
Mid-Regional Pro-Adrenomedullin as a Prognostic Factor for Severe COVID-19 ARDS
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Population Characteristics
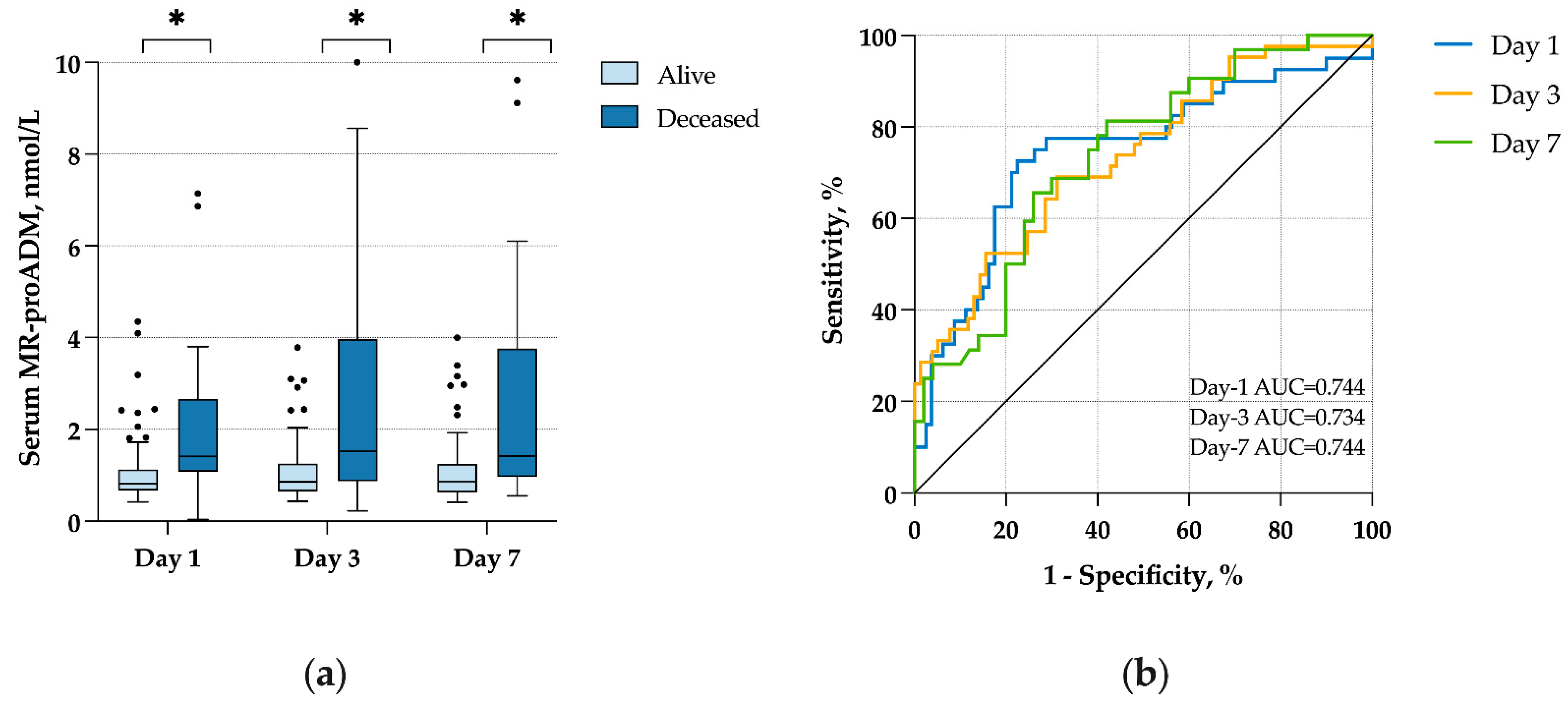
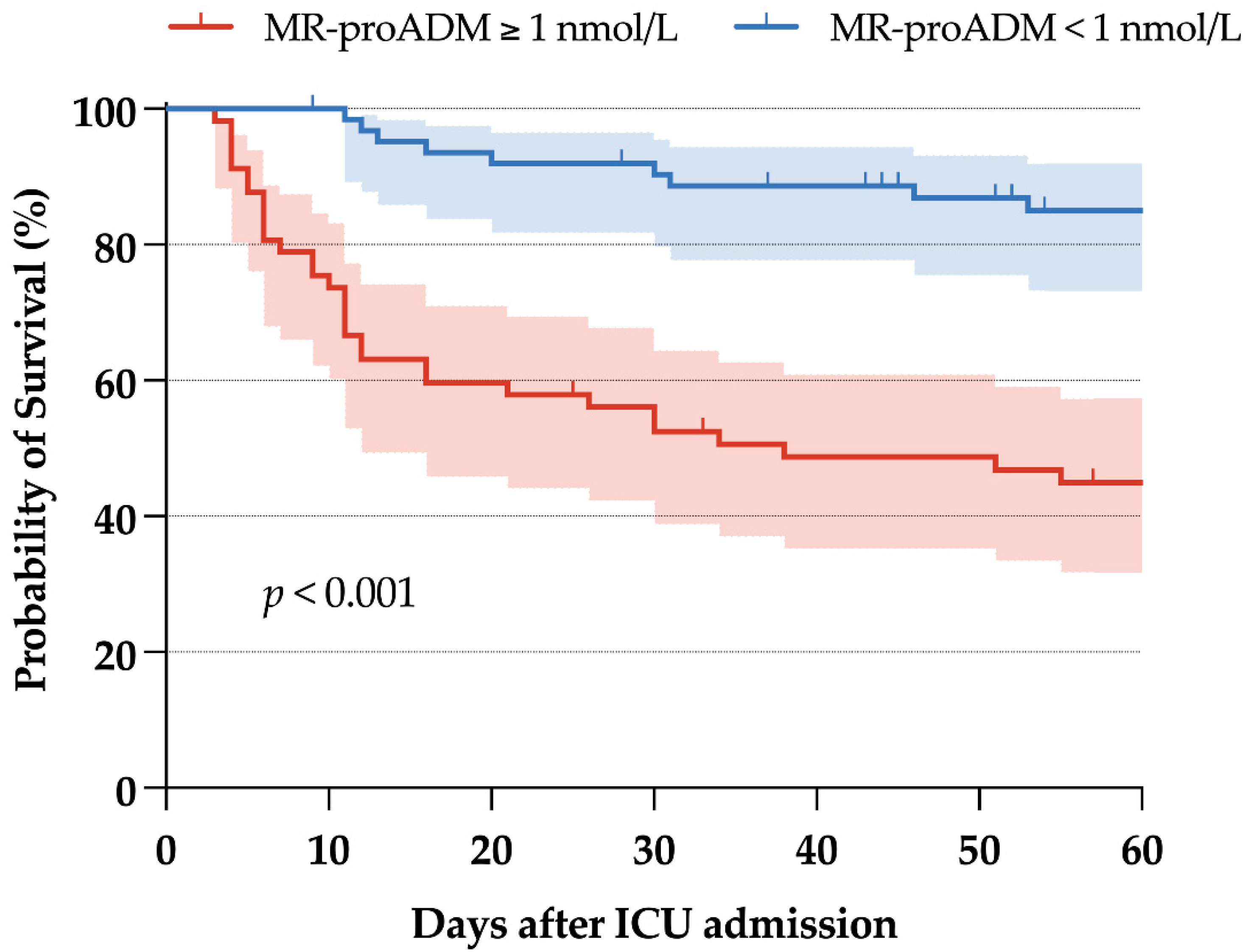
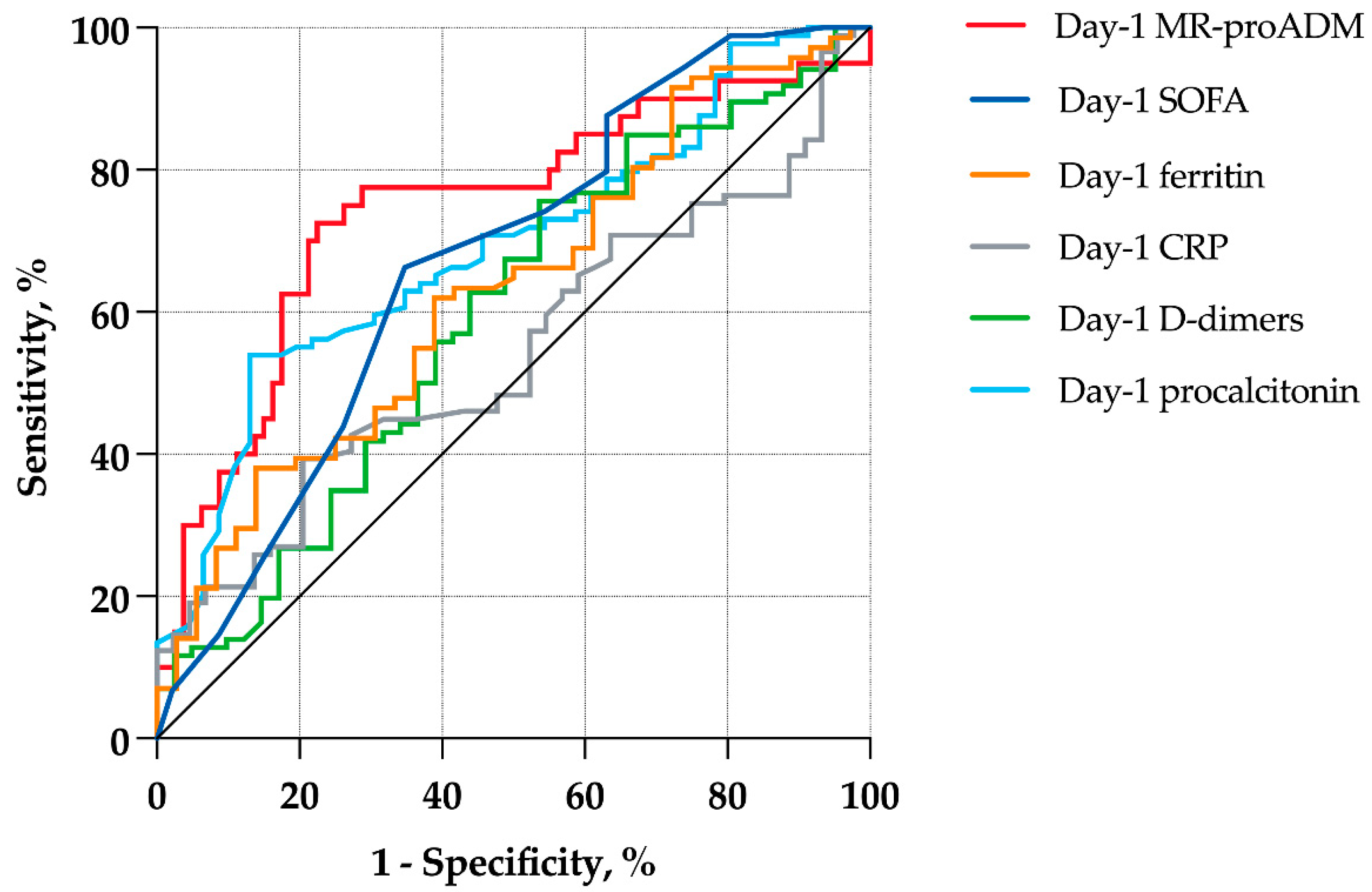
2.2. Mid-Regional Pro-Adrenomedullin and Day-60 Mortality
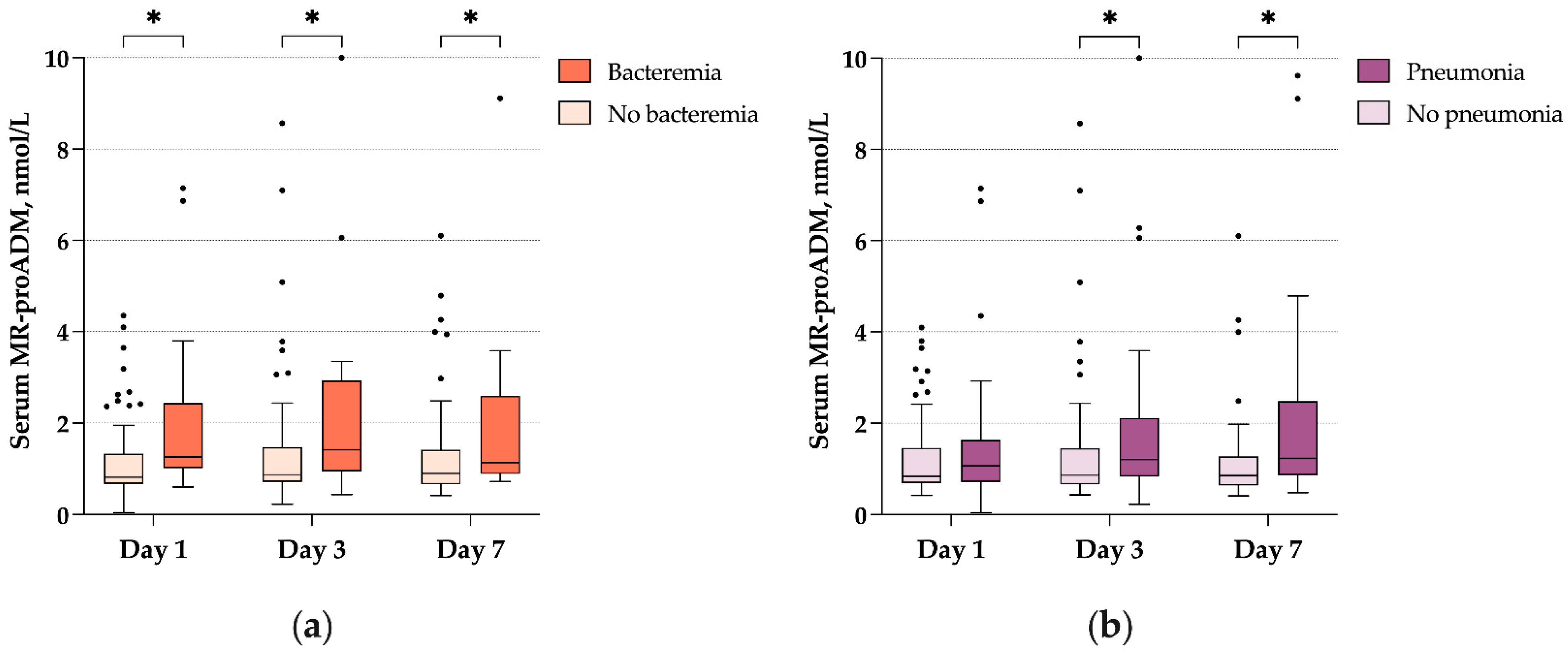
2.3. Mid-Regional Pro-Adrenomedullin and Bacterial Infections
3. Discussion
3.1. Main Findings
3.2. Interpretation
3.3. Strenghts and Limitations
4. Materials and Methods
4.1. Study Population
4.2. Data Collection and Definitions
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 22 August 2022).
- COVID-ICU Group on behalf of the REVA Network and the COVID-ICU Investigators. Clinical Characteristics and Day-90 Outcomes of 4244 Critically Ill Adults with COVID-19: A Prospective Cohort Study. Intensive Care Med. 2021, 47, 60–73. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial Cell Infection and Endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Bonaventura, A.; Vecchié, A.; Dagna, L.; Martinod, K.; Dixon, D.L.; Van Tassell, B.W.; Dentali, F.; Montecucco, F.; Massberg, S.; Levi, M.; et al. Endothelial Dysfunction and Immunothrombosis as Key Pathogenic Mechanisms in COVID-19. Nat. Rev. Immunol. 2021, 21, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Calabretta, E.; Moraleda, J.M.; Iacobelli, M.; Jara, R.; Vlodavsky, I.; O’Gorman, P.; Pagliuca, A.; Mo, C.; Baron, R.M.; Aghemo, A.; et al. COVID-19-induced Endotheliitis: Emerging Evidence and Possible Therapeutic Strategies. Br. J. Haematol. 2021, 193, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Temmesfeld-Wollbrück, B.; Brell, B.; Dávid, I.; Dorenberg, M.; Adolphs, J.; Schmeck, B.; Suttorp, N.; Hippenstiel, S. Adrenomedullin Reduces Vascular Hyperpermeability and Improves Survival in Rat Septic Shock. Intensive Care Med. 2007, 33, 703–710. [Google Scholar] [CrossRef]
