
Design of Wearable Breathing Sound Monitoring System for Real-Time Wheeze Detection




Abstract
:1. Introduction
2. Methods and Materials
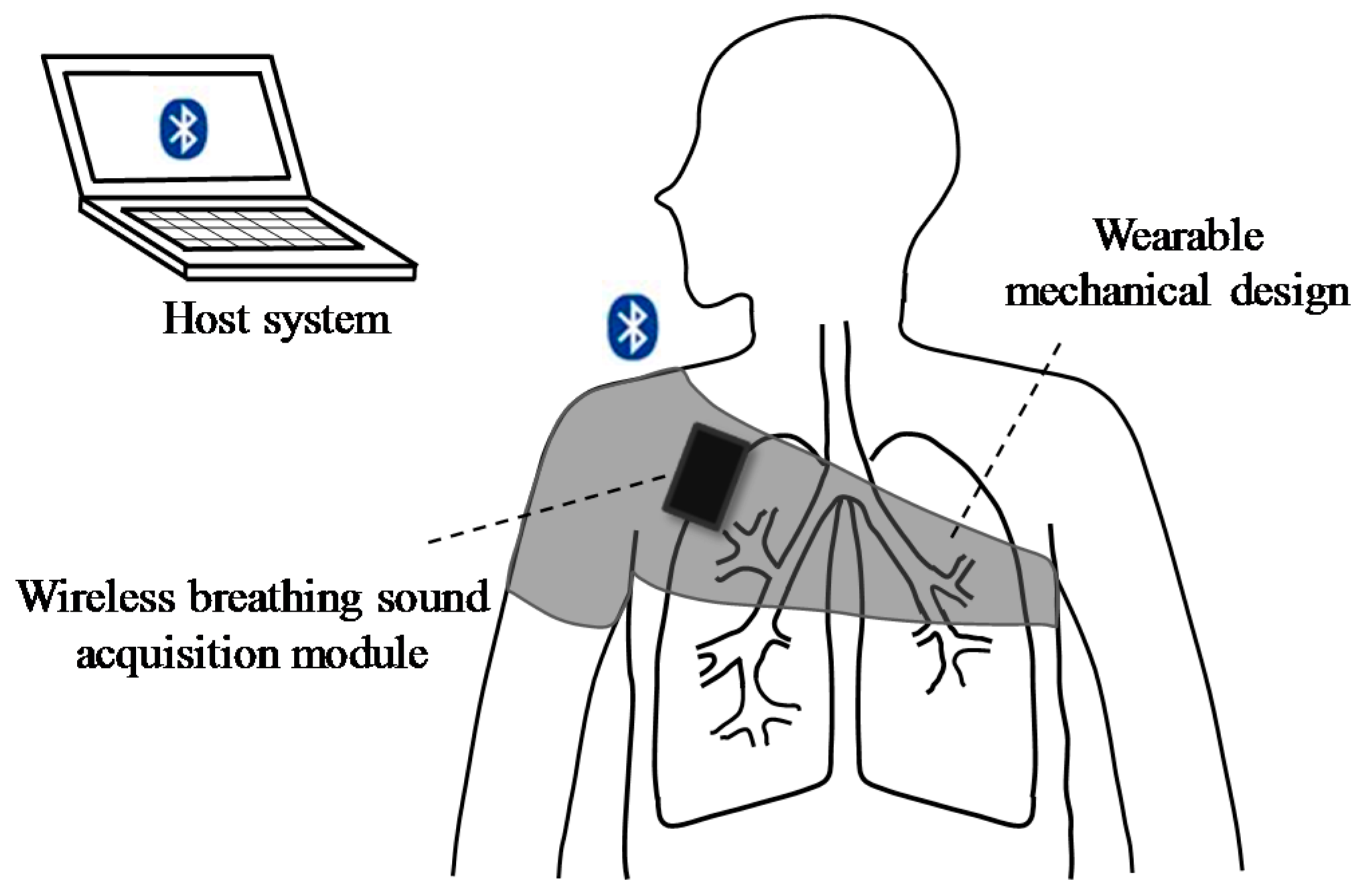
2.1. System Hardware Design and Implementation
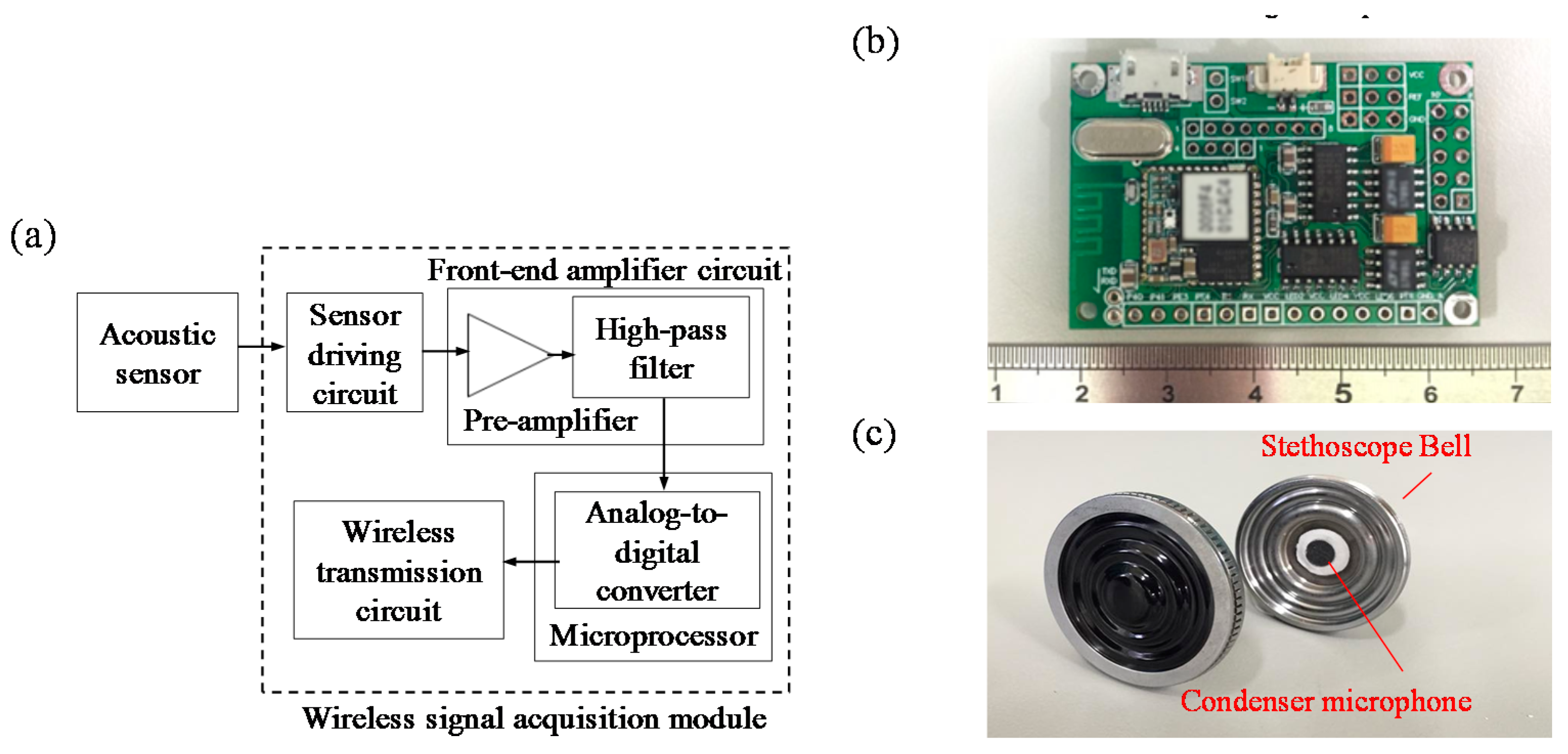
2.1.1. Wireless Breathing Sound Acquisition Module
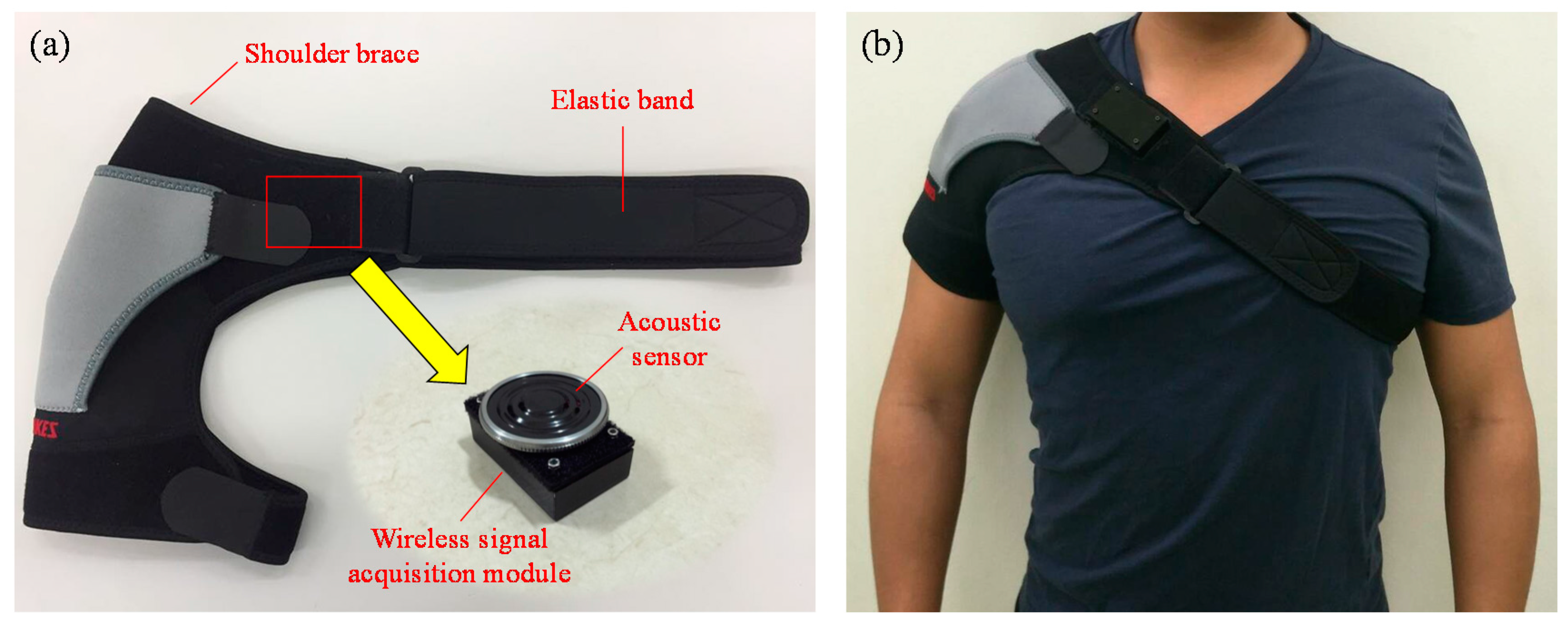
2.1.2. Wearable Mechanical Design
2.1.3. Host System
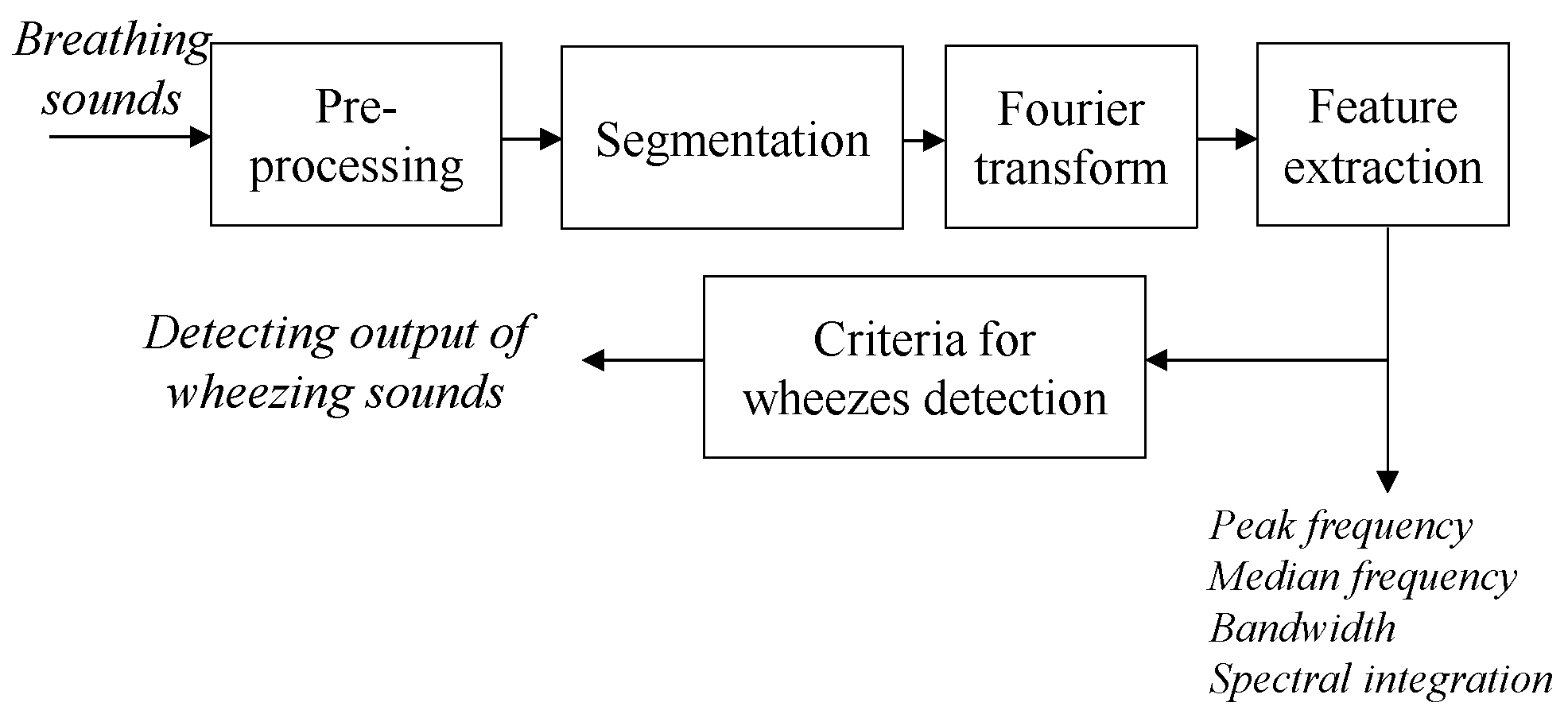
2.2. Breathing Sound Analysis Algorithm
- (i)
- Score1 = –230.54489 + 402.72499 × + 500.32269 × + 677.28994 × .Score2 = –266.87228 + 418.88239 × + 554.36286 × + 699.35894 × .If Score1 < Score 2, then this segment will be recognized as an abnormal breathing sound.
- (ii)
- If the duration of abnormal breathing sound > 250 ms [22].
2.3. Experimental Design
3. Results
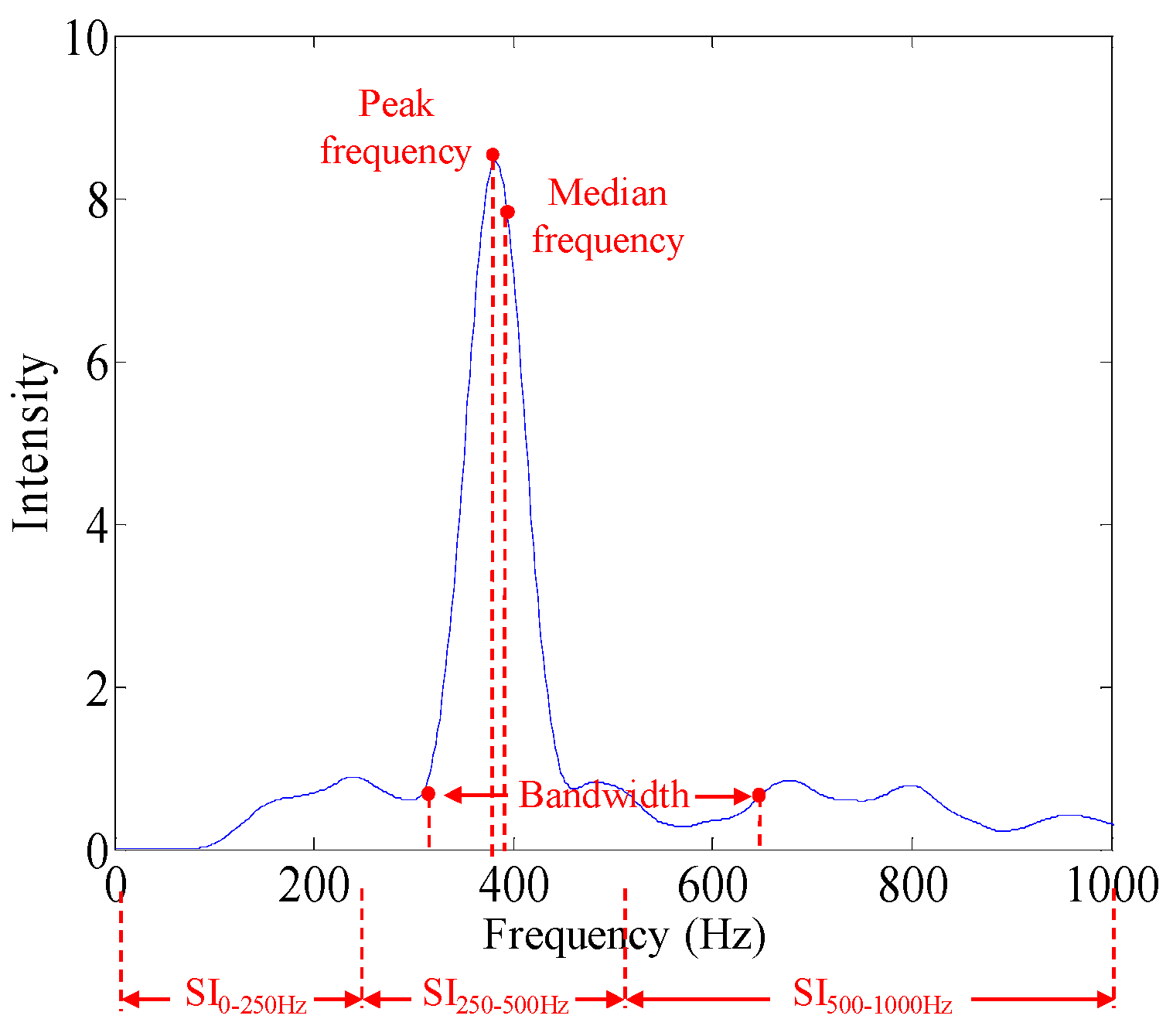
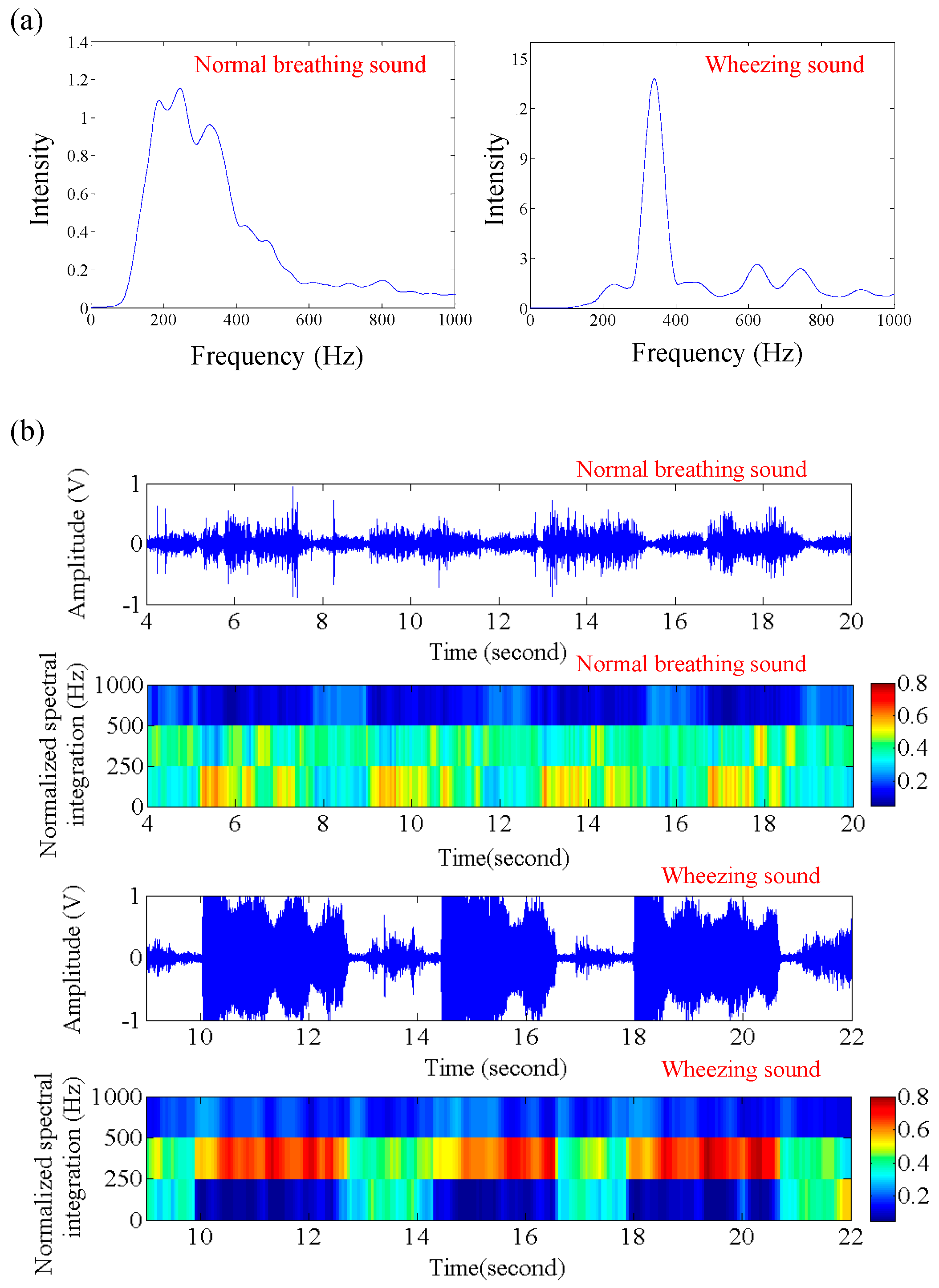
3.1. Feature Patterns of Wheezing and Healthy Breathing Sounds
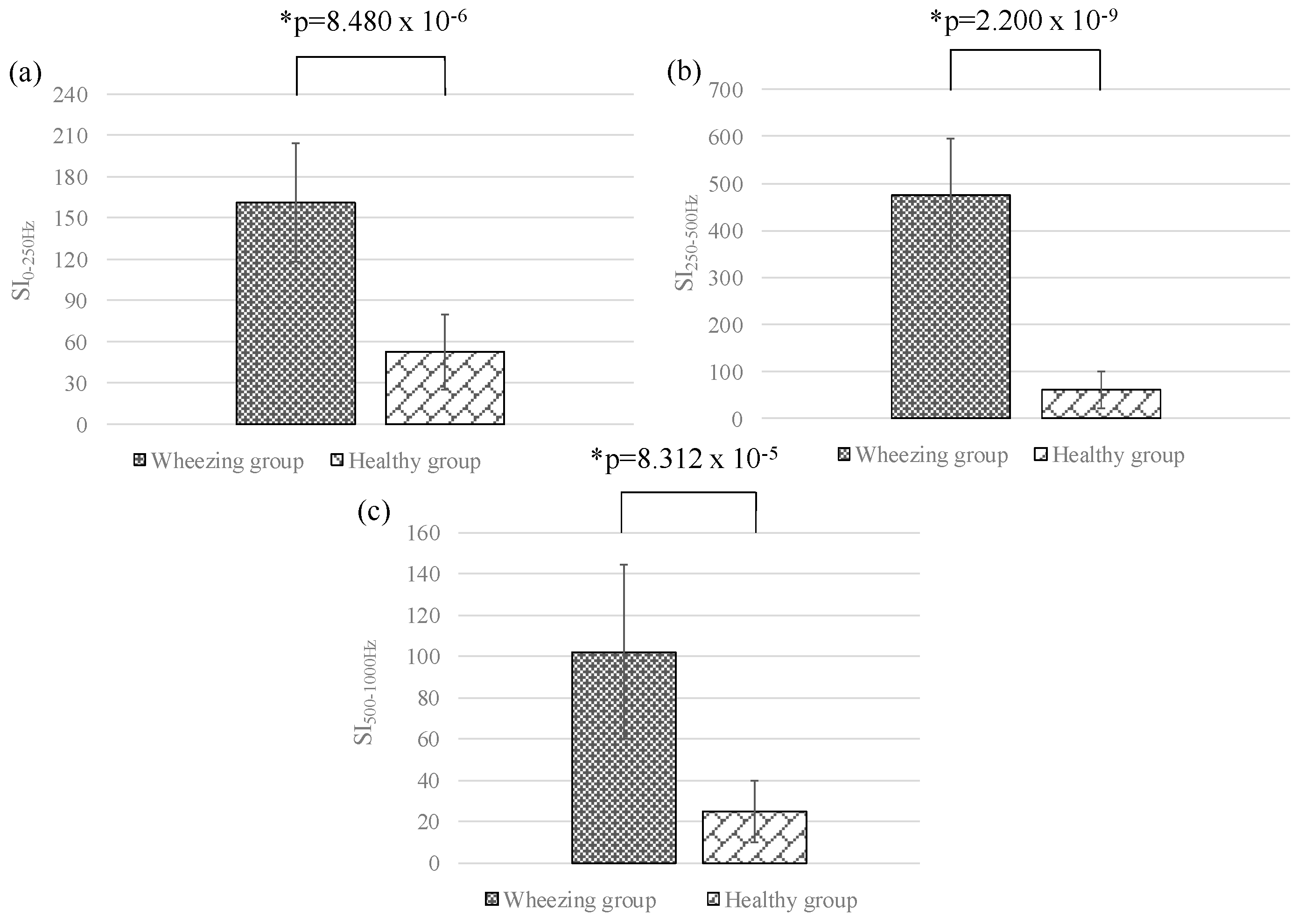
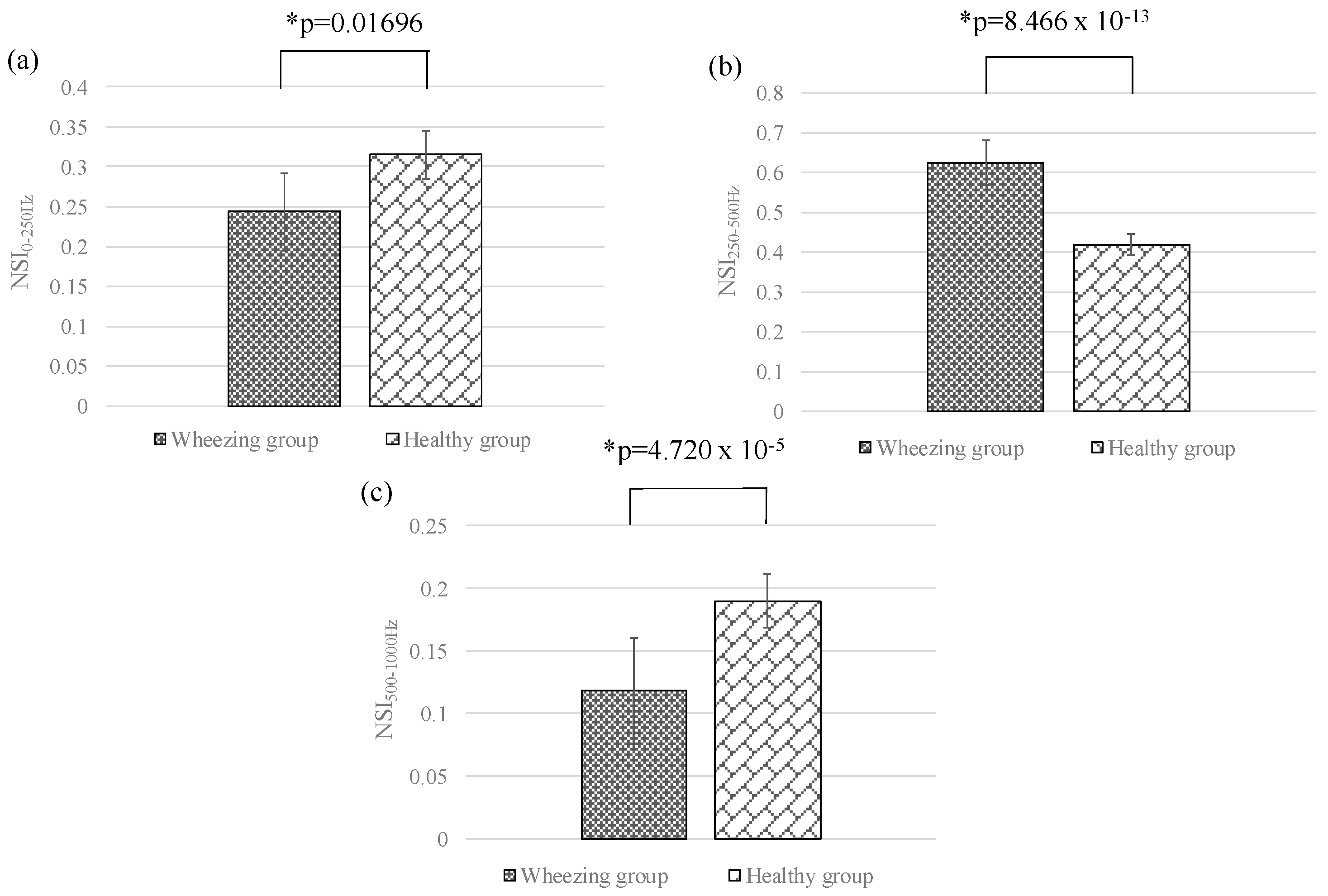
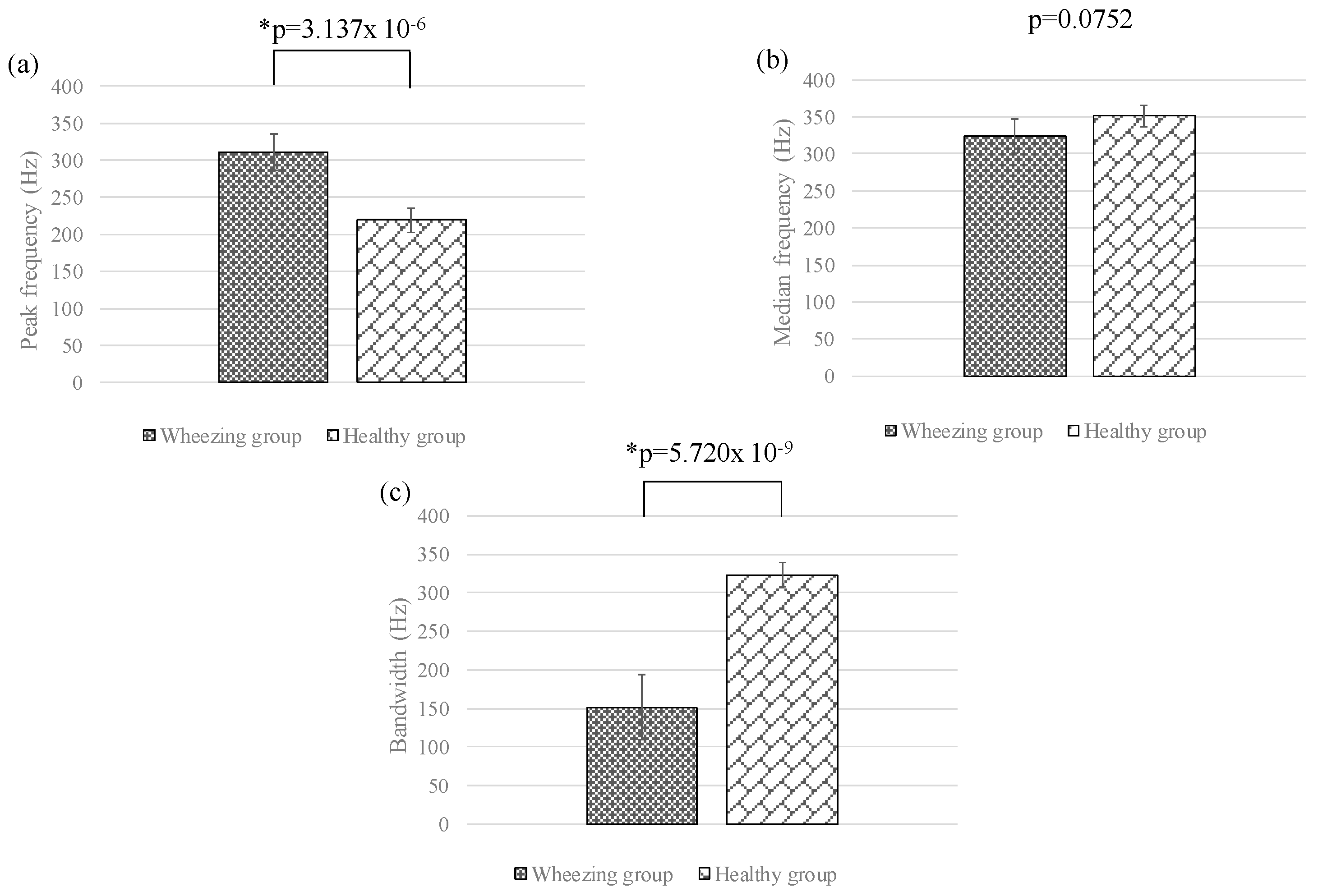
3.2. Feature Difference between Wheezing and Healthy Breathing Sounds
3.3. Performance of Breathing Sound Analysis Algorithm
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Moretz, C.; Zhou, Y.; Dhamane, A.D.; Burslem, K.; Saverno, K.; Jain, G.; Devercelli, G.; Kaila, S.; Ellis, J.J.; Hernandez, G.; et al. Development and validation of a predictive model to identify individuals likely to have undiagnosed chronic obstructive pulmonary disease using an administrative claims database. J. Manag. Care Spec. Pharm. 2015, 21, 1149–1159. [Google Scholar] [CrossRef] [PubMed]
