Cranberry Extract for Symptoms of Acute, Uncomplicated Urinary Tract Infection: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria and Study Selection
2.3. Risk of Bias
2.4. Data Extraction
3. Results
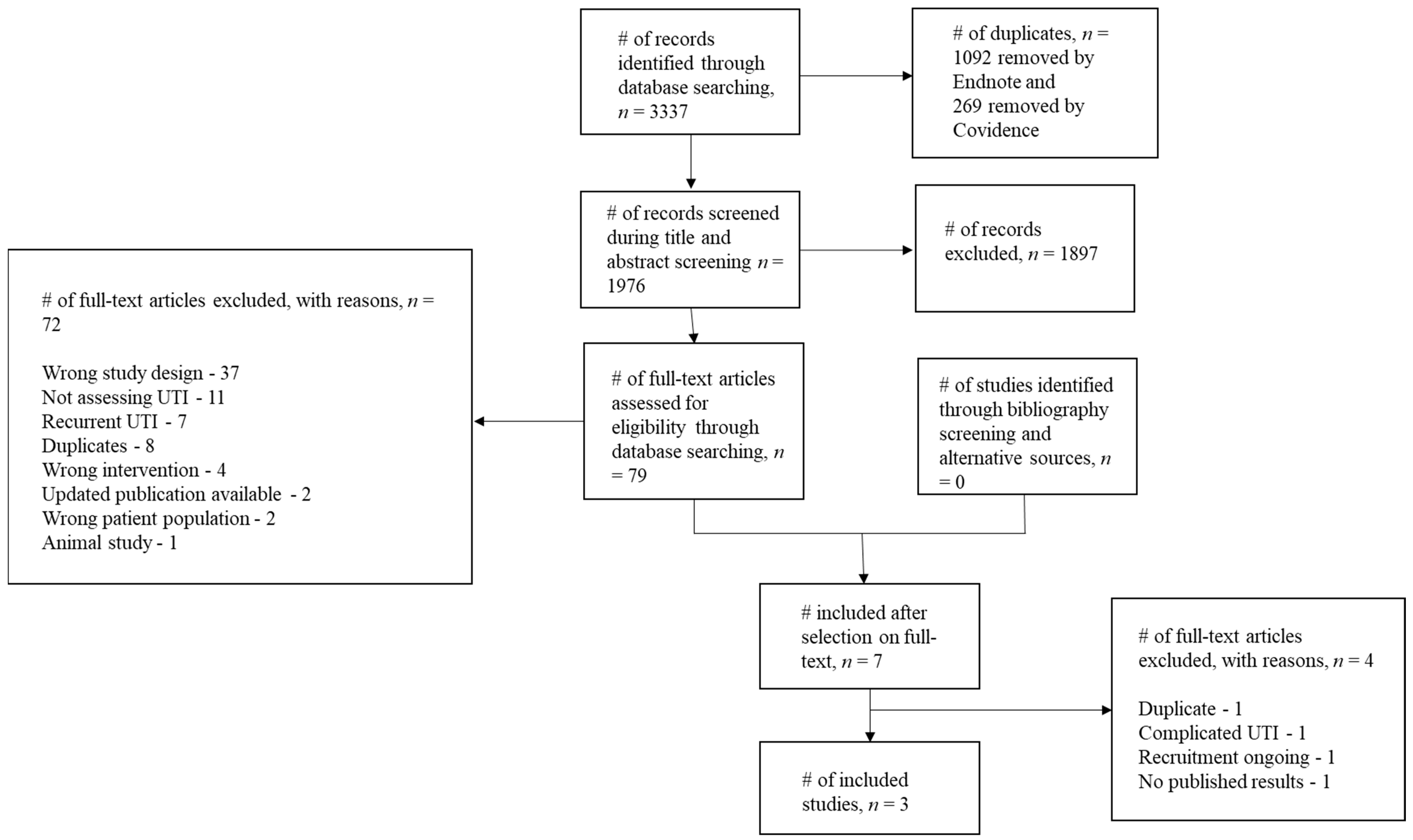
3.1. Study Screening
3.2. Study Characteristics
3.3. Risk of Bias
3.4. Symptoms
3.5. Antibiotic Use
3.6. Microbiological Assessment
3.7. Time to Reconsultation
3.8. Serious Adverse Events
4. Discussion
4.1. Comparison with Existing Literature
4.2. Strengths and Limitations
4.3. Implications for Future Research and Clinical Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Little, P.; Merriman, R.; Turner, S.; Rumsby, K.; Warner, G.; Lowes, J.A.; Smith, H.; Hawke, C.; Leydon, G.; Mullee, M.; et al. Presentation, pattern, and natural course of severe symptoms, and role of antibiotics and antibiotic resistance among patients presenting with suspected uncomplicated urinary tract infection in primary care: Observational study. BMJ 2010, 340, b5633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, C.C.; Hawking, M.K.; Quigley, A.; McNulty, C.A. Incidence, severity, help seeking, and management of uncomplicated urinary tract infection: A population-based survey. Br. J. Gen. Pract. 2015, 65, e702–e707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, M.; Trill, J.; Simpson, C.; Webley, F.; Radford, M.; Stanton, L.; Maishman, T.; Galanopoulou, A.; Flower, A.; Eyles, C. Uva-ursi extract and ibuprofen as alternative treatments for uncomplicated urinary tract infection in women (ATAFUTI): A factorial randomized trial. Clin. Microbiol. Infect. 2019, 25, 973–980. [Google Scholar] [CrossRef] [Green Version]
- Gágyor, I.; Bleidorn, J.; Kochen, M.M.; Schmiemann, G.; Wegscheider, K.; Hummers-Pradier, E. Ibuprofen versus fosfomycin for uncomplicated urinary tract infection in women: Randomised controlled trial. BMJ 2015, 351, h6544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bleidorn, J.; Gágyor, I.; Kochen, M.M.; Wegscheider, K.; Hummers-Pradier, E. Symptomatic treatment (ibuprofen) or antibiotics (ciprofloxacin) for uncomplicated urinary tract infection?-results of a randomized controlled pilot trial. BMC Med. 2010, 8, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kronenberg, A.; Bütikofer, L.; Odutayo, A.; Mühlemann, K.; da Costa, B.R.; Battaglia, M.; Meli, D.N.; Frey, P.; Limacher, A.; Reichenbach, S. Symptomatic treatment of uncomplicated lower urinary tract infections in the ambulatory setting: Randomised, double blind trial. BMJ 2017, 359, j4784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polashock, J.; Zelzion, E.; Fajardo, D.; Zalapa, J.; Georgi, L.; Bhattacharya, D.; Vorsa, N. The