Integration of a Social Robot in a Pedagogical and Logopedic Intervention with Children: A Case Study

 ,
, 
 ,
,  and
and 
Abstract
:1. Introduction
- Are actual robots prepared to be incorporated into pedagogical and logopedic intervention with children?
- What are the requirements expected by the therapist?
- What hardware–software architecture best suits the requirements of those sessions?
- Will the initial results be encouraging enough for the continuation of the present project?
2. Background
- Following instructions, as in imitative games [28]. These skills play an important role in the development of social cognition and communication, not only in children but in human beings in general.
- Provoking unexpected situations. Breakdowns as not planned situations [31] as robots are unable to identify misunderstandings.
Robotic Platform
3. Method
3.1. Experimental Design
3.2. Participants
3.3. Environmental Setup
3.4. Data Collection and Analysis
- Therapist personal diary of each session;
- Programmer personal diary of each session;
- Semi-structured interviews conducted to the therapist;
- Video recording of the sessions.
- A verbatim transcript of the content of the interviews and videotape recording.
- Data analysis with a reading of the transcribed material and viewing videos, in order to identify content units and establish initial categories.
- Successive meetings to establish the dynamics of coding, review the material, and resolve by consensus the observational categories. Discrepancies were resolved by discussion.
- We agreed during the process a “book of categories” in which a brief description of the specified category, an expanded definition, criteria about when using the category, and its grouping in families. This book allowed a more global view of the categories (parent nodes) and emerged families (tree nodes) of the analysis.
- This process was completed by saturating the information.
- Finding important quotes that describe the main ideas, grouping them to examine the general ideas, and finding the correlations between them.
- Constructing a narrative that connects the findings.
4. Architecture: Description and Evolution
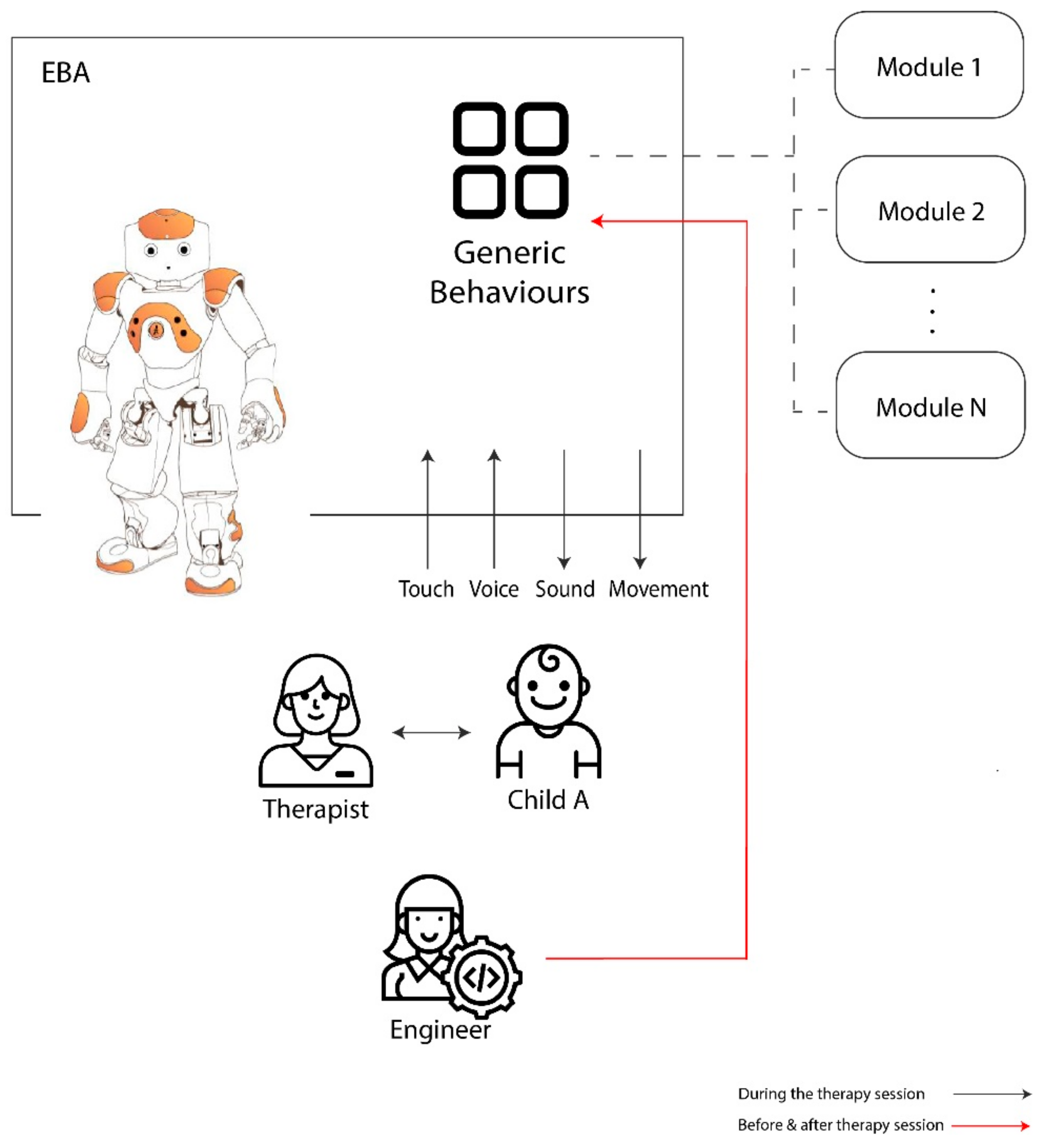
4.1. Initial Architecture
- Reading comprehension;
- dictations, stories and vocabulary, improvement of oral comprehension;
- articulation and phonetic-phonological pronunciation;
- phonological awareness and phonetic segmentation;
- literacy skills.
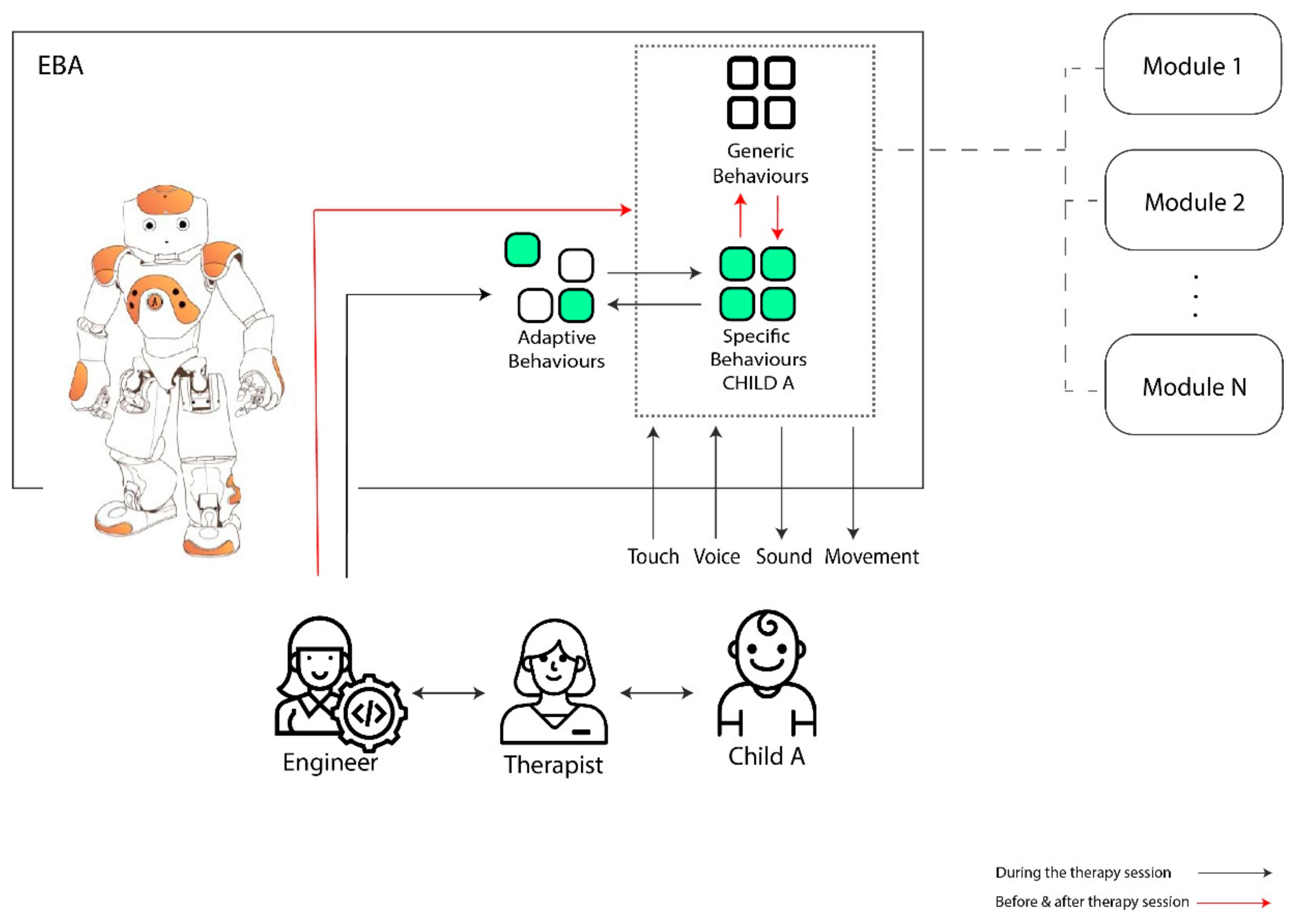
4.2. Final Adaptive Architecture Description
Example of an Adaptive Behavior and/or Specific Behavior
5. Preliminary Qualitative Results and Discussion
5.1. Technical Observations
- individualized software per children;
- individualized software per disorder;
- individualized software per type of work to be done in the session.
5.2. Learnings from the Sessions with the Robot
- Two interviews with the speech-therapist about the process (one before starting the experiment and one when the experiment was finished);
- Programmer and therapist diaries about the sessions;
- Video recordings of some sessions of children with EBA.
