
A Study on the Public’s Crisis Management Efficacy and Anxiety in a Pandemic Situation—Focusing on the COVID-19 Pandemic in South Korea



1
Department of Public Administration, Chungbuk National University, Cheongju 28644, Korea
2
National Crisisonomy Institute, Chungbuk National University, Cheongju 28644, Korea
*
Author to whom correspondence should be addressed.
Sustainability 2021, 13(15), 8393; https://doi.org/10.3390/su13158393
Submission received: 10 June 2021
/
Revised: 23 July 2021
/
Accepted: 24 July 2021
/
Published: 27 July 2021
(This article belongs to the Special Issue Social Resilience and Household Economics: Perspectives for Sustainability)
Abstract
:Social distancing, shutdown, and lockdown policies have recently been implemented worldwide to help slow the spread of the Coronavirus disease 2019 (COVID-19), which has caused economic, social, and cultural crises on a global scale. To help create safe communities, we aimed to analyze the factors affecting the public’s anxiety and efficacy to overcome crises. The results show that efficacy is associated with sex, education, central government support, the public hygiene environment, and public hygiene behaviors. Anxiety was shown to have a negative relationship with central government support, a positive relationship with civilian support, and a negative relationship with efficacy. For a country to prevent the spread of a novel infectious disease, alleviate the anxiety of the population, and construct a safe community in the midst of a global pandemic, active central government support and response, protection of vulnerable populations, publicization of policies, and crisis management communication are essential. In particular, identifying an evidence-based method to understand and address the psychological and social influences of COVID-19, such as excessive fear and discrimination, providing insight into risk factors associated with future society for policy makers, and establishing potential and sustainable public health communication strategies are of paramount importance.
1. Introduction
To stop the spread of Coronavirus disease 2019 (COVID-19), which began in 2019 and was recognized as a global pandemic in 2020, various governmental policies have been introduced throughout the world. Countries have responded by closing schools and public institutions and supporting policies such as social distancing to reduce the rate of transmission in the civilian sector [1].
The Oxford COVID-19 Government Response Tracker systematically presents and compares policies between countries and companies to understand how governmental responses to COVID-19 have evolved. Research shows that governments in most countries have enforced stronger policies and countermeasures as the number of cases has rapidly increased. In addition, faster enactment of strong lockdown measures has been shown to be an important factor in more effectively inhibiting the spread of infections [2]. However, the speed and scale of responses have differed depending on each government’s awareness of the threat, and higher government awareness has been associated with a lower rate of confirmed cases [2,3,4].
COVID-19 has had an impact on many different aspects of people’s lives. It has caused isolation and a number of psychological problems, such as panic disorder, anxiety, and depression [5]. Qiu et al. [6] analyzed data from 52,370 persons in six provinces and administrative regions in Hong Kong, Macao, and Taiwan, and reported that 35% of respondents had experienced psychological distress due to COVID-19.
There have been active collaborative research efforts involving public health experts and sociologists worldwide to slow the spread of COVID-19. The subject matter of this research includes public messages, self-perceived risk due to COVID-19, fear of COVID-19, societal moral foundations, and positive behavioral changes (e.g., social distancing and improved hand hygiene) introduced through policies [7].
In their study regarding government policies to prevent the spread of COVID-19 in Vietnam, La et al. [8] highlighted the need for immediate, genuine cooperation between the government, civilian society, and individual citizens and hypothesized that trust, based on timely communication from the government and the press would help societies to overcome the crisis.
Because COVID-19 is a global pandemic, there is an urgent need for policy plans in the public health, environmental, science and technology, and social sciences sectors. In particular, we need to have in-depth discussions about the role of government based on research showing that the spread of infectious diseases can be inhibited depending on the speed with which governments implement responsive measures and strong policies [9,10,11,12].
However, the government’s role and policies only become effective when they have the support and trust of the public [13,14,15]. There is active research regarding the role of society in the changing times of COVID-19 [16] and how the government can exert control over the people by enacting rules and policies [3,12,17]. However, it is difficult to find a study on public awareness of the effectiveness of government policy. In this study, we analyzed factors affecting the public’s efficacy and anxiety in relation to crisis management, with the aim of helping to improve future crisis management policies.
1.1. Crisis Management Efficacy
Effective crisis management depends on the abilities of administrators, decision-makers, related organizations, and interested parties who contribute to the specific stages and activities of crisis management. Crises in modern society are gradually transcending the bounds of individual organizations and sectors, requiring intermittent or continuous mediation and cooperation between different fields and levels of government [18].
Research on successful crisis management has previously examined the importance of social capital-related factors (e.g., trust, shared norms, networks, administrative culture) as activating or deactivating factors in crisis management [19,20]. In the same way, researchers are now emphasizing the importance of software factors (e.g., psychological, cultural) [21,22,23].
Previous research shows that trust in government, public trust, and institutional trust are essential for the validity and effectiveness of institutional agreements [24,25]. Persson et al. [22] claimed that for the EU to ensure the public support, resources, and the validity needed to construct a properly functioning crisis management and disaster response institution, it is essential for citizens, who are the primary actors in this field, to have high efficacy based on trust in the EU. Christensen et al. [26] reported that a government needs to be both capable and lawful to implement a properly operating crisis management system. In particular, the validity of the ruling structure is based on trust in government.
Christensen and Lægreid [27] reported that the reason for the positive appraisal of the Norwegian government’s successful crisis management response to COVID-19, compared to other countries, should be understood in terms of a high-trust society with a reliable and expert bureaucracy, strong control, a good economic situation, robust welfare, and low population density. In particular, Norway was able to execute a control strategy based on the government’s cooperative and practical decision-making, successful communication with the public, ample resources, and citizens’ high level of trust in the government.
Citizen participation to overcome disasters has a positive effect on improving community resilience [28,29,30]. According to a study by Kweit and Kweit [31], rather than disaster recovery systems based on bureaucratic guidance, recovery projects based on political comfort and trust that promote widespread citizen participation are effective at increasing citizen satisfaction.
In particular, Frisby et al. [32] reported that efficient crisis management arises from efficacy based on learned perceptions. According to Bandura et al. [33], efficacy is a major factor in people’s behaviors and beliefs. Bandura [34,35] defines self-efficacy as an individual’s certainty that the behaviors and cognitive ability that they believe to be correct can be used successfully to achieve a goal or complete a task.
Zimmerman et al. [36], Abdalla [37], Ancis and Phillips [38], Garavalia and Gredler [39], and Dunlap [40] have reported that people with high self-efficacy think and act differently than those with low self-efficacy, and those with higher self-efficacy are more likely to make decisions based on their goals and the available information, and are ultimately more likely to succeed. In addition, high self-efficacy is derived from education. In other words, learning can have an effect on self-efficacy [41,42,43].
Self-efficacy shows strong correlations in health-related fields, which is clear in Ajzen’s theory of planned behavior [44,45] and Bandura’s social learning theory [34,35]. Reuter et al. [46] and Perkins et al. [47] found that self-efficacy causes changes in health-related habits, diet, and behaviors.
Mileti and Sorensen [48] as well as Mileti and Fitzpatrick [49] discussed self-efficacy in terms of crisis management communications, claiming that self-efficacy should be recognized as an outcome variable when designing messages in response to threats or crises. It is important to produce behaviors that provide protection from a threat or crises through the perception of messages [50,51,52]. The goal of improving self-efficacy in such a situation is to rapidly and effectively warn and direct people in potential danger to take the proper action to protect themselves.
Based on the above results, we can infer that factors affecting successful crisis management start with the validity of the governmental organization and voluntary participation by citizens, and that these are supported by the high self-efficacy of individuals. Thus, we set the following hypotheses:
Hypothesis 1 (H1).
The government’s policies supporting crisis management during the COVID-19 pandemic will have a positive effect on crisis management efficacy.
Research results from Christensen and Lægreid [27], Weible et al. [11], and Parker et al. [53] demonstrate expeditious control of infectious diseases through usage of control strategies based on the good leadership of politicians and administrative authorities, a highly trustworthy society with reliable and professional bureaucracy, resilient economy, cooperative and practical decision-making procedures in the case of welfare states, successful communication with the public, abundant resources, and a mutually trusting relationship between the society and the government.
Hypothesis 2 (H2).
Better individual practice of behaviors to overcome the spread of COVID-19 (hygienic tendencies) will have a positive effect on crisis management efficacy.
Analysis based on results from various studies including those by Vung et al. [54], Hozak et al. [55], Loftus et al. [56], and Mbakaya et al. [57] indicate that personal hygienic tendencies and behaviors increase disease resistance and efficiency of crisis management.
Hypothesis 3 (H3).
Perceptions of the level of access to public hygiene facilities will have a positive effect on crisis management efficacy.
Studies by Banik et al. [58], Ssemugabo et al. [59], and Dhesi et al. [60] posit that poor awareness of the accessibility of public hygiene facilities or a lack of an established system leads to proportional vulnerability in crisis management.
Hypothesis 4 (H4).
