
Hand Exoskeleton—Development of Own Concept
 , , , , , , , , , ,
, , , , , , , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Featured Application
Abstract
1. Introduction
2. State-of-the-Art in the Area of Hand Exoskeletons
2.1. Impact of Medical Hand Exoskeletons on Patient Recovery
2.2. Specificity of Hand Exoskeletons Manufactured Using 3D Printing
3. Own Hand Exoskeleton
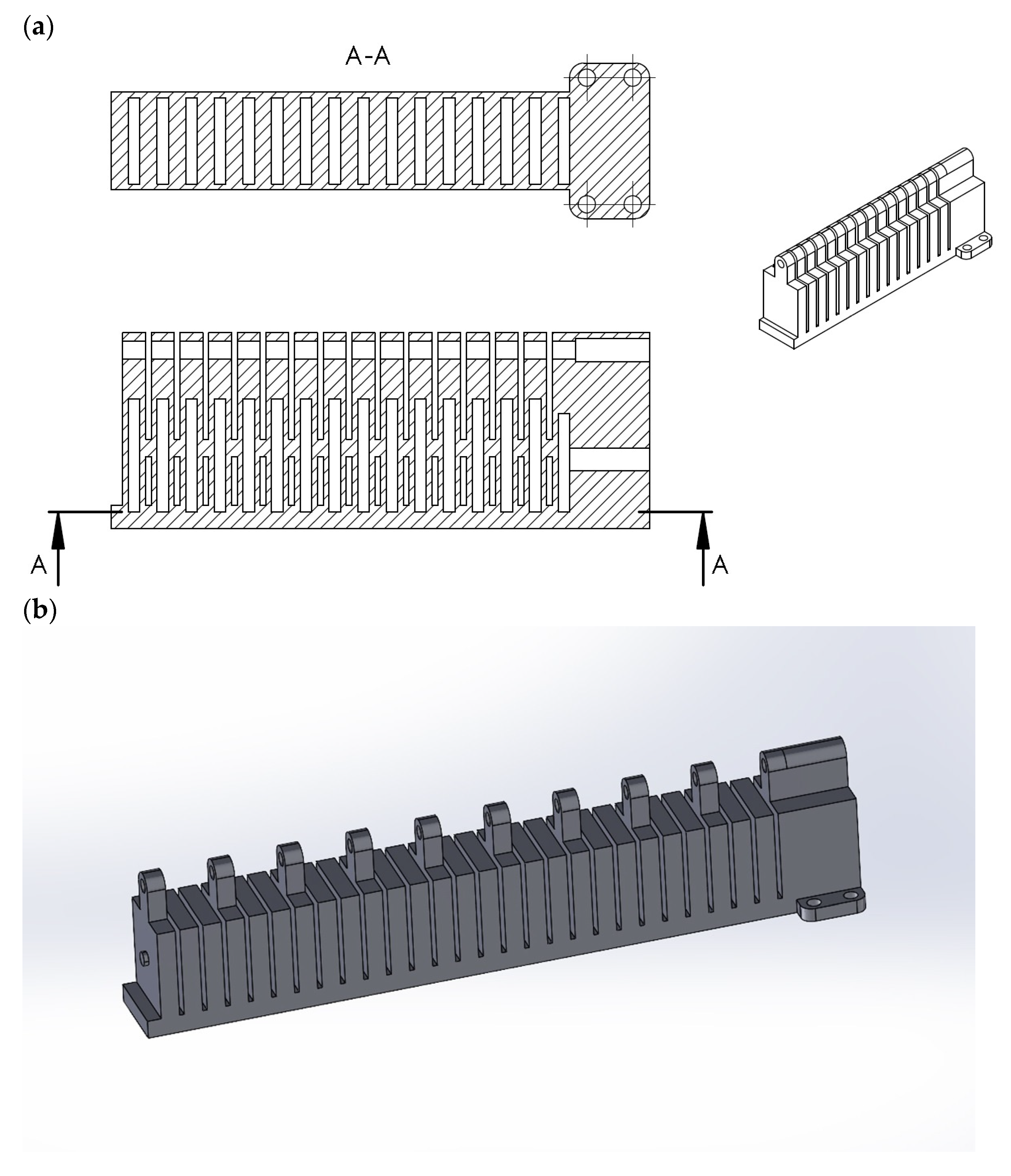
3.1. Design
3.2. Features
- Product type: BioFlex F3DFilament;
- Diameter: 1.75 mm (±0.03 mm);
- Net weight: 1 kg (±2%);
- Printing temperature: 200 °C to 225 °C;
- Nozzle type: steel, in sizes from 0.4 mm to 0.8 mm;
- Worktable: Glass/PC/COROPad;
- Table temperature: 60–80 °C;
- Closed chamber: no;
- Adhesive agent: StickIt;
- Retraction: no;
- Print cooling: maximum 80%.
