
Personalization of the 3D-Printed Upper Limb Exoskeleton Design—Mechanical and IT Aspects

Faculty of Computer Science, Kazimierz Wielki University, Chodkiewicza 30, 85-064 Bydgoszcz, Poland
*
Author to whom correspondence should be addressed.
Appl. Sci. 2023, 13(12), 7236; https://doi.org/10.3390/app13127236
Submission received: 20 May 2023
/
Revised: 14 June 2023
/
Accepted: 14 June 2023
/
Published: 17 June 2023
(This article belongs to the Special Issue 3D Printing and Biomaterials for Biomedical Application)
Abstract
:Featured Application
The application of this work relates to the use of 3D printing and artificial intelligence as systems to support the personalisation of medical devices, in particular powered upper limb exoskeletons and passive orthoses.
Abstract
The human hand is the most precise and versatile tool that nature has given man, and any deficits in this area affect the functional capabilities and quality of human life. Scientists, engineers and clinicians are constantly looking for solutions in the field of diagnosis, treatment, rehabilitation and care of patients with hand function deficits. One such solution is a hand exoskeleton. In the process of designing and testing the hand exoskeleton, emphasis should be placed on the full usability and comfort of the system; hence, the issues of personalization, matching and testing are crucial for the development of the discussed group of solutions. The aim of this paper is to present the possibilities of personalizing 3D-printed medical devicesbased on our own experience in functional user assessment andthe material selection, design, optimization using artificial intelligence and production and testing of several generations of different upper limb exoskeletons, incorporatingthe considerations of the Medical Device Regulation (MDR), ISO 13485 and ISO 10993 standards.The novelty and possible contribution of the proposed approach consist of the possibilities and limitations of the personalization of the upper limb exoskeleton discussed in the article as well as the directions of further development of significant scientific, technical and clinical importance.
1. Introduction
The 3D-printed medical devices, including exoskeletons, are a distinct and an easily personalised group of medical devices [1,2,3,4,5]. 3D printing technology forms the basis of mass customisation in the manufacturing industry, especially in the area of healthcare, but also in agriculture, automotive or aerospace [1]. Furthermore, 4D printing is an extension of 3D printing technology to include the aspect of pre-programmable changes to the shape or properties of a 3D-printed product over time. This brings with it not only improved capabilities for the creation of personalised products (including complex geometries and components impossible to manufacture using traditional manufacturing techniques) but also improved supply chain efficiency and reduced costs and lead times (from measurement through design to finished product). It also provides the possibility for the structure of the device to respond to temperature (body or environment), humidity (body, dressing or environment), light or other physical quantities [2,3,5]. Added value also comes from the combined use of 3D scanning, 3D printing, reverse engineering and artificial intelligence (AI) (not only for design but also, for example, to optimise material selection and minimise waste) in the workflow for the development of a personalised (customised) product [4]. A gap was observed in the area of research and between research and engineering practice and clinical practice, which needs to be filled as quickly and thoroughly as possible. It is necessary to simultaneously maintain the rigid methodological requirements and flexible therapeutic efficacy inherent in medical devices and to develop new business models dedicated to achieving and maintaining the viability of industrial mass production of personalised exoskeletons. In an era dominated by Industry 4.0 and Industry 5.0 paradigms, there should no longer be regulations holding back the development of 3D scanning, 3D printing and reverse engineering within the healthcare system as this would inhibit the transfer of proven solutions into clinical practice. The widespread use of pro-environmental 3D printing in everyday clinical practice already requires the preparation of interdisciplinary teams, including medical specialists, as well as systemic organisational changes to ensure that the needs of patients and clinicians are met as efficiently as possible [6].
1.1. Possibilities
Personalization improves usability and comfort of medical devices, including exoskeletons, and allows to solve a number of practical problems, e.g., observed differences in interaction between users and the system, user preferences, expected level and method of support. This applies to various activities (activities of daily living), from simple, related to self-service, to complex, e.g., climbing stairs while holding onto the handrail [7]. For the purposes of upper limb exoskeletons, it is already possible to automate or semi-automatically (based on AI) design 3D-printed chainmail with individually programmable properties—especially with variable stiffness/flexibility depending on the direction, with an adjustable one- or two-way bending module [8]. The model of human–machine cooperation is also subject to personalization. It is usually created using large datasets derived from kinematic analyzes of the users’ elbow, wrist and finger movements. This is the basis for the development of a personalized exoskeleton prototype for the purpose of evaluating a specific modeling method and testing the prototype [9]. Innovative methods of design, adjustment and personalization are in great demand in this area, and not all of them are developed and widely available today. The inclusion of motor imaging (MI) signals from electroencephalography (EEG) in the exoskeleton control also requires an individual approach to design. This allows to better read the intention of the exoskeleton user’s movement [10]. This is a great step towards bionic neuroprostheses, which are the future of the development of this group of solutions (including the feeling of thermal sensations and the sense of shape or surface even from amputated organs). This would allow people with dentures to function better. The development of personalized exoskeletons will be necessary due to the constant pursuit of physical improvement and overcoming physical limitations, including in people with congenital or acquired deficits [11]. The Assist as Needed (AAN) algorithm is already used to control the elbow exoskeleton. Force Sensing Sensor (FSR) and electromyography sensors on the biceps provide data for machine learning algorithms personalized for each patient and havereached an accuracy of up to 91.22%. The challenge is to provide patients with real-time visual feedback on their movement and for learning how to control the exoskeleton using VR [12]. From gait studies, kinematic data is known to provide general characteristics of movement efficiency, but limited conclusions can be drawn about neural control strategies, and some kinematic/kinetic parameters are a consequence of exoskeleton control. Aforementioned data should be supplemented with an assessment of muscular coordination and control strategies [13]. Surface electromyography (sEMG) and machine learning-based adaptive controllers of upper limb exoskeletons require personalization. They have achieved an average accuracy of over 93% for users with muscular dystrophy and neurodegenerative diseases without previous exposure to these types of controllers [14]. Upper limb exoskeletons support individually selected neuromotor rehabilitation including restoring the function of the upper limb and improving the quality of life of patients. The effectiveness of rehabilitation depends on the possibility of introducing personalized training plans and the availability of objective assessment of the patient’s progress (monitoring the effects of the above-mentioned rehabilitation plans) [15]. As part of the personalization, a device was also developed to dynamically adjust the load on the exoskeleton (torque adjustment) taking into account its posture [16]. Another element of personalization is patient-oriented biofeedback based on human–exoskeleton interaction. This improves the compliance of the patient with the exoskeleton in terms of joint movement strategies and user participation strategies by means of audio and vibration cues [17]. However, the use of personalized human–exoskeleton cooperation systems translates into an increase in the number of motor tasks that are not subject to assessment. This causes the need to amend the standards for human ergonomics and biomechanical risk assessment in the human–exoskeleton relationship [18]. Platforms have even been developed that include an exoskeleton and a simulator for estimating the user’s kinetic parameters (i.e., for analyzing individual variables that need to be taken into account for personalization) [19]. A multimodal upper limb exoskeleton control strategy was also developed to support patient training [20].
1.2. Challenges
The group of users of hand exoskeletons includes many people with congenital defects, after hand injuries or after a stroke, who, even after completing a rehabilitation program, continue to experience functional problems with their hand in activities of daily living, such as maintaining hygiene, dressing or preparing meals, and also in daily life in the community, studying and working [21]. Globally, it is estimated that more than 50 million people suffer from a hand function deficit or hand impairment after a stroke or spinal cord injury (SCI). The main challenges in designing and testing hand exoskeletons for patients with hand function deficits stem from the fact that human hand is the most precise and versatile tool that nature has given man, and any deficit in this area affects the functional capabilities and quality of life of the human being. Scientists, engineers and clinicians are constantly seeking solutions for the diagnosis, treatment, rehabilitation and care of patients with deficits in hand function. One such solution is the hand exoskeleton.
1.3. Novelty and Contribution
The novelty and possible contribution of the proposed approach consist of the possibilities and limitations of the personalization of the upper limb exoskeleton discussed in the article as well as the guidelines and directions of further development of significant scientific, technical and clinical importance.The scientific significance lies in the better use of existing and development of new research methodologies better suited to design, production plan, and produce personalized medical devices and services based on them. The technical significance has an impact on the combination of existing technologies and production models with the paradigms of Industry 4.0, Industry 5.0 and the Green Deal. In the case of medical devices, this also involves ensuring compliance with clinical indications and contraindications as well as standards for clinical devices. The clinical significance lies in the mechanical, material and control possibilities personalized to a particular patient, and thus faster and easier achievement of clinical goals and the possibility of implementing more complex therapeutic methods, including those in which the exoskeleton is used as a carrier of diagnostic or therapeutic devices in the future. In the article, we present the possibility of personalizing the exoskeleton of the hand, including the movements of the exoskeleton of the hand and the patient using such an exoskeleton. In the process of designing and testing the hand exoskeleton, emphasis should be placed on the full usability and comfort of the system; hence, the issues of fitting and testing are crucial for the development of the discussed group of solutions.
1.4. Aim of the Study
The aim of this paper is to present the possibilities of personalizing 3D-printed medical devicesbased on our own experience in functional user assessment and the material selection, design, optimization using artificial intelligence and production and testing of several generations of different upper limb exoskeletons, incorporating the considerations of the Medical Device Regulation (MDR), ISO 13485 (Quality management systems) and ISO 10993 (Biocompatibility) standards. With the Industry 4.0 and Industry 5.0 paradigms in mind, it is also worth considering ISO 27001 (Information security management systems).
2. Materials and Methods
Two independent experts used the Appraisal of Guidelines for Research and Evaluation (AGREE) II [22,23]. This solution is well-known, proven and has been frequently used to date to evaluate medical devices and procedures [24,25,26,27,28], including exoskeletons [29]. The PubMed database shows 1231 publications with the keyword “AGREE II”. AGREE II was developed to address the variability in guideline quality and to ensure the best possible quality of guidelines. It assesses the methodological rigor and transparency with which guidelines are produced. AGREE II can be used by healthcare providers, guideline developers, policy makers or educators, among others, to conduct their own evaluation of guidelines before adopting their recommendations into their practice, to create and adhere to a structured and rigorous development methodology, to help decide which guidelines can be recommended for use in practice or to inform decisions and to help improve critical appraisal skills.
