
COVID-19 Vaccination Intent and Willingness to Pay in Bangladesh: A Cross-Sectional Study

 ,
,  , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Participants’ Characteristics
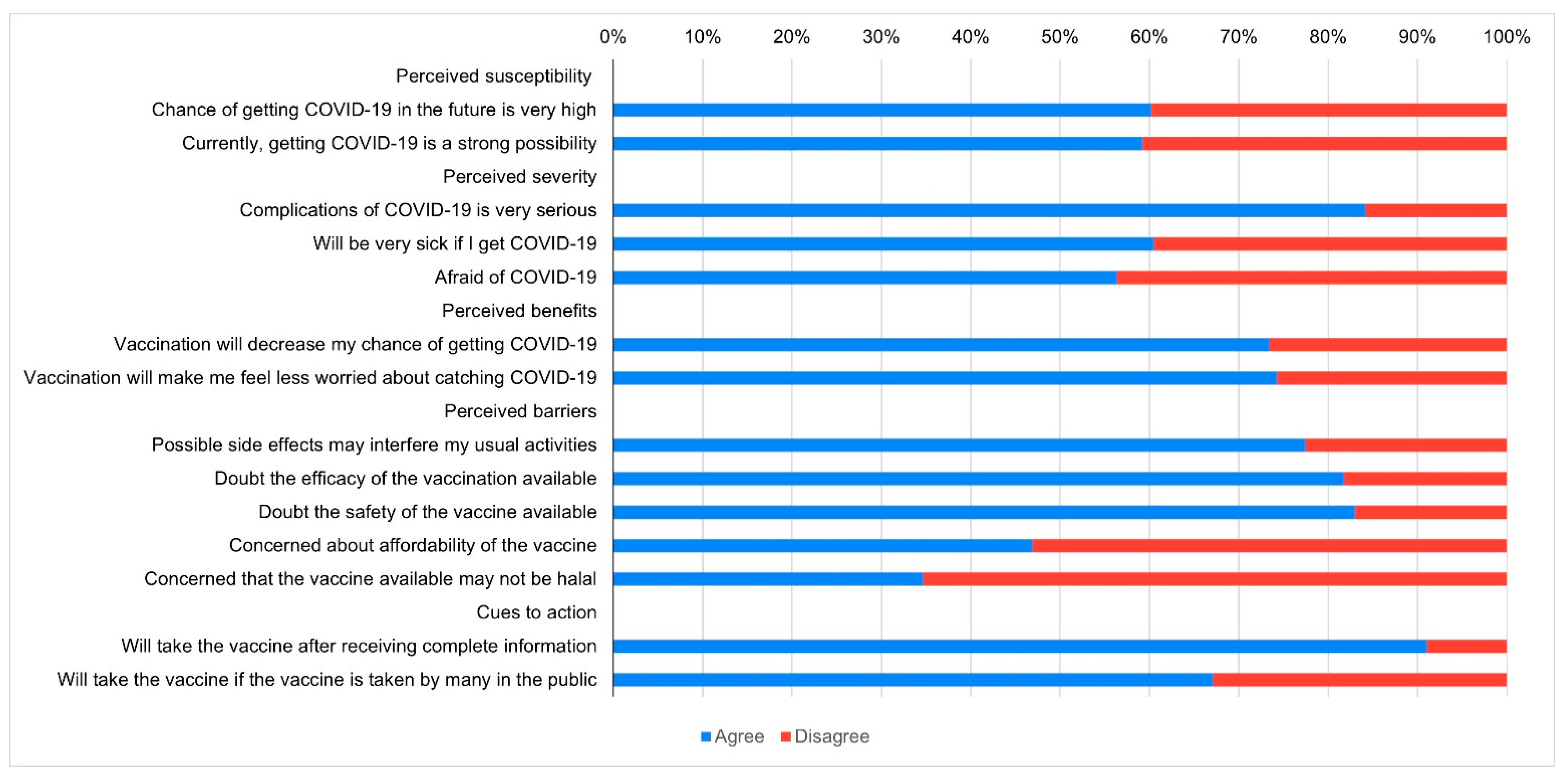
3.2. Perceived COVID-19-Related Health Beliefs
3.3. COVID-19 Vaccination Intent and Predictors
3.4. Willingness to Pay and Vaccination Preference
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Adhikari, S.P.; Meng, S.; Wu, Y.-J.; Mao, Y.-P.; Ye, R.-X.; Wang, Q.-Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [Green Version]
- Pillai, S.; Siddika, N.; Hoque Apu, E.; Kabir, R. COVID-19: Situation of European Countries so Far. Arch. Med Res. 2020, 51, 723–725. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/table (accessed on 12 February 2021).