American cranberry: First insights into the whole genome of a species adapted to bog habitat. BMC Plant Biol. 2014, 14, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szajdek, A.; Borowska, E. Bioactive compounds and health-promoting properties of berry fruits: A review. Plant Foods Hum. Nutr. 2008, 63, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Ruel, G.; Pomerleau, S.; Couture, P.; Lemieux, S.; Lamarche, B.; Couillard, C. Favourable impact of low-calorie cranberry juice consumption on plasma HDL-cholesterol concentrations in men. Br. J. Nutr. 2006, 96, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Pappas, E.; Schaich, K. Phytochemicals of cranberries and cranberry products: Characterization, potential health effects, and processing stability. Crit. Rev. Food Sci. Nutr. 2009, 49, 741–781. [Google Scholar] [CrossRef] [PubMed]
- Bodet, C.; Grenier, D.; Chandad, F.; Ofek, I.; Steinberg, D.; Weiss, E. Potential oral health benefits of cranberry. Crit. Rev. Food Sci. Nutr. 2008, 48, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Howell, A.B.; Reed, J.D.; Krueger, C.G.; Winterbottom, R.; Cunningham, D.G.; Leahy, M. A-type cranberry proanthocyanidins and uropathogenic bacterial anti-adhesion activity. Phytochemistry 2005, 66, 2281–2291. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-H.; Fang, C.-C.; Chen, N.-C.; Liu, S.S.-H.; Yu, P.-H.; Wu, T.-Y.; Chen, W.-T.; Lee, C.-C.; Chen, S.-C. Cranberry-containing products for prevention of urinary tract infections in susceptible populations: A systematic review and meta-analysis of randomized controlled trials. Arch. Intern. Med. 2012, 172, 988–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luís, Â.; Domingues, F.; Pereira, L. Can cranberries contribute to reduce the incidence of urinary tract infections? A systematic review with meta-analysis and trial sequential analysis of clinical trials. J. Urol. 2017, 198, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Jepson, R.G.; Williams, G.; Craig, J.C. Cranberries for preventing urinary tract infections. Cochrane Libr. 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicariotto, F. Effectiveness of an association of a cranberry dry extract, D-mannose, and the two microorganisms Lactobacillus plantarum LP01 and Lactobacillus paracasei LPC09 in women affected by cystitis: A pilot study. J. Clin. Gastroenterol. 2014, 48, S96–S101. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- OCEBM Levels of Evidence. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 26 September 2020).
