1. Introduction
Major depressive disorder (MDD) is a common disease affecting more than 300 million people every year with a 12-month prevalence of 6% [
1,
2]. The lifetime prevalence is between 15% and 18%, ultimately affecting up to one in five individuals. Contrary to popular belief, it is equally common in high- and low-income countries, regardless of culture, origin or ethnicity [
3]. Moreover, MDD is currently the main cause of disability worldwide, representing 7.5% of years lived with disability (YLD) across the globe at an estimated annual cost of over
$US 1 trillion [
2,
4].
The DSM-5 describes a major depressive episode (MDE) as the combination of depressed mood and loss of interest or pleasure in almost all activities (anhedonia) with other symptoms such as weight change, sleep disturbances (insomnia or hypersomnia), psychomotor retardation (or agitation), fatigue, …, and suicidal ideation during the same 2-week period. These symptoms should cause clinically significant distress or social impairment and should not be attributable to a psychoactive substance or to another medical condition [
5]. MDE are part of MDD or bipolar disorder (BP) if a history of (hypo-)mania is present. However, MDD cannot be reduced to these symptoms, as clinical heterogeneity is important. Indeed, depression may differ by symptom presentation (MDD with psychotic, melancholic, atypical, anxious, catatonic, or mixed features), severity, clinical course, age of onset, and response to treatment [
6,
7].
Unfortunately, despite its cost and prevalence, the treatment of MDD, which is essentially based on antidepressant drugs and psychotherapy, still has poor results [
8]. Indeed, only one-third of patients achieve complete remission after a first-line antidepressant treatment, while one-third show no clinical response. Additionally, the cumulative complete remission rate reaches only 67% after four treatment steps with current therapeutic interventions [
9,
10]. Thus, it is mandatory to identify biomarkers of MDD that may help to improve disease prognosis [
11].
One of the main issues regarding MDD is that the underlying mechanisms of the disorder remain largely unknown despite significant advances, likely contributing to the low effectiveness of care [