- Morillo, D.S.; Moreno, S.A.; Granero, M.A.F.; Jimenez, A.L. Computerized analysis of respiratory sounds during COPD exacerbations. Comput. Biol. Med. 2013, 43, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Nagasaka, Y. Lung sounds in bronchial asthma. Allergol. Int. 2012, 61, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Burrows, B.; Huang, N.; Hughes, R.; Johnston, R.; Kilburn, K.; Kuhn, C.; Miller, W.; Mitchell, M.; Snider, G. Pulmonary Terms and Symbols. Chest 1975, 67, 583–593. [Google Scholar] [CrossRef]
- Taplidou, S.A.; Hadjileontiadis, L.J. Wheeze detection based on time frequency analysis of breath sounds. Comput. Biol. Med. 2007, 37, 1073–1083. [Google Scholar] [CrossRef] [PubMed]
- Shaharum, S.M.; Sundaraj, K.; Palaniappan, R. A survey on automated wheeze detection systems for asthmatic patients. Bosn. J. Basic. Med. Sci. 2012, 12, 249–255. [Google Scholar] [PubMed]
- Jacome, C.; Marques, A. Computerized Respiratory Sounds in Patients with COPD: A Systematic Review. COPD 2015, 12, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Gurung, A.; Scrafford, C.G.; Tielsch, J.M.; Levine, O.S.; Checkley, W. Computerized lung sound analysis as diagnostic aid for the detection of abnormal lung sounds: A systematic review and meta-analysis. Respir. Med. 2011, 105, 1396–1403. [Google Scholar] [CrossRef] [PubMed]
- Homs-Cobera, A.; Fiz, J.A.; Morera, J.; Jane, R. Time-frequency detection and analysis of wheezes during forced exhalation. IEEE Trans. Biomed. Eng. 2004, 51, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Mineshita, M.; Matsuoka, S.; Miyazawa, T. Effects of bronchodilators on regional lung sound distribution in