- The Cochrane Collaboration. Review Manager (RevMan)[Computer Program] Version 5.3; The Nordic Cochrane Centre: Copenhagen, Denmark, 2014. [Google Scholar]
- AL-Zobaidy, M.A.-H.; Jebur, M.H.; Hindi, N.K.K. Development, Evaluation of Antimicrobial Activity of the Aquatic Extracts of Zea Mays, Cranberries and Raisins against Bacterial isolates from Urinary Tract Infection in Babylon Province, Iraq. J. Indian J. Public Health Res. 2019, 10, 854–861. [Google Scholar] [CrossRef]
- Howell, A.B.; Vorsa, N.; Marderosian, A.D.; Foo, L.Y. Inhibition of the adherence of P-fimbriated Escherichia coli to uroepithelial-cell surfaces by proanthocyanidin extracts from cranberries. N. Engl. J. Med. 1998, 339, 1085–1086, Erratum in 1998, 339, 1408. [Google Scholar] [CrossRef]
- Rahbar, M.; Diba, K. In vitro activity of cranberry extract against etiological agents of urinary tract infections. Afr. J. Pharm. Pharmacol. 2010, 4, 286–288. [Google Scholar]
- Magariños, H.; Sahr, C.; Selaive, S.; Costa, M.; Figuerola, F.; Pizarro, O. In vitro inhibitory effect of cranberry (Vaccinium macrocarpum Ait.) juice on pathogenic microorganisms. Appl. Biochem. Microbiol. 2008, 44, 300–304. [Google Scholar] [CrossRef]
- Cunningham, E. Do Cranberries Aid in the Treatment of Urinary Tract Infections? J. Acad. Nutr. Diet. 2002, 102, 1118. [Google Scholar] [CrossRef]
- LaPlante, K.L.; Gill, C.M.; Rowley, D. Cranberry Capsules for Bacteriuria Plus Pyuria in Nursing Home Residents. JAMA 2017, 317, 1078. [Google Scholar] [CrossRef] [PubMed]
- Eydelnant, I.A.; Tufenkji, N. Cranberry derived proanthocyanidins reduce bacterial adhesion to selected biomaterials. Langmuir 2008, 24, 10273–10281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taherpour, A.; Noorabadi, P.; Abedi, F.; Taherpour, A. Effect of aqueous cranberry (Vaccinium arctostaphylos L.) extract accompanied with antibiotics on urinary tract infections caused by Escherichia coli in vitro. J. Pure Appl. Microbiol. 2008, 2, 135–138. [Google Scholar]
- Howell, A.; Souza, D.; Roller, M.; Fromentin, E. Comparison of the anti-adhesion activity of three different cranberry extracts on uropathogenic p-fimbriated Escherichia coli: A randomized, double-blind, placebo controlled, ex vivo, acute study. Nat. Prod. Commun. 2015, 10, 1934578X1501000720. [Google Scholar] [CrossRef] [Green Version]
- Bukhari, S.; Chiragh, S.; Tariq, S.; Alam, M.A.; Wazir, M.S.; Suleman, M. In vitro activity of vaccinium macrocarpon (cranberry) on urinary tract pathogens in uncomplicated urinary tract infection. J. Ayub Med. Coll. Abbottabad 2015, 27, 660–663. [Google Scholar]
- Hidalgo, G.; Chan, M.; Tufenkji, N. Inhibition of Escherichia coli CFT073 fliC expression and motility by cranberry materials. Appl. Environ. Microbiol. 2011, 77, 6852–6857. [Google Scholar] [CrossRef] [Green Version]
- Rafsanjany, N.; Senker, J.; Brandt, S.; Dobrindt, U.; Hensel, A. In vivo consumption of cranberry exerts ex vivo antiadhesive activity against FimH-dominated uropathogenic Escherichia coli: A combined in vivo, ex vivo, and in vitro study of an extract from Vaccinium macrocarpon. J. Agric. Food Chem. 2015, 63, 8804–8818. [Google Scholar] [CrossRef]
- Enache, E.; Chen, Y. Survival of Escherichia coli O157: H7, Salmonella, and Listeria monocytogenes in cranberry juice concentrates at different Brix levels. J. Food Protect. 2007, 70, 2072–2077. [Google Scholar] [CrossRef]
- Allison, D.; Cronin, M.; Hawker, J.; Freeman, S. Influence of cranberry juice on attachment of Escherichia coli to glass. J. Basic Microbiol. Int. J. Biochem. Physiol. Genet. Morphol. Ecol. Microorg. 2000, 40, 3–6. [Google Scholar]