Knowledge about public hygiene information will have a positive effect on crisis management efficacy.
Studies by Johnson and Hariharan [61], Checchi et al. [62], and Kumwenda [63] show that knowledge and the accessibility of public hygiene information increase crisis management efficacy and reduce personal fears.
Hypothesis 5 (H5).
Perceptions of hygiene facilities that are widely used by the public will have a positive effect on crisis management efficacy.
An analysis of studies by Heuvelink et al. [64], Michael et al. [65], and Muoki et al. [66] indicates that perceptions and customs surrounding public hygiene facilities influence the efficacy of crisis management.
Hypothesis 6 (H6).
Knowledge about the population’s hygiene will have a positive effect on crisis management efficacy.
1.2. The Public’s Anxiety
Individuals struggle to make clear, logical judgments when they are wrapped up in fear and anxiety [70,71,72]. According to a study by Harper et al. [7], anxious, negative emotions are generally shown by individuals who will actively protect themselves. To fulfill this protective function and avoid infectious diseases, individuals are keen to implement behavioral changes in adherence to public health principles (e.g., hand washing and social distancing).
The government’s fight against fear is an important aspect of crisis management policy—citizens who are faced with disasters look to the government for protection [73]. In addition, the anxiety experienced in a crisis encourages citizens to consent to national surveillance and voluntary release of their data. Hillebrand [74] investigated anxiety and its effect on the public in Germany early in the COVID-19 pandemic and found that: (1) anxiety increased consent to voluntary release of data; (2) anxiety increased the rate of consent to direct and indirect national surveillance by modulating mistrust in others; and (3) there was a voluntary, robust increase in trust in government. This shows that anxiety among the public leads to changes in behavior and trust in government.
When anxiety from a crisis accumulates, individuals show more dependence on and expectations of the government, compared to peer or personal dependence [75,76]. According to Carayannopoulos [77], there are various actors in crisis management, including the government, individuals, and civilian sectors, but the government plays the most important role in controlling crisis management because of factors such as means and processes for support in crisis management, facilitated data management and infrastructure, suitable budgeting, and a responsibility framework.
The above studies show that the public’s anxiety about a threat or crisis can result in support of not only government policy and civilian support, but also community trust. Hence, we set the following hypotheses:
Hypothesis 7 (H7).
The government’s crisis management support policies surrounding COVID-19 will decrease public anxiety.
Studies by Altiparmakis et al. [78], Abate et al. [79], and Mintrom and O’Connor [80] found that diverse support policies of the government overcome national industrial crises, resolve social polarization and national conflicts, and increase trust toward the national leader and the government.
Hypothesis 8 (H8).
Civilian crisis management support policies will increase public anxiety.
Studies by Mahmud et al. [81], Chen and Hang [82], and García-Sánchez and García-Sánchez [83] demonstrate that the introduction of diverse social responsibilities can be used for civilian support, which mollifies economic and social damage with the combined effort of local communities. Further, the positive image of public effort and cooperation can also be strengthened.
Hypothesis 9 (H9).
Efficacy of the government, medical staff, national population, and individuals will decrease public anxiety.
2. Materials and Methods
This study utilized an online questionnaire in South Korea to measure the characteristics of self-efficacy and anxiety among the public regarding crisis situations. The questionnaire data were collected through Macomill Embrain, an online survey company, from 18 to 25 May 2020. Participants were recruited through arbitrary online sampling accounting for sex, age, and region. An email invitation to complete the survey was sent to 7320 panelists aged 20 years and older and a total of 620 requests to participate in the survey were received (response rate = 8.5%). Prior to completing the survey, those who had agreed to participate were asked if they consented to voluntarily completing the survey. Only those who agreed were allowed access to the questionnaire. Panelists who completed the survey received an incentive equivalent to approximately US $3.00. Statistical analysis was performed using the statistical program IBM SPSS Statistics 25. Frequency distributions, reliability analyses, and regression analyses were conducted.
The respondents shown in Table 1 were 51.8% male and 48.2% female. With regard to age, 18.1% of the respondents were 20–29 years old, 17.6% were 30–39 years old, 21.5% were 40–49 years old, 23.5% were 50–59 years old, and 19.4% were ≥60 years old. Regarding place of residence, 47.9% lived in the greater capital region, 25% in Gyeongsang-do, 12.9% in Jeolla-do or Jeju-do, and 14.2% in Chungcheong-do or Gangwon-do. Regarding education, 20% of respondents had a high school education or lower, 16.1% had graduated from a technical college, 55.3% had graduated from a 4-year university, and 8.5% had graduated from graduate school. Almost one-half (49.4%) of the respondents were employed full-time, 5.5% were employed part-time, 11.6% were the company owner or self-employed, 7.1% were students, 13.9% were homemakers, and 8.4% were unemployed. The monthly household income was <2 million KRW (Korean Won) for 8.2% of respondents, 2–4 million KRW for 32.4%, 4–6 million KRW for 29.4%, 6–8 million KRW for 16.5%, 8–10 million KRW for 8.7%, and ≥10 million KRW for 4.8%.
The questionnaire was converted into a web survey that was easy to respond to online and distributed via e-mail to respondents. All variables were measured using a 5-point Likert scale ranging from 1 (absolutely not) to 5 (very much) with higher scores indicating more positive responses. The reliability and validity were measured for analysis, and the questionnaire items’ reliability coefficients are shown in Table 2. The reliability coefficient (Cronbach’s alpha) exceeded the cutoff value (.60) for all concepts, indicating that the results were reliable.
3. Results
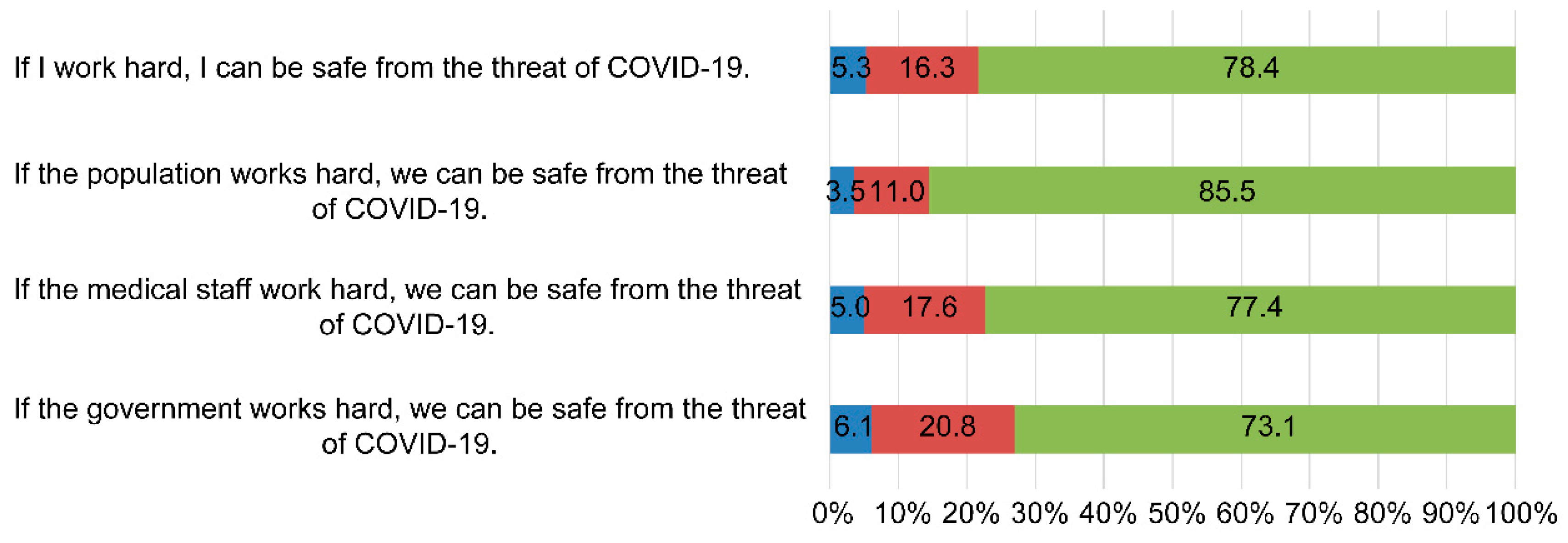
Figure 1 shows the perceptions of efficacy with regard to four different crisis management support mechanisms: self-efficacy, efficacy of the population, medical staff efficacy, and government efficacy.
The results of the survey showed 73.1% agreement with government efficacy (scores of 4 or 5 on the Likert scale), 77.4% agreement with medical staff efficacy, 85.5% agreement with efficacy of the population, and 78.4% agreement with self-efficacy. The fact that the efficacy of the population was highest (85.5%) demonstrates strong agreement about overcoming the crisis through social unity.
