
Impact of COVID-19 on Tuberculosis Case Detection and Treatment Outcomes in Sierra Leone

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Population
2.2. Data Collection, Definitions and Clinic Procedures
2.3. Reconfiguration of TB Service Delivery in Sierra Leone during the COVID-19 Pandemic
2.4. Key Time Points and Periods
2.5. Research Questions
- What was the impact of the COVID-19 pandemic on TB case detection, i.e., referrals for TB testing and laboratory-confirmed TB case notifications at the Chest Clinic at Connaught Hospital in Freetown, Sierra Leone?
- How did TB treatment outcomes compare between patients using self-administration of anti-TB medications at home during April to June of 2020 (intra-COVID-19 period), versus patients using clinic-based DOT during April to June of 2019 (baseline)?
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
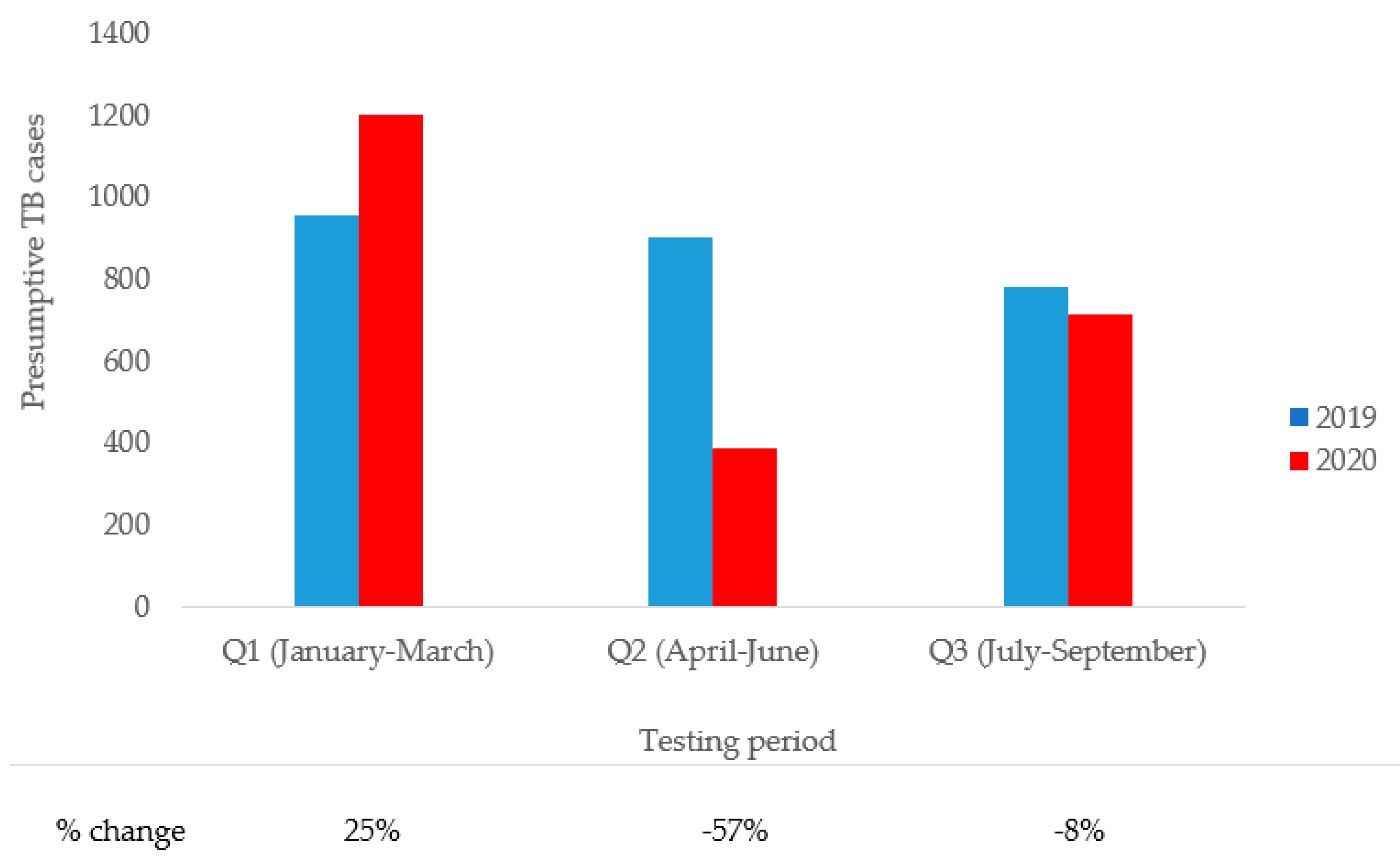
