Measurement of Serum Testosterone in Nondiabetic Young Obese Men: Comparison of Direct Immunoassay to Liquid Chromatography-Tandem Mass Spectrometry

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Study Samples
2.3. Testosterone Analysis
2.3.1. Immunoassay
2.3.2. LC-MS/MS
2.4. Definition of Hypoandrogenemia
2.5. Ethical Approval
2.6. Statistical Analysis
3. Results
3.1. Cohort Descriptive Characteristics
3.2. IA and LC-MS/MS Assessment
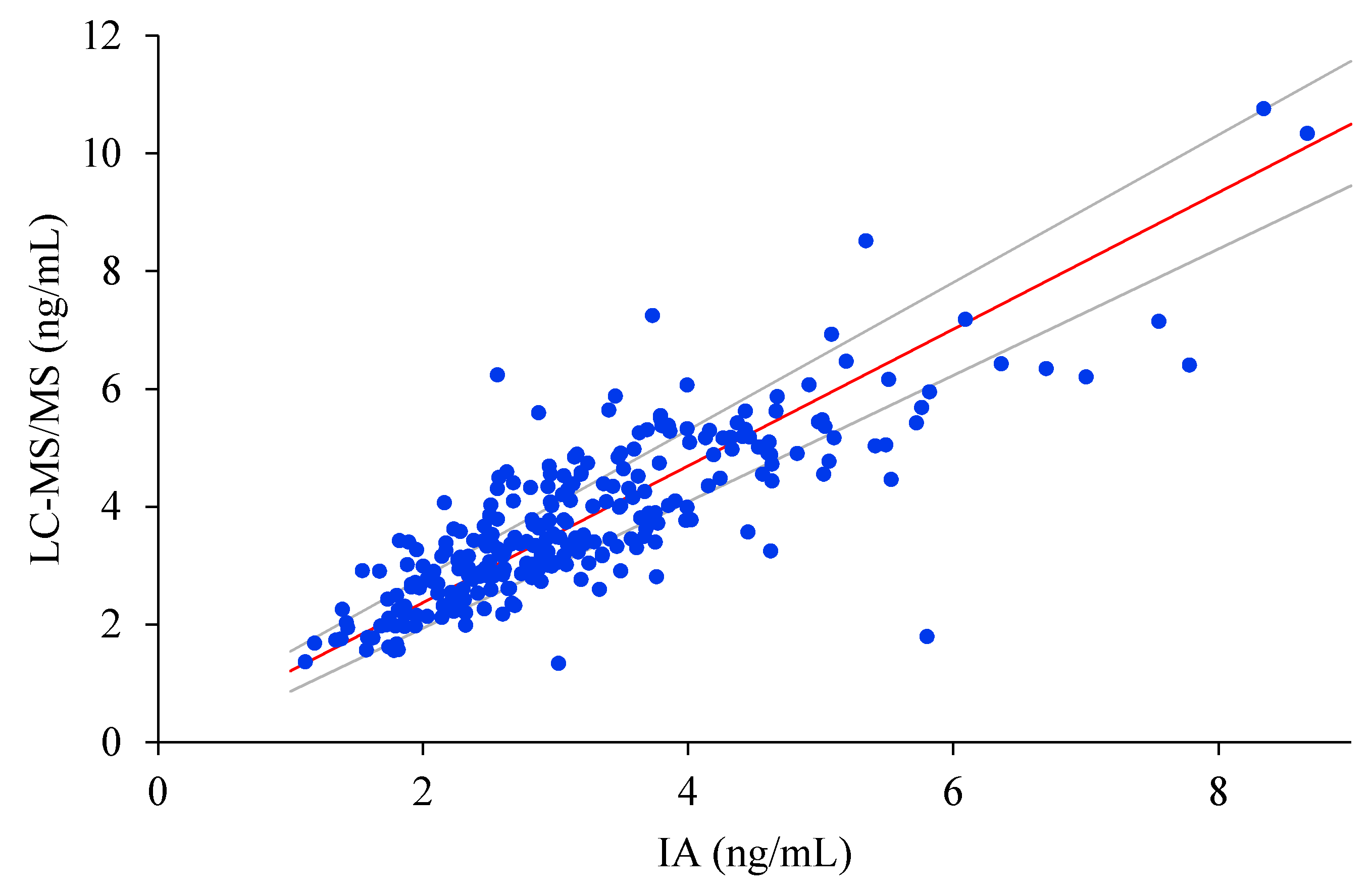
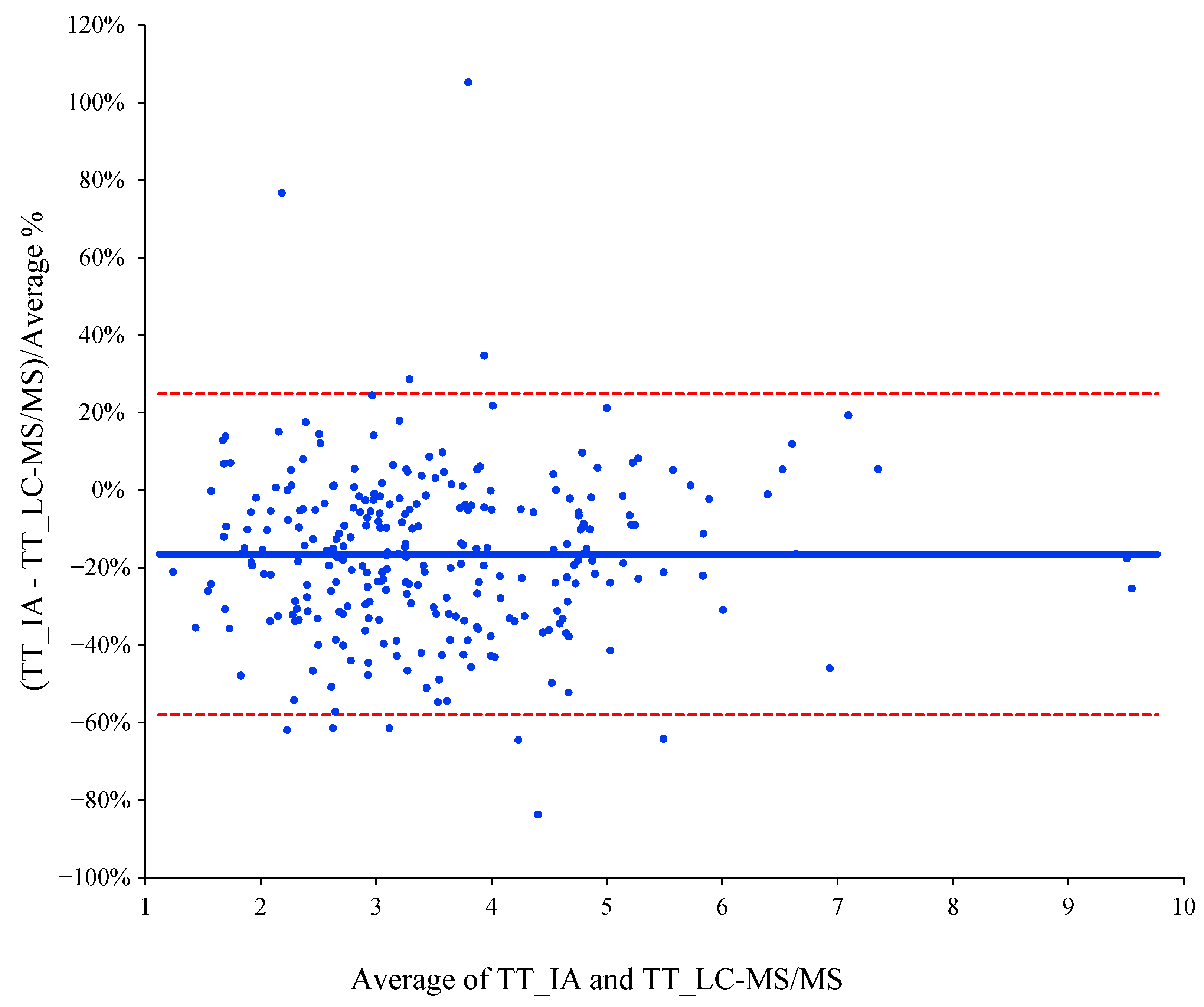
3.3. Correlation and Agreement between IA and LC-MS/MS
3.4. Impact of Assay Performance on Clinical Assessment
3.5. Factors Involved in Testosterone Determination Disagreement
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Liu, P.Y.; Iranmanesh, A.; Nehra, A.X.; Keenan, D.M.; Veldhuis, J.D. Mechanisms of hypoandrogenemia in healthy aging men. Endocrinol. Metab. Clin. 2005, 34, 935–955. [Google Scholar] [CrossRef]
- Zarotsky, V.; Huang, M.Y.; Carman, W.; Morgentaler, A.; Singhal, P.K.; Coffin, D.; Jones, T.H. Systematic literature review of the risk factors, comorbidities, and consequences of hypogonadism in men. Andrology 2014, 2, 819–834. [Google Scholar] [CrossRef]
- Dhindsa, S.; Miller, M.G.; McWhirter, C.L.; Mager, D.E.; Ghanim, H.; Chaudhuri, A.; Dandona, P. Testosterone Concentrations in Diabetic and Nondiabetic Obese Men. Diabetes Care 2010, 33, 1186–1192. [Google Scholar] [CrossRef] [Green Version]
- Feldman, H.A.; Longcope, C.; Derby, C.A.; Johannes, C.B.; Araujo, A.B.; Coviello, A.D.; Bremner, W.J.; McKinlay, J.B. Age Trends in the Level of Serum Testosterone and Other Hormones in Middle-Aged Men: Longitudinal Results from the Massachusetts Male Aging Study. J. Clin. Endocrinol. Metab. 2002, 87, 589–598. [Google Scholar] [CrossRef]
- Lamm, S.; Chidakel, A.; Bansal, R. Obesity and Hypogonadism. Urol. Clin. 2016, 43, 239–245. [Google Scholar] [CrossRef]