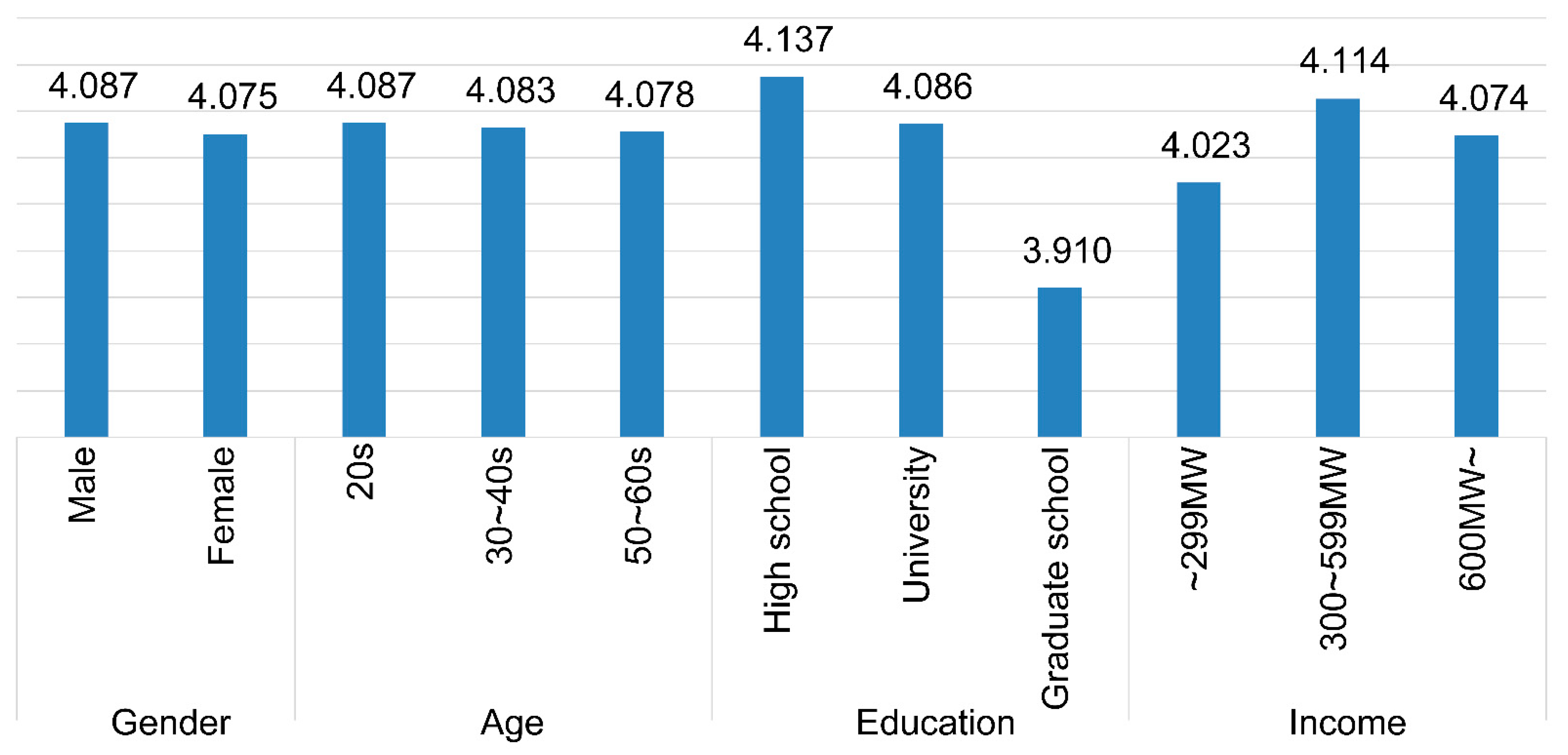
Figure 2 presents the means of the efficacy variables by demographic characteristics. Scores range from 1 to 5, with higher scores indicating higher efficacy ratings. In the demographic analysis of crisis management efficacy (Figure 2), males showed higher perceived efficacy than females [88,89]. Meanwhile, there was little difference between age groups. High school graduates had the highest perceived efficacy, while respondents with an income level of 3–6 million KRW showed higher perceived efficacy than other income groups.
To investigate the relationships between the variables, we performed a simple correlation analysis controlling for age, income, sex, education, and social status, and the results are shown in Table 3. Efficacy was correlated with public hygiene behaviors, public hygiene environment, public hygiene information, public hygiene facilities, public hygiene of the population, government support, civilian support, and anxiety. In particular, there was a strong positive correlation with government support and a negative correlation with anxiety. This indicates that government support has a positive relationship with crisis management efficacy and that efficacy is associated with lower levels of anxiety. Thus, suitable governmental support policies are needed.
There were positive correlations between public hygiene behaviors, public hygiene environment, public hygiene information, public hygiene facilities, and public hygiene of the population. Higher levels of behaviors related to public hygiene (e.g., hand washing, wearing masks, social distancing) were associated with the public hygiene environment, information, and facilities, which implies that it is important to construct the appropriate environment, information, and facilities, and to develop various methods of communications and publicity to promote behaviors for safe public hygiene.
We performed a regression analysis to measure the perceptions of efficacy and anxiety. The results are summarized in Table 4 and Table 5.
When sociodemographic variables were inspected in detail, sex and education level were found to affect efficacy. O’Connor et al. [89] and Ding et al. [90] reported that females perceive the world as more dangerous than males, and this leads to more active perceptions of efficacy based on positive perceptions of response behaviors and overcoming difficult situations.
Education level also showed a correlation indicating that lower levels of education are associated with higher ratings of the efficacy of crisis management, which is consistent with a study by Calderón-Larrañaga et al. [91], in which an elderly, vulnerable population with low education was found to be at more risk both biologically and economically. In addition, Tian et al. [92] reported that COVID-19 has a negative psychosocial impact on citizens with low education and in a vulnerable working environment. Based on these findings, we can infer that vulnerable groups with high awareness of danger show higher perceived efficacy for successful crisis management. However, in our regression analysis, age and income did not show any major effect on efficacy.
With regard to support factors, central government support was found to have a significant effect on perceived crisis management efficacy. Local government support and civilian support did not have a significant effect on perceived crisis management efficacy. This may be because COVID-19 does not only affect specific regions, but has global effects. Therefore, the role of the central government and the nation are emphasized rather than the effects of support from local governments [93,94,95].
Finally, public hygiene behaviors to avoid contracting COVID-19 (e.g., social distancing, washing hands) and the public hygiene environment in the country had effects on crisis management efficacy, while public hygiene information, public hygiene facilities, and public hygiene of the population did not have major effects. This may be because case studies of countries implementing hygiene activities, such as social distancing [96,97,98], daily mask use [99,100,101], and a safe public hygiene environment [102,103,104,105] have already been recognized as scientific evidence for the prevention of COVID-19. These public hygiene behaviors and public hygiene environment variables had an effect on efficacy for successful crisis management [17,96,97,98,99,100,101,102,103,104,105,106,107].
Table 5 shows the results of the regression analysis for anxiety. Examining the effects of sociodemographic variables on perceived anxiety in detail revealed that neither sex, age, income, nor education level had a major effect on anxiety. As shown in studies by Roy et al. [108], Huang and Zhao [109], and Salari et al. [110], because COVID-19 is infecting large numbers of people across international borders and different communities, most survey participants have shown high levels of perceived anxiety, negating the impact of any single sociodemographic variable.
Among support-related variables, central government support and civilian support have effects on perceived anxiety. In particular, central government support reduced perceived anxiety. According to a study by Hale et al. [2], an immediate response and support from the government affect the rate of transmission of COVID-19, and the rate of transmission has a direct effect on public anxiety. Civilian support increased anxiety. This may be due to infection clusters caused by a small minority of civilian organizations failing to properly adhere to the government’s quarantine guidelines [111,112]. Finally, crisis management efficacy reduced anxiety among the general public.
4. Discussion
The purpose of this study was to examine measures taken to inhibit the spread of the COVID-19 pandemic and to determine their effects on the efficacy and anxiety of the general public regarding crisis resolution. In particular, we aimed to help improve future crisis management policy by analyzing these factors.
Our findings have several important implications. First, some groups that are vulnerable to crises (e.g., females, those with lower education status) showed a need to overcome the crisis via strong efficacy. Thus, crisis management systems and policies for infectious diseases should be designed to meet the needs of the groups that are vulnerable to crises. It is a clear fact that the inequality that appears in groups vulnerable to COVID-19 pandemic also applies to developed countries. Accordingly, policy makers should react to COVID-19 while considering the measures to ease the inequality as well as the risks for the vulnerable groups [113,114,115,116].
Second, in a pandemic, the role of the central government is much more prominent than that of local governments. Since COVID-19 is not restricted to certain regions, the central government is essential in the implementation of organizations, systems, and institutions that can effectively respond to the pandemic. In particular, it is difficult to respond to the spread of new diseases due to the lack of knowledge and information and expertise, so the risk management should be implemented based on the official control of the central government and distribution of the resources [117,118,119].
Third, personal hygiene behaviors and the public health environment have direct effects on the efficacy of the public, meaning that active publicity and communication need to be developed for related policies.