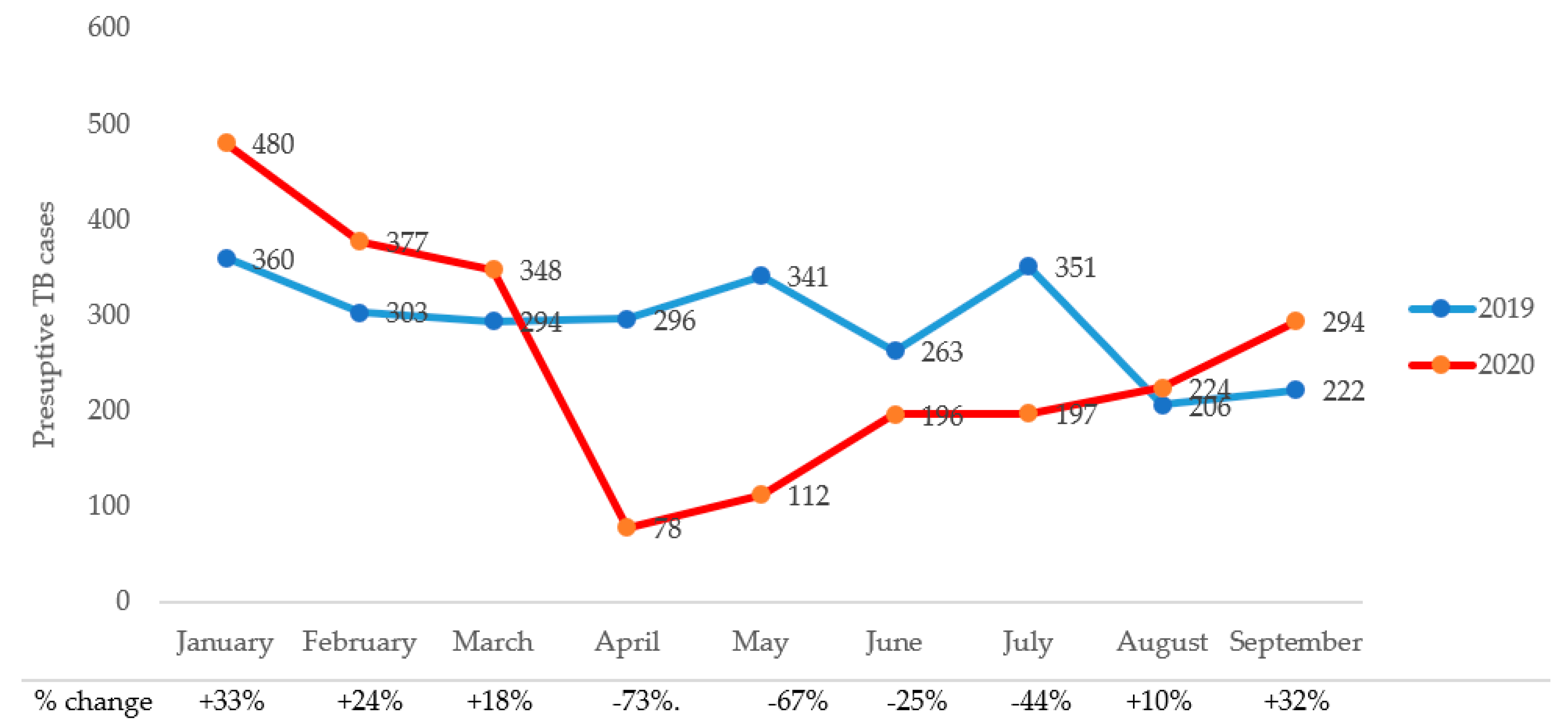
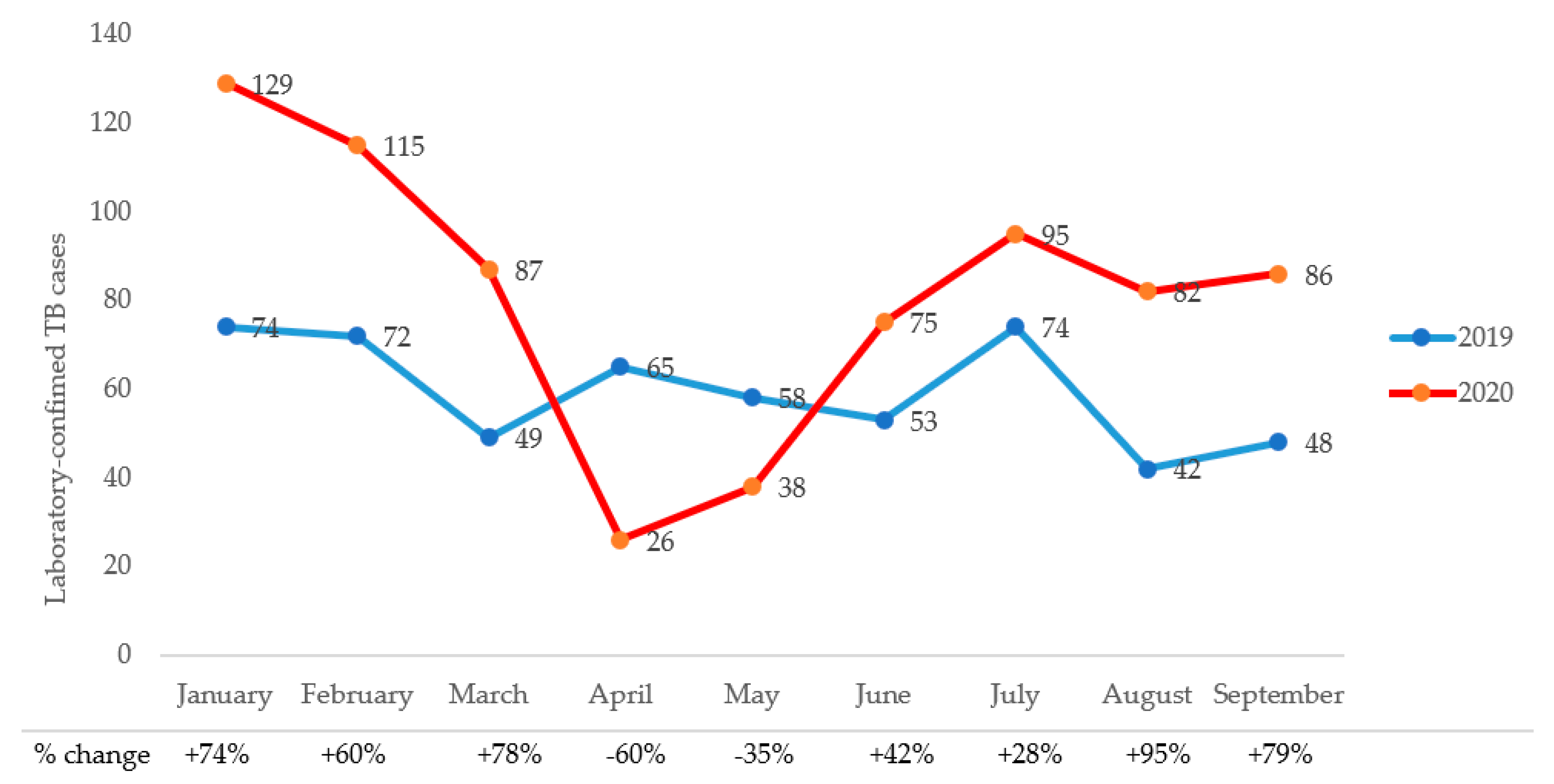
3.1. Comparison of Presumptive and Laboratory-Confirmed TB Cases during the Pre- and Intra-COVID-19 Periods
3.2. Comparison TB Treatment Outcomes during the Pre- and Intra-COVID-19 Periods
3.3. Predictors of TB Treatment Success during the Pre- and Intra-COVID-19 Periods
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int/ (accessed on 10 June 2020).