- Example print parameters for Original Prusai3 MK3S+, 0.4 mm nozzle:
- Nozzle temperature: 230 °C;
- Table temperature: 50 °C;
- Retraction: 0.8 mm; 35 mm/s.;
- Print cooling: max. 50%.
- Equivalent strain (ESTRN) ESTRN = 2 [(ε1 + ε2)/3](1/2)
- where:
- ε1 = 0.5 [(EPSX−ε*)2 + (EPSY − ε*)2 + (EPSZ − ε*)2]
- ε2 = [(GMXY)2 + (GMXZ)2 + (GMYZ)2]/4
- ε* = (EPSX + EPSY + EPSZ)/3
- Total Strain Energy = ∑ [(SX * EPSX + SY * EPSY + SZ * EPSZ + TXY * GMXY + TXZ * GMXZ + TYZ * GMYZ) * Vol(i) * W(i)/2] for I =1, N int
- N int are the integration points (or Gaussian points),
- W(i) is the weighted constant at the integration point, i,
- and
- (SX = X normal stress, SY = Y normal stress, SZ = Z normal stress, TXY = Shear in the Y direction on the YZ plane, TXZ = Shear in the Z direction on the YZ plane, and TYZ = Shear in the Z direction on the XZ plane);
- Strain energy density = Total Strain Energy/Volume where Volume = ∑ [Vol(i) * W(i)], i = 1, N int.
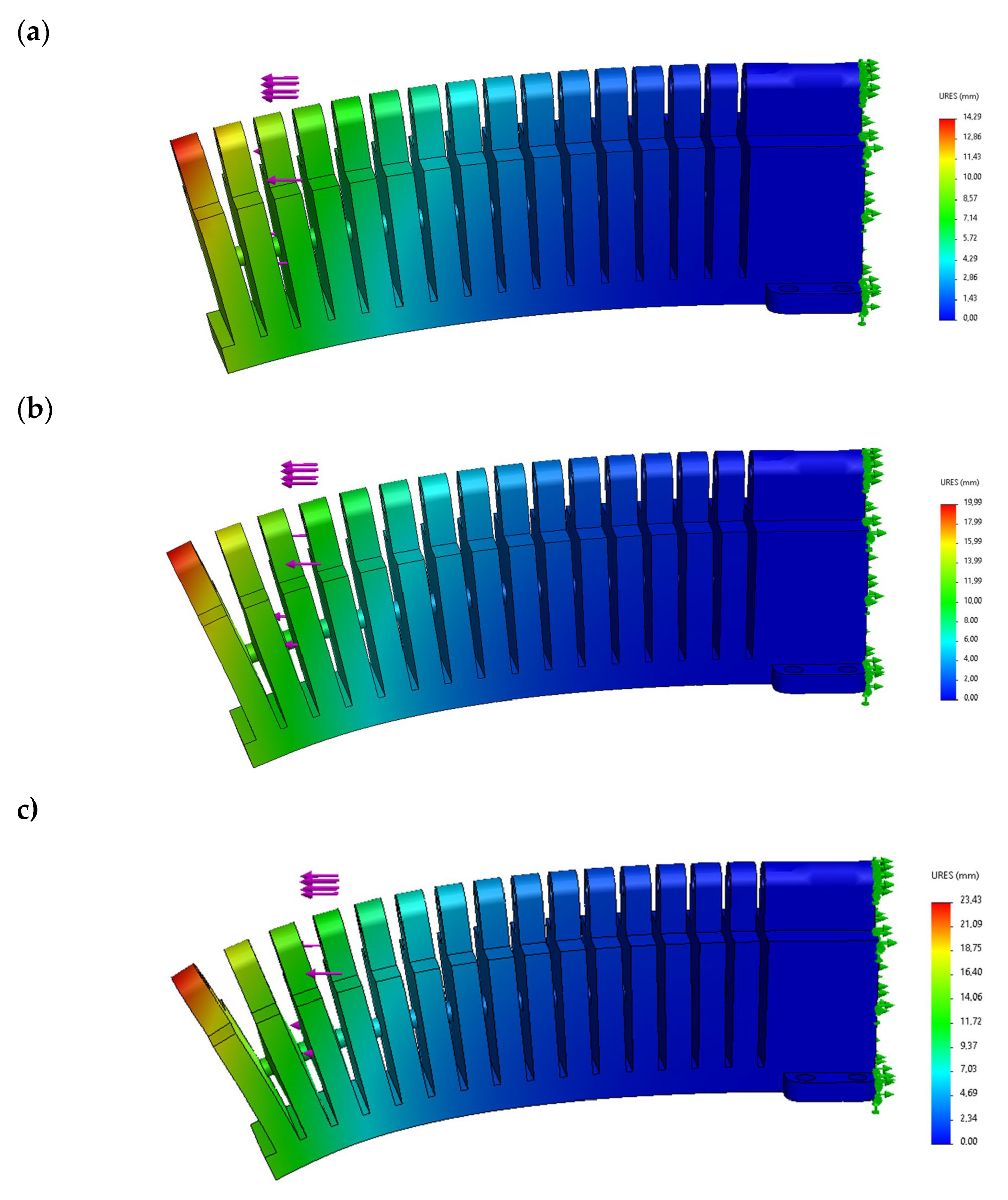
3.3. Testing
4. Discussion
4.1. Limitations to the Development of Hand Exoskeletons
4.2. Development Directions for Hand Exoskeletons
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nizamis, K.; Athanasiou, A.; Almpani, S.; Dimitrousis, C.; Astaras, A. Converging Robotic Technologies in Targeted Neural Rehabilitation: A Review of Emerging Solutions and Challenges. Sensors 2021, 21, 2084. [Google Scholar] [CrossRef] [PubMed]
- McConnell, A.C.; Moioli, R.C.; Brasil, F.L.; Vallejo, M.; Corne, D.W.; Vargas, P.A.; Stokes, A.A. Robotic devices and brain-machine interfaces for hand rehabilitation post-stroke. J. Rehabil. Med. 2017, 49, 449–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenfeld, J.V.; Wong, Y.T. Neurobionics and the brain-computer interface: Current applications and future horizons. Med. J. Aust. 2017, 206, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.; Valè, N.; Posteraro, F.; Morone, G.; Dell’orco, A.; Botticelli, A.; Dimitrova, E.; Gervasoni, E.; Goffredo, M.; Zenzeri, J.; et al. Italian Consensus Conference on Robotics in Neurorehabilitation (CICERONE). State of the art and challenges for the classification of studies on electromechanical and robotic devices in neurorehabilitation: A scoping review. Eur. J. Phys. Rehabil. Med. 2021, 57, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Macko, M.; Szczepański, Z.; Mikołajewski, D.; Mikołajewska, E.; Listopadzki, S. The method of artificial organs fabrication based on reverse engineering in medicine. In Lecture Notes in Mechanical Engineering; Rusiński, E., Pietrusiak, D., Eds.; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Mikołajewska, E.; Mikołajewski, D. Ethical considerations in the use of brain-computer interfaces. Cent. Eur. J. Med. 2013, 8, 720–724. [Google Scholar] [CrossRef]