Fourth, to alleviate the nation’s anxiety, the government needs to reinforce its role in moderating, managing, and supervising civilians who refuse to comply or interfere with the government’s support and policies. The prompt measures taken by the government to effectively convey crisis information to the public during crises can cause a positive influence on citizen participation [120,121,122].
5. Limitations
This study has several limitations. First, of the many variables in public crisis management, this study focused only on the risk perception of the public in regard to anxiety and efficacy. There is a need to explore other variables (e.g., social capital, culture, beliefs, values, etc.) that influence public crisis management in the future. Second, the participants in this study were limited to Koreans during the COVID-19 pandemic. Since research on overcoming a pandemic has a worldwide impact, there is a need to examine various countries, types of damage, victims, and private organizations, and to compare the results in the future.
Third, this study was not able to include data of individuals who were infected or cured of COVID-19 in its analysis. Research on individuals infected with or undergoing treatment for infectious diseases has hitherto focused mainly on analyzing medical connections [123,124,125,126]. Thus, additional research on public awareness of the danger of anxiety due to concerns over employment, family health (spreading the infectious disease), and financial difficulties of individuals infected with or undergoing treatment for infectious diseases is warranted.
6. Conclusions
In conclusion, the central government should implement active support and response measures to protect the vulnerable populations, promote policies, and improve crisis management communication to ensure a safe community, slow the spread of COVID-19, and alleviate the anxiety of the national population.
Further, identifying an evidence-based method to understand and address the psychological and social influences of COVID-19, such as excessive fear (or apathy or adequate attention) and discrimination, is crucial [127,128,129]. Analysis of public anxiety and danger awareness will provide insight regarding future risk factors for policy makers and assist in the optimization of potential and sustainable public health communication strategies [130,131,132].
Author Contributions
Conceptualization, S.-A.K. and E.-J.L.; methodology, S.-A.K.; software, S.-A.K.; validation, E.-J.L.; formal analysis, S.-A.K.; investigation, S.-A.K.; resources, S.-A.K.; data curation S.-A.K.; writing—original draft, S.-A.K.; writing—review and editing, S.-A.K. and E.-J.L.; visualization, S.-A.K.; supervision, E.-J.L. Both authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2020S1A5B8103910).
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Ethics Approval and Consent to Participate
This study received ethics approval from the Research Ethics Committee of Chungbuk National University (CBNU 202006-0109). All participants provided informed consent before completing the survey.
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| SE | standard error of the mean |
References
- Hsiang, S.; Allen, D.; Annan-Phan, S.; Bell, K.; Bolliger, I.; Chong, T.; Druckenmiller, H.; Huang, L.Y.; Hultgren, A.; Krasovich, E.; et al. The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature 2020, 584, 262–267. [Google Scholar] [CrossRef]
- Hale, T.; Angrist, N.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S. Variation in Government Responses to COVID-19. Blavatnik School of Government, University of Oxford Working Paper. Available online: https://www.bsg.ox.ac.uk/sites/default/files/2020-05/BSG-WP-2020-032-v6.0.pdf (accessed on 30 September 2020).
- Chen, S.; Yang, J.; Yang, W.; Wang, C.; Bärnighausen, T. COVID-19 control in China during mass population movements at New Year. Lancet 2020, 395, 764–766. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.; Barceló, J.; Hartnett, A.S.; Kubinec, R.; Messerschmidt, L. COVID-19 Government Response Event Dataset (CoronaNet v. 1.0). Nat. Hum. Behav. 2020, 4, 756–768. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatr. 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R.D. Functional fear predicts public health compliance in the COVID-19 pandemic. Int. J. Ment. Health Addict. 2020, 1–14. [Google Scholar] [CrossRef]
- La, V.P.; Pham, T.H.; Ho, M.T.; Nguyen, M.H.; Nguyen, K.L.P.; Vuong, T.T.; Nguyen, H.K.T.; Tran, T.; Khuc, Q.; Ho, M.T.; et al. Policy response, social media and science journalism for the sustainability of the public health system amid the COVID-19 outbreak: The Vietnam lessons. Sustainability 2020, 12, 2931. [Google Scholar] [CrossRef] [Green Version]
- Studdert, D.M.; Hall, M.A. Disease control, civil liberties, and mass testing—calibrating restrictions during the COVID-19 pandemic. N. Engl. J. Med. 2020, 383, 102–104. [Google Scholar] [CrossRef]
- Jia, J.; Ding, J.; Liu, S.; Liao, G.; Li, J.; Duan, B.; Wang, G.; Zhang, R. Modeling the Control of COVID-19: Impact of Policy Interventions and Meteorological Factors. arXiv 2020, arXiv:2003.02985, preprint. [Google Scholar]
- Weible, C.M.; Nohrstedt, D.; Cairney, P.; Carter, D.P.; Crow, D.A.; Durnová, A.P.; Heikkila, T.; Ingold, K.; McConnell, A.; Stone, D. COVID-19 and the policy sciences: Initial reactions and perspectives. Policy Sci. 2020, 53, 225–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, Y.; Nie, Y.; Penny, M. Transmission dynamics of the COVID-19 outbreak and effectiveness of government interventions: A data-driven analysis. J. Med. Virol. 2020, 92, 645–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, Z.D.; Evans, N.G.; Phelan, A.L.; Silverman, R.D. Covid-19: Control measures must be equitable and inclusive. BMJ 2020, 368, m1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulin, J.; Sevä, I.J. Who do you trust? How trust in partial and impartial government institutions influences climate policy attitudes. Clim. Policy 2021, 21, 33–46. [Google Scholar] [CrossRef]
- He, A.J.; Ma, L. Citizen participation, perceived public service performance, and trust in government: Evidence from health policy reforms in Hong Kong. Public Perform. Manag. Rev. 2020, 1–23. [Google Scholar] [CrossRef]
- Brammer, S.; Branicki, L.; Linnenluecke, M.K. COVID-19, socialization and the future of business in society. Acad. Manag. Perspect. 2020, 34. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Alias, H.; Wong, L.P. Knowledge, attitudes, impact, and anxiety regarding COVID-19 infection among the public in China. Front. Public Health 2020, 8, 236. [Google Scholar] [CrossRef]
- Boin, A.; Rhinard, M.; Ekengren, M. Managing transboundary crises: The emergence of European Union capacity. J. Contingencies Crisis Manag. 2014, 22, 131–142. [Google Scholar] [CrossRef]
- Kapucu, N. Interagency communication networks during emergencies: Boundary spanners in multiagency coordination. Am. Rev. Public Adm. 2006, 36, 207–225. [Google Scholar] [CrossRef]
- Boin, A.; ’t Hart, P. Organising for effective emergency management: Lessons from research. Aust. J. Public Adm. 2010, 69, 357–371. [Google Scholar] [CrossRef] [Green Version]
- Lewis, G. Organizational Crisis Management: The Human Factor; Auerbach Publications: Boca Raton, FL, USA, 2006. [Google Scholar]
- Persson, T.; Parker, C.F.; Widmalm, S. Social trust, impartial administration and public confidence in EU crisis management institutions. Public Adm. 2017, 95, 97–114. [Google Scholar] [CrossRef]
- Widmalm, S.; Parker, C.F.; Persson, T. Civil Protection Cooperation in the European Union: How Trust and Administrative Culture Matter for Crisis Management; Springer: New York, NY, USA, 2019. [Google Scholar]
