
First-In-Human Results on the Biodistribution, Pharmacokinetics, and Dosimetry of [177Lu]Lu-DOTA.SA.FAPi and [177Lu]Lu-DOTAGA.(SA.FAPi)2

Abstract
:1. Introduction
2. Results
2.1. Patients
2.2. Safety
2.3. Biodistribution and Pharmacokinetics of Normal Organs
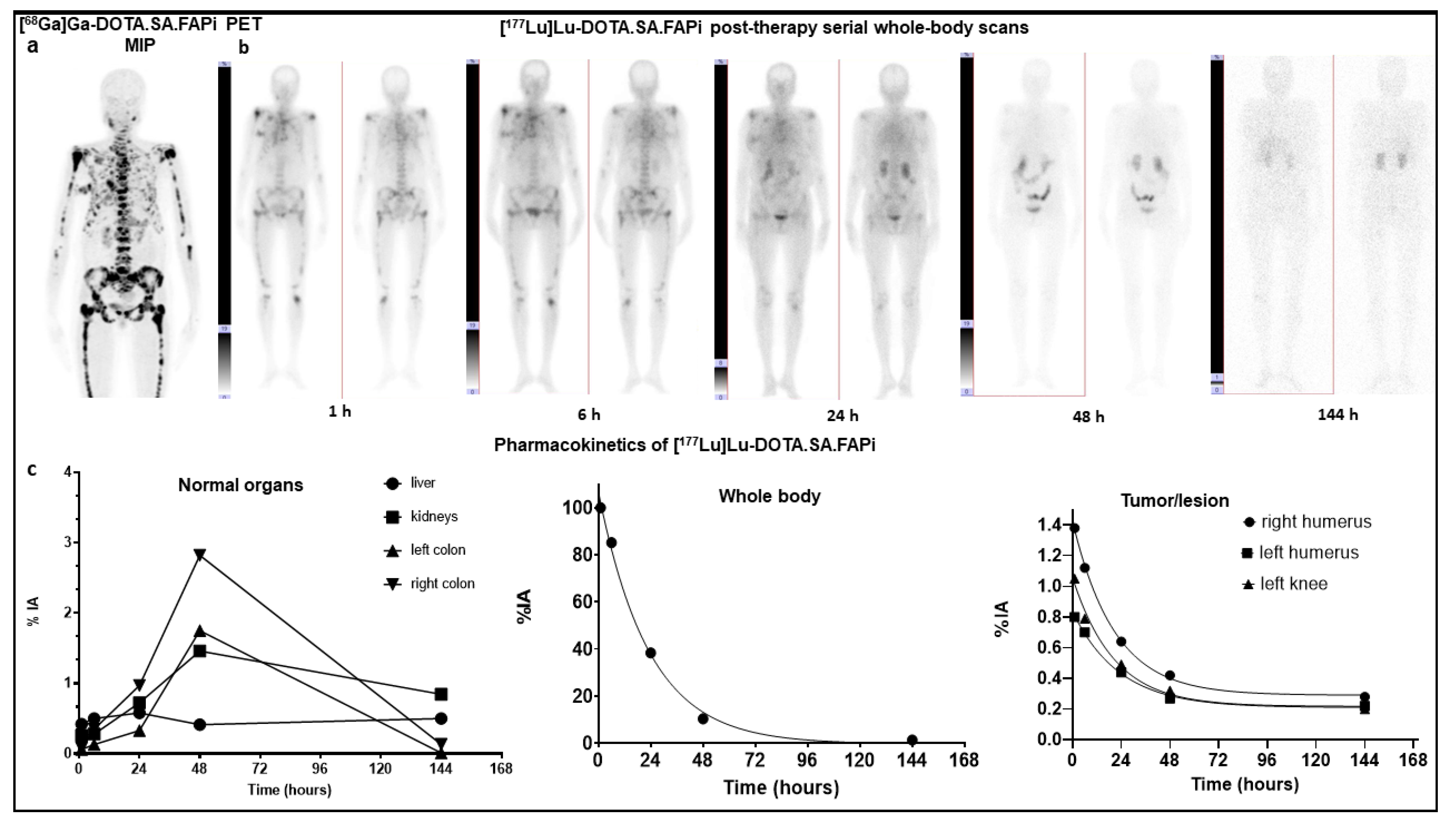
2.3.1. [177Lu]Lu-DOTA.SA.FAPi
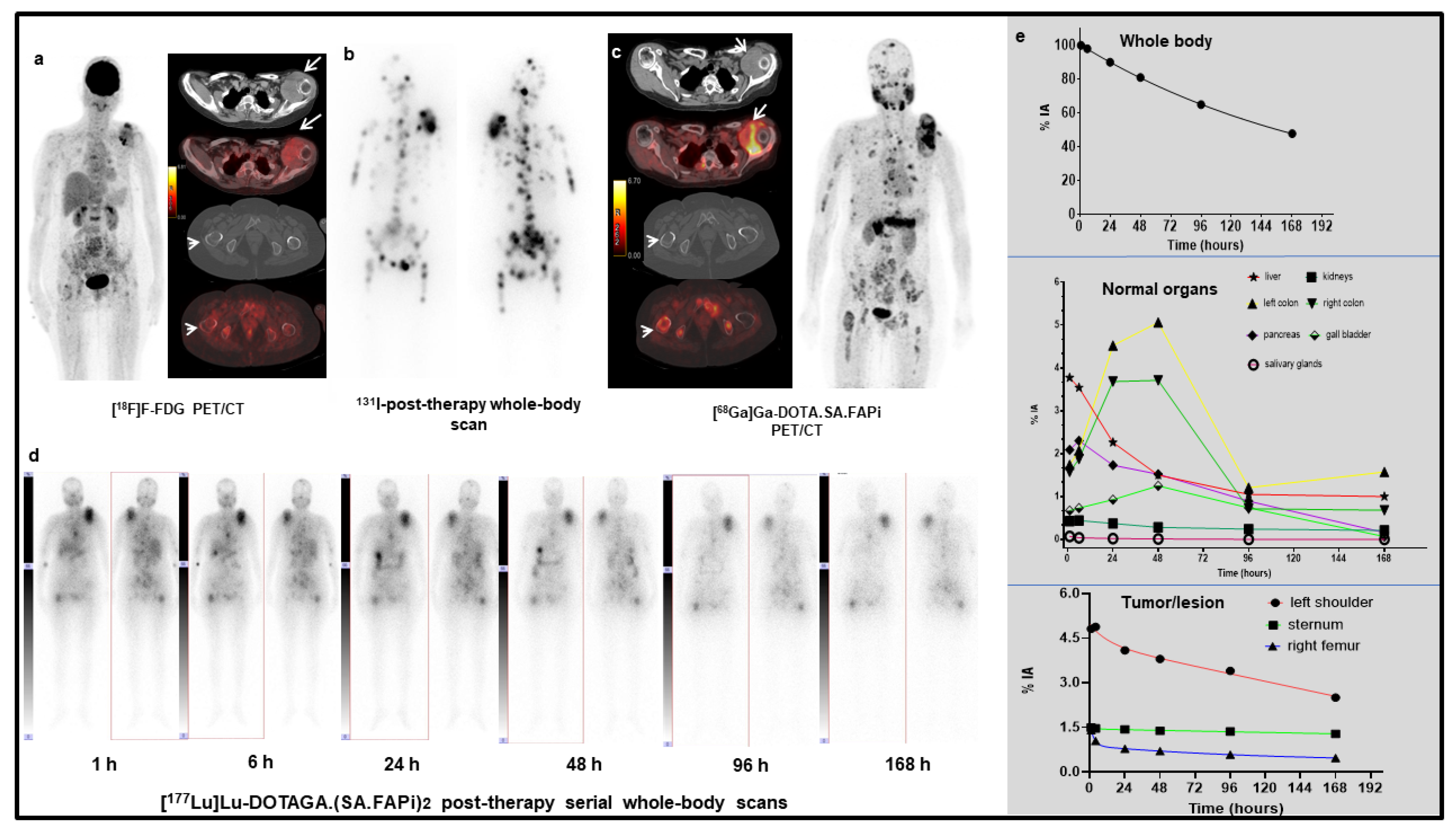
2.3.2. [177Lu]Lu-DOTAGA.(SA.FAPi)2
2.4. Dosimetry Estimate and Te of Normal Organs
2.5. Tumor Pharmacokinetics, Effective Half-Lives, and Absorbed Dose Estimate
2.6. Response Assessment
3. Discussion
3.1. Limitations
3.2. Future Prospects
4. Materials and Methods
4.1. Patient Recruitment
4.2. [68Ga]Ga-DOTA.SA.FAPi PET/CT Imaging
4.3. [177Lu]Lu-DOTA.SA.FAPi and [177Lu]Lu-DOTAGA.(SA.FAPi)2 Radiolabelling
4.4. Post-Therapy [177Lu]Lu-DOTA.SA.FAPi and [177Lu]Lu-DOTAGA.(SA.FAPi)2 Whole Body Scintigraphy
4.5. Image Analysis
4.6. Internal Dose Estimation
4.7. Tumor Dosimetry
4.8. Lood Dosimetry
4.9. Safety
4.10. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jiang, G.-M.; Xu, W.; Du, J.; Zhang, K.-S.; Zhang, Q.-G.; Wang, X.-W.; Liu, Z.-G.; Liu, S.-Q.; Xie, W.-Y.; Liu, H.-F.; et al. The application of the fibroblast activation protein α-targeted immunotherapy strategy. Oncotarget 2016, 7, 33472–33482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamson, E.J.; Keane, F.M.; Tholen, S.; Schilling, O.; Gorrell, M.D. Understanding fibroblast activation protein (FAP): Substrates, activities, expression and targeting for cancer therapy. Proteom.-Clin. Appl. 2014, 8, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Lindner, T.; Loktev, A.; Altmann, A.; Giesel, F.; Kratochwil, C.; Debus, J.; Jäger, D.; Mier, W.; Haberkorn, U. Development of quinoline-based theranostic liganIthe targeting of fibroblast activation protein. J. Nucl. Med. 2018, 59, 1415–1422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loktev, A.; Lindner, T.; Burger, E.M.; Altmann, A.; Giesel, F.; Kratochwil, C.; Debus, J.; Marmé, F.; Jäger, D.; Mier, W.; et al. development of