- Cousins, S. Bangladesh’s COVID-19 testing criticised. Lancet 2020, 396, 591. [Google Scholar] [CrossRef]
- McArthur, L.; Sakthivel, D.; Ataide, R.; Chan, F.; Richards, J.S.; Narh, C.A. Review of Burden, Clinical Definitions, and Management of COVID-19 Cases. Am. J. Trop. Med. Hyg. 2020, 103, 625–638. [Google Scholar] [CrossRef] [PubMed]
- Thanh Le, T.; Andreadakis, Z.; Kumar, A.; Gómez Román, R.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 vaccine development landscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. DRAFT Landscape of COVID-19 Candidate Vaccines. 20 April 2020. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 24 February 2021).
- Mishra, S.K.; Tripathi, T. One year update on the COVID-19 pandemic: Where are we now? Acta Trop. 2021, 214, 105778. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Lists Two Additional COVID-19 Vaccines for Emergency Use and COVAX Roll-Out. Available online: https://www.who.int/news/item/15-02-2021-who-lists-two-additional-covid-19-vaccines-for-emergency-use-and-covax-roll-out (accessed on 17 February 2021).
- World Health Organization. Ten Threats to Global Health. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 7 January 2021).
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- Iboi, E.; Ngonghala, C.N.; Gumel, A.B. Will an imperfect vaccine curtail the COVID-19 pandemic in the U.S.? medRxiv 2020, 5, 510–524. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Feleszko, W.; Lewulis, P.; Czarnecki, A.; Waszkiewicz, P. Flattening the Curve of COVID-19 Vaccine Rejection—A Global Overview. 2020. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3631972 (accessed on 2 April 2021). [CrossRef]
- Al-Mohaithef, M.; Padhi, B.K. Determinants of COVID-19 Vaccine Acceptance in Saudi Arabia: A Web-Based National Survey. J. Multidiscip. Healthc. 2020, 13, 1657–1663. [Google Scholar] [CrossRef]
- Fu, C.; Wei, Z.; Pei, S.; Li, S.; Sun, X.; Liu, P. Acceptance and preference for COVID-19 vaccination in health-care workers (HCWs). medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Thunstrom, L.; Ashworth, M.; Finnoff, D.; Newbold, S. Hesitancy towards a COVID-19 Vaccine and Prospects for Herd Immunity. 2020. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3593098 (accessed on 2 April 2021). [CrossRef]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef]
- Daly, M.; Robinson, E. Willingness to vaccinate against COVID-19 in the US: Longitudinal evidence from a nationally representative sample of adults from April–October 2020. medRxiv 2020. [Google Scholar] [CrossRef]
- Siam, Z.S.; Arifuzzaman, M.; Ahmed, M.S.; Khan, F.A.; Rashid, M.H.; Islam, M.S. Dynamics of COVID-19 transmission in Dhaka and Chittagong: Two business hubs of Bangladesh. Clin. Epidemiol. Glob. Health 2021, 10, 100684. [Google Scholar] [CrossRef]
- Biswas, R.K.; Huq, S.; Afiaz, A.; Khan, H.T.A. A systematic assessment on COVID-19 preparedness and transition strategy in Bangladesh. J. Eval. Clin. Pract. 2020, 26, 1599–1611. [Google Scholar] [CrossRef] [PubMed]
- Ahamad, M.G.; Islam, A.K.M.N.; Talukder, B.; Ahmed, M.U. COVID-19 Vaccination in Bangladesh: Challenges on Price, Misinformation, and Trust. SocArXiv 2021. [Google Scholar] [CrossRef]