‘... It was a moment that ‘EBA’ said “Speaks me higher” and the child saw that EBA didn’t respond because he could not hear. She started up inadvertently, i.e., not gave the command “turn up the volume of your voice” because she has fully retracted that order. But she needed EBA listening to her, then there appeared the volume. So, there has been a significant change and from there it is true that parents have spoken with me and they say they have noticed that she speaks a little higher....’ [Second Interview with speech-therapist]
“She tells it to her friends in class and had to send a photo of the robot…. She told me that she is one of the few children in the school who has a robot. She says so and therefore she does her best to work or play with EBA.” [Second Interview with speech-therapist]
“I remember one day in a session were EBA had a broken finger, … Well, the parents had to phone me! Their child was scared because we had put an electrical tape on EBA finger, and he thought it was a cast. He had normalized EBA as if it were human. When the parents phone me they told that their child had slept badly, that “poor EBA”,…, that “Daddy please, phone EBA to see how is she, because she is in the hospital for sure….” But of course, you have toget to know this child. That this child says that and sees a fellow man as his fellow man..., because his equals... well, he has many behavior problems because he has an oppositional defiant disorder. So, normally, he attacks his peers. His greatest communication is to attack…. And suddenly, being so worried about EBA? It was a great leap that has also taken him out. That is very nice, it moves me.” [Second Interview with speech-therapist]
“He likes to show that he is smarter than the robot” [Diary of the Therapist].