AGREE II consists of 23 items numbered 1–23 and divided into 6 domains with each covering a specific dimension of guideline quality:
- Domain 1: scope and purpose of the guideline, specific health issues and target population (1–3);
- Domain 2: degree of guideline development by relevant stakeholders (4–6);
- Domain 3: process of evidence collection and synthesis, methods of evidence formulation, methods of recommendation formulation and updating (7–14);
- Domain 4: the language, structure and format of the guidelines (15–17).
- Domain 5: applicability in light of barriers and facilitators to implementation and the impact of guideline use (18–21);
- Domain 6: independence of the formulation from recommendations and absence of conflicting interests (22–23).
Finally, these are followed by two global assessment items: overall assessment—an assessment of the overall quality of the guideline and an assessment of whether the guideline would be recommended for use in practice.
Each of the 23 AGREE II items and the final two global assessment items are rated the same: on a 7-point scale from 1 (strongly disagree) to 7 (strongly agree).
In case of doubt, the provisions of the original user’s manual were conclusive in the study.
Short syntheses were used to evaluate and compare different approaches and recommendations, considering only the most recent version.
3. Results
The tool used in the study (AGREE II) provides a framework for assessing guideline quality, provides a methodological strategy for guideline development and determines what information should be provided in the guidelines and how.
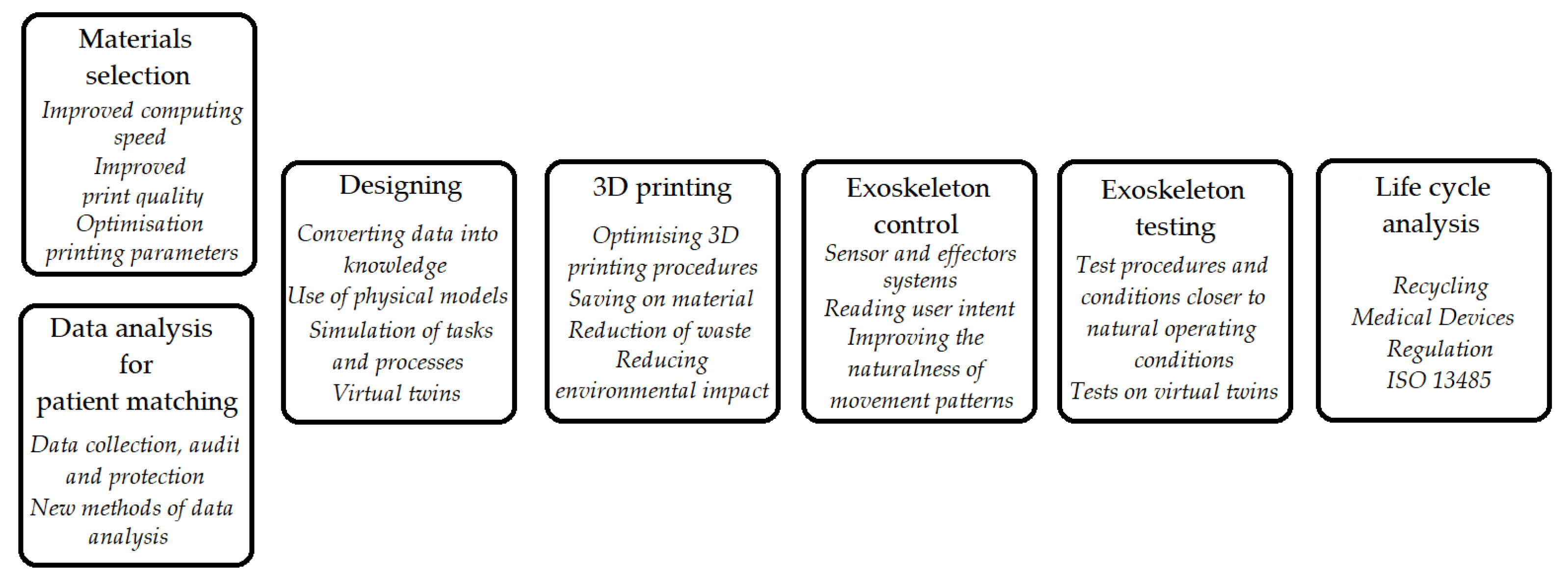
According to expert consensus, the main areas of personalization of the upper limb exoskeleton especially due to AIuse can include (Figure 1):
- Personalized selection and optimalization of materials for the exoskeleton, including in terms of weight, mechanical properties (flexibility, including preprogrammed in different directions) and chemical properties (contact with tissue and body fluids);
- Individual functional assessment and AI-based selection of exoskeleton model/settings to the type and level of deficit/deficits in a particular patient;
- Patient-tailored template-based exoskeleton design;
- 3D printing optimized due to AI use for material consumption and waste (preferring green technologies);
- Individual settings of the exoskeleton control system, AI mediated;
- Exoskeleton testing and adjustment (Table 1).
All domains scored above 70%, indicating a lack of prioritization of a single domain.
Most of the above-mentioned solutions can be effectively supported by artificial intelligent solutions, primarily data-driven approaches, i.e., machine learning (ML)—both traditional artificial neural networks and deep learning, and also fuzzy logic, multifractal analysis or random forests. Wisely and planned AI-based solutions will allow for almost leapfrogging improvements in efficiency while keeping data and processes safe (so-called ethical AI) and avoiding a significant proportion of risks (including the so-called black box).
Unfortunately, there is still no consensus on the timing, frequency and duration of training sessions and the exact characteristics of subjects that could benefit from the implementation of upper limbs exoskeletons.
4. Case Studies and Applications
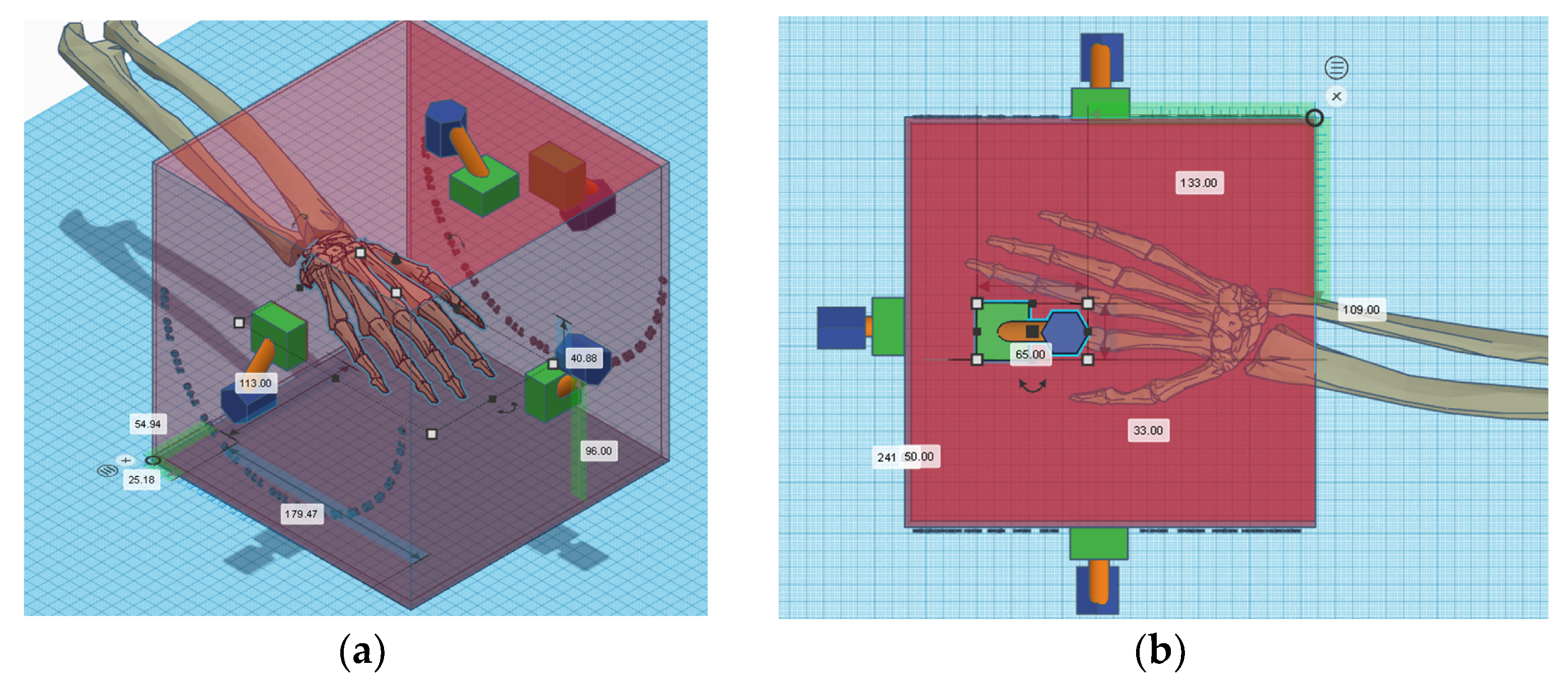
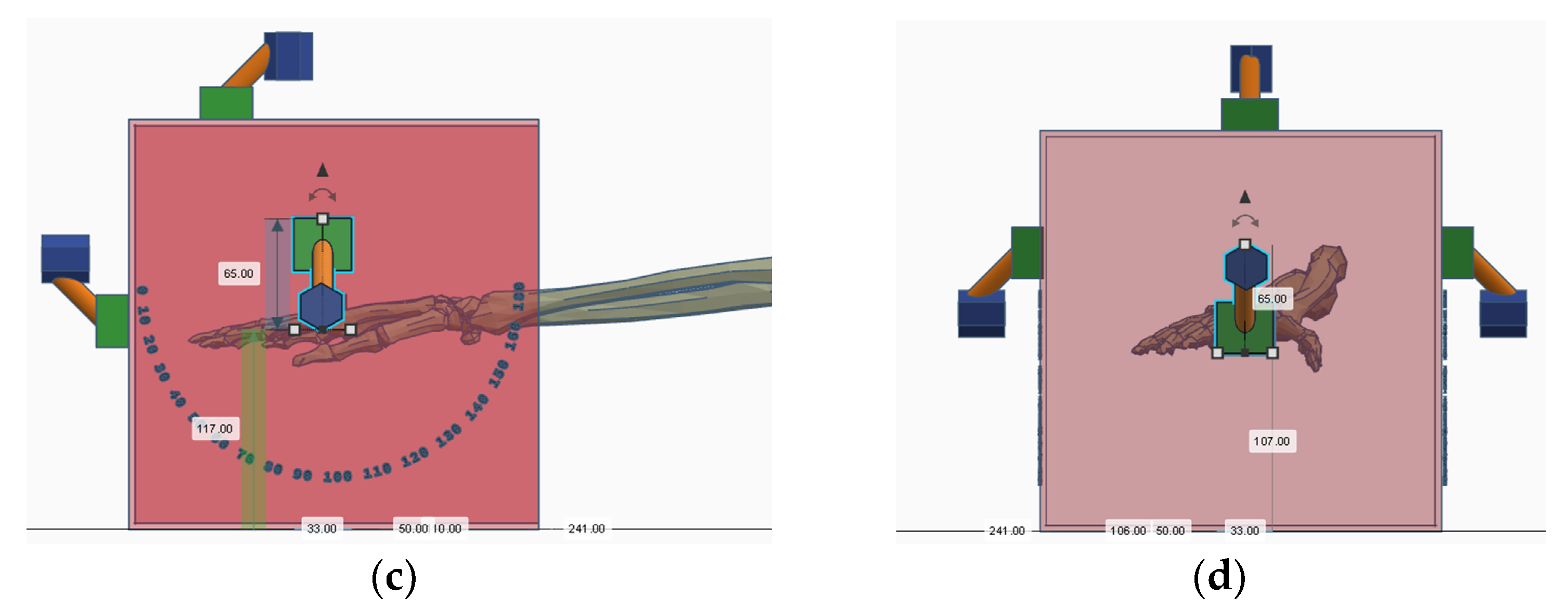
As an example shown in Figure 2, the motion analysis station is based on motion capture from high-speed cameras in 3D and post hoc analysis using proprietary software, including those based on artificial intelligence. The software allows the extraction of new, more useful hand and arm movement markers in the exoskeleton, including for early diagnosis and rehabilitation. The novelty and possible contribution of the proposed approach consist of the possibilities and limitations of our research discussed in the article as well as directions for further development of significant scientific, technical and clinical importance.