- Molina-Vega, M.; Muñoz-Garach, A.; Damas-Fuentes, M.; Fernández-García, J.C.; Tinahones, F.J. Secondary male hypogonadism: A prevalent but overlooked comorbidity of obesity. Asian J. Androl. 2018, 20, 531–538. [Google Scholar]
- Molina-Vega, M.; Asenjo-Plaza, M.; García-Ruiz, M.C.; Varea-Marineto, E.; Casal-Nievas, N.; Álvarez-Millán, J.J.; Cabezas-Sanchez, P.; Cardona-Díaz, F.; Queipo-Ortuño, M.I.; Castellano-Castillo, D.; et al. Cross-Sectional, Primary Care–Based Study of the Prevalence of Hypoandrogenemia in Nondiabetic Young Men with Obesity. Obesity 2019, 27, 1584–1590. [Google Scholar] [CrossRef]
- Bhasin, S.; Brito, J.P.; Cunningham, G.R.; Hayes, F.J.; Hodis, H.N.; Matsumoto, A.M.; Snyder, P.J.; Swerdloff, R.S.; Wu, F.C.; Yialamas, M.A. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2018, 103, 1715–1744. [Google Scholar] [CrossRef] [Green Version]
- Rosner, W.; Auchus, R.J.; Azziz, R.; Sluss, P.M.; Raff, H. Utility, Limitations, and Pitfalls in Measuring Testosterone: An Endocrine Society Position Statement. J. Clin. Endocrinol. Metab. 2007, 92, 405–413. [Google Scholar] [CrossRef]
- Handelsman, D.J. Mass spectrometry, immunoassay and valid steroid measurements in reproductive medicine and science. Hum. Reprod. 2017, 32, 1147–1150. [Google Scholar] [CrossRef] [Green Version]
- Demers, L.M. Androgen deficiency in women; role of accurate testosterone measurements. Maturitas 2010, 67, 39–45. [Google Scholar] [CrossRef]
- Huhtaniemi, I.T.; Tajar, A.; Lee, D.M.; O’Neill, T.W.; Finn, J.D.; Bartfai, G.; Boonen, S.; Casanueva, F.F.; Giwercman, A.; Han, T.S.; et al. Comparison of serum testosterone and estradiol measurements in 3174 European men using platform immunoassay and mass spectrometry; relevance for the diagnostics in aging men. Eur. J. Endocrinol. 2012, 166, 983–991. [Google Scholar] [CrossRef]