1]. This lack of knowledge is due to multiple factors. First, the high clinical heterogeneity of MDD is likely associated with diverse pathophysiology, leading the National Institute of Mental Health (NIMH) to propose a new classification framework to improve research discoveries and clinical outcomes [
7,
12,
13]. Second, the underlying mechanisms of MDD are associated with various biological pathways intertwined with psychological and social factors [
14].
Among the different biological pathways, the monoaminergic hypothesis was the most explored. This theory emerged with observations of the mechanisms of action of the first antidepressant drugs. Nonetheless, this model failed to sufficiently explain MDD to effectively manage it [
15,
16]. Current data suggest that genetic, epigenetic (i.e., gene-environment interactions), and neuroendocrinological (e.g., hypothalamic-pituitary-adrenal axis changes) mechanisms are equally involved in MDD [
1,
15]. Additionally, inflammatory dysregulations (i.e., the inflammatory hypothesis of depression) and neuroanatomical modifications (e.g., affecting neuroplasticity and neurogenesis, inducing structural and functional brain changes) were also described to be related to the pathophysiology of MDD [
1,
15,
17,
18].
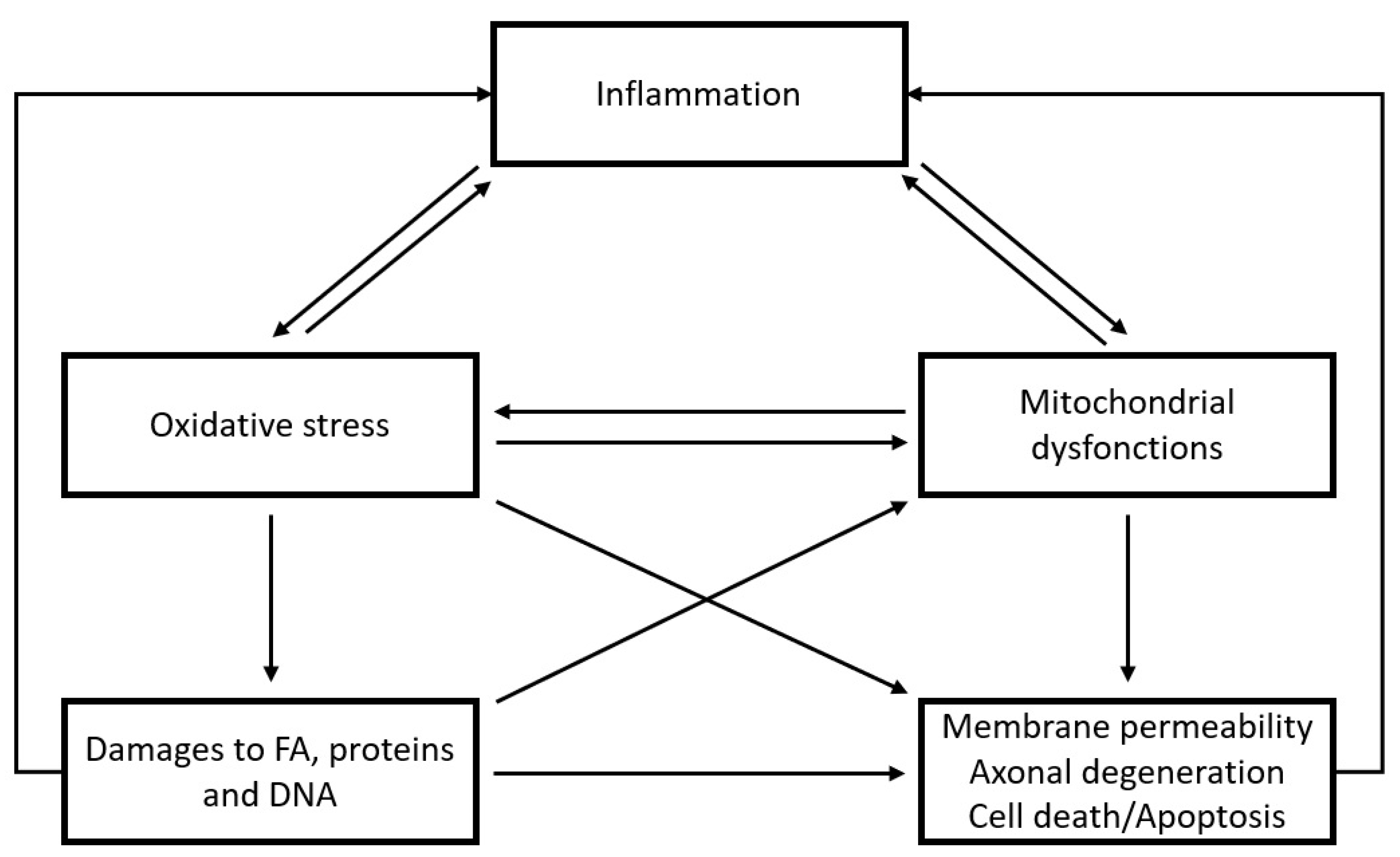
One of the main causes of neuroanatomical and inflammatory disturbances is oxidative stress [
18,
19,
20]. Oxidative stress is the consequence of an accumulation of oxidative damage when antioxidant defenses fail to counteract the effects of free radical agents (reactive oxygen species (ROS) and reactive nitrogen species (RNS)). It is sometimes referred to as “oxidated distress” as opposed to “oxidative eustress” since free radical agents are involved in physiological processes [
20,
21]. Indeed, under normal conditions, ROS and RNS are implicated in many biological pathways secondary to redox signaling (e.g., cellular growth, survival, and regulation) [
21,
22]. However, oxidative stress impairments are commonly described in disease pathophysiology. Interestingly, the brain is more vulnerable to oxidative stress due to its high metabolic rate and lower antioxidant levels [