- Christ-Crain, M.; Morgenthaler, N.G.; Struck, J.; Harbarth, S.; Bergmann, A.; Müller, B. Mid-Regional pro-Adrenomedullin as a Prognostic Marker in Sepsis: An Observational Study. Crit. Care 2005, 9, R816. [Google Scholar] [CrossRef] [PubMed]
- Elke, G.; Bloos, F.; Wilson, D.C.; Brunkhorst, F.M.; Briegel, J.; Reinhart, K.; Loeffler, M.; Kluge, S.; Nierhaus, A.; Jaschinski, U.; et al. The Use of Mid-Regional Proadrenomedullin to Identify Disease Severity and Treatment Response to Sepsis-a Secondary Analysis of a Large Randomised Controlled Trial. Crit. Care 2018, 22, 79. [Google Scholar] [CrossRef]
- Ara-Somohano, C.; Bonadona, A.; Carpentier, F.; Pavese, P.; Vesin, A.; Hamidfar-Roy, R.; Minet, C.; Vanzetto, G.; Schwebel, C.; Timsit, J.-F. Evaluation of Eight Biomarkers to Predict Short-Term Mortality in Patients with Acute Severe Dyspnea. Minerva Anestesiol. 2017, 83, 824–835. [Google Scholar] [CrossRef]
- Liu, D.; Xie, L.; Zhao, H.; Liu, X.; Cao, J. Prognostic Value of Mid-Regional pro-Adrenomedullin (MR-ProADM) in Patients with Community-Acquired Pneumonia: A Systematic Review and Meta-Analysis. BMC Infect. Dis. 2016, 16, 232. [Google Scholar] [CrossRef]
- Li, P.; Wang, C.; Pang, S. The Diagnostic Accuracy of Mid-Regional pro-Adrenomedullin for Sepsis: A Systematic Review and Meta-Analysis. Minerva Anestesiol. 2021, 87, 1117–1127. [Google Scholar] [CrossRef]