- de Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Figueroa, J.P.; Bottazzi, M.E.; Hotez, P.; Batista, C.; Ergonul, O.; Gilbert, S.; Gursel, M.; Hassanain, M.; Kim, J.H.; Lall, B.; et al. Urgent needs of low-income and middle-income countries for COVID-19 vaccines and therapeutics. Lancet 2021, 397, 562–564. [Google Scholar] [CrossRef]
- Ess, S.M.; Szucs, T.D. Economic evaluation of immunization strategies. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2002, 35, 294–297. [Google Scholar] [CrossRef] [Green Version]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Kabamba Nzaji, M.; Kabamba Ngombe, L.; Ngoie Mwamba, G.; Banza Ndala, D.B.; Mbidi Miema, J.; Luhata Lungoyo, C.; Lora Mwimba, B.; Cikomola Mwana Bene, A.; Mukamba Musenga, E. Acceptability of Vaccination Against COVID-19 Among Healthcare Workers in the Democratic Republic of the Congo. Pragmat. Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef]
- Roozenbeek, J.; Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; van der Linden, S. Susceptibility to misinformation about COVID-19 around the world. R. Soc. Open Sci. 2020, 7, 201199. [Google Scholar] [CrossRef] [PubMed]
- Szmyd, B.; Bartoszek, A.; Karuga, F.F.; Staniecka, K.; Błaszczyk, M.; Radek, M. Medical Students and SARS-CoV-2 Vaccination: Attitude and Behaviors. Vaccines 2021, 9, 128. [Google Scholar] [CrossRef]
- Szmyd, B.; Karuga, F.F.; Bartoszek, A.; Staniecka, K.; Siwecka, N.; Bartoszek, A.; Błaszczyk, M.; Radek, M. Attitude and Behaviors towards SARS-CoV-2 Vaccination among Healthcare Workers: A Cross-Sectional Study from Poland. Vaccines 2021, 9, 218. [Google Scholar] [CrossRef]
- Edwards, B.; Biddle, N.; Gray, M.; Sollis, K. COVID-19 vaccine hesitancy and resistance: Correlates in a nationally representative longitudinal survey of the Australian population. medRxiv 2020. [Google Scholar] [CrossRef]
- Ward, J.K.; Alleaume, C.; Peretti-Watel, P.; Group, C. The French public’s attitudes to a future COVID-19 vaccine: The politicization of a public health issue. Soc. Sci. Med. 2020, 265, 113414. [Google Scholar] [CrossRef]
- Khoo, Y.S.K.; Ghani, A.A.; Navamukundan, A.A.; Jahis, R.; Gamil, A. Unique product quality considerations in vaccine development, registration and new program implementation in Malaysia. Hum. Vaccines Immunother. 2020, 16, 530–538. [Google Scholar] [CrossRef] [Green Version]
- The New York Times. Is the Vaccine Halal? Indonesians Await the Answer. Available online: https://www.nytimes.com/2021/01/05/world/asia/indonesia-sinovac-vaccine-halal.html (accessed on 2 April 2021).
- Shams, A.B.; Hoque Apu, E.; Rahman, A.; Sarker Raihan, M.M.; Siddika, N.; Preo, R.B.; Hussein, M.R.; Mostari, S.; Kabir, R. Web Search Engine Misinformation Notifier Extension (SEMiNExt): A Machine Learning Based Approach during COVID-19 Pandemic. Healthcare 2021, 9, 156. [Google Scholar] [CrossRef]
- Zainudin, E.N.H.E.; Mohammad, K.A.; Aris, A.; Shahdan, I.A. Vaccination: Influencing Factors and View from an Islamic Perspective. IIUM Med. J. Malays. 2018, 17, 273–280. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef] [PubMed]
- Sarasty, O.; Carpio, C.E.; Hudson, D.; Guerrero-Ochoa, P.A.; Borja, I. The demand for a COVID-19 vaccine in Ecuador. Vaccine 2020, 38, 8090–8098. [Google Scholar] [CrossRef] [PubMed]