- Caillet, S.; Côté, J.; Sylvain, J.-F.; Lacroix, M. Antimicrobial effects of fractions from cranberry products on the growth of seven pathogenic bacteria. Food Control 2012, 23, 419–428. [Google Scholar] [CrossRef]
- Di Martino, P.; Agniel, R.; Gaillard, J.; Denys, P. Effects of cranberry juice on uropathogenic Escherichia coli in vitro biofilm formation. J. Chemother. 2005, 17, 563–565. [Google Scholar] [CrossRef] [PubMed]
- Jepson, R.G.; Mihaljevic, L.; Craig, J.C. Cranberries for treating urinary tract infections. Cochrane Database Syst. Rev. 2009, 4, CD001322. [Google Scholar] [CrossRef] [PubMed]
- Nicolosi, D.; Tempera, G.; Genovese, C.; Furneri, P.M. Anti-adhesion activity of A2-type proanthocyanidins (a cranberry major component) on uropathogenic E. coli and P. mirabilis strains. Antibiotics 2014, 3, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Gonzaález de Llano, D.; Liu, H.; Khoo, C.; Moreno-Arribas, M.V.; Bartolomé, B. Some new findings regarding the antiadhesive activity of cranberry phenolic compounds and their microbial-derived metabolites against uropathogenic bacteria. J. Agric. Food Chem. 2019, 67, 2166–2174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotchkiss, A.T., Jr.; Nunñez, A.; Strahan, G.D.; Chau, H.K.; White, A.K.; Marais, J.P.; Hom, K.; Vakkalanka, M.S.; Di, R.; Yam, K.L.; et al. Cranberry xyloglucan structure and inhibition of Escherichia coli adhesion to epithelial cells. J. Agric. Food Chem. 2015, 63, 5622–5633. [Google Scholar] [CrossRef]
- Wojnicz, D.; Tichaczek-Goska, D.; Korzekwa, K.; Kicia, M.; Hendrich, A.B. Study of the impact of cranberry extract on the virulence factors and biofilm formation by Enterococcus faecalis strains isolated from urinary tract infections. Int. J. Food Sci. Nutr. 2016, 67, 1005–1016. [Google Scholar] [CrossRef]
- Huang, Y.; Nikolic, D.; Pendland, S.; Doyle, B.J.; Locklear, T.D.; Mahady, G.B. Effects of cranberry extracts and ursolic acid derivatives on P-fimbriated Escherichia coli, COX-2 activity, pro-inflammatory cytokine release and the NF-κβ transcriptional response in vitro. Pharm. Biol. 2009, 47, 18–25. [Google Scholar] [CrossRef] [Green Version]
- González de Llano, D.; Esteban-Fernández, A.; Sánchez-Patán, F.; Martínlvarez, P.J.; Moreno-Arribas, M.; Bartolomé, B. Anti-adhesive activity of cranberry phenolic compounds and their microbial-derived metabolites against uropathogenic Escherichia coli in bladder epithelial cell cultures. Int. J. Mol. Sci. 2015, 16, 12119–12130. [Google Scholar] [CrossRef]
- Wojnicz, D.; Sycz, Z.; Walkowski, S.; Gabrielska, J.; Aleksandra, W.; Alicja, K.; Anna, S.-Ł.; Hendrich, A.B. Study on the influence of cranberry extract Żuravit S· O· S® on the properties of uropathogenic Escherichia coli strains, their ability to form biofilm and its antioxidant properties. Phytomedicine 2012, 19, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Scharf, B.; Sendker, J.; Dobrindt, U.; Hensel, A. Influence of cranberry extract on Tamm-Horsfall protein in human urine and its antiadhesive activity against uropathogenic Escherichia coli. Planta Med. 2019, 85, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Côté, J.; Caillet, S.; Doyon, G.; Dussault, D.; Sylvain, J.-F.; Lacroix, M. Antimicrobial effect of cranberry juice and extracts. J. Food Control 2011, 22, 1413–1418. [Google Scholar] [CrossRef]
- Ermel, G.; Georgeault, S.; Inisan, C.; Besnard, M. Inhibition of adhesion of uropathogenic Escherichia coli bacteria to uroepithelial cells by extracts from cranberry. J. Med. Food 2012, 15, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Howell, A.B.; Zhang, D.J.; Khoo, C. A randomized, double-blind, placebo-controlled pilot study to assess bacterial anti-adhesive activity in human urine following consumption of a cranberry supplement. Food Funct. 2019, 10, 7645–7652. [Google Scholar] [CrossRef] [Green Version]