fibroblast activation protein-targeted radiotracers with improved tumor retention. J. Nucl. Med. 2019, 60, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Moon, E.S.; Elvas, F.; Vliegen, G.; De Lombaerde, S.; Vangestel, C.; De Bruycker, S.; Bracke, A.; Eppard, E.; Greifenstein, L.; Klasen, B.; et al. Targeting fibroblast activation protein (FAP): Next generation PET radiotracers using squaramide coupled bifunctional DOTA and DATA5m (superscript) chelators. EJNMMI Radiopharm. Chem. 2020, 5, 19. [Google Scholar] [CrossRef] [PubMed]
- Ballal, S.; Yadav, M.P.; Moon, E.S.; Kramer, V.S.; Roesch, F.; Kumari, S.; Tripathi, M.; ArunRaj, S.T.; Sarswat, S.; Bal, C. Biodistribution, pharmacokinetics, dosimetry of [68Ga]Ga-DOTA.SA.FAPi, and the head-to-head comparison with [18F]F-FDG PET/CT in patients with various cancers. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1915–1931. [Google Scholar] [CrossRef] [PubMed]
- Ballal, S.; Yadav, M.P.; Kramer, V.; Moon, E.S.; Roesch, F.; Tripathi, M.; Mallick, S.; ArunRaj, S.T.; Bal, C. A theranostic approach of [68Ga]Ga-DOTA.SA.FAPi PET/CT-guided [177Lu]Lu-DOTA.SA.FAPi radionuclide therapy in an end-stage breast cancer patient: New frontier in targeted radionuclide therapy. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 942–944. [Google Scholar] [CrossRef] [PubMed]
- Jansen, K.; De Winter, H.; Heirbaut, L.; Cheng, J.D.; Joossens, J.; Lambeir, A.-M.; De Meester, I.; Augustyns, K.; Van der Veken, P. Selective inhibitors of fibroblast activation protein (FAP) with a xanthine scaffold. MedChemComm 2014, 5, 1700–1707. [Google Scholar] [CrossRef]
- Jansen, K.; Heirbaut, L.; Verkerk, R.; Cheng, J.D.; Joossens, J.; Cos, P.; Maes, L.; Lambeir, A.M.; De Meester, I.; Augustyns, K.; et al. Extended structure-activity relationship and pharmaco-kinetic investigation of (4-quinolinoyl)glycyl-2-cyanopyrrolidine inhibitors of fibroblast activation protein (FAP). J. Med. Chem. 2014, 57, 3053–3074. [Google Scholar] [CrossRef] [PubMed]