- Rojek, I.; Mikołajewski, D.; Dostatni, E. Digital twins in product lifecycle for sustainability in manufacturing and maintenance. Appl. Sci. 2021, 11, 31. [Google Scholar] [CrossRef]
- Luneski, A.; Konstantinidis, E.; Bamidis, P.D. Affective medicine. A review of affective computing efforts in medical informatics. Methods Inf. Med. 2010, 49, 207–218. [Google Scholar] [CrossRef] [Green Version]
- Gojanovic, B.; Fourchet, F.; Gremeaux, V. Cognitive biases cloud our clinical decisions and patient expectations: A narrative review to help bridge the gap between evidence-based and personalized medicine. Ann. Phys. Rehabil. Med. 2021, 65, 101551. [Google Scholar] [CrossRef]
- Pastorino, R.; Loreti, C.; Giovannini, S.; Ricciardi, W.; Padua, L.; Boccia, S. Challenges of Prevention for a Sustainable Personalized Medicine. J. Pers. Med. 2021, 11, 311. [Google Scholar] [CrossRef]
- Wang, W.; Yan, Y.; Guo, Z.; Hou, H.; Garcia, M.; Tan, X.; Anto, E.O.; Mahara, G.; Zheng, Y.; Li, B.; et al. Suboptimal Health Study Consortium and European Association for Predictive, Preventive and Personalised Medicine. All around suboptimal health—A joint position paper of the Suboptimal Health Study Consortium and European Association for Predictive, Preventive and Personalised Medicine. EPMA J. 2021, 12, 403–433. [Google Scholar]
- Xiloyannis, M.; Chiaradia, D.; Frisoli, A.; Masia, L. Physiological and kinematic effects of a soft exosuit on arm movements. J. Neuroeng. Rehabil. 2019, 16, 29. [Google Scholar] [CrossRef] [Green Version]
- Rojek, I.; Jagodziński, M. Hybrid artificial intelligence system in constraint based scheduling of integrated manufacturing ERP. In Proceedings of the 7th International Conference on Hybrid Artificial Intelligent Systems (HAIS), Hybrid Artificial Intelligent Systems, Salamanca, Spain, 28–30 March 2012; Pt. II 7209; pp. 229–240. [Google Scholar]
- Chandra, M.; Kumar, K.; Thakur, P.; Chattopadhyaya, S.; Alam, F.; Kumar, S. Digital technologies, healthcare and Covid-19: Insights from developing and emerging nations. Health Technol. 2022, 12, 547–568. [Google Scholar] [CrossRef]
- Görtz, M.; Byczkowski, M.; Rath, M.; Schütz, V.; Reimold, P.; Gasch, C.; Simpfendörfer, T.; März, K.; Seitel, A.; Nolden, M.; et al. A Platform and Multisided Market for Translational, Software-Defined Medical Procedures in the Operating Room (OP 4.1): Proof-of-Concept Study. JMIR Med. Inform. 2022, 10, e27743. [Google Scholar] [CrossRef]
- Nassour, J.; Zhao, G.; Grimmer, M. Soft pneumatic elbow exoskeleton reduces the muscle activity, metabolic cost and fatigue during holding and carrying of loads. Sci. Rep. 2021, 11, 12556. [Google Scholar] [CrossRef]
- Cui, L.; Phan, A.; Allison, G. Design and fabrication of a three dimensional printable non-assembly articulated hand exoskeleton for rehabilitation. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2015, 2015, 4627–4630. [Google Scholar]
