Hydroxytyrosol Supplementation Modifies Plasma Levels of Tissue Inhibitor of Metallopeptidase 1 in Women with Breast Cancer

 , , ,
, , ,
Abstract
:1. Introduction
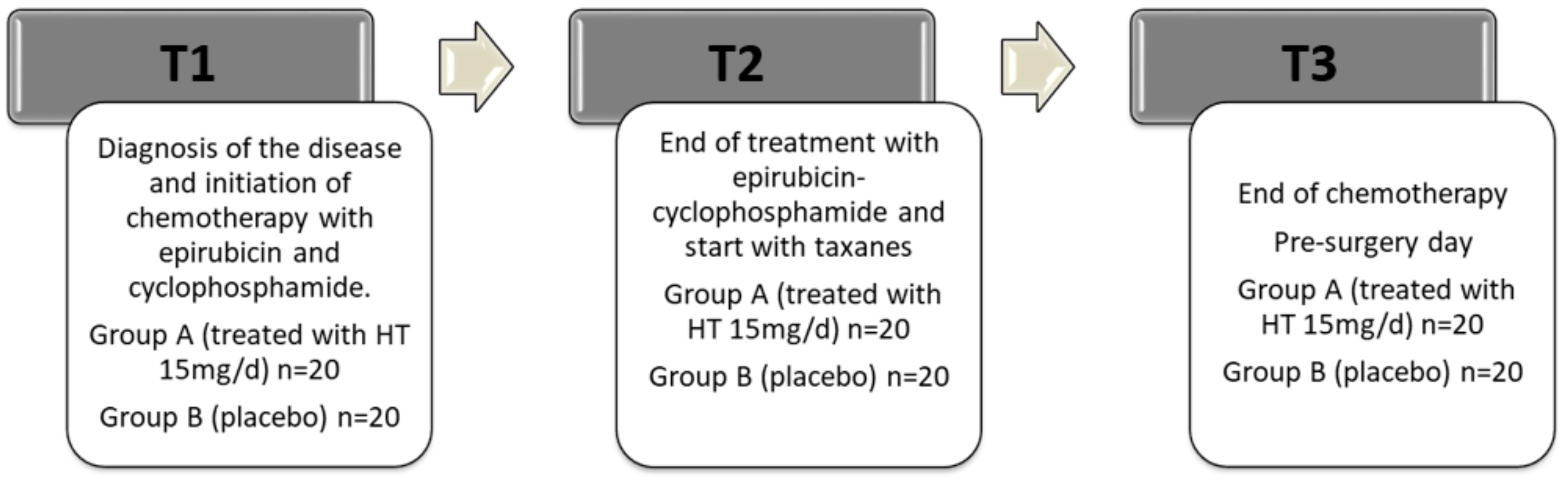
2. Materials and Methods
2.1. Plasma Metalloproteinase-9 (MMP-9) Assay
2.2. Plasma Tissue Inhibitor of Metalloproteinases-1 (TIMP-1) Assay
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Population and Homogeneity of the Experimental Groups at the Beginning of the Study
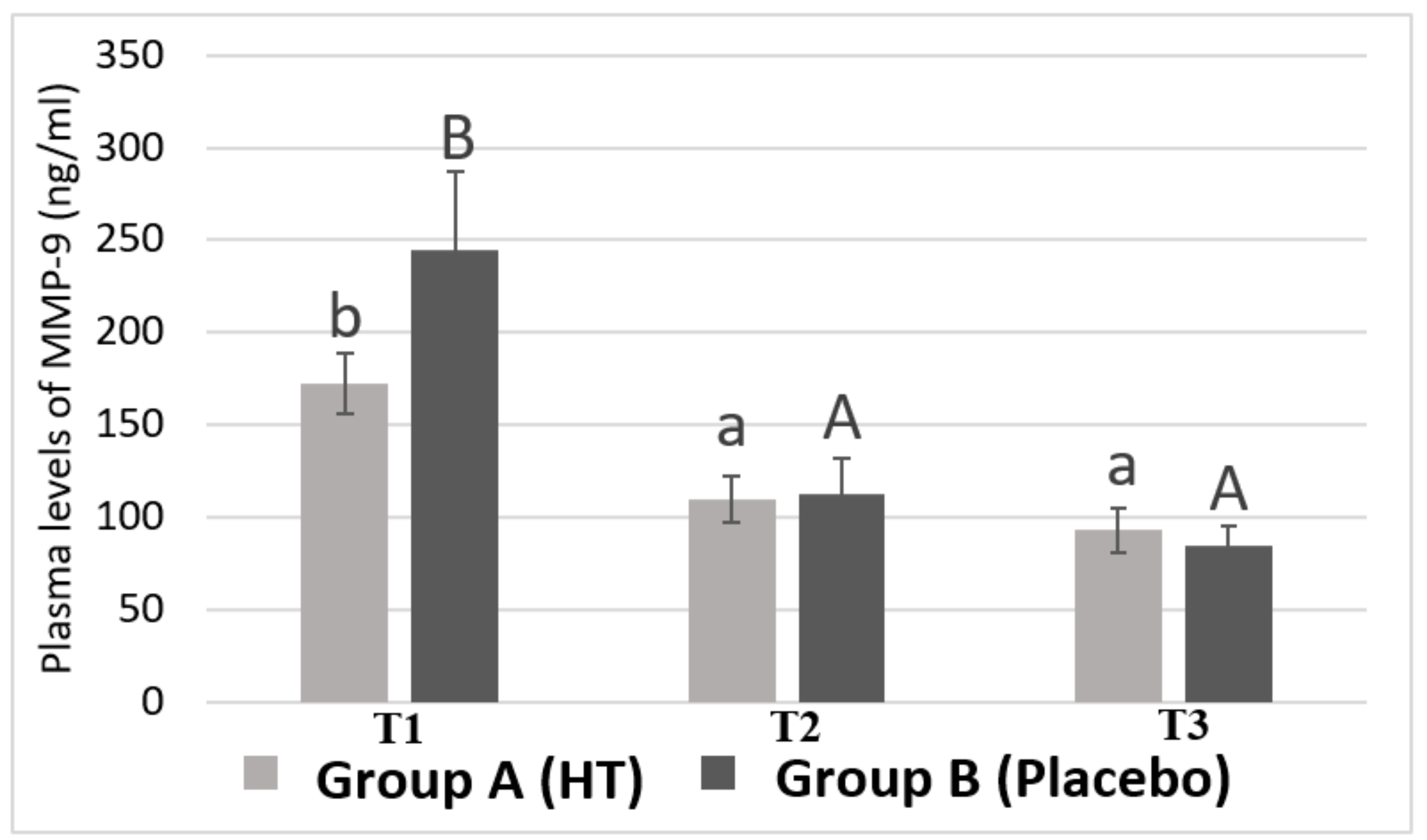
3.2. Plasma Levels of MMP-9 in Breast Cancer Patients
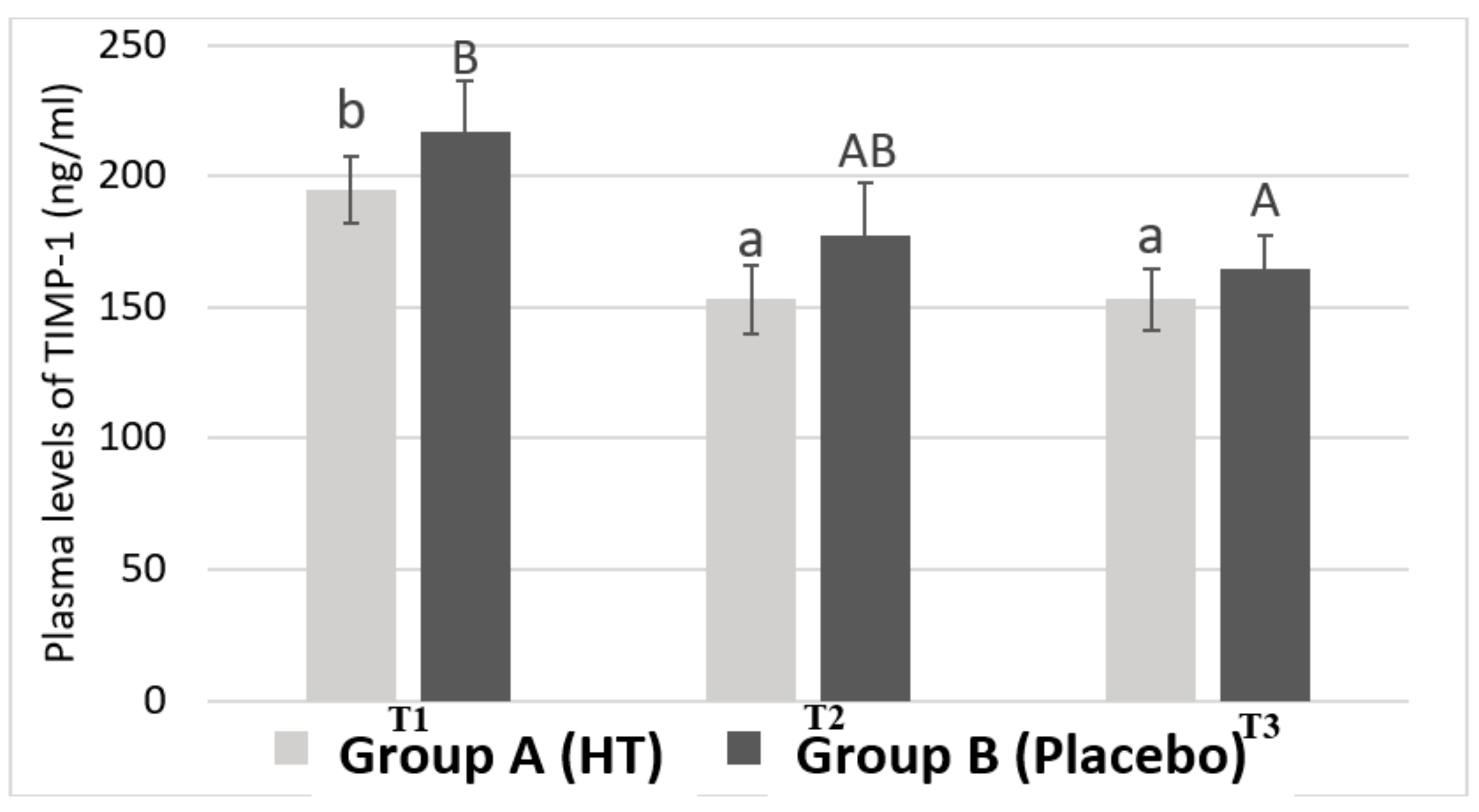
3.3. Plasma Levels of TIMP-1 in Breast Cancer Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vera-Ramirez, L.; Ramirez-Tortosa, M.C.; Perez-Lopez, P.; Granados-Principal, S.; Battino, M.; Quiles, J.L. Long-term effects of systemic cancer treatment on DNA oxidative damage: The potential for targeted therapies. Cancer Lett. 2012, 327, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Vera-Ramirez, L.; Sanchez-Rovira, P.; Ramirez-Tortosa, M.C.; Ramirez-Tortosa, C.L.; Granados-Principal, S.; Lorente, L.A.; Quiles, J.L. Oxidative stress status in metastatic breast cancer patients receiving palliative chemotherapy and its impact on survival rates. Free Radic. Res. 2012, 46, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Júnior, A.; Paz, M.; Da Silva, L.; Carvalho, S.; Sobral, A.; Machado, K. Serum Oxidative Stress Markers and Genotoxic Profile Induced by Chemotherapy in Patients with Breast Cancer: A Pilot Study. Oxidative Med. Cell. Longev. 2015. [Google Scholar] [CrossRef]
- Tong, L.; Chuang, C.; Wu, S.; Zuo, L. Reactive oxygen species in redox cancer therapy. Cancer Lett. 2015, 367, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Hecht, F.; Pessoa, C.; Gentile, L.; Rosenthal, D.; Carvalho, D.; Fortunato, R. The role of oxidative stress on breast cancer development and therapy. Tumor Biol. 2016, 37, 4281–4291. [Google Scholar] [CrossRef] [PubMed]