“For Child 5 EBA looks like a robot. Child 5 is older than the others (12 years old). It is the only case that sees EBA as a robot. As a resource to learn. That is, child 5 is not going to become a friend of EBA.” [Second Interview with speech-therapist]
“Well, David is part of the furniture in the sessions. In mean, the children just greeted me and EBA. At the beginning I had to tell them, ‘Hey this is David, greets him’ … “ but then I gave up, because I realized that, for the children, he didn’t exist directly. Look! Not only did they not be aware that David was there, but they didn’t even realize there was a camera recording them” [Second Interview with the speech-therapist]
6. Conclusions and Future Works
- Structured language: EBA’s language is structured in a better way. The speech-therapist attributes certain positive effects on children to this.
- Absence of value judgments: According to the speech-therapist, thanks to the objective responses of EBA, the value of the reinforcer emitted by EBA to the children is higher.
- While the children see ‘EBA’ in the form of an equal (expressing some kind of empathy towards it), or as its student (the child becomes the teacher), some changes can be done in the way of working the objectives of the sessions. This turns into an amelioration of the children vocalization, improvement in construction and structures of sentences and, as a result, in an increase of the self-confidence of the children.
- The use of a robot in the therapy is helpful as a good learning tool for children and as a useful tool for the therapist to improve the observations of each session to discover new elements to include in each child’s therapy.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO World Report on Disability. 2011. Available online: http://www.who.int/disabilities/world_report/2011/en/ (accessed on 11 December 2017).
- Gates, B. A Robot in Every Home. Sci. Am. 2008, 296, 44–51. [Google Scholar] [CrossRef]
- Van der Loos, M.H.; Reinkensmeyer, D.J.; Guglielmelli, E. Rehabilitation and Health Care Robotics. In Springer Handbook of Robotics; Siciliano, B., Khatib, O., Eds.; Springer Handbooks: Cham, Switzerland, 2016; pp. 1685–1728. [Google Scholar] [CrossRef]
- Broekens, J.; Heerink, M.; Rosendal, H. Assistive social robots in elderly care: A review. Gerontechnology 2009, 8, 94–103. [Google Scholar] [CrossRef] [Green Version]
- Belpaeme, T.; Baxter, P.; Read, R.; Wood, R.; Cuay’ahuitl, H.; Kiefer, B.; Racioppa, S.; Kruijff-Korbayov’a, I.; Athanasopoulos, G.; Enescu, V.; et al. Multimodal Child-Robot Interaction: Building Social Bonds. J. Hum. Robot. Interact. 2012, 1, 33–53. [Google Scholar] [CrossRef] [Green Version]
- Chita-Tegmark, M.; Scheutz, M. Assistive Robots for the Social Management of Health: A Framework for Robot Design and Human–Robot Interaction Research. Int. J. Soc. Robot. 2020, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Belpaeme, T.; Kennedy, J.; Ramachandran, A.; Scassellati, B. Social robots for education: A review. Sci. Robot. 2018, 3. [Google Scholar] [CrossRef] [Green Version]
- Shiwa, T.; Kanda, T.; Imai, M.; Ishiguro, H.; Hagita, N. How Quickly Should Communication Robots Respond? In Proceedings of the Third International Conference on Human Robot Interation—HRI′08. Amsterdam, The Netherlands, 12–15 March 2008. [Google Scholar] [CrossRef]
- Abbas, T.; Khan, V.-J.; Gadiraju, U.; Barakova, E.; Markopoulos, P. Crowd of Oz: A Crowd-Powered Social Robotics System for Stress Management. Sensors 2020, 20, 569. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Luximon, Y. Trust in AI Agent: A Systematic Review of Facial Anthropomorphic Trustworthiness for Social Robot Design. Sensors 2020, 20, 5087. [Google Scholar] [CrossRef]
- Martín, A.; Pulido, J.C.; González, J.C.; García-Olaya, Á.; Suárez, C. A Framework for User Adaptation and Profiling for Social Robotics in Rehabilitation. Sensors 2020, 20, 4792. [Google Scholar] [CrossRef]
- Dawe, J.; Sutherland, C.; Barco, A.; Broadbent, E. Can social robots help children in healthcare contexts? A scoping review. BMJ Paediatr. Open 2018, 3. [Google Scholar] [CrossRef] [Green Version]
- De Greef, J.; Belpaeme, T. Why Robots Should Be Social: Enhancing Machine Learning through Social Human-Robot Interaction. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, J.; Baxter, P.; Belpaeme, T. The Impact of Robot Tutor Nonverbal Social Behavior on Child Learning. Front. Ict 2017, 4, 6. [Google Scholar] [CrossRef] [Green Version]
- Serholt, S. Child–Robot Interaction in Education. Gothenburg: University of Gothenburg 2017. Available online: http://hdl.handle.net/2077/52564 (accessed on 23 October 2017).