- Kaspar, K.L.; Howell, A.B.; Khoo, C. A randomized, double-blind, placebo-controlled trial to assess the bacterial anti-adhesion effects of cranberry extract beverages. Food Funct. 2015, 6, 1212–1217. [Google Scholar] [CrossRef]
- Liu, H.; Khoo, C. A Randomized, Double-Blind, Placebo-Controlled Pilot Study to Assess the Urinary Anti-Adhesion Activity Following Consumption of Cranberry+ health™ Cranberry Supplement (P06-114-19). Curr. Dev. Nutr. 2019, 3, 633. [Google Scholar] [CrossRef] [Green Version]
- Tong, H.; Heong, S.; Chang, S. Effect of ingesting cranberry juice on bacterial growth in urine. Am. J. Health-Syst. Pharm. 2006, 63, 1417–1419. [Google Scholar] [CrossRef]
- Howell, A.B.; Foxman, B. Cranberry juice and adhesion of antibiotic-resistant uropathogens. JAMA 2002, 287, 3082–3083. [Google Scholar] [CrossRef]
- Habash, M.B.; Van der Mei, H.C.; Busscher, H.J.; Reid, G. The effect of water, ascorbic acid, and cranberry derived supplementation on human urine and uropathogen adhesion to silicone rubber. Can. J. Microbiol. 1999, 45, 691–694. [Google Scholar] [CrossRef]
- Gbinigie, O.; Allen, J.; Boylan, A.-M.; Hay, A.; Heneghan, C.; Moore, M.; Williams, N.; Butler, C. Does cranberry extract reduce antibiotic use for symptoms of acute uncomplicated urinary tract infections (CUTI)? Protocol for a feasibility study. Trials 2019, 20, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bass-Ware, A.; Weed, D.; Johnson, T.; Spurlock, A. Evaluation of the effect of cranberry juice on symptoms associated with a urinary tract infection. Urol. Nurs. 2014, 34, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Zafriri, D.; Ofek, I.; Pocino, M.; Sharon, N. Inhibition of lectin-mediated adherence of urinary isolates of Escherichia-coli by cranberry cocktail. Israel J. Med. Sci. 1988, 24, 380. [Google Scholar]
- Avorn, J.; Monane, M.; Gurwitz, J.; Glynn, R.; Choodnovsky, I.; Lipsitz, L. Reduction of bacteriuria and pyuria with cranberry beverage: A randomized trial. J. Am. Geriatr. Soc. 1993, 41, 751–754. [Google Scholar]
- Habash, M.; Van der Mei, H.; Busscher, H.; Reid, G. Adsorption of urinary components influences the zeta potential of uropathogen surfaces. Colloids Surf. B-Biointerfaces 2000, 19, 13–17. [Google Scholar] [CrossRef]
- Cranberry Extracts for Urinary Tract Infections. Available online: http://www.who.int/trialsearch/Trial2.aspx?TrialID=ISRCTN32556347 (accessed on 20 September 2020).
- Lavigne, J.P.; Bourg, G.; Combescure, C.; Botto, H.; Sotto, A. In-vitro and in-vivo evidence of dose-dependent decrease of uropathogenic Escherichia coli virulence after consumption of commercial Vaccinium macrocarpon (cranberry) capsules. Clin. Microbiol. Infect. 2008, 14, 350–355. [Google Scholar] [CrossRef]
- Di Martino, P.; Agniel, R.; David, K.; Templer, C.; Gaillard, J.; Denys, P.; Botto, H. Reduction of Escherichia coli adherence to uroepithelial bladder cells after consumption of cranberry juice: A double-blind randomized placebo-controlled cross-over trial. World J. Urol. 2006, 24, 21–27. [Google Scholar] [CrossRef]
- Avorn, J.; Monane, M.; Gurwitz, J.H.; Glynn, R.J.; Choodnovskiy, I.; Lipsitz, L.A. Reduction of bacteriuria and pyuria after ingestion of cranberry juice. JAMA 1994, 271, 751–754. [Google Scholar] [CrossRef]
- Botto, H.; Sotto, A.; Lebret, T.; Lavigne, J.P. Inhibition of E. coli adherence to uro-epithelial cells by Urell Express®(Cranberry Compund): Comparative study vs placebo in healthy volunteers. J. Urol. 2008, 179, 84–85. [Google Scholar] [CrossRef]