- Valko, M.; Rhodes, C.J.; Moncol, J.; Izakovic, M.; Mazur, M. Free radicals, metals and antioxidants in oxidative stress-induced cancer. Chem. Biol. Interact. 2006, 160, 1–40. [Google Scholar] [CrossRef] [PubMed]
- Comito, G.; Calvani, M.; Giannoni, E.; Bianchini, F.; Calorini, L.; Torre, E. HIF-1α stabilization by mitochondrial ROS promotes Met-dependent invasive growth and vasculogenic mimicry in melanoma cells. Free Radic. Biol. Med. 2011, 51, 893–904. [Google Scholar] [CrossRef] [PubMed]
- Huang, H. Matrix metalloproteinase-9 (MMP-9) as a cancer biomarker and MMP-9 biosensor: Recent advances. Sensors 2018, 18, 3249. [Google Scholar] [CrossRef]
- Granados-Principal, S.; El-Azem, N.; Pamplona, R.; Ramirez-Tortosa, C.; Pulido-Moran, M.; Vera-Ramirez, L.; Quiles, J.L.; Sanchez-Rovira, P.; Naudí, A.; Portero-Otin, M.; et al. Hydroxytyrosol ameliorates oxidative stress and mitochondrial dysfunction in doxorubicin-induced cardiotoxicity in rats with breast cancer. Biochem. Pharmacol. 2014, 90, 25–33. [Google Scholar] [CrossRef]
- Ramirez-Tortosa, M.C.; Pulido-Moran, M.; Granados, S.; Gaforio, J.J.; Quiles, J.L. Hydroxytyrosol as a Component of the Mediterranean Diet and Its Role in Disease Prevention. In The Mediterranean Diet: An Evidence-Based Approach; Preedy, V.R.W., Watson, R.R., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; Volume 1, pp. 205–215. [Google Scholar]
- Robles-Almazan, M.; Pulido-Moran, M.; Moreno-Fernandez, J.; Ramirez-Tortosa, C.; Rodriguez-Garcia, C.; Quiles, J.L.; Ramirez-Tortosa, M. Hydroxytyrosol: Bioavailability, toxicity, and clinical applications. Food Res. Int. 2018, 105, 654–667. [Google Scholar] [CrossRef]
- Echevarría, F.; Ortiz, M.; Videla, L.A. Hydroxytyrosol and cytoprotectin: A projection for clinical interventions. Int. J. Mol. Sci. 2017, 18, 930. [Google Scholar] [CrossRef]
- Rosignoli, P.; Fuccelli, R.; Sepporta, M.V.; Fabiani, R. In Vitro chemo-preventive activities of hydroxytyrosol: The main phenolic compound present in extra-virgin olive oil. Food Funct. 2016, 7, 301–307. [Google Scholar] [CrossRef] [PubMed]