- Thornton, J. COVID-19: Africa’s case numbers are rising rapidly, WHO warns. BMJ 2020, 369, m2394. [Google Scholar] [CrossRef]
- Lawal, Y. Africa’s low COVID-19 mortality rate: A paradox? Int. J. Infect. Dis. 2021, 102, 118–122. [Google Scholar] [CrossRef]
- Mwananyanda, L.; Gill, C.J.; MacLeod, W.; Kwenda, G.; Pieciak, R.; Mupila, Z.; Lapidot, R.; Mupeta, F.; Forman, L.; Ziko, L.; et al. COVID-19 deaths in Africa: Prospective systematic postmortem surveillance study. BMJ 2021, 372, n334. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.; Hansen, K.S.; Kiragga, A.N.; Kambugu, A.; Kissa, J.; Mbonye, A.K. Predicting the Impact of COVID-19 and the Potential Impact of the Public Health Response on Disease Burden in Uganda. Am. J. Trop. Med. Hyg. 2020, 103, 1191–1197. [Google Scholar] [CrossRef] [PubMed]
- Shrock, E.; Fujimura, E.; Kula, T.; Timms, R.T.; Lee, I.-H.; Leng, Y.; Robinson, M.L.; Sie, B.M.; Li, M.Z.; Chen, Y.; et al. Viral epitope profiling of COVID-19 patients reveals cross-reactivity and correlates of severity. Science 2020, 370, eabd4250. [Google Scholar] [CrossRef] [PubMed]
- Iesa, M.A.M.; Osman, M.E.M.; Hassan, M.A.; Dirar, A.I.A.; Abuzeid, N.; Mancuso, J.J.; Pandey, R.; Mohammed, A.A.; Borad, M.J.; Babiker, H.M.; et al. SARS-CoV-2 and Plasmodium falciparum common immunodominant regions may explain low COVID-19 incidence in the malaria-endemic belt. New Microbes New Infect. 2020, 38, 100817. [Google Scholar] [CrossRef]
- Adepoju, P. Tuberculosis and HIV responses threatened by COVID-19. Lancet HIV 2020, 7, e319–e320. [Google Scholar] [CrossRef]
- McQuaid, C.F.; Vassall, A.; Cohen, T.; Fiekert, K.; COVID/TB Modelling Working Group; White, R.G. The impact of COVID-19 on TB: A review of the data. Int. J. Tuberc. Lung Dis. 2021, 25, 436–446. [Google Scholar] [CrossRef]
- World Health Organization. Global Tuberculosis Report 2020; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/336069/9789240013131-eng.pdf (accessed on 30 March 2021).
- World Health Organization. Impact of the COVID-19 Pandemic on TB Detection and Mortality in 2020; World Health Organization: Geneva, Switzerland, 2020; Available online: https://cdn.who.int/media/docs/default-source/hq-tuberculosis/impact-of-the-covid-19-pandemic-on-tb-detection-and-mortality-in-2020.pdf?sfvrsn=3fdd251c_16&download=true (accessed on 6 June 2021).
- The Global Fund. Audit Report—Global Fund Grants to the Republic of Sierra Leone, 2019. Available online: https://www.theglobalfund.org/media/8204/oig_gf-oig-19-001_report_en.pdf (accessed on 6 June 2021).
- World Health Organization. Definitions and Reporting Framework for Tuberculosis 2013 Revision (Updated December 2014). Available online: https://apps.who.int/iris/bitstream/handle/10665/79199/9789241505345_eng.pdf;jsessionid=6D09C47DEA7798F96DC37FA635517FDD?sequence=1 (accessed on 17 June 2021).
- Odume, B.; Falokun, V.; Chukwuogo, O.; Ogbudebe, C.; Useni, S.; Nwokoye, N.; Aniwada, E.; Faleye, B.O.; Okekearu, I.; Nongo, D.; et al. Impact of COVID-19 on TB active case finding in Nigeria. Public Health Action 2020, 10, 157–162. [Google Scholar] [CrossRef]
- Beyne, N.W.; Sitota, A.L.; Tegegn, B.; Bobobsha, K. The impact of COVID-19 on the tuberculosis control activities in Addis Ababa. Pan Afr. Med. J. 2021, 38, 243. [Google Scholar] [CrossRef]
- Thekkur, P.; Tweya, H.; Phiri, S.; Mpunga, J.; Kalua, T.; Kumar, A.; Satyanarayana, S.; Shewade, H.; Khogali, M.; Zachariah, R.; et al. Assessing the Impact of COVID-19 on TB and HIV Programme Services in Selected Health Facilities in Lilongwe, Malawi: Operational Research in Real Time. Trop. Med. Infect. Dis. 2021, 6, 81. [Google Scholar] [CrossRef]