In Table 2, we have presented case studies or examples where personalized 3D-printed upper limb exoskeletons have been successfully applied in real-life scenarios along with a brief discussion of the results, limitations and potential benefits of these applications. These cases can serve as an inspiration for further research work developing exoskeletons as well as ready-made proposals for deployment in various areas of Industry 4.0 and Industry 5.0 due to the environmentally friendly aspect of our solutions.
Integrated and systematic/continuous use of the above or similar solutions seems to be the best approach. Time and money spent on just one solution can pay off much more slowly than the same infrastructure (sensors, databases, servers, cloud technology subscriptions and AI/ML environments) used in many different ways.
5. Discussion
In the case of exoskeletons, there is a lack of research on side effects and adverse events. Meanwhile, the most commonly reported effects include discomfort and limited usability of the exoskeleton, followed by changes in muscle activity, mobility, task performance, balance and posture [30]. Studies of exoskeletons in the population of patients with a neurological deficit have shown that the satisfaction felt by users relates to the safety, effectiveness and comfort of using the devices, and the problems requiring improvement or optimization relate to the ease of adjustment, size and weight of the exoskeleton and ease of use [31]. The implementation of a rehabilitation program using an exoskeleton in clinical practice required taking into account the specificity of the intervention, patients and the environment, and the barriers were skin problems, falls and equipment failures [32]. The variety of available exoskeletons for rehabilitation is important, and their selection should be based on the severity of the deficit and changes/comorbidities [33]. For passive shoulder or back exoskeletons, the main features considered are acceptability and usability, comfort, effort/fatigue, occupational health and safety, especially in static tasks [34]. In children, the selection takes into account spatio-temporal, kinematic/kinetic parameters, muscular activity and physiological parameters. Therefore, here the scope of adaptation may be the largest and also the number of solutions the largest [35]. Interestingly, even in children with cerebral palsy, improvement due to the use of exoskeletons is expected in all areas: walking, graphomotor, play and social interaction [36]. Interestingly, there is no evidence that the use of exoskeletons is superior to other interventions, except for patients with advanced Parkinson’s disease and more severe symptoms [37]. Therefore, so far it has been difficult to rely on medical evidence when optimizing the parameters of the exoskeleton [38]. Observed gaps in the capabilities of exoskeletons include their effectiveness at different levels of performance required for each use, including in healthy individuals (e.g., in the military) [39]. There are still no clear indications regarding the clinical use of exoskeletons (although there are contraindications developed by the manufacturers) [40]. There are still no clear indications regarding the clinical use of exoskeletons (although there are contraindications developed by the manufacturers) [41,42,43]. The gap between the results of research on therapy using exoskeletons and its application in clinical practice is still significant [44]. It is crucial to study the impact of exoskeletons on spatio-temporal and kinematic/kinetic parameters depending on age and advancement of the disease [45]. Postural instability, resting tremor, stiffness and bradykinesia in Parkinson’s disease are highly disabling as the disease progresses and reduce the quality of life even with the use of an exoskeleton, except for balance [46]. Similar limitations can be observed in many diseases [47,48,49]. The reason for the difficulties in the assessment is the methodological variability of the research [49,50,51]. Research on the use of exoskeletons has a number of limitations in design and implementation; therefore, scientists and clinicians should not fully rely on them when making decisions. Further basic and applied research and clinical indications are needed [52]. Analyzes of the required support in people with different types and degrees of deficits will help advance the design of exoskeletons based on user needs [53]. The physiological mechanisms associated with pain in candidates for wearing soft exoskeletons differ between healthy individuals and patients with chronic pain. Higher speeds of movement and amount of tissue compression may be unacceptable to some users [54], particularly in multi-modality rehabilitation approach [55,56,57]. In weakened people, the use of exoskeletons is less energy-intensive and burdening to the cardiovascular systemthan traditional therapy, but the effectiveness depends on the type of exoskeleton, the type of activity and the effort involved [58]. Studies of exoskeleton-assisted movement are increasingly analyzed using fixed and random effects meta-analysis models. As a result, risks are reduced due to newer generations of exoskeletons and improved patient eligibility criteria [59]. Exoskeletons are a safe, practical, easy-to-learn, non-burdening to working memory and low-intensive method of rehabilitation [60].
Impaired function of the upper extremities results in patients experiencing limited dexterity, both in activities requiring one hand, especially with deficits in the dominant hand, and requiring the use of both hands, which reduces independence in daily life [21].
The proposed solution allows to objectively evaluate both the movement of the hand (healthy and with deficits of different types and levels), the exoskeleton itself and the hand (healthy, with deficits) in the exoskeleton. This makes it possible to compare the results of movement assessment so far carried out by specialists on the basis of their knowledge and experience, and sometimes differing in assessment, among other things, under the influence of different assessment conditions (e.g., in different lighting). The accuracy of assessments also increases, and it is achievable without the support of a specialized hand movement laboratory, even at the level of an ordinary clinic. Thus, a new automated model for assessing hand movements is being created, improving the efficiency of diagnosis, therapy and care (including, detection of swelling or its changes). Multiple testing of solutions is supported by the possibility of using new antibacterial polymers for 3D printing to prevent skin infections during rehabilitation but also exoskeleton testing [21]. To date, the purpose of such studies has mainly been to determine the functional and neuromuscular changes in the participant induced by the 3D-printed exoskeleton, and evaluation has primarily used clinimetric scores and scales (Fugl–Meyer Assessment and Box and Block Test) and tests the participant’s forearm muscle strength and activation (EMG), possibly through patient satisfaction questionnaires [21]. In a study by Mayer et al. [61], 22 people were tested in three different exoskeleton conditions for each grip task, i.e., 90 repetitions in random order. The study shows that the effect of the exoskeleton varies depending on the gripping task and the gender of the participant, and significant individual differences were also observed [2]. An area of particular risk is children and those with sensory deficits. In a study by Lieber et al. [62], it was shown that in a group of children and adolescents, the Box and Block test, the Selective Upper Limb Control Scale and finger extensor muscle strength differentiated well participants who improved their scores after using the exoskeleton and those who did not [62]. All participants needed help wearing the exoskeleton module, andthe median donning times were 62–160 s (i.e., less than 3 min) with high user acceptance of the exoskeleton [62]. Problems were observed with the durability of the transmission system, electronics and exoskeleton attachment system [62].
In addition to testing, it is worth conducting an exploratory analysis of the effects of using the exoskeleton in order to monitor it from the point of view of safety and applicable regulations (e.g., Medical Devices Regulations—MDR, ISO13484 and ISO 27001) [61]. Before the wider introduction of exoskeletons, recommendations are needed on technical issues, how to wear and remove the exoskeletons and how to use them in therapy or as a device to assist the patient’s daily functioning at home.
5.1. Sensor Technology and Data Acquisition
Sensors and artificial intelligence-based solutions are increasingly being used to collect data during activities of daily living, which can be useful in planning and monitoring rehabilitation and controlling adherence to home therapy programs [63].
In a study by Casas et al., immediate improvements in range of motion (ROM) and upper limb function were seen in 50% of hand exoskeleton users, with the most challenging task being the gripping and releasing of various objects [64]. In a subsequent study by Casas et al. [65], nine subjects (69.23%) could not perform functional tasks without assistance and only one showed improvement in task performance with the exoskeleton [65]. Thus, the use of an exoskeleton alone does not guarantee improvement and must be combined with a thoughtful, targeted rehabilitation plan. Another study addressed the use of a hand exoskeleton in a group of post-stroke patients with flexor hypertonia and finger extensor weakness [66]. Such a deficit has a direct negative impact on the opening movement of the hand, and therefore, the correct execution of the grip. The HandSOME (Hand Spring Operated Movement Enhancer) hand exoskeleton supports the patient’s hand opening by stretching the finger joints and compensating for flexor hypertonia. Design, after calibration, was subjected to functional and usability testing with eight post-stroke patients with the above-mentioned hand deficits, which showed an increase in the patients’ range of movement and functional abilities [66]. Sometimes it is necessary to develop a dedicated compact flexible actuator that, however, requires separate validation at the prototype stage [67].