patients with chronic obstructive pulmonary disease. Respiration 2013, 87, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.P.; Parrillo, J.E.; Kushnir, A.; Rossi, M.; Kushnir, I. Dynamic visualization of lung sounds with a vibration response device: A case series. Respiration 2008, 75, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Maher, T.M.; Gat, M.; Allen, D.; Devaraj, A.; Wells, A.U.; Geddes, D.M. Reproducibility of dynamically represented acoustic lung images from healthy individuals. Thorax 2008, 63, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Anantham, D.; Herth, F.J.; Majid, A.; Michaud, G.; Ernst, A. Vibration response imaging in the detection of pleural effusions: A feasibility study. Respiration 2009, 77, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Guntupalli, K.K.; Alapat, P.M.; Bandi, V.D.; Kushnir, I. Validation of automatic wheeze detection in patients with obstructed airways and in healthy subjects. J. Asthma 2008, 45, 903–907. [Google Scholar] [CrossRef] [PubMed]
- Schreur, H.J.; Vanderschoot, J.; Zwinderman, A.H.; Dijkman, J.H.; Sterk, P.J. Abnormal lung sounds in patients with asthma during episodes with normal lung function. Chest 1994, 106, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Kiyokawa, H.; Yonemaru, M.; Horie, S.; Kasuga, I.; Ichinose, Y.; Toyama, K. Detection of nocturnal wheezing in bronchial asthma using intermittent sleep tracheal sounds recording. Respirology 1999, 4, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Gross, V.; Fachiger, P.; Penzel, T.; Koehler, U.; Wichert, P.V.; Vogelmeier, C. Detection of bronchial breathing caused by pneumonia. Biomed. Tech. 2002, 47, 146–150. [Google Scholar] [CrossRef]