18,
21]. Therefore, growing evidence shows the involvement of oxidative stress in brain-related diseases, such as Alzheimer’s disease, schizophrenia, and MDD [
19,
20,
23].
Hence, the first aim of this narrative review is to consolidate current data on peripheral and genetic biomarkers of oxidative stress in MDD, particularly in relation to its clinical features. The second aim is to provide a better understanding of pathophysiological processes underlying unipolar depression.
3. Results
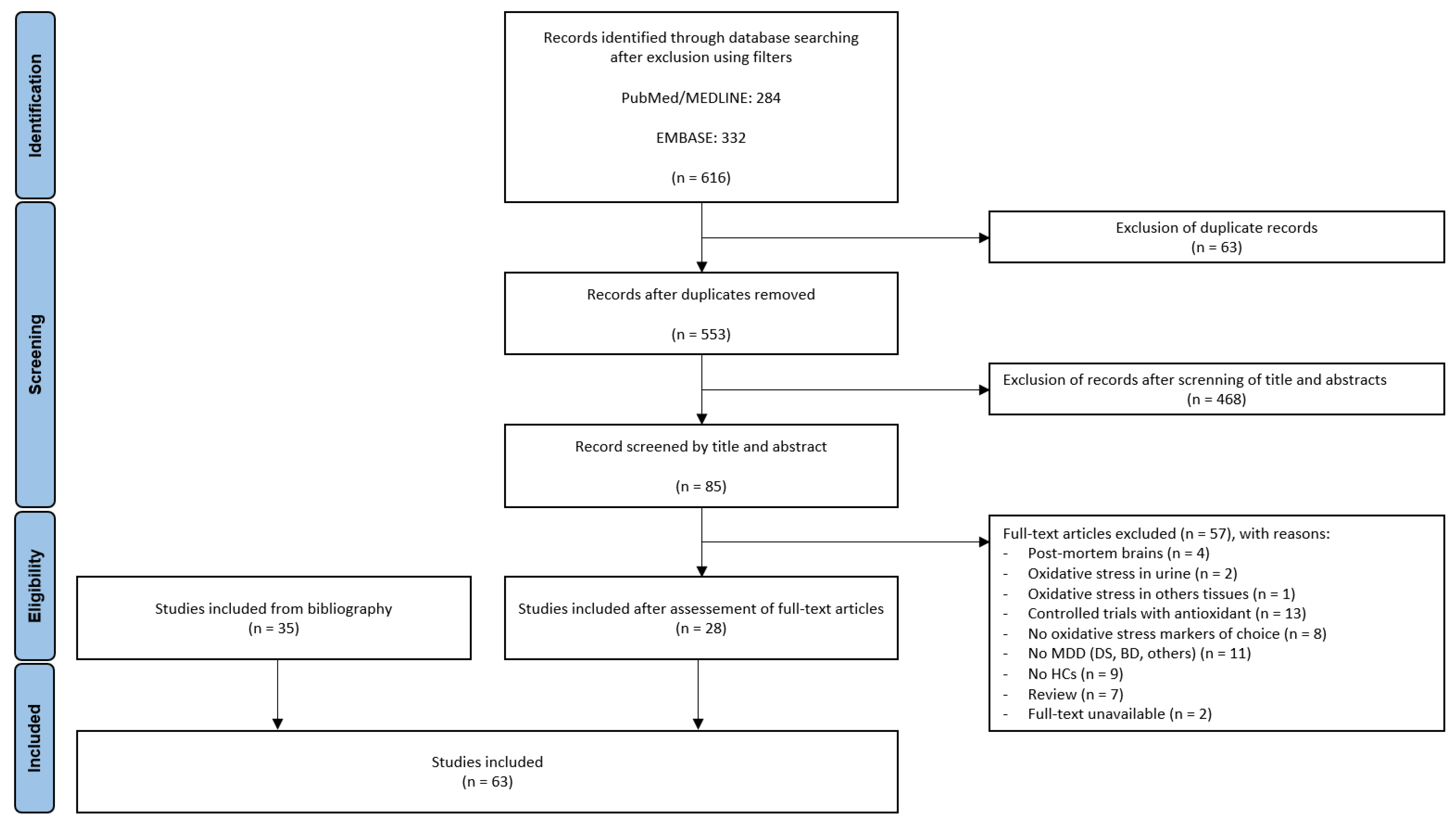
In total, 616 articles (284 from PubMed and 332 from Embase) were identified. After removing duplicate records, 553 publications were screened by their titles and abstracts. Following this first screening, 85 full-text articles were assessed for eligibility. Among them, 28 were relevant according to the criteria. Thirty-five supplemental articles identified in the bibliographies were added. Thus, 63 studies were included in this narrative review. The selected articles were comparative studies between healthy subjects and patients suffering from an MDE in the context of MDD, according to disease stage and clinical features. A summary of the biomarkers identified from the 63 articles is provided in
Table 1,
Table 2,
Table 3,
Table 4,
Table 5,
Table 6,
Table 7,
Table 8 and
Table 9. Biomarkers were grouped according to their nature (e.g., antioxidant enzymes, non-enzymatic antioxidants, ROS-producing enzymes, ROS/RNS, oxidative damage products and others), the examined biological matrix (i.e., serum, plasma, erythrocytes), and clinical characteristics.
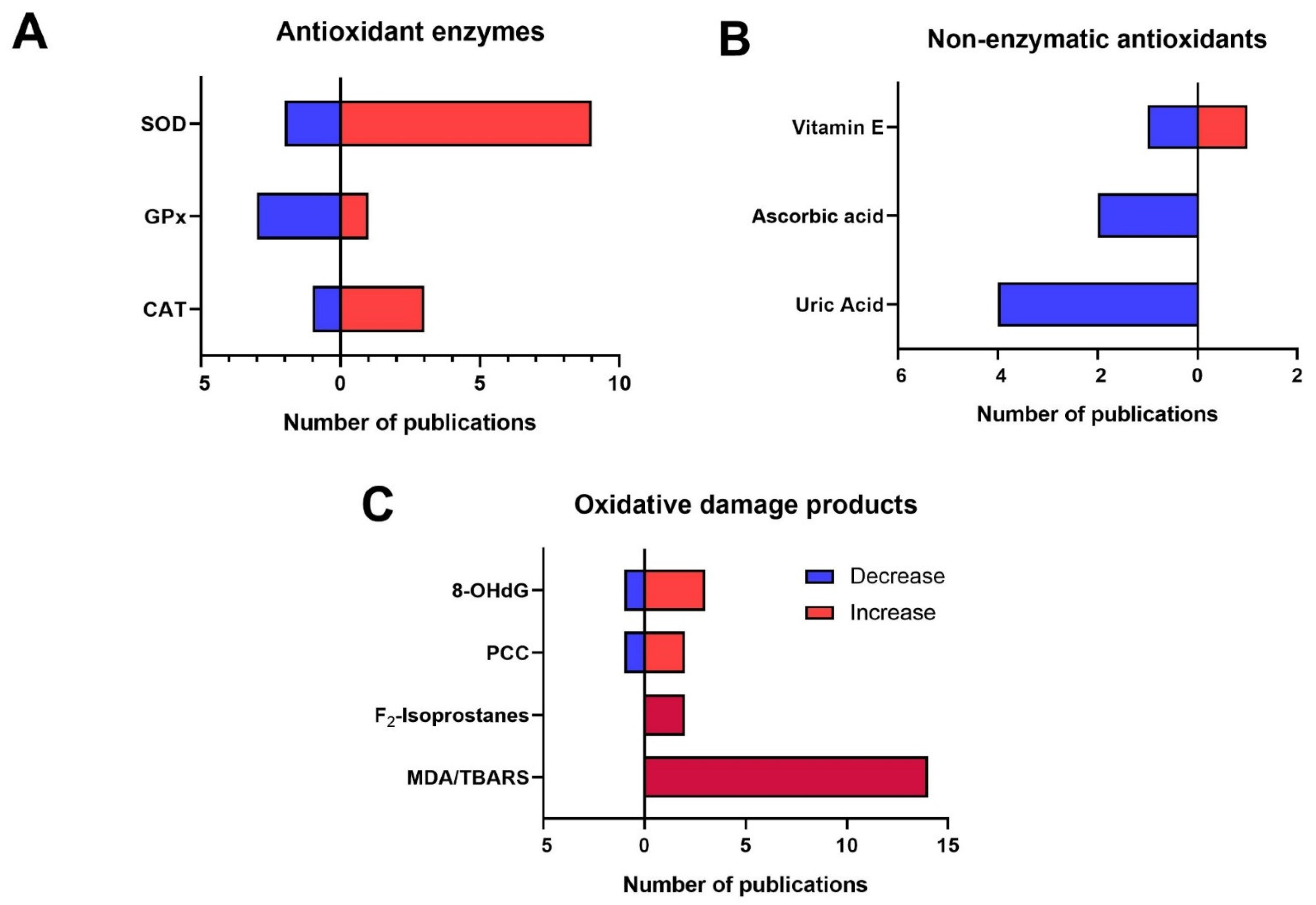
Among the 63 articles, 39 did not provide enough specific clinical information to specifically characterize the depressive episode. They were qualified as “unspecified MDD”. Globally, in depressed patients, an oxidative stress imbalance was observed with changes in antioxidant enzymes, decreases in non-enzymatic antioxidants, increases in ROS and RNS, and, accordingly, increases in oxidative damage products of DNA, lipids, and proteins (see
Table 1 and
Figure 2). Detailed results are discussed further.