The proposed solution, through the use of cameras, is ready to be used as a data source for digital models, virtual twins and virtual reality (VR). Research by Topini et al. [9] has shown that VR can support patient engagement in therapy, improve the friendliness of the robotic environment, simulate real-life manipulation tasks and modify them in real time, thus increasing the effectiveness of exercises and shaping their support and requirements. Unfortunately, the solution has only been tested on one userso far [68].
Brain-computer interfaces (BCIs) involving the control of hand movement through motor imagery have proven effective, but there are few prototypes due to the high price. One such solution is the Hand Exoskeleton for Rehabilitation Objectives (HERO) combining 3D printing (including 3D-printed actuators that convert the torque of DC motors into a linear force transmitted through Bowden strings) and textiles. Two-dimensional (2D) tracking software and correlation analysis were performed to assess ergonomics. With an exoskeleton weight of 102 g, a classification accuracy of motion intention read from the electroencephalogram of 91.5% was achieved [69]. Such a solution is more difficult in signal analysis [70,71] but more future-proof and ultimately more effective and closer to natural limb control solutions [72,73].
5.2. Mechanical Design Aspects
Support strength and range of movement are key values for a hand exoskeleton. A study by Nazari et al. [74] of the Tenoexo hand exoskeleton showed that a prototype of a lightweight rehabilitation hand exoskeleton combining rigid parts with a soft mechanism could produce a contact force of up to 8 N and overcome a range of motion of 91.5° in 3 s [74]. Other important parameters arehigh power-to-weight ratio and fast start-up time. They are difficult to achieve with traditional solutions; hence, there is a search for new categories of actuators made of highly twisted nylon fibers with a high pitch per cycle with reversible contraction. At the moment, twisted and coiled polymer (TCP) actuators with different nylon fibers require further research but are a promising technology [74].
HandMATE (Hand Movement Support Exoskeleton) showed minimal errors in assisting grip strength (<1%) comparable to the performance of a healthy hand without an exoskeleton. The exoskeleton communicates wirelessly with a tablet (Android operating system) and dedicated software, offering guided exercises, therapeutic games and feedback on the effects of the exoskeleton [75]. Force myography (FMG) control of the hand exoskeleton uses two strands of sensors with a force-sensing resistor (FSR). Sensor arm bands measure forces produced by muscle contraction/relaxation, and hand movements are identified by classifying threshold values [76]. An alternative is to measure the intention of motion by compressing the elastic elements in the actuator. This allows the use of a virtual dynamic system combining user support with maintenanceof motion stability. However, the performance was tested using the integrated one-finger exoskeleton gauntlet mechanism using two types of input motion, making this hand exoskeleton testing system more difficult to use than our proposed one [77].
Monitoring of the patient’s home use of the exoskeleton is facilitated by the recording of sessions and the ability to reproduce the use of the exoskeleton on a virtual twin. It also allows for the assessment of changes in the patient’s health and their functional capabilities, allowing modifications of the rehabilitation plan and the settings/construction of the exoskeleton. Thus, the need for cyclical visits to the clinic is reduced, and the importance of telerehabilitation is increasing (in study [78] with spinal muscular atrophy), reducing the burden on the health care system [78].
The integration of the dexterity of the hand movement in the exoskeleton when performing everyday tasks gives rise to various concepts. In RELAbtenoexo [79], there is a generation using a remote activation system of the four most frequently used grips (individually created for each user). This provides the range of motion and fingertip strength required for 80% of all finger gripping activities. The key factors for acceptance by users were low weight, small size, high comfort of use and attractive appearance [79]. Development (modifications to the family of exoskeletons or modernization with newer elements) remains an important element of the life cycle of the hand exoskeleton [80,81]. In bilateral therapy, the exoskeleton of the deficient hand follows and repeats the movement of the other unaffected hand during bi-handed activity, but this solution has significant limitations due to the fact that both hands are involved in therapy and has a poor translation into everyday life activities [82].
5.3. 3D Printing Techniques
Complex requirements for hand exoskeletons often require unconventional solutions, e.g., modification of a 3D printer to produce three new materials that meet many often conflicting requirements [83]. The importance of solving problems related to the hand exoskeleton is shown by the study of a soft hand exoskeleton designed for spacewalk astronauts to avoid hand fatigue in pressurized EVA gloves (reducing the stiffness of the suit glove). This exoskeleton is based on a set of six flexible actuators with shape memory wire (SMA) as the actuator. The small volume and high force-to-weight ratio made positional and force control testing for healthy, trained users crucial here. Thus, the exoskeleton on hand is a real space supertechnology [84].
Efficiency usually depends on optimizing the combination of technological parameters and material properties. Computational optimization of the 3D printing process using artificial intelligence allows you to balance technical requirements with user safety constraints [85]. The research results so far show that the mere fulfillment of the initial functional requirements by the hand exoskeleton is insufficient, and mechanical complexity (e.g., limited numbers of actuators), susceptibility to modifications (including in CAD) and the ability to adapt to different hand sizes are important [86].
5.4. Control and Actuation Systems
BiomHED (Biomi-metic Hand Exoskeleton Device) uses exotendons that mimic the geometry of the main tendons of the hand. This made it possible to avoid angular displacements of the joints and to better reproduce the spatial coordination patterns required to perform functional tasks [87].
Non-stationarity and susceptibility to artifacts of signals collected from the cerebral cortex so far do not ensure control reliability and safety in everyday use of an exoskeleton controlled in this way, hence, the attempts to combine electroencephalography (EEG) and electrooculography (EEG) into a hybrid interaction system (BNCI). The disadvantage, however, remains the range of motion limited to 25% of the full movement of the grip [88].
In the Hand Exoskeleton Rehabilitation Robot (HEXORR) design [84], the thumb actuator allows for a variable plane of thumb movement (different degrees of extension and adduction/adduction), which places additional demands on the testing/adduction solutions. The average increase in range of movement was significant (43%), which places further demands on the safety of the exoskeleton and not exceeding physiological values [89].
5.5. Human–Computer Interaction
Consideration of recovery requires that the hand exoskeleton test protocols be adapted to both deficient and healthy individuals, regardless of control system and mechanical complexity [90]. Complex functional tasks can cause problems for evaluating their performance during tests. An example of this is the repeated removal of the cap from a water bottle, both with and without the exoskeleton of the hand. Now, it isperformed by measuring the time it takes to complete a task (rather than its accuracy or compliance with natural patterns), and the time in the exoskeleton is five times shorter [91].
In the case of myoelectric pattern recognition for real-time control of the hand exoskeleton, the system constructed by Lu et al. [92,93], based on four channels of surface electromyography signals, detects the user’s intention and classifies it into one of six hand movements within 250 ms, but results on both healthy subjects and SCI patients indicate the need for further research [93].
5.6. Limitations of Current Approach
Personalization of medical devices, especially individually tailored and made by 3D printing (including within the Industry 4.0 and Industry 5.0 paradigm), is a major challenge and a research gap. In accordance with the above-mentioned paradigm, technical control takes place at all stages of planning, design and production, and even the life cycle of a medical device and the range of possible changes in the dimensions of the tested object is significant (possible differences in hand sizes, finger construction or even deformations and/or fingers/digits amputations).
This is a significant research gap in technical sciences (medical informatics, mechanical engineering and biomedical engineering) as well as in clinical practice, which has not found a satisfactory solution so far. This gap must be filled as soon as possible because the market of 3D-printed medical devices is growing dynamically, and it is necessary to automate the process of testing, wearing and selecting 3D-printed rehabilitation supplies.
Despite the personalization of the arm exoskeleton, the procedure for its selection (e.g., for type and level of deficit and type of activity) and testing should be comparable and reproducible. Therefore, there is a need to standardize and structure tests to ensure replication and thus provide a simple, fast, accurate and generally recognized test environment. Ultimately, this will benefit everyone: designers, manufacturers, clinicians and, most importantly, users of arm exoskeletons and their families/carers.
The guidelines for testing require it to be: reproducible, accurate, fast and, in most cases, also versatile (general applicability), i.e., it should not be limited to a selected group of cases, and it should allow testing of both the healthy hand and the hand with a deficit as well as in an exoskeleton, left and right.
So far, robotic devices for the rehabilitation of motor deficits have been studied, especially in stroke patients. It should be noted, however, that most of the tested devices only allow the practice of stereotypical elements of simulated functional tasks in the clinic. In addition, few exoskeletons have been studied so far that can support movements during real functional activities, including at home. Hand exoskeletons, singled out as a subgroup in upper limb exoskeletons and despite significant advances, face several design challenges:
- Achieving the intended size and functional capabilities at the lightest possible weight;
- Ensuring sufficient grip strength;
- Conforming to natural patterns of grasping movements;
- Ensuring the safety of the user’s hands;
- Maintaining short donning (arming) and doffing times in emergency situations;
5.7. Directions for Further Research
In the course of the analysis of the our results and the discussed publications, the following future directions of research can be indicated:
- Increasing the number of tested parameters and, where required, ensuring that it is related to the so-called standards;
- Developing testing standards for individual product groups;
- Wider use of artificial intelligence (including machine learning as a data-driven approach) in data analysis and prediction;
- Inclusion of the proposed solution in wider environments, including defect detection (material and dimensional) or allowing to draw conclusions about the progress of the rehabilitation process of the hand or, in general, the changes in the patient’s health condition
Our proposed solution combines the advantages of two systems and has vision-based and AI-based technical control at each stage of the manufacturing process (or even at each stage of the product life cycle), resulting from the Industry 4.0 paradigm for the personalization of mass-produced medical devices. For the aforementioned reasons, it is a future-proof solution that can be built (in the form of a product family) into scalable manufacturing environments for handheld exoskeletons from clinics and physiotherapy practices to large rehabilitation centers and clinics. In doing so, it represents a variationof medical digital models with a reliance on virtual twins as opposed to current matching and testing concepts, which are mainly based on performing traditional clinimetric tests [96,97,98].