- Icer, S.; Gengec, S. Classification and analysis of non-stationary characteristics of crackle and rhonchus lung adventitious sounds. Digit. Signal Process. 2014, 28, 18–27. [Google Scholar] [CrossRef]
- Sello, S.; Strambi, S.; Michelle, G.D.; Ambrosino, N. Respiratory sound analysis in healthy and pathological subjects: A wavelet approach. Biomed. Signal Process. Control 2008, 3, 181–191. [Google Scholar] [CrossRef]
- Riella, R.J.; Nohama, P.; Maia, J.M. Method for automatic detection of wheezing in lung sounds. Braz. J. Med. Biol. Res. 2009, 42, 674–684. [Google Scholar] [CrossRef] [PubMed]
- Charbonneau, G.; Ademovic, E.; Cheetham, B.M.G.; Malmberg, L.P.; Vanderschoot, J.; Sovijarvi, A.R.A. Basic techniques for respiratory sound analysis. Eur. Respir. Rev. 2000, 10, 625–635. [Google Scholar]
- Sovijarvi, A.R.A.; Vanderschoot, J.; Malmerg, L.P.; Righini, G.; Stoneman, S.A.T. Definition of terms for applications of respiratory sounds. Eur. Respir. Rev. 2000, 10, 597–610. [Google Scholar]
- Felton, T.R.; Pasterkamp, H.; Tal, A.; Chernick, V. Automated spectral characterization of wheezing in asthmatic children. IEEE Trans. Biomed. Eng. 1985, 32, 50–55. [Google Scholar]
- Sovijarvi, A.R.A.; Malmberg, L.P.; Charbonneau, G.; Vanderschoot, J.; Dalmasso, F.; Sacco, C.; Rossi, M.; Earis, J.E. Characteristics of breath sounds and adventitious respiratory sounds. Eur. Respir. Rev. 2000, 10, 591–596. [Google Scholar]
