
Lipid-Based Nanocarriers as Topical Drug Delivery Systems for Intraocular Diseases

 , ,
, ,
Abstract
:1. Introduction
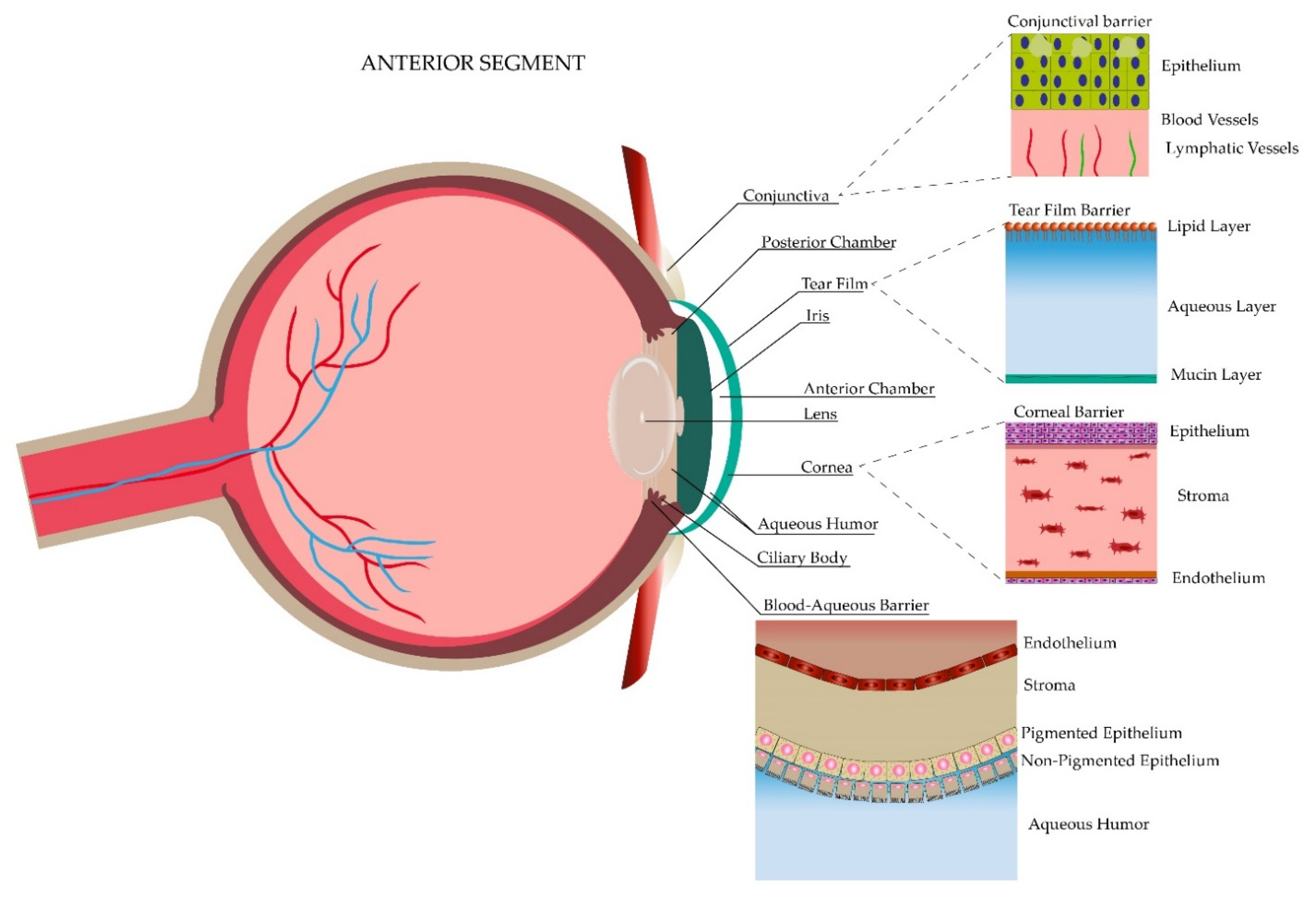
2. General Anatomy of the Ocular Globe
3. Ocular Drug Barriers
3.1. Static Barriers
3.2. Dynamic Barriers
3.3. Metabolic Barriers
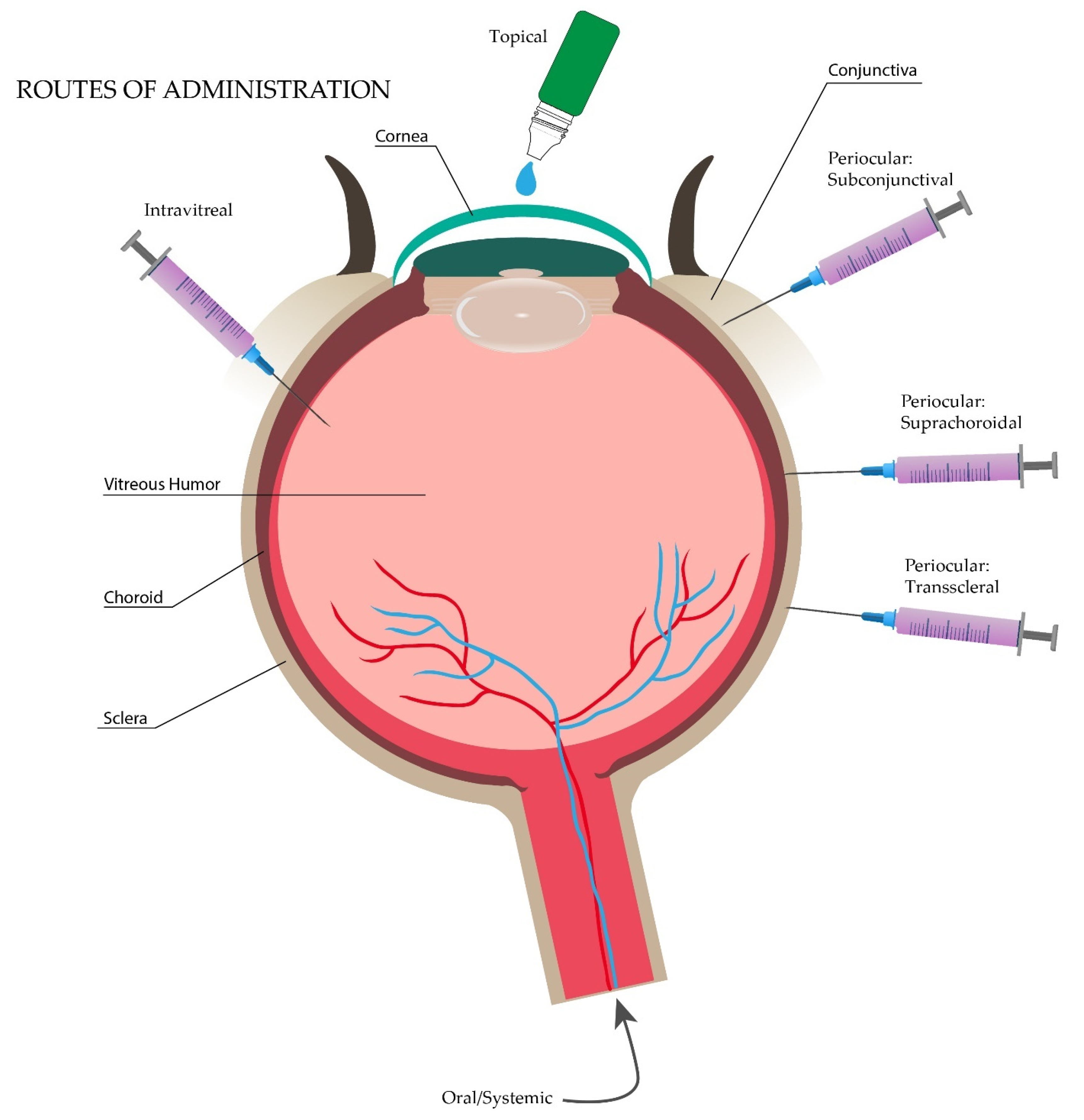
4. Ocular Drug Delivery Routes
5. Topical Nanosystems for Intraocular Drug Delivery
5.1. Topical Polymeric Nanosystems for Intraocular Drug Delivery
5.2. Topical Non-Polymeric Nanosystems for Intraocular Drug Delivery
5.3. Lipid-Based Nanosystems for Intraocular Drug Delivery
6. Topical Lipid-Based Nanosystems for Intraocular Drug Delivery
6.1. Emulsion-Based
6.2. Vesicle-Based
6.3. Particulate Systems
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, A.; Cholkar, K.; Agrahari, V.; Mitra, A.K. Ocular drug delivery systems: An overview. World J. Pharmacol. 2013, 2, 47. [Google Scholar] [CrossRef]
- Humayun, M.; Santos, A.; Altamirano, J.C.; Ribeiro, R.; Gonzalez, R.; de la Rosa, A.; Shih, J.; Pang, C.; Jiang, F.; Calvillo, P. Implantable micropump for drug delivery in patients with diabetic macular edema. Transl. Vis. Sci. Technol. 2014, 3, 5. [Google Scholar] [CrossRef] [Green Version]
- Faraji, A.H.; Wipf, P. Nanoparticles in cellular drug delivery. Bioorg. Med. Chem. 2009, 17, 2950–2962. [Google Scholar] [CrossRef]
- Hyman, P. Bacteriophages and nanostructured materials. Adv. Appl. Microbiol. 2012, 78, 55–73. [Google Scholar] [PubMed]
- Saji, V.S.; Choe, H.C.; Yeung, K.W. Nanotechnology in biomedical applications: A review. Int. J. Nano Biomater. 2010, 3, 119–139. [Google Scholar] [CrossRef]
- Al-Halafi, A.M. Nanocarriers of nanotechnology in retinal diseases. Saudi J. Ophthalmol. 2014, 28, 304–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, H.-H.; Chan, E.C.; Lee, J.H.; Bee, Y.-S.; Lin, T.-W.; Dusting, G.J.; Liu, G.-S. Nanocarriers for treatment of ocular neovascularization in the back of the eye: New vehicles for ophthalmic drug delivery. Nanomedicine 2015, 10, 2093–2107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, D.K.; Shandilya, R.; Mishra, P.K. Lipid based nanocarriers: A translational perspective. Nanomed. Nanotechnol. Biol. Med. 2018, 14, 2023–2050. [Google Scholar] [CrossRef]
- Jain, A.K.; Thareja, S. In vitro and in vivo characterization of pharmaceutical nanocarriers used for drug delivery. Artif. Cells Nanomed. Biotechnol. 2019, 47, 524–539. [Google Scholar] [CrossRef] [Green Version]
- Navarro-Partida, J.; Altamirano-Vallejo, J.C.; Lopez-Naranjo, E.J.; Gonzalez-De la Rosa, A.; Manzano-Ramírez, A.; Apatiga-Castro, L.M.; Armendáriz-Borunda, J.; Santos, A. Topical Triamcinolone Acetonide-Loaded Liposomes as Primary Therapy for Macular Edema Secondary to Branch Retinal Vein Occlusion: A Pilot Study. J. Ocul. Pharmacol. Ther. 2020, 36, 393–403. [Google Scholar] [CrossRef]
- Navarro-Partida, J.; Altamirano-Vallejo, J.C.; Armendariz-Borunda, J.; Castro-Castaneda, C.R.; Santos, A. Safety and Tolerability of Topical Ophthalmic Triamcinolone Acetonide-Loaded Liposomes Formulation and Evaluation of Its Biologic Activity in Patients with Diabetic Macular Edema. Pharmaceutics 2021, 13, 322. [Google Scholar] [CrossRef]
- Gaudana, R.; Ananthula, H.K.; Parenky, A.; Mitra, A.K. Ocular drug delivery. AAPS J. 2010, 12, 348–360. [Google Scholar] [CrossRef]
- Varela-Fernández, R.; Díaz-Tomé, V.; Luaces-Rodríguez, A.; Conde-Penedo, A.; García-Otero, X.; Luzardo-Álvarez, A.; Fernández-Ferreiro, A.; Otero-Espinar, F.J. Drug delivery to the posterior segment of the eye: Biopharmaceutic and pharmacokinetic considerations. Pharmaceutics 2020, 12, 269. [Google Scholar] [CrossRef] [Green Version]
- Altamirano-Vallejo, J.C.; Navarro-Partida, J.; Gonzalez-De la Rosa, A.; Hsiao, J.H.; Olguín-Gutierrez, J.S.; Gonzalez-Villegas, A.C.; Keller, B.C.; Bouzo-Lopez, L.; Santos, A. Characterization and pharmacokinetics of triamcinolone acetonide-loaded liposomes topical formulations for vitreoretinal drug delivery. J. Ocul. Pharmacol. Ther. 2018, 34, 416–425. [Google Scholar] [CrossRef]
- Mason, J.O., III; Somaiya, M.D.; Singh, R.J. Intravitreal concentration and clearance of triamcinolone acetonide in nonvitrectomized human eyes. Retina 2004, 24, 900–904. [Google Scholar] [CrossRef] [PubMed]
- Ammar, H.O.; Salama, H.; Ghorab, M.; Mahmoud, A. Nanoemulsion as a potential ophthalmic delivery system for dorzolamide hydrochloride. AAPS Pharmscitech 2009, 10, 808–819. [Google Scholar] [CrossRef] [Green Version]
- Kels, B.D.; Grzybowski, A.; Grant-Kels, J.M. Human ocular anatomy. Clin. Dermatol. 2015, 33, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Goel, M.; Picciani, R.G.; Lee, R.K.; Bhattacharya, S.K. Aqueous humor dynamics: A review. Open Ophthalmol. J. 2010, 4, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sunderland, D.K.; Sapra, A. Physiology, Aqueous Humor Circulation; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Santos, A.; Altamirano-Vallejo, J.; Navarro-Partida, J. Breaking down the Barrier: Topical Liposomes as Nanocarriers for Drug Delivery into the Posterior Segment of the Eyeball. In Role of Novel Drug Delivery Vehicles in Nanobiomedicine; IntechOpen: London, UK, 2019. [Google Scholar]
- Murthy, K.R.; Goel, R.; Subbannayya, Y.; Jacob, H.K.; Murthy, P.R.; Manda, S.S.; Patil, A.H.; Sharma, R.; Sahasrabuddhe, N.A.; Parashar, A.; et al. Proteomic analysis of human vitreous humor. Clin. Proteom. 2014, 11, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nayak, K.; Misra, M. A review on recent drug delivery systems for posterior segment of eye. Biomed. Pharmacother. 2018, 107, 1564–1582. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, B.; Kompella, U.B. Ocular drug delivery. In Pharmacologic Therapy of Ocular Disease; Springer: Berlin/Heidelberg, Germany, 2016; pp. 57–93. [Google Scholar]