- Taieb, J.; Mathian, B.; Millot, F.; Patricot, M.C.; Mathieu, E.; Queyrel, N.; Lacroix, I.; Somma-Delpero, C.; Boudou, P. Testosterone measured by 10 immunoassays and by isotope-dilution gas chromatography-mass spectrometry in sera from 116 men, women, and children. Clin. Chem. 2003, 49, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Comas, I.; Ferrer, R.; Planas, J.; Celma, A.; Regis, L.; Morote, J. A systematic review of methods for quantifying serum testosterone in patients with prostate cancer who underwent castration. Actas Urol. Esp. 2018, 42, 86–93. [Google Scholar] [CrossRef] [PubMed]
- La’ulu, S.L.; Kalp, K.J.; Straseski, J.A. How low can you go? Analytical performance of five automated testosterone immunoassays. Clin. Biochem. 2018, 58, 64–71. [Google Scholar]
- Sikaris, K.; McLachlan, R.I.; Kazlauskas, R.; de Kretser, D.; Holden, C.A.; Handelsman, D.J. Reproductive hormone reference intervals for healthy fertile young men: Evaluation of automated platform assays. J. Clin. Endocrinol. Metab. 2005, 90, 5928–5936. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Catlin, D.H.; Demers, L.M.; Starcevic, B.; Swerdloff, R.S. Measurement of total serum testosterone in adult men: Comparison of current laboratory methods versus liquid chromatography-tandem mass spectrometry. J. Clin. Endocrinol. Metab. 2004, 89, 534–543. [Google Scholar] [CrossRef] [Green Version]
- Stanczyk, F.Z.; Clarke, N.J. Advantages and challenges of mass spectrometry assays for steroid hormones. J. Steroid Biochem. Mol. Biol. 2010, 121, 491–495. [Google Scholar] [CrossRef]
- Handelsman, D.J.; Wartofsky, L. Requirement for Mass Spectrometry Sex Steroid Assays in the Journal of Clinical Endocrinology and Metabolism. J. Clin. Endocrinol. Metab. 2013, 98, 3971–3973. [Google Scholar] [CrossRef] [Green Version]
- Kanakis, G.A.; Tsametis, C.P.; Goulis, D.G. Measuring testosterone in women and men. Maturitas 2019, 125, 41–44. [Google Scholar] [CrossRef]