- El-Azem, N.; Pulido-Moran, M.; Ramirez-Tortosa, C.L.; Quiles, J.L.; Cara, F.E.; Sanchez-Rovira, P.; Granados-Principal, S.; Ramirez-Tortosa, M.C. Modulation by hydroxytyrosol of oxidative stress and antitumor activities of paclitaxel in breast cancer. Eur. J. Nutr. 2019, 58, 1203–1211. [Google Scholar] [CrossRef]
- Granados-Principal, S.; Quiles, J.L.; Ramirez-Tortosa, C.; Camacho-Corencia, P.; Sánchez-Rovira, P.; Vera-Ramírez, L.; Ramírez-Tortosa, M.C. Hydroxytyrosol inhibits growth and cell proliferation and promotes high expression of sfrp4 in rat mammary tumours. Mol. Nutr. Food Res. 2011, 55, 117–126. [Google Scholar] [CrossRef]
- Gonzalez-Avila, G.; Sommer, B.; Mendoza-Posada, D.A.; Ramos, C.; Garcia-Hernandez, A.A.; Falfan-Valencia, R. Matrix metalloproteinases participation in the metastatic process and their diagnostic and therapeutic applications in cancer. Crit. Rev. Oncol./Hematol. 2019, 137, 57–83. [Google Scholar] [CrossRef] [PubMed]
- Javadian, M.; Gharibi, T.; Shekari, N.; Abdollahpour-Alitappeh, M.; Mohammadi, A.; Hossieni, A.; Mohammadi, H.; Kazemi, T. The role of microRNAs regulating the expression of matrix metalloproteinases (MMPs) in breast cancer development, progression, and metastasis. J. Cell. Physiol. 2019, 234, 5399–5412. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Liu, X.; Yang, F.; Liu, T.; Yan, Q.; Yang, X. By inhibiting Ras/Raf/ERK and MMP-9, knockdown of EpCAM inhibits breast cancer cell growth and metastasis. Oncotarget 2015, 6, 27187–27198. [Google Scholar] [CrossRef]
- Scarpa, S.; Vasaturo, F.; Solai, F.; Malacrino, C.; Nardo, T.; Vincenzi, B.; Modesti, M. Plasma levels of matrix metalloproteinases 2 and 9 correlate with histological grade in breast cancer patients. Oncol. Lett. 2012, 5, 316–320. [Google Scholar] [Green Version]
- Lawicki, S.; Głażewska, E.; Sobolewska, M.; Będkowska, G.; Szmitkowski, M. Plasma Levels and Diagnostic Utility of Macrophage Colony-Stimulating Factor, Matrix Metalloproteinase-9, and Tissue Inhibitor of Metalloproteinases-1 as New Biomarkers of Breast Cancer. Ann. Lab. Med. 2016, 36, 223–229. [Google Scholar] [CrossRef]