- Giddens, A. The Consequences of Modernity; Polity Press: Cambridge, UK, 1990. [Google Scholar]
- Kaltenthaler, K.; Anderson, C.J.; Miller, W.J. Accountability and independent central banks: Europeans and distrust of the European Central Bank. J. Common Mark. Stud. 2010, 48, 1261–1281. [Google Scholar] [CrossRef]
- Christensen, T.; Lægreid, P.; Rykkja, L.H. Organizing for crisis management: Building governance capacity and legitimacy. Public Adm. Rev. 2016, 76, 887–897. [Google Scholar] [CrossRef]
- Christensen, T.; Lægreid, P. Balancing governance capacity and legitimacy: How the Norwegian government handled the COVID-19 crisis as a high performer. Public Adm. Rev. 2020, 80, 774–779. [Google Scholar] [CrossRef]
- Stark, A.; Taylor, M. Citizen participation, community resilience and crisis-management policy. Aust. J. Political Sci. 2014, 49, 300–315. [Google Scholar] [CrossRef]
- Wu, W.N.; Chang, K.; Tso, Y.E. If only we knew what we know: Factors for mobilizing citizen participation in community-based emergency preparedness. Chin. Public Adm. Rev. 2016, 7, 77–109. [Google Scholar]
- Dückers, M.L. A multilayered psychosocial resilience framework and its implications for community-focused crisis management. J. Contingencies Crisis Manag. 2017, 25, 182–187. [Google Scholar] [CrossRef]
- Kweit, M.G.; Kweit, R.W. Citizen participation and citizen evaluation in disaster recovery. Am. Rev. Public Adm. 2004, 34, 354–373. [Google Scholar] [CrossRef]
- Frisby, B.N.; Sellnow, D.D.; Lane, D.R.; Veil, S.R.; Sellnow, T.L. Instruction in crisis situations: Targeting learning preferences and self-efficacy. Risk Manag. 2013, 15, 250–271. [Google Scholar] [CrossRef]
- Bandura, A.; Barbaranelli, C.; Caprara, G.V.; Pastorelli, C. Multifaceted impact of self-efficacy beliefs on academic functioning. Child Dev. 1996, 67, 1206–1222. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy mechanism in human agency. Am. Psychol. 1982, 37, 122–147. [Google Scholar] [CrossRef]
- Zimmerman, B.J.; Bandura, A.; Martinez-Pons, M. Self-motivation for academic attainment: The role of self-efficacy beliefs and personal goal setting. Am. Educ. Res. J. 1992, 29, 663–676. [Google Scholar] [CrossRef]
- Abdalla, I.A. Sex, sex-role, self-concepts and career decision making self-efficacy among Arab students. Soc. Behav. Pers. 1995, 23, 389–401. [Google Scholar] [CrossRef]
- Ancis, J.R.; Phillips, S.D. Academic gender bias and women’s behavioral agency self-efficacy. J. Couns. Dev. 1996, 75, 131–137. [Google Scholar] [CrossRef]
- Garavalia, L.S.; Gredler, M.E. An exploratory study of academic goal setting, achievement calibration and self-regulated learning. J. Instr. Psychol. 2002, 29, 221–230. [Google Scholar]
- Dunlap, J.C. Problem-based learning and self-efficacy: How a capstone course prepares students for a profession. Educ. Technol. Res. Dev. 2005, 53, 65–83. [Google Scholar] [CrossRef]
- Kang, J.Y.; Choi, Y.J. Effects of a psychological first aid simulated training for pregnant flood victims on disaster relief workers’ knowledge, competence, and self-efficacy. Appl. Nurs. Res. 2020, 57, 151348. [Google Scholar] [CrossRef]
- Kılıç, N.; Şimşek, N. The effects of psychological first aid training on disaster preparedness perception and self-efficacy. Nurse Educ. Today 2019, 83, 104203. [Google Scholar] [CrossRef] [PubMed]
- Peleg, K.; Bodas, M.; Shenhar, G.; Adini, B. Wisdom of (using) the crowds: Enhancing disasters preparedness through public training in Light Search and Rescue. Int. J. Disaster Risk Reduct 2018, 31, 750–757. [Google Scholar] [CrossRef]
- Ajzen, I. From intentions to actions: A theory of planned behavior. In Action Control: From Cognition to Behavior; Kuhl, J., Beckmann, J., Eds.; Springer: Heidelberg, Germany, 1985; pp. 11–39. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Reuter, T.; Ziegelmann, J.P.; Wiedemann, A.U.; Geiser, C.; Lippke, S.; Schüz, B.; Schwarzer, R. Changes in intentions, planning, and self-efficacy predict changes in behaviors: An application of latent true change modelling. J. Health Psychol. 2010, 15, 935–947. [Google Scholar] [CrossRef]
- Perkins, K.A.; Parzynski, C.; Mercincavage, M.; Conklin, C.A.; Fonte, C.A. Is self-efficacy for smoking abstinence a cause of, or a reflection on, smoking behavior change? Clin. Psychopharmacol. 2012, 20, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mileti, D.S.; Sorensen, J.H. Communication of Emergency Public Warnings: A Social Science Perspective and State-of-the-Art Assessment; ORNL-6609; Oak Ridge National Laboratory: Oak Ridge, TN, USA, 1990. [CrossRef] [Green Version]
- Mileti, D.S.; Fitzpatrick, C. Communication of public risk: Its theory and its application. Sociol. Pract. Rev. 1991, 2, 20–28. [Google Scholar]
- Kim, Y.; Lee, J.; Ham, S. The effects of narrative messages on optimistic bias in South Korea: A focus on controllability, collectivism, and risk perception in a massive fire crisis. Asian J. Commun. 2018, 28, 638–657. [Google Scholar] [CrossRef]
- Malecki, K.M.C.; Keating, J.A.; Safdar, N. Crisis communication and public perception of COVID-19 risk in the era of social media. Clin. Infect. Dis. 2020, 72, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Fischer, D.; Putzke-Hattori, J.; Fischbach, K. Crisis warning apps: Investigating the factors influencing usage and compliance with recommendations for action. In ICT and Artificial Intelligence for Crisis and Emergency Management, Proceedings of the 52nd Hawaii International Conference on System Sciences, Grand Wailea, HI, USA, 8–11 January 2019; University of Hawaii at Manoa: Honolulu, HI, USA, 2019; Available online: https://hdl.handle.net/10125/59504 (accessed on 1 June 2021).
- Parker, C.F.; Persson, T.; Widmalm, S. The effectiveness of national and EU-level civil protection systems: Evidence from 17 member states. J. Eur. Public Policy 2019, 26, 1312–1334. [Google Scholar] [CrossRef] [Green Version]
- Vung, N.N.; Choi, Y.S.; Kim, I. High resistance to Sacbrood virus disease in Apiscerana (Hymenoptera: Apidae) colonies selected for superior brood viability and hygienic behavior. Apidologie 2020, 51, 61–74. [Google Scholar] [CrossRef]
- Hozak, S.V.; Stankevych, T.V. Yelizarova, O.T.; Parats, A.N. Hygienic recommendations for saving health of children in the quarantine. Med. Sci. Ukr. 2021, 17, 93–103. [Google Scholar] [CrossRef]
- Loftus, M.J.; Guitart, C.; Tartari, E.; Stewardson, A.J.; Amer, F.; Bellissimo-Rodrigues, F.; Lee, Y.F.; Mehtar, S.; Sithole, B.L.; Pittet, D. Hand hygiene in low-and middle-income countries. Int. J. Infect. Dis. 2019, 86, 25–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mbakaya, B.C.; Lee, P.H.; Lee, R.L. Hand hygiene intervention strategies to reduce diarrhoea and respiratory infections among schoolchildren in developing countries: A systematic review. Int. J. Env. Res. Public Health 2017, 14, 371. [Google Scholar] [CrossRef] [Green Version]
- Banik, R.; Rahman, M.; Sikder, T.; Gozal, D. COVID-19 in Bangladesh: Public awareness and insufficient health facilities remain key challenges. Public Health 2020, 183, 50. [Google Scholar] [CrossRef]
- Ssemugabo, C.; Wafula, S.T.; Ndejjo, R.; Osuret, J.; Musoke, D.; Halage, A.A. Characteristics of sanitation and hygiene facilities in a slum community in Kampala, Uganda. Int. Health 2021, 13, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Dhesi, S.; Isakjee, A.; Davies, T. Public health in the Calais refugee camp: Environment, health and exclusion. Crit. Public Health 2018, 28, 140–152. [Google Scholar] [CrossRef]
- Johnson, E.J.; Hariharan, S. Public health awareness: Knowledge, attitude and behaviour of the general public on health risks during the H1N1 influenza pandemic. J. Public Health 2017, 25, 333–337. [Google Scholar] [CrossRef]