- Kreppel, B.; Gärtner, F.C.; Marinova, M.; Attenberger, U.; Meisenheimer, M.; Toma, M.; Kristiansen, G.; Feldmann, G.; Moon, E.S.; Roesch, F.; et al. [68Ga]Ga-DATA5m.SA.FAPi PET/CT: Specific Tracer-uptake in Focal Nodular Hyperplasia and potential Role in Liver Tumor Imaging. Nuklearmedizin 2020, 59, 387–389. [Google Scholar] [CrossRef] [PubMed]
- Moon, E.S.; Ballal, S.; Yadav, M.P.; Bal, C.; Rymenant, Y.V.; Stephan, S.; Bracke, A.; der Veken, P.V.; Meester, I.D.; Roesch, F. Fibroblast Activation Protein (FAP) targeting homodimeric FAP inhibitor radiotheranostics: A step to improve tumor uptake and retention time. AJNMMI 2021, accepted. [Google Scholar]
- Koustoulidou, S.; Hoorens, M.W.; Dalm, S.U.; Mahajan, S.; Debets, R.; Seimbille, Y.; de Jong, M. Cancer-Associated Fibroblasts as Players in Cancer Development and Progression and Their Role in targeted Radionuclide Imaging and Therapy. Cancers 2021, 13, 1100. [Google Scholar] [CrossRef] [PubMed]
- Emami, B.; Lyman, J.; Brown, A. Three-Dimensional Photon Treatment Planning Report of the Collaborative Working Group on the Evaluation of Treatment Planning for External Photon Beam RadiotherapyTolerance of normal tissue to therapeutic irradiation. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 109–122. [Google Scholar] [CrossRef]
- Bodei, L.; Cremonesi, M.; Ferrari, M.; Pacifici, M.; Grana, C.M.; Bartolomei, M.; Baio, S.M.; Sansovini, M.; Paganelli, G. Long-term evaluation of renal toxicity after peptide receptor radionuclide therapy with 90Y-DOTATOC and 177Lu-DOTATATE: The role ofassociated risk factors. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 1847–1856. [Google Scholar] [CrossRef] [PubMed]
- Grimm, J.; Lacouture, T.; Croce, R.; Yeo, I.; Zhu, Y.; Xue, J. Dose tolerance limits and dose volume histogram evaluation for stereotactic body radiotherapy. J. Appl. Clin. Med. Phys. 2011, 12, 267–292. [Google Scholar] [CrossRef] [PubMed]