- Kaczmarek, M.; Nowak, J.; Olszewski, W.L.; Zaleska, M. Estimation of hydromechanical parameters of limb lymphedematous tissue with the use of chamber tests. Acta Bioeng. Biomech. 2021, 23, 149–161. [Google Scholar] [CrossRef]
- Kaczmarek, M.; Nowak, J.; Olszewski, W.L.; Zaleska, M. Simulation-based reasoning of residual tissue deformations in a two-chamber test of a lymphedematous leg. Int. J. Numer. Methods Biomed. Eng. 2022, 38, e3537. [Google Scholar] [CrossRef]
- Burns, M.K.; van Orden, K.; Patel, V.; Vinjamuri, R. Towards a wearable hand exoskeleton with embedded synergies. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2017, 2017, 213–216. [Google Scholar]
- Dudley, D.R.; Knarr, B.A.; Siu, K.C.; Peck, J.; Ricks, B.; Zuniga, J.M. Testing of a 3D printed hand exoskeleton for an individual with stroke: A case study. Disabil. Rehabil. Assist. Technol. 2021, 16, 209–213. [Google Scholar] [CrossRef]
- Yoo, H.J.; Lee, S.; Kim, J.; Park, C.; Lee, B. Development of 3D-printed myoelectric hand orthosis for patients with spinal cord injury. J. Neuroeng. Rehabil. 2019, 16, 162. [Google Scholar] [CrossRef] [Green Version]
- Rojek, I.; Mikołajewski, D.; Dostatni, E.; Macko, M. AI-Optimized Technological Aspects of the Material Used in 3D Printing Processes for Selected Medical Applications. Materials 2020, 13, 5437. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Chen, J.; He, G.; Cui, L.; Chen, C.; Secco, E.L.; Yao, W.; Xie, J.; Xu, G.; Wurdemann, H. Attention Enhancement for Exoskeleton-Assisted Hand Rehabilitation Using Fingertip Haptic Stimulation. Front. Robot. AI 2021, 8, 602091. [Google Scholar] [CrossRef]
- Araujo, R.S.; Silva, C.R.; Netto, S.P.N.; Morya, E.; Brasil, F.L. Development of a Low-Cost EEG-Controlled Hand Exoskeleton 3D Printed on Textiles. Front. Neurosci. 2021, 15, 661569. [Google Scholar] [CrossRef] [PubMed]
- Noronha, B.; Ng, C.Y.; Little, K.; Xiloyannis, M.; Kuah, C.W.K.; Wee, S.K.; Kulkarni, S.R.; Masia, L.; Chua, K.S.G.; Accoto, D. Soft, Lightweight Wearable Robots to Support the Upper Limb in Activities of Daily Living: A Feasibility Study on Chronic Stroke Patients. IEEE Trans. Neural. Syst. Rehabil. Eng. 2022, 30, 1401–1411. [Google Scholar] [CrossRef] [PubMed]
- Geethanjali, P. Myoelectric control of prosthetic hands: State-of-the-art review. Med. Devices 2016, 9, 247–255. [Google Scholar] [CrossRef] [Green Version]
- Kladovasilakis, N.; Kostavelis, I.; Sideridis, P.; Koltzi, E.; Piliounis, K.; Tzetzis, D.; Tzovaras, D. A Novel Soft Robotic Exoskeleton System for Hand Rehabilitation and Assistance Purposes. Appl. Sci. 2023, 13, 553. [Google Scholar] [CrossRef]
- Guo, K.; Lu, J.; Liu, C.; Yang, H. Development, Research, Optimization and Experiment of Exoskeleton Robot for Hand Rehabilitation Training. Appl. Sci. 2022, 12, 10580. [Google Scholar] [CrossRef]