- Checchi, F.; Warsame, A.; Treacy-Wong, V.; Polonsky, J.; Van Ommeren, M.; Prudhon, C. Public health information in crisis-affected populations: A review of methods and their use for advocacy and action. Lancet 2017, 390, 2297–2313. [Google Scholar] [CrossRef]
- Kumwenda, S. Challenges to hygiene improvement in developing countries. Relev. Hyg. Health Dev. Ctries. 2019, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Heuvelink, A.E.; Valkenburgh, S.M.; Tilburg, J.J.H.C.; Van Heerwaarden, C.; Zwartkruis-Nahuis, J.T.M.; De Boer, E. Public farms: Hygiene and zoonotic agents. Epidemiol. Infect. 2007, 135, 1174–1183. [Google Scholar] [CrossRef] [PubMed]
- Michael, J.; Iqbal, Q.; Haider, S.; Khalid, A.; Haque, N.; Ishaq, R.; Saleem, F.; Hassali, M.A.; Bashaar, M. Knowledge and practice of adolescent females about menstruation and menstruation hygiene visiting a public healthcare institute of Quetta, Pakistan. BMC Women’s Health 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Muoki, M.A.; Tumuti, D.S.; Rombo, D. Nutrition and public hygiene among children under five years of age in Mukuru slums of Makadara Division, Nairobi. East Afr. Med. J. 2008, 85, 386–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jefferson, C.D.; Drake, C.L.; Scofield, H.M.; Myers, E.; McClure, T.; Roehrs, T.; Roth, T. Sleep hygiene practices in a population-based sample of insomniacs. Sleep 2005, 28, 611–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sood, A.; Amre, D.; Midha, V.; Sharma, S.; Sood, N.; Thara, A.; Bansal, M.; Juyal, G.; Thelma, B.K.; Seidman, E. Low hygiene and exposure to infections may be associated with increased risk for ulcerative colitis in a North Indian population. Ann. Gastroenterol. Q. Publ. Hell. Soc. Gastroenterol. 2014, 27, 219. [Google Scholar]
- Dong, X.; Simon, M.A.; Mosqueda, L.; Evans, D.A. The prevalence of elder self-neglect in a community-dwelling population: Hoarding, hygiene, and environmental hazards. J. Aging Health 2012, 24, 507–524. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Huang, L.Y.; Zhang, Y.; Ni, S. Effects of intuition and deliberation on escape judgment and decision-making under different complexities of crisis situations. Saf. Sci. 2016, 89, 106–113. [Google Scholar] [CrossRef]
- Lu, Y.; Huang, Y.H.C. Getting emotional: An emotion-cognition dual-factor model of crisis communication. Public Relat. Rev. 2018, 44, 98–107. [Google Scholar] [CrossRef]
- Coombs, W.T.; Holladay, S.J.; Claeys, A.S. Debunking the myth of denial’s effectiveness in crisis communication: Context matters. J. Commun. Manag. 2016, 20, 381–395. [Google Scholar] [CrossRef]
- Christensen, D.A.; Aars, J. Countering fear: Democratic states’ ability to ease citizens’ fear of terrorism. In Societal Security and Crisis Management; Lægreid, P., Rykkja, L., Eds.; Palgrave Macmillan: Cham, Switzerland; London, UK, 2019; pp. 285–302. [Google Scholar]
- Hillebrand, K. State surveillance: Exploiting fear during the pandemic crisis? SSRN 2020, 30. [Google Scholar] [CrossRef]
- Drennan, L.T.; McConnell, A.; Stark, A. Risk and Crisis Management in the Public Sector, 2nd ed.; Routledge: London, UK, 2015. [Google Scholar]
- Regester, M.; Larkin, J. Risk Issues and Crisis Management in Public Relations: A Casebook of Best Practice, 4th ed.; Kogan Page Publishers: London, UK, 2008. [Google Scholar]
- Carayannopoulos, G. Whole of government: The solution to managing crises? Aust. J. Public Adm. 2017, 76, 251–265. [Google Scholar] [CrossRef]
- Altiparmakis, A.; Bojar, A.; Brouard, S.; Foucault, M.; Kriesi, H.; Nadeau, R. Pandemic politics: Policy evaluations of government responses to COVID-19. West Eur. Polit. 2021, 44, 1–21. [Google Scholar] [CrossRef]
- Abate, M.; Christidis, P.; Purwanto, A.J. Government support to airlines in the aftermath of the COVID-19 pandemic. J. Air Transp. Manag. 2020, 89, 101931. [Google Scholar] [CrossRef]
- Mintrom, M.; O’Connor, R. The importance of policy narrative: Effective government responses to Covid-19. Policy Des. Pract. 2020, 3, 205–227. [Google Scholar]
- Mahmud, A.; Ding, D.; Hasan, M.M. Corporate social responsibility: Business responses to Coronavirus (COVID-19) pandemic. SAGE Open 2021, 11, 2158244020988710. [Google Scholar] [CrossRef]
- Chen, Z.; Hang, H. Corporate social responsibility in times of need: Community support during the COVID-19 pandemics. Tour Manag. 2021, 87, 104364. [Google Scholar] [CrossRef]
- García-Sánchez, I.M.; García-Sánchez, A. Corporate social responsibility during COVID-19 pandemic. J. Open Innov. Technol. Mark. Complex. 2020, 6, 126. [Google Scholar] [CrossRef]
- Chen, S.H.; Dai, J.M.; Hu, Q.; Chen, H.; Wang, Y.; Gao, J.L.; Zhang, P.P.; Fu, H. Public anxiety and its influencing factors in the initial outbreak of COVID-19. Fudan Univ. J. Med. Sci. 2020, 47. [Google Scholar] [CrossRef]
- Goodwin, R.; Wiwattanapantuwong, J.; Tuicomepee, A.; Suttiwan, P.; Watakakosol, R. Anxiety and public responses to covid-19: Early data from Thailand. J. Psychiatr. Res. 2020, 129, 118–121. [Google Scholar] [CrossRef]
- Wong, L.P.; Hung, C.C.; Alias, H.; Lee, T.S.H. Investigation into public anxiety symptoms and preventive measures during the COVID-19 outbreak in Taiwan. BMC Psychiatry 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Ao, Y.; Zhu, H.; Meng, F.; Wang, Y.; Ye, G.; Yang, L.; Dong, N.; Martek, L. The impact of social support on public anxiety amidst the COVID-19 pandemic in China. Int. J. Env. Res. Public Health 2020, 17, 9097. [Google Scholar] [CrossRef] [PubMed]
- Gartzia, L.; Ryan, M.K.; Balluerka, N.; Aritzeta, A. Think crisis–think female: Further evidence. Eur. J. Work. Organ Psychol. 2012, 21, 603–628. [Google Scholar] [CrossRef]
- O’Connor, R.E.; Bord, R.J.; Fisher, A. Risk perceptions, general environmental beliefs, and willingness to address climate change. Risk Anal. 1999, 19, 461–471. [Google Scholar] [CrossRef]
- Ding, Y.; Du, X.; Li, Q.; Zhang, M.; Zhang, Q.; Tan, X.; Liu, Q. Risk perception of coronavirus disease 2019 (COVID-19) and its related factors among college students in China during quarantine. PLoS ONE 2020, 15, 0237626. [Google Scholar] [CrossRef]
- Calderón-Larrañaga, A.; Dekhtyar, S.; Vetrano, D.L.; Bellander, T.; Fratiglioni, L. COVID-19: Risk accumulation among biologically and socially vulnerable older populations. Ageing Res. Rev. 2020, 63, 101149. [Google Scholar] [CrossRef] [PubMed]
- Tian, F.; Li, H.; Tian, S.; Yang, J.; Shao, J.; Tian, C. Psychological symptoms of ordinary Chinese citizens based on SCL-90 during the level I emergency response to COVID-19. Psychiatry Res. 2020, 288, 112992. [Google Scholar] [CrossRef] [PubMed]
- Lin, Q.; Zhao, S.; Gao, D.; Lou, Y.; Yang, S.; Musa, S.S.; Wang, M.H.; Cai, Y.; Wang, W.; Yang, L.; et al. A conceptual model for the Coronavirus disease 2019 (COVID-19) outbreak in Wuhan, China with individual reaction and governmental action. Int. J. Infect. Dis. 2020, 93, 211–216. [Google Scholar] [CrossRef]
- Sibley, C.G.; Greaves, L.M.; Satherley, N.; Wilson, M.S.; Overall, N.C.; Lee, C.H.J.; Milojev, P.; Bulbulia, J.; Orborne, D.; Milfont, T.L.; et al. Effects of the COVID-19 pandemic and nationwide lockdown on trust, attitudes toward government, and wellbeing. Am. Psychol. 2020, 75, 618–630. [Google Scholar] [CrossRef] [PubMed]
- Gostin, L.O.; Wiley, L.F. Governmental public health powers during the COVID-19 pandemic: Stay-at-home orders, business closures, and travel restrictions. JAMA 2020, 323, 2137–2138. [Google Scholar] [CrossRef] [PubMed]
- Blocken, B.; Malizia, F.; van Druenen, T.; Marchal, T. Towards Aerodynamically Equivalent COVID-19 1.5 m Social Distancing for Walking and Running. Available online: http://www.urbanphysics.net/COVID19_Aero_Paper.pdf (accessed on 21 April 2020).