- Takanishi, A.; Endo, N.; Petersen, K. Towards Natural Emotional Expression and Interaction: Development of Anthropomorphic Emotion Expression and Interaction Robots. Int. J. Synth. Emot (IJSE) 2012, 3, 1–30. [Google Scholar] [CrossRef]
- Dieh, J.; Schmitt, L.; Villano, M.; Crowell, C. The clinical use of robots for individuals with Autism Spectrum Disoirders: A critical Review. Res. Autism C2A0Spectr. Disord. 2012, 6, 249–262. [Google Scholar] [CrossRef] [Green Version]
- Scassellati, B.; Admoni, H.; Mataric, M. Robots for Use in Autism Research. Annu. Rev. Biomed. Eng. 2012, 14, 275–294. [Google Scholar] [CrossRef] [Green Version]
- Cao, H.-L.; Esteban, P.G.; Bartlett, M.; Baxter, P.; Belpaeme, T.; Billing, E.; Cai, H.; Coeckelbergh, M.; Costescu, C.; David, D.; et al. Robot-EnhancedTherapy. Development and Validation Of Supervised Autonomous Robotic System For Autism Spectrum Disorders Therapy. IEEE Robot. Autom. Mag. 2019, 26, 49–58. [Google Scholar] [CrossRef]
- García-Varea, I.; Jiménez-Picazo, A.; Martínez-Gómez, J.; Revuelta-Martínez, A.; Rodríguez-Ruiz, L.; Bustos, P.; Nuñez-Trujillo, P.M. APEDROS: Asistencia a Personas con Discapacidad mediante Robots Sociales. Retrieved from VI Congreso Iberoamericano de Tecnologias de Apoyo a la Discapacidad IBERDISCAP June 2011. Available online: https://www.researchgate.net/publication/235938148_APEDROS_ASISTENCIA_A_PERSONAS_CON_DISCAPACIDAD_MEDIANTE_ROBOTS_SOCIALES (accessed on 11 December 2017).
- Lee, H.; Hyun, E. The Intelligent Robot Contents for Children with Speech-Language Disorder. J. Educ. Techno. Soc. 2015, 3, 100–113. [Google Scholar]
- Peñeñory, V.M.; Manresa-Yee, C.; Riquelme, I.; Collazos, C.A.; Fardoun, H.M. Scoping Review of Systems to Train Psychomotor Skills in Hearing Impaired Children. Sensors 2018, 18, 2546. [Google Scholar] [CrossRef] [Green Version]
- Leyzberg, D.; Spaulding, S.; Scassellati, B. Personalizing robot tutors to individuals′ learning differences. In Proceedings of the 2014 ACM/IEEE International Conference on Human-Robot Interaction, Bielefeld, Germany, 3–6 March 2014; pp. 423–430. [Google Scholar]
- Westlund, J.M.; Dickens, L.; Jeong, S.; Harris, P.L.; DeSteno, D.; Breazeala, C.L. Children Use Non-Verbal Cues to Learn New Words From Robots as well as People. Int. J. Child. Comput. Interact. 2017, 13, 1–9. [Google Scholar] [CrossRef]
- Cherney, L.R.; Halper, A.S.; Holland, A.L.; Cole, R. Computerized script training for aphasia: Preliminary results. Am. J. Speech Lang. Pathol. 2008, 17, 19–34. [Google Scholar] [CrossRef] [Green Version]
- Jeon, K.H.; Yeon, S.J.; Kim, Y.T.; Song, S.; Kim, J. Robot-based augmentative and alternative communication for nonverbal children with communication disorders. In Proceedings of the 2014 ACM International Joint Conference on Pervasive and Ubiquitous Computing (UbiComp ′14), Seattle, WA, USA, 13–17 September 2014; pp. 853–859. [Google Scholar] [CrossRef]
- Malik, N.A.; Yussof, H.; Hanapiah, F.A. Development of Imitation Learning through Physical Therapy Using a Humanoid Robot. Procedia Comput. Sci. 2014, 42, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Nehaniv, C.L.; Dautenhahn, K. Imitation and Social Learning in ROBOTS, HUMANS and Animals: Behavioural, Social and Communicative Dimensions; Cambridge University Press: Cambridge, UK, 2007. [Google Scholar] [CrossRef]