- Hayat, A.; Dias, M.; Bhuyan, B.P.; Tomar, R. Human Activity Recognition for Elderly People Using Machine and Deep Learning Approaches. Information 2022, 13, 275. [Google Scholar] [CrossRef]
- Monoscalco, L.; Simeoni, R.; Maccioni, G.; Giansanti, D. Information Security in Medical Robotics: A Survey on the Level of Training, Awareness and Use of the Physiotherapist. Healthcare 2022, 10, 159. [Google Scholar] [CrossRef]
- Singh, N.; Saini, M.; Kumar, N.; Srivastava, M.V.P.; Mehndiratta, A. Evidence of neuroplasticity with robotic hand exoskeleton for post-stroke rehabilitation: A randomized controlled trial. J. Neuroeng. Rehabil. 2021, 18, 76. [Google Scholar] [CrossRef]
- Saini, M.; Singh, N.; Kumar, N.; Srivastava, M.V.P.; Mehndiratta, A. A novel perspective of associativity of upper limb motor impairment and cortical excitability in sub-acute and chronic stroke. Front. Neurosci. 2022, 16, 832121. [Google Scholar] [CrossRef]
- Scotto di Luzio, F.; Cordella, F.; Bravi, M.; Santacaterina, F.; Bressi, F.; Sterzi, S.; Zollo, L. Modification of Hand Muscular Synergies in Stroke Patients after Robot-Aided Rehabilitation. Appl. Sci. 2022, 12, 3146. [Google Scholar] [CrossRef]
- Goffredo, M.; Pournajaf, S.; Proietti, S.; Gison, A.; Posteraro, F.; Franceschini, M. Retrospective Robot-Measured Upper Limb Kinematic Data from Stroke Patients Are Novel Biomarkers. Front. Neurol. 2021, 12, 803901. [Google Scholar] [CrossRef]
- Giang, C.; Pirondini, E.; Kinany, N.; Pierella, C.; Panarese, A.; Coscia, M.; Miehlbradt, J.; Magnin, C.; Nicolo, P.; Guggisberg, A.; et al. Motor improvement estimation and task adaptation for personalized robot-aided therapy: A feasibility study. Biomed. Eng. Online 2020, 19, 33. [Google Scholar] [CrossRef]
- Vélez-Guerrero, M.A.; Callejas-Cuervo, M.; Mazzoleni, S. Design, Development, and Testing of an Intelligent Wearable Robotic Exoskeleton Prototype for Upper Limb Rehabilitation. Sensors 2021, 21, 5411. [Google Scholar] [CrossRef]
- Kopke, J.V.; Ellis, M.D.; Hargrove, L.J. Determining User Intent of Partly Dynamic Shoulder Tasks in Individuals With Chronic Stroke Using Pattern Recognition. IEEE Trans. Neural. Syst. Rehabil. Eng. 2020, 28, 350–358. [Google Scholar] [CrossRef]
- Zhang, F.; Fu, Y.; Zhang, Q.; Wang, S. Experiments and kinematics analysis of a hand rehabilitation exoskeleton with circuitous joints. Biomed. Mater. Eng. 2015, 26 (Suppl. 1), S665–S672. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.H.; Koh, C.L.; Hsu, C.H.; Chen, P.C.; Chen, J.W.; Lan, Y.H.; Yang, Y.; Lin, Y.D.; Wu, C.H.; Liu, H.K.; et al. An Instrumented Glove-Controlled Portable Hand-Exoskeleton for Bilateral Hand Rehabilitation. Biosensors 2021, 11, 495. [Google Scholar] [CrossRef]