- Taylor, A.E.; Keevil, B.; Huhtaniemi, I.T. Mass spectrometry and immunoassay: How to measure steroid hormones today and tomorrow. Eur. J. Endocrinol. 2015, 173, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gayoso-Diz, P.; Otero-González, A.; Rodriguez-Alvarez, M.X.; Gude, F.; García, F.; De Francisco, A.; Quintela, A.G. Insulin resistance (HOMA-IR) cut-off values and the metabolic syndrome in a general adult population: Effect of gender and age: EPIRCE cross-sectional study. BMC Endocr. Disord. 2013, 13, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhasin, S.; Pencina, M.; Jasuja, G.K.; Travison, T.G.; Coviello, A.; Orwoll, E.; Wang, P.Y.; Nielson, C.; Wu, F.; Tajar, A.; et al. Reference Ranges for Testosterone in Men Generated Using Liquid Chromatography Tandem Mass Spectrometry in a Community-Based Sample of Healthy Nonobese Young Men in the Framingham Heart Study and Applied to Three Geographically Distinct Cohorts. J. Clin. Endocrinol. Metab. 2011, 96, 2430–2439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermeulen, A.; Verdonck, L.; Kaufman, J.M. A critical evaluation of simple methods for the estimation of free testosterone in serum. J. Clin. Endocrinol. Metab. 1999, 84, 3666–3672. [Google Scholar] [CrossRef]
- Montagna, G.; Balestra, S.; D’Aurizio, F.; Romanelli, F.; Benagli, C.; Tozzoli, R.; Risch, L.; Giovanella, L.; Imperiali, M. Establishing normal values of total testosterone in adult healthy men by the use of four immunometric methods and liquid chromatography-mass spectrometry. Clin. Chem. Lab. Med. 2018, 56, 1936–1944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCartney, C.R.; Burt Solorzano, C.M.; Patrie, J.T.; Marshall, J.C.; Haisenleder, D.J. Estimating testosterone concentrations in adolescent girls: Comparison of two direct immunoassays to liquid chromatography-tandem mass spectrometry. Steroids 2018, 140, 62–69. [Google Scholar] [CrossRef]
- Cabarkapa, S.; Perera, M.; Sikaris, K.; O’Brien, J.S.; Bolton, D.M.; Lawrentschuk, N. Reporting and ideal testosterone levels in men undergoing androgen deprivation for prostate cancer—Time for a rethink? Prostate Int. 2018, 6, 1–6. [Google Scholar] [CrossRef]