- Dautenhahn, K.; Werry, I. A Quantitative technique for analysing robot-human. In Proceedings of the IROS2002, IEEE/RSJ International Conference on Intelligent Robots, Lausanne, Switzerland, 30 September–4 October 2002; pp. 1132–1138. [Google Scholar]
- Kennedy, J.; Baxter, P.; Belpaeme, T. Nonverbal Immediacy as a Characterisation of Social Behaviour for Human–Robot Interaction. Int. J. Soc. Robot. 2017, 9, 109–128. [Google Scholar] [CrossRef]
- Serholt, S. Breakdowns in children’s interactions with a robotic tutor: A longitudinal study. Comput. Hum. Behav. 2017, 81, 250–264. [Google Scholar] [CrossRef]
- Beukelman, D.R.; Light, J.C. Augmentative and Alternative Communication: Supporting Children and Adults with Complex Communication Needs; Paul Brookes Publishing: Baltimore, MD, USA, 2020; pp. 1–17. [Google Scholar]
- Vasalou, A.; Khaled, R.; Holmes, W.; Gooch, D. Digital games-based learning for children with dyslexia: A social constructivist perspective on engagement and learning during group game-play. Comput. Educ. 2017, 114, 175–192. [Google Scholar] [CrossRef] [Green Version]
- Gouaillier, D.; Hugel, V.; Blazevic, P.; Kilner, C.; Monceaux, J.; Lafourcade, P.; Marnier, B.; Serre, J.; Maisonnier, B. The NAO humanoid: A combination of performance and affordability. CoRR 2008. abs/0807.3223. [Google Scholar]
- Gomilko, S.; Zimina, A.; Shandarov, E. Attention Training Game with Aldebaran Robotics NAO and Brain-Computer Interface. In Interactive Collaborative Robotics; Ronzhin, A., Rigoll, G., Meshcheryakov, R., Eds.; Springer Cham: Basel, Switzerland, 2016; Volume 9812, pp. 27–31. [Google Scholar] [CrossRef]
- Nalin, M.; Bergamini, L.; Giusti, A.; Baroni, I.; Sanna, A. Children’s perception of a Robotic Companion in a mildly constrained setting. Proceedings of IEEE/ACM Human-Robot Interaction 2011 Conference (Robots with Children Workshop), Lausanne, Switzerland, 6–9 March 2011. [Google Scholar]
- Ismail, L.; Shamsudin, S.; Yussof, H.; Hanapiah, F.; Zahari, N.I. Robot-based Intervention Program for Autistic Children with Humanoid Robot NAO: Initial Response in Stereotyped Behavior. Procedia Eng. 2012, 41, 1441–1447. [Google Scholar] [CrossRef] [Green Version]
- Vrochidou, E.; Najoua, A.; Lytridis, C.; Salonidis, M.; Ferelis, V.; Papakostas, G. Social robot NAO as a self-regulating didactic mediator: A case study of teaching/learning numeracy. In Proceedings of the 26th International Conference on Software, Telecommunications and Computer Networks (SoftCOM), Split, Croatia, 13–15 September 2018. [Google Scholar]
- Andreasson, R.; Alenljung, B.; Billing, E.; Lowe, R. Affective Touch in Human–Robot Interaction: Conveying Emotion to the Nao Robot. Int. J. Soc. Robot. 2018, 10, 473–491. [Google Scholar] [CrossRef] [Green Version]
- Alenljung, B.; Andreasson, R.; Lowe, R.; Billing, E.; Lindblom, J. Conveying emotions by touch to the Nao Robot: A user experience perspective. Multimod. Technol. Interact. 2018, 2, 82. [Google Scholar] [CrossRef] [Green Version]