- Singh, R.; Adhikari, R. Age-structured impact of social distancing on the COVID-19 epidemic in India. arXiv 2020, arXiv:2003.12055. preprint. [Google Scholar]
- Thunström, L.; Newbold, S.C.; Finnoff, D.; Ashworth, M.; Shogren, J.F. The benefits and costs of using social distancing to flatten the curve for COVID-19. J. Benefit Cost Anal. 2020, 11, 179–195. [Google Scholar] [CrossRef]
- Feng, S.; Shen, C.; Xia, N.; Song, W.; Fan, M.; Cowling, B.J. Rational use of face masks in the COVID-19 pandemic. Lancet Respir. Med. 2020, 8, 434–436. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Schmid, M.B.; Czypionka, T.; Bassler, D.; Gruer, L. Face masks for the public during the COVID-19 crisis. BMJ 2020, 369, m1435. [Google Scholar] [CrossRef] [Green Version]
- Eikenberry, S.E.; Mancuso, M.; Iboi, E.; Phan, T.; Eikenberry, K.; Kuang, Y.; Kostelich, E.; Gumel, A.B. To mask or not to mask: Modeling the potential for face mask use by the general public to curtail the COVID-19 pandemic. Infect. Dis. Model. 2020, 5, 293–308. [Google Scholar] [CrossRef]
- Iyengar, K.; Mabrouk, A.; Jain, V.K.; Venkatesan, A.; Vaishya, R. Learning opportunities from COVID-19 and future effects on health care system. Diabetes Metab. Syndr. 2020, 14, 943–946. [Google Scholar] [CrossRef]
- Venkateswaran, J.; Damani, O. Effectiveness of testing, tracing, social distancing and hygiene in tackling Covid-19 in India: A system dynamics model. arXiv 2020, arXiv:2004.08859. preprint. [Google Scholar]
- Gwenzi, W. Leaving no stone unturned in light of the COVID-19 faecal-oral hypothesis? A water, sanitation and hygiene (WASH) perspective targeting low-income countries. Sci. Total. Environ. 2021, 753, 141751. [Google Scholar] [CrossRef]
- Abdoul-Azize, H.T.; El Gamil, R. Social protection as a key tool in crisis management: Learnt lessons from the COVID-19 pandemic. Glob. Soc. Welf. 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Cho, W.; Kim, M.H.; Hur, J.Y. Public health emergency and crisis management: Case study of SARS-CoV-2 outbreak. Int. J. Environ. Res. Public Health 2020, 17, 3984. [Google Scholar] [CrossRef]
- Huang, J.; Liu, F.; Teng, Z.; Chen, J.; Zhao, J.; Wang, X.; Wu, Y.; Xiao, J.; Wang, Y.; Wu, R. Public behavior change, perceptions, depression, and anxiety in relation to the COVID-19 outbreak. Open Forum Infect. Dis. 2020, 7, ofaa273. [Google Scholar] [CrossRef] [PubMed]
- Roy, D.; Tripathy, S.; Kar, S.K.; Sharma, N.; Verma, S.K.; Kaushal, V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J. Psychiatr. 2020, 51, 102083. [Google Scholar]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Swami, V.; Barron, D. Analytic Thinking, Rejection of Coronavirus (COVID-19) Conspiracy Theories, and Compliance with Mandated Social-Distancing: Direct and Indirect Relationships in a Nationally Representative Sample of Adults in the United Kingdom. Available online: osf.io/nmx9w (accessed on 1 June 2021).
- BBC. South Korea Church Coronavirus Cluster Causes Alarm. Available online: https://www.bbc.com/news/world-asia-53803011 (accessed on 2 February 2020).
- Lancet, T. Redefining vulnerability in the era of COVID-19. Lancet 2020, 395, 1089. [Google Scholar] [CrossRef]
- Chen, Y.; Klein, S.L.; Garibaldi, B.T.; Li, H.; Wu, C.; Osevala, N.M.; Li, T.; Pawele, J.B.M.G.; Leng, S.X. Aging in COVID-19: Vulnerability, immunity and intervention. Ageing Res. Rev. 2020, 65, 101205. [Google Scholar] [CrossRef] [PubMed]
- Napier, A.D. Rethinking vulnerability through Covid-19. Anthropol. Today 2020, 36, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, M.; Pullano, G.; Pinotti, F.; Valdano, E.; Poletto, C.; Boëlle, P.Y.; D’Ortenzio, E.; Yazdanpanah, P.Y.; Eholie, S.P.; Pharm, M.A.; et al. Preparedness and vulnerability of African countries against importations of COVID-19: A modelling study. Lancet 2020, 395, 871–877. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.; Zhang, J.; Meadows, M.E.; Liu, Y.; Hua, T.; Fu, B. A systematic approach is needed to contain COVID-19 globally. Sci. Bull. 2020, 65, 876. [Google Scholar] [CrossRef] [Green Version]
- Špaček, D. COVID-19–National Government Approach in the Czech Republic. Good Public Gov. Glob. Pandemic 2020, 1, 259–268. [Google Scholar]
- Ang, Y.Y. When COVID-19 meets centralized, personalized power. Nat. Hum. Behav. 2020, 4, 445–447. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Min, C.; Zhang, W.; Wang, G.; Ma, X.; Evans, R. Unpacking the black box: How to promote citizen engagement through government social media during the COVID-19 crisis. Comput. Hum. Behav. 2020, 110, 106380. [Google Scholar] [CrossRef]
- Gao, X.; Yu, J. Public governance mechanism in the prevention and control of the COVID-19: Information, decision-making and execution. J. Chin. Gov. 2020, 5, 178–197. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, R.; Kalogeropoulos, A.; Nielsen, R.K. Trust in UK government and news media COVID-19 information down, concerns over misinformation from government and politicians up. Reuters Inst. Study Journal. 2020, 1–26. [Google Scholar]
- Hornuss, D.; Lange, B.; Schroeter, N.; Rieg, S.; Kern, W.V.; Wagner, D. Anosmia in COVID-19 patients. Clin. Microbiol. Infect. 2020, 26, 1426. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; Salzano, G.; Deiana, G.; De Riu, G. Anosmia and ageusia: Common findings in COVID-19 patients. Laryngoscope 2020, 130, 1787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, T.; Lu, H.; Zhang, W. Clinical observation and management of COVID-19 patients. Emerg. Microbes Infect. 2020, 9, 687–690. [Google Scholar] [CrossRef]
- Vaira, L.A.; Salzano, G.; Fois, A.G.; Piombino, P.; De Riu, G. Potential pathogenesis of ageusia and anosmia in COVID-19 patients. Int. Forum. Allergy Rhinol. 2020, 10, 1103–1104. [Google Scholar] [CrossRef]
- Sell, T.K.; Hosangadi, D.; Trotochaud, M. Misinformation and the US Ebola communication crisis: Analyzing the veracity and content of social media messages related to a fear-inducing infectious disease outbreak. BMC Public Health 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Asmundson, G.J.; Taylor, S. Coronaphobia: Fear and the 2019-nCoV outbreak. J. Anxiety Disord 2020, 70, 102196. [Google Scholar] [CrossRef]
- Oh, S.H.; Lee, S.Y.; Han, C. The effects of social media use on preventive behaviors during infectious disease outbreaks: The mediating role of self-relevant emotions and public risk perception. Health Commun. 2021, 36, 972–981. [Google Scholar] [CrossRef]
- Fardin, M.A. COVID-19 and anxiety: A review of psychological impacts of infectious disease outbreaks. Arch. Clin. Infect. Dis. 2020, 15. [Google Scholar] [CrossRef] [Green Version]
- Hoppe, T. “Spanish flu”: When infectious disease names blur origins and stigmatize those infected. Am. J. Public Health 2018, 108, 1462–1464. [Google Scholar] [CrossRef] [PubMed]
- Alfaro, L.; Faia, E.; Lamersdorf, N.; Saidi, F. Social Interactions in Pandemics: Fear, Altruism, and Reciprocity; No. w27134; National Bureau of Economic Research: Cambridge, MA, USA, 2020. [Google Scholar]
Figure 1.
Attitudes toward crisis management support mechanisms.

Figure 2.
Mean efficacy scores by sociodemographic variables.


{kind=link}
{kind=link}
Table 1.
Descriptive statistics of survey participants (N = 620).
| Characteristics | n (%) |
|---|---|
| Sex | |
| Male | 321 (51.8) |
| Female | 299 (48.2) |
| Age | |
| 20–29 | 112 (18.1) |
| 30–39 | 109 (17.6) |
| 40–49 50–59 | 133 (21.5) 146 (23.5) |
| ≥60 | 120 (19.4) |
| Place of residence | |
| Greater capital region | 297 (47.9) |
| Gyeongsang-do | 155 (25) |
| Jeolla-do or Jeju-do | 80 (12.9) |
| Chungcheong-do or Gangwon-do | 88 (14.2) |
| Education | |
| High school | 124 (20) |
| College | 100 (16.1) |
| Four-year university | 343 (55.3) |
| Graduate school | 53 (8.5) |
| Employment | |
| Employed full-time | 306 (49.4) |
| Employed part-time | 34 (5.5) |
| Company owner or self-employed | 72 (11.6) |
| Students | 44 (7.1) |
| Homemakers | 86 (13.9) |
| Unemployed | 52 (8.4) |
| Other | 26 (4.2) |
| Monthly household income | |
| 2 million KWR | 51 (8.2) |
| 2–4 million KRW | 201 (32.4) |
| 4–6 million KRW | 182 (29.4) |
| 6–8 million KRW | 102 (16.5) |
| 8–10 million | 54 (8.7) |
| ≥10 million KRW | 30 (4.8) |
Table 2.