- Peters, E.; Colby, K. The tear film. In Foundation Volume 2: Physiology of the Eye and Visual System; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Eghrari, A.O.; Riazuddin, S.A.; Gottsch, J.D. Overview of the cornea: Structure, function, and development. Prog. Mol. Biol. Transl. Sci. 2015, 134, 7–23. [Google Scholar]
- Gote, V.; Sikder, S.; Sicotte, J.; Pal, D. Ocular drug delivery: Present innovations and future challenges. J. Pharmacol. Exp. Ther. 2019, 370, 602–624. [Google Scholar] [CrossRef]
- Hornof, M.; Toropainen, E.; Urtti, A. Cell culture models of the ocular barriers. Eur. J. Pharm. Biopharm. 2005, 60, 207–225. [Google Scholar] [CrossRef]
- Bachu, R.D.; Chowdhury, P.; Al-Saedi, Z.H.; Karla, P.K.; Boddu, S.H. Ocular drug delivery barriers—Role of nanocarriers in the treatment of anterior segment ocular diseases. Pharmaceutics 2018, 10, 28. [Google Scholar] [CrossRef] [Green Version]
- Halasz, K.; Kelly, S.J.; Iqbal, M.T.; Pathak, Y.; Sutariya, V. Micro/nanoparticle delivery systems for ocular diseases. Assay Drug Dev. Technol. 2019, 17, 152–166. [Google Scholar] [CrossRef]
- Wang, W.; Sasaki, H.; Chien, D.-S.; Lee, V.H. Lipophilicity influence on conjunctival drug penetration in the pigmented rabbit: A comparison with corneal penetration. Curr. Eye Res. 1991, 10, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Hämäläinen, K.M.; Kontturi, K.; Auriola, S.; Murtomäki, L.; Urtti, A. Estimation of pore size and pore density of biomembranes from permeability measurements of polyethylene glycols using an effusion-like approach. J. Control. Release 1997, 49, 97–104. [Google Scholar] [CrossRef]
- Lee, J.; Pelis, R.M. Drug transport by the blood–aqueous humor barrier of the eye. Drug Metab. Dispos. 2016, 44, 1675–1681. [Google Scholar] [CrossRef]
- Coca-Prados, M. The blood-aqueous barrier in health and disease. J. Glaucoma 2014, 23, S36–S38. [Google Scholar] [CrossRef] [PubMed]
- Pradeep, T.; Mehra, D.; Le, P.H. Histology, Eye; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Shah, S.S.; Denham, L.V.; Elison, J.R.; Bhattacharjee, P.S.; Clement, C.; Huq, T.; Hill, J.M. Drug delivery to the posterior segment of the eye for pharmacologic therapy. Expert Rev. Ophthalmol. 2010, 5, 75–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, M.; Humphries, P. The blood-retina barrier. In Biology and Regulation of Blood-Tissue Barriers; Springer: Berlin/Heidelberg, Germany, 2013; pp. 70–84. [Google Scholar]
- Gaudana, R.J.; Barot, M.; Patel, A.; Khurana, V.; Mitra, A.K. Barriers for posterior segment ocular drug delivery. Treatise Ocul. Drug Deliv. 2013, 1, 68. [Google Scholar]
- Farid, R.M.; El-Salamouni, N.S.; El-Kamel, A.H.; El-Gamal, S.S. Lipid-based nanocarriers for ocular drug delivery. In Nanostructures for Drug Delivery; Elsevier: Amsterdam, The Netherlands, 2017; pp. 495–522. [Google Scholar]
- Norn, M. Tear secretion in normal eyes: Estimated by a New Method: The Lacrimal Streak Dilution Test. Acta Ophthalmol. 1965, 43, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Boddu, S.H.; Gunda, S.; Earla, R.; Mitra, A.K. Ocular microdialysis: A continuous sampling technique to study pharmacokinetics and pharmacodynamics in the eye. Bioanalysis 2010, 2, 487–507. [Google Scholar] [CrossRef] [PubMed]
- Chen, L. Ocular lymphatics: State-of-the-art review. Lymphology 2009, 42, 66. [Google Scholar] [PubMed]
- Agrahari, V.; Mandal, A.; Agrahari, V.; Trinh, H.M.; Joseph, M.; Ray, A.; Hadji, H.; Mitra, R.; Pal, D.; Mitra, A.K. A comprehensive insight on ocular pharmacokinetics. Drug Deliv. Transl. Res. 2016, 6, 735–754. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, R.; Harris, A.; Wentz, S.M.; Moore, N.A.; Siesky, B.A. Anatomy and regulation of the optic nerve blood flow. Encyclopedia of the Eye; Academic Press: Cambridge, MA, USA, 2017. [Google Scholar]
- Abarca, E.M.; Salmon, J.H.; Gilger, B.C. Effect of choroidal perfusion on ocular tissue distribution after intravitreal or suprachoroidal injection in an arterially perfused ex vivo pig eye model. J. Ocul. Pharmacol. Ther. 2013, 29, 715–722. [Google Scholar] [CrossRef]
- Duvvuri, S.; Majumdar, S.; Mitra, A.K. Role of metabolism in ocular drug delivery. Curr. Drug Metab. 2004, 5, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Joseph, R.R.; Venkatraman, S.S. Drug delivery to the eye: What benefits do nanocarriers offer? Nanomedicine 2017, 12, 683–702. [Google Scholar] [CrossRef] [Green Version]
- Tsai, C.-H.; Wang, P.-Y.; Lin, I.; Huang, H.; Liu, G.-S.; Tseng, C.-L. Ocular drug delivery: Role of degradable polymeric nanocarriers for ophthalmic application. Int. J. Mol. Sci. 2018, 19, 2830. [Google Scholar] [CrossRef] [Green Version]
- Bourne, R.R.; Flaxman, S.R.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; Leasher, J.; Limburg, H. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e888–e897. [Google Scholar] [CrossRef] [Green Version]
- Souto, E.B.; Dias-Ferreira, J.; López-Machado, A.; Ettcheto, M.; Cano, A.; Camins Espuny, A.; Espina, M.; Garcia, M.L.; Sánchez-López, E. Advanced formulation approaches for ocular drug delivery: State-of-the-art and recent patents. Pharmaceutics 2019, 11, 460. [Google Scholar] [CrossRef] [Green Version]
- Prausnitz, M.R.; Noonan, J.S. Permeability of cornea, sclera, and conjunctiva: A literature analysis for drug delivery to the eye. J. Pharm. Sci. 1998, 87, 1479–1488. [Google Scholar] [CrossRef]
- Davis, B.M.; Normando, E.M.; Guo, L.; Turner, L.A.; Nizari, S.; O’Shea, P.; Moss, S.E.; Somavarapu, S.; Cordeiro, M.F. Topical delivery of Avastin to the posterior segment of the eye in vivo using annexin A5-associated liposomes. Small 2014, 10, 1575–1584. [Google Scholar] [CrossRef]
- Nguyen, H.; Eng, S.; Ngo, T.; Dass, C.R. Delivery of therapeutics for deep-seated ocular conditions–status quo. J. Pharm. Pharmacol. 2018, 70, 994–1001. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Jones, L.; Gu, F.X. Nanomaterials for ocular drug delivery. Macromol. Biosci. 2012, 12, 608–620. [Google Scholar] [CrossRef]