- Wodicka, G.R.; Stevens, K.N.; Golub, H.L.; Cravalho, E.G.; Shannon, D.C. A model of acoustic transmission in the respiratory system. IEEE Trans. Biomed. Eng. 1989, 36, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Bahoura, M. Pattern recognition methods applied to respiratory sounds classification into normal and wheeze classes. Comput. Biol. Med. 2009, 39, 824–843. [Google Scholar] [CrossRef] [PubMed]
- Kraman, S.S. The forced expiratory wheeze. Its site of origin and possible association with lung compliance. Respiration 1983, 44, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Gavriely, N.; Kelly, K.B.; Grotberg, J.B.; Loring, S.H. Forced expiratory wheezes are a manifestation of airflow limitation. J. Appl. Physiol. 1987, 62, 2398–2403. [Google Scholar] [PubMed]
- Gavriely, N.; Kelly, K.B.; Grotberg, J.B.; Loring, S.H. Critical pressure required for generation of forced expiratory wheezes. J. Appl. Physiol. 1989, 66, 1136–1142. [Google Scholar] [PubMed]
- Beck, R.; Gavriely, N. The reproducibility of forced expiratory wheezes. Am. Rev. Respir. Dis. 1990, 141, 1418–1422. [Google Scholar] [CrossRef] [PubMed]
- Fiz, J.A.; Jane, R.; Salvatella, D.; Izquierdo, J.; Lores, L.; Caminal, P.; Morera, J. Analysis of tracheal sounds during forced exhalation in asthma patients and normal subjects. Chest 1999, 116, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Fiz, J.A.; Jane, R.; Homs, A.; Izquierdo, J.; Garcia, M.A.; Morera, J. Detection of wheezing during maximal forced exhalation in patients with obstructed airways. Chest 2002, 122, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.; Aitken, S.; Carter, R.; Macleod, J.E.S.; Moran, F. Variation of breath sound and airway caliber induced by histamine challenge. Am. Rev. Respir. Dis. 1990, 141, 1147–1150. [Google Scholar] [CrossRef] [PubMed]