- Thekkur, P.; Takarinda, K.; Timire, C.; Sandy, C.; Apollo, T.; Kumar, A.; Satyanarayana, S.; Shewade, H.; Khogali, M.; Zachariah, R.; et al. Operational Research to Assess the Real-Time Impact of COVID-19 on TB and HIV Services: The Experience and Response from Health Facilities in Harare, Zimbabwe. Trop. Med. Infect. Dis. 2021, 6, 94. [Google Scholar] [CrossRef]
- Mbithi, I.; Thekkur, P.; Chakaya, J.M.; Onyango, E.; Owiti, P.; Njeri, N.C.; Kumar, A.M.V.; Satyanarayana, S.; Shewade, H.D.; Khogali, M.; et al. Assessing the Real-Time Impact of COVID-19 on TB and HIV Services: The Experi-ence and Response from Selected Health Facilities in Nairobi, Kenya. Trop. Med. Infect. Dis. 2021, 6, 74. [Google Scholar] [CrossRef]
- Frost, I.; Craig, J.; Osena, G.; Hauck, S.; Kalanxhi, E.; Schueller, E.; Gatalo, O.; Yang, Y.; Tseng, K.K.; Lin, G.; et al. Modelling COVID-19 transmission in Africa: Countrywise projections of total and severe infections under different lockdown scenarios. BMJ Open 2021, 11, e044149. [Google Scholar] [CrossRef]
- Seidu, A.-A. Mixed effects analysis of factors associated with barriers to accessing healthcare among women in sub-Saharan Africa: Insights from demographic and health surveys. PLoS ONE 2020, 15, e0241409. [Google Scholar] [CrossRef]
- Ahinkorah, B.O.; Budu, E.; Seidu, A.-A.; Agbaglo, E.; Adu, C.; Ameyaw, E.K.; Ampomah, I.G.; Archer, A.G.; Kissah-Korsah, K.; Yaya, S. Barriers to healthcare access and healthcare seeking for childhood illnesses among childbearing women in sub-Saharan Africa: A multilevel modelling of Demographic and Health Surveys. PLoS ONE 2021, 16, e0244395. [Google Scholar] [CrossRef]
- Hamilton, D.O.; Nunes, J.V.; Grobusch, M.P. Improving the diagnostics of tuberculosis and drug resistance with Xpert MTB/RIF in a district general hospital in Sierra Leone: A quality improvement project. BMJ Open Qual. 2019, 8, e000478. [Google Scholar] [CrossRef] [Green Version]
- Lakoh, S.; Jiba, D.F.; Adekanmbi, O.; Poveda, E.; Sahr, F.; Deen, G.F.; Foray, L.M.; Gashau, W.; Hoffmann, C.J.; Salata, R.A.; et al. Diagnosis and treatment outcomes of adult tuberculosis in an urban setting with high HIV prevalence in Sierra Leone: A retrospective study. Int. J. Infect. Dis. 2020, 96, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Chaves Torres, N.M.; Quijano Rodríguez, J.J.; Porras Andrade, P.S.; Arriaga, M.B.; Netto, E.M. Factors predictive of the success of tuberculosis treatment: A systematic review with meta-analysis. PLoS ONE 2019, 14, e0226507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akanbi, K.; Ajayi, I.; Fayemiwo, S.; Gidado, S.; Oladimeji, A.; Nsubuga, P. Predictors of tuberculosis treatment success among HIV-TB co-infected patients attending major tuberculosis treatment sites in Abeokuta, Ogun State, Nigeria. Pan Afr. Med. J. 2019, 32 (Suppl. 1), 7. [Google Scholar] [CrossRef] [PubMed]
- Peetluk, L.S.; Ridolfi, F.M.; Rebeiro, P.F.; Liu, D.; Rolla, V.C.; Sterling, T.R. Systematic review of prediction models for pulmonary tuberculosis treatment outcomes in adults. BMJ Open 2021, 11, e044687. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for Treatment of Drug-Susceptible Tuberculosis and Patient Care, 2017 Update. Available online: https://www.afro.who.int/sites/default/files/2017-06/9789241550000-eng.pdf (accessed on 17 June 2021).
- World Health Organization. Guidelines for Treatment of Drug-Resistant Tuberculosis. Available online: https://apps.who.int/iris/bitstream/handle/10665/332678/9789240007062-eng.pdf (accessed on 17 June 2021).