- Vadlapudi, A.D.; Mitra, A.K. Nanomicelles: An emerging platform for drug delivery to the eye. Ther. Deliv. 2013, 4, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szebeni, J. Complement activation-related pseudoallergy: A new class of drug-induced acute immune toxicity. Toxicology 2005, 216, 106–121. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Park, K. Polymeric micelles and alternative nanonized delivery vehicles for poorly soluble drugs. Int. J. Pharm. 2013, 453, 198–214. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Sun, L.; Zhou, L.; Cheng, Y.; Cao, F. Functional chitosan oligosaccharide nanomicelles for topical ocular drug delivery of dexamethasone. Carbohydr. Polym. 2020, 227, 115356. [Google Scholar] [CrossRef] [PubMed]
- Almeida, H.; Amaral, M.H.; Lobão, P.; Silva, A.C.; Loboa, J.M.S. Applications of polymeric and lipid nanoparticles in ophthalmic pharmaceutical formulations: Present and future considerations. J. Pharm. Pharm. Sci. 2014, 17, 278–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yenice, İ.; Mocan, M.C.; Palaska, E.; Bochot, A.; Bilensoy, E.; Vural, İ.; İrkeç, M.; Hıncal, A.A. Hyaluronic acid coated poly-ε-caprolactone nanospheres deliver high concentrations of cyclosporine A into the cornea. Exp. Eye Res. 2008, 87, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, S.K.; Dilnawaz, F.; Krishnakumar, S. Nanotechnology in ocular drug delivery. Drug Discov. Today 2008, 13, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Gupta, U.; Perumal, O. Chapter 15—Dendrimers and its biomedical applications. In Natural and Synthetic Biomedical Polymers; Kumbar, S., Laurencin, C., Deng, M., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; pp. 243–257. [Google Scholar]
- Gaudana, R.; Jwala, J.; Boddu, S.H.; Mitra, A.K. Recent perspectives in ocular drug delivery. Pharm. Res. 2009, 26, 1197–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.; Tyagi, P.; Kadam, R.S.; Holden, C.A.; Kompella, U.B. Hybrid dendrimer hydrogel/PLGA nanoparticle platform sustains drug delivery for one week and antiglaucoma effects for four days following one-time topical administration. ACS Nano 2012, 6, 7595–7606. [Google Scholar] [CrossRef] [PubMed]
- Sultana, F.; Manirujjaman, M.; Imran-Ul-Haque, M.A.; Sharmin, S. An overview of nanogel drug delivery system. J. Appl. Pharm. Sci. 2013, 3, 95–105. [Google Scholar]
- Soni, K.S.; Desale, S.S.; Bronich, T.K. Nanogels: An overview of properties, biomedical applications and obstacles to clinical translation. J. Control. Release 2016, 240, 109–126. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Sun, L.; Fang, S.; Wang, S.; Chen, J.; Xiao, X.; Liu, C. Thermosensitive in situ nanogel as ophthalmic delivery system of curcumin: Development, characterization, in vitro permeation and in vivo pharmacokinetic studies. Pharm. Dev. Technol. 2016, 21, 576–582. [Google Scholar] [CrossRef]
- Mohammed, N.; Rejinold, N.S.; Mangalathillam, S.; Biswas, R.; Nair, S.V.; Jayakumar, R. Fluconazole loaded chitin nanogels as a topical ocular drug delivery agent for corneal fungal infections. J. Biomed. Nanotechnol. 2013, 9, 1521–1531. [Google Scholar] [CrossRef]
- Masse, F.; Ouellette, M.; Lamoureux, G.; Boisselier, E. Gold nanoparticles in ophthalmology. Med. Res. Rev. 2019, 39, 302–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, F.-Y.; Zhang, J.-W.; Li, R.-F.; Wang, Z.-X.; Wang, W.-J.; Wang, W. Unique roles of gold nanoparticles in drug delivery, targeting and imaging applications. Molecules 2017, 22, 1445. [Google Scholar] [CrossRef] [Green Version]
- Connor, E.E.; Mwamuka, J.; Gole, A.; Murphy, C.J.; Wyatt, M.D. Gold nanoparticles are taken up by human cells but do not cause acute cytotoxicity. Small 2005, 1, 325–327. [Google Scholar] [CrossRef]
- Dobrovolskaia, M.A.; McNeil, S.E. Immunological properties of engineered nanomaterials. Nat. Nanotechnol. 2007, 2, 469. [Google Scholar] [CrossRef]
- Villiers, C.L.; Freitas, H.; Couderc, R.; Villiers, M.-B.; Marche, P.N. Analysis of the toxicity of gold nano particles on the immune system: Effect on dendritic cell functions. J. Nanopart. Res. 2010, 12, 55–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orlando, A.; Colombo, M.; Prosperi, D.; Corsi, F.; Panariti, A.; Rivolta, I.; Masserini, M.; Cazzaniga, E. Evaluation of gold nanoparticles biocompatibility: A multiparametric study on cultured endothelial cells and macrophages. J. Nanopart. Res. 2016, 18, 1–12. [Google Scholar] [CrossRef]
- Fan, J.; Hung, W.; Li, W.; Yeh, J. Biocompatibility study of gold nanoparticles to human cells. In Proceedings of the 13th International Conference on Biomedical Engineering, Singapore, 3–6 December 2008; pp. 870–873. [Google Scholar]
- Ayata, N.; Sezer, A.D.; Bucak, S.; Turanli, E.T. Preparation and in vitro characterization of monoclonal antibody ranibizumab conjugated magnetic nanoparticles for ocular drug delivery. Braz. J. Pharm. Sci. 2020, 56, e18171. [Google Scholar] [CrossRef]
- Masse, F.; Ouellette, M.; Boisselier, E. Ultrastable gold nanoparticles as a new drug vector for glaucoma therapy. Investig. Ophthalmol. Vis. Sci. 2018, 59, 3512. [Google Scholar]
- Cho, W.-K.; Kang, S.; Choi, H.; Rho, C.R. Topically administered gold nanoparticles inhibit experimental corneal neovascularization in mice. Cornea 2015, 34, 456–459. [Google Scholar] [CrossRef]
- Mehmood, A.; Ghafar, H.; Yaqoob, S.; Gohar, U.F.; Ahmad, B. Mesoporous silica nanoparticles: A review. J. Dev. Drugs 2017, 6. [Google Scholar] [CrossRef]
- Narayan, R.; Nayak, U.Y.; Raichur, A.M.; Garg, S. Mesoporous silica nanoparticles: A comprehensive review on synthesis and recent advances. Pharmaceutics 2018, 10, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.-N.; Ko, S.A.; Park, C.G.; Lee, S.H.; Huh, B.K.; Park, Y.H.; Kim, Y.K.; Ha, A.; Park, K.H.; Choy, Y.B. Amino-functionalized mesoporous silica particles for ocular delivery of brimonidine. Mol. Pharm. 2018, 15, 3143–3152. [Google Scholar] [CrossRef]
- Van Meer, G.; Voelker, D.R.; Feigenson, G.W. Membrane lipids: Where they are and how they behave. Nat. Rev. Mol. Cell Biol. 2008, 9, 112–124. [Google Scholar] [CrossRef]