- Moore, N.; Williams, R.; Mori, M.; Bertolusso, B.; Vernet, G.; Lynch, J.; Philipson, P.; Ledgerwood, T.; Kidd, S.P.; Thomas, C.; et al. Mid-Regional Proadrenomedullin (MR-ProADM), C-Reactive Protein (CRP) and Other Biomarkers in the Early Identification of Disease Progression in Patients with COVID-19 in the Acute NHS Setting. J. Clin. Pathol. 2022. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Zaninotto, M.; Mion, M.M.; Marchioro, L.; Padoan, A.; Plebani, M. Endothelial Dysfunction and Mid-Regional ProAdrenomedullin: What Role in SARS-CoV-2 Infected Patients? Clin. Chim. Acta 2021, 523, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Gregoriano, C.; Koch, D.; Kutz, A.; Haubitz, S.; Conen, A.; Bernasconi, L.; Hammerer-Lercher, A.; Saeed, K.; Mueller, B.; Schuetz, P. The Vasoactive Peptide MR-pro-Adrenomedullin in COVID-19 Patients: An Observational Study. Clin. Chem. Lab. Med. 2021, 59, 995–1004. [Google Scholar] [CrossRef]
- Sozio, E.; Tascini, C.; Fabris, M.; D’Aurizio, F.; De Carlo, C.; Graziano, E.; Bassi, F.; Sbrana, F.; Ripoli, A.; Pagotto, A.; et al. MR-ProADM as Prognostic Factor of Outcome in COVID-19 Patients. Sci. Rep. 2021, 11, 5121. [Google Scholar] [CrossRef] [PubMed]
- Minieri, M.; Di Lecce, V.N.; Lia, M.S.; Maurici, M.; Bernardini, S.; Legramante, J.M. Role of MR-ProADM in the Risk Stratification of COVID-19 Patients Assessed at the Triage of the Emergency Department. Crit. Care Lond. Engl. 2021, 25, 407. [Google Scholar] [CrossRef]
- De Guadiana-Romualdo, L.G.; Martínez, M.M.; Mulero, M.D.R.; Esteban-Torrella, P.; Olivo, M.H.; García, M.J.A.; Campos-Rodríguez, V.; Sancho-Rodríguez, N.; Martínez, M.G.; Alcaraz, A.; et al. Circulating MR-ProADM Levels, as an Indicator of Endothelial Dysfunction, for Early Risk Stratification of Mid-Term Mortality in COVID-19 Patients. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2021, 111, 211–218. [Google Scholar] [CrossRef]