- Kramer, V.; Fernández, R.; Lehnert, W.; Jiménez-Franco, L.D.; Soza-Ried, C.; Eppard, E.; Ceballos, M.; Meckel, M.; Benešová, M.; Umbricht, C.A.; et al. Biodistribution and dosimetry of a single dose of albumin-binding ligand [177Lu]Lu-PSMA-ALB-56 in patients with mCRPC. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Stabin, M.G. MIRDOSE: Personal computer software for internal dose assessmentin nuclear medicine. J. Nucl. Med. 1996, 37, 538–546. [Google Scholar] [PubMed]
- Howard, D.M.; Kearfott, K.J.; Wilderman, S.J.; Dewaraja, Y.K. Comparison of I-131 radioimmunotherapy tumor dosimetry: Unit density sphere model versuspatientspecific Monte Carlo calculations. Cancer Biother. Radiopharm. 2011, 26, 615–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sgouros, G. Bone marrow dosimetry for radioimmunotherapy: Theoretical considerations. J. Nucl. Med. 1993, 34, 689–694. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compound | IC50 (µM) | IC50 (nM) | |||
|---|---|---|---|---|---|
| DPP4 | DPP8 | DPP9 | PREP | FAP | |
| DOTAGA.(SA.FAPi)2 | 0.4 ± 0.07 | 0.42 ± 0.04 | 0.16 ± 0.02 | 0.39 ± 0.02 | 0.92 ± 0.06 |
| [natLu]Lu-DOTAGA.(SA.FAPi)2 | 0.63 ± 0.07 | 0.41 ± 0.03 | 0.18 ± 0.02 | 0.56 ± 0.04 | 1.54 ± 0.15 |
| [natGa]Ga-DOTA.SA.FAPi | >1 | N/A | >1 | 8.7 ± 0.9 | 1.4 ± 0.2 |
| [natLu]Lu-DOTA.SA.FAPi | >1 | N/A | >1 | 2.5 ± 0.4 | 0.8 ± 0.2 |
| Parameters | [177Lu]Lu-DOTA.SA.FAPi | [177Lu]Lu-DOTAGA.(SA.FAPi)2 |
|---|---|---|
| Number of patients | 3 | 7 |
| Age (years) [mean ±SD; range] | 50 ± 17.2 (31–63) | 51 ± 12.7 (26–63) |
| Gender | ||
| Male | 0 | 4 |
| Female | 3 | 3 |
| Type of cancer | ||
| Breast cancer | 3 | 1 |
| Thyroid cancer | 0 | 5 |
| Paraganglioma | 0 | 1 |
| The extent of disease on [68Ga]Ga-DOTA.SA.FAPi PET/CT scan | ||
| Primary | 1 | 0 |
| Lymph nodes | 1 | 3 |
| Skeletal metastases | 3 | 4 |
| Brain metastases | 1 | 0 |
| Liver metastases | 1 | 1 |
| Lung mass | 0 | 1 |
| Injected activity (GBq; IQR) | 2.96 GBq (IQR: 2.2–3 GBq) | 1.48 GBq (IQR: 0.6–1.5) |
| [177Lu]Lu-DOTA.SA.FAPi Group | [177Lu]Lu-DOTAGA.(SA.FAPi)2 Group | |||||
|---|---|---|---|---|---|---|
| Parameters | Baseline (Mean, 95% CI of Mean) | Post-Treatment (Mean, 95% CI of Mean) | p Value | Baseline (Mean, 95% CI of Mean) | Post-Treatment (Mean, 95% CI of Mean) | p Value |