- Liu, Y.; Lin, X.; Tang, X. Lipid emulsions as a potential delivery system for ocular use of azithromycin. Drug Dev. Ind. Pharm. 2009, 35, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Ying, L.; Tahara, K.; Takeuchi, H. Drug delivery to the ocular posterior segment using lipid emulsion via eye drop administration: Effect of emulsion formulations and surface modification. Int. J. Pharm. 2013, 453, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Talegaonkar, S.; Azeem, A.; Ahmad, F.J.; Khar, R.K.; Pathan, S.A.; Khan, Z.I. Microemulsions: A novel approach to enhanced drug delivery. Recent Pat. Drug Deliv. Formul. 2008, 2, 238–257. [Google Scholar] [CrossRef] [PubMed]
- Kale, S.N.; Deore, S.L. Emulsion micro emulsion and nano emulsion: A review. Syst. Rev. Pharm. 2017, 8, 39. [Google Scholar] [CrossRef] [Green Version]
- Karunaratne, D.N.; Pamunuwa, G.; Ranatunga, U. Introductory chapter: Microemulsions. In Properties and Uses of Microemulsions; IntechOpen: London, UK, 2017. [Google Scholar]
- Gautam, N.; Kesavan, K. Development of microemulsions for ocular delivery. Ther. Deliv. 2017, 8, 313–330. [Google Scholar] [CrossRef]
- Lawrence, M.J.; Rees, G.D. Microemulsion-based media as novel drug delivery systems. Adv. Drug Deliv. Rev. 2000, 45, 89–121. [Google Scholar] [CrossRef]
- Fialho, S.L.; Da Silva-Cunha, A. New vehicle based on a microemulsion for topical ocular administration of dexamethasone. Clin. Exp. Ophthalmol. 2004, 32, 626–632. [Google Scholar] [CrossRef]
- Vandamme, T.F. Microemulsions as ocular drug delivery systems: Recent developments and future challenges. Prog. Retin. Eye Res. 2002, 21, 15–34. [Google Scholar] [CrossRef]
- Shah, J.; Nair, A.B.; Jacob, S.; Patel, R.K.; Shah, H.; Shehata, T.M.; Morsy, M.A. Nanoemulsion based vehicle for effective ocular delivery of moxifloxacin using experimental design and pharmacokinetic study in rabbits. Pharmaceutics 2019, 11, 230. [Google Scholar] [CrossRef] [Green Version]
- Kaur, I.P.; Kakkar, S. Nanotherapy for posterior eye diseases. J. Control. Release 2014, 193, 100–112. [Google Scholar] [CrossRef] [PubMed]
- Bangham, A.; Standish, M.M.; Watkins, J.C. Diffusion of univalent ions across the lamellae of swollen phospholipids. J. Mol. Biol. 1965, 13, 238–252. [Google Scholar] [CrossRef]
- Perrie, Y. Gregory Gregoriadis: Introducing liposomes to drug delivery. J. Drug Target. 2008, 16, 518–519. [Google Scholar] [CrossRef]
- Rahimpour, Y.; Hamishehkar, H. Liposomes in cosmeceutics. Expert Opin. Drug Deliv. 2012, 9, 443–455. [Google Scholar] [CrossRef]
- Kumar, R. Lipid-based nanoparticles for drug-delivery systems. In Nanocarriers for Drug Delivery; Elsevier: Amsterdam, The Netherlands, 2019; pp. 249–284. [Google Scholar]
- Van Hoogevest, P.; Wendel, A. The use of natural and synthetic phospholipids as pharmaceutical excipients. Eur. J. Lipid Sci. Technol. 2014, 116, 1088–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, R.; Iezhitsa, I.; Agarwal, P.; Abdul Nasir, N.A.; Razali, N.; Alyautdin, R.; Ismail, N.M. Liposomes in topical ophthalmic drug delivery: An update. Drug Deliv. 2016, 23, 1075–1091. [Google Scholar] [CrossRef]
- Lipowsky, R. Generic interactions of flexible membranes. Handb. Biol. Phys. 1995, 1, 521–602. [Google Scholar]
- Knoll, G.; Burger, K.; Bron, R.; van Meer, G.; Verkleij, A.J. Fusion of liposomes with the plasma membrane of epithelial cells: Fate of incorporated lipids as followed by freeze fracture and autoradiography of plastic sections. J. Cell Biol. 1988, 107, 2511–2521. [Google Scholar] [CrossRef]
- Wojewodzka, J.; Pazdzior, G.; Langner, M. A method to evaluate the effect of liposome lipid composition on its interaction with the erythrocyte plasma membrane. Chem. Phys. Lipids 2005, 135, 181–187. [Google Scholar] [CrossRef]
- Mishra, G.P.; Bagui, M.; Tamboli, V.; Mitra, A.K. Recent applications of liposomes in ophthalmic drug delivery. J. Drug Deliv. 2011, 2011. [Google Scholar] [CrossRef] [Green Version]
- Tiwari, R.; Dubey, V.; Kesavan, K. Ocular self-microemulsifying drug delivery system of prednisolone improves therapeutic effectiveness in the treatment of experimental uveitis. Ocul. Immunol. Inflamm. 2019, 27, 303–311. [Google Scholar] [CrossRef]
- Bulbake, U.; Doppalapudi, S.; Kommineni, N.; Khan, W. Liposomal formulations in clinical use: An updated review. Pharmaceutics 2017, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Lajunen, T.; Nurmi, R.; Kontturi, L.; Viitala, L.; Yliperttula, M.; Murtomäki, L.; Urtti, A. Light activated liposomes: Functionality and prospects in ocular drug delivery. J. Control. Release 2016, 244, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Inokuchi, Y.; Hironaka, K.; Fujisawa, T.; Tozuka, Y.; Tsuruma, K.; Shimazawa, M.; Takeuchi, H.; Hara, H. Physicochemical properties affecting retinal drug/coumarin-6 delivery from nanocarrier systems via eyedrop administration. Investig. Ophthalmol. Vis. Sci. 2010, 51, 3162–3170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathod, S.; Deshpande, S. Design and evaluation of liposomal formulation of pilocarpine nitrate. Indian J. Pharm. Sci. 2010, 72, 155. [Google Scholar] [CrossRef] [Green Version]
- Mehanna, M.M.; Elmaradny, H.A.; Samaha, M.W. Mucoadhesive liposomes as ocular delivery system: Physical, microbiological, and in vivo assessment. Drug Dev. Ind. Pharm. 2010, 36, 108–118. [Google Scholar] [CrossRef]
- Li, N.; Zhuang, C.; Wang, M.; Sun, X.; Nie, S.; Pan, W. Liposome coated with low molecular weight chitosan and its potential use in ocular drug delivery. Int. J. Pharm. 2009, 379, 131–138. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, S. Topical use of Coenzyme Q10-loaded liposomes coated with trimethyl chitosan: Tolerance, precorneal retention and anti-cataract effect. Int. J. Pharm. 2009, 372, 66–75. [Google Scholar] [CrossRef]