It is encouraging that, in previous studies, even a low-cost 3D-printed exoskeleton has shown effectiveness in supporting users (including stroke patients) during functional assessment and potential for home rehabilitation. Further objectification and improvement of measurement accuracy as well as the development of functional tests carried out by the hand in the exoskeleton in our solution (e.g., gripping and squeezing objects of various shapes, including precise movements) will help to increase the efficiency of the use of exoskeletons and their dissemination, including in patients with hand function. Automation and computerization of research in this area will foster the exchange of data and standardization of research, including in order to create standards and reference values and in difficult areas such as examining the hands of children, people after strokes or people with neurodegenerative diseases, where, for example, tremor occurs [99,100,101].
Standardization of the guidelines and the process itself for the selection, production, life-cycle monitoring and safety of a personalized product of this type should be carried out in accordance with the MDR and the ISO 13485, ISO 10993 and ISO 27001 standards as well as the paradigms of Industry 4.0, Industry 5.0 and the Green Deal. This can create a manufacturing environment operating under constraint satisfaction.
6. Conclusions
Customization of the upper limb exoskeleton means a better fit to the users’ requirements and tracking accuracy of at least 93% but requires an individual approach to assessment, design, production and operation. This poses challenges for the mass production of medical exoskeletons in accordance with MDR and ISO 13485, which in addition should be affordable. The use of AI (ML) to personalize solutions is already a standard procedure at the level of research, adjustment, production and predictive maintenance, but it still requires implementation in the area of life cycle analysis required by MDR and ISO 13485. Optimization of solutions and their thorough clinical validation are required.
The method of personalizing medical devices proposed in the article is part of the natural development of medical devices and legal acts in this area, and it is also consistent with the paradigms of Industry 4.0 (computerization, automatization, robotization and technical control at every stage of product production and service provision), Industry 5.0 (man and his environment are the focus of planning and manufacturing processes) as well as the Green Deal (sustainable development of man and his environment). Such compatibility makes it not only compatible and prospective for many years ahead but also flexible and susceptible to changes depending on the needs. This gives significant opportunities to take advantage of new technologies such as virtual twins and wireless industrial Internet of Things based on LoRAWAN or its successors but also the expected computing revolution using quantum computers, without forgetting about the three pillars of building such systems, i.e., ensuring access to data, cyber security and reasoning and prediction from data based on ethical artificial intelligence.
Author Contributions
Conceptualization, D.M. and I.R.; methodology, D.M., I.R., P.K., J.D. and J.K.; software, D.M., I.R., P.K., J.D. and J.K.; validation, D.M., I.R., P.K., J.D. and J.K.; formal analysis, D.M., I.R., P.K., J.D. and J.K.; investigation, D.M., I.R., P.K., J.D. and J.K.; resources, D.M., I.R., P.K., J.D. and J.K.; data curation, D.M., I.R., P.K., J.D. and J.K.; writing—original draft preparation, D.M., I.R., P.K., J.D. and J.K.; writing—review and editing, D.M., I.R., P.K., J.D. and J.K.; visualization, D.M., I.R., P.K., J.D. and J.K.; supervision, I.R.; project administration, I.R.; funding acquisition, D.M. and I.R. All authors have read and agreed to the published version of the manuscript.
Funding
The work presented in the paper has been financed under a grant to maintain the research potential of Kazimierz Wielki University.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Shahrubudin, N.; Lee, T.C.; Ramlan, R. An Overview on 3D Printing Technology: Technological, Materials, andApplications. Procedia Manuf. 2019, 35, 1286–1296. [Google Scholar] [CrossRef]
- Kantaros, A.; Ganetsos, T.; Piromalis, D. 3D and 4D Printing as Integrated Manufacturing Methods of Industry 4.0. Am. J. Eng. Appl. Sci. 2023, 16, 12–22. [Google Scholar] [CrossRef]
- Schubert, C.; van Langeveld, M.C.; Donoso, L.A. Innovations in 3D printing: A 3D overview from optics to organs. Br. J. Ophthalmol. 2014, 98, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Kantaros, A.; Soulis, E.; Ganetsos, T.; Petrescu, F.I.T. Applying a Combination of Cutting-Edge Industry 4.0 Processes towards Fabricating a Customized Component. Processes 2023, 11, 1385. [Google Scholar] [CrossRef]
- Kantaros, A.; Ganetsos, T.; Piromalis, D. 4D Printing: Technology Overview and Smart Materials Utilized. J. Mechatron. Robot. 2023, 7, 1–14. [Google Scholar] [CrossRef]
- Rojek, I.; Mikołajewski, D.; Dostatni, E.; Kopowski, J. Specificity of 3D Printing and AI-Based Optimization of Medical Devices Using the Example of a Group of Exoskeletons. Appl. Sci. 2023, 13, 1060. [Google Scholar] [CrossRef]
- Böhme, M.; Köhler, H.-P.; Thiel, R.; Jäkel, J.; Zentner, J.; Witt, M. Preliminary Biomechanical Evaluation of a Novel Exoskeleton Robotic System to Assist Stair Climbing. Appl. Sci. 2022, 12, 8835. [Google Scholar] [CrossRef]
- Rojek, I.; Kopowski, J.; Kotlarz, P.; Dorożyński, J.; Dostatni, E.; Mikołajewski, D. Deep Learning in Design of Semi-Automated 3D Printed Chainmail with Pre-Programmed Directional Functions for Hand Exoskeleton. Appl. Sci. 2022, 12, 8106. [Google Scholar] [CrossRef]
- Meng, Q.; Shen, Z.; Nie, Z.; Meng, Q.; Wu, Z.; Yu, H. Modeling and Evaluation of a Novel Hybrid-Driven Compliant Hand Exoskeleton Based on Human-Machine Coupling Model. Appl. Sci. 2021, 11, 10825. [Google Scholar] [CrossRef]
- Echtioui, A.; Mlaouah, A.; Zouch, W.; Ghorbel, M.; Mhiri, C.; Hamam, H. A Novel Convolutional Neural Network Classification Approach of Motor-Imagery EEG Recording Based on Deep Learning. Appl. Sci. 2021, 11, 9948. [Google Scholar] [CrossRef]
- De la Tejera, J.A.; Bustamante-Bello, R.; Ramirez-Mendoza, R.A.; Izquierdo-Reyes, J. Systematic Review of Exoskeletons towards a General Categorization Model Proposal. Appl. Sci. 2021, 11, 76. [Google Scholar] [CrossRef]
- Delgado, P.; Yihun, Y. Integration o Task-Based Exoskeleton with an Assist-as-Needed Algorithm for Patient-Centered Elbow Rehabilitation. Sensors 2023, 23, 2460. [Google Scholar] [CrossRef]
- Zhvansky, D.S.; Sylos-Labini, F.; Dewolf, A.; Cappellini, G.; d’Avella, A.; Lacquaniti, F.; Ivanenko, Y. Evaluation of Spatiotemporal Patterns of the Spinal Muscle Coordination Output during Walking in the Exoskeleton. Sensors 2022, 22, 5708. [Google Scholar] [CrossRef] [PubMed]
- Schabron, B.; Desai, J.; Yihun, Y. Wheelchair-Mounted Upper Limb Robotic Exoskeleton with Adaptive Controller for Activities of Daily Living. Sensors 2021, 21, 5738. [Google Scholar] [CrossRef] [PubMed]
- Vélez-Guerrero, M.A.; Callejas-Cuervo, M.; Mazzoleni, S. Design, Development, and Testing of an Intelligent Wearable Robotic Exoskeleton Prototype for Upper Limb Rehabilitation. Sensors 2021, 21, 5411. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.; Kang, O.; Joe, H.-M. Design of a Payload Adjustment Device for an Unpowered Lower-Limb Exoskeleton. Sensors 2021, 21, 4037. [Google Scholar] [CrossRef]
- Pinheiro, C.; Figueiredo, J.; Magalhães, N.; Santos, C.P. Wearable Biofeedback Improves Human-Robot Compliance during Ankle-Foot Exoskeleton-Assisted Gait Training: A Pre-Post Controlled Study in Healthy Participants. Sensors 2020, 20, 5876. [Google Scholar] [CrossRef] [PubMed]
- Ranavolo, A.; Ajoudani, A.; Cherubini, A.; Bianchi, M.; Fritzsche, L.; Iavicoli, S.; Sartori, M.; Silvetti, A.; Vanderborght, B.; Varrecchia, T.; et al. The Sensor-Based Biomechanical Risk Assessment at the Base of the Need for Revising of Standards for Human Ergonomics. Sensors 2020, 20, 5750. [Google Scholar] [CrossRef]
- Cardona, M.; García Cena, C.E.; Serrano, F.; Saltaren, R. ALICE: Conceptual Development of a Lower Limb Exoskeleton Robot Driven by an On-Board Musculoskeletal Simulator. Sensors 2020, 20, 789. [Google Scholar] [CrossRef] [Green Version]
- Wu, Q.; Wu, H. Development, Dynamic Modeling, and Multi-Modal Control of a Therapeutic Exoskeleton for Upper Limb Rehabilitation Training. Sensors 2018, 18, 3611. [Google Scholar] [CrossRef] [Green Version]
- Dudley, D.R.; Knarr, B.A.; Siu, K.C.; Peck, J.; Ricks, B.; Zuniga, J.M. Testing of a 3D printed hand exoskeleton for an individual with stroke: A case study. Disabil. Rehabil. Assist. Technol. 2021, 16, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Appraisal of Guidelines for Research & Evaluation II (AGREEII). The AGREE Next Steps Consortium 2009, Update 2017. Available online: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf (accessed on 10 April 2023).