For clinical features, three different clinical contexts were identified in five articles: melancholic features, psychotic features, and suicidal symptoms (i.e., suicide attempt or suicidal ideation) (see
Table 2). Although biomarker modifications were also observed in patients without melancholic features compared to healthy controls, more modifications with greater variability were observed in patients with melancholic symptoms compared to healthy controls. Similarly, more changes were observed in patients with suicidal symptoms than without. For MDD with psychotic features, no differences were highlighted between depressed patients and healthy subjects.
Three different stages of MDD were also identified: first depressive episode (see
Table 3), recurrent MDD (see
Table 4), and MDD in remission (see
Table 5). Six articles described modifications in the first MDE, revealing a decrease in antioxidant capacity and an increase in two biomarkers associated with oxidative damage (see
Table 3). Modifications in recurrent MDD were described in four articles and showed a higher level of ROS, lower levels of antioxidant enzymes, and a higher level of oxidative damage (see
Table 4). Concerning the three articles describing MDD in remission, no clear difference between patients and healthy controls was observed (see
Table 5).
Oxidative stress biomarkers were also assessed according to the severity of MDD in five articles (see
Table 6). All groups of depressed patients (i.e., mild, moderate, and severe MDD) showed increases in antioxidant enzymes and oxidative damage products compared to healthy controls. With respect to the age of MDD onset, two groups were described in five articles: child and adolescent depression and geriatric depression (see
Table 7). In child and adolescent depression, an increased total oxidant status (TOS) and a decreased total antioxidant capacity (TAC) were observed. For geriatric depression, lower antioxidant activities associated with higher levels of ROS and oxidative damage products were revealed.
Table 1.
Peripheral biomarkers of oxidative stress in unspecified MDD patients compared to healthy controls. MDD: Major depressive disorder—CAT: Catalase—GPx: Glutathion Peroxydase—SOD: Superoxide dismutase (information about isoform was not provided)—Cu/ZnSOD: Type 1 isoform of SOD—GSSG: Glutathione disulfide—GSH: Reduced form of glutathione—XO: Xanthine oxidase—H2O2: Hydrogen peroxide—NO: Nitric oxide—MDA: Malondialdehyde—TBARS—Thiobarbituric Acid-Reactive Substances—oxLDL: Oxide LDL—PCC: Protein carbonyl content—8-OHdG: 8-hydroxy-2′-deoxyguanosine—TAC: Total antioxidant capacity– TOS: Total oxidant status—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
Table 1.
Peripheral biomarkers of oxidative stress in unspecified MDD patients compared to healthy controls. MDD: Major depressive disorder—CAT: Catalase—GPx: Glutathion Peroxydase—SOD: Superoxide dismutase (information about isoform was not provided)—Cu/ZnSOD: Type 1 isoform of SOD—GSSG: Glutathione disulfide—GSH: Reduced form of glutathione—XO: Xanthine oxidase—H2O2: Hydrogen peroxide—NO: Nitric oxide—MDA: Malondialdehyde—TBARS—Thiobarbituric Acid-Reactive Substances—oxLDL: Oxide LDL—PCC: Protein carbonyl content—8-OHdG: 8-hydroxy-2′-deoxyguanosine—TAC: Total antioxidant capacity– TOS: Total oxidant status—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
| Biomarkers | Biological Matrix | Modification in MDD Patients |
|---|
| Antioxidant enzymes |
| CAT | Serum | ↗ [24,25] |
| Erythrocytes | ↗ [26], ↘ [27] |
| GPx | Serum | ↗ [24], ↘ [28], ↔ [25] |
| Plasma | ↔ [29,30] |
| Erythrocytes | ↘ [27], ↔ [26,31] |
| Whole blood | ↘ [32], ↔ [33] |
| SOD | Serum | ↗ [24,25,34,35], ↘ [28,36,37], ↔ [38,39] |
| Plasma | ↔ [29] |
| Erythrocytes | ↗ [33], ↔ [27] |
| Cu/ZnSOD | Serum | ↗ [40] |
| Erythrocytes | ↗ [26,31] |
| Non-enzymatic antioxidants |