- Law, S.; Huang, K.; Chiang, C. Acyclovir-containing liposomes for potential ocular delivery: Corneal penetration and absorption. J. Control. Release 2000, 63, 135–140. [Google Scholar] [CrossRef]
- Barber, R.; Shek, P. Tear-induced release of liposome-entrapped agents. Int. J. Pharm. 1990, 60, 219–227. [Google Scholar] [CrossRef]
- Barber, R.F.; Shek, P. Liposomes and tear fluid. I. Release of vesicle-entrapped carboxyfluorescein. Biochim. Biophys. Acta Lipids Lipid Metab. 1986, 879, 157–163. [Google Scholar] [CrossRef]
- Chetoni, P.; Rossi, S.; Burgalassi, S.; Monti, D.; Mariotti, S.; Saettone, M.F. Comparison of liposome-encapsulated acyclovir with acyclovir ointment: Ocular pharmacokinetics in rabbits. J. Ocul. Pharmacol. Ther. 2004, 20, 169–177. [Google Scholar] [CrossRef]
- Shen, Y.; Tu, J. Preparation and ocular pharmacokinetics of ganciclovir liposomes. AAPS J. 2007, 9, E371–E377. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-De la Rosa, A.; Navarro-Partida, J.; Altamirano-Vallejo, J.C.; Hernandez-Gamez, A.G.; Garcia-Banuelos, J.J.; Armendariz-Borunda, J.; Santos, A. Novel triamcinolone acetonide-loaded liposomes topical formulation for the treatment of cystoid macular edema after cataract surgery: A pilot study. J. Ocul. Pharmacol. Ther. 2019, 35, 106–115. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Guan, P.; Wang, T.; Chang, D.; Jiang, T.; Wang, S. Freeze-dried liposomes as potential carriers for ocular administration of cytochrome c against selenite cataract formation. J. Pharm. Pharmacol. 2009, 61, 1171–1178. [Google Scholar] [CrossRef]
- Natarajan, J.V.; Ang, M.; Darwitan, A.; Chattopadhyay, S.; Wong, T.T.; Venkatraman, S.S. Nanomedicine for glaucoma: Liposomes provide sustained release of latanoprost in the eye. Int. J. Nanomed. 2012, 7, 123. [Google Scholar]
- Kaiser, J.M.; Imai, H.; Haakenson, J.K.; Brucklacher, R.M.; Fox, T.E.; Shanmugavelandy, S.S.; Unrath, K.A.; Pedersen, M.M.; Dai, P.; Freeman, W.M. Nanoliposomal minocycline for ocular drug delivery. Nanomed. Nanotechnol. Biol. Med. 2013, 9, 130–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhardwaj, P.; Tripathi, P.; Gupta, R.; Pandey, S. Niosomes: A review on niosomal research in the last decade. J. Drug Deliv. Sci. Technol. 2020, 56, 101581. [Google Scholar] [CrossRef]
- Rajera, R.; Nagpal, K.; Singh, S.K.; Mishra, D.N. Niosomes: A controlled and novel drug delivery system. Biol. Pharm. Bull. 2011, 34, 945–953. [Google Scholar] [CrossRef] [Green Version]
- Gharbavi, M.; Amani, J.; Kheiri-Manjili, H.; Danafar, H.; Sharafi, A. Niosome: A promising nanocarrier for natural drug delivery through blood-brain barrier. Adv. Pharmacol. Sci. 2018, 2018. [Google Scholar] [CrossRef]
- Lalu, L.; Tambe, V.; Pradhan, D.; Nayak, K.; Bagchi, S.; Maheshwari, R.; Kalia, K.; Tekade, R.K. Novel nanosystems for the treatment of ocular inflammation: Current paradigms and future research directions. J. Control. Release 2017, 268, 19–39. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, P.; Patil, A.; Majumdar, S. Recent advances in topical nano drug-delivery systems for the anterior ocular segment. Ther. Deliv. 2018, 9, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Barriga, H.M.; Holme, M.N.; Stevens, M.M. Cubosomes: The next generation of smart lipid nanoparticles? Angew. Chem. Int. Ed. 2019, 58, 2958–2978. [Google Scholar] [CrossRef] [Green Version]
- Abdelkader, H.; Longman, M.R.; Alany, R.G.; Pierscionek, B. Phytosome-hyaluronic acid systems for ocular delivery of L-carnosine. Int. J. Nanomed. 2016, 11, 2815. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharya, S. Phytosomes: The new technology for enhancement of bioavailability of botanicals and nutraceuticals. Int. J. Health Res. 2009, 2, 225–232. [Google Scholar] [CrossRef]
- Sánchez-López, E.; Espina, M.; Doktorovova, S.; Souto, E.; García, M. Lipid nanoparticles (SLN, NLC): Overcoming the anatomical and physiological barriers of the eye—Part II—Ocular drug-loaded lipid nanoparticles. Eur. J. Pharm. Biopharm. 2017, 110, 58–69. [Google Scholar] [CrossRef]
- Meza-Rios, A.; Navarro-Partida, J.; Armendariz-Borunda, J.; Santos, A. Therapies Based on Nanoparticles for Eye Drug Delivery. Ophthalmol. Ther. 2020, 9, 1–14. [Google Scholar] [CrossRef]
- del Pozo-Rodriguez, A.; Delgado, D.; Solinis, M.; Gascon, A.; Pedraz, J. Solid lipid nanoparticles for retinal gene therapy: Transfection and intracellular trafficking in RPE cells. Int. J. Pharm. 2008, 360, 177–183. [Google Scholar] [CrossRef]
- Singh, M.; Guzman-Aranguez, A.; Hussain, A.; Srinivas, C.S.; Kaur, I.P. Solid lipid nanoparticles for ocular delivery of isoniazid: Evaluation, proof of concept and in vivo safety & kinetics. Nanomedicine 2019, 14, 465–491. [Google Scholar] [PubMed]
- Hippalgaonkar, K.; Adelli, G.R.; Hippalgaonkar, K.; Repka, M.A.; Majumdar, S. Indomethacin-loaded solid lipid nanoparticles for ocular delivery: Development, characterization, and in vitro evaluation. J. Ocul. Pharmacol. Ther. 2013, 29, 216–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakkar, S.; Karuppayil, S.M.; Raut, J.S.; Giansanti, F.; Papucci, L.; Schiavone, N.; Kaur, I.P. Lipid-polyethylene glycol based nano-ocular formulation of ketoconazole. Int. J. Pharm. 2015, 495, 276–289. [Google Scholar] [CrossRef] [PubMed]
- Abrishami, M.; Abrishami, M.; Mahmoudi, A.; Mosallaei, N.; Vakili Ahrari Roodi, M.; Malaekeh-Nikouei, B. Solid lipid nanoparticles improve the diclofenac availability in vitreous after intraocular injection. J. Drug Deliv. 2016, 2016, 1368481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- del Pozo-Rodriguez, A.; Pujals, S.; Delgado, D.; Solinís, M.; Gascón, A.; Giralt, E.; Pedraz, J. A proline-rich peptide improves cell transfection of solid lipid nanoparticle-based non-viral vectors. J. Control. Release 2009, 133, 52–59. [Google Scholar] [CrossRef]