- Karumbi, J.; Garner, P. Directly observed therapy for treating tuberculosis. Cochrane Database Syst. Rev. 2015, 2015, 1–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaren, Z.M.; Milliken, A.A.; Meyer, A.J.; Sharp, A.R. Does directly observed therapy improve tuberculosis treatment? More evidence is needed to guide tuberculosis policy. BMC Infect. Dis. 2016, 16, 537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benbaba, S.; Isaakidis, P.; Das, M.; Jadhav, S.; Reid, T.; Furin, J. Direct Observation (DO) for Drug-Resistant Tuberculosis: Do We Really DO? PLoS ONE 2015, 10, e0144936. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | 2019 (Baseline) | 2019 Totals | 2020 (Intra-COVID-19) | 2020 Totals | % Change in 2019 and 2020 Totals | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Q1 (January–March) | Q2 (April–June) | Q3 (July–September) | Q1 (January–March) | Q2 (April–June) | Q3 (July–September) | |||||
| Presumptive cases | 957 | 900 | 779 | 2636 | 1199 | 386 | 715 | 2300 | −12.7% | |
| Gender | ||||||||||
| Male | 504 | 480 | 432 | 1416 | 709 | 247 | 428 | 1384 | −2.3% | <0.001 |
| Female | 453 | 420 | 347 | 1220 | 490 | 139 | 287 | 916 | −24.9% | |
| Age category | ||||||||||
| Children (≤15 years) | 62 | 71 | 35 | 168 | 102 | 11 | 22 | 135 | −19.6% | <0.001 |
| Adults (>15 years) | 895 | 829 | 744 | 2468 | 1097 | 375 | 693 | 2165 | −12.3% | |
| Mode of referral | ||||||||||
| Self-reporting | 219 | 229 | 160 | 608 | 367 | 104 | 184 | 655 | + 7.7% | <0.001 |
| Health facility | 322 | 348 | 320 | 990 | 770 | 238 | 443 | 1451 | +46.6% | |
| Community-initiated | 416 | 323 | 299 | 1038 | 62 | 44 | 88 | 194 | −81.3% | |
| HIV positivity rate | 31.7% | 30.2% | 34.3% | 31.9% | 32.2% | 30.8% | 38.3% | 33.9% | +2.0% | 0.011 |
| Laboratory-confirmed TB | 195 | 176 | 164 | 535 | 331 | 139 | 263 | 733 | +37.0% | <0.001 |
| Characteristics | Notified TB Cases (N = 1208) | Pre-COVID-19 (April–June 2019) (N = 613) | Intra-COVID-19 (April–June 2020) (N = 595) | p-Value |
|---|---|---|---|---|
| Gender | ||||
| Male | 756 (62.6) | 388 (63.3) | 368 (61.8) | 0.603 |
| Female | 452 (37.4) | 225 (36.7) | 227 (38.2) | |
| Age, years | ||||
| ≤24 | 300 (24.8) | 151 (24.6) | 149 (25.0) | 0.544 |
| 25–34 | 346 (28.6) | 186 (30.3) | 160 (26.9) | |
| 35–44 | 255 (21.1) | 131 (21.4) | 124 (20.8) | |
| 45–54 | 174 (14.4) | 80 (13.1) | 94 (15.8) | |
| ≥55 | 133 (11.0) | 65 (10.6) | 68 (11.4) | |
| Patient type | ||||
| Newly diagnosed | 1069 (88.5) | 551 (89.9) | 518 (87.1) | 0.124 |
| Relapsed | 139 (11.5) | 62 (10.1) | 77 (12.9) | |
| Type of tuberculosis | ||||
| Pulmonary | 1152 (95.4) | 584 (95.3) | 568 (95.5) | 0.873 |
| Extrapulmonary | 56 (4.6) | 29 (4.7) | 27 (4.5) | |
| Mode of diagnosis | ||||
| Laboratory confirmed | 720 (59.6) | 341 (55.6) | 379 (63.7) | 0.004 |
| Clinical diagnosis | 488 (40.4) | 272 (44.4) | 216 (36.3) | |
| HIV status | ||||
| Positive | 425 (35.2) | 206 (33.6) | 219 (36.8) | 0.399 |
| Negative | 752 (62.3) | 389 (63.5) | 363 (61.0) | |
| Unknown | 31 (2.6) | 18 (2.9) | 13 (2.2) | |
| Treatment method | ||||
| Directly Observed Therapy | 849 (70.3) | 613 (100) | 236 (39.7) | <0.001 |