- Van Oers, J.A.H.; Kluiters, Y.; Bons, J.A.P.; de Jongh, M.; Pouwels, S.; Ramnarain, D.; de Lange, D.W.; de Grooth, H.-J.; Girbes, A.R.J. Endothelium-Associated Biomarkers Mid-Regional Proadrenomedullin and C-Terminal Proendothelin-1 Have Good Ability to Predict 28-Day Mortality in Critically Ill Patients with SARS-CoV-2 Pneumonia: A Prospective Cohort Study. J. Crit. Care 2021, 66, 173–180. [Google Scholar] [CrossRef]
- Oblitas, C.-M.; Galeano-Valle, F.; Ramírez-Navarro, J.; López-Cano, J.; Monterrubio-Manrique, Á.; García-Gámiz, M.; Sancho-González, M.; Arenal-López, S.; Álvarez-Sala Walther, L.-A.; Demelo-Rodríguez, P. Mid-Regional Pro-Adrenomedullin, Methemoglobin and Carboxyhemoglobin as Prognosis Biomarkers in Critically Ill Patients with COVID-19: An Observational Prospective Study. Viruses 2021, 13, 2445. [Google Scholar] [CrossRef]
- Montrucchio, G.; Sales, G.; Rumbolo, F.; Palmesino, F.; Fanelli, V.; Urbino, R.; Filippini, C.; Mengozzi, G.; Brazzi, L. Effectiveness of Mid-Regional pro-Adrenomedullin (MR-ProADM) as Prognostic Marker in COVID-19 Critically Ill Patients: An Observational Prospective Study. PLoS ONE 2021, 16, e0246771. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M. Pooled Analysis of Mid-Regional pro-Adrenomedullin Values in COVID-19 Patients with Critical Illness. Intern. Emerg. Med. 2021, 16, 1723–1725. [Google Scholar] [CrossRef]
- Musuuza, J.S.; Watson, L.; Parmasad, V.; Putman-Buehler, N.; Christensen, L.; Safdar, N. Prevalence and Outcomes of Co-Infection and Superinfection with SARS-CoV-2 and Other Pathogens: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0251170. [Google Scholar] [CrossRef] [PubMed]