- Araújo, J.; Nikolic, S.; Egea, M.A.; Souto, E.B.; Garcia, M.L. Nanostructured lipid carriers for triamcinolone acetonide delivery to the posterior segment of the eye. Colloids Surf. B Biointerfaces 2011, 88, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Nie, S.-F.; Kong, J.; Li, N.; Ju, C.-Y. A controlled-release ocular delivery system for ibuprofen based on nanostructured lipid carriers. Int. J. Pharm. 2008, 363, 177–182. [Google Scholar] [CrossRef]
- Khosa, A.; Reddi, S.; Saha, R.N. Nanostructured lipid carriers for site-specific drug delivery. Biomed. Pharmacother. 2018, 103, 598–613. [Google Scholar] [CrossRef] [PubMed]
- Haider, M.; Abdin, S.M.; Kamal, L.; Orive, G. Nanostructured lipid carriers for delivery of chemotherapeutics: A review. Pharmaceutics 2020, 12, 288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.; Liu, J.; Zhang, Q.; Li, X.; Yu, S.; Yang, X.; Kong, J.; Pan, W. Enhanced cellular uptake and anti-proliferating effect of chitosan hydrochlorides modified genistein loaded NLC on human lens epithelial cells. Int. J. Pharm. 2014, 471, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Luo, Q.; Zhao, J.; Zhang, X.; Pan, W. Nanostructured lipid carrier (NLC) coated with Chitosan Oligosaccharides and its potential use in ocular drug delivery system. Int. J. Pharm. 2011, 403, 185–191. [Google Scholar] [CrossRef]
- Liu, R.; Liu, Z.; Zhang, C.; Zhang, B. Nanostructured lipid carriers as novel ophthalmic delivery system for mangiferin: Improving in vivo ocular bioavailability. J. Pharm. Sci. 2012, 101, 3833–3844. [Google Scholar] [CrossRef]
- Sánchez-López, E.; Espina, M.; Doktorovova, S.; Souto, E.; García, M. Lipid nanoparticles (SLN, NLC): Overcoming the anatomical and physiological barriers of the eye—Part I—Barriers and determining factors in ocular delivery. Eur. J. Pharm. Biopharm. 2017, 110, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Mira, E.; Egea, M.; Garcia, M.; Souto, E. Design and ocular tolerance of flurbiprofen loaded ultrasound-engineered NLC. Colloids Surf. B Biointerfaces 2010, 81, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Hegde, R.R.; Verma, A.; Ghosh, A. Microemulsion: New insights into the ocular drug delivery. Int. Sch. Res. Not. 2013, 2013, 826798. [Google Scholar] [CrossRef] [PubMed]
- Hegde, R.R.; Bhattacharya, S.S.; Verma, A.; Ghosh, A. Physicochemical and pharmacological investigation of water/oil microemulsion of non-selective beta blocker for treatment of glaucoma. Curr. Eye Res. 2014, 39, 155–163. [Google Scholar] [CrossRef]
- Chan, J.; El Maghraby, G.M.; Craig, J.P.; Alany, R.G. Phase transition water-in-oil microemulsions as ocular drug delivery systems: In vitro and in vivo evaluation. Int. J. Pharm. 2007, 328, 65–71. [Google Scholar] [CrossRef]
- Üstündag-Okur, N.; Gökçe, E.H.; Eğrilmez, S.; Özer, Ö.; Ertan, G. Novel ofloxacin-loaded microemulsion formulations for ocular delivery. J. Ocul. Pharmacol. Ther. 2014, 30, 319–332. [Google Scholar] [CrossRef]
- Kalam, M.A.; Alshamsan, A.; Aljuffali, I.A.; Mishra, A.K.; Sultana, Y. Delivery of gatifloxacin using microemulsion as vehicle: Formulation, evaluation, transcorneal permeation and aqueous humor drug determination. Drug Deliv. 2016, 23, 886–897. [Google Scholar] [CrossRef]
- Bharti, S.K.; Kesavan, K. Phase-transition W/O microemulsions for ocular delivery: Evaluation of antibacterial activity in the treatment of bacterial keratitis. Ocul. Immunol. Inflamm. 2017, 25, 463–474. [Google Scholar] [CrossRef]
- Silva-Cunha, A.; da Silva, G.R.; de Castro, W.V.; Fialho, S.L. Evaluation of the pharmacokinetics and ocular tolerance of a microemulsion containing tacrolimus. J. Ocul. Pharmacol. Ther. 2014, 30, 59–65. [Google Scholar] [CrossRef]
- Ismail, A.; Nasr, M.; Sammour, O. Nanoemulsion as a feasible and biocompatible carrier for ocular delivery of travoprost: Improved pharmacokinetic/pharmacodynamic properties. Int. J. Pharm. 2020, 583, 119402. [Google Scholar] [CrossRef]
- Morsi, N.; Ibrahim, M.; Refai, H.; El Sorogy, H. Nanoemulsion-based electrolyte triggered in situ gel for ocular delivery of acetazolamide. Eur. J. Pharm. Sci. 2017, 104, 302–314. [Google Scholar] [CrossRef]
- Kassaee, S.N.; Mahboobian, M.M. Besifloxacin-loaded ocular nanoemulsions: Design, formulation and efficacy evaluation. Drug Deliv. Transl. Res. 2021, 1–11. [Google Scholar] [CrossRef]
- Oliverio, G.W.; Spinella, R.; Postorino, E.I.; Inferrera, L.; Aragona, E.; Aragona, P. Safety and Tolerability of an Eye Drop Based on 0.6% Povidone–Iodine Nanoemulsion in Dry Eye Patients. J. Ocul. Pharmacol. Ther. 2021, 37, 90–91. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, Z.; Tao, C.; Lin, X.; Zhang, M.; Zeng, L.; Chen, X.; Song, H. Cationic nanoemulsions with prolonged retention time as promising carriers for ophthalmic delivery of tacrolimus. Eur. J. Pharm. Sci. 2020, 144, 105229. [Google Scholar] [CrossRef]
- Shimazawa, M.; Inoue, Y.; Masuda, T.; Onodera, R.; Tahara, K.; Shimizu, Y.; Mibe, Y.; Tsuruma, K.; Takeuchi, H.; Hara, H. Topical diclofenac-loaded liposomes ameliorate laser-induced choroidal neovascularization in mice and non-human primates. Curr. Neurovascul. Res. 2017, 14, 46–52. [Google Scholar] [CrossRef] [PubMed]
- El-Nabarawi, M.A.; Abd El Rehem, R.T.; Teaima, M.; Abary, M.; El-Mofty, H.M.; Khafagy, M.M.; Lotfy, N.M.; Salah, M. Natamycin niosomes as a promising ocular nanosized delivery system with ketorolac tromethamine for dual effects for treatment of candida rabbit keratitis; in vitro/in vivo and histopathological studies. Drug Dev. Ind. Pharm. 2019, 45, 922–936. [Google Scholar] [CrossRef] [PubMed]
- Kaur, I.P.; Aggarwal, D.; Singh, H.; Kakkar, S. Improved ocular absorption kinetics of timolol maleate loaded into a bioadhesive niosomal delivery system. Graefe’s Arch. Clin. Exp. Ophthalmol. 2010, 248, 1467–1472. [Google Scholar] [CrossRef] [PubMed]
- Khalil, R.M.; Abdelbary, G.A.; Basha, M.; Awad, G.E.; El-Hashemy, H.A. Enhancement of lomefloxacin Hcl ocular efficacy via niosomal encapsulation: In vitro characterization and in vivo evaluation. J. Liposome Res. 2017, 27, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Gaballa, S.A.; El Garhy, O.H.; Moharram, H.; Abdelkader, H. Preparation and evaluation of cubosomes/cubosomal gels for ocular delivery of beclomethasone dipropionate for management of uveitis. Pharm. Res. 2020, 37, 1–23. [Google Scholar] [CrossRef]