- Borriello, A.; Master, D.; Pellegrini, A.; Rose, J.M. Preferences for a COVID-19 vaccine in Australia. Vaccine 2021, 39, 473–479. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Isha, S.; Apu, E.; Siddika, N.; Kabir, R. Oral health status of the Rohingya refugees in Bangladesh and the COVID-19 pandemic. Adv. Hum. Biol. 2021, 11, 135–136. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Gender | |
| Male | 372 (53.4) |
| Female | 325 (46.6) |
| Age | |
| 18–29 years | 457 (65.6) |
| 30–39 years | 126 (18.1) |
| 40–49 years | 72 (10.3) |
| 50 years or more | 42 (6.0) |
| Education | |
| Primary or below | 19 (2.7) |
| Secondary | 108 (15.5) |
| Tertiary (college/university) | 570 (81.8) |
| Occupation | |
| Unemployed | 58 (8.3) |
| General worker | 24 (3.4) |
| Student | 297 (42.6) |
| Self-employed | 38 (5.5) |
| Private service | 95 (13.6) |
| Government service | 50 (7.2) |
| Health professionals | 135 (19.4) |
| Area of residence | |
| Dhaka | 500(71.7) |
| Outside of Dhaka | 197(28.3) |
| Religion | |
| Islam | 658 (94.4) |
| Other | 39 (5.6) |
| Participant has chronic disease | |
| No | 554 (79.5) |
| Yes | 143 (20.5) |
| Family member has chronic disease | |
| No | 261 (37.4) |
| Yes | 436 (62.6) |
| Participant diagnosed with COVID-19 | |
| No | 595(85.4) |
| Yes | 102(14.6) |
| Family member diagnosed with COVID-19 | |
| No | 501 (71.9) |
| Yes | 196 (28.1) |
| Characteristics | Definite Intent | Definite or Probable Intent | Definite Intent against Vaccination |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Gender | |||
| Female | 1 | 1 | 1 |
| Male | 1.32 (0.91–1.92) | 1.20 (0.84–1.70) | 0.63 (0.32–1.21) |
| Age | |||
| 18–29 years | 1 | 1 | 1 |
| 30–39 years | 1.11 (0.63–1.99) | 0.87 (0.52–1.45) | 0.80 (0.29–2.24) |
| 40–49 years | 1.37 (0.67–2.80) | 1.04 (0.53–2.01) | 2.60 (0.96–7.07) |
| 50 years or more | 1.78 (0.70–4.53) | 0.86 (0.37–1.98) | 3 (0.87–10.24) |
| Education | |||
| Tertiary (college/university) | 1 | 1 | 1 |
| Secondary | 0.90 (0.53–1.52) | 0.99 (0.61–1.60) | 2.01 (0.91–4.45) |
| Primary or below | 0.99 (0.24–4.05) | 0.67 (0.22–1.98) | 2.81 (0.64–12.36) |
| Occupation | |||
| Unemployed | 1 | 1 | 1 |
| General worker | 0.53 (0.12–2.35) | 0.56 (0.18–1.69) | 4.30 (0.93–19.84) |
| Student | 1.71 (0.73–4.03) | 0.59 (0.26–1.30) | 1.04 (0.28–3.84) |
| Self-employed | 0.71 (0.22–2.24) | 0.48 (0.18–1.24) | 3.33 (0.81–13.65) |
| Private service | 0.58 (0.22–1.52) | 0.40 (0.18–0.90) * | 1.97 (0.52–7.40) |
| Government service | 1.82 (0.70–4.70) | 0.70 (0.27–1.74) | 2.96 (0.74–11.40) |
| Health professionals | 2.06 (0.88–4.83) | 0.71 (0.32–1.59) | 0.73 (0.18–3.01) |
| Area of residence | |||
| Dhaka | 1 | 1 | 1 |
| Outside of Dhaka | 0.77 (0.51–1.16) | 0.85 (0.58–1.22) | 0.30 (0.13–0.74) ** |
| Religion | |||
| Other | 1 | 1 | 1 |
| Islam | 0.52 (0.25–1.08) | 0.36 (0.15–0.89) * | 1.11 (0.24–5.17) |
| Participant has chronic disease | |||
| No | 1 | 1 | 1 |
| Yes | 0.68 (0.40–1.15) | 1.05 (0.67–1.67) | 0.44 (0.18–1.07) |
| Family member with chronic disease | |||
| No | 1 | 1 | 1 |
| Yes | 0.95 (0.65–1.40) | 1.23 (0.87–1.75) | 1.07 (0.57–2.04) |
| Participant’s history of SARS-CoV-2 infection | |||
| No | 1 | 1 | 1 |
| Yes | 2.86 (1.71–4.79) ** | 1.25 (0.74–2.11) | 0.52 (0.16–1.65) |
