and Continuous Glucose Monitoring in Adolescents with Obesity: A Pilot Study" Nutrients 13, no. 11: 3697. https://doi.org/10.3390/nu13113697