| GSSG | Plasma | ↔ [30] |
| GSH | Plasma | ↔ [30] |
| Uric acid | Serum | ↘ [41,42,43,44], ↔ [31,45,46,47] |
| Whole blood | ↔ [33] |
| Ascorbic acid | Serum | ↘ [36], ↔ [30,31] |
| Plasma | ↘ [34], ↔ [33] |
| Vitamin E | Serum | ↘ [48], ↔ [31] |
| Plasma | ↗ [33] |
| Thiols | Plasma | ↗ [49] |
| ROS/RNS-producing enzymes |
| XO | Serum | ↗ [37] |
| NO synthase | Serum | ↗ [35] |
| Plasma | ↘ [50] |
| Reactive oxygen species (ROS) and reactive nitrogen species (RNS) |
| H2O2 | Plasma | ↗ [51] |
| NO | Serum | ↗ [39], ↔ [37] |
| Erythrocytes | ↘ [27] |
| Oxidative damage products |
| MDA/TBARS | Serum | ↗ [28,34,36,38,39,52,53], ↔ [25,35,45,47,54,55] |
| Plasma | ↗ [29,31,33,56] |
| Erythrocytes | ↗ [26,27,33] |
| F2-Isoprostanes | Serum | ↗ [57], ↔ [58] |
| Plasma | ↗ [30] |
| oxLDL | Serum | ↗ [51], ↔ [31] |
| PCC | Serum | ↗ [54,55], ↘ [25], ↔ [45,47] |
| 8-OHdG | Serum | ↗ [59], ↘ [58], ↔ [25] |
| Plasma | ↗ [30,60] |
| Others |
| TAC | Serum | ↘ [33,52,61] |
| Plasma | ↘ [44,62] |
| Erythrocytes | ↘ [26] |
| TOS | Serum | ↗ [61] |
| Plasma | ↗ [62] |
Table 2.
Peripheral biomarkers of oxidative stress in MDD patients according to clinical features compared to healthy controls. MDD: Major depressive disorder—CAT: Catalase—GPx: Glutathion Peroxydase—GR: Glutathion Reductase—SOD: Superoxide dismutase (information about isoform was not provided)—GSH: Reduced form of glutathione—MDA: Malondialdehyde—TBARS—Thiobarbituric Acid-Reactive Substances—PCC: Protein carbonyl content—TAC: Total antioxidant capacity—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
Table 2.
Peripheral biomarkers of oxidative stress in MDD patients according to clinical features compared to healthy controls. MDD: Major depressive disorder—CAT: Catalase—GPx: Glutathion Peroxydase—GR: Glutathion Reductase—SOD: Superoxide dismutase (information about isoform was not provided)—GSH: Reduced form of glutathione—MDA: Malondialdehyde—TBARS—Thiobarbituric Acid-Reactive Substances—PCC: Protein carbonyl content—TAC: Total antioxidant capacity—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
| Biomarkers | Biological Matrix | Modification in MDD |
|---|
| MDD with melancholic features |
|---|
| Antioxidant enzymes | | |
| CAT | Erythrocytes | ↔ [63] |
| GPx | Plasma | ↔ [63] |
| Erythrocytes | ↗ [63] |
| GR | Plasma | ↗ [63] |
| Erythrocytes | ↔ [63] |
| SOD | Erythrocytes | ↗ [63] |
| Oxidative damage products | | |
| MDA | Plasma | ↗ [63] |
| Erythrocytes | ↗ [63] |
| TBARS | Serum | ↗ [53], ↔ [54] |
| PCC | Serum | ↗ [54] |
| MDD without melancholic characteristics |
| Antioxidant enzymes | | |
| CAT | Erythrocytes | ↔ [63] |
| GPx | Plasma | ↔ [63] |
| Erythrocytes | ↔ [63] |
| GR | Plasma | ↔ [63] |
| Erythrocytes | ↔ [63] |
| SOD | Erythrocytes | ↗ [63] |
| Oxidative damage products | | |
| MDA | Plasma | ↗ [63] |
| Erythrocytes | ↗ [63] |
| TBARS | Serum | ↔ [54] |
| PCC | Serum | ↗ [54] |
| MDD with suicidal symptoms |
| Non-enzymatic antioxidants | | |
| Uric acid | Serum | ↘ [64] |
| Oxidative damage products | | |
| TBARS | Serum | ↗ [53] |
| MDD without suicidal symptoms |
| Non-enzymatic antioxidant | | |
| Uric acid | Serum | ↔ [64] |
| MDD with psychotic features |
| Antioxidant enzymes | | |
| GPx | Erythrocytes | ↔ [65] |
| Non-enzymatic antioxidants | | |
| GSH | Erythrocytes | ↔ [65] |
| Oxidative damage products | | |
| LOOH | Plasma | ↔ [65] |
| Others | | |
| TAC | Plasma | ↔ [65] |
Table 3.
Peripheral biomarkers of oxidative stress in patients with a first major depressive episode compared to healthy controls. MDE: Major depressive episode—CAT: Catalase—GPx: Glutathion Peroxydase—GST: Glutathion-S-Transferase—SOD: Superoxide dismutase (information about isoform was not provided)—Cu/ZnSOD: Type 1 isoform of SOD—MDA: Malondialdehyde—8-OHdG: 8-hydroxy-2′-deoxyguanosine—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
Table 3.