- Huang, J.; Peng, T.; Li, Y.; Zhan, Z.; Zeng, Y.; Huang, Y.; Pan, X.; Wu, C.-Y.; Wu, C. Ocular cubosome drug delivery system for timolol maleate: Preparation, characterization, cytotoxicity, ex vivo, and in vivo evaluation. AAPS Pharmscitech 2017, 18, 2919–2926. [Google Scholar] [CrossRef]
- Nasr, M.; Teiama, M.; Ismail, A.; Ebada, A.; Saber, S. In vitro and in vivo evaluation of cubosomal nanoparticles as an ocular delivery system for fluconazole in treatment of keratomycosis. Drug Deliv. Transl. Res. 2020, 10, 1841–1852. [Google Scholar] [CrossRef] [PubMed]
- Khames, A.; Khaleel, M.A.; El-Badawy, M.F.; El-Nezhawy, A.O. Natamycin solid lipid nanoparticles–sustained ocular delivery system of higher corneal penetration against deep fungal keratitis: Preparation and optimization. Int. J. Nanomed. 2019, 14, 2515. [Google Scholar] [CrossRef] [Green Version]
- Cavalli, R.; Gasco, M.R.; Chetoni, P.; Burgalassi, S.; Saettone, M.F. Solid lipid nanoparticles (SLN) as ocular delivery system for tobramycin. Int. J. Pharm. 2002, 238, 241–245. [Google Scholar] [CrossRef]
- Tatke, A.; Dudhipala, N.; Janga, K.Y.; Balguri, S.P.; Avula, B.; Jablonski, M.M.; Majumdar, S. In situ gel of triamcinolone acetonide-loaded solid lipid nanoparticles for improved topical ocular delivery: Tear kinetics and ocular disposition studies. Nanomaterials 2019, 9, 33. [Google Scholar] [CrossRef] [Green Version]
- Lakhani, P.; Patil, A.; Taskar, P.; Ashour, E.; Majumdar, S. Curcumin-loaded Nanostructured Lipid Carriers for ocular drug delivery: Design optimization and characterization. J. Drug Deliv. Sci. Technol. 2018, 47, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Puglia, C.; Santonocito, D.; Ostacolo, C.; Maria Sommella, E.; Campiglia, P.; Carbone, C.; Drago, F.; Pignatello, R.; Bucolo, C. Ocular formulation based on palmitoylethanolamide-loaded nanostructured lipid carriers: Technological and pharmacological profile. Nanomaterials 2020, 10, 287. [Google Scholar] [CrossRef] [Green Version]
- Lakhani, P.; Patil, A.; Wu, K.-W.; Sweeney, C.; Tripathi, S.; Avula, B.; Taskar, P.; Khan, S.; Majumdar, S. Optimization, stabilization, and characterization of amphotericin B loaded nanostructured lipid carriers for ocular drug delivery. Int. J. Pharm. 2019, 572, 118771. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Segment of the Eye | Ocular Drug Barriers | Main Functions | |
|---|---|---|---|
| Anterior | Static | Cornea | Allows passive transport of hydrophobic drugs and blocks transport of hydrophilic drugs. |
| Conjunctiva | Formation of tear film, lipophilic affinity to drugs due to its paracellular spaces. | ||
| Blood Aqueous Barrier | Limitation of ion and small solute diffusion and hydrophilic drugs. Regulation of aqueous humor secretion through ion transporters and gap junctions, connexin 43. | ||
| Efflux pumps (ABC proteins) | Enhance or restrict transportation of substrates and drug bioavailability, including both hydrophilic and hydrophobic. | ||
| Dynamic | Tear film, turnover, and drainage | Mucous layer creates a hydrophilic gel layer clearing pathogens and restricting drug delivery, especially hydrophobic drugs. Production and flow of lacrimal fluid avoids the accumulation of drugs. | |
| Conjunctival lymph and blood flow | Maintain metabolic function and immune protection. | ||
| Aqueous humor | Protects avascular structures of the anterior chamber and provides nutrition to maintain ocular homeostasis. Easy drug distribution pathway for the anterior segment. | ||
| Choroidal lymph and blood circulation | Responsible for 85% of the eye’s perfusion and helps in drug clearance by decreasing the concentration of hydrophilic drugs. | ||
| Posterior | Static | Sclera | Permeation dependent on chemical or structural properties. Allows a more rapidly hydrophilic permeation than hydrophobic. |
| Bruch’s membrane | Helps in the prevention of hydrophilic compounds permeation. | ||
| Blood Retinal Barrier | Regulates the passage of solutes to the subretinal space. Presents with hydrophilic permeation. | ||
| Efflux pumps | Enhance or restrict transportation of substrates and drug bioavailability, including both hydrophilic and hydrophobic. | ||
| Dynamic | Choroidal lymph and blood circulation | Responsible for 85% of the eye’s perfusion and helps in drug clearance by decreasing the concentration of hydrophilic drugs. | |
| Anterior and Posterior | Metabolic | Cytochrome P450 | Metabolize substances by conjugation or oxidation to avoid drug accumulation. Or convert prodrugs into active drugs modifying the solubility, bioavailability, and concentration. |
| Enzymes: peptidases, esterases | |||
| Segment of the Eye | Disease | Lipid Nanocarrier | Development Stage | Description | Main Findings | Reference |
|---|---|---|---|---|---|---|
| Anterior | Uveitis | Emulsion-based | Preclinical study: rabbit | Microemulsions containing dexamethasone coated with chitosan or microemulsion with prednisolone administered topically. | Increased residence time in the precorneal area, better bioavailability and enhanced anti-inflammatory effect. | [103,145] |
| Glaucoma | Emulsion-based | Preclinical study: rabbit | Microemulsions with timolol maleate or pilocarpine hydrochloride administered topically. | Better bioavailability, increased retention, and maintained or increased drug efficacy (reduction of IOP). | [87,146,147] | |
| Bacterial Keratitis | Emulsion-based | Preclinical study: rabbit | Microemulsions containing ofloxacin, gatifloxacin or moxifloxacin administered topically. | Sustained release, increased ocular concentration and therapeutic efficacy. | [87,148,149,150] | |
| Inflammatory diseases | Emulsion-based | Preclinical study: rabbit | Microemulsions with tacrolimus topically administered. | Enhanced penetration and concentration, sustained release. | [87,151] | |