- Wicky, P.-H.; Niedermann, M.S.; Timsit, J.-F. Ventilator-Associated Pneumonia in the Era of COVID-19 Pandemic: How Common and What Is the Impact? Crit. Care Lond. Engl. 2021, 25, 153. [Google Scholar] [CrossRef] [PubMed]
- Segala, F.V.; Bavaro, D.F.; Di Gennaro, F.; Salvati, F.; Marotta, C.; Saracino, A.; Murri, R.; Fantoni, M. Impact of SARS-CoV-2 Epidemic on Antimicrobial Resistance: A Literature Review. Viruses 2021, 13, 2110. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Lausen, B.; Sauerbrei, W.; Schumacher, M. Dangers of Using “Optimal” Cutpoints in the Evaluation of Prognostic Factors. J. Natl. Cancer Inst. 1994, 86, 829–835. [Google Scholar] [CrossRef]
- Spoto, S.; Cella, E.; de Cesaris, M.; Locorriere, L.; Mazzaroppi, S.; Nobile, E.; Lanotte, A.M.; Pedicino, L.; Fogolari, M.; Costantino, S.; et al. Procalcitonin and MR-Proadrenomedullin Combination with SOFA and QSOFA Scores for Sepsis Diagnosis and Prognosis: A Diagnostic Algorithm. Shock 2018, 50, 44–52. [Google Scholar] [CrossRef]
- Charles, P.-E.; Péju, E.; Dantec, A.; Bruyère, R.; Meunier-Beillard, N.; Dargent, A.; Prin, S.; Wilson, D.; Quenot, J.-P. Mr-Proadm Elevation Upon Icu Admission Predicts the Outcome of Septic Patients and Is Correlated with Upcoming Fluid Overload. Shock 2017, 48, 418–426. [Google Scholar] [CrossRef]
- Stalenhoef, J.E.; van Nieuwkoop, C.; Wilson, D.C.; van der Starre, W.E.; Delfos, N.M.; Leyten, E.M.S.; Koster, T.; Ablij, H.C.; Van’t Wout, J.J.W.; van Dissel, J.T. Biomarker Guided Triage Can Reduce Hospitalization Rate in Community Acquired Febrile Urinary Tract Infection. J. Infect. 2018, 77, 18–24. [Google Scholar] [CrossRef]
- Oussalah, A.; Lagneaux, A.-S.; Alix, T.; Filhine-Tresarrieu, P.; Callet, J.; Ferrand, J.; Jung, J.; Broseus, J.; Salignac, S.; Luc, A.; et al. Ascitic Fluid Mid-Regional-pro-Adrenomedullin (MR-pro-ADM): A Novel Rapid-Assay Sepsis Biomarker to Diagnose Spontaneous Bacterial Peritonitis in Cirrhotic Patients. J. Hepatol. 2022, 77, S905–S906. [Google Scholar] [CrossRef]