- Schreur, H.J.; Vanderschoot, J.; Zwinderman, A.H.; Dijkman, J.H.; Sterk, P.J. The effect of methacholine-induced acute airway narrowing on lung sounds in normal and asthmatic subjects. Eur. Respir. J. 1995, 8, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Malmberg, L.P.; Sorva, R.; Sovijarvi, A.R.A. Frequency distribution of breath sounds as an indicator of bronchoconstriction during histamine challenge test in asthmatic children. Pediatr. Pulmonol. 1994, 18, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Malmberg, L.P.; Sovijarvi, A.R.A.; Paajanen, E.; Piirila, P.; Haahtela, T.; Katila, T. Changes in frequency spectra of breath sounds during histamine challenge test in adult asthmatics and healthy control subjects. Chest 1994, 105, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Malmberg, L.P.; Pesu, L.; Sovijarvi, A.R.A. Significant differences in flow standardized breath sound spectra in patients with chronic obstructive pulmonary disease, stable asthma, and healthy lungs. Thorax 1995, 50, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Uwaoma, C.; Mansingh, G. Detection and classification of abnormal respiratory sounds on a resource-constraint mobile device. Int. J. Appl. Inform. Syst. 2014, 7, 35–40. [Google Scholar] [CrossRef]
- Jin, F.; Krishnan, S.S.; Sattar, F. Adventitious sounds identification and extraction using temporal-spectral dominance-based features. IEEE Trans. Biomed. Eng. 2011, 58, 3078–3087. [Google Scholar] [PubMed]