- Jackson, H.W.; Defamie, V.; Waterhouse, P.; Khokha, R. TIMPs: Versatile extracellular regulators in cancer. Nat. Rev. Cancer 2017, 17, 38–53. [Google Scholar] [CrossRef]
- Grunwald, B.; Schoeps, B.; Kruger, A. Recognizing the molecular multifunctionality and interactome of TIMP-1. Trends Cell Biol. 2019, 29. [Google Scholar] [CrossRef] [PubMed]
- Lawicki, S.; Zajkowska, M.; Glazewska, E.K.; Bedkowska, G.E.; Szmitkowski, M. Plasma levels and diagnostic utility of VEGF, MMP-9 and TIMP-1 in the diagnosis of patients with breast cancer. Onco Targets Ther. 2016, 9, 911–919. [Google Scholar] [PubMed]
- Schrohl, A.; Mueller, V.; Christensen, I.; Pantel, K.; Thomssen, C.; Bruenner, N. A Comparative Study of Tissue Inhibitor of Metalloproteinases-1 Levels in Plasma and Tumour Tissue from Patients with Primary Breast Cancer and in Plasma from Patients with Metastatic Breast Cancer. Tumor Biol. 2008, 29, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Vera-Ramirez, L.; Sanchez-Rovira, P.; Ramirez-Tortosa, M.C.; Ramirez-Tortosa, C.L.; Granados-Principal, S.; Fernandez-Navarro, M.; Lorente, J.A.; Quiles, J.L. Does chemotherapy-induced oxidative stress improve the survival rates of breast cancer patients? Antioxid. Redox Signal. 2012, 15, 903–909. [Google Scholar] [CrossRef] [PubMed]
- García-Vilas, J.; Quesada, A.; Medina, M. Hydroxytyrosol targets extracellular matrix remodeling by endothelial cells and inhibits both Ex Vivo and In Vivo angiogenesis. Food Chem. 2017, 221, 1741–1746. [Google Scholar] [CrossRef] [PubMed]
- Scoditti, E.; Nestola, A.; Massaro, M.; Calabriso, N.; Storelli, C.; De Caterina, R.; Carluccio, M. Hydroxytyrosol suppresses MMP-9 and COX-2 activity and expression in activated human monocytes via PKCα and PKCβ1 inhibition. Atherosclerosis 2014, 32, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Coskun, U.; Yamac, D.; Gulbahar, O.; Sancak, B.; Karaman, N.; Ozkan, S. Locally advanced breast carcinoma treated with neoadjuvant chemotherapy: Are the changes in serum levels of YKL-40, MMP-2 and MMP-9 correlated with tumor response? Neoplasma 2007, 54, 348–352. [Google Scholar] [PubMed]