- Rossi, S.; Larafa, M.; Ruocco, M. Emotional and Behavioural Distraction by a Social Robot for Children Anxiety Reduction During Vaccination. Int. J. Soc. Robot. 2019, 12, 765–777. [Google Scholar] [CrossRef]
- Dahl, T.; Kamel Boulos, M.N. Robots in health and social care: A complementary technology to home care and telehealthcare? Robotics 2013, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- Huisman, C.; Kort, H. Two-year use of care robot Zora in Dutch nursing homes: An evaluation study. Healthcare 2019, 7. [Google Scholar] [CrossRef] [Green Version]
- Taheri, A.; Meghdari, A.; Alemi, M.; Pouretemad, H. Human–Robot Interaction in Autism Treatment: A Case Study on Three Pairs of Autistic Children as Twins, Siblings, and Classmates. Int. J. Soc. Robot. 2018, 10, 93–113. [Google Scholar] [CrossRef]
- Tapus, A.; Peca, A.; Aly, A.; Pop, C.; Jisa, L.; Pintea, S.; Rusu, A.; David, D. Children with autism social engagement in interaction with Nao, an imitative robot—A series of single case experiments. Interact. Stud. 2012, 13, 315–347. [Google Scholar] [CrossRef]
- Yin, R.K. Case Study Research: Design and Methods; Sage Publications: Thousand Oaks, CA, USA, 2003; Volume 5. [Google Scholar]
- Stake, R.E. The Art of Case Study Research; Sage Publications: Thousand Oaks, Ca, USA, 1995. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Module | Objectives | EBA Mission |
|---|---|---|
| Reading comprehension | To strengthen reading |
|
| To work memory and sustained attention |
| |
| Dictations, stories, and vocabulary. Improvement of oral comprehension | To strengthen vocabulary, as well as written and oral comprehension |
|
| ||
| ||
| Articulation and phonetic-phonological pronunciation | To develop the grapheme-phoneme correspondence. |
|
| To recognize and to identify the auditory discrimination of the different phonemes. |
| |
| To develop pronunciation skills. |
| |
| Phonological awareness and phonetic segmentation | To strength the lexical and phonological routes of reading and writing. |
|
| To enhance the grapheme-phoneme conversion. |
| |
| To identify syllabic structures cv, vc, cvvc, cvcv, ccv, cvv, ccvc. |
| |
| Literacy skills | To increase the concentration of the child and strengthen auditory processing. |
|
| To be able to respond to a verbal question. |
| |
| To develop active listening skills. |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Egido-García, V.; Estévez, D.; Corrales-Paredes, A.; Terrón-López, M.-J.; Velasco-Quintana, P.-J. Integration of a Social Robot in a Pedagogical and Logopedic Intervention with Children: A Case Study. Sensors 2020, 20, 6483. https://doi.org/10.3390/s20226483
Egido-García V, Estévez D, Corrales-Paredes A, Terrón-López M-J, Velasco-Quintana P-J. Integration of a Social Robot in a Pedagogical and Logopedic Intervention with Children: A Case Study. Sensors. 2020; 20(22):6483. https://doi.org/10.3390/s20226483
Chicago/Turabian StyleEgido-García, Verónica, David Estévez, Ana Corrales-Paredes, María-José Terrón-López, and Paloma-Julia Velasco-Quintana. 2020. "Integration of a Social Robot in a Pedagogical and Logopedic Intervention with Children: A Case Study" Sensors 20, no. 22: 6483. https://doi.org/10.3390/s20226483