- Pickens, C.O.; Gao, C.A.; Cuttica, M.J.; Smith, S.B.; Pesce, L.L.; Grant, R.A.; Kang, M.; Morales-Nebreda, L.; Bavishi, A.A.; Arnold, J.M.; et al. Bacterial Superinfection Pneumonia in Patients Mechanically Ventilated for COVID-19 Pneumonia. Am. J. Respir. Crit. Care Med. 2021, 204, 921–932. [Google Scholar] [CrossRef]
- Bhakta, S.; Sanghavi, D.K.; Johnson, P.W.; Kunze, K.L.; Neville, M.R.; Wadei, H.M.; Bosch, W.; Carter, R.E.; Shah, S.Z.; Pollock, B.D.; et al. Clinical and Laboratory Profiles of the SARS-CoV-2 Delta Variant Compared with Pre-Delta Variants. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2022, 120, 88–95. [Google Scholar] [CrossRef]
- Bouzid, D.; Visseaux, B.; Kassasseya, C.; Daoud, A.; Fémy, F.; Hermand, C.; Truchot, J.; Beaune, S.; Javaud, N.; Peyrony, O.; et al. Comparison of Patients Infected with Delta Versus Omicron COVID-19 Variants Presenting to Paris Emergency Departments: A Retrospective Cohort Study. Ann. Intern. Med. 2022, 175, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-Related Organ Failure Assessment) Score to Describe Organ Dysfunction/Failure. On Behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Vesin, A.; Azoulay, E.; Ruckly, S.; Vignoud, L.; Rusinovà, K.; Benoit, D.; Soares, M.; Azeivedo-Maia, P.; Abroug, F.; Benbenishty, J.; et al. Reporting and Handling Missing Values in Clinical Studies in Intensive Care Units. Intensive Care Med. 2013, 39, 1396–1404. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients n = 135 | Day-60 Survivors n = 89 | Day-60 Decedents n = 46 | p | |
|---|---|---|---|---|