- Bianco, L.; Perrelli, E.; Towle, V.; Van Ness, P.H.; Juthani-Mehta, M. Pilot randomized controlled dosing study of cranberry capsules for reduction of bacteriuria plus pyuria in female nursing home residents. J. Am. Geriatr. Soc. 2012, 60, 1180–1181. [Google Scholar] [CrossRef] [Green Version]
- Howell, A.B. Bacterial anti-adhesion activity of human urine after cranberry juice or powder consumption. In Proceedings of the 238th National Meeting & Exposition, Washington DC, USA, 16–20 August 2009. [Google Scholar]
- Howell, A.B.; Botto, H.; Combescure, C.; Blanc-Potard, A.-B.; Gausa, L.; Matsumoto, T.; Tenke, P.; Sotto, A.; Lavigne, J.-P. Dosage effect on uropathogenic Escherichia coli anti-adhesion activity in urine following consumption of cranberry powder standardized for proanthocyanidin content: A multicentric randomized double blind study. BMC Infect. Dis. 2010, 10, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peron, G.; Sut, S.; Pellizzaro, A.; Brun, P.; Voinovich, D.; Castagliuolo, I.; Dall’Acqua, S. The antiadhesive activity of cranberry phytocomplex studied by metabolomics: Intestinal PAC-A metabolites but not intact PAC-A are identified as markers in active urines against uropathogenic Escherichia coli. Fitoterapia 2017, 122, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Clinical Dosage and Effectiveness Study of ShanStar® Cranberry Supplement for Prevention and Treatment against Women’s Urinary Tract Infections. Available online: http://www.who.int/trialsearch/Trial2.aspx?TrialID=ISRCTN55813586 (accessed on 5 October 2020).
- Ballester, F.S.; Vidal, V.R.; Alcina, E.L.; Perez, C.D.; Fontano, E.E.; Benavent, A.M.O.; García, A.M.; Bustamante, M.A.S. Cysticlean® a highly pac standardized content in the prevention of recurrent urinary tract infections: An observational, prospective cohort study. BMC Urol. 2013, 13, 28. [Google Scholar]
- Nieman, K.M.; Dicklin, M.R.; Schild, A.L.; Kaspar, K.L.; Khoo, C.; Derrig, L.H.; Gupta, K.; Maki, K.C. Cranberry Beverage Consumption Reduces Antibiotic Use for Clinical Urinary Tract Infection in Women with a Recent History of Urinary Tract Infection. FASEB J. 2017. [Google Scholar] [CrossRef]
- Cranberry Juice for Treatment of Urinary Tract Infections. Available online: https://clinicaltrials.gov/show/NCT00093054 (accessed on 8 October 2020).
- Avorn, J.; Monane, M.; Gurwitz, J.; Glynn, R.; Choodnovskiy, I.; Lipsitz, L. Cranberry juice’s effects on urinary tract infection. A condensed version of a Journal of the American Medical Association study on the effects of drinking cranberry juice on bacteriuria and pyuria. Community Nurse 1996, 2, 38–39. [Google Scholar]
- Avorn, J. The effect of cranberry juice on the presence of bacteria and white blood cells in the urine of elderly women. In Toward Anti-Adhesion Therapy for Microbial Diseases; Springer: Berlin, Germany, 1996; pp. 185–186. [Google Scholar]
- Stothers, L.; Brown, P.; Fenster, H.; Levine, M.; Berkowitz, J. Dose response of cranberry in the treatment of lower urinary tract infections in women: MP26-05. J. Urol. 2016, 195, E355. [Google Scholar] [CrossRef]
- Tehmas, A.; ul Haq, M.; Javed, M. Comparison of antibiotics and cranberry’s effects in people having urinary tract infection (UTI). Indo Am. J. Pharm. Sci. 2019, 6, 7233–7237. [Google Scholar]
- Placebo-Controlled Study to Evaluate the Effect of Adjuvant Treatment with Compound Cranberry Extract Tablets (UmayC) in Acute Bacterial Cystitis. Available online: https://apps.who.int/trialsearch/Trial3.aspx?trialid=NCT00305071 (accessed on 5 October 2020).
- Effect of Adjuvant Treatment with Compound Cranberry Extract Tablets in Acute Bacterial Cystitis. Available online: https://clinicaltrials.gov/show/NCT00305071 (accessed on 6 October 2020).