| Monthly dispensing for self-administration | 359 (29.7) | - | 359 (29.7) | |
| WHO treatment outcomes | ||||
| Cured | 384 (31.8) | 176 (28.7) | 208 (35.0) | <0.001 |
| Completed | 233 (19.3) | 110 (17.9) | 123 (20.7) | |
| Lost to follow up | 227 (18.8) | 130 (21.3) | 97 (16.3) | |
| Transferred/not evaluated) | 193 (16.0) | 83 (13.5) | 110 (18.5) | |
| Failed treatment | 9 (0.7) | 5 (0.8) | 4 (0.7) | |
| Died | 162 (13.4) | 109 (17.8) | 53 (8.9) | |
| Treatment success * | ||||
| Yes | 617 (51.1) | 286 (46.7) | 331 (55.6) | 0.002 |
| No | 591 (48.9) | 327 (53.3) | 264 (44.4) |
| Characteristics | Treatment Success | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|---|
| Yes (N = 617) | No (N = 591) | Crude OddsRatio (95% Confidence Interval) | p-Value | Adjusted Odds Ratio (95% Convidence Interval) | p-Value | |
| Gender | ||||||
| Male | 376 (60.9) | 380 (64.3) | 0.87 (0.69–1.10) | 0.228 | 0.78 (0.61–1.00) | 0.053 |
| Female | 241 (39.1) | 211 (35.7) | Reference | Reference | ||
| Age, years | ||||||
| <55 | 565 (91.6) | 510 (86.3) | 1.73 (1.19–2.49) | 0.003 | 1.74 (1.08–2.56) | 0.005 |
| ≥55 | 52 (8.4) | 81 (13.7) | Reference | Reference | ||
| Patient type | ||||||
| Newly diagnosed | 532 (86.2) | 537 (90.9) | 1.59 (1.11–2.28) | 0.012 | 1.69 (1.16–2.47) | 0.007 |
| Relapsed | 85 (13.8) | 54 (9.1) | Reference | Reference | ||
| Type of tuberculosis | ||||||
| Pulmonary | 603 (97.7) | 549 (92.9) | 3.30 (1.78–6.10) | <0.001 | 3.17 (1.67–6.04) | <0.001 |
| Extrapulmonary | 14 (2.3) | 42 (7.1) | Reference | Reference | ||
| Mode of diagnosis | ||||||
| Laboratory-confirmed | 395 (64.0) | 325 (55.0) | 1.46 (1.16–1.83) | 0.001 | 1.14 (0.88–1.47) | 0.318 |
| Clinical diagnosis | 222 (36.0) | 266 (45.0) | Reference | Reference | ||
| HIV status | ||||||
| Positive | 194 (32.1) | 231 (40.4) | Reference | 0.003 | Reference | <0.001 |
| Negative | 411 (67.9) | 341 (59.6) | 1.43 (1.13–1.82) | 1.60 (1.24–2.06) | ||
| Treatment method | ||||||
| Directly Observed Therapy | 404 (65.5) | 445 (75.3) | Reference | <0.001 | Reference | 0.001 |
| Monthly Dispensing for Self-administration | 213 (34.5) | 146 (24.7) | 1.61 (1.25–2.06) | 1.56 (1.21–2.03) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lakoh, S.; Jiba, D.F.; Baldeh, M.; Adekanmbi, O.; Barrie, U.; Seisay, A.L.; Deen, G.F.; Salata, R.A.; Yendewa, G.A. Impact of COVID-19 on Tuberculosis Case Detection and Treatment Outcomes in Sierra Leone. Trop. Med. Infect. Dis. 2021, 6, 154. https://doi.org/10.3390/tropicalmed6030154
Lakoh S, Jiba DF, Baldeh M, Adekanmbi O, Barrie U, Seisay AL, Deen GF, Salata RA, Yendewa GA. Impact of COVID-19 on Tuberculosis Case Detection and Treatment Outcomes in Sierra Leone. Tropical Medicine and Infectious Disease. 2021; 6(3):154. https://doi.org/10.3390/tropicalmed6030154
Chicago/Turabian StyleLakoh, Sulaiman, Darlinda F. Jiba, Mamadu Baldeh, Olukemi Adekanmbi, Umu Barrie, Alhassan L. Seisay, Gibrilla F. Deen, Robert A. Salata, and George A. Yendewa. 2021. "Impact of COVID-19 on Tuberculosis Case Detection and Treatment Outcomes in Sierra Leone" Tropical Medicine and Infectious Disease 6, no. 3: 154. https://doi.org/10.3390/tropicalmed6030154