- Lin, B.S.; Wu, H.D.; Chen, S.J. Automatic wheezing detection based on signal processing of spectrogram and back-propagation neural network. J. Healthc. Eng. 2015, 6, 649–672. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.S.; Lin, B.S. Automatic Wheezing Detection Using Speech Recognition Technique. J. Med. Biol. Eng. 2016, 36, 545–554. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wheezing Sound Group | Normal Breathing Sound Group | p-Value | |
|---|---|---|---|
| Peak frequency (Hz) | 310.52 ± 40.94 | 219.13 ± 49.79 | * 3.137 × 10−6 |
| Median frequency (Hz) | 323.52 ± 36.70 | 350.88 ± 59.34 | 0.0752 |
| Bandwidth (Hz) | 151.47 ± 48.43 | 323.44 ± 68.85 | * 5.720 × 10−9 |
| SI0–250Hz | 161.12 ± 64.64 | 52.42 ± 55.045 | * 8.480 × 10−6 |
| SI250–500Hz | 475.38 ± 215.21 | 60.66 ± 50.43 | * 2.200 × 10−9 |
| SI500–1000Hz | 101.97 ± 75.31 | 24.92 ± 18.65 | * 8.312 × 10−5 |
| NSI0–250Hz | 0.243 ± 0.091 | 0.315 ± 0.088 | * 0.01696 |
| NSI250–500Hz | 0.623 ± 0.071 | 0.417 ± 0.028 | * 8.466 × 10−13 |
| NSI500–1000Hz | 0.118 ± 0.042 | 0.190 ± 0.046 | * 4.720 × 10−5 |
| Duration of wheezing sounds (milliseconds) | 736.86 ± 311.40 | - | - |
| Wheezing Sounds Events Detected by Proposed Algorithm | ||||
|---|---|---|---|---|
| + | – | Total | ||
| Real breathing sound event | + | 496 (TP) | 46 (FN) | 542 |
| – | 0 (FP) | 410 (TN) | 410 | |
| Total | 496 | 456 | 952 | |
| R. J. Riella et al. [20] | F. Jin et al. [39] | C. Uwaoma et al. [38] | S. Içer et al. [18] | B. S. Lin et al. [40] | B. S. Lin et al. [41] | Proposed System | |
|---|---|---|---|---|---|---|---|
| Breathing sounds | Wheezing sounds | Wheezing sounds | Wheezing and crackle sounds | Rhonchus and crackles sounds | Wheezing sounds | Wheezing sounds | Wheezing sounds |
| Sensing technique | – | Electrical condenser microphone | Smart-phone | Electronic stethoscope | Electrical condenser microphone | Electrical condenser microphone | Electrical condenser microphone |