- Thiel, I.; Ardjomand-Woelkart, K.; Bornik, M.; Klein, T.; Kompek, A. Vaccinium macrocarpon (cranberry) reduces intake of antibiotics in the treatment of non-severe lower urinary tract infections: A drug monitoring study. Planta Med. 2015, 81, 1425. [Google Scholar] [CrossRef]
- Bass-Ware, A. The Impact of Daily Consumption of Cranberry Juice on Symptoms of Urinary Tract Infections. Ph.D. Thesis, Troy University, Troy, Alabama, USA, May 2013. [Google Scholar]
- Evaluation of Cranberry Juice on Bacteriuria and Puria in Spinal Cord Lesion. Available online: http://www.who.int/trialsearch/Trial2.aspx?TrialID=IRCT201112073912N4 (accessed on 28 September 2020).
- Papas, P.N.; Brusch, C.A.; Ceresia, G.C. Cranberry juice in the treatment of urinary tract infections. Southwest Med. 1966, 47, 17–20. [Google Scholar]
- Howell, A. In vivo evidence that cranberry proanthocyanidins inhibit adherence of P-fimbriated E. coli bacteria to uroepithelial cells. FASEB J. 2001, 15, A284. [Google Scholar]
- Single-Site, Open, Randomized Clinical Trial to Assess the Non-Inferiority of Cysticlean® versus Fosfomicina in the Treatment of Cystitis in Women in Spain. Available online: https://apps.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2018-001448-78-ES (accessed on 1 October 2020).
- Greenberg, J.A.; Newmann, S.J.; Howell, A.B. Consumption of sweetened dried cranberries versus unsweetened raisins for inhibition of uropathogenic Escherichia coli adhesion in human urine: A pilot study. J. Altern. Complement. Med. 2005, 11, 875–878. [Google Scholar] [CrossRef] [PubMed]
- Cranberries for Urinary Tract Infection. Available online: http://www.who.int/trialsearch/Trial2.aspx?TrialID=ISRCTN10399299 (accessed on 5 October 2020).
- Barbosa-Cesnik, C.; Brown, M.B.; Buxton, M.; Zhang, L.; DeBusscher, J.; Foxman, B. Cranberry juice fails to prevent recurrent urinary tract infection: Results from a randomized placebo-controlled trial. Clin. Infect. Dis. 2011, 52, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, P.; Turner, S.; Rumsby, K.; Warner, G.; Moore, M.; Lowes, J.; Smith, H.; Hawke, C.; Turner, D.; Leydon, G. Dipsticks and diagnostic algorithms in urinary tract infection: Development and validation, randomised trial, economic analysis, observational cohort and qualitative study. Health Technol. Assess. 2009, 13, 1–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sengupta, K.V.; Alluri, K.; Golakoti, T.V.; Gottumukkala, G.; Raavi, J.; Kotchrlakota, L.C.; Sigalan, S.; Dey, D.; Ghosh, S.; Chatterjee, A. A randomized, double blind, controlled, dose dependent clinical trial to evaluate the efficacy of a proanthocyanidin standardized whole cranberry (Vaccinium macrocarpon) powder on infections of the urinary tract. Curr. Bioact. Compd. 2011, 7, 39–46. [Google Scholar] [CrossRef]
- Little, P.; Turner, S.; Rumsby, K.; Warner, G.; Moore, M.; Lowes, J.A.; Smith, H.; Hawke, C.; Mullee, M. Developing clinical rules to predict urinary tract infection in primary care settings: Sensitivity and specificity of near patient tests (dipsticks) and clinical scores. Br. J. Gen. Pract. 2006, 56, 606–612. [Google Scholar] [PubMed]
- Vik, I.; Bollestad, M.; Grude, N.; Bærheim, A.; Damsgaard, E.; Neumark, T.; Bjerrum, L.; Cordoba, G.; Olsen, I.C.; Lindbæk, M. Ibuprofen versus pivmecillinam for uncomplicated urinary tract infection in women—A double-blind, randomized non-inferiority trial. PLoS Med. 2018, 15, e1002569. [Google Scholar] [CrossRef]
- Choi, S.; Oh, D.-S.; Jerng, U.M. A systematic review of the pharmacokinetic and pharmacodynamic interactions of herbal medicine with warfarin. PLoS ONE 2017, 12, e0182794. [Google Scholar] [CrossRef] [Green Version]
- Gettman, M.T.; Ogan, K.; Brinkley, L.J.; Adams-Huet, B.; Pak, C.Y.; Pearle, M.S. Effect of cranberry juice consumption on urinary stone risk factors. J. Urol. 2005, 174, 590–594. [Google Scholar] [CrossRef]
- Dumas-Mallet, E.; Button, K.S.; Boraud, T.; Gonon, F.; Munafo, M.R. Low statistical power in biomedical science: A review of three human research domains. R. Soc. Open. Sci. 2017, 4, 160254. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D.G. Comparisons against baseline within randomised groups are often used and can be highly misleading. Trials 2011, 12, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Respiratory Tract Infections (Self-Limiting): Prescribing Antibiotics. Available online: https://www.nice.org.uk/guidance/cg69 (accessed on 4 October 2020).