Peripheral biomarkers of oxidative stress in patients with a first major depressive episode compared to healthy controls. MDE: Major depressive episode—CAT: Catalase—GPx: Glutathion Peroxydase—GST: Glutathion-S-Transferase—SOD: Superoxide dismutase (information about isoform was not provided)—Cu/ZnSOD: Type 1 isoform of SOD—MDA: Malondialdehyde—8-OHdG: 8-hydroxy-2′-deoxyguanosine—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
| Biomarkers | Biological Matrix | Modification in First MDE |
|---|
| Antioxidant enzymes |
| CAT | Erythrocytes | ↔ [66] |
| GPx | Serum | ↔ [28] |
| GST | Serum | ↔ [67] |
| SOD | Serum | ↘ [28], ↔ [38] |
| Plasma | ↔ [67] |
| Erythrocytes | ↘ [66] |
| Cu/ZnSOD | Plasma | ↗ [68] |
| Oxidative damage products |
| MDA | Serum | ↔ [28] |
| Plasma | ↗ [66], ↔ [67] |
| 8-OHdG | Serum | ↗ [59] |
Table 4.
Peripheral biomarkers of oxidative stress in recurrent MDD patients compared to healthy controls. rcMDD: Recurrent major depressive disorder—GPx: Glutathion Peroxydase—GR: Glutathion Reductase—SOD: Superoxide dismutase (information about isoform was not provided)—Cu/ZnSOD: Type 1 isoform of SOD—MnSOD: Type 2 isoform of SOD—GSH: Reduced form of glutathione—H2O2: Hydrogen peroxide—MDA: Malondialdehyde—8-OHdG: 8-hydroxy-2′-deoxyguanosine—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
Table 4.
Peripheral biomarkers of oxidative stress in recurrent MDD patients compared to healthy controls. rcMDD: Recurrent major depressive disorder—GPx: Glutathion Peroxydase—GR: Glutathion Reductase—SOD: Superoxide dismutase (information about isoform was not provided)—Cu/ZnSOD: Type 1 isoform of SOD—MnSOD: Type 2 isoform of SOD—GSH: Reduced form of glutathione—H2O2: Hydrogen peroxide—MDA: Malondialdehyde—8-OHdG: 8-hydroxy-2′-deoxyguanosine—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
| Biomarkers | Biological Matrix | Modification in rcMDD |
|---|
| Antioxidant enzymes |
| GPx | Serum | ↘ [28] |
| Erythrocytes | ↘ [69] |
| GR | Erythrocytes | ↗ [69] |
| SOD | Serum | ↘ [28] |
| Cu/ZnSOD | Erythrocytes | ↘ [69] |
| MnSOD | Serum | ↘ [70] |
| Non-enzymatic antioxidants |
| GSH | Whole blood | ↗ [69] |
| Reactive oxygen species (ROS) |
| H2O2 | Plasma | ↗ [69] |
| Oxidative damage products |
| MDA | Serum | ↗ [28] |
| Erythrocytes | ↗ [69] |
| 8-OHdG | Serum | ↗ [59] |
Table 5.
Peripheral biomarkers of oxidative stress in MDD patients in remission compared to healthy controls. rMDD: Major depressive disorder in remission—GPx: Glutathion Peroxydase—SOD: Superoxide dismutase (information about isoform was not provided)—MDA: Malondialdehyde—TBARS—Thiobarbituric Acid-Reactive Substances—8-OHdG: 8-hydroxy-2′-deoxyguanosine—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
Table 5.
Peripheral biomarkers of oxidative stress in MDD patients in remission compared to healthy controls. rMDD: Major depressive disorder in remission—GPx: Glutathion Peroxydase—SOD: Superoxide dismutase (information about isoform was not provided)—MDA: Malondialdehyde—TBARS—Thiobarbituric Acid-Reactive Substances—8-OHdG: 8-hydroxy-2′-deoxyguanosine—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
| Biomarkers | Biological Matrix | Modification in rMDD |
|---|
| Antioxidant enzymes |
| GPx | Plasma | ↔ [29] |
| SOD | Plasma | ↔ [29] |
| Non-enzymatic antioxidants |
| Uric acid | Serum | ↘ [71] |
| Oxidative damage products |
| MDA/TBARS | Plasma | ↔ [29] |
| F2-Isoprostanes | Plasma | ↔ [58] |
| 8-OHdG | Plasma | ↔ [58] |
Table 6.
Peripheral biomarkers of oxidative stress according to severity of MDD patients compared to healthy controls. MDD: Major depressive disorder—GR: Glutathion Reductase—SOD: Superoxide dismutase (information about isoform was not provided)—MDA: Malondialdehyde—oxLDL: Oxide LDL—8-OhdG: 8-hydroxy-2′-deoxyguanosine—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
Table 6.
Peripheral biomarkers of oxidative stress according to severity of MDD patients compared to healthy controls. MDD: Major depressive disorder—GR: Glutathion Reductase—SOD: Superoxide dismutase (information about isoform was not provided)—MDA: Malondialdehyde—oxLDL: Oxide LDL—8-OhdG: 8-hydroxy-2′-deoxyguanosine—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
| Biomarkers | Biological Matrix | Modifications in MDD |
|---|
| | | Mild MDD | Moderate MDD | Severe MDD |
|---|
| Antioxidant enzymes | | | | |
| GR | Plasma | ↗ [72] | ↗ [72] | ↗ [72] |
| SOD | Erythrocytes | ↗ [33] | ↗ [33] | ↗ [33] |
| ROS/RNS-producing enzymes | | | | |
| NO synthase | Plasma | ↗ [73] | ↗ [73] | ↗ [73] |
| Oxidative damage products | | | | |
| MDA | Serum | ↗ [74] | ↗ [74] | ↗ [74] |
| Plasma | ↗ [33] | ↗ [33] | ↗ [33] |
| Erythrocytes | ↗ [33] | ↗ [33] | ↗ [33] |
| OxLDL | Plasma | ↗ [72] | ↗ [72] | ↗ [72] |
| 8-OhdG | Serum | ↔ [59] | | ↗ [59] |
Table 7.