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREEII: Advancing guideline development, reporting and evaluation in healthcare. CMAJ 2010, 182, E839–E842. [Google Scholar] [CrossRef] [Green Version]
- Xin, C.; Wei, L.; Guo, X.; Zhang, Y.; Zhang, Y.; Gai, Y. Evidence summary of early rehabilitation of adults with veno-venous extracorporeal membrane oxygenation. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2022, 34, 1041–1047. [Google Scholar] [CrossRef] [PubMed]
- Yin, Q.; Liang, J.; Zhang, Y.; Chen, C.; Yu, W.; Wang, X.; Ji, J. Critical review on quality of methodology and recommendations of clinical practice guidelines for peri-implantitis. BMC Oral Health 2023, 23, 189. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, A.; Arsalani, N.; Fallahi-Khoshknab, M.; Mohammadi-Shahbolaghi, F. The principles of physical restraint use for hospitalized elderly people: An integrated literature review. Syst. Rev. 2021, 10, 129. [Google Scholar] [CrossRef]
- Morone, G.; Palomba, A.; Martino Cinnera, A.; Agostini, M.; Aprile, I.; Arienti, C.; Paci, M.; Casanova, E.; Marino, D.; LaRosa, G.; et al. Systematic review of guidelines to identify recommendations for upper limb robotic rehabilitation after stroke. Eur. J. Phys. Rehabil. Med. 2021, 57, 238–245. [Google Scholar] [CrossRef]
- Jarl, G.; HellstrandTang, U.; Nordén, E.; Johannesson, A.; Rusaw, D.F. Nordic clinical guidelines for orthotic treatment of osteoarthritis of the knee: A systematic review using the AGREE II instrument. Prosthet. Orthot. Int. 2019, 43, 556–563. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Sorrentino, G.; Cassio, A.; Mazzoli, D.; Andrenelli, E.; Bizzarini, E.; Campanini, I.; Carmignano, S.M.; Cerulli, S.; Chisari, C.; et al. Robotic-assisted gait rehabilitation following stroke: A systematic review of current guidelines and practicalclinical recommendations. Eur. J. Phys. Rehabil. Med. 2021, 57, 460–471. [Google Scholar] [CrossRef]
- Kranenborg, S.E.; Greve, C.; Reneman, M.F.; Roossien, C.C. Side-effects and adverse events of a shoulder- and back-support exoskeleton in workers: A systematic review. Appl. Ergon. 2023, 111, 104042. [Google Scholar] [CrossRef]
- Cumplido-Trasmonte, C.; Molina-Rueda, F.; Puyuelo-Quintana, G.; Plaza-Flores, A.; Hernández-Melero, M.; Barquín-Santos, E.; Destarac-Eguizabal, M.A.; García-Armada, E. Satisfaction analysis of over ground gait exoskeletons in people with neurological pathology – a systematic review. J. Neuroeng. Rehabil. 2023, 20, 47. [Google Scholar] [CrossRef]
- Charette, C.; Déry, J.; Blanchette, A.K.; Faure, C.; Routhier, F.; Bouyer, L.J.; Lamontagne, M.E. A Systematic Review of the Determinants of Implementation of a Locomotor Training Program Using a Powered Exoskeleton for Individuals with a SpinalCord Injury. Clin. Rehabil. 2023. [Google Scholar] [CrossRef] [PubMed]
- Stampacchia, G.; Gazzotti, V.; Olivieri, M.; Andrenelli, E.; Bonaiuti, D.; Calabro, R.S.; Carmignano, S.M.; Cassio, A.; Fundaro, C.; Companini, I.; et al. Gait robot-assisted rehabilitation in persons with spinal cord injury: A scoping review. NeuroRehabilitation 2022, 51, 609–647. [Google Scholar] [CrossRef] [PubMed]
- Baldassarre, A.; Lulli, L.G.; Cavallo, F.; Fiorini, L.; Mariniello, A.; Mucci, N.; Arcangeli, G. Industrial exoskeletons from bench to field: Human-machine interface and user experience in occupational settings and tasks. Front. Public Health 2022, 10, 1039680. [Google Scholar] [CrossRef]
- Hunt, M.; Everaert, L.; Brown, M.; Muraru, L.; Hatzidimitriadou, E.; Desloovere, K. Effectivness of robotic exoskeletons for improving gait in children with cerebral palsy: A systematic review. Gait Posture 2022, 98, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Peña Novoa, N.; SuarezDiaz, M.J.; Lis Herrera, K.L. Sanchez Lozano A.L. Feedback strategies in assistive technology to promote social participation in children with cerebral palsy: Systematic review. Rehabilitacion 2022, 56, 364–374. [Google Scholar] [CrossRef]
- Carmignano, S.M.; Fundarò, C.; Bonaiuti, D.; Calabrò, R.S.; Cassio, A.; Mazzoli, D.; Bizzarini, E.; Campanini, I.; Cerulli, S.; Chisari, C.; et al. Robot-assisted gait training in patients with Parkinson’s disease: Implications for clinical practice. A systematic review. NeuroRehabilitation 2022, 51, 649–663. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Lin, F.; Sun, L.; Chen, C. Comparison of Efficacy of Lokomat and Wearable Exoskeleton-Assisted Gait Training in People with Spinal Cord Injury: A Systematic Review and Network Meta-Analysis. Front. Neurol. 2022, 13, 772660. [Google Scholar] [CrossRef]
- Farris, D.J.; Harris, D.J.; Rice, H.M.; Campbell, J.; Weare, A.; Risius, D.; Armstrong, N.; Rayson, M.P. A systematic literature review of evidence for the use of assistive exoskeletons in defence and security use cases. Ergonomics 2023, 66, 61–87. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Cassio, A.; Mazzoli, D.; Andrenelli, E.; Bizzarini, E.; Campanini, I.; Carmignano, S.M.; Cerulli, S.; Chisari, C.; Colombo, V.; et al. What does evidence tell us about the use of gait robotic devices in patients with multiple sclerosis? A comprehensive systematic review on functional outcomes and clinical recommendations. Eur. J. Phys. Rehabil. Med. 2021, 57, 841–849. [Google Scholar] [CrossRef]
- Moggio, L.; de Sire, A.; Marotta, N.; Demeco, A.; Ammendolia, A. Exoskeleton versus end-effector robot-assisted therapy forfinger-hand motor recovery in stroke survivors: Systematic review and meta-analysis. Top. Stroke Rehabil. 2022, 29, 539–550. [Google Scholar] [CrossRef]
- Cumplido, C.; Delgado, E.; Ramos, J.; Puyuelo, G.; Garcés, E.; Destarac, M.A.; Plaza, A.; Hernández, M.; Gutiérrez, A.; García, E. Gait-assisted exoskeletons for children with cerebral palsy or spinal muscular atrophy: A systematic review. NeuroRehabilitation 2021, 49, 333–348. [Google Scholar] [CrossRef] [PubMed]
- Bunge, L.R.; Davidson, A.J.; Helmore, B.R.; Mavrandonis, A.D.; Page, T.D.; Schuster-Bayly, T.R.; Kumar, S. Effectiveness of powered exoskeleton use on gait in individuals with cerebral palsy: A systematic review. PLoS ONE 2021, 16, e0252193. [Google Scholar] [CrossRef] [PubMed]
- Proietti, T.; Guigon, E.; Roby-Brami, A.; Jarrassé, N. Modifying upper-limb inter-joint coordination in healthy subjects by training with a robotic exoskeleton. J Neuroeng Rehabil. 2017, 14, 1–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nedergård, H.; Arumugam, A.; Sandlund, M.; Bråndal, A.; Häger, C.K. Effect of robotic-assisted gait training on objective biomechanical measures of gait in persons post-stroke: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2021, 18, 64. [Google Scholar] [CrossRef] [PubMed]
- Picelli, A.; Capecci, M.; Filippetti, M.; Varalta, V.; Fonte, C.; Di Censo, R.; Zadra, A.; Chignola, I.; Scarpa, S.; Amico, A.P.; et al. Effects of robot-assisted gait training on postural instability in Parkinson’s disease: A systematic review. Eur. J. Phys. Rehabil. Med. 2021, 57, 472–477. [Google Scholar] [CrossRef]
- Bowman, T.; Gervasoni, E.; Amico, A.P.; Antenucci, R.; Benanti, P.; Boldrini, P.; Bonaiuti, D.; Burini, A.; Castelli, E.; Draicchio, F.; et al. What is the impact of robotic rehabilitation on balance and gait outcomes in people with multiple sclerosis? A systematic review of randomized controltrials. Eur. J. Phys. Rehabil. Med. 2021, 57, 246–253. [Google Scholar] [CrossRef]
- Peters, S.E.; Jha, B.; Ross, M. Rehabilitation following surgery for flexor tendon injuries of the hand. Cochrane Database Syst. Rev. 2021, 1, CD012479. [Google Scholar] [CrossRef]
- Lobato Garcia, L.; González González, Y.; Da Cuña Carrera, I.; AlonsoCalvete, A. Benefits of roboticsin gait rehabilitation in cerebral palsy: A systematic review. Rehabilitacion 2020, 54, 128–136. [Google Scholar] [CrossRef]
- Colomera, J.A.; Nahuelhual, P. Effectiveness of robotic assistance for gait training in children with cerebral palsy. A systematic review. Rehabilitacion 2020, 54, 107–115. [Google Scholar] [CrossRef]
- Moucheboeuf, G.; Griffier, R.; Gasq, D.; Glize, B.; Bouyer, L.; Dehail, P.; Cassoudesalle, H. Effects of robotic gait training after stroke: A meta-analysis. Ann. Phys. Rehabil. Med. 2020, 63, 518–534. [Google Scholar] [CrossRef]
- Dijkers, M.P.; Akers, K.G.; Dieffenbach, S.; Galen, S.S. Systematic Reviews of Clinical Benefits of Exoskeleton Use for Gait and Mobility in Neurologic Disorders: A Tertiary Study. Arch. Phys. Med. Rehabil. 2021, 102, 300–313. [Google Scholar] [CrossRef]
- Ghaffar, A.; Dehghani-Sanij, A.A.; Xie, S.Q. A review of gait disorders in the elderly and neurological patients for robot-assisted training. Disabil. Rehabil. Assist. Technol. 2020, 15, 256–270. [Google Scholar] [CrossRef]
- Kermavnar, T.; Power, V.; de Eyto, A.; O’Sullivan, L. Cuff Pressure Algometry in Patients with Chronic Pain as Guidance forCircumferential Tissue Compression for Wearable Soft Exoskeletons: A Systematic Review. Soft Robot. 2018, 5, 497–511. [Google Scholar] [CrossRef] [Green Version]