| Haemoglobin (g/dL) | 10.9 (8.9–11.7) | 11 (8.7–11.6) | - | 10.8 (9.1–11.9) | 10.07 (6.9–11) | 0.1121 |
| Platelets (lakhs/µL) | 199 (178–201) | 199 (188–201) | - | 225 (156–295) | 198 (81–239) | 0.2554 |
| Leukocytes 109/L | 6500 (5600–7800) | 7700 (6780–7877) | - | 6781.6 (4216–9348) | 6947.4 (5239–8655) | 0.8571 |
| Creatinine (mg/dL) | 0.8 (0.7–0.9) | 0.77 (0.7–0.9) | - | 0.70 (0.2–1.2) | 0.50 (0.3–0.64) | 0.3853 |
| ALP | 212 (168–225) | 188 (160–234) | - | 98.3 (73.4–123) | 90.5 (70.6–110) | 0.3042 |
| [177Lu]Lu-DOTA.SA.FAPi | [177Lu]Lu-DOTAGA.(SA.FAPi)2 | ||
|---|---|---|---|
| Organ | Mean Absorbed Doses (Gy/GBq) | Organ | Mean Absorbed Doses (Gy/GBq) |
| Adrenals | 7.79E-03 ± 3.69E-04 | Adrenals | 1.27E-02 ± 4.63E-03 |
| Brain | 2.06E-05 ± 2.09E-05 | Brain | 1.17E-04 ± 3.93E-05 |
| Breasts | 4.39E-04 ± 2.64E-04 | Breasts | 6.39E-04 ± 5.30E-05 |
| Esophagus | 1.80E-03 ± 9.12E-04 | Esophagus | 3.07E-03 ± 6.35E-04 |
| Eyes | 2.13E-05 ± 2.04E-05 | Eyes | 9.96E-05 ± 4.11E-05 |
| Gallbladder Wall | 6.06E-03 ± 1.91E-04 | Gallbladder Wall | 7.95E-01 ± 2.58E-01 |
| Left colon | 4.30E-01 ± 9.40E-02 | Left colon | 2.87E+00 ± 1.74E+00 |
| Small Intestine | 2.71E-03 ± 1.74E-04 | Small Intestine | 9.24E-03 ± 4.92E-03 |
| Stomach Wall | 2.03E-03 ± 3.74E-04 | Stomach Wall | 6.62E-03 ± 1.84E-03 |
| Right Colon | 4.72E-01 ± 3.93E-02 | Right Colon | 1.16E+00 ± 8.58E-01 |
| Rectum | 5.08E-04 ± 5.31E-05 | Rectum | 2.02E-03 ± 1.04E-03 |
| Heart Wall | 1.40E-03 ± 1.09E-03 | Heart Wall | 2.57E-03 ± 1.39E-03 |
| Kidneys | 6.18E-01 ± 1.54E-02 | Kidneys | 3.74E-01 ± 2.57E-01 |
| Liver | 1.15E-01 ± 9.02E-03 | Liver | 2.09E-01 ± 2.38E-02 |
| Lungs | 6.10E-02 ± 1.04E-01 | Lungs | 2.21E-03 ± 5.66E-04 |
| Ovaries | 9.08E-04 ± 7.3E-05 | Ovaries | 2.23E-03 ± 2.50E-04 |
| Pancreas | 3.69E-03 ± 2.33E-04 | Pancreas | 6.51E-01 ± 1.37E-01 |
| Prostate | - | Prostate | 2.57E-03 ± 1.35E-03 |
| Salivary glands | 6.56E-05 ± 6.79E-05 | Salivary glands | 1.17E-01 ± 9.53E-03 |