Concepts, measures, and reliability.
| Concept | Questions | Reliability |
|---|---|---|
| Public hygiene environment | Q1 South Korea has an environment that allows citizens to wash their hands as necessary, without any particular restrictions. Q2 South Korea has an environment that allows citizens to care for their hygiene as necessary. | 0.902 |
| Public hygiene information | Q1 South Korea provides information for citizens’ hygiene as necessary. Q2 South Korea enables easy access to hygiene information for citizens. | 0.889 |
| Public hygiene facilities | Q1 The overall quality of hygiene in public facilities in South Korea is excellent. Q2 The overall quality of hygiene in civilian facilities in South Korea is excellent. | 0.807 |
| Public hygiene of the population | Q1 The South Korean population has high overall awareness of public hygiene. Q2 The South Korean population has a high overall rate of performance of public hygiene. | 0.917 |
| Public hygiene behaviors | Q1 I am practicing social distancing to overcome the COVID-19 crisis. Q2 I am restricting outdoor activities and staying at home to overcome the COVID-19 crisis. Q3 I always wear a mask during outdoor activities to overcome the COVID-19 crisis. Q4 I wash my hands regularly to overcome the COVID-19 crisis. Q5 I have purchased masks to overcome the COVID-19 crisis. Q6 I have purchased soap to overcome the COVID-19 crisis. Q7 I have purchased hand disinfectant to overcome the COVID-19 crisis. Q8 I have purchased disinfectant to overcome the COVID-19 crisis. | 0.870 |
| Central government support | Q1 The current state of the COVID-19 situation reported by the central government (information about confirmed cases, etc.) is helping to overcome COVID-19. Q2 Information provided by the central government about behaviors to overcome COVID-19 (e.g., wearing a mask, disinfecting hands, coughing etiquette, etc.) is helping to overcome COVID-19. Q3 The central government is actively providing citizens with information to overcome COVID-19. Q4 The central government is performing infection prevention activities to overcome COVID-19. Q5 The central government is actively managing infected persons to overcome COVID-19. Q6 The central government is actively managing potential infections to overcome COVID-19. Q7 The central government is making efforts to alleviate economic damages suffered by citizens due to COVID-19. | 0.944 |
| Local government support | Q1 The current state of the COVID-19 situation reported by the local government (information about confirmed cases, etc.) is helping to overcome COVID-19. Q2 Information provided by the local government about behaviors to overcome COVID-19 (e.g., wearing a mask, disinfecting hands, coughing etiquette, etc.) is helping to overcome COVID-19. Q3 The local government is actively providing citizens with information to overcome COVID-19. Q4 The local government is performing infection prevention activities to overcome COVID-19. Q5 The local government is actively managing infected persons to overcome COVID-19. Q6 The local government is actively managing potential infections to overcome COVID-19. Q7 The local government is making efforts to alleviate economic damages suffered by citizens due to COVID-19. | 0.953 |
| Civilian support | Q1 The civilian sector is actively sharing information to overcome COVID-19. Q2 The civilian sector is actively participating in infection prevention activities to overcome COVID-19. Q3 The civilian sector is actively managing infected persons (self-isolation) to overcome COVID-19. Q4 The civilian sector is actively managing potential infections (self-isolation) to overcome COVID-19. Q5 The civilian sector is making efforts to alleviate economic damages suffered by citizens due to COVID-19 (e.g., reducing rent, encouraging purchase of small business owners’ or farmers’ goods). | 0.897 |
| Anxiety | Q1 Since COVID-19, I am more sensitive and I do not feel at rest. Q2 Since COVID-19, I feel more anxious. Q3 Since COVID-19, I get surprised for no reason. Q4 Since COVID-19, I feel more afraid. Q5 Since COVID-19, my heart starts beating rapidly. Q6 Since COVID-19, I feel tense. Q7 Since COVID-19, I sometimes feel full of fear. Q8 Since COVID-19, I am nervous and cannot stay still. Q9 Since COVID-19, even familiar things feel new or unrealistic. Q10 Since COVID-19, I feel a sense of urgency and restlessness about everything. | 0.953 |
| Efficacy | Q1 If the government works hard, we can be safe from the threat of COVID-19. Q2 If the medical staff work hard, we can be safe from the threat of COVID-19. Q3 If the population works hard, we can be safe from the threat of COVID-19. Q4 If I work hard, I can be safe from the threat of COVID-19. | 0.890 |
COVID-19: Coronavirus disease 2019.
Table 3.
Correlational analysis of crisis management effectiveness.
| Efficacy | Public Hygiene Behaviors | Public Hygiene Environment | Public Hygiene Information | Public Hygiene Facilities | Public Hygiene of the Population | Government Support | Civilian Support | Anxiety | |
|---|---|---|---|---|---|---|---|---|---|
| Efficacy | - | 0.128 ** | 0.231 ** | 0.220 ** | 0.182 ** | 0.213 ** | 0.482 ** | 0.327** | −0.228 ** |
| Public hygiene behaviors | - | - | 0.231 ** | 0.301 ** | 0.204 ** | 0.230 ** | 0.112 ** | 0.186** | 0.039 |
| Public hygiene environment | - | - | - | 0.682 ** | 0.600 ** | 0.565 ** | 0.261 ** | 0.289** | −0.050 |
| Public hygiene information | - | - | - | - | 0.610 ** | 0.589 ** | 0.359 ** | 0.354** | −0.023 |
| Public hygiene facilities | - | - | - | - | - | 0.703 ** | 0.367 ** | 0.404** | −0.039 |
| Public hygiene of the population | - | - | - | - | - | - | 0.374 ** | 0.472** | −0.036 |
| Government support | - | - | - | - | - | - | - | 0.575** | −0.2400 ** |
| Civilian support | - | - | - | - | - | - | - | - | −0.055 |
Note: ** p < 0.01.
Table 4.
Multiple regression analysis for level of efficacy.
| B | SE | Beta | t | p | |
|---|---|---|---|---|---|
| (Efficacy) | 1.682 | 0.245 | 6.875 | <0.001 | |
| Sex | −0.139 ** | 0.054 | −0.092 | −2.582 | 0.010 |
| Age | −0.003 | 0.002 | −0.049 | −1.347 | 0.178 |
| Income | 0.000 | 0.000 | 0.039 | 1.096 | 0.274 |
| Education level | −0.083 ** | 0.030 | −0.100 | −2.810 | 0.005 |
| Central government support | 0.465 *** | 0.057 | 0.433 | 8.191 | <0.001 |
| Local government support | 0.024 | 0.055 | 0.023 | 0.441 | 0.659 |
| Civilian support | 0.084 | 0.050 | 0.081 | 1.687 | 0.092 |
| Public hygiene behaviors | 0.086 * | 0.044 | 0.074 | 1.981 | 0.048 |
| Public hygiene environment | 0.159 *** | 0.049 | 0.165 | 3.253 | 0.001 |
| Public hygiene information | −0.045 | 0.052 | −0.046 | −0.874 | 0.383 |
| Public hygiene facilities | −0.084 | 0.052 | −0.087 | −1.611 | 0.108 |
| Public hygiene of the population | −0.016 | 0.050 | −0.017 | −0.316 | 0.752 |
Note: * p < 0.05; ** p < 0.01; *** p < 0.001. B: regression coefficient; SE: standard error of the mean. F-value 19.019 *** R2/Adjusted R2 0.273/0.259.
Table 5.
Multiple regression analysis for level of anxiety.
| B | SE | Beta | t | p | |
|---|---|---|---|---|---|
| (Anxiety) | 3.018 | 0.321 | 9.406 | <0.001 | |
| Sex | 0.028 | 0.068 | 0.017 | 0.412 | 0.680 |
| Age | −0.003 | 0.003 | −0.043 | −1.073 | 0.284 |
| Income | 0.000 | 0.000 | −0.005 | −0.128 | 0.898 |
| Education level | 0.008 | 0.038 | 0.008 | 0.204 | 0.838 |
| Central government support | −0.326 *** | 0.076 | −0.268 | −4.309 | <0.001 |
| Local government support | 0.023 | 0.069 | 0.020 | 0.337 | 0.736 |
| Civilian support | 0.142 * | 0.063 | 0.120 | 2.244 | 0.025 |
| Public hygiene behaviors | 0.073 | 0.055 | 0.055 | 1.312 | 0.190 |
| Public hygiene environment | −0.060 | 0.062 | −0.055 | −0.955 | 0.340 |
| Public hygiene information | 0.075 | 0.066 | 0.068 | 1.143 | 0.253 |
| Public hygiene facilities | 0.006 | 0.066 | 0.005 | 0.086 | 0.931 |
| Public hygiene of the population | 0.011 | 0.063 | 0.011 | 0.180 | 0.857 |
| Efficacy | −0.178 *** | 0.051 | −0.158 | −3.475 | 0.001 |
Note: * p < 0.05; *** p < 0.001. B: regression coefficient; SE: standard error of the mean. F-value 4.903 *** R2/Adjusted R2 0.095/0.076.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lee, J.-E.; Kwon, S.-A. A Study on the Public’s Crisis Management Efficacy and Anxiety in a Pandemic Situation—Focusing on the COVID-19 Pandemic in South Korea. Sustainability 2021, 13, 8393. https://doi.org/10.3390/su13158393
AMA Style
Lee J-E, Kwon S-A. A Study on the Public’s Crisis Management Efficacy and Anxiety in a Pandemic Situation—Focusing on the COVID-19 Pandemic in South Korea. Sustainability. 2021; 13(15):8393. https://doi.org/10.3390/su13158393
Chicago/Turabian StyleLee, Jae-Eun, and Seol-A Kwon. 2021. "A Study on the Public’s Crisis Management Efficacy and Anxiety in a Pandemic Situation—Focusing on the COVID-19 Pandemic in South Korea" Sustainability 13, no. 15: 8393. https://doi.org/10.3390/su13158393
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.