- Hayes, S.C.; James Wilcox, C.R.; Forbes White, H.S.; Vanicek, N. The effects of robot assisted gait training on temporal-spatial characteristics of people with spinal cord injuries: A systematic review. J. Spinal Cord Med. 2018, 41, 529–543. [Google Scholar] [CrossRef]
- Gandara-Sambade, T.; Fernandez-Pereira, M.; Rodriguez-Sotillo, A. Robotic systems for gait re-education in cases of spinal cord injury: A systematic review. Rev. Neurol. 2017, 64, 205–213. [Google Scholar]
- Highsmith, M.J.; Nelson, L.M.; Carbone, N.T.; Klenow, T.D.; Kahle, J.T.; Hill, O.T.; Maikos, J.T.; Kartel, M.S.; Randolph, B.J. Outcomes Associated with the Intrepid Dynamic Exoskeletal Orthosis (IDEO): A Systematic Review of the Literature. Mil. Med. 2016, 181, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Lefeber, N.; Swinnen, E.; Kerckhofs, E. The immediate effects of robot-assistance on energy consumption and cardiorespiratory load during walking compared to walking with outrobot-assistance: A systematic review. Disabil. Rehabil. Assist. Technol. 2017, 12, 657–671. [Google Scholar] [CrossRef]
- Miller, L.E.; Zimmermann, A.K.; Herbert, W.G. Clinical effectiveness and safety of powered exoskeleton-assisted walking in patients with spinal cord injury: Systematic review with meta-analysis. Med. Devices 2016, 9, 455–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Federici, S.; Meloni, F.; Bracalenti, M.; DeFilippis, M.L. The effectiveness of powered, active lower limb exoskeletons in neurorehabilitation: A systematic review. NeuroRehabilitation 2015, 37, 321–340. [Google Scholar] [CrossRef] [PubMed]
- Mayer, T.A.; Harsch, A.K.; Koska, D.; Hensel-Unger, R.; Maiwald, C. Effects of an active hand exoskeleton on forearm muscle activity in industrial assembly grips. Work 2022, 72, 1577–1591. [Google Scholar] [CrossRef] [PubMed]
- Lieber, J.; Dittli, J.; Lambercy, O.; Gassert, R.; Meyer-Heim, A.; van Hedel, H.J.A. Clinical utility of a pediatric hand exoskeleton: Identifying users, practicability, and acceptance, and recommendations for design improvement. J. Neuroeng. Rehabil. 2022, 19, 17. [Google Scholar] [CrossRef]
- Casas, R.; Martin, K.; Sandison, M.; Lum, P.S. A tracking device for a wearable high-DOF passive hand exoskeleton. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 2021, 6643–6646. [Google Scholar] [CrossRef]
- Casas, R.; Sandison, M.; Chen, T.; Lum, P.S. Clinical Test of a Wearable, High-DOF, Spring Powered Hand Exoskeleton (HandSOMEII). IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1877–1885. [Google Scholar] [CrossRef]
- Chen, J.; Lum, P.S. Pilot testing of the spring operated wearable enhancer for arm rehabilitation (SpringWear). J. Neuroeng. Rehabil. 2018, 15, 13. [Google Scholar] [CrossRef] [PubMed]
- Brokaw, E.B.; Black, I.; Holley, R.J.; Lum, P.S. Hand Spring Operated Movement Enhancer (HandSOME): A portable, passive hand exoskeleton for stroke rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2011, 19, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Refour, E.M.; Sebastian, B.; Chauhan, R.J.; Ben-Tzvi, P. A General Purpose Robotic Hand Exoskeleton with Series Elastic Actuation. J. Mech. Robot. 2019, 11, 060902. [Google Scholar] [CrossRef] [PubMed]
- Topini, A.; Sansom, W.; Secciani, N.; Bartalucci, L.; Ridolfi, A.; Allotta, B. Variable Admittance Control of a Hand Exoskeleton for Virtual Reality-Based Rehabilitation Tasks. Front. Neurorobot. 2022, 15, 789743. [Google Scholar] [CrossRef] [PubMed]
- Araujo, R.S.; Silva, C.R.; Netto, S.P.N.; Morya, E.; Brasil, F.L. Development of a Low-Cost EEG-Controlled Hand Exoskeleton 3D Printed on Textiles. Front. Neurosci. 2021, 15, 661569. [Google Scholar] [CrossRef] [PubMed]
- Kawala-Sterniuk, A.; Pelc, M.; Martinek, R.; Wójcik, G.M. Editorial: Currents in biomedical signals processing - methods and applications. Front. Neurosci. 2022, 16, 989400. [Google Scholar] [CrossRef]
- Schneider, P.; Wójcik, G.M.; Kawiak, A.; Kwaśniewicz, L.; Wierzbicki, A. Modeling and Comparing Brain Processes in Message and Earned Source Credibility Evaluation. Front. Hum. Neurosci. 2022, 16, 808382. [Google Scholar] [CrossRef]
- Martinek, R.; Ladrova, M.; Sidikova, M.; Jaros, R.; Behbehani, K.; Kahankova, R.; Kawala-Sterniuk, A. Advanced Bioelectrical Signal Processing Methods: Past, Present and Future Approach-Part II: Brain Signals. Sensors 2021, 21, 6343. [Google Scholar] [CrossRef] [PubMed]
- Mikolajewska, E.; Mikolajewski, D. Ethical considerations in the use of brain-computer interfaces. Cent. Eur. J. Med. 2013, 8, 720–724. [Google Scholar] [CrossRef]
- Nazari, V.; Pouladian, M.; Zheng, Y.P.; Alam, M. A Compact and Lightweight Rehabilitative Exoskeleton to Restore Grasping Functions for People with Hand Paralysis. Sensors 2021, 21, 6900. [Google Scholar] [CrossRef] [PubMed]
- Bahrami, S.; Dumond, P. Testing of Coiled Nylon Actuators for Use in Spastic Hand Exoskeletons. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2018, 2018, 1853–1856. [Google Scholar] [CrossRef] [PubMed]
- Sandison, M.; Phan, K.; Casas, R.; Nguyen, L.; Lum, M.; Pergami-Peries, M.; Lum, P.S. HandMATE: Wearable Robotic Hand Exoskeleton and Integrated Android App for At Home Stroke Rehabilitation. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2020, 2020, 4867–4872. [Google Scholar] [CrossRef]
- Islam, M.R.U.; Bai, S. Effective Multi-Mode Grasping Assistance Control of a Soft Hand Exoskeleton Using Force Myography. Front. Robot. AI 2020, 7, 567491. [Google Scholar] [CrossRef]
- Chauhan, R.J.; Ben-Tzvi, P. A series elastic actuator design and control in a linkage based hand exoskeleton. In Proceedings of the 2019 Dynamic Systems and Control Conference, Park City, UT, USA, 8–11 October 2019; Volume 3. [Google Scholar] [CrossRef]
- Secciani, N.; Brogi, C.; Pagliai, M.; Buonamici, F.; Gerli, F.; Vannetti, F.; Bianchini, M.; Volpe, Y.; Ridolfi, A. Wearable Robots: An Original Mechatronic Design of a Hand Exoskeleton for Assistive and Rehabilitative Purposes. Front. Neurorobot. 2021, 15, 750385. [Google Scholar] [CrossRef]
- Bützer, T.; Lambercy, O.; Arata, J.; Gassert, R. Fully Wearable Actuated Soft Exoskeleton for Grasping Assistance in Everyday Activities. Soft Robot. 2021, 8, 128–143. [Google Scholar] [CrossRef]
- Rojek, I.; Mikołajewski, D.; Dostatni, E. Digital Twins in Product Lifecycle for Sustainability in Manufacturing and Maintenance. Appl. Sci. 2021, 11, 31. [Google Scholar] [CrossRef]
- Ou, Y.K.; Wang, Y.L.; Chang, H.C.; Chen, C.C. Design and Development of a Wearable Exoskeleton System for Stroke Rehabilitation. Healthcare 2020, 8, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Haghshenas-Jaryani, M.; Pande, C.; Muthu Wijesundara, B.J. Soft Robotic Bilateral Hand Rehabilitation System for Fine Motor Learning. IEEE Int. Conf. Rehabil. Robot. 2019, 2019, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, W.; Harwin, W.; Janko, B.; Bell, G. Multi-Compliance Printing Techniques for the Fabrication of Customisable Hand Exoskeletons. IEEE Int. Conf. Rehabil. Robot. 2019, 2019, 488–493. [Google Scholar] [CrossRef]
- Villoslada, Á.; Rivera, C.; Escudero, N.; Martín, F.; Blanco, D.; Moreno, L. Hand Exo-Muscular System for Assisting Astronauts During Extravehicular Activities. Soft Robot. 2019, 6, 21–37. [Google Scholar] [CrossRef] [PubMed]
- Rojek, I.; Mikołajewski, D.; Dostatni, E.; Macko, M. AI-Optimized Technological Aspects of the Material Used in 3D Printing Processes for Selected Medical Applications. Materials 2020, 13, 5437. [Google Scholar] [CrossRef] [PubMed]
- Almenara, M.; Cempini, M.; Gómez, C.; Cortese, M.; Martín, C.; Medina, J.; Vitiello, N.; Opisso, E. Usability test of a hand exoskeleton for activities of daily living: An example of user-centered design. Disabil. Rehabil. Assist. Technol. 2017, 12, 84–96. [Google Scholar] [CrossRef]
- Lee, S.W.; Landers, K.A.; P ark, H.S. Development of a biomimetic hand exotendon device (BiomHED) for restoration of functional hand movement post-stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 886–898. [Google Scholar] [CrossRef] [Green Version]
- Witkowski, M.; Cortese, M.; Cempini, M.; Mellinger, J.; Vitiello, N.; Soekadar, S.R. Enhancing brain-machine interface (BMI) control of a hand exoskeleton using electrooculography (EOG). J. Neuroeng. Rehabil. 2014, 11, 165. [Google Scholar] [CrossRef] [Green Version]
- Schabowsky, C.N.; Godfrey, S.B.; Holley, R.J. Lum, P. S. Development and pilot testing of HEXORR: Hand EXOskeleton rehabilitation robot. J. Neuroeng. Rehabil. 2010, 7, 36. [Google Scholar] [CrossRef] [Green Version]
- Lince, A.; Celadon, N.; Battezzato, A.; Favetto, A.; Appendino, S.; Ariano, P.; Paleari, M. Design and testing of an under-actuated surface EMG-driven hand exoskeleton. IEEE Int. Conf. Rehabil. Robot. 2017, 2017, 670–675. [Google Scholar] [CrossRef]