- Little, P.; Moore, M.; Kelly, J.; Williamson, I.; Leydon, G.; McDermott, L.; Mullee, M.; Stuart, B. Delayed antibiotic prescribing strategies for respiratory tract infections in primary care: Pragmatic, factorial, randomised controlled trial. BMJ 2014, 348, g1606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, P.; Moore, M.; Turner, S.; Rumsby, K.; Warner, G.; Lowes, J.; Smith, H.; Hawke, C.; Leydon, G.; Arscott, A. Effectiveness of five different approaches in management of urinary tract infection: Randomised controlled trial. BMJ 2010, 340, c199. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Study ID and Country | Design | Participants and Setting | Number of Participants | Age (years) | Study Duration | Intervention | Control | Results |
|---|---|---|---|---|---|---|---|---|
| Barbosa-Cesnik et al. (2011), USA [85] | Randomised placebo-controlled trial | Women with an acute UTI (three or more urinary symptoms) presenting for urinalysis at the University of Michigan Health Service laboratory with symptoms of UTI | 319 (155 received cranberry, 164 received placebo) | 18–40 | 6 months | 8 ounces of 27% low-calorie cranberry juice twice daily | 8 ounces of placebo juice twice daily | The presence of urinary and vaginal symptoms was similar between groups at 3 days and at 1–2 weeks. |
| Little et al. (2009), UK [86] | Randomised controlled trial | Non-pregnant women presenting to General Practices in South-West England with a suspected uncomplicated UTI | 309 (241 women in the juice comparisons: 75 advised to take cranberry juice, 78 advised to take orange juice, 88 advised to drink water) | 17–70 | Average follow-up time of 575 days (range 35–968 days) | Advice to drink cranberry juice | Advice to drink water | No significant impact of advice to consume cranberry juice on the duration of symptoms rated moderately bad or worse (IRR 1.18 (95% CI: 1.95 to 1.47), p = 0.13), frequency symptom severity (mean difference −0.01 (95% CI: −0.37 to 0.34), p = 0.94), severity of unwell symptoms (mean difference 0.02 (95% CI: −0.36 to 0.39), p = 0.93), use of antibiotics (odds ratio 1.27 (95% CI: 0.47 to 3.43) p = 0.64) or time to re-consultation (hazard ratio 0.74 (95% CI: 0.49 to 1.13), p = 0.17). |
| Sengupta et al. (2011), India [87] | Randomised controlled trial | Women with mild symptoms of a UTI, urine culture positive and with a negative pregnancy test | 60 (16 untreated controls, 21 received low dose cranberry, 23 received high dose cranberry) | 18–40 | 90 days | Encapsulated PAC Standardised Whole Cranberry Powder (PS-WCP)—500 (low dose) and 1000 mg (high dose) | No treatment | Significant within-group improvement of symptoms at day 10 compared to the baseline in both treatment groups, but not in the untreated controls. Significant within-group reduction in E. coli load in both treatment groups after 10 days of treatment (low dose, p < 0.01; high dose p < 0.0001; at a statistical significance level of 95%), but not in the untreated controls (p = 0.72). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gbinigie, O.A.; Spencer, E.A.; Heneghan, C.J.; Lee, J.J.; Butler, C.C. Cranberry Extract for Symptoms of Acute, Uncomplicated Urinary Tract Infection: A Systematic Review. Antibiotics 2021, 10, 12. https://doi.org/10.3390/antibiotics10010012
Gbinigie OA, Spencer EA, Heneghan CJ, Lee JJ, Butler CC. Cranberry Extract for Symptoms of Acute, Uncomplicated Urinary Tract Infection: A Systematic Review. Antibiotics. 2021; 10(1):12. https://doi.org/10.3390/antibiotics10010012
Chicago/Turabian StyleGbinigie, Oghenekome A., Elizabeth A. Spencer, Carl J. Heneghan, Joseph J. Lee, and Christopher C. Butler. 2021. "Cranberry Extract for Symptoms of Acute, Uncomplicated Urinary Tract Infection: A Systematic Review" Antibiotics 10, no. 1: 12. https://doi.org/10.3390/antibiotics10010012