| Family history of SARS-CoV-2 infection | |||
| No | 1 | 1 | 1 |
| Yes | 0.74 (0.48–1.17) | 1.05 (0.70–1.59) | 1.23 (0.59–2.54) |
| HBM Constructs | Definite Intent | Definite or Probable Intention | Definite Intent against Vaccination |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Perceived susceptibility | |||
| Chance of getting COVID-19 in the future is very high | 0.70 (0.43–1.14) | 0.53 (0.33–0.83) ** | 2.01 (0.93–4.36) |
| Currently, getting COVID-19 is a strong possibility | 0.88 (0.54–1.42) | 0.80 (0.50–1.27) | 0.97 (0.44–2.14) |
| Perceived severity | |||
| Complications of COVID-19 is very serious | 1.93 (1.04–3.59) * | 0.91 (0.53–1.60) | 0.83 (0.34–2.02) |
| Will be very sick if I get COVID-19 | 0.81 (0.52–1.26) | 0.79 (0.50–1.22) | 1.28 (0.56–2.89) |
| Afraid of COVID-19 | 1.17 (.72–1.74) | 0.99 (0.64–1.52) | 1.10 (0.51–2.38) |
| Perceived benefits | |||
| Vaccination will decrease my chance of getting COVID-19 | 1.71 (0.94–3.14) | 2.23(1.39–3.59) ** | 0.59(0.26–1.33) |
| Vaccination will make me feel less worried about catching COVID-19 | 4.42 (2.25–8.68) ** | 4.31 (2.73–6.82) ** | 0.20 (0.09–0.46) ** |
| Perceived barriers | |||
| Possible side effects may interfere my usual activities | 0.34 (0.21–0.53) ** | 0.49 (0.29–0.84) ** | 2.53 (0.85–7.45) |
| Doubt the efficacy of the vaccination available | 1.39 (0.72–2.67) | 1.68 (0.94–3.02) | 0.59 (0.23–1.49) |
| Doubt the safety of the vaccine available | 0.62 (0.33–1.18) | 0.79 (0.42–1.48) | 1.29 (0.46–3.62) |
| Concerned about affordability of the vaccine | 1.51 (1.01–2.25) * | 1.30 (0.88–1.90) | 1.40 (0.72–2.74) |
| Concerned that the vaccine available may not be halal | 0.66 (0.42–1.01) | 0.92 (0.62–1.38) | 2.03 (1.04–3.96) * |
| Cues to action | |||
| Will take the vaccine after receiving complete information | 0.85 (0.41–1.75) | 1.20 (0.61–2.34) | 0.41 (0.16–1.04) |
| Will take the vaccine if the vaccine is taken by many in the public | 0.44 (0.29–0.67) ** | 1.21 (0.80–1.83) | 0.40 (0.20–0.79) ** |
| Willingness to Pay and Preference | Participants |
|---|---|
| Willing to pay | 68.4% |
| Median amount willing to pay in USD | 7.08 |
| Prefer buying a vaccine from available alternatives over the free one provided by the government | 32.9% |
| Country of origin of the vaccine matters | 52.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kabir, R.; Mahmud, I.; Chowdhury, M.T.H.; Vinnakota, D.; Jahan, S.S.; Siddika, N.; Isha, S.N.; Nath, S.K.; Hoque Apu, E. COVID-19 Vaccination Intent and Willingness to Pay in Bangladesh: A Cross-Sectional Study. Vaccines 2021, 9, 416. https://doi.org/10.3390/vaccines9050416
Kabir R, Mahmud I, Chowdhury MTH, Vinnakota D, Jahan SS, Siddika N, Isha SN, Nath SK, Hoque Apu E. COVID-19 Vaccination Intent and Willingness to Pay in Bangladesh: A Cross-Sectional Study. Vaccines. 2021; 9(5):416. https://doi.org/10.3390/vaccines9050416
Chicago/Turabian StyleKabir, Russell, Ilias Mahmud, Mohammad Tawfique Hossain Chowdhury, Divya Vinnakota, Shah Saif Jahan, Nazeeba Siddika, Samia Naz Isha, Sujan Kanti Nath, and Ehsanul Hoque Apu. 2021. "COVID-19 Vaccination Intent and Willingness to Pay in Bangladesh: A Cross-Sectional Study" Vaccines 9, no. 5: 416. https://doi.org/10.3390/vaccines9050416