- Wang, X.; Zhao, Z.; Chen, M.; Yuan, Q.; Li, Y.; Jiang, C. Epirubicin inhibits growth and alters the malignant phenotype of the U-87 glioma cell line. Mol. Med. Rep. 2015, 12, 5917–5923. [Google Scholar] [CrossRef]
- Karakiulakis, G.; Missirlis, E.; Maragoudakis, M.E. Basement membrane collagen-degrading activity from a malignant tumour is inhibited by anthracycline antibiotics. Biochim. Biophys. Acta 1990, 1035, 218–222. [Google Scholar] [CrossRef]
- Hursting, S.D.; Hursting, M.J. Growth signals, inflammations, and vascular perturbations: Mechanistic links between obesity, metabolic syndrome and cancer. Arterioscler. Thormb. Vasc. Biol. 2012, 32, 1766–1770. [Google Scholar] [CrossRef]
- Illesca, P.; Valenzuela, R.; Espinosa, A.; Echeverria, F.; Soto-Alarcon, S.; Ortiz, M.; Videla, L.A. Hydroxytyrosol supplementation ameliorates the metabolic disturbances in white adipose tissue from mice fed a high-fat diet through recovery of transcription factor Nrf2, SREBP-1C, PPAR-gamma and NF-KB. Biomed. Pharmacother. 2019, 109, 2472–2481. [Google Scholar] [CrossRef] [PubMed]
- Valenzuel, R.; Illesca, P.; Echeverria, F.; Espinosa, A.; Rincon-Cervera, M.A.; Ortiz, M.; Hernandez-Rodas, M.C.; Valenzuela, A.; Videla, L.A. Molecular adaptations underlying the beneficial effects of hydroxytyrosol in the pathogenic alterations induced by a high-fat diet in mouse liver PPAR-a and Nrf2 activation and NF-kB down-regulation. Food Funct. 2017, 8, 1526–1537. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Tao, Q.; Sun, M.; Wu, J.Z.; Yang, W.; Jian, P.; Peng, J.; Hu, Y.; Liu, C.; Liu, P. Kupffer cell are associated with apoptosis, inflammations and fibrotic effects in hepatic fibrosis in rats. Lab. Investig. 2010, 90, 1805–1816. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.R.; Leco, K.J.; Beatudry, P.P.; Atadja, P.W.; Veillette, C.; Riabowol, K.T. Differential effects of transforming growth factor-beta 1 on the expression of matrix metallo protinases and tissue inhibitiors of metalloproteinases in young and old human fibroblast. Exp. Gerontol. 1996, 31, 207–223. [Google Scholar] [CrossRef]