- Janse, F.; Eijkemans, M.J.; Goverde, A.J.; Lentjes, E.G.; Hoek, A.; Lambalk, C.B.; Hickey, T.E.; Fauser, B.C.; Norman, R.J. Assessment of androgen concentration in women: Liquid chromatography-tandem mass spectrometry and extraction RIA show comparable results. Eur. J. Endocrinol. 2011, 165, 925–933. [Google Scholar] [CrossRef] [Green Version]
- Cao, Z.T.; Botelho, J.C.; Rej, R.; Vesper, H. Accuracy-based proficiency testing for testosterone measurements with immunoassays and liquid chromatography-mass spectrometry. Clin. Chim. Acta 2017, 469, 31–36. [Google Scholar] [CrossRef] [Green Version]
- Tsametis, C.P.; Isidori, A.M. Testosterone replacement therapy: For whom, when and how? Metabolism 2018, 86, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Hackbarth, J.S.; Hoyne, J.B.; Grebe, S.K.; Singh, R.J. Accuracy of calculated free testosterone differs between equations and depends on gender and SHBG concentration. Steroids 2011, 76, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Handelsman, D.J. Free Testosterone: Pumping up the Tires or Ending the Free Ride? Endocr. Rev. 2017, 38, 297–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Mean ± SD | Median (p 50) | p 2.5 | p 97.5 |
|---|---|---|---|---|
| Age—years | 37.2 ± 7.8 | 38 | 21.00 | 49.15 |
| BMI—kg/m2 | 39.0 ± 6.8 | 37.63 | 30.55 | 56.73 |
| WC—cm | 124.2 ± 15.3 | 122 | 101.9 | 160 |
| Fat mass—% | 42.62 ± 14.79 | 39.6 | 23.14 | 78.57 |
| Glucose—mg/dl | 93.1 ± 10.0 | 91 | 78.00 | 122.3 |
| Insulin—uIU/mL | 20.1 ±15.4 | 16.93 | 6.44 | 51.42 |
| HbA1c—% | 5.4 ± 0.4 | 5.4 | 4.78 | 6.2 |
| hs-CRP—mg/dl | 3.45 ± 5.97 | 1.77 | 0.17 | 34.99 |
| LH—mUI/mL | 3.86 ± 2.11 | 3.39 | 1.31 | 8.14 |
| TT (IA)—ng/mL | 3.20 ± 1.24 | 2.95 | 1.43 | 6.41 |
| TT (LC-MS/MS)—ng/mL | 3.78 ± 1.40 | 3.46 | 1.67 | 6.96 |
| SHBG—nmol/L | 25.9 ± 12.7 | 23.5 | 9.90 | 55.32 |
| FT (LC-MS/MS)—pg/mL | 90.17 ± 30.9 | 86.6 | 42.03 | 169 |
| FT (IA)—pg/mL | 74.7 ± 26.9 | 69.1 | 32.56 | 143.9 |
| Assay | Mean ± SD | Range | LoD | LoQ | Imprecision | Accuracy | |||