Peripheral biomarkers of oxidative stress in MDD patients according to the disorder onset compared to healthy controls. MDD: Major depressive disorder—GPx: Glutathion Peroxydase—GR: Glutathion Reductase—GST: Glutathion-S-Transferase—SOD: Superoxide dismutase (information about type was not provided)—GSH: Reduced form of glutathione—NO: Nitric oxide—MDA: Malondialdehyde—TBARS—Thiobarbituric Acid-Reactive Substances—PCC: Protein carbonyl content—TAC: Total antioxidant capacity—TOS: Total oxidant status—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
Table 7.
Peripheral biomarkers of oxidative stress in MDD patients according to the disorder onset compared to healthy controls. MDD: Major depressive disorder—GPx: Glutathion Peroxydase—GR: Glutathion Reductase—GST: Glutathion-S-Transferase—SOD: Superoxide dismutase (information about type was not provided)—GSH: Reduced form of glutathione—NO: Nitric oxide—MDA: Malondialdehyde—TBARS—Thiobarbituric Acid-Reactive Substances—PCC: Protein carbonyl content—TAC: Total antioxidant capacity—TOS: Total oxidant status—↗: Values significantly higher in depressed patients compared to controls—↘: Values significantly lower in depressed patients compared to controls—↔: No significant difference between depressed patients and controls.
| Biomarkers | Biological Matrix | Modification in MDD |
|---|
| Child and adolescent depression |
|---|
| Antioxidant enzymes | | |
| SOD | Serum | ↘ [75] |
| Non-enzymatic antioxidants | | |
| Uric acid | Serum | ↗ [76] |
| Oxidative damage products | | |
| MDA | Serum | ↗ [75] |
| Others | | |
| TAC | Serum | ↘ [75] |
| TOS | Serum | ↗ [75] |
| Geriatric depression |
| Antioxidant enzymes | | |
| GPx | Plasma | ↘ [77] |
| GR | Plasma | ↔ [77] |
| GST | Plasma | ↔ [77] |
| SOD | Serum | ↘ [78] |
| Non-enzymatic antioxidants | | |
| GSH | Serum | ↘ [78] |
| ROS & RNS | | |
| NO | Serum | ↗ [78] |
| Oxidative damage products | | |
| F2-Isoprostanes | Plasma | ↗ [77,79] |
| TBARS | Plasma | ↔ [77] |
| PCC | Serum | ↗ [78] |
| Plasma | ↔ [77] |
Of note, among the 63 studies, 18 realized pre- and post-treatment follow-up of patients and described changes in biomarkers of oxidative stress after an antidepressant treatment in patients with unipolar depression, while the other studies were only cross-sectional studies. Results in
Table 8 described parameter values in depressed patients before and after treatment, independently of clinical features and stage of the disorder (see
Table 8). Thus, no clear difference in antioxidant enzymes was observed. As well, increases in non-enzymatic antioxidants were found. Reduced levels of ROS and oxidative damage products were also identified in depressed patients after antidepressant treatment compared to before.
Table 8.
Evolution of peripheral biomarkers of oxidative stress in MDD patients after antidepressant treatment. MDD: Major depressive disorder—CAT: Catalase—GPx: Glutathion Peroxydase—GR: Glutathion Reductase—GST: Glutathion-S-Transferase—SOD: Superoxide dismutase (information about isoform was not provided)—Cu/ZnSOD: Type 1 isoform of SOD—GSSG: Glutathione disulfide—GSH: Reduced form of glutathione—XO: Xanthine oxidase—H2O2: Hydrogen peroxide—NO: Nitric oxide—MDA: Malondialdehyde—TBARS—Thiobarbituric Acid-Reactive Substances—oxLDL: Oxide LDL—PCC: Protein carbonyl content—8-OHdG: 8-hydroxy-2′-deoxyguanosine—TAC: Total antioxidant capacity—TOS: Total oxidant status—↗: Values significantly higher in depressed patients after treatment compared to before—↘: Values significantly lower in depressed patients after treatment compared to before—↔: No significant difference between depressed patients after treatment compared to before.
Table 8.
Evolution of peripheral biomarkers of oxidative stress in MDD patients after antidepressant treatment. MDD: Major depressive disorder—CAT: Catalase—GPx: Glutathion Peroxydase—GR: Glutathion Reductase—GST: Glutathion-S-Transferase—SOD: Superoxide dismutase (information about isoform was not provided)—Cu/ZnSOD: Type 1 isoform of SOD—GSSG: Glutathione disulfide—GSH: Reduced form of glutathione—XO: Xanthine oxidase—H2O2: Hydrogen peroxide—NO: Nitric oxide—MDA: Malondialdehyde—TBARS—Thiobarbituric Acid-Reactive Substances—oxLDL: Oxide LDL—PCC: Protein carbonyl content—8-OHdG: 8-hydroxy-2′-deoxyguanosine—TAC: Total antioxidant capacity—TOS: Total oxidant status—↗: Values significantly higher in depressed patients after treatment compared to before—↘: Values significantly lower in depressed patients after treatment compared to before—↔: No significant difference between depressed patients after treatment compared to before.