- Saber, S.; Goda, R.; El-Tanbouly, G.S.; Ezzat, D. Lisinopril inhibits nuclear transcription factor kappa B and augments sensitivity to silymarin in experimental liver fibrosis. Int. Immunopharmacol. 2018, 64, 340–349. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Group A (Hydroxytyrosol) | Group B (Placebo) | p Value | ||
|---|---|---|---|---|---|
| % | % | ||||
| Age (years) | 51.20 ± 2.02 | - | 50.85 ± 1.80 | - | 0.80 |
| Weight (Kg) | 68.05 ± 3.13 | - | 68.34 ± 2.90 | - | 0.88 |
| BMI | 26.67 ± 1.11 | - | 27.57 ± 1.31 | - | 0.91 |
| % Estrogen Receptor (biopsy) | 92.75 ± 2.47 | - | 86.15 ± 5.55 | - | 0.53 |
| % Progesterone Receptor (biopsy) | 57.55 ± 8.02 | 39.8 ± 8.07 | 0.12 | ||
| % Ki67 (biopsy) | 21.79 ± 3.34 | - | 32.90 ± 5.11 | - | 0.14 |
| Subtypes of breast cancer (biopsy) | % Luminal A | - | 50 | - | 25 |
| % Luminal B | - | 50 | - | 75 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramirez-Tortosa, C.; Sanchez, A.; Perez-Ramirez, C.; Quiles, J.L.; Robles-Almazan, M.; Pulido-Moran, M.; Sanchez-Rovira, P.; Ramirez-Tortosa, M. Hydroxytyrosol Supplementation Modifies Plasma Levels of Tissue Inhibitor of Metallopeptidase 1 in Women with Breast Cancer. Antioxidants 2019, 8, 393. https://doi.org/10.3390/antiox8090393
Ramirez-Tortosa C, Sanchez A, Perez-Ramirez C, Quiles JL, Robles-Almazan M, Pulido-Moran M, Sanchez-Rovira P, Ramirez-Tortosa M. Hydroxytyrosol Supplementation Modifies Plasma Levels of Tissue Inhibitor of Metallopeptidase 1 in Women with Breast Cancer. Antioxidants. 2019; 8(9):393. https://doi.org/10.3390/antiox8090393
Chicago/Turabian StyleRamirez-Tortosa, Cesar, Ana Sanchez, Cristina Perez-Ramirez, Jose Luis Quiles, María Robles-Almazan, Mario Pulido-Moran, Pedro Sanchez-Rovira, and MCarmen Ramirez-Tortosa. 2019. "Hydroxytyrosol Supplementation Modifies Plasma Levels of Tissue Inhibitor of Metallopeptidase 1 in Women with Breast Cancer" Antioxidants 8, no. 9: 393. https://doi.org/10.3390/antiox8090393