| Anterior | Glaucoma | Emulsion-based | Preclinical study: rabbit | Nanoemulsion with dorzolamide hydrochloride, y travoprost, or acetazolamide after topical administration. | Increased therapeutic effect with a rapid and sustained action, enhanced absorption. | [16,152,153] |
| Bacterial Conjunctivitis | Emulsion-based | Preclinical study: rabbit | Nanoemulsion carrying moxifloxacin or besifloxacin administered topically. | Increased concentration and bioavailability, better efficacy and decreased dose application. | [91,154] | |
| Dry eye | Emulsion-based | Clinical trial | Nanoemulsion with Povidone-iodine topically administered. | Better therapeutic efficacy and improvement of symptoms. | [155] | |
| Inflammatory anterior ocular diseases | Emulsion-based | Preclinical study: rabbit | Nanoemulsion with tacrolimus for topical treatment. | Increased residence precorneal time and better bioavailability. | [156] | |
| Anterior | Keratitis | Vesicle-based | Preclinical study: rabbit | Liposomes containing acyclovir, ganciclovir, tobramycin or fluconazole administered topically. | Increased bioavailability half-life of the drug and therapeutic efficacy, and better permeation. | [98] |
| Glaucoma | Vesicle-based | Preclinical study: rabbit | Liposome with pilocarpine, latanoprost or acetazolamide administered topically. | Better entrapment, increased and sustained therapeutic effect and duration of action. | [98] | |
| Posterior | Refractory macular edema | Vesicle-based | Preclinical study: rabbit Phase I clinical trial | Liposome carrying triamcinolone acetonide topically administered. | Improved permeation to the posterior segment (vitreous and retina) and therapeutic effect. | [10,11] |
| Age-related macular degeneration | Vesicle-based | Preclinical study: rabbit and rat | Liposome with Bevacizumab administed topically. | Enhanced delivery and increased concentration (vitreous and retina). | [51] | |
| Choroidal neovascularization secondary to laser use | Vesicle-based | Preclinical study: mice | Liposome with diclofenac administered topically. | Enhanced permeability to posterior segment and therapeutic efficacy. | [157] | |
| Anterior | Fungal keratitis | Vesicle-based | Preclinical study: rabbit | Niosome with natamycin plus ketorolac tromethamine administered topically. | Increased corneal infiltration and a higher level in the hypopyon. | [158] |
| Glaucoma | Vesicle-based | Preclinical study: | Niosome containing timolol maleate topically administered. | Increased and maintained concentration in the aqueous humor. | [159] | |
| Conjunctivitis | Vesicle-based | Preclinical study: rabbits | Niosome with lomefloxacin HCl administered topically. | Improvement in penetration and therapeutic efficacy. | [160] | |
| Anterior | Uveitis | Vesicle- based | Preclinical study: rabbit | Cubosome containing beclomethasone dipropionate administered topically. | Increased permeation through the corneal tissue with a better anti-inflammatory effect and tolerability. | [161] |
| Glaucoma | Vesicle-based | Preclinical study: rabbit | Cubosomes with timolol maleate administered topically | Increased residence time, penetration and therapeutic effect. | [162] | |
| Keratomycosis | Vesicle based | Preclinical study: mice | Cubosome containing fluconazole topically administered. | Enhanced therapeutic effect. | [163] | |
| Cataracts | Vesicle-based | Ex vivo study: pig | Phytosome carrying L-carnosine. | Longer residence time and better therapeutic effect. | [126] | |
| Anterior | Fungal keratitis | Particulate system | Ex vivo study: goat | SLN with Natamycin. | Sustained release with better permeation and increased therapeutic effect. | [164] |
| Tuberculosis | Particulate system | Ex vivo: pig | SLN with isoniazid. | Improved corneal permeation. | [131] | |
| Keratitis | Particulate system | Preclinical study: rabbit | SLN containing tobramycin administered topically. | Increased bioavailability and drug retention. | [165] | |
| Anterior and Posterior | Posterior ocular diseases (Diabetic macular edema, inflammation, uveitis) | Particulate system | Preclinical study: rabbit | SLN with triamcinolone acetonide administered topically. | Increased corneal permeation and residence time, higher concentration on both, aqueous and vitreous humor (sustained release). | [166] |
| Anterior | Anterior diseases | Particulate system | Ex vivo study: rabbit | NLC loaded with curcumin. | Enhanced permeability. | [167] |
| Posterior | Diabetic retinopathy | Particulate system | Preclinical study: mice | NLC with palmitoylethanolamide administered topically. | Increased retinal concentration and therapeutic efficacy. | [168] |
| Anterior and Posterior | Fungal infections (keratomycosis) | Particulate system | Preclinical study: rabbit | NLC loaded with amphotericin B administered topically. | Increased therapeutic effect and higher bioavailability in anterior and posterior ocular tissues. | [169] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro-Partida, J.; Castro-Castaneda, C.R.; Santa Cruz-Pavlovich, F.J.; Aceves-Franco, L.A.; Guy, T.O.; Santos, A. Lipid-Based Nanocarriers as Topical Drug Delivery Systems for Intraocular Diseases. Pharmaceutics 2021, 13, 678. https://doi.org/10.3390/pharmaceutics13050678
Navarro-Partida J, Castro-Castaneda CR, Santa Cruz-Pavlovich FJ, Aceves-Franco LA, Guy TO, Santos A. Lipid-Based Nanocarriers as Topical Drug Delivery Systems for Intraocular Diseases. Pharmaceutics. 2021; 13(5):678. https://doi.org/10.3390/pharmaceutics13050678
Chicago/Turabian StyleNavarro-Partida, Jose, Carlos Rodrigo Castro-Castaneda, Francisco J. Santa Cruz-Pavlovich, Luis Abraham Aceves-Franco, Tomer Ori Guy, and Arturo Santos. 2021. "Lipid-Based Nanocarriers as Topical Drug Delivery Systems for Intraocular Diseases" Pharmaceutics 13, no. 5: 678. https://doi.org/10.3390/pharmaceutics13050678