| Demographics and comorbidities | ||||
| Age, years | 62.7 (51.6–71.2) | 58.3 (49.2–66.1) | 71.1 (62.3–75.9) | <0.01 |
| Female gender | 43 (31.9) | 30 (33.7) | 13 (28.3) | 0.52 |
| Body Mass Index | 29 (25.8–34) | 29.6 (26.3–34) | 28.6 (24.3–31.2) | 0.09 |
| Diabetes | 40 (29.6) | 17 (19.1) | 23 (50) | <0.01 |
| Chronic diseases (Knaus ≥ 1) | 60 (44.4) | 36 (40.4) | 24 (52.2) | 0.19 |
| Immunodepression | 16 (11.9) | 5 (5.6) | 11 (23.9) | <0.01 |
| Characteristics at ICU admission | ||||
| SAPS II | 27 (21–39) | 25 (18–34) | 34 (26–48) | <0.01 |
| Time from 1st symptoms to ICU admission, days | 9 (7–12) | 9 (7–12) | 8 (7–15) | 0.80 |
| Respiratory SOFA | 3 (1–4) | 3 (1–4) | 3 (2–4) | 0.50 |
| Extra-respiratory SOFA | 1 (0–4) | 1 (0–3) | 1 (1–6) | <0.01 |
| Ventilatory status at day 1 | 0.25 | |||
| None | 27 (20) | 19 (21.3) | 8 (17.4) | . |
| NIV/HFNC/CPAP | 78 (57.8) | 54 (60.7) | 24 (52.2) | . |
| IMV/ECMO | 30 (22.2) | 16 (18) | 14 (30.4) | . |
| Steroid therapy at day 1 | 127 (94.1) | 85 (95.5) | 42 (91.3) | 0.44 |
| Laboratory data | ||||
| MR-proADM, nmol/L | ||||
| Day 1 | 1 (0.7–1.6) | 0.8 (0.7–1.1) | 1.4 (1.1–2.7) | <0.01 |
| Day 3 | 0.9 (0.7–1.7) | 0.9 (0.7–1.2) | 1.5 (0.9–3.6) | <0.01 |
| Day 7 | 1 (0.7–1.9) | 0.9 (0.6–1.2) | 1.4 (1–3.6) | <0.01 |
| IL-6 at day 1, pg/mL | 36.3 (9–88) | 29.4 (7.6–72) | 58.3 (13.2–168) | 0.11 |
| CRP at day 1, mg/L | 127 (68–177) | 129 (57–177) | 123.5 (93–172) | 0.40 |
| Procalcitonin at day 1, μg/L | 0.3 (0.1–1.4) | 0.2 (0.1–1) | 0.6 (0.3–2) | <0.01 |
| LDH at day 1, UI/L | 439 (337–573) | 427 (335.5–550) | 474 (362–632) | 0.16 |
| Lymphocytes at day 1, G/L | 0.97 (0.59–1.32) | 1.01 (0.63–1.39) | 0.85 (0.46–1.12) | 0.04 |
| D-dimers at day 1, μg/L | 916 (556–1768) | 811 (537–1431) | 1161 (667–2594) | 0.07 |