| Red Marrow | 9.84E-04 ± 2.58E-04 | Red Marrow | 1.73E-02 ± 1.82E-02 |
| Osteogenic Cells | 1.18E-03 ± 2.89E-04 | Osteogenic Cells | 8.57E-03 ± 6.95E-03 |
| Spleen | 3.99E-03 ± 2.18E-04 | Spleen | 6.36E-03 ± 1.52E-03 |
| Testes | - | Testes | 1.71E-04 ± 9.97E-05 |
| Thymus | 1.22E-03 ± 1.49E-03 | Thymus | 1.00E-03 ± 3.09E-04 |
| Thyroid | 4.53E-04 ± 5.25E-04 | Thyroid | 3.98E-04 ± 8.53E-05 |
| Urinary Bladder Wall | 4.05E-04 ± 4.12E-05 | Urinary Bladder Wall | 1.28E-03 ± 4.29E-04 |
| Uterus | 7.84E-04 ± 7.47E-04 | Uterus | 2.18E-03 ± 2.70E-04 |
| Total Body | 1.10E-02 ± 1.72E-03 | Total Body | 2.33E-02 ± 6.15E-03 |
| Patient S.No | Cancer Type | Site of Lesion | Te Tumor (h) | No of Disintegrations or Residence Time | Mass of Lesion (g) | Absorbed Dose (Gy/GBq) |
|---|---|---|---|---|---|---|
| 1. | Right breast cancer | Right breast primary tumor | 17 | 2.44E+00 | 800 | 2.52E-01 |
| Right shoulder skeletal lesion | 13.7 | 3.09E-01 | 46.1 | 5.40E-01 | ||
| 2. | B/L breast cancer | Right shoulder skeletal lesion | 14 | 4.30E-01 | 22 | 1.57E+00 |
| Left shoulder skeletal lesion | 16 | 3.54E-01 | 15 | 1.89E+00 | ||
| Left knee skeletal lesion | 14 | 0.41E-01 | 15 | 2.13E+00 | ||
| 3. | Right breast cancer | Ileum | 12.6 | 2.80E-01 | 32 | 6.03E-01 |
| Pubis | 12 | 1.02E-01 | 35 | 2.34E-01 | ||
| Total number of lesions | 7 | |||||
| Median (IQR) | 14 (12.8–15.5) | 3.00E-01 (1.46E-01–4.11E-01) | 32 (16.8–43.3) | 6.03E-01 (2.30E-01–1.81E+00) |
| Patient S.No | Cancer Type | Site of Lesion | Te in Tumor (h) | Number of Disintegrations or Residence Time | Mass of Lesion (g) | Absorbed Dose (Gy/GBq) |
|---|---|---|---|---|---|---|
| 1 | Radioiodine refractory follicular thyroid cancer | Right ileum skeletal lesion | 99 | 3.37E+00 | 65.4 | 4.16E+00 |
| Femur bone lesion | 231 | 9.80E+00 | 158 | 7.99E+00 | ||
| 2 | Triple negative breast cancer | Right lung mass | 40.7 | 3.47E+00 | 50.7 | 5.51E+00 |
| 3 | Radioiodine refractory papillary thyroid cancer | Right lung nodule | 86.6 | 6.02E+00 | 1.5 | 3.17E+02 |