- Rojek, I. Neural networks as prediction models for water intake in water supply system. In Proceedings of the Artificial Intelligence and Soft Computing—ICAISC 2008, Proceedings of the 9th International Conference, Zakopane, Poland, 22–26 June 2008; Rutkowski, L., Tadeusiewicz, R., Zadeh, L.A., Zurada, J.M., Eds.; Lecture Notes in Computer Science. Springer: Berlin/Heidelberg, Germany, 2008; Volume 5097, pp. 1109–1119. [Google Scholar]
- Rojek, I.; Dostatni, E.; Hamrol, A. Ecodesign of technological processes with the use of decision trees method. In Proceedings of the International Joint Conference SOCO’17-CISIS’17-ICEUTE’17, León, Spain, 6–8 September 2017; Pérez García, H., Alfonso-Cendón, J., Sánchez González, L., Quintián, H., Corchado, E., Eds.; Advances in Intelligent Systems and Computing. Springer: Cham, Switzerland, 2018; Volume 649, pp. 318–327. [Google Scholar]
- Pahlevanzadeh, F.; Mokhtari, H.; Bakhsheshi-Rad, H.R.; Emadi, R.; Kharaziha, M.; Valiani, A.; Poursamar, S.A.; Ismail, A.F.; RamaKrishna, S.; Berto, F. Recent Trends in Three-Dimensional Bioinks Based on Alginate for Biomedical Applications. Materials 2020, 13, 3980. [Google Scholar] [CrossRef]
- Rudd, G.; Daly, L.; Jovanovic, V.; Cuckov, F. A Low-Cost Soft Robotic Hand Exoskeleton for Use in Therapy of Limited Hand–Motor Function. Appl. Sci. 2019, 9, 3751. [Google Scholar] [CrossRef] [Green Version]
- Sänger, J.; Yao, Z.; Schubert, T.; Wolf, A.; Molz, C.; Miehling, J.; Wartzack, S.; Gwosch, T.; Matthiesen, S.; Weidner, R. Evaluation of Active Shoulder Exoskeleton Support to Deduce Application-Oriented Optimization Potentials for Overhead Work. Appl. Sci. 2022, 12, 10805. [Google Scholar] [CrossRef]
- Nava-Téllez, I.A.; Elias-Espinosa, M.C.; Cervantes-Culebro, H.; Flores-González, A.E. Parametric Design of a Finger Rehabilitation Mechanism with Double Action and Two Degrees of Freedom. Appl. Sci. 2022, 12, 10701. [Google Scholar] [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojek, I.; Kaczmarek, M.; Kotlarz, P.; Kempiński, M.; Mikołajewski, D.; Szczepański, Z.; Kopowski, J.; Nowak, J.; Macko, M.; Szczepańczyk, A.; et al. Hand Exoskeleton—Development of Own Concept. Appl. Sci. 2023, 13, 3238. https://doi.org/10.3390/app13053238
Rojek I, Kaczmarek M, Kotlarz P, Kempiński M, Mikołajewski D, Szczepański Z, Kopowski J, Nowak J, Macko M, Szczepańczyk A, et al. Hand Exoskeleton—Development of Own Concept. Applied Sciences. 2023; 13(5):3238. https://doi.org/10.3390/app13053238
Chicago/Turabian StyleRojek, Izabela, Mariusz Kaczmarek, Piotr Kotlarz, Marcin Kempiński, Dariusz Mikołajewski, Zbigniew Szczepański, Jakub Kopowski, Joanna Nowak, Marek Macko, Andrzej Szczepańczyk, and et al. 2023. "Hand Exoskeleton—Development of Own Concept" Applied Sciences 13, no. 5: 3238. https://doi.org/10.3390/app13053238