| Biomarkers | Biological Matrix | Modification after Treatment |
|---|
| Antioxidant enzymes |
| CAT | Serum | ↔ [25] |
| Erythrocytes | ↔ [26,27,63] |
| GPx | Serum | ↘ [28], ↔ [25] |
| Plasma | ↘ [63], ↔ [30] |
| Erythrocytes | ↗ [27], ↔ [26,31,63] |
| Whole blood | ↔ [33] |
| GR | Plasma | ↘ [63] |
| Erythrocytes | ↔ [63] |
| GST | Serum | ↔ [67] |
| SOD | Serum | ↗ [37], ↘ [28,34], ↔ [25,67] |
| Erythrocytes | ↘ [31,63], ↔ [27,33] |
| Cu/ZnSOD | Erythrocytes | ↔ [26] |
| Non-enzymatic antioxidants |
| GSSG | Plasma | ↔ [30] |
| GSH | Plasma | ↔ [30] |
| Uric acid | Serum | ↗ [41], ↔ [31] |
| Whole blood | ↔ [33] |
| Ascorbic acid | Serum | ↔ [30] |
| Plasma | ↗ [34], ↔ [31,33] |
| Vitamin E | Plasma | ↔ [31,33] |
| ROS-producing enzymes |
| XO | Serum | ↘ [37] |
| NO synthase | Plasma | ↗ [50] |
| Reactive oxygen species (ROS) and reactive nitrogen species (RNS) |
| NO | Serum | ↘ [37] |
| Oxidative damage products |
| MDA/TBARS | Serum | ↘ [34], ↗ [28], ↔ [25,52] |
| Plasma | ↘ [63], ↔ [33,67] |
| Erythrocytes | ↘ [26,63], ↔ [27,33] |
| F2-Isoprostanes | Plasma | ↔ [30,58] |
| oxLDL | Serum | ↔ [31] |
| PCC | Serum | ↔ [25] |
| 8-OHdG | Serum | ↔ [25] |
| Plasma | ↘ [58,60], ↗ [30] |
| Others |
| TAC | Serum | ↗ [61], ↔ [52] |
| Plasma | ↔ [26,33,62] |
| TOS | Serum | ↘ [61] |
| Plasma | ↔ [62] |
Finally, concerning the genetics of enzymes involved in oxidative stress, eight polymorphisms (two of
SOD2, one of
GPX1, one of
GPX4, two of
CAT, one of
GSTM1 and one of
GSTT1) were assessed in seven articles (see
Table 9). Among them, one of
SOD2 (rs4880), one of
CAT (rs7943316), and those of
GPX1,
GPX4,
GSTM1, and
GSTT1 were described as associated with MDD prevalence. Nonetheless, most of these results have not been replicated in independent cohorts.
Table 9.
Associations between genetic polymorphisms of antioxidant enzymes and the prevalence of MDD. MDD: Major depressive disorder—CAT: coding for catalase—GPX: coding for glutathione peroxidase—GST: coding for glutathione-S-Transferase—SOD2: coding for MnSOD.
Table 9.
Associations between genetic polymorphisms of antioxidant enzymes and the prevalence of MDD. MDD: Major depressive disorder—CAT: coding for catalase—GPX: coding for glutathione peroxidase—GST: coding for glutathione-S-Transferase—SOD2: coding for MnSOD.
| Genes | Genetic Polymorphisms | Associations with MDD |
|---|
| | | Protective Effect | Risk Factor | No Association |
|---|
| CAT | rs7943316 | | x [80] | |
| | rs1001179 | | | x [81] |
| GPX1 | rs1050450 | x [82] | | |
| GPX4 | rs713041 | x [80] | | |
| GSTM1 | Gene deletion | x [83] | | x [84] |
| GSTT1 | Gene deletion | x [83] | | x [84] |
| SOD2 | rs4880 | x [80,85] | | x [82,86] |
| | rs1141718 | | | x [85] |
Figure 2.
Number of publications according to modifications evidenced in main peripheral biomarkers of oxidative stress in unspecified MDD patients compared to healthy controls. MDD: Major depressive disorder—CAT: Catalase—GPx: Glutathion Peroxydase—SOD: Superoxide dismutase (information about isoform was not provided)—MDA: Malondialdehyde—TBARS—Thiobarbituric Acid-Reactive Substances—PCC: Protein carbonyl content—8-OHdG: 8-hydroxy-2′-deoxyguanosine. (A) According to the antioxidant enzymes. (B) According to the non-enzymatic antioxidants. (C) According to the oxidative damage products.
Figure 2.
Number of publications according to modifications evidenced in main peripheral biomarkers of oxidative stress in unspecified MDD patients compared to healthy controls. MDD: Major depressive disorder—CAT: Catalase—GPx: Glutathion Peroxydase—SOD: Superoxide dismutase (information about isoform was not provided)—MDA: Malondialdehyde—TBARS—Thiobarbituric Acid-Reactive Substances—PCC: Protein carbonyl content—8-OHdG: 8-hydroxy-2′-deoxyguanosine. (A) According to the antioxidant enzymes. (B) According to the non-enzymatic antioxidants. (C) According to the oxidative damage products.

 ,
, 
{kind=link}
{kind=link}
{kind=link}