| Ferritin at day 1, μg/L | 851 (397–1668) | 804 (344–1448) | 1088 (575–2418) | 0.03 |
| Hazard Ratio | 95% Confidence Interval | p | |
|---|---|---|---|
| Landmark at day 1 (n = 135) | |||
| Day-1 MR-proADM | 1.17 | (1.06–1.28) | <0.01 |
| Day-1 CRP | 1.00 | (1–1) | 0.50 |
| Day-1 lymphocytes count | 1.00 | (1–1) | 0.28 |
| Day-1 LDH | 1.00 | (1–1) | <0.01 |
| Landmark at day 3 (n = 135) | |||
| Day-3 MR-proADM | 1.17 | (1.06–1.28) | <0.01 |
| Day-1 CRP | 1.00 | (0.99–1) | 0.50 |
| Day-1 lymphocytes count | 1.00 | (1–1) | 0.28 |
| Day-1 LDH | 1.00 | (1–1) | <0.01 |
| Landmark at day 7 (n = 128) | |||
| Day-7 MR-proADM | 1.19 | (1.1–1.31) | <0.01 |
| Day-1 CRP | 1.00 | (0.99–1) | 0.65 |
| Day-1 lymphocytes count | 1.00 | (1–1) | 0.62 |
| Day-1 LDH | 1.00 | (1–1) | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Montmollin, E.; Peoc’h, K.; Marzouk, M.; Ruckly, S.; Wicky, P.-H.; Patrier, J.; Jaquet, P.; Sonneville, R.; Bouadma, L.; Timsit, J.-F. Mid-Regional Pro-Adrenomedullin as a Prognostic Factor for Severe COVID-19 ARDS. Antibiotics 2022, 11, 1166. https://doi.org/10.3390/antibiotics11091166
de Montmollin E, Peoc’h K, Marzouk M, Ruckly S, Wicky P-H, Patrier J, Jaquet P, Sonneville R, Bouadma L, Timsit J-F. Mid-Regional Pro-Adrenomedullin as a Prognostic Factor for Severe COVID-19 ARDS. Antibiotics. 2022; 11(9):1166. https://doi.org/10.3390/antibiotics11091166
Chicago/Turabian Stylede Montmollin, Etienne, Katell Peoc’h, Mehdi Marzouk, Stéphane Ruckly, Paul-Henri Wicky, Juliette Patrier, Pierre Jaquet, Romain Sonneville, Lila Bouadma, and Jean-François Timsit. 2022. "Mid-Regional Pro-Adrenomedullin as a Prognostic Factor for Severe COVID-19 ARDS" Antibiotics 11, no. 9: 1166. https://doi.org/10.3390/antibiotics11091166