| 4 | Radioiodine refractory papillary thyroid cancer | Left shoulder bone lesion | 86.6 | 6.41E+00 | 189 | 2.64E+00 |
| Sternum | 89.5 | 4.47E+00 | 3.96 | 8.97E+01 | ||
| Right head of femur lesion | 48.6 | 3.97E+00 | 23.2 | 1.37E+01 | ||
| 5 | Paraganglioma | Skull | 27.7 | 1.82E-01 | 6 | 2.40E+00 |
| Anterior rib lesion | 27.9 | 6.48E-01 | 5.6 | 9.33E+00 | ||
| Posterior rib lesion | 23.9 | 8.51E-01 | 30 | 2.28E+00 | ||
| 6 | Anaplastic thyroid cancer | Right Neck mass | 90.2 | 1.54E+01 | 250 | 5.02E+00 |
| 7 | Medullary thyroid cancer | Liver lesion | 115.5 | 3.51E+01 | 33.4 | 8.44E+01 |
| Total number of lesions | 12 | |||||
| Median (IQR) | 86.6 (34.3–94.6) | 4.22E+00 (2.11E+0–8.10 E+00) | 31.7 (5.8–111.7) | 6.70E+00 (3.40E+00 to 4.9E+01) |
| Te | [177Lu]Lu-DOTA.SA.FAPi | [177Lu]Lu-DOTAGA.(SA.FAPi)2 | p-Value |
|---|---|---|---|
| Whole body Te | N = 3 patients | N = 7 patients | |
| Median (IQR) | 23.1 (17.8–31.5) | 46.2 (38.5–70.1) | 0.0167 |
| Tumor Te | N = 7 lesions | N = 12 lesions | |
| Median (IQR) | 14 (12.8–15.5) | 86.6 (34.3–94.6) | 0.0004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ballal, S.; Yadav, M.P.; Moon, E.S.; Kramer, V.S.; Roesch, F.; Kumari, S.; Bal, C. First-In-Human Results on the Biodistribution, Pharmacokinetics, and Dosimetry of [177Lu]Lu-DOTA.SA.FAPi and [177Lu]Lu-DOTAGA.(SA.FAPi)2. Pharmaceuticals 2021, 14, 1212. https://doi.org/10.3390/ph14121212
Ballal S, Yadav MP, Moon ES, Kramer VS, Roesch F, Kumari S, Bal C. First-In-Human Results on the Biodistribution, Pharmacokinetics, and Dosimetry of [177Lu]Lu-DOTA.SA.FAPi and [177Lu]Lu-DOTAGA.(SA.FAPi)2. Pharmaceuticals. 2021; 14(12):1212. https://doi.org/10.3390/ph14121212
Chicago/Turabian StyleBallal, Sanjana, Madhav Prasad Yadav, Euy Sung Moon, Vasko S Kramer, Frank Roesch, Samta Kumari, and Chandrasekhar Bal. 2021. "First-In-Human Results on the Biodistribution, Pharmacokinetics, and Dosimetry of [177Lu]Lu-DOTA.SA.FAPi and [177Lu]Lu-DOTAGA.(SA.FAPi)2" Pharmaceuticals 14, no. 12: 1212. https://doi.org/10.3390/ph14121212