- Gasser, B.W.; Bennett, D.A.; Durrough, C.M.; Goldfarb, M. Design and preliminary assessment of Vanderbilt hand exoskeleton. IEEE Int. Conf. Rehabil. Robot. 2017, 2017, 1537–1542. [Google Scholar] [CrossRef]
- Lu, Z.; Chen, X.; Zhang, X.; Tong, K.Y.; Zhou, P. Real-Time Control of an Exoskeleton Hand Robot with Myoelectric Pattern Recognition. Int. J. Neural Syst. 2017, 27, 1750009. [Google Scholar] [CrossRef] [PubMed]
- Mikolajczyk, T.; Mikołajewska, E.; Al-Shuka, H.F.N.; Malinowski, T.; Kłodowski, A.; Pimenov, D.Y.; Paczkowski, T.; Hu, F.; Giasin, K.; Mikołajewski, D.; et al. Recent Advances in Bipedal Walking Robots: Review ofGait, Drive, Sensors and ControlSystems. Sensors 2022, 22, 4440. [Google Scholar] [CrossRef]
- Prokopowicz, P.; Mikołajewski, D.; Mikołajewska, E.; Kotlarz, P. Fuzzy system as an assessment tool for analysis of thehealth-related quality of life for the people after stroke. In Artificial Intelligence and Soft Computing; Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Berlin/Heidelberg, Germany, 2017; Volume 10245, pp. 10–721. [Google Scholar]
- Rojek, I.; Macko, M.; Mikołajewski, D.; Saga, M.; Burczynski, T. Modern methods in the field of machine modeling and simulation as a research and practical issue related to Industry 4.0. Bull. Pol. Acad. Sci. Tech. Sci. 2021, 69, e136719. [Google Scholar] [CrossRef]
- Rojek, I.; Mikołajewski, D.; Macko, M.; Szczepański, Z.; Dostatni, E. Optimization of Extrusion-Based 3D Printing Process Using Neural Networks for Sustainable Development. Materials 2021, 14, 2737. [Google Scholar] [CrossRef]
- Rojek, I.; Mikołajewski, D.; Kotlarz, P.; Macko, M.; Kopowski, J. Intelligent system supporting technological process planning for machining and 3D printing. Bull. Pol. Acad. Sci. Tech. Sci. 2021, 69, e136722. [Google Scholar]
- Aghdam, H.A.; Sanatizadeh, E.; Motififard, M.; Aghadavoudi, F.; Saber-Samandari, S.; Esmaeili, S.; Sheikhbahaei, E.; Safari, M.; Khandan, A. Effect of calcium silicate nanoparticle on surface feature of calcium phosphates hybridbio-nanocomposite usingfor bone substitute application. Powder Technol. 2020, 361, 917–929. [Google Scholar] [CrossRef]
- Jamnezhad, S.; Asefnejad, A.; Motififard, M.; Yazdekhasti, H.; Kolooshani, A.; Saber-Samandari, S.; Khandan, A. Development and investigation of novel alginate-hyaluronic acid bone fillers using freeze drying technique for orthopedic field. Nanomed. Res. J. 2020, 5, 306–315. [Google Scholar] [CrossRef]
- Esmaeili, S.; Shahali, M.; Kordjamshidi, A.; Torkpoor, Z.; Namdari, F.; Samandari, S.S.; Ghadiri Nejad, M.; Khandan, A. An artificial blood vessel fabricated by 3D printing for pharmaceutical application. Nanomed. J. 2019, 6, 183–194. [Google Scholar] [CrossRef]
Figure 1.
Basic areas of upper limb exoskeleton personalizationespecially due to AI use.

Figure 2.
Operation of the research cage: (a) general, (b) top view, (c) side view and (d) front view.
Figure 2.
Operation of the research cage: (a) general, (b) top view, (c) side view and (d) front view.



{kind=link}
{kind=link}
{kind=link}
Table 1.
Scores of appraisal according to the AGREE II.
| Domain 1: Scope and Purpose | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Item 1 | Item 2 | Item 3 | - | - | - | - | - | Total | |
| Appraiser 1 | 5 | 6 | 6 | - | - | - | - | - | 17 |
| Appraiser 2 | 6 | 6 | 7 | - | - | - | - | - | 19 |
| Total | 11 | 12 | 13 | - | - | - | - | - | 36 |
| Scaled domain score: 36/42 (85.71%) | |||||||||
| Domain 2: Stakeholder involvement | |||||||||
| Item 4 | Item 5 | Item 6 | - | - | - | - | - | Total | |
| Appraiser 1 | 5 | 5 | 6 | - | - | - | - | - | 16 |
| Appraiser 2 | 5 | 6 | 6 | - | - | - | - | - | 17 |
| Total | 10 | 11 | 12 | - | - | - | - | - | 33 |
| Scaled domain score: 33/42 (78.57%) | |||||||||
| Domain 3: Rigor of development | |||||||||
| Item 7 | Item 8 | Item 9 | Item 10 | Item 11 | Item 12 | Item 13 | Item 14 | Total | |
| Appraiser 1 | 5 | 5 | 6 | 5 | 5 | 6 | 5 | 5 | 42 |
| Appraiser 2 | 5 | 6 | 6 | 5 | 6 | 6 | 5 | 6 | 45 |
| Total | 10 | 11 | 12 | 10 | 11 | 12 | 10 | 11 | 87 |
| Scaled domain score: 87/112 (77.68%) | |||||||||
| Domain 4: Clarity of presentation | |||||||||
| Item 15 | Item 16 | Item 17 | - | - | - | - | - | Total | |
| Appraiser 1 | 5 | 5 | 6 | - | - | - | - | - | 16 |
| Appraiser 2 | 6 | 6 | 7 | - | - | - | - | - | 19 |
| Total | 11 | 11 | 13 | - | - | - | - | - | 35 |
| Scaled domain score: 35/42 (83.33%) | |||||||||
| Domain 5: Applicability | |||||||||
| Item 18 | Item 19 | Item 20 | Item 21 | - | - | - | - | Total | |
| Appraiser 1 | 5 | 5 | 5 | 5 | - | - | - | - | 20 |
| Appraiser 2 | 6 | 6 | 6 | 5 | - | - | - | - | 23 |
| Total | 11 | 11 | 11 | 10 | - | - | - | - | 43 |
| Scaled domain score: 43/56 (76.79%) | |||||||||
| Domain 6: Editorial independence | |||||||||
| Item 22 | Item 23 | - | - | - | - | - | - | Total | |
| Appraiser 1 | 6 | 6 | - | - | - | - | - | - | 12 |
| Appraiser 2 | 6 | 7 | - | - | - | - | - | - | 13 |
| Total | 12 | 13 | - | - | - | - | - | - | 25 |
| Scaled domain score: 25/26 (96.15%) | |||||||||
Table 2.
Case studies or examples where personalized 3D-printed upper limb exoskeletons have been successfully applied in real-life scenarios.
Table 2.
Case studies or examples where personalized 3D-printed upper limb exoskeletons have been successfully applied in real-life scenarios.
| Name | Outcomes | Limitations | Potential Benefits |
|---|---|---|---|
| Selection of materials for the exoskeleton | Calculation speed increased by up to 1.5 times while maintaining the same print quality | Need for deep learning based solutions application | Shorter lead times, improved quality and new and better sets of printing parameters |
| Analysis of patient data for exoskeleton selection | Faster and more efficient:
| The need for AI-based solutions applied to data collection. | Reducing the time and cost of patient services. |
| Design of an exoskeleton using a digital twin | Monitoring of processes and process parameters allows continuous improvement of existing processes in terms of intelligent eco-design and planning and monitoring of production processes | It is necessary to use simulation models to improve physical tasks and processes | Effective in the context of sustainable production and maintenance |
| AI-based optimization of 3D printing | Obtaining even one free print after every seven prints (i.e., from materials that were previously wasted) | Need to implement improved AI-based design and injection simulation | Reduced consumption, material savings, reduced waste and reduced environmental impact |
| Automated or semi-automated efficient and practical design of 3D-printed chainmail for exoskeletons with programmed properties | Personalized mechanical parameters such as stiffness and flexion angles in different directionsto suit the needs and goals of the therapy for a specific patient | The need to combine the use of real-world data from hand exoskeleton research and new methods to analyze it using deep neural networks, with a clear and scalable 3D-printed fabric product design | Better reflect individual user needs, including different types and degrees of deficit |
| AI-based analysis of the harm caused by 3D printing | Program shall specify whether and what precautions are to be taken | Estimating the amount of pollution generated by 3D printing systems requires accurate data | A self-learning programme that will improve as more data is entered—complementing previously used metric |
| Optimization of the therapy programme using the exoskeleton | Integration of the exoskeleton in medical automation and robotics systems, including for telemedicine purposes | Different types and levels of motor skill deficits in the hand (or both hands) can occur as a result of multiple injuries and neurological and neurodegenerative diseases | Remote monitoring helps with early diagnosis and early intervention within the framework of preventive medicine (medicine for healthy people) and also inpeople involved in intensive sport. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Mikołajewski, D.; Rojek, I.; Kotlarz, P.; Dorożyński, J.; Kopowski, J. Personalization of the 3D-Printed Upper Limb Exoskeleton Design—Mechanical and IT Aspects. Appl. Sci. 2023, 13, 7236. https://doi.org/10.3390/app13127236
AMA Style
Mikołajewski D, Rojek I, Kotlarz P, Dorożyński J, Kopowski J. Personalization of the 3D-Printed Upper Limb Exoskeleton Design—Mechanical and IT Aspects. Applied Sciences. 2023; 13(12):7236. https://doi.org/10.3390/app13127236
Chicago/Turabian StyleMikołajewski, Dariusz, Izabela Rojek, Piotr Kotlarz, Janusz Dorożyński, and Jakub Kopowski. 2023. "Personalization of the 3D-Printed Upper Limb Exoskeleton Design—Mechanical and IT Aspects" Applied Sciences 13, no. 12: 7236. https://doi.org/10.3390/app13127236
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.