| Measurement Location | – | Anterior chest | – | Six zones on posterior chest | Trachea | Trachea | Anterior chest |
| Feature extraction technique | Spectral projection, artificial neural network | Time-frequency decomposition, k-nearest neighbor | Time-frequency threshold dependent algorithm | PSD based on welch method, support vector machine | Order truncate average, back-propagation neural network | Mel frequency cepstral coefficient, Gaussian mixture model | Normalized spectral integration |
| Computational complexity | High | High | Low | Medium | High | Medium | Low |
| Wearable device | – | No | No | No | No | No | Yes |
| Wireless transmission | No | No | No | No | No | No | Yes |
| Applications | Wheeze detection | Wheeze detection | Wheeze detection | Analysis of abnormal breathing sound | Wheeze detection | Wheeze detection | Wheeze detection, breathing sound analysis |
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, S.-H.; Lin, B.-S.; Tsai, C.-H.; Yang, C.-T.; Lin, B.-S. Design of Wearable Breathing Sound Monitoring System for Real-Time Wheeze Detection. Sensors 2017, 17, 171. https://doi.org/10.3390/s17010171
Li S-H, Lin B-S, Tsai C-H, Yang C-T, Lin B-S. Design of Wearable Breathing Sound Monitoring System for Real-Time Wheeze Detection. Sensors. 2017; 17(1):171. https://doi.org/10.3390/s17010171
Chicago/Turabian StyleLi, Shih-Hong, Bor-Shing Lin, Chen-Han Tsai, Cheng-Ta Yang, and Bor-Shyh Lin. 2017. "Design of Wearable Breathing Sound Monitoring System for Real-Time Wheeze Detection" Sensors 17, no. 1: 171. https://doi.org/10.3390/s17010171