|---|---|---|---|---|---|---|---|---|---|
| Low | High | ng/mL | CV% Intraassay | CV% Interassay | % | ||||
| IA | 3.20 ± 1.24 | 1.11 | 8.67 | 0.033 | 0.062 | 0.98 | 2.6 | 7.24 | 106.1 |
| 4.1 | 4.7 | 6.69 | |||||||
| 8.89 | 3.4 | 7.57 | |||||||
| LC-MS/MS | 3.78 ± 1.4 | 1.35 | 10.76 | 0.024 | 0.073 | 0.2 | 2.09 | 8.43 | 103.7 |
| 1.49 | 3.67 | 2.64 | |||||||
| 8.08 | 1.64 | 2.64 | |||||||
| Multivariate | |||
|---|---|---|---|
| OR | 95% CI | p | |
| Age—years | 0.985 | 0.949–1.022 | 0.432 |
| HOMA-IR > 1.85 | 2.978 | 1.092–8.115 | 0.033 |
| Fat mass—% | 0.989 | 0.944–1.037 | 0.657 |
| SHBG—nmol/L | 1.042 | 1.015–1.070 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Escribano, A.; Maroto-García, J.; Ruiz-Galdón, M.; Barrios-Rodríguez, R.; Álvarez-Millán, J.J.; Cabezas-Sánchez, P.; Plaza-Andrades, I.; Molina-Vega, M.; Tinahones, F.J.; Queipo-Ortuño, M.I.; et al. Measurement of Serum Testosterone in Nondiabetic Young Obese Men: Comparison of Direct Immunoassay to Liquid Chromatography-Tandem Mass Spectrometry. Biomolecules 2020, 10, 1697. https://doi.org/10.3390/biom10121697
Martínez-Escribano A, Maroto-García J, Ruiz-Galdón M, Barrios-Rodríguez R, Álvarez-Millán JJ, Cabezas-Sánchez P, Plaza-Andrades I, Molina-Vega M, Tinahones FJ, Queipo-Ortuño MI, et al. Measurement of Serum Testosterone in Nondiabetic Young Obese Men: Comparison of Direct Immunoassay to Liquid Chromatography-Tandem Mass Spectrometry. Biomolecules. 2020; 10(12):1697. https://doi.org/10.3390/biom10121697
Chicago/Turabian StyleMartínez-Escribano, Ana, Julia Maroto-García, Maximiliano Ruiz-Galdón, Rocío Barrios-Rodríguez, Juan J. Álvarez-Millán, Pablo Cabezas-Sánchez, Isaac Plaza-Andrades, María Molina-Vega, Francisco J. Tinahones, María Isabel Queipo-Ortuño, and et al. 2020. "Measurement of Serum Testosterone in Nondiabetic Young Obese Men: Comparison of Direct Immunoassay to Liquid Chromatography-Tandem Mass Spectrometry" Biomolecules 10, no. 12: 1697. https://